Embed Size (px)
Citation preview
Development of a New Glaucoma Drainage Device
Mr Kin Sheng Lim m b chB FRCOphth
2001
Thesis for the degree o f
Doctor of Medicine (MD)
University o f London
Biomaterials Research GroupDepartment of Pharmacy University of Brighton Cockcroft Building Brighton BN2 4GJ
Wound Healing Research GroupDepartment of Pathology & Glaucoma Institute of Ophthalmology & Moorfields Eye Hospital Bath Street London EClV 9EL

ProQuest Number: U642114
All rights reserved
INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uest.
ProQuest U642114
Published by ProQuest LLC(2015). Copyright of the Dissertation is held by the Author.
All rights reserved.This work is protected against unauthorized copying under Title 17, United States Code.
Microform Edition © ProQuest LLC.
ProQuest LLC 789 East Eisenhower Parkway
P.O. Box 1346 Ann Arbor, Ml 48106-1346

TABLE OF CONTENTSA B S T R A C TA C K N O W L E D G E M E N T SS T A T E M E N T O F O R G IN A L IT Y A N D P U B L IC A T IO N S A R IS IN G FR O M T H E T H E SIS
CHAPTER ONE - Introduction1.1 Definition o f Glaucoma1.2 Classification1.3 Prevalence o f Glaucoma1.4 Disease Mechanism1.5 Adequate Pressure Reduction1.6 The Need for a New Glaucoma Filtration Procedure1.7 Glaucoma Drainage Devices
1.7.1 Early Devices1.7.2 Contemporary Devices
1.8 Evaluation o f Results1.9 Complication Mechanisms
1.9.1. Poor Flow Control1.9.1.1 Devices with No Resistance Mechanism1.9.1.2 Devices with No Set Resistance1.9.1.3 Devices with Set Resistance
1.9.2 Poor Tissue Compatibility1.10 Strategies to Improve Success Rates
1.10.1 Plate Surface Area1.10.2 Antimetabolites
1.11 Current Indications1.12 New Design Concepts
1.12.1 Tube without Plate1.12.2 New Biomaterial
1.13 The Future
CHAPTER TW O - Design Changes to Control FlowAbstract2.1 Introduction2.2 Fluid Mechanics2.3 Materials & Methods (Internal Flow Control)
2.3.1 Preparation o f Polyimide discs & Excimer Laser Ablations2.3.2 Flow Rig2.3.3 Scanning Electron Microscopy & Image Analysis
2.4 Materials & Methods (External Flow Control)2.4.1 Artificial Anterior Chamber2.4.2 Occluded Device Implantation
2.5 Results2.6 Discussions2.7 Conclusions
CHAPTER THREE - Biocompatibility StudiesAbstract3.1 Introduction3.2 Bioinert Materials
3.2.1 Heparin Coating3.2.2 Surface Passivation3.2.3 Hydrogels3.2.4 Polyethylene Oxide Polymers3.2.5 Biomimetic Bioinert Materials
3.3 Biocompatibility in the Context o f Glaucoma Drainage Devices3.3.1 Protein & Cell Adhesion - Tube Occlusion3.3.2 Protein & Cell Adhesion - Chronic Inflammation & Bleb
Fibrosis3.3.3 Cell Damage - Endothelial Failure3.3.4 Bacteria Adhesion - Endophthalmitis
3.4 Aims3.5 Materials & Methods
3.5.1 Preparation o f Discs3.5.2 Cell & Protein Adhesion
3.5.2.1 Fibrinogen Adsorption3.5.2.2 Fibrin Adhesion3.5.2.3 Human Scleral Fibroblast Adhesion3.5.2.4 Macrophage Adhesion3.5.2.5 Data Analysis
3.5.3 Endothelial Damage3.5.4 Bacteria Adhesion
3.6 Results3.6.1 Protein & Cell Adhesion3.6.2 Endothelial Damage3.6.3 Bacteria Adhesion
3.7 Discussion3.7.1 Choice o f Biomaterials3.7.2 Cell & Protein Adhesion3.7.3 Endothelial Damage3.7.4 Bacteria Adhesion
3.8 Conelusion
CHAPTER FOUR - Prototyping & In Vivo StudyAbstract4.1 Introduction4.2 Materials & Methods
4.2.1 Prototyping4.2.2 Flow Rig4.2.3 Implantation o f Prototype Glaucoma Drainage Device4.2.4 Follow-up Examination4.2.5 Sacrifice
4.3 Results4.3.1 Pre-operative Flow Testing4.3.2 Adverse Reactions4.3.3 Intraocular Pressure

4.4 Discussion4.5 Conclusion
CHAPTER FIVE - Concluding Discussion & Future Development5.1 Discussion5.2 Future Development
5.2.1 Extrusion Moulding & Hot Drawing5.2.2 Photolithography
5.3 Conclusion
REFERENCES
APPENDICES

ABSTRACT
Glaucoma filtration surgery has been shown to be more effective at preventing disease
progression than other primary treatment modalities in open angle glaucoma. If it
were possible to avoid complications associated with poor flow control, primary
glaucoma filtration surgery would probably be offered more widely. Trabeculectomy,
the procedure o f choice in conventional glaucoma filtration surgery, has remained
essentially unchanged for over a quarter o f a century. Local control over wound
healing with antimetabolite agents such as 5-fluorouracil and mitomycin C has
improved the prognosis for cases with high risk o f filtration failure; but flow control
remains imprecise despite the introduction o f a variety o f suture adjustment
techniques. Glaucoma drainage devices have the potential to regulate flow
consistently, eliminating hypotony after surgery. Design, material, and manufacturing
deficiencies have left this potential unfulfilled in existing glaucoma drainage devices,
all o f which exhibit problems with poor flow control and suboptimal tissue
compatibility.
This thesis will examine whether a new flow resistor produced by excimer laser
ablation in a polymer substrate and a new external glaucoma drainage device design
could prevent hypotony in a series o f in vitro experiments and a limited in vivo study.
It will also investigate whether phosphorylcholine coating o f polymethyl methacrylate
can reduce the adhesion o f cells and proteins compared to current biomaterials used in
the construction o f glaucoma drainage devices.

PUBLICATIONS AND PRESENTATIONS ARISING FROM THE THESIS & STATEMENT OF ORIGINALITY
Publications
Glaucoma filtration implants. Past, present and future.Lim KS, Allan B, Muir A, Lloyd AW, Khaw FT.British Journal o f Ophthalmology 1998;82(9); 1083-1089
Cell and protein adhesion studies in glaucoma drainage device development Lim KS, Allan B, Muir A, Lloyd AW, Khaw FT, et al.British Journal o f Ophthalmology 1999; 83: 1168-1171
Experimental flow studies in the development o f glaucoma drainage device Lim KS, Allan B, Muir A, Lloyd AW, Khaw FT, et al.British Journal o f Ophthalmology (in press)
Glaucoma valves: Truth versus myth II Lim KS, Allan B, Khaw FT.Ophthalmology (in press)
Comeal endothelial cell damage fi"om glaucoma drainage devices’ materials Lim KS, Allan B, Muir A, Lloyd AW, Khaw FT, et al.Submitted to Cornea
Presentations
Biomimetic coatings to reduce fibrin blockage o f glaucoma filtration implants.Allan B, Lim KS, Dropcova S, Muir A, Lloyd AW, Khaw FT, et al. 1997 Investigative Ophthalmology & Visual Science', 38(4):1252-1252
Consistent Flow Control in a New Glaucoma Filtration Implant.Lim KS, Allan B, Muir A, Lloyd AW, Khaw FT, et al. 1998 Investigative Ophthalmology & Visual Science', 39(4):2176-S475
In Vitro Ocular Compatibility o f Glaucoma Filtration Implant Materials.Denyer SF, Lim KS, Faragher RGA, Allan B, Muir A, Lloyd AW, Khaw FT, et al. 1998 Investigative Ophthalmology & Visual Science', 39(4):2176-S475
Comeal Endothelial Cell DamageLim KS, Allan B, Muir A, Lloyd AW, Khaw FT, et al.Investigative Ophthalmology & Visual Science', 1999
STATEMENT OF ORIGINALITY
The experiments were carried out personally. The experimental designs were conceived and designed by myself with guidance firom my supervisors.

ACK NO W LEDG EM ENTS
This thesis simply would not exist without Bruce Allan. I would like to thank Bruce for his tireless support throughout the project and also the countless hours spent correcting this thesis.
I am extremely thankful to Peng Khaw and Andrew Lloyd for their support and advice, Richard Faragher, for his help with the biocompatibility studies, and everyone from the Biomaterial Research and Wound Healing Research Groups for all their help and friendship.
Finally, I would like to express my sincere gratitude to the Department o f Trade and Industry, the Department o f Health and International Glaucoma Association for their financial support thus made all the work possible.

To my paren ts
CHAPTER ONE - Introduction
1.1 Definition of Glaucoma
The glaucomas are a group o f disorders characterised by optic nerve head damage,
visual field loss and an intraocular pressure (IGF) sufficiently raised to affect the
functioning o f the optic nerve head.
1.2 Classification
Glaucomas are most commonly classified as either open or closed angle, and may
occur in isolation (primary glaucomas) or in association with other ocular pathology
(secondary glaucomas). In open angle glaucoma, the primary cause o f raised 10? is
increased resistance to fluid drainage within the trabecular mesh work. In closed angle
glaucomas, iris occlusion o f the anterior chamber drainage angle prevents aqueous
escape.
1.3 Prevalence o f Glaucoma
Glaucoma is a leading worldwide cause o f blindness. Pooled estimates from a variety
o f population studies suggest an overall prevalence o f around 0.5% for primary open
angle glaucoma, rising with age to 2% in those aged 70-75 years (Hart 1989).
Analysis by Quigley (Quigley 1996), using population projections, suggested that
there would be around 66.7 million people with primary glaucoma worldwide in the
year 2000, with 6.7 million suffering from bilateral blindness. In England, glaucoma

10
is the second commonest cause o f severe visual impairment, accounting for
approximately 15% o f blind registrations (Grey 1989).
1.4 Disease Mechanism
Although the pathogenesis o f glaucoma is not fully understood, the disease
mechanism proposed by Maumenee (Maumenee 1983) is widely accepted. Raised
lOP leads to outward bowing o f the ocular coats at their weakest point: the lamina
cribosa. Increasing obliquity and distortion o f pores in the lamina cribosa strangles
optic nerve fibres as they exit, interrupting axoplasmic flow. Retinal ganglion cell
death follows. With progressive posterior bowing o f the lamina cribosa and nerve
fibre attrition, the optic disc becomes cupped in appearance, and visual field defects
advance. Non-IOP mediated vascular mechanisms o f glaucomatous damage may exist
(Schulzer 1990), but their identification remains incomplete. Direct evidence that an
adequate reduction in lOP will arrest disease progression is provided by studies
involving normal tension glaucoma (Collarborative NTG study group 1998; Membrey
2000). Although results from primary open angle glaucoma patients are not yet
available, they are widely expected to reaffirm this finding.
1.5 Adequate Pressure Reduction
The widely quoted figure o f 21mmHg for the upper limit o f normal lOP is derived
from population studies showing a Gaussian lOP distribution with 20.5mmHg at two
standard deviations above the mean (Schottenstein 1989). This figure has little
functional significance, since progression o f glaucomatous visual field loss can

11
certainly occur at a lower pressure level (Drance 1992). Hence studies demonstrating
continued visual field loss despite normalisation o f the lOP after filtration surgery
may simply demonstrate pressure control at a statistically normal, but functionally
inadequate level (Table 1). Currently, it is generally accepted that the greater the
existing damage to the optic nerve head, the lower the TOP needs to be to prevent
further functional damage (Grant & Burke 1982; Jay & Allan 1989). Mao et al (1991)
reviewed data from a group o f 55 glaucomatous patients with early disc damage
followed for 4-11 years. One eye was selected randomly for study in each patient.
They found no disease progression in patients with a mean lOP level <17 mmHg, and
universal progression in patients with a mean TOP level > 21 mmHg. lOP control at a
lower level (<15 mmHg) may be required where disc damage is more advanced
(Grant & Burke 1982) or in progressive normal pressure glaucoma (Hitchings 1992).
Unfortunately, no methods are available to determine, for any given optic nerve, the
pressure level required to prevent the onset or progression o f damage (Drance 1992).
Even if this guidance were available, information about lOP control gained by
snapshot readings at intermittent clinic visits is necessarily incomplete. But decisions
in medicine are rarely taken on a basis o f absolute certainty. In broad terms, it is
reasonable to conclude that simply reducing the lOP to a statistically normal level
(<21 mmHg) will often be inadequate; and that methods producing TOP control in the
low teens (<15 mmHg) are preferable to those in which TOP control in the high teens
(15-21 mmHg) is a more usual result (Table 1 ).

12
Table 1 Final intraocular pressure after glaucoma surgery and visual prognosis. Pooled analysis from various studies, (adapted from Khaw et al 1995)
Mean lO P after surgery Worse Follow-up Authors15.0 mmHg 18% 5 years Kidd, O ’Connor 198515.7 mmHg 10% 4+ years Kolker 197716.0 mmHg 35% 3.5 years Werner et al 197717.3 mmHg 35% 4 years Greve, Dake 197918.1 mmHg 29% 5 years Rollins, Drance 198119.1 mmHg 58% 5 years Roth et al 1988
1.6 The need for a new glaucoma filtration procedure
Current conventional practice is to use medical therapy, aimed at lowering lOP, as the
primary treatment modality in primary open-angle glaucoma. Argon laser
trabeculoplasty (ALT) is occasionally offered when medical therapy fails to provide
satisfactory lOP control. Glaucoma filtration surgery (GPS) is usually only offered to
patients who have failed either or both o f the other treatment modalities.
Randomised trials comparing these modalities in the initial therapy o f primary open-
angle glaucoma, show trabeculectomy to be more effective than medical treatments or
ALT (Jay & Allan 1992; Migdal 1992) in preventing progressive visual field loss.
These trials also demonstrate lOP control at a lower average level for GPS in
comparison with drug treatments (Jay 1992; Migdal 1992). In addition, prolonged use
o f topical anti-glaucoma medications as a primary treatment modality can increase the
probability o f drainage failure in subsequent GPS (Broadway et al 1994, Lavin et al
1990).
These studies pre-date newer generation topical treatments such as Brimonidine
(Melamed 2000) and Latanoprost (Nordmann 2000), and the use o f antimetabolites in

13
primary trabeculectomy for high risk patients. Whatever the true picture regarding the
relative efficacy o f newer drug treatments and GFS, there are powerful health
economic arguments for preferring a one-stop intervention to lifelong drug therapy.
Drug therapies are also impractical in the developing world. GFS would probably be
offered widely as the primary treatment in glaucoma if techniques were safer and
quicker.
Complications associated with GFS are listed in Table 2. The most important early
postoperative complications in GFS are associated with poor flow control and
resultant hypotony (I0PD5m m Hg). These include anterior chamber flattening, and
choroidal detachment, hypotony maculopathy (Costa et al 1993; Stamper et al 1992;
Cheung et al 1997)) and delayed suprachoroidal haemorrhage (Paysee 1996; Gressel
1984).
Poor initial flow control may also compromise later filtration function. The aqueous
concentration o f fibroblast stimulating cytokines (Joseph et al 1989) is increased in
conditions o f blood aqueous barrier breakdown promoted by hypotony (Addicks et al
1983), and an association between prolonged postoperative hypotony and a higher
final lOP has been observed (Migdal & Hitchings 1988; Blondeau & Phelps 1981).

14
Table 2. Complications associated with trabeculectomy with or without antimetabolites
ComplicationsChoroidal effusionHyphaemaHypotony maculopathyShallow anterior chamberIris to comeal touchSuprachoroidal haemorrhageW ound leakW ound dehiscenceBlebitis/EndophthalmitisCataractFailure
Trabeculectomy, the procedure o f choice in conventional GFS, has remained
essentially unchanged for over a quarter o f a century. Local control over wound
healing with antimetabolite agents such as 5-fluorouracil and mitomycin C has
improved the prognosis for cases with a high risk o f filtration failure (Katz 1995); but
flow control remains inexact despite the introduction o f a variety o f suture adjustment
techniques (Raina 1998, Blok 1992, Singh 1996). Early postoperative hypotony has
been observed in 25-75% o f cases either initially or after suture removal (Blok et al
1992; Fluorouracil filtering surgery study group 1989).
Trabeculectomy is also relatively slow and technically demanding, taking up to two to
three times as long as current cataract operations. A variety o f laser sclerostomy
techniques were developed in an attempt to make GFS simpler and quicker (Allan
1994, Iwach 1996, Wetzel 1994, Latina 1992). These techniques had a universally
poor safety profile, and were not widely practised. Again, the problem was poor flow
control. Attempts to regulate sclerostomy diameter and the resulting outflow

15
resistance were unsuccessful (Allan 1994), and all laser sclerostomy procedures were
effectively unguarded filtration operations, with hypotony in almost every case.
In the last few years, non-penetrating deep sclerectomy has gained popularity as a
safer alternative to trabeculectomy. The main advantage o f this procedure lie in the
fact that the globe is not penetrated during the surgery as a thin layer o f trabecular
meshwork tissue is left (Karlen 1999). This thin layer o f tissue is thought to provide
enough outflow resistance to prevent post-operative hypotony. Further more, as the
globe is not penetrated, no peripheral iridectomy is performed and this results in less
hyphaema and post-operative intraocular inflammation. However, the scope for
human error in regulating factors such as dissection depth in deep sclerectomy, is
considerable, and complication such as inadvertent perforation o f the trabecular
meshwork is common (Karlen 1999). With the limited short term follow up data
available from randomised prospective trials comparing this technique with
trabeculectomy; this new procedure has not established any clear advantage either in
complication or success rate (El Sayyad 2000, Gandolfi 2000).
A new GFS procedure is required which is both simple to perform and offers
consistent protection from over drainage. Flow control after conventional and laser
techniques remains suboptimal. Exquisite dimensional control is required to impart
consistent flow resistance in a fine bore sclerostomy channel. Even if this level o f
control were available, it is likely that dimensions o f cut tissue surfaces would quickly
be modified by biological spoliation. The logical alternative is a glaucoma drainage
device (GDD) in which key dimensions are reproduced in a controlled manufacturing
16
environment, and materials resistant to biological spoliation are used to help ensure
that flow resistance characteristics are preserved after implantation.
1.7 Glaucoma Drainage Devices
Glaucoma drainage devices (GDDs) have the potential to regulate flow consistently,
eliminating hypotony after GFS. Design, material, and manufacturing deficiencies
have left this potential unfulfilled in existing GDDs, all o f which exhibit problems
with poor flow control and suboptimal tissue compatibility. The role o f GDDs in
contemporary GFS remains poorly defined, but possibilities offered by new
biomaterials and the goal o f accurate flow control have stimulated considerable recent
interest in GDD development.
1.7.1 Early Devices
In 1906, horsehair (Rollett 1906) was placed through a comeal paracentesis in an
attempt to drain a hypopyon externally. The same technique was later used to treat
two patients with painful absolute glaucoma (Rollett 1907). Sporadic attempts using
implants to shunt aqueous to a variety o f unconventional sites, including the vortex
veins (Lee 1974), and the nasolacrimal duct (Mascati 1967) have since been reported.
Results were generally unfavourable or too poorly documented to evaluate, and
attention has focused on devices shunting aqueous fluid to the subconjunctival space
as with conventional GFS.

17
The first transi imbal GDD, reported by Zorab in 1912, was silk thread used as a seton
to aid drainage o f anterior chamber fluid to the subconjunctival space. This was
followed by similar use o f gold (Stefansson 1925), tantalum (Bick 1949) and platinum
thread/wire (Muldoon 1951). Results were universally poor however. These and other
early translimbal setons (Table 3) did not address lack o f flow control and hypotony
associated with full thickness (unguarded) GFS, and added a foreign body chronic
inflammatory stimulus. Simple translimbal tube devices (La Rocca 1958, Ellis 1960)
were similarly unsuccessful, with high rates o f early filtration failure.
Translimbal drainage implants, or anterior GDDs, were implanted with the intention
o f preventing filtration failure by maintaining patency o f a drainage fistula or
sclerostomy. Anterior GDDs failed to improve filtration failure rates in comparison
with conventional GFS, but it took almost half a century for investigators to begin to
rationalise this lack o f success.

Table 3. Developments o f glaucoma drainage devices.
18
Year Investigator Type M aterial M ethod Flow Control D rainage Site
1907 Rollet seton Horse hair Paracentesis None External cornea
1912 Zorab seton Silk thread Translimbal None Anteriorsubconjunctival
1925 Stefansson seton/tube Gold Translimbal None Anteriorsubconjunctival
1934 Row seton Platinum Cyclodialysis None Suprachoroidal
1940 Troncoso seton Magnesium Cyclodialysis None Suprachoroidal
1942 Gibson tube Lacrimal canaliculus Transcleral None Anteriorsubconjunctival
1949 Bick seton/tube Tantalum Cyclodialysis None Suprachoroidal
1951 Muldoon seton Platinum Translimbal None Anteriorsubconjunctival
1952 Losche tube Supramid Cyclodialysis None Suprachoroidal
1955 Bietti tube Polyethylene Cyclodialysis None Suprachoroidal
1958 La Rocca tube Polyvinyl Translimbal None Anteriorsubconjunctival
1960 Ellis tube Silicone Translimbal None Anteriorsubconjunctival
1967 Mascati tube Plastic Translimbal None Lacrimal sac
1969 Molteno tube & plate Acrylic Translimbal None Anteriorsubconjunctival
1974 Lee & Wong tube Collagen Translimbal None Vortex vein
1976 Krupin tube Silicone & Supramid Translimbal Slit valve Anteriorsubconjunctival
1979 Honrubia tube Silicone Translimbal None Anteriorsubconjunctival
1982 Schocket tube & band Silicone Translimbal None Posteriorsubconjunctival
1985 White tube & plate Silicone Silicone Valve & pump Posteriorsubconjunctival
1986 Joseph tube & band Silicone Translimbal Slit valve Posteriorsubconjunctival
1990 Krupin tube & plate Silicone Translimbal Slit valve Posteriorsubconjunctival
1990 Baerveldt1991)
tube & plate Silicone Translimbal None Posteriorsubconjunctival
1993 Ahmed1995)
tube & plate Silicone & Polypropylene Translimbal Venturi valve Posteriorsubconjunctival
1995 OptiMed1996)
tube & plate Silicone & PMMA Translimbal Microtubules Posteriorsubconjunctival
1995 Smith seton Hydrogel Translimbal None Intrascleral
1996 Pandya tube & plate Silicone & Hydroxylapatite
Translimbal None Posteriorsubconjunctival
1997 Glovinsky & Belkin
tube Stainless steel Translimbal None Anteriorsubconjunctival
1997 Helies artificialmeshwork
PTFE Transcleral None Anteriorsubconjunctival

19
In 1969, Molteno (Molteno 1969) hypothesised that filtration failure was primarily
attributable to subconjunctival fibrosis, with fistula closure occurring as a secondary
event. This was later confirmed in histological studies o f animal models o f GFS
(Miller et al 1989 and Jampel et al 1990). Realising that simple anterior GDDs would
have little impact on this process, Molteno launched the concept o f tube and plate
GDDs, in which aqueous fluid is shunted to a plate device designed to maintain
patency o f a subconjunctival filtration reservoir in the face o f continuing
subconjunctival fibrosis. Although confined to use in complex cases by the advent o f
trabeculectomy and relatively successful conventional guarded GFS, these were the
first GDDs to gain widespread acceptance and the Molteno tube remains the
benchmark against which other tube devices are compared.
1.7.2 Contemporary Devices
Tube and plate devices dominate the contemporary GDD market. Prominent
examples, in chronological order, are the Molteno, Krupin, Baerveldt, Ahmed, and
OptiMed GDDs (Figures 1-5). Molteno (1976) moved the plate element o f his early
devices posteriorly away from the limbus to avoid problems with dellen formation
and poor filtration associated with pre-existing anterior conjunctival scarring.
Posterior placement beneath Tenon's capsule was also thought to improve protection
from extrusion (Molteno 1976, Melamed 1990). Subsequent tube and plate GDDs
share the essential design concept o f posterior filtration via a tube in the anterior
chamber to a plate element secured beneath Tenon's capsule, but differ in plate design

20
and their provision for a flow control mechanism to protect from early postoperative
hypotony (Table 4).
Table 4. Contemporary Glaucoma Drainage Devices.
G DDs Year o f Introduction
T ube D iam eter/ M aterial
Plate Size/ M aterial
ResistanceM echanism
Molteno 1979 0.63mm OD 0.30mm ID Silicone
135mm^Polypropylene
None
Baerveldt 1990 0.63mm OD 0.30mm ID Silicone
200,250,350.425,500mm"Silicone
None
Krupin with Disk 1990 0.58mm OD 0.38mm ID Silicone
180mm"Silicone
Slit Valve
Ahmed 1993 0.63mm OD 0.30mm ID Silicone
185mm"Polypropylene with Silicone valve
Venturi Valve
OptiMed Model- 1014
1995 0.56mm OD 0.30mm ID Silicone
140 mm"Silicone with PMMA matrix
Microtubules
OD = outside diameter ID = inside diameter

21
Figure la . Single plate M olteno implant. (Scale: bar = 1 cm)
Figure lb. Dual chamber double plate Molteno implant. (Scale: bar = 1 cm)
Figure le. A schematic drawing of the resistance mechanism of a dual chamber double-plate Molteno implant. The thin V-shaped ridge (see Figure lb) has the same height as the circumferential rim of the polypropylene plate. The top surface of the plate is divided into one smaller and one larger chamber by the apposition of the overlying conjunctival and Tenon’s layers (dashed line). Aqueous flows (black arrow) into the smaller proximal chamber until sufficient pressure is achieved within the chamber to lift (white arrow) the overlying conjunctival layer to allow free drainage.
Sclera
22
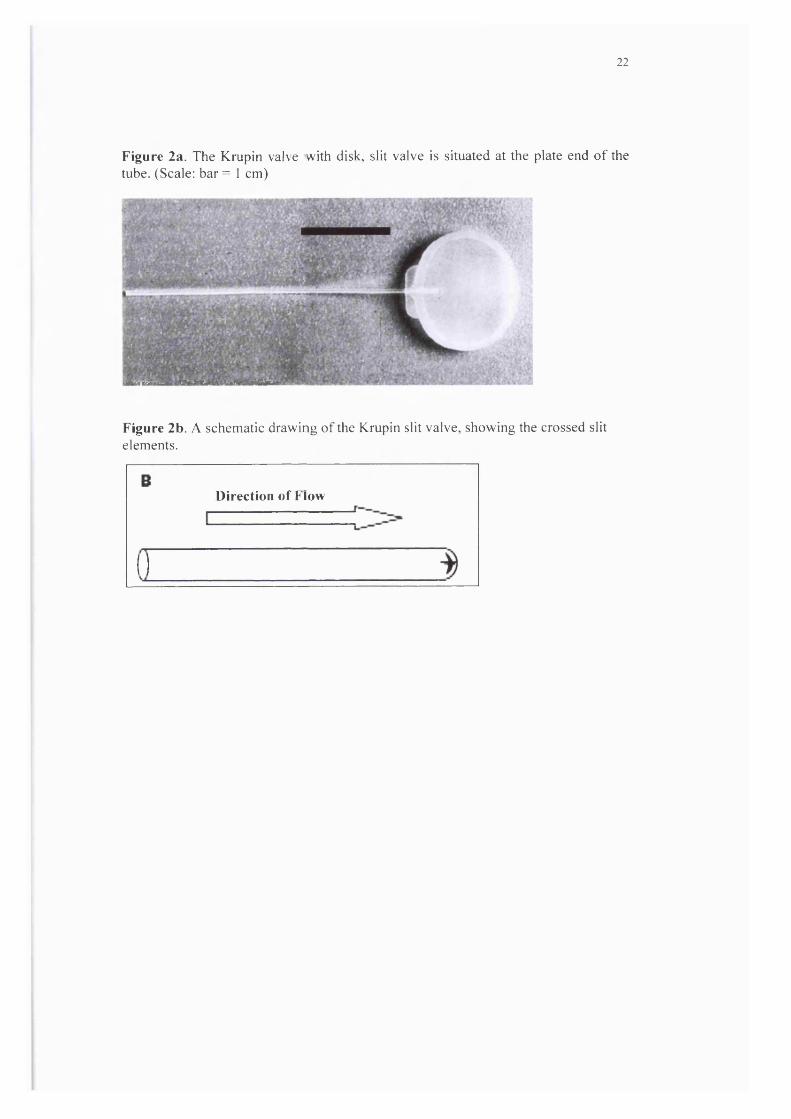
Figure 2a. The Krupin valve with disk, slit valve is situated at the plate end of the tube. (Scale: bar = 1 cm)
Figure 2b. A schematic drawing of the Krupin slit valve, showing the crossed slit elements.
Direction of Flow

Figure 3a. The Baerveldt implant. (Scale: bar = 1 cm)
23
(■■Ms.
I '
-#:T
Figure 3b. A schematic drawing of the appositional resistance mechanism included in some embodiments of the Baerveldt GDD. An annular ridge projecting from the underside of the plate element provides a temporary seal against the sclera. Absorbable sutures are used to hold the plate in apposition. As the sutures degrade, the plate element lifts clear, allowing free aqueous drainage.
i l l ' V i . '

24
Figure 4a. The Ahm ed glaucoma valve implant. (Scale: bar = 1 cm)
Figure 4b. A schematic drawing of the resistance mechanism of the Ahmed valve. Aqueous flows (black arrow) through the tube into a chamber within the plate element. A folded over silicone membrane (black line) forms this chamber with its free edges forming a one-way valve. The manufacturers claim that the two halves of the polypropylene body of the plate element pre-tension the valve to open at a specific level of lOP. They also claim that the venturi effect produced by the tapering trapezoidal shape of the space enclosed by the folded silicone membrane acts to improve flow regulation (increasing fluid velocity as the chamber tapers acts to reduce internal pressure proximal to the slit opening in accordance with the inverse relationship between fluid velocity and pressure expressed in the Bernoulli’s theorem). Neither of these claims is supported by published experimental evidence.
B

25
Figure 5a. The OptiMed implant is made up of a silicone tube with a PMMA plate. The “flow-restricting” element of this device is housed within the rectangular box situated at the end of the tube within the plate. (Scale: bar = 1 cm)
Figure 5b. A schematic drawing of the OptiMed implant’s “flow-restricting” unit, which is made up of multiple microtubules providing a pressure gradient, governed by Poiseuille’s formula (Appendix 1).
B
Direction of flow

26
1.8 Evaluation of Results
Most GDDs have been developed with little available data to substantiate
manufacturers’ claims for flow performance (Prata et al 1995) or biocompatibility.
Clinical data is largely restricted to uncontrolled retrospective case series (Krawczyk
1995) with variable follow-up and differing definitions o f surgical success. Evaluation
is further complicated by the heterogeneity o f inclusion criteria. Series include a
variable proportion o f complex cases, neovascular glaucoma in particular, with a
predetermined high risk o f filtration failure.
Existing results are summarised in table 3. Overall success rates, in terms o f IGF
control, appear similar between devices (Table 5), with a reasonably high proportion
o f cases achieving a final 10? in the target range at one year after surgery. H alf to two
thirds o f these cases still require glaucoma medications however; and, as already
argued, target lOPs in the low teens (<16mmHg) may be more realistic in terms o f
preventing disease progression than commonly adopted target levels (<21 or
22mmHg).
Another important caveat concerns attrition rates, or continued increments in the
proportion o f filtration failures with lengthening postoperative follow-up. Again,
evaluation is difficult, with few series including either long-term data or survival
analysis. Mills (1996) (Table 5) reported a 10% failure rate per post-operative year in
a series including longer term follow-up for single and double plate Molteno tubes.
Extrapolating from this, it would appear that most GDDs have a functional lifespan o f
less than five years before failure though fibrous encapsulation.

27
Table 5. Success Rates o f current Glaucoma drainage devices.
Type Investigator Year Diagnosis No.ofEyes
Follow-Up (Months) Mean ± SD
Definition of Success*
Success RatewithoutMedication
Success Rate with Medications
M olteno SP & D P M ills 1997 Mixed (25%
Neovascular)77 44/+ lO P < 22 m m H g 23% 3 4 %
SP M erm oud 1993 Neovascular 60 24 .7± 13 .4 I 0 P < 2 1 17% 20%SP
DP
H euer 1992 Mixed (No Neovascular)
50
52
14.9±8.9
16.4 ± 6 .8
5 < I 0 P < 2 1 10%
12%
40%
63%
SP M inckler 1988 Mixed (50% Neovascular)
90 17.6 I 0 P < 2 1 7% 40%
Ahmed C olem an 1995 Mixed 60 9.3++ lO P < 22+ NA NA(78%)^
C olem an 1997 PenetratingKeratoplasty**
31 16++ I0 P < 2 2 + " 26% 39%
C olem an 1997 Paediatric-Mixed
24 16.3±11.2 lO P < 22+ 33% 38%
KrupinDisk
K rupin S tudy G roup
1994 Mixed 50 25 .4± 2 .4 IO P < 19 33% 47%
Fellenbaum 1994 Mixed 25 13.2 6 < 1 0 P < 2 1 28% 36%Baerveldt200 ,250 ,350,500m m "
Siegner 1995 Mixed 103 13.6±0.9 5 < IO P < 2 2 27% 45%
200,350 ,500mm"
Sidoti 1995 Neovascular 36 15.7±7.2 6 < I O P < 2 1 17% 33%
350 mm" Lloyd 1994 Mixed 37 15.5±4.8 6 < 1 0 P < 2 1 14% 70%
500 mm" 36 14.1±5.4 36% 47%
* With no further glaucoma surgery or devastating complication** Without graft failure § Total success rate only §§ Concurrent or Prior+ Or reduction o f >20% if pre-operative IOP>22 mmHg. Data from same patients may appear in more than one o f these three series.++ Median follow-ups in months. Mean values not available in these reports, making direct comparison difficult Molteno SP = Molteno single plate Molteno DP = Molteno double plates

28
1.9 Complication Mechanisms
Clinical series reporting ODD procedures are characterised by frequent problems in
addition to filtration failure (Table 6), with overall complication rates typically
around 60 - 70% (Siegner 1995, Heuer 1992). W hilst partly attributable to the
complex nature o f cases most usually selected for implantation, the range o f
complications observed also reflects design and material inadequacies inherent in
contemporary GDDs.
The origin o f most complications can be traced to just two fundamental mechanisms:
poor flow control and suboptimal material biocompatibility.

Table 6. Cumulative complication rates in the currently used GDDs.
29
Com plications Ahmed Valve Krupin Valve with Disk
BaerveldtIm plant
M oltenoIm plant
(n=115)C olem an 1995 C olem an 1997 C olem an 1997
(n=75)K rupin S tudy G roup 1994Fellenbaum 1994
(n=249)L loyd 1994 S idoti 1995 Sm ith 1993 S iegner 1995
(n=395)M ills 1996 M inck ler 1988 L loyd 1992 H euer 1992
H ypo tony /F la t an te rio r C ham ber
3.5% 27% 16.5% 5%
C horoidalE ffusion /H aem orrhage
14% 33% 23% 7%
Suprachoro idalH aem orrhage
3.5% 1.3% 0.8% 0.5%
H yphaem a 0 1.3% 11% 4%V itreous H aem orrhage 3.5% 1.3% 7% 2%U veitis 1.7% 9.3% 3.6% 0 .5%M alignan t G laucom a 0.9% 2.7% 2% 0.5%M otility Problem 3.5% 4% 21% 0.3%C ataract N /A N /A 9.9% § 12%*T ube B locked 7.8% 11% 10 6%T ube R etraction 5.2% 2.7% 2.4% 0 .8%T ube/P la te E xtrusion 4.3% N /A 1.2 0 .5%T ube/P la te Erosion 0 2.7% 2 3%C orneal Touch 2.6% N /A 4% 3%C orneal D ecom pensation 3.5% 5.3% 11.6% 14%R etinal D etachm ent 0 0 5% 3.5%E ncapsu la ted B leb 3.5% 1.3% 1.6% N /APhthisis 0 1.3% 2.4% 4%O thers 1.7% Wound Leak 1.3% Wound Leak
1.3% Endophthalmitis 1.3% Decompression Retinopathy
1.6% Wound Leak 0.4%Endophthalmitis
0.3% Epiretinal Membrane 0.3% Perforation
* cataract developed in 11 out o f 91 phakic patients. Mean follow-up more than 40 months.§ cataract developed in 7 out o f 69 phakic patients. Mean follow-up 14.4 months.
30
1.9.1 Poor Flow Control
Modifications to GDDs and implantation techniques since Molteno's original device
have largely been driven by attempts to minimise rates o f early postoperative
hypotony. Hypotony is associated with a catalogue o f early and late complications in
GFS, including anterior chamber shallowing, maculopathy, delayed suprachoroidal
haemorrhage and late filtration failure (see 1.6 above). Anterior chamber flattening is
especially hazardous in the context o f GDD implantation in which contact with the
tube element can cause significant comeal endothelial and lens epithelial damage.
GDDs can be categorised into those with no internal resistance mechanism, no set
internal resistance, and those aiming to provide set internal flow resistance.
1.9.1.1 Devices with No Resistance Mechanism
Early Molteno and Baerveldt implants were simple tube and plate devices with no
internal resistance mechanism.
After GFS, resistance to flow distal to the sclerostomy or GDD generally remains low
until limited subconjunctival wound healing has occurred and the initially diffuse
aqueous escape becomes confined within a maturing filtration bleb. Having observed
frequent problems with hypotony in early single stage implantation (Molteno 1977),
Molteno recognised that some allowance for this early period o f minimal distal flow
resistance would be required. A two-stage procedure was initially explored (Molteno

31
1983), in which the device was implanted and allowed to encapsulate prior to
insertion o f the tube element into the anterior chamber at a second operation after 2-6
weeks. In addition to a second operation, a separate provision for initial lOP control in
the intervening period was required, and while the two stage approach was successful
in reducing problems with hypotony, variations o f a modified single stage procedure
are now widely preferred for GDDs with no internal resistance mechanism. These
include ligation with an absorbable suture (Molteno 1986), laser suture-lysis (Price
1989), and occlusion with a supramid stent which is later removed through a small
conjunctival incision (Egbert 1983). Single stage methods seek to occlude the lumen
o f the tube element temporarily to allow partial encapsulation o f the plate. They rely
on external leakage with or without a slit incision through the subconjunctival portion
o f the tube proximal to the occlusion to provide initial outflow. Neither o f these initial
flow mechanisms is well controlled, and problems with either too much or too little
initial aqueous escape remain frequent.
1.9.1.2 Devices with No Set Resistance
Later incarnations o f the Molteno and Baerveldt GDD incorporate resistance
mechanisms, which depend on tissue apposition to limit flow.
The Molteno dual ridge device seeks to limit the initial drainage area by dividing the
top part o f the plate into two separate spaces (Figure lb & 1C). Aqueous escapes
directly into the channel between two concentric ridges on the plate element, but must
overcome resistance associated with conjunctival tissue apposition to flow further.
With later partial encapsulation o f the plate element, the overlying tissues balloon

32
clear o f the inner pressure ridge, and aqueous flow into the space overlying the plate
is unrestricted (Freeman et al 1992).
Apposition o f the "Bioseal" element o f the modified Baerveldt implant to the sclera
with absorbable sutures (Figure 3b) also aims to provide early flow resistance,
limiting initial aqueous escape from beneath the device (Baerveldt 1997).
The essential problem with both approaches is that, as with trabeculectomy, the force
o f tissue apposition is poorly controlled. Early flow resistance varies and initial lOP
levels remain unpredictable.
1.9.1.3 Devices with Set Resistance
Devices which aim to set the initial lOP level by incorporating a non-adjustable
resistance mechanism include the Krupin (Figure 2b), Ahmed (Figure 4b), and
OpitMed (Appendix 1) (Figure 5b) GDDs.
Early independent examination o f the flow characteristics for each o f these deviees
suggests a wide divergence between observed function and manufacturers claims for
flow resistance (Prata et al 1995). Valved devices (Ahmed and Krupin) appear not to
close after initial opening in perfusion tests at physiological flow rates. Resistance
values also vary considerably between devices from the same manufaeturer,
indicating deficiencies in quality control (Porter et al 1997). Although subsequent
flow examinations (Eisenberg 1999, Francis 1998) showed that Ahmed valve might
indeed have a higher opening pressure, clinically, hypotony were still reported in 5-20
33
% of cases after Ahmed GDD implantation (Coleman AJO 97; Coleman Arch Oph
97).
All the commonly used devices feature a round silicone anterior chamber tube with a
diameter o f between 0.56 mm and 0.63 mm (Table 4). The recommended technique
for insertion is through a paracentesis track created by either a 22 gauge or 23 gauge
(0.65 mm) hypodermic needle. Debate over the optimum needle gauge continues
(Coleman 1995), but insertion often requires considerable manipulation. The resulting
tube to paracentesis fit is often poor and uncontrolled leakage external to the tube
remains common.
Whether due primarily to lack o f internal flow regulation or uncontrolled extrinsic
leakage, problems associated with excessive early aqueous outflow and hypotony
have not been adequately addressed by current GDD designs and implantation
techniques.
1.9.2 Poor Tissue Compatibility
Biocompatibility refers to the ability o f a synthetic material to interface with living
tissues without provoking a detrimental reaction. W ithin the context o f GDD
implantation, suboptimal biocompatibility is manifest in an array o f complications
including early fibrinous occlusion, comeal endothelial failure, tube migration,
extrusion, and fibrous encapsulation leading to filtration failure. Key elements in the
mechanism o f these complications are protein adhesion and micromotion.

34
Elastomeric silicone (polydimethylsiloxane) remains the most commonly used
material in current GDDs. Silicone, PMMA, and other hydrophobic polymers used in
GDDs have a relatively high binding affinity for plasma and interstitial fluid proteins
including albumin, IgG and fibrinogen. These proteins are adsorbed within hours o f
implantation (Pitt et al 1988). Cellular adhesion, cytokine release and chronic
inflammation are thought to be mediated via elements o f this protein film (Tang &
Eaton 1995).
Micromotion, or microscopic shearing o f the implant relative to the surrounding
tissues exacerbates continuing low-grade inflammation. Plate elements o f
contemporary GDDs often impinge on the extraocular muscles, either directly or
through adhesions with septal elements o f the orbital tissues. Even where this does not
produce a frank motility disturbance (Table 6), it is likely that shear forces
transmitted through the relatively rigid materials used in GDD construction produce
significant micromotion. Rabbit experiments in which the Baerveldt GDD was
fenestrated to improve fibrous tissue anchoring, reducing micromotion, demonstrated
a significant reduction in fibrous encapsulation thickness compared with
unfenestrated controls at explantation six months postoperatively (Jacob-Labarre et al
1996). In addition to helping drive subconjunctival fibrosis after GDD implantation,
micromotion transmitted via the tube element o f contemporary GDDs to the anterior
chamber may lead to continuing comeal endothelial cell loss. Superimposed on
perioperative endothelial damage, this is the likely mechanism o f comeal endothelial
failure in association with GDDs.

35
Progressive fibrous encapsulation limits the filtration life o f all contemporary GDDs.
As with poor flow control, suboptimal biocompatibility and the resultant continuing
low grade inflammatory drive to progressive subconjunctival fibrosis have not yet
been adequately addressed.
1.10 Strategies to Improve Success Rates
1.10.1 Plate Surface Area
One strategy for delaying filtration failure has been to increase plate size. In 1981,
Molteno published a series (Molteno 1981) o f 20 patients who received one plate (135
mm^), two plate (270 mm^) or four plate (540 mm^) Molteno implants. Mean post
operative 1 0 ? ’s were significantly lower for two and four plates compared with single
plate implantation, but did not differ significantly between two and four plates. A
subsequent randomised controlled trial involving 132 patients (Heuer 1992) showed a
higher success rate in the double-plate (270 mm^) Molteno group compared with the
single-plate (135 mm^) Molteno group. A similar trial (Lloyd et al 1994, Britt et al
1999) comparing Baerveldt implants with two different plate areas (350 & 500 mm^)
was less clear cut. Although fewer medications were required for the patients with
500mm^ implants to achieve the target 10? for success (<21 mmHg), some
complications were more frequent with this larger plate size. Overall, a larger
filtration area would appear to improve filtration function (Minckler 1987) at least in
the medium term, but eventual subconjunctival fibrosis over a wider area may
adversely influence the prognosis for repeat GFS.

36
1.10.2 Antimetabolites
In addition to pioneering departures in GDD design, Molteno was amongst the first to
attempt to control subconjunctival wound healing after GFS pharmacologically. He
used steroids, fluphenamic acid and colchicine systemically (Molteno 1983).
Although filtration function appeared to improve, systemic complications and
uncertain benefits lead to the abandonment o f this regime (Minckler 1988).
Successful modulation o f fibroblast function with locally applied antimetabolite drugs
followed however (Skuta 1992; 5-FU Filtering Surgery Study Group 1989), and the
use o f 5-fluorouracil (5-FU Study Group 1989) and M itomycin-C (MMC) (Katz
1995) in conventional GFS has become widespread over the last decade.
In a rabbit study using Baerveldt implants with and without MMC, Prata et al (1995)
were able to show a consistently lower 10? in the MMC treated eyes. The difference
remained statistically significant for up to ten weeks post-operatively. Early clinical
data has been less easy to interpret. A series o f 21 patients who underwent double
plate Molteno tube implantation with adjunctive intraoperative MMC had a higher
success rate (10P<21mmHg) at 12 months than 18 historic controls (68% v 17%)
(Perkins 1995); but the success rate o f only 17% in the control group was unusually
low (Table 3). In another series o f 21 patients (no controls) using intraoperative MMC
and a modified Molteno implant, the success rate (10P<21mmHg) was 76.2% after a
mean follow-up o f 9.4 ± 6.4 months (Susanna 1994).
More recently, a series o f 49 patients with Molteno tube and intraoperative MMC
achieved a one-year success rate o f 76.1% compared with a historical control o f

37
78.7% in 51 patients (Lee 1997). This finding appeared to be confirmed by a
randomised trial, which showed similar lOP, visual acuity and complication rate at 12
months after surgery using pressure-ridged Molteno implants (Cantor 1998).
However, the small sample group in this study (12 MMC and 13 controlled) make it
difficult to draw any definitive conclusion regarding the effect o f MMC on the
success and complications o f GDD implantation.
1.11 Current Indications
High complication rates and the likelihood o f filtration failure within five years have
confined GDD surgery to situations in which trabeculectomy is unlikely to succeed
(Melamed 1990). Improved filtration performance in trabeculectomy with adjunctive
antimetabolite treatment for cases at a high risk o f failure has relegated GDD surgery
still further, and the position relative to other treatment modalities,
(trabeculectomy/MMC or contemporary cycloablation techniques) has not been
clearly defined by clinical trials.
1.12 New Design Concepts
W hilst the post-antimetabolite era o f GFS may have presaged a downturn in the use o f
contemporary GDDs, it also heralds an opportunity to deconstruct some dated design
concepts and move forward.

38
1.12.1 Tube without Plate
The rational basis for using a plate element to physically maintain a drainage reservoir
might be questioned if subconjunctival fibrosis could be controlled pharmacologically
(Kee & Youn 1995). A large surface area o f relatively rigid foreign material may
simply exacerbate the inflammatory stimulus to progressive fibrosis. Realising this, a
number o f investigators are currently re-exploring anterior GDDs (transcleral
implants with no plate element) (Helies 1997; Glovinsky 1997) Clinical results are not
available yet, but success will depend on a marriage o f design and biomaterials
improvements with well controlled pharmacological modulation o f wound healing.
1.12.2 New Biomaterials
Relatively recent advances in biomaterials technology (Ikada 1994; Hall 1989) offer
the prospect o f implanting biologically inert GDDs with rigidity and biointegration
characteristics designed to eliminate micromotion. These new biomaterials should
enhance filtration longevity and prevent modification o f flow resistance by the
accumulation o f biological debris. If these bioinert materials can be incorporated
alongside good dimensional control in manufacture and design departures to prevent
extrinsic leakage, there is no reason in principle why GDDs might not be used in
routine GFS.

39
1.13 Conclusion
The current standing o f GDDs is in some ways analogous to that o f intraocular lenses
in the early seventies, with frequent complications attributable to design and material
inadequacies. Just as improved intraocular lenses have revolutionised cataract surgery
in the recent past, new materials and design departures may transform filtration
surgery with GDDs in the near future.
With the fundamental aim o f developing a new generation o f GDDs suitable for use
as an efficient one-stop intervention in the primary treatment o f glaucoma, the
premises explored in this thesis are: first, that reproducible control over internal flow
resistance and external leakage are possible in a GDD; and second, that new bioinert
materials have the potential to enhance device performance significantly.

40
CHAPTER TWO - Design Changes to Control Flow
Abstract
AIMS.
Firstly, to examine whether small holes produced by 248 nm excimer laser ablation in
a polymer substrate could consistently produce a pressure drop in the desired target
range (5-15 mmHg) at physiological aqueous flow rates for use as a flow restrictor in
a GDD. Secondly, to investigate whether redesigning the GDD exterior to facilitate
introduction and bear evenly on a standard sized slit incision in the eye wall would
reduce external leakage compared to conventional insertion techniques for existing
devices.
M ETHODS.
Single holes with target diameters o f 10pm, 15pm, 20pm and 25pm were drilled
using a 248 nm excimer laser in sample discs (n=6 at each diameter) punched from
75pm thick polyimide sheet. Sample discs were tested in a flow rig designed to
measure the pressure drop across the discs. Using filtered and degassed water at a
flow rate o f 1.4 pl/min. Repeated flow measurements were taken (n=6) for each disc.
After flow testing, all discs were imaged using a scanning electron microscope and
the dimensions o f each hole were derived using image analysis software. In the
external leakage study, corneoscleral buttons (n=13) were prepared from cadaver pig
eyes and mounted on an artificial anterior chamber infused with Tyrode solution.
After the pressure had stabilised, standard occluded silicone tube implants were
inserted through 23G needle stab incisions at the limbus, these were compared against
prototype PM MA implants with a novel shape profile inserted through 1.15 mm width

41
MVR stab incisions at the limbus. The infusion rate was maintained and a second
pressure measurement was taken when the pressure had stabilised. The difference
between the first and second pressure measurement was then compared, as an index o f
external leakage.
RESULTS
Ablated tubes were found to have a near perfect circular outline on both the entry and
exit side. The observed pressure drops across the ablated sample discs at each target
diameter were as follows: 10pm - 25.66±4.9 (mmHg; mean±SD); 15pm - 6.76±1.15;
20 pm - 1.66+1.07; and 25 pm - <0.1 mmHg. The correlation coefficient between
observed pressure drops and those predicted by Poiseuille’s formula was 0.996.
Target ablations o f 15 pm diameter produced tubes that consistently achieved a
pressure drop within the desired range (5-15mmHg). In the external leakage study,
pre-insertion pressures (mmHg; mean ± SD) were 19.00+4.3 (conventional method)
and 20.00+3.9 (new technique with PMMA prototypes). Post-insertion pressures were
significantly reduced (10.40+7.7; p<0.01) for the conventional technique and were
essentially unchanged for the new techniques (18.80+4.9; p>0.1).
CONCLUSIONS
These studies have shown that it is possible in principle to control the dimensions o f a
manufactured tubular lumen in a GDD accurately enough to provide consistent
protection from hypotony in the early period after glaucoma filtration surgery. By
redesigning the external profile o f the device and the incision technique, we have also
shown that it is possible to eliminate uncontrolled external leakage.

42
2.1 Introduction
This chapter will describe a series o f flow experiments to look at ways to improve
flow control in a new generation o f GDDs.
Glaucoma filtration surgery (GFS) involves the creation o f a channel, or fistula,
between the anterior chamber and the subconjunctival space, bypassing the
compromised physiological aqueous drainage pathway through the trabecular
mesh work. Many o f the early postoperative complications o f GFS relate to poor
initial control over aqueous outflow, and safety could be considerably enhanced if
resistance to flow through the drainage fistula (fistular resistanee) were regulated
more effectively.
Early postoperative hypotony (I0P<5mmFIg) is a consistent feature o f unguarded
filtration procedures including laser sclerostomy, and remains eommon after
trabeculectomy both in the immediate postoperative period and after suture release
(Block 1992; 5-FU Filtering Surgery Study Group 1989). Consistent control over
fistular resistance in eonventional GFS is difficult to achieve. The scope for human
error in regulating faetors such as suture tension and flap dimensions in
trabeculectomy, or dissection depth in deep sclerectomy, is considerable. Here we
explore the possibility that a GDD might be used to impart reproducible flow
resistanee in routine GFS.
Existing valved GDDs have been unsuceessful in preventing hypotony in a significant
proportion o f cases (Krupin Eye Valve Study Group 1994; Coleman 1995). Recently
43
examined pressure/flow relationships in leading eurrent devices found that valved
devices tended not to close after initial perfusion (Prata 1995). Simple non-valved
flow resistors (single or multiple small diameter tubes) may therefore be preferable.
Flow resistance in a tubular channel varies with the fourth power o f tube diameter in
accordance with Poiseuille's formula (McEwen 1958). To impart a consistent level o f
flow resistance, tube dimensions (the diameter in particular) must be controlled very
accurately. The required level o f control has never been approached by current laser
sclerostomy techniques (Allan 1993). Far greater accuracy should be possible for laser
ablation o f a homogeneous synthetic polymer substrate in controlled conditions. We
set out to examine whether small tubular holes produced by 248 nm excimer laser
ablation in a polymer substrate could consistently impart a flow resistance in the
desired target range: producing a pressure drop across specimen tubes mounted in an
experimental flow rig o f 5-15 mmHg at physiological flow rates.
Insertion o f conventional GDDs into the paracentesis track produced by a standard
hypodermic needle often requires considerable manipulation. Debate over the
optimum needle gauge (G) continues (Coleman 1995), and hypotony due to external
leakage remains a significant clinical problem. Redesigning the exterior o f the device
to facilitate introduction and improve fit should help prevent external leakage. In a
further series o f flow experiments, external leakage for the tube element common to
existing devices (Table 4; Chapter 1: Page 20) introduced conventionally was
compared with a redesigned GDD and insertion technique.

44
2.2 Fluid Mechanics
If small cylindrical tubes are to be used as the flow resistanee element for a GDD, the
internal dimensions required to provide a given pressure gradient can be calculated
using Poiseuille’s equation if the rate o f production o f human aqueous is known, and
flow through the tube is laminar.
Aqueous flow in normal subjeets during waking hours is thought to be 2.75 ± 0.63
pl/min (Brubaker 1991), but ean be as low as 1.4 ± 0.19 pl/m in (2.3x10’" m^sec'*)
during sleep (Reiss 1984). Sinee the main aim in device design was to provide
eonsistent proteetion from hypotony, the rate o f aqueous flow used in this experiment
was set at 1.4 pl/min, the lowest likely physiological level. The viscosity o f human
aqueous is only slightly greater than water (1.029 compared to 1.000 for water)
(Cavazzani 1909) and for these ealculations, the value o f water was used.
Turbulent flow oeeurs in tubes when the Reynolds number reaches a certain level. At
this point, the pressure gradient aeross the tube will increase markedly as more
mechanical energy is lost. It was therefore essential in GDD design to ensure that
flow remains laminar. It is generally agreed that the lower critical Reynolds number is
2000 above whieh the transition from laminar to turbulent flow oeeurs. Reynolds
numbers can be calculated by using the following formula (Batchelor 2000):
Re = pdu/p

45
WhereRe= Reynolds numberp= density o f aqueous = 1000 kg m'^d ^ tube diameter in metre (10-30 pm)u= average flo w velocity = rate/area = msec^p= viscosity o f the fluid=0.001 Nsecm'^therefore,
Re = kgNsec'^m’’
In Figure 6, Reynolds numbers are plotted against a range o f possible diameters for
short cylinders designed to provide TOP control in the desired range (5-15mmHg) at
physiological flow rates. It is clear that the Reynolds numbers for all the tube sizes
used are well below 2000. Flow in these systems should be laminar (Batchelor 2000).
Figure 6. The relationship between Reynolds number and tube diameter at physiological aqueous flow rate.
0.35
^ 0.25 -
3 0.20
0.10
100 120
Tube Diameter in ^m

46
The application o f Poiseuille’s formula in this context is based on the assumption that
tube length is considerably greater than the diameter. For shorter cylindrical tubes, the
distance required to establish a laminar flow pattern (the entry length) can be
calculated by the following formula:
Entry length = 0.057 x Reynolds Number x hole diameter
Using this formula it can be seen that a laminar flow pattern develops within a short
distance o f entry for all likely flow systems in GDDs. For example, with a 10 pm
diameter hole, the entry length is only 1.6 pm.
Other factors such as abrupt contraction or enlargement o f the tube, and diffuser
effects associated with the entry edges are not significant because o f the low
Reynolds’ number produced by flow systems at physiological aqueous production
rates (Batchelor 2000).
Finally, an estimate o f the diameter required for an ideal tube can be obtained from a
simplified Poiseuille’s formula, as applied by M cEwen (1958) for aqueous outflow.
The pressure drop across the tube is given by:
4Pressure drop = 128. p.I.Q /1 3 6 . Ti.d
Where
ju = aqueous viscosity = 0.001 Nsec/m2 (Cavazzani 1909)/ = length (thickness o f polymer disc used in this study) = 0.075 mm Q = aqueous flo w rate = 1.4 pl/min d = diameter in metre

47
Figure 7a. The pressure drop across a tube versus tube diameter from Poiseuille's formula at a flow rate o f 0.7pl/m in (plain line), 1.4pl/min (dotted line) and 2.8pl/min (dashed line):
Pressure drop = 128//1Q / 1367id^
Where
JU = aqueous viscosity = 0.001 Nsec/m2 I = length = 0.075 mm in this study Q = aqueous flo w rate d = diameter in metres
XBSa.2021
1800 n
1600
1400
1200 -
1000
800 -
600
400
200 -
10 20 30
Tube Diameter (pm)
40 50
48
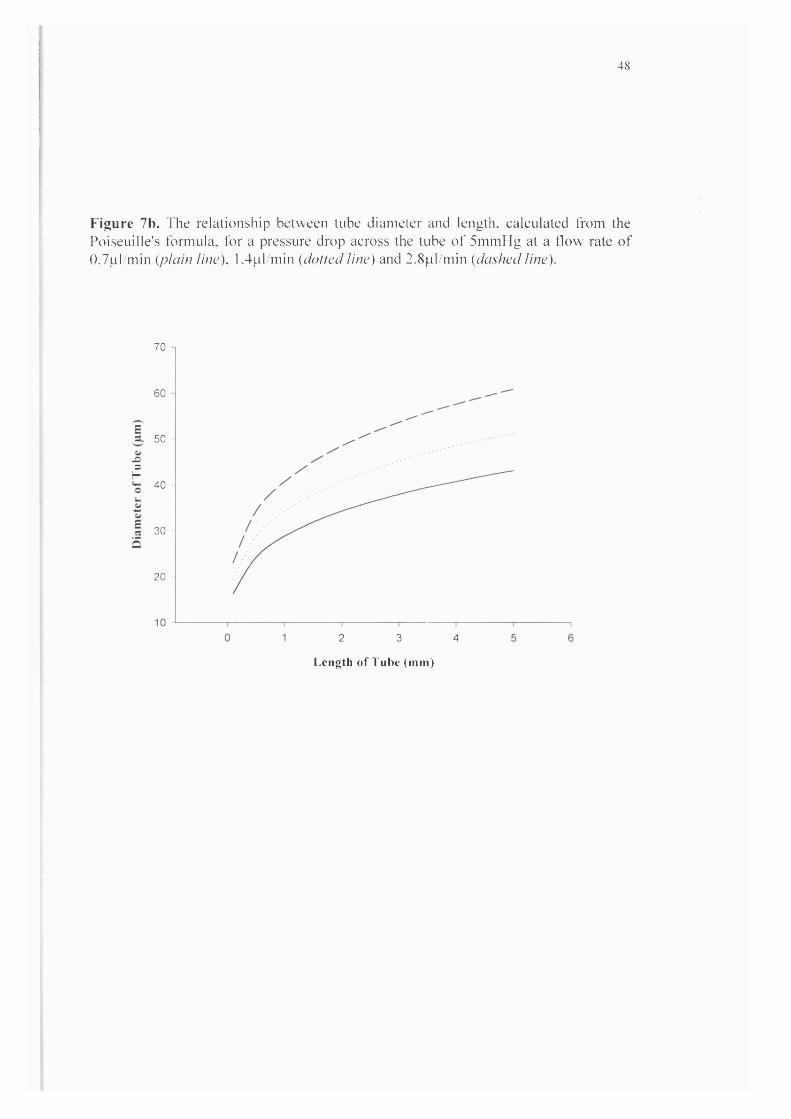
Figure 7b. I he relationship between tube diameter and length, calculated from the Poiseuille's formula, for a pressure drop across the tube o f 5mmHg at a flow rate o f 0.7pl/min {plain line), 1.4pl/min {dotted line) and 2.8pl/min {dashed line).
.a3f-
70 1
60 -
50 -
40 -
30 -
20 -
T
2 3 4
Length o f Tube (mm)
49
The relationship between pressure drop and diameter o f a tube 50 pm in length is
shown in Figure 7. For example, to obtain a pressure drop o f 5 mmHg, the diameter
o f the tube would be 16.2 pm.
W ith a multiple tube system, the flow rate through each hole will be correspondingly
reduced depending on the total number o f holes. The formula for the pressure gradient
is thus given by the following formula:
4Pressure drop = 128. p.l.Q / 136.N.7i.d
Where
N = Number o f tubes
2.3 Materials & Methods (Internal Flow Control)
2.3.1 Preparation of Polyimide discs & Excimer Laser Ablations
Single holes with target diameters o f 10pm, 15pm, 20pm and 25pm were drilled
using a 248 nm excimer laser (Figure 8) (Exitech Ltd, Oxford UK) in sample discs
(n=6 at each diameter) punched from 75pm thick polyimide sheet (Goodfellow Ltd
Cambridge, UK). Sample discs were mounted in a flow rig (Figure 9) designed to
measure the pressure drop across the discs, using filtered and degassed water as
previously described (Prata 1995). A flow rate o f 1.4 pl/m in was used throughout.
Repeated flow measurements (Figure 10) were taken (n=6) for each disc. Specimen
discs were removed from their holder and remounted between each measurement.

50
Figure 8. A schematic drawing o f the 248 nm (Krypton/Fluorine) excimer laser delivery system used (Model EX-PS-2000, Exitech Ltd, Oxford UK) (not to scale). Beam area at the target surface, and hence ablation diameter, was controlled by the mask aperture. The pulse repetition rate was set at 40Hz and a total o f 100 pulses were delivered to each disc. Specimens with target diameters o f 10 and 15 pm were ablated at a fluence o f 200 mJ/cm^ with mask diameters o f 300 and 450 pm respectively. Those with target diameters o f 20 and 25 pm were ablated at 170 mJ/cm^ with mask diameters o f 600 and 750 pm.
W orkpiece
248 nm Excimer Laser
ProjectionLensC ondenser Lens
M ask H older
51
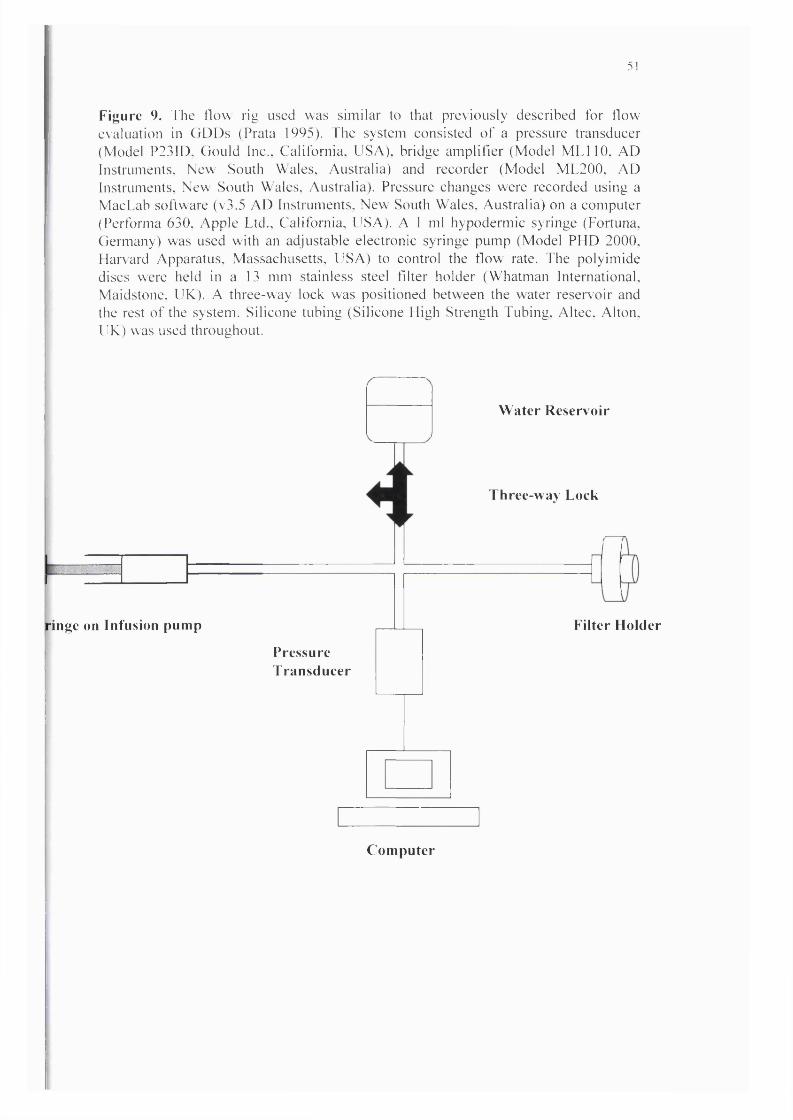
Figure 9. I 'he tlow rig used was similar to that previously deseribed for flow evaluation in GDDs (Prata 1995). The system eonsisted o f a pressure transdueer (Model P23ID. Gould Inc., California. USA), bridge amplifier (Model M L llO . AD Instruments. New South Wales. Australia) and recorder (Model ML200, AD Instruments. New South Wales. Australia). Pressure changes were recorded using a Mae Lab software (v3.5 AD Instruments. New South Wales, Australia) on a computer (Pertbrma 630. Apple Ltd.. California, USA). A 1 ml hypodermic syringe (Fortuna. Germany) was used with an adjustable electronic syringe pump (Model PHD 2000, Harvard Apparatus. Massachusetts. USA) to control the flow rate. The polyimide discs were held in a 13 mm stainless steel filter holder (Whatman International, Maidstone. UK). A three-way lock was positioned between the water reservoir and the rest o f the system. Silicone tubing (Silicone High Strength Tubing. Altee. Alton. UK) was used throughout.
Water Reservoir
Three-way Lock
ringe on Infusion pump
PressureTransducer
Filter Holder
Computer

52
Figure 10. A typical flow tracing, demonstrating stabilisation o f the pressure recording within approximately 3 minutes o f commencing infusion.
Pressuredrop
(mmHg)
sD
Tim e in m inutes
2.3.2 Flow Rig
The flow rig used was similar to that previously described for flow evaluation in
GDDs (Porter 1997; Prata 1995). The system consisted o f a pressure transducer
(Model P23ID, Gould Inc., California, USA), bridge amplifier (Model M LllO , AD
Instruments, New South Wales, Australia) and recorder (Model ML200, AD
Instruments, New South Wales, Australia). Pressure changes were recorded using a
MacLab software (v3.5 AD Instruments, New South Wales, Australia) on a computer
(Performa 630, Apple Ltd., California, USA). A 1 ml hypodermic syringe (Fortuna,
Germany) was used with an adjustable electronic syringe pump (Model PHD 2000,
Harvard Apparatus, Massachusetts, USA) to control the flow rate. The polyimide
discs were held in a 13 mm stainless steel filter holder (W hatman International,
53
Maidstone, UK). A three-way lock was positioned between the water reservoir and
the rest o f the system. Silicone tubing (Silicone High Strength Tubing, Altec, Alton,
UK) was used throughout. The transducer and the recording system were calibrated
using a water manometer daily prior to experimentation. Once the system was filled
with water, all gas bubbles were flushed out with the disc submerged in water within
the filter holder. At this point, the three-way lock was turned to open the system to
atmospheric pressure and the pressure reading zeroed on the computer. The three-way
lock was then turned to obtain a closed system and infusion pump started. The
pressure reading was allowed to stabilise over 20 minutes and the average reading
from the final 10 minutes was then taken as the pressure drop for the experiment. This
recording was repeated six times for each disc.
Pressure Drop = P 1-P2
Pi = back pressure in mmHg
P2 = atmospheric pressure in mmHg
2.3.3 Scanning Electron Microscopy & Image Analysis
After flow testing, all discs were coated in palladium and imaged using a scanning
electron microscope (JEOL, Akishima Japan). The dimensions o f each hole were
derived using image analysis software (Scion Image, Maryland USA) (Figure 11).
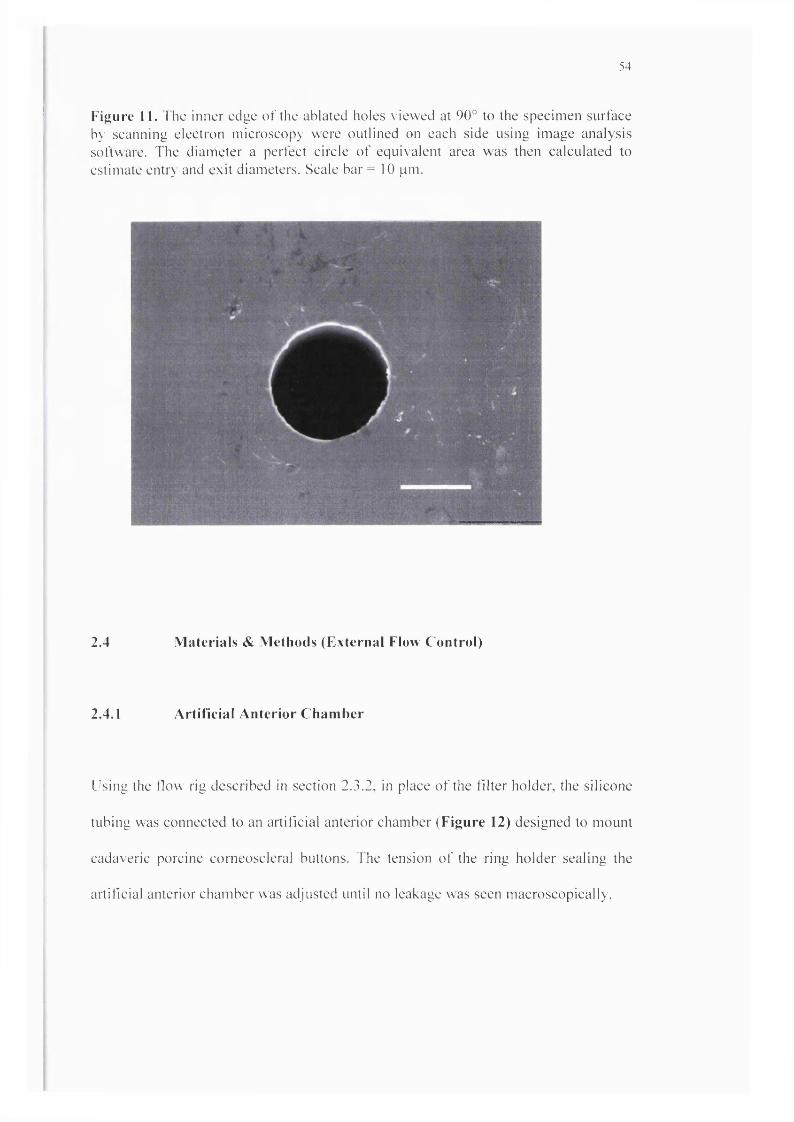
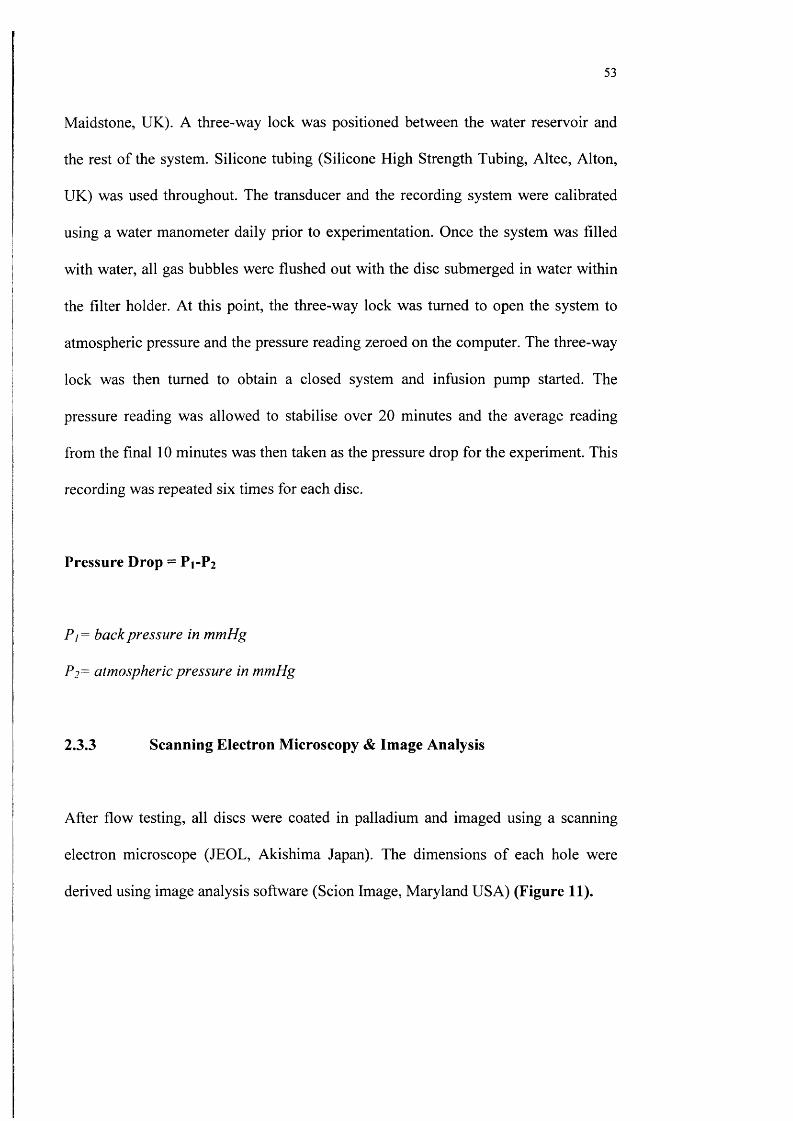
54
Figure 11. 1 he inner edge of the ablated holes viewed at 90° to the specimen surface by scanning electron microscopy were outlined on each side using image analysis software. The diameter a perfect circle of equivalent area was then calculated to estimate entry and exit diameters. Scale bar = 10 pm.
2.4 Materials & Methods (External Flow Control)
2.4.1 Artifleial Anterior Chamber
Using the flow rig described in section 2.3.2, in place o f the filter holder, the silicone
tubing was connected to an artificial anterior chamber (Figure 12) designed to mount
cadaveric porcine corneoscleral buttons. The tension o f the ring holder sealing the
artificial anterior chamber was adjusted until no leakage was seen macroscopieally.

55
Figure 12. Artificial anterior chamber designed to mount cadaveric porcine corneoscleral buttons and the tension of the ring holder sealing the artificial anterior chamber until no leakage was observed. Scale bar = 1 cm.
r

56
2.4.2 Occluded device implantation
Corneoscleral buttons (n=13) were prepared from cadaver pig eyes and mounted on
the artificial anterior chamber (Figure 12) infused with Tyrode solution. The infusion
rate was adjusted to produce a target pressure in the range o f 15-28 mmHg. After the
pressure had stabilised, standard occluded silicone tube implants (0.63 mm external
diameter) were inserted through 23G needle stab incisions at the limbus (conventional
technique), these were compared against prototype PM M A implants with a novel
hape profile (Figure 13) (0.6mm x 1.15 mm) inserted through 1.15 mm width (20G)
A Y R blade (Visitech, USA) stab incisions at the limbus (new technique). The
nfusion rate was maintained and a second pressure measurement was taken when the
iressure had stabilised. The difference between the first and second pressure
neasurement was then compared, as an index o f external leakage. Incisions were
utured and repeated at a different site in such that each implant was inserted in each
:ye with the order o f insertion randomised.

57
Figure 13. This is one embodiment o f a novel glaueoma drainage deviee (patent pending) ineorporating a small diameter hole (A; white cirele) to provide the required fistular resistance and a larger diameter hole (B; dotted circle) temporarily occluded by a thin ablatable membrane. 1 o give the lowest final lOP, resistance is bypassed by ablating this thin membrane using a Y AG laser delivered through a gonioseope once a mature bleb is established. The shape o f this implant is designed to eliminate external leakage after placement through a standardised slit incision. C = external part o f the deviee (Designed by Bruce Allan).

58
2.5 Results
Ablated tubes were found to have a near perfect circular outline on both the entry and
exit side. Observed entry and exit diameters are given in Table 7. All holes exhibited
a slight taper with entry diameters consistently larger than exit diameters.
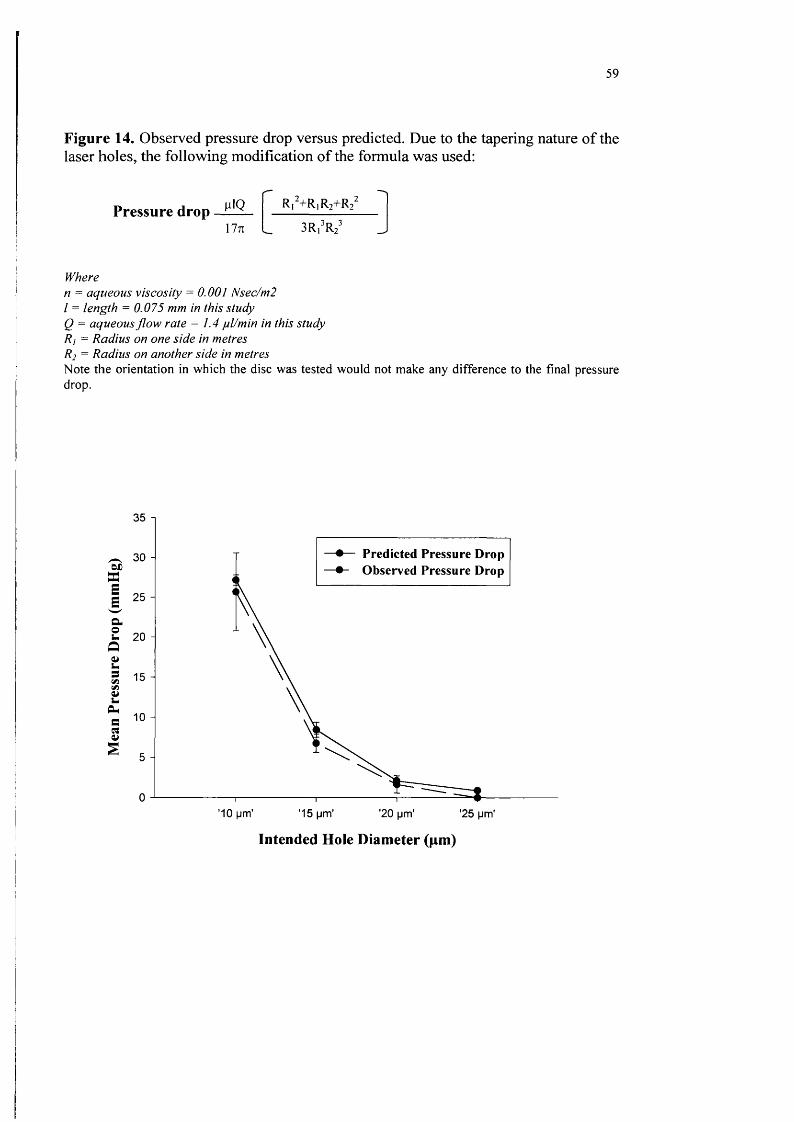
The observed pressure drop for the specimens examined correlated very closely with
that predicted by a correction o f the Poiseuille’s formula for tapered tubes using the
observed entry and exit diameters (Figure 14). Target ablations o f 15pm diameter
produced tubes that consistently achieved a pressure drop within the desired range (5-
15mmHg). Some variation between repeated flow measurements for the same
specimen was observed (Figure 15).
Table 7. Summary o f results. Target and observed holes’ diameters with the observed pressure drop in each group o f discs. The ’25 pm ’ group all have < 1 mmHg pressure drop.SD = standard deviation
Target Hole Diameter Observed Hole Diameter Observed Pressure Drop
(pm) (Mean ±SD pm) (Mean ± SD mmHg)
10 12.61 ± 0.05 (Entry side)
11 ± 0.05 (Exit side)25.66 ±4.9
15 16.67 ± 0.82 (Entry side)
15.1 ±0.25 (Exit side)6.76±1.15
20 24.32 ± 1.48 (Entry side)
21.26 ± 0 .3 (Exit side)1.66 ±1.07
59
Figure 14. Observed pressure drop versus predicted. Due to the tapering nature o f the laser holes, the fbllo\ving modification o f the formula was used:
Pressure drop glQ17%
Ri“+R|R2+R23R/R^
Wheren = aqueous viscosity ^ 0.00 i Msec/m2 I = length = 0.075 mm in this study Q = aqueous flo w rate ^ 1 . 4 yl/m in in this study Rj = Radius on one side in metres R2 = Radius on another side in metresNote the orientation in which the disc was tested would not make any difference to the final pressure drop.
35 1
-#— Predicted Pressure Drop Observed Pressure Drop3 -
I 2 5 -
'10 pm’ '15 pm' '20 pm' '25 pm'
Intended Hole Diameter (pm)

60
Figure 15. The pressure drop across 5pm tubes o f 75pm length was consistently within the desired target range (5-15m mHg) at a flow rate o f 1.4pl/min. Some variation between specim ens attributable to dimensional variation was observed along with some variation between m easurem ents (n=6; SD shown above by error bars) for the same specimen.
12 1
0 1 2 3 4 5 6
Disc Number

61
In the external leakage study, pre-insertion pressures (mmHg; mean ± SD) were
19.00±4.3 (conventional method) and 20.00±3.9 (new technique with PMMA
prototypes). Post-insertion pressures were significantly reduced (10.40±7.7; p<0.01)
for the conventional technique and were essentially unchanged for the new technique
(18.80±4.9; p>0.1) (Figure 16) PM M A prototypes were considerably easier to insert
than conventional silicone tubing.

62
Figure 16. Graph showing the mean pre-insertion and post-insertion pressures (error bars = SD) for standard occluded tubes and prototypes with the modified external cross-section. Post-insertion pressures were significantly reduced (10.40±7.7; p<0.01) for the conventional technique and were essentially unchanged for the new technique.
Pre Post Pre Post
25
nin
Hg
20
15
10
IVIVR P a ra cen tes is & P ro to ty p e 23G P a ra c en tes is & C o n v en tio n a l T u b e

63
2.6 Discussion
Leading current GDDs have been developed with little available data to substantiate
manufacturers’ claims for flow performance (Krawczyk 1995) or biocompatibility.
Recent evaluation has exposed design flaws (Lee 1998), poor quality control in
manufacture (Porter 1997), and poor flow control (Prata 1995). To gain acceptance as
a method o f preventing hypotony in routine GFS, a new GDD must demonstrate
consistent control over internal flow (flow through the GDD), good protection from
external leakage (leakage between the exterior o f the GDD and the sclerocomeal
tissues through which it is implanted), and excellent biocompatibility. We have
adapted existing methods o f evaluating GDD flow performance in an examination o f
internal flow control using single small diameter tubes as flow resistors.
The good fit between the observed pressure drop across specimen tubes and that
predicted by the Poiseuille's formula was an expected finding. Poiseuille's formula is
applicable where laminar flow exists in a fluid o f uniform viscosity contained within a
rigid tube. Uniform viscosity can be assumed for aqueous, and the likelihood o f
turbulence within a system increases with flow velocity. Physiological flow rates are
sufficiently slow that laminar flow would be established within 2pm o f tube entrance,
and edge effects would be insignificant. Low level lumenal elasticity would be
tolerated in any GDD system using small diameter tubes as flow restrictors.
Polyimide is widely available, inexpensive, and absorbs light strongly at 248nm.
Relatively thin sheets (75 pm) were used to facilitate accurate ablation, and to allow
for the possibility o f subsequent perforation using a Nd:YAG laser to abolish fistular

64
resistance. The logic here is that fistular resistance would only normally be required in
the early postoperative period, prior to the development o f a mature conjunctival
filtration bleb and adequate resistance to flow distal to the GDD. A <20pm hole could
block even with a single macrophage and is unlikely to be practical as a flow resistor
in vivo. Longer tubes imparting equivalent fistular resistance would allow the use o f
larger diameters (Figure 7b), and could be incorporated alongside a larger diameter,
low resistance tube guarded by a thin Y AG ablatable membrane in a GDD with
reversible fistular resistance (Figure 13).
The observed variation between flow measurements for given specimens (Figure 15)
may have been attributable to minor accretions o f debris within the tube lumens
during specimen handling. This highlights the importance o f using a material that
would resist protein conditioning and cellular adhesion in vivo. In the following
chapter we explore the use o f phosphorylcholine (Hall 1989) based polymers in this
context.
The excimer laser system used was non-dedicated. Improvements in laser delivery are
possible that would enhance accuracy and reduce the taper produced by a convergent
beam. Extrusion and moulding technologies may also be applicable, particularly
where longer tubes are used. Even with the system used, ablation was considerably
more accurate than for laser sclerostomy (Allan 1993).
The needle used to form the paracentesis tract in conventional GDD implantation is
either a 22G or 23G (Coleman 1995). Our study o f protection from external leakage
has shown that, even through the smaller 23G paracentesis tracts, insertions were
65
liable to cause significant leakage in some eyes. In addition to protecting from
external leakage effectively, our shape modifications and the use o f a standardised
MVR blade incision reduced the effort and manipulation required for device insertion
considerably.
2.6 Conclusions
We have shown that it is possible in principle to control the dimensions o f a
manufactured tubular lumen in a GDD accurately enough to provide consistent
protection from hypotony in the early period after GFS. We have also demonstrated
good protection from external leakage using a prototype device with a modified
external profile designed to bear evenly on a standardised slit incision.

66
CHAPTER THREE - Biocompatibility Studies
Abstract
Aim
We set out to compare phosphorylcholine coated polymethyl methacrylate (PC-
PMMA) with materials used in existing and experimental glaucoma drainage devices
in a series o f in vitro assays reflecting key dimensions o f biocompatibility in the
context o f glaucoma drainage device implantation.
Methods
Sample discs o f PC-PMMA and control materials (silicone, PMMA, polypropylene,
and PTFE) were exposed to fibrinogen, fibrin, human tenons capsule fibroblasts,
human macrophages and a conjunctival bacterial isolate (staphylococcus epidermidis)
in standardised quantitative assays designed to measure the adherent biomass. Areas
o f damage to cultured monolayers o f bovine comeal endothelial cells produced by
standardised direct contact with test material discs were also measured.
Results
Fibrinogen and fibrin adhesion to PC-PMMA were significantly lower than uncoated
PM M A (p=0.004). Phosphorylcholine coating o f PMMA also significantly reduced
the adhesion o f human scleral fibroblast (p=0.002), bacteria (p= 0.002) and
macrophage (p=0.01) compared with uncoated PMMA. All the other biomaterials
showed either similar or insignificantly different levels o f adhesion to all the proteins
and cells tested, except for polypropylene, which had a significantly higher level of
bacteria adhesion than PMMA (P = 0.026). PC-PMMA also had the lowest area o f
endothelial damage.

67
Conclusion
Phosphorylcholine coating is a new material technology that offers considerable
promise in the field o f glaucoma drainage device development.
68
3.1 Introduction
The high complication rates associated with existing GDDs have restricted their use to
circumstances in which trabeculectomy is unlikely to succeed (Melamed 1990).
Although laser technologies and new design concepts described in Chapter Two,
suggest the possibility o f using GDDs to provide consistent flow control in routine
glaucoma filtration surgery, acceptance would require an improvement in the
biocompatibility o f materials used in construction. In particular, since the internal
dimensions o f a GDD flow pathway could quickly be modified in vivo by biological
spoliation, leading to marked and uncontrolled increases in flow resistance, a material
which resists non-specific protein and cellular spoliation effectively would be vital.
This chapter will highlight the problems associated with poor biocompatibility in the
context o f GDDs and examine the biocompatibility indices o f a new bioinert material.
Biocompatibility refers to the ability o f a synthetic material to interface with living
tissues without provoking a detrimental reaction. W ithin the context o f GDD
implantation, suboptimal biocompatibility is manifest in an array o f complications
including tube occlusion, endophthalmitis, comeal endothelial failure, tube migration,
extrusion, and fibrous encapsulation leading to filtration failure. Key elements in the
mechanism o f these complications are protein adhesion and micromotion.
Elastomeric silicone (polydimethylsiloxane) remains the most commonly used
material in current GDDs. Silicone, polymethyl methacrylate (PMMA),

69
polypropylene (Figure 17) and other hydrophobic polymers used in GDDs have a
relatively high binding affinity for plasma and interstitial fluid proteins including
albumin, IgG and fibrinogen. These proteins are adsorbed within seconds o f
implantation (Pitt et al 1988). Cellular adhesion, cytokine release and chronic
inflammation all occur as secondary events following the deposition o f a conditioning
protein film (Tang & Eaton 1995).
Bioinert materials are designed to resist protein and cell adhesion non-specifically,
minimising inflammatory responses, and preventing occlusion in implants used in
fluid contacting environments (Allan 1999).

70
Figure 17. Polymers commonly used in ophthalmology.
C = 0 Polymethyl meethacrylate (PMMA)
Silicone
[-CH2-C-]-
CH2OH
[-CH2-CH-]
Poly(2-hydroxyethyl methacrylate) [polyHEMA hydrogel]
Polypropylene (PP)
-[-CF2-CF2-]- Poly(tetrafluoroethylene)

71
3.2 Bioinert Materials
3.2.1 Heparin Coating
Covalently linked heparin surface modification (Figure 18) has been used as a
strategy to reduce cellular spoliation and inflammation associated with intraocular
lens implantation after cataract surgery (Larsson 1989). In comparison with uncoated
PMMA, reported clinical benefits include reduced post-operative inflammation
(Starvou 1994) and less giant cell spoliation (Trocme 2000). In vitro results suggest
less bacterial (Portoles 1993) and lens epithelial cell (Majima 1996) adhesion.
Heparin prevents thrombus formation by binding to antithrombin III (ATIII) and
catalysing the action o f ATIII to neutralise thrombin, thus preventing catalysis and
cleavage o f fibrinogen to fibrin.
Although heparin coating allows PMMA to become more bioinert, modem alternative
lOL materials, including dimethyl siloxane (silicone) and 2-hydroxyethl methacrylate
HEMA have proved to be superior in both in vivo (Ravalico 1997) and in vitro (Joo
1992, M ajima 1996). Most contemporary GDDs use elastomeric silicone for at least
the tube component.

72
Figure 18. A schematic representation o f heparin immobilized onto the surface o f a polymer substrate using hydrophilic spacer groups.
HepariiHeparii
Heparii
Hydrophilic spacer groups
Substrate

73
3.2.2 Surface Passivation
In contrast to the use o f a molecule such as heparin with a specific biological action to
prevent biological spoliation, surface passivation refers to the process o f making a
surface unreactive by coating with a thin layer o f a relatively unreactive material.
Polymer surfaces passivated by albumin have been shown to reduce occlusion in
extracorporeal circulation systems (Mulvihill 1990) and to reduce the level o f platelet,
neutrophil, and macrophage adhesion (Tang 1993) compared with unmodified control
materials.
Early in vitro studies indicated reduced endothelial cell damage on contact with
surface passivated intraocular lenses (Balyeat 1989). However, this optimism was not
translated to later clinical (Umezawa 1993, Amon 1996, Ravalico 1997), and
experimental studies (K ochounianl991, Majima 1996, Lawin-Brussel 1992), and
albumin surface passivation has not been pursued as a strategy for rendering
ophthalmic implant materials bioinert.
3.2.3 Hydrogels
Hydrogels are cross-linked polymeric structures with high water content (Figure 17).
A hydrogel in routine ophthalmic use as a soft contact lens material and in intraocular
lenses is HEMA (Barrett 1987). HEMA is closely related to PMMA. Synthesis
involves the adding o f a methylol group to the common methyl methacrylate side
group. This addition results in an extremely hydrophilic polymer (HEMA). Increased
74
hydration appears to reduce protein and cell spoliation, but protein deposition remains
a significant clinical problem for HEMA contact lenses, and HEMA has not been
widely adopted as an lOL material (Allan 1999). Suitability for use in GDDs has been
thrown into doubt by reports o f hydrogel fragmentation (D ’Hermies 1998) and
extensive cell adhesion (Ayyala 2000) when placed sub-conjunctivally.
3.2.4 Polyethylene Oxide Polymers
Polyethylene oxide polymers (PEG) are another potentially useful group o f bioinert
materials, which loosely reflect some o f the properties o f natural mucous membrane
surfaces. PEG polymers are highly hydrophilic, mobile, long chain molecules, which
trap a large hydration shell. They enhance resistance to protein and cell spoliation
when grafted onto a variety o f material surfaces (Kim 1996, Cao 1996). PEG
polymers are also amenable to end group coupling for surface immobilisation o f
biologically active molecules such as heparin to add specific functionality (Cao 1996).
3.2.5 Biomimetic bioinert materials
Increasingly, biomaterials solutions are sought through mimicking or incorporation
natural structures in synthetic materials (Allan 1999). This biomimetic approach has
been adopted in the synthesis o f a new class o f polymers based on phosphorylcholine
(PC) (Figures 19-21). PC is the hydrophilic head group o f the predominant
phospholipids (lecithin and sphingomyelin) in the outer envelope o f mammalian cell
membranes (Hayward 1984; Durrani 1986; Kojima 1991). PC polymers are designed
to approximate the chemical properties o f the natural cell wall, and in particular the

75
ability to resist non-specific protein attachment. As coatings or bulk materials, these
biomimetic bioinert polymers are thought to have enhanced resistance to non-specific
protein adhesion. Early applications o f this technology have included chest drains
(Hunter 1993) and contact lenses (Knzler 1994).

76
Figure 19. A schematic representation o f the mammalian cell wall. Highly hydrated phosphorylcholine head groups (small spheres) are orientated externally in this selfassembling bilayer. Biocompatibles PC technology is based on the observation that the outside leaflet o f a red blood cell membrane is haemocompatible, while the inner leaflet is thrombogenic.
Figure 20. The inner, thrombogenic surface contains negatively charged phospholipids while the outer bilayer is composed o f zwitterionic phospholipids. These have both positive and negative charges in close proximity but are electrically neutral overall.

77
Figure 21. The phosphorylcholine (PC) coating mimics the zwitterionic structure of
natural membranes, thereby conferring properties of haemocompatibility. (A) The PC
headgroups bind large numbers of water molecules tightly around them, making it
energetically unfavourable for other materials to interact with the PC surface. (B)
Further away the water molecules are bound less strongly, sliding over one another
resulting in a low coefficient o f friction.

78
3.3 Biocompatibility in the Context o f Glaucoma Drainage Devices
Key dimensions o f biocompatibility in relation to GDD implantation are: resistance to
non-specific biological spoliation and tube occlusion, resistance to fibrotic
encapsulation and drainage failure (foreign body reactions), reduced contact
associated corneal endothelial damage, and resistance to bacterial adhesion. Each o f
these elements is considered below.
3.3.1 Protein & Cell Adhesion - Tube Occlusion
Valve mechanisms in glaucoma drainage devices (GDDs) have largely failed to
provide consistent flow control and protection from hypotony. Limitations o f
currently marketed valved devices have recently been exposed in theoretical (Lee
1998) experimental (Prata 1995; Porter 1997) and clinical examinations (Lim 1998).
Flow control in non-valved devices is critically dependent on the internal dimensions
o f the flow passage. For tube devices, resistance varies with the fourth power o f tube
diameter in accordance with Poiseuilie's law (McEwen 1958). Small changes in
diameter induced by protein or cellular spoliation may lead to substantial changes in
flow performance. Resistance to surface spoliation is therefore a key requirement for
materials used in GDDs which seek to control flow using single or multiple small
bore tubes as flow resistors.

79
Protein and cellular components, which are likely to play an important role in tube
surface spoilation in the post-operative aqueous environment, include fibrinogen,
fibrin, and macrophages. Small-bore filtration channels may also be capped off
externally by scleral fibroblasts growing into a fibrin scaffold (Shahinian 1992).
3.3.2 Protein and Cell Adhesion - Chronic Inflammation & Bleb Fibrosis
As with all implanted biomaterials, GDDs stimulate a foreign body reaction and a
variable degree o f chronic inflammation. In the context o f GDD implantation, this
chronic inflammatory process will lead to progressive fibrous encapsulation. This
chain o f events limits the filtration life o f all contemporary GDDs (Table 5; Chapter
1: Page 27).
In vivo studies using rabbits have suggested that both physical and chemical
properties o f biomaterials may determine the level o f inflammation (Ayyala 2000)
and consequent fibrous encapsulation thickness (Jacob-Labarre et al 1996) related to
subconjunctival implants. Although the mechanism o f foreign body reactions is
incompletely understood, it is likely that fibrinogen adhesion is important in the
initiation o f inflammatory responses (Tang 1993). Adherent macrophages may play a
major role (Schoen 1996) in orchestrating the cytokine drive to chronic inflammation.

80
3.3.3 Cell Damage - Endothelial Failure
Comeal endothelial failure is a common complication GDDs implantation (Chapter
1), occurring in up to 34% o f cases after a mean follow up o f two years in GDDs
implantation after previous comeal graft surgery (Beebe 1990).
The mechanism for endothelial failure after GDD implantation is not fully
understood. Continued small movements o f the tube element relative to the com ea
(micro-motion) transmitted from repeated minor displacement o f the GDD plate
element during eye movement may be important in accelerating endothelial loss. This
gradual attrition may be superimposed on significant intraoperative endothelial
damage, and damage in the early postoperative period from macroscopic contact
between the implant and the com ea in association with poor tube positioning or
anterior chamber shallowing.
Each o f these possible elements o f the mechanism for endothelial failure after GDD
implantation involves contact between the endothelium and the implant. Studies o f
comeal endothelial cell damage resulting from standardised direct contact with
intraocular lenses have shown variation between materials (Kassar 1980, Barrett
1984, Mateo 1989, Balyeat 1989). A material for which contact induced endothelial
damage is relatively low should help reduce endothelial loss in association with GDD
implantation.

81
3.3.4 Bacterial Adhesion - Endophthalmitis
Endophthalmitis associated with GDD is a rare but serious complication, with an
overall incidence o f less than 0.5% (Table 6; Chapter 1: Page 29). The possible
routes o f bacterial entry include; contaminated surgical instruments or GDD and GDD
erosion. The initial adhesion o f bacteria to polymer substrata is a complex process but
can be assumed to be dependent upon the host environment, materials and the type o f
cells involved (Gristina 1996). Once bacteria are organised within a ‘biofilm ’
(Gristina 1987), they become relatively resistant to both antibiotics and host defence
mechanisms.
3.4 Aims
We set out to compare PC-coated polymethyl methacrylate (PMMA) with materials
used in existing and experimental GDDs (Table 3; Chapter 1: Page 18) in a series o f
in vitro assays reflecting key dimensions o f biocompatibility in the context o f GDD
implantation.
3.5 Materials & Methods
3.5.1 Preparation of Discs
Sample discs (8mm diameter) were punched from 0.5mm thick sheet PMMA cast
from polymer beads (ICI, London, UK), polypropylene (Goodfellow, Cambridge,
UK), PTFE (Goodfellow, Cambridge UK), and silicone (Goodfellow, Cambridge,

82
UK). Additional PMMA discs were eoated with P C I008 (2:1 copolymer o f lauryl
methacrylate and methacryloyl phosphorylcholine) (Biocompatibles, Famham UK).
Sample discs were washed sequentially with a 7X-PF detergent (ICN
Pharmaceuticals, Hants. UK) and distilled water. The coated discs were then air-dried
in sterile conditions for 10-15 minutes at room temperature prior to experimentation.
Six dises o f eaeh material were used for each o f the adhesion assays.
3.5.2 Cell and Protein Adhesion
3.5.2.1 Fibrinogen Adsorption
I'^^-labelled fibrinogen (ICN Pharmaceutical, Hants. UK) was diluted (ratio 1:9) with
unlabelled human fibrinogen (Sigma, Dorset, UK) in 12.6ml o f phosphate buffered
saline (PBS). A total o f 25.2ng o f fibrinogen in 40pl o f solution was pipetted onto
each disc in a 24 well plate and incubated at room temperature for 2 hours. The discs
were then washed (x3) in PBS, transferred to scintillation vials and submerged in
scintillation fluid. The scintillation count for each vial was then measured over one
minute in a Liquid Scintillation Counter (Model 1209 Rack Beta, LKB Ltd., USA).
3.5.2.2 Fibrin Adhesion
Fresh venous blood (20ml) was obtained from a healthy adult male volunteer in a
citrated vial to prevent clotting. The blood was centrifuged for 10 minutes at 3000
rpm to obtain plasma. 0.1ml o f plasma was diluted with 1ml o f normal saline. 0.1ml
o f 0.025M calcium chloride solution was then added to this mixture to initiate

83
clotting. 0.2ml o f this solution was immediately pipetted onto centre o f each sample
disc. These discs were incubated for 2 hours at room temperature to allow the
formation and adherence o f fibrin, before being washed (x3) in PBS and transferred to
a sterile 24 well plate. Fibrin deposits were dissolved by adding 0.2ml o f 4M
guanidine thiocyanate into each well with constant agitation (30 rpm) for 1 hour at
room temperature. The tyrosine residue in 0.1ml o f this solution was measured as a
quantification marker for dissolved fibrin using a spectrophotofluorometer (Model
7687, American Instrument Company, Maryland, USA) (excitation wavelength
275nm; emission wavelength 310nm).
3.5.2.3 Human Scleral Fibroblast Adhesion
Eye bank scleral rim tissue from adult donors (Moorfields Eye Hospital Eye Bank)
was cultured to produce a strain o f scleral fibroblasts in Eagle’s minimal essential
medium (MEM) (Gibco, Life Technology Ltd., Paisley, UK) supplemented with 10%
foetal calf serum, 1% penicillin and 1% streptomycin. Cells were serially passaged to
6-7 population doublings by standard trypsin-EDTA dispersion. The fibroblasts were
then seeded in MEM at a density o f 6000 cells cm'^ into wells containing the sample
discs, and incubated at 37°C under 5% CO2 to allow attachment for 48 hours. The
discs were then washed (x3) in PBS and transferred to a new 24 well plate.
Intracellular ATP was liberated by incubating each disc with 100 ml o f sterile
hypotonic lysis buffer (0 .0IM Tris-Acetate pH8, 2mM EDTA). After 30 minutes the
ATP solution was diluted 1:1 with an additional buffer (0.2M Tris-HCl, 0.2mM
EDTA, pH 7.3). ATP levels in this buffered lysate were then measured as a
quantification marker for the adherent fibroblasts by ATP dependent luminometry.

84
using a commercial luciferase test kit (BioOrbit-W allac, Turku, Finland) and a 96
well plate luminometer (Amersham, Bucks. UK).
3.S.2.4 Macrophage Adhesion
M ononuclear cells were purified using commercial gravity separation media as
described below. Fresh venous blood was obtained from a healthy 32 year-old male
volunteer. The blood was defibrinated by agitation in a vial containing sterile glass
beads for 5 minutes. The blood was then diluted 1:1 with Macrophage Serum Free
Medium (RPMI1640 medium, Gibco, Life Technology Ltd., Paisley, UK) and slowly
pipetted into a tube containing a purification medium (LymphoSep, ICN-
Pharmaceuticals, Hants. UK). The mixture was centrifuged at 400g for 20 minutes to
separate the cells. The central layer containing the mononuclear cells was sampled.
The mononuclear cells were then pelleted by a further centrifugation at 400g for 10
minutes. The mononuclear cells were re-suspended in RPMI1640 medium and
counted using a haemocytometer. Sample discs were placed in a 24 well tissue culture
plate and 2x10^ cells in 0.5 ml o f media are pipetted onto each disc in sequence. The
plates were incubated for 24 hours in a 37°C incubator under 5% COi.The discs were
then washed (x3) with PBS and fixed in 4% paraformaldehyde for 10 minutes at room
temperature. The fixed cells were then permeabalised by incubation with a 1%
solution o f Triton X I00 (Sigma, Dorset, UK) for 2 minutes, and macrophages
detected using the protocol described below using an Avidin-Biotin-Peroxidase kit
(RapidStain, Sigma, Dorset, UK).

85
Endogenous peroxidase activity in the cells was quenched by 72 hours incubation in
9% H2O2 and repeated washing in PBS. Mouse anti-human macrophage (CD68)
monoclonal antibody (Dako Ltd. Bucks. UK, diluted 1:100 in PBS + 1% Foetal C alf
Serum) was added to each disc and allowed to incubate overnight at 4°C in a
humidified chamber. The discs were then washed (x3) in PBS and macrophages were
observed using a high affinity biotin conjugated anti-mouse antibody and an avidin-
peroxidase detection system with AEG as a chromogen. The average number o f
macrophages (stained red) was determined in 50 randomly selected fields under light
microscopy.
3.5.2.5 Data Analysis
For each o f the cell adhesion assays above, results are presented graphically as box-
plots showing the 10̂ *̂ , 25̂ *̂ ’ 50^ '̂ and 90^ ̂ centiles as vertical boxes with error
bars. Statistical analysis was performed using SPSS for W indows software (SPSS
Inc., Chicago, USA). The Mann-W hitney non-parametric test was used to detect any
statistically significant differences between uncoated PM MA and the other test
materials.
3.5.3 Endothelial Damage
A commercially available strain o f BCE cells (Strain CRT-2048, American Type
Cultural Collection, New Jersey, USA) was purchased and seeded in 24 well culture
plates in D ulbecco’s Modified Eagle’s Medium (Gibco, Life Technology Ltd.,
Paisley, UK) supplemented with 10% foetal calf serum and 5% foetal bovine serum.
The BCE cells were grown to confluence at 37®C in 5% CO2 with a change o f media

86
every two days. Before each contact assay, media were aspirated from the
monolayers, which were rinsed with Im L o f fresh medium to remove all unattached
cells.
13 mm diameter discs o f silicone, PMMA, PTFE, polypropylene and PC-PMMA
(n=6) were gently lowered onto the BCE monolayers using a vacuum suction device
with a 2.4 g o f titanium weight placed on top o f each disc. The weights and discs were
removed using a pair o f forceps and a vacuum suction device after 5 minutes o f
contact. A 0.4% trypan blue solution was used to stain damaged cells.
After staining, the central area o f each plate was photographed at low magnification
under a light microscope. Digital photographs were then analysed and areas with
staining and stripping o f cells were outlined. The total area o f damage in each well
(including the area stripped o f cells) was measured using image analysis software
(Scion Image, M aryland USA) and expressed as a percentage o f the total disc area to
derive a damage coefficient for each material.
Analysis o f variance (ANOVA) using the Bonferroni method was performed using
SPSS for Windows software (SPSS Inc., Chicago, USA) to compare endothelial
damage coefficients between materials.
3.5.4 Bacterial Adhesion
Staphylococcus Epidermidis strain 901, a clinical isolate, was grown in liquid culture
in Oxoid No. 2 broth at 37^C in 5% CO2. Bacterial cells were pelleted in a refrigerated
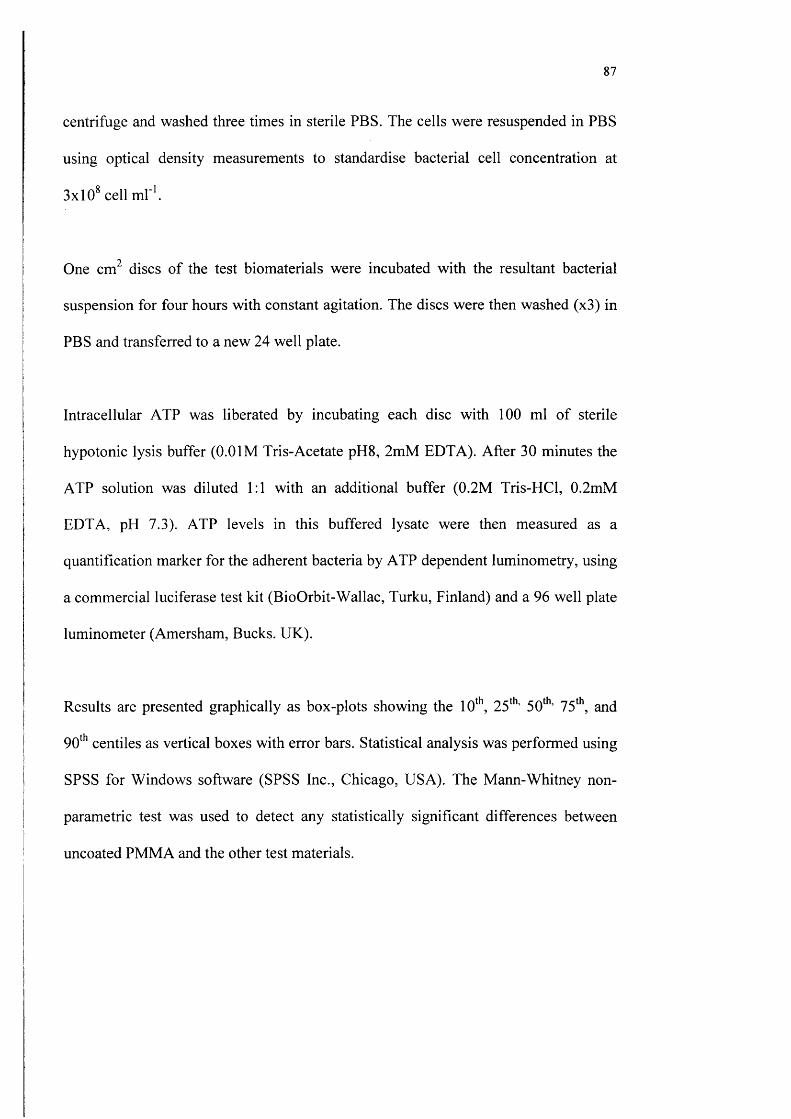
87
centrifuge and washed three times in sterile PBS. The cells were resuspended in PBS
using optical density measurements to standardise bacterial cell concentration at
3x10* cell m l''.
One cm^ discs o f the test biomaterials were incubated with the resultant bacterial
suspension for four hours with constant agitation. The discs were then washed (x3) in
PBS and transferred to a new 24 well plate.
Intracellular ATP was liberated by incubating each disc with 100 ml o f sterile
hypotonic lysis buffer (0.0IM Tris-Acetate pH8, 2mM EDTA). After 30 minutes the
ATP solution was diluted 1:1 with an additional buffer (0.2M Tris-HCl, 0.2mM
EDTA, pH 7.3). ATP levels in this buffered lysate were then measured as a
quantification marker for the adherent bacteria by ATP dependent luminometry, using
a commercial luciferase test kit (BioOrbit-W allac, Turku, Finland) and a 96 well plate
luminometer (Amersham, Bucks. UK).
Results are presented graphically as box-plots showing the 10‘*̂, 25**̂ ’ 50̂ *̂ ’ 75* ,̂ and
90̂ '̂ centiles as vertical boxes with error bars. Statistical analysis was performed using
SPSS for Windows software (SPSS Inc., Chicago, USA). The M ann-W hitney non-
parametric test was used to detect any statistically significant differences between
uncoated PMMA and the other test materials.

88
3.6 Results
3.6.1 Proteins & Cell Adhesion
Fibrinogen adsorption is illustrated in Figure 22. Only PC-coated PMMA discs
reduced the amount o f fibrinogen adsorption significantly (p=0.004), relative to
PMMA. Figure 23 shows fibrin adhesion on the test materials. Fibrin adhesion to the
PC-coated PMMA discs was minimal, and significantly lower than un-coated PMMA
(p=0.004), with other materials exhibiting similarly elevated fibrin adhesion levels.
PC coating the PMMA discs also modified the cellular adhesion profiles and these
results are shown in Figures 24 and 25. The reduction in human scleral fibroblast
adhesion to PC-coated PMMA was statistically significant (p=0.002) compared to un
coated PMMA discs (Figures 24). The adhesion o f human scleral fibroblasts to
silicone, polypropylene and PTFE discs was not significantly reduced in comparison
with PMMA (Figure 24). The adhesion o f human macrophages was also significantly
reduced by PC coating o f PMMA (p=0.01) (Figure 25). Although both the PP and
PTFE discs have a higher mean number o f macrophages adherent per field in
comparison with un-coated PMMA discs, these differences are not statistically
significant (p=0.057).
3.6.2 Bovine Endothelial Cell Damage
Percentage areas o f damage (mean ±SD) after standardised contact were as follows:
PMMA 5.95+4.60%; polypropylene 1.63±0.81%; PTFE 1.00±0.19%; silicone

89
3.08+2.68% and PC-PMM A 0.15±0.25% (Figure 26). The uncoated PMMA discs
tested caused considerable damage, evidenced by the marked stripping o f endothelial
cells (Figure 27). Significant endothelial cell disruption was also a feature o f contact
with silicone specimen discs. Only PC-PMMA discs had a level o f damage (p=0.04)
significantly lower than that observed for uncoated PMMA.
3.6.3 Bacterial Adhesion
The mean light unit o f bacteria adhered to polymer surfaces were as follows: PMMA
0.33 ± 0.32, PC-PMM A 0.02 ± 0.01, silicone 0.37 ± 0.03, PTFE 0.30 ± 0.19 and
Polypropylene 4.06 ± 3.2. %. Results are presented graphically as box-plots showing
the 10*'\ 25‘̂ ’ 50̂ *̂ ’ 75‘'\ and 90*'’ centiles as vertical boxes with error bars (Figure 28).
The uncoated PMMA disc tested had considerable more bacteria adhered to its
surface compared with PC-coated PMMA disc (Figure 29). Only PC-PMMA discs
had a significantly lower level o f bacterial adhesion (p= 0.0.002) than other test
materials. Polypropylene discs had significantly higher levels o f bacterial adhesion
compared to PMMA (p=0.026).
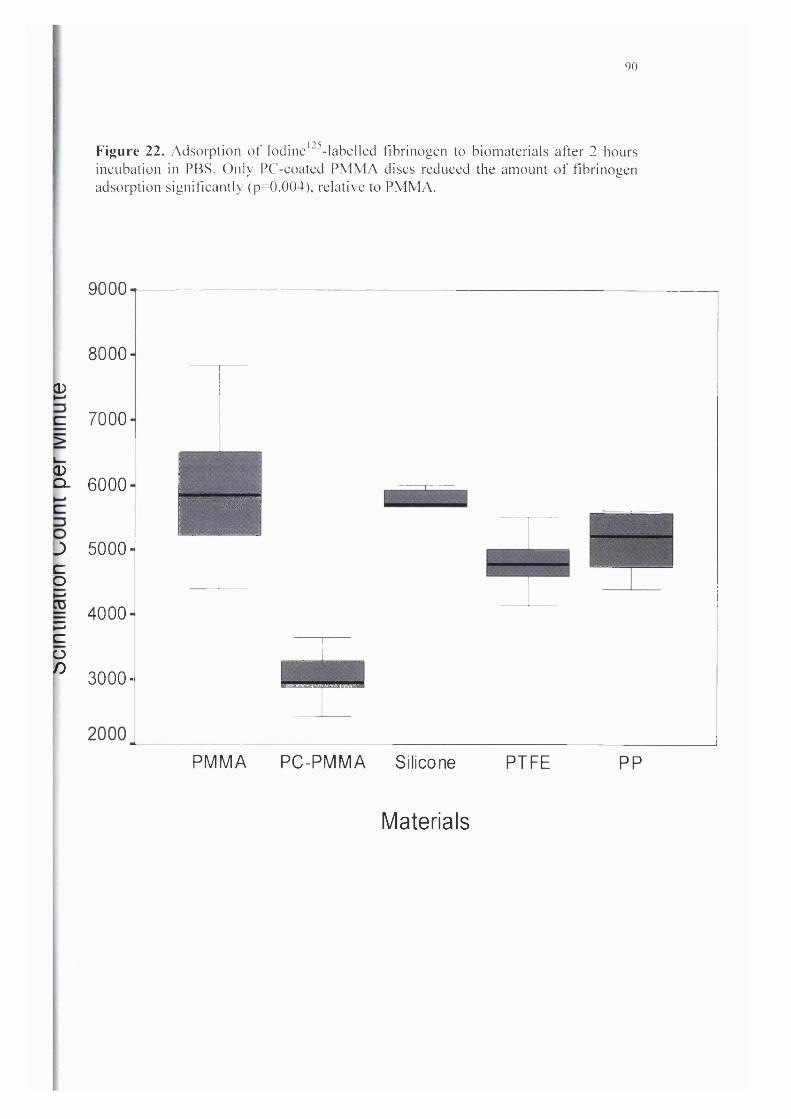
90
Figure 22. Adsorption o f Iodine’"^-labelled fibrinogen to biomaterials after 2 hours incubation in PBS. Only PC-coated PM M A discs reduced the amount o f fibrinogen adsorption significantly (p=0.004), relative to PMMA.
CD
9000
8000
7000
CDp- 6000
J 5000bo
pcon
4000
3000-
W -
PMMA PC-PMMA Silicone PTFE PP
Materials

91
Figure 23. Adhesion o f fibrin to biomaterials from fresh plasma after 2 hours incubation. The level o f fibrin adhesion to PC-coated PMMA discs was minimal, and significantly lower than un-coated PMMA (p=0.004).
PMMA PC-PMMA Silicone
M ateria ls
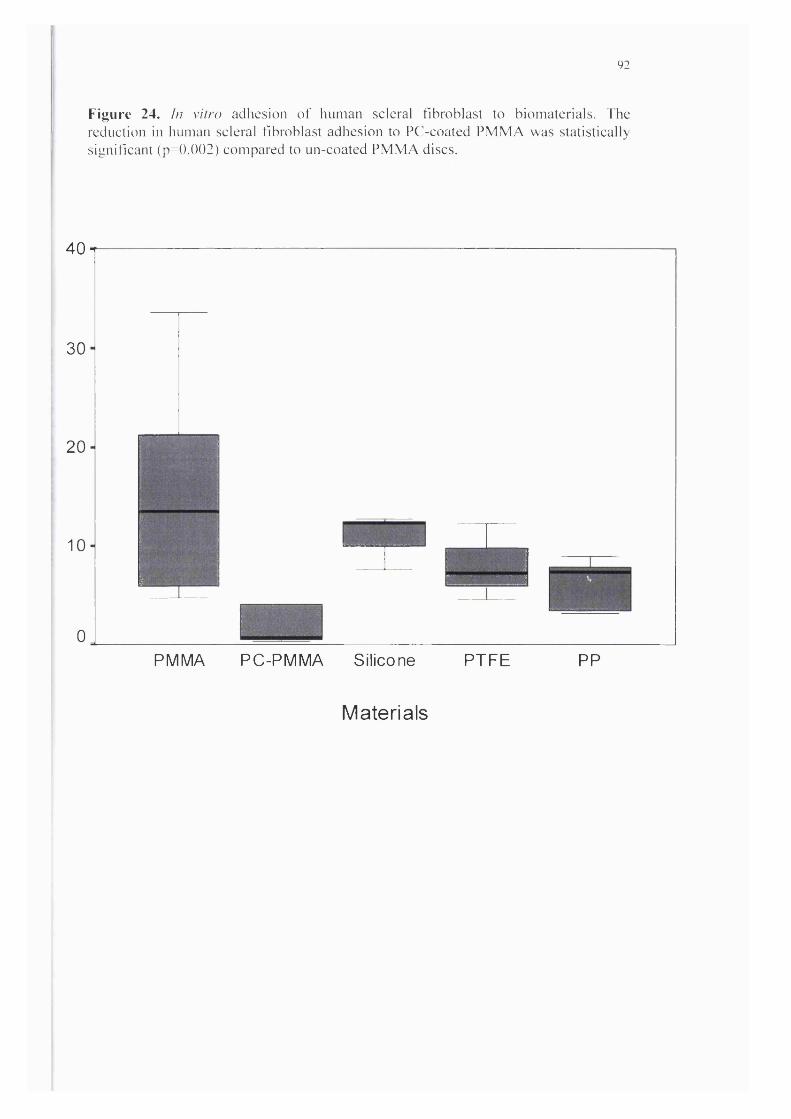
92
Figure 24. In vitro adhesion o f human scleral fibroblast to biomaterials. The reduction in human scleral fibroblast adhesion to PC-coated PM M A was statistically significant (p=0.002) compared to un-coated PMMA discs.
40
30
20
10
0
I_____
PMMA
‘i
PC-PMMA Silicone PTFE PP
M ateria ls

93
Figure 25. In vitro adhesion o f macrophage to biomaterials. The adhesion o f human macrophages was significantly reduced by PC coating o f PMMA (p=0.01 )
I 10
PMMA PC-PMMA Silicone PTFE
M ateria ls

94
Figure 26. Mean percentage damage to the bovine corneal endothelial monolayer culture alter standardised contact with different biomaterials. PC-PM M A discs had a level o f damage (p=0.04) significantly lower than that observed for uncoated PMMA.
01CQE
Q
OX)CQ
CQJUimQJ
a .
P M M A P C - P M M A Si l i cone PP
Materials
P T F E
95
Figure 27. Light microscopy photographs of typical damage to the bovine comeal endothelial monolayer culture after contact with PMMA and PC-coated PMMA. The red dashed line dividing the area A, which had stripped endothelial monolayer, from area B, which showed relatively intact endothelial monolayer. Scale bar = 10 pm.
PMMA PC-PM M A
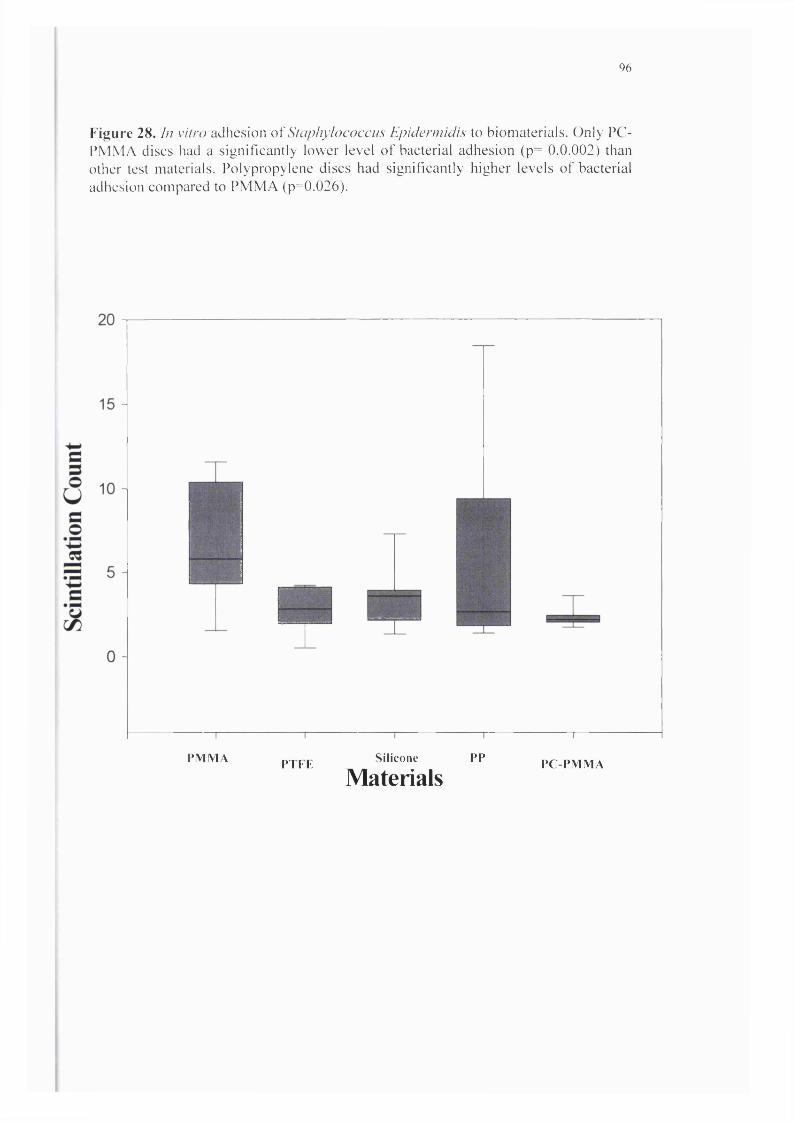
96
Figure 28. In vitro adhesion o\'Staphylococcus Epiderm idis to biomaterials. Only PC- PMMA discs had a significantly lower level o f bacterial adhesion (p= 0.0.002) than other test materials. Polypropylene discs had significantly higher levels of bacterial adhesion compared to PMMA (p=0.026).
P M M A P T F E Si l i cone PP
MaterialsP C - P M M A
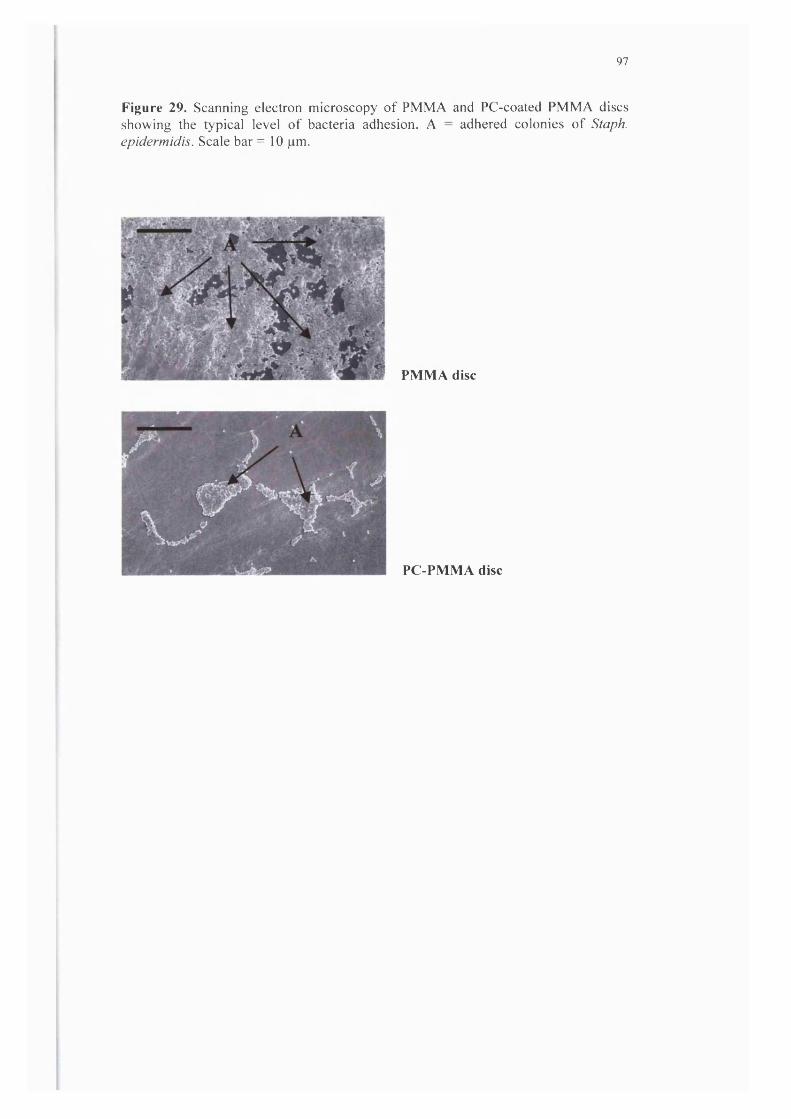
97
Figure 29. Scanning electron microscopy of PMMA and PC-coated PMMA discs showing the typical level of bacteria adhesion. A = adhered colonies of Staph, epidermidis. Scale bar = 10 pm.
PMMA disc
PC-PMMA disc

98
3.7 Discussion
3.7.1 Choice o f Test Biomaterials
PC coatings have been developed specifically to enhance biocompatibility for
materials used in fluid contacting applications. We chose PC-coated PMMA as a
candidate material for our novel GDD. Polypropylene and silicone are the most
common biomaterials used in the construction o f current GDDs (Table 4; Chapter 1;
Page 20). We also included PTFE, as it had been proposed as a potential biomaterial
for the construction o f GDDs (Helies 1997).
3.7.2 Cell & Protein Adhesion
Implanted polymeric materials quickly adsorb proteins from the surrounding fluid or
tissue environment. Adsorption occurs via a range o f bonding mechanisms, and
results in a biologically conditioned surface with modified interfacial properties. Cells
interact predominantly with this modified surface rather than the material surface
itself (Tang 1995). The biological adhesion characteristics o f a material are therefore
governed by its protein adsorption properties.
Fibrinogen adsorption may be o f particularly importance. In addition to its role as a
fibrin precursor, fibrinogen appears to be pivotal in establishing inflammatory
responses to implanted synthetic polymers (Tang 1993). Histological studies in
complement or immunoglobulin depleted mice have revealed inflammatory responses
similar to non-depleted controls (Tang 1993). In contrast, fibrinogen depleted mice

99
did not mount an inflammatory response unless the test material was pre-coated with
fibrinogen (Tang 1993). Fibrinogen is also thought to promote cell adhesion by
integrin binding to an RGD m otif similar to fibronectin (Collins 1987).
In our study, fibrinogen adhesion on PC-coated PMMA was approximately half that
seen for the other test materials. An indication o f the possible importance o f this
reduction in fibrinogen binding is given by the results o f the fibrin-binding assay in
which adhesion was virtually eliminated by the PC coating. Fibrinous occlusion is a
common complication with all forms o f GFS. In clinical series, 8 - 11% o f GDDs are
occluded by fibrin in the early postoperative period (Chapter 1). Partial occlusion or
significant fibrinous surface spoilation may be considerably more prevalent.
Partial occlusion is o f particular relevance to GDDs in which small bore filtration
channels are used as a resistance mechanism. From Poiseuille's formula, typical
diameters required to regulate flow effectively at physiological aqueous outflow rates
lie in the range 20-60pm for single tubes up to 6mm in length (Chapter 2). At these
diameters, small accretions o f biological debris could lead to relatively large
percentage changes in cross-sectional area and flow performance.
In these studies, the PC-coating also reduced cellular adhesion for both macrophages
and scleral fibroblasts significantly. Differences between PC-coated PMMA and other
test materials were less dramatic than those observed in the protein adhesion assays.
This relative reduction in effect may again be attributable to protein conditioning. Pre
coating with albumin passivates material surfaces (Kottke-Marchant 1989), reducing
subsequent adhesion o f other protein and cellular elements. Albumin in the culture
100
media used may have exerted a partial passivation effect in our assays reducing cell
adsorption to the un-coated materials. Differences between PC-coated and other test
materials were significant nonetheless.
Beyond surface spoliation, macrophage adhesion in particular is thought to be an
important initiator o f chronic inflammatory responses to implanted foreign material
(Tang 1995; Smetana 1997). Progressive fibrous encapsulation driven by a low-grade
foreign body inflammatory response limits the functional lifespan o f contemporary
GDDs (Table 5; Chapter 1; Page 27). The use o f materials which reduce fibroblast
and macrophage adhesion may significantly lengthen ODD filtration life.
The precise mechanism by which PC-polymers resist non-specific protein and cell
adhesion is not well understood. The natural cell wall phospholipid bilayer is self
assembling. Stability is achieved by sequestering hydrophobic lipid moieties to the
interior in an aqueous environment. PC polymers may mimic natural cell surfaces by
preferentially adsorbing a self-assembling phospholipid monolayer in the correct
configuration (Ishihara 1992). Alternatively, resistance to protein and cell adhesion
may be mediated by properties intrinsic to the PC molecule (Hayward 1984, Durrani
1986). Phosphorylcholine is zwitterionic, possessing both positive and negative
electrical charges in close proximity, but is overall electrically neutral. The
zwitterionic nature o f the PC head group attracts a large hydration shell, and it is
possible that this relatively large and stable surrounding barrier o f water molecules
mediates resistance to protein adhesion

101
3.7.3 Bovine Corneal Endothelial Damage
The amount o f endothelial damage caused by tube implantation, both at the time o f
operation and in association with subsequent micro-motion, probably varies with
physical force and the area o f contact. Where these factors are equal, as in our study,
the key determinant o f damage is the strength o f tissue to polymer adhesion. Comeal
endothelial cell damage caused by contact with silicone discs was less than that
caused by PM MA discs; but a PC polymer coating reduced endothelial damage to a
negligible level.
Standardised direct contact assays have previously used cadaveric animal corneas
(Kassar 1980, Barrett 1984, Mateo 1989). The use o f a cultured monolayer in this
assay has the advantage o f less inter-sample variation in association with pre-test
comeal condition and material to surface curvature mismatches. Although the strength
o f intercellular and cell to basement membrane adhesion in this culture model might
not perfectly mimic the conditions in-vivo, our findings for conventional materials are
consistent with those from previous studies in cadaver eyes (Kassar 1980, Barrett
1984, Mateo 1989).
Several factors are known to influence the strength o f cell adhesion to different
material surfaces. These include surface hydrophilicity (Ratner 1981), specific surface
chemistry (Moroudas 1973), surface rigidity (Yasuda 1978), and surface energy
(Kaufman 1977). Relatively hydrophobic surfaces such as PM MA were found to be
damaging to the endothelium in the nineteen seventies when the prevalence o f
pseudophakic bullous keratopathy began to increase (Knight 1979). Further in vitro

102
experimentation confirmed that hydrophilic surface modification o f PM M A or
substitution with more hydrophilic polymers could reduce endothelial damage in
standard touch tests (Barrett 1984, Mateo 1989, Balyeat 1989, Knight 1979).
Elastomeric silicone is also relatively hydrophobic, but has a lower surface free
energy than PMMA. Lower endothelial damage coefficients in both our own and
previous studies reflect this. Although less damaging than PMMA, the high rate o f
corneal endothelial failure after conventional tube implantation (Table 6; Chapter 1:
Page 29) suggests that the extent o f endothelial damage induced by contact with
silicone remains clinically significant.
PC polymers diminish contact induced comeal endothelial damage. This could help to
reduce the relatively high rate o f comeal endothelial failure associated with clinical
ODD implantation.
3.7.4 Bacterial Adhesion
The bacterial adhesion study demonstrated that modification o f PMMA discs with PC
polymer lead to a considerable reduction in the biomass o f adherent bacteria observed
in conditions o f standardised exposure to a clinical bacterial isolate. As with previous
studies (Raskin 1993, Dilly 1989), polypropylene showed a higher level o f bacterial
adhesion than the other test materials. An unusually high rate o f endophthalmitis has
been observed in association with intraocular lenses incorporating polypropylene
haptics (Bainbridge 1998).
Bacterial adhesion assays typically involve direct visualisation with scanning electron
or light microscopy (Raskin 1993, Dilly 1989), or radiolabelling o f bacteria (Raskin
103
1993). The bacterial biomass assay we used is objective, reproducible and devoid o f
radio hazard (Faragher 1996).
Many workers relate the adhesion o f bacteria to surfaces to the DLVO theory
(Derjaguin and Landau 1941, Verwey and Overbeek 1948) o f particle adhesion that
balances repulsive electrostatic interactions against attractive van der W aal’s
interactions between the surface and the organism (Garbassi 1998). Negatively
charged surfaces will have a tendency to repel bacteria which themselves possess a
negative charge (Dankert 1986). To some extent, this can be overcome by the ability
o f organisms to extend pili to provide an initial focal point o f attachment (Oga 1988).
In addition to charge, free surface energy and hydration may influence the ease o f
attachment. M aterials with a low surface energy, such as PTFE, are relatively inert
and resistant to attachment. Although most hydrogels have a relatively high free
surface energy, interfacial properties are modified by bound water (Tromp 1986). The
large hydration shell surrounding phosphorylcholine molecules in PC-PMMA may
explain the very low levels o f bacterial adhesion observed in this study.
PC-PMMA may diminish the risk o f endophthalmitis in ODD implantation.
3.8 Conclusion
Bioinert materials have been developed to improve the clinical performance o f
medical implants used in fluid contacting applications. To date, GDDs have been
constructed using conventional medical polymers. Our testing has demonstrated that a

104
highly promising new family o f bioinert polymers, PC polymers, out-perform these
conventional materials in each o f a panel o f in vitro assays designed to reflect
important dimensions o f biocompatibility in the context o f GDD implantation.
105
CHAPTER FOUR - Prototyping & In Vivo Study
Abstract
AIMS.
To assess the reproducibility o f the prototyping process for a novel glaucoma drainage
device (GDD) and the performance o f prototypes in vivo.
METHODS
Prototypes were machined from PMMA block, and micro drilling was carried out
using an excimer laser aiming to create a quasi-cylindrical flow resistance pathway
(average diameter 35 pm). The pressure drop across each prototype device was
measured on a custom flow rig, with the flow rate set at 2 pl/min. Prototype glaucoma
drainage devices, which produced the required pressure drop across the device (5-20
mmHg), were implanted in New Zealand White rabbits. lOPs were monitored using a
pressure transducer linked to the anterior chamber via a 27g cannula for 30 minutes
after the operation.
RESULTS
50 prototype GDDs were machined and laser drilled. All were coated with PC
polymers. 48 glaucoma drainage devices were rejected after the flow rig assessment.
The two remaining prototype GDDs were implanted without complications and
produced good flow control, with lOPs in the target range throughout the monitoring
period, and no evidence o f fibrinous occlusion.

106
CONCLUSIONS
Despite material homogeneity and controlled manufacturing conditions, laser drilling
for PMMA was insufficiently accurate over a 1mm depth to produce good flow
control in the majority o f prototype GDDs. Prototypes which passed preoperative
flow control tests also performed well in vivo, providing good protection from
hypotony. Alternative manufacturing techniques will be required to realise the clinical
potential for new GDDs.

107
4.1 Introduction
In vitro experimentation had shown that it was possible, in principle, to control the
dimensions o f a manufactured tubular lumen in a GDD accurately enough to provide
consistent protection from hypotony in the early period after GFS. Blank prototype
devices with a modified external profile also demonstrated good protection from
external leakage. Having demonstrated the promise o f PC polymers as bioinert
coatings for GDDs, we aimed to produce a batch o f prototype PC coated GDDs
incorporating a single channel flow restrictor and the novel external profile. We also
aimed to assess the correlation between pre-clinical flow testing and flow control after
implantation in an animal model.
Our original flow control experimentation (chapter 2) was based on ablation through
75pm thick polyimide sheets. At this thickness, a 15pm diameter ablation was found
to produce a flow pathway with the correct resistance characteristics, giving a
pressure drop across the device, which lay consistently within the desired target range
(5-15mmHg). A single macrophage could block GDDs in vivo if the flow pathway
were this narrow. Accordingly, a decision was taken to scale-up the diameter in
prototype construction, whilst maintaining flow resistance by lengthening the flow
pathway (Figure 7b; Chapter 2; Page 48). From the Poiseuille's formula, for a tube
with length o f 500 pm, a diameter o f 35pm should impart the correct flow resistance
at physiological aqueous production rates.

108
4.2 Materials & M ethods
4.2.1 Prototyping
Prototype GDDs were machined from PMMA (ICI, UK) by Pearson Matthews
Design Partnership (Kingston-on-Thames, UK) (Figure 13; Chapter 2: Page 57).
The GDDs were 4 mm in length with a tapering end and a Tune’ profile externally. A
large-bore hole (0.5 mm diameter) was drilled to within 0.5 mm o f the tapered end o f
the device. Excimer laser drilling was then carried out at Excitech Ltd (Oxford, UK)
to produce a small round hole with an average diameter o f 35 pm connecting the
leading end o f the device to the large-bore, zero resistance portion. Prototype GDDs
were then coated with a PC based polymer (Biocompatibles Ltd., UK) by immersion.
4.2.2 Flow Rig
The flow rig used was similar to that previously described for flow evaluation in
GDDs (Porter 1997; Prata 1995). The system consisted o f a pressure transducer
(Model P23ID, Gould Inc., California, USA), bridge amplifier (Model M LIIO, AD
Instruments, N ew South Wales, Australia) and recorder (Model ML200, AD
Instruments, New South Wales, Australia). Pressure changes were recorded using a
MacLab software (v3.5 AD Instruments, New South Wales, Australia) on a computer
(Performa 630, Apple Ltd., California, USA). A I ml hypodermic syringe (Fortuna,
Germany) was used with an adjustable electronic syringe pump (Model PHD 2000,
Harvard Apparatus, M assachusetts, USA) to control the flow rate. A three-way lock

109
was positioned between the water reservoir and the rest o f the system. Silicone tubing
(Silicone High Strength Tubing, Altec, Alton, UK) was used throughout. The free end
o f the tubing was sealed with silicone adhesive and left to dry. Once solidified, a
small slit incision was made through the sealed end with a standard M VR blade
(Visitech, UK) and prototype GDD implanted. No leakage around the GDD was
observed throughout the experiment. The transducer and the recording system were
calibrated using a water manometer daily prior to experimentation. Once the system
was filled with water, all gas bubbles were flushed out with the device submerged so
that flow through the device exit was not affected by surface tension generated at an
air interface (Figure 30). At this point, the three-way lock was turned to open the
system to atmospheric pressure and the pressure reading zeroed on the computer. The
three-way lock was then turned to obtain a closed system and infusion pump started.
The flow rate was set at 2 □ 1/minute. The pressure reading was allowed to stabilise
over 20 minutes, and the average reading from the final 10 minutes was then taken as
the pressure drop for the experiment. This recording was repeated six times for each
GDD. Devices producing a pressure drop o f 5-20mmHg were accepted for
implantation.
4.2.3 Animal model
Healthy adult New Zealand White rabbits were selected with weights between 2 and 3
kilograms. Baseline examinations were carried out and all eyes involved in the study
were normal. Throughout the experimentation, animals were cared for by experienced
animal handlers in accordance with the Helsinki Declaration and ARVO protocols for
the welfare o f experimental animals.

1 10
Figure 30. A schematic drawing of the How rig to test the prototype GDDs. The system consisted o f a pressure transducer (Model P23ID, Gould Inc., California. USA), bridge amplifier (Model M L llO . AD Instruments. New South Wales.Australia) and recorder (Model ML200. AD Instruments. New South Wales,Australia). Pressure changes were recorded using a MacLab software (v3.5 AD Instruments. New South Wales. Australia) on a computer (Performa 630. Apple Ltd., California. USA). A 1 ml hypodermic syringe (Fortuna. Germany) was used with an adjustable electronic syringe pump (Model PHD 2000, Harvard Apparatus,Massachusetts, USA) to control the flow rate. A three-way lock was positionedbetween the water reservoir and the rest o f the system. Silicone tubing (Silicone High Strength Tubing, Altec. Alton. UK) was used throughout. The free end o f the tubing was sealed with silicone adhesive and left to dry. Once solidified, a small slit incision was made through the sealed end with a standard MVR blade (Visitech. UK) and prototype GDD implanted.
W a t e r Rese rvo i r
T h re e -w ay Lock
Ma}>nifled View o f tube end
e on Infusion p u m p
Pres su reT r a n s d u c e r
G D D im p la n t ed at the sealed end
C om puter

I l l
4.2.4 Study Design
This was a prospective, internal, unmasked, efficacy study. Two rabbits were
implanted with GDDs shown to produce a cross-device pressure drop in the target
range (5-15mmHg) in preoperative testing. Each rabbit was implanted with the GDD
in one eye only under general anaesthesia. Implants were flushed with Balanced Salt
Solution (BSS). lOP was monitored continuously using a pressure transducer for 30
minutes after the operation with anterior chamber (AC) infused (F igure 31). The
rabbits were examined and assessed for TOP, AC depth/inflammation and bleb
morphology daily in the first week and then twice weekly for the next five weeks. On
day 42, the rabbits were sacrificed.
4.2.5 General Anaesthesia
The rabbit was held firmly by the shoulders and intramuscular ketamine (50 mg/Kg)
and xylazine (10 mg/Kg) given intramuscularly into the most muscular part o f the
thigh. A 5ml syringe was used with a disposable 23 gauge needle for the injection.
The anaesthetic was allowed to take effect and further procedures were carried out
when the rabbits were fully anaesthetised.

112
Figure 31. A schematic drawing o f the intraocular pressure monitoring set-up. The 27 gauge needle primed with balance salt solution was inserted into the anterior chamber and connected to a pressure transducer and computer to record the real time intraocular pressure changes.
W ater Reservoir O peratingM icroscope
Three-w ay Lock
27g needle inserted into AC
D
PressureTransducer
Computer
BP Am plifier
PowerLab 200

113
4.2.6 Implantation of Prototype Glaucoma Drainage Device
The anaesthetised rabbits were placed under the operating microscope with the
eyelids held open with a speculum. A fine 7/0 silk traction suture was placed through
the superficial limbal tissues to pull the eye down. A 27 gauge butterfly needle (filled
with BSS) connected to a digital pressure transducer was used to monitor the lOP
changes (Figure 31). The 27 gauge needle was carefully introduced through a comeal
stab incision parallel to and well anterior to iris plane. A fomix based conjunctival
flap was fashioned, and a selerocorneal slit incision was made parallel to the iris
plane using a standard 1.19mm width mierovitreoretinal (MVR) blade to enter the
anterior chamber. The GDD was inserted through the wound, and sutured with 10/0
nylon (Figures 32-33). The conjunctiva was sutured with 10/0 vicryl. A sub
conjunctival injection o f betnesol and cefuroxime was administered at the end o f the
procedure. lOP was monitored continuously for over 30 minutes before the removal
o f the 27-gauge needle from the anterior chamber and conjunctival closure.

1 14
Figure 32. A schematic drawing o f the glaucoma drainage deviee in-si In. Fornix based conjunctival flap was fashioned, and a selerocorneal slit incision was made parallel to the iris plane using a standard 1.19mm width mierovitreoretinal (MVR) blade to enter the anterior chamber. The glaucoma drainage device was inserted through the wound, and sutured with 10/0 nylon, dhe conjunctiva was sutured with 10/0 vicrvl.
Conjunctiva
Cornea
Sclera
Pro to ty p e g l a uc om a d ra i n a g e device

15
Figure 33. Prototype glaucoma drainage device in situ. Week 2 post operation. The tip of the device (A) is just visible in the anterior chamber. The external part of the device (B) is sutured with 10.0 nylon and covered by conjunctiva.

] 16
4.2.7 Follow-up Examination
Eyes were examined under topical anaesthesia using a portable slit-lamp. The anterior
chamber depth, the degree o f inflammation and the bleb morphology were graded and
recorded. Eyes were then photographed with a standard 35mm camera. lOP was
measured using a Tonopen. Examinations were repeated daily for the first week, and
twice weekly for the next 5 weeks to monitor for the following adverse events; AC
fibrinous reaction, systemic illness, com eal abrasion, corneal oedema, hypopyon and
device extrusion.
117
4.2.8 Sacrifice
Animals were sacrificed using a lethal intravenous injection o f phenobarbitone under
general anaesthesia.
4.3 Results
4.3.1 Pre-operative flow testing
O f the 50 prototype GDDs that were machined, laser drilled and coated with PC
polymers, only 2 prototype GDDs fulfilled the pressure drop requirements after flow
rig assessment.
4.3.2 Adverse Reactions
The anterior chamber remained well formed through out the study period, and no
fibrinous reaction was observed in the anterior chamber. No systemic adverse reaction
was observed at any stage post implantation.
4.3.3 Intraocular Pressure
Rabbit 1
The implanted GDD had a cross-device pressure drop measured at 19 mmHg, at a
flow rate o f 2 □ 1/minute and the baseline IGF in the right and left eye were 19 mmHg

118
and 21 mmHg respectively. For the fist 30 minutes after implantation, the implanted
eye’s TOP maintained a pressure o f between 19 mmHg and 21 mmHg. Controlled
fluid escape through the GDD was visible throughout the monitoring period. There
was no anterior chamber shallowing, or evidence o f external leakage. The tonometric
10? of both eyes during the period o f the study is shown in Figure 34. The lO P’s in
the operated eye were lower than the control eye in most measurement until the third
week and no bleb was visible after day 8 (the error o f lOP measurement in rabbits
using Tonopen is ± 3 mmHg).
Figure 34. The intraocular pressures o f both eyes o f rabbit 1 during the study.
lO P in m m H g
22
20
18 -
16
14
12
Control Eye GDD Eye
10 20 30 40
Post-O perative D ay
50

119
Rabbit 2
The implanted GDD has a pressure gradient o f 6 mmHg at a flow rate o f 2 □ 1/minute
and the baseline lOP in the right and left eyes were 21 mmHg and 20 mmHg
respectively. For the first 30 minutes after implantation, I OP was maintained at 17-18
mmHg. Again, controlled flow was visible through the GDD, and no anterior chamber
shallowing was observed. The lOP o f both eyes during the follow up period is shown
in Figure 35. The lO P’s in the operated eye were lower than the control eye in most
measurement until the second week and no bleb was visible after day 8.
Figure 35. The intraocular pressures o f both eyes o f rabbit 2 during the study.
lO P in m m H g
28
22
Control Eye GDD Eye
10 20 30 40 50
Post-O perative D ay
120
4.4 Discussion
Using current machining and the excimer laser techniques, critical dimensional
control was too poor to provide a reproducible internal flow resistance in the desired
target range (5-20mmHg for this phase o f the study). In contrast to earlier studies
(chapter 2) in which excimer laser ablation o f 75 pm thickness polyimide sheeting was
found to produce a high level o f dimensional reproducibility, and flow control within
a finer target range (5-15mmHg); we had selected a longer (500pm), larger-bore
(35 pm) resistance channel for this set o f prototypes, and chosen PMMA as a
manufacturing material. The choice o f PMMA was based on ease o f PC-polymer
coating, and a long track record o f safety for this material in the eye. As explained
above, a larger-bore resistance channel was felt to be necessary in vivo to minimise
the chances o f blockage with a single cell or pre-formed accretions o f biological
debris. Both the change in material and the change in dimensions may have
contributed to the inaccuracy o f ablation. Polyimide is superior to PM MA as an
ablation substrate, and the high aspect ratio o f the longer resistance channel would
tend to lead to variable masking effects caused by inadequate exhaust o f ablation
products between pulses.
Although the poor yield from prototyping only afforded a very preliminary view o f
the clinical potential for the new GDDs, the devices that were implanted performed
well. The tapered front section facilitated implantation with minimal tissue
manipulation, and implantation for the lune-shaped prototypes through a slit incision
was a simple process compared to that for existing GDDs. Selected prototype GDDs

121
good flow control with no hypotony or shallowing o f the anterior chamber. PC-
coating o f PMMA has no notable adverse systemic or local reaction in rabbits.
Notably for the rabbit model, there was no evidence o f fibrinous occlusion, or any rise
in lOP, which might suggest partial occlusion during the immediate post implantation
observation phase.
4.5 Conclusion
Although these studies fall some way short o f securing proof o f principle for the
design concepts developed in vitro, they do provide a tantalising glimpse o f the
possibilities for a new generation o f GDDs in vivo. Further exploration o f micro
manufacturing techniques required to produce the requisite level o f critical
dimensional control will be necessary before this potential can be realised in clinical
trials.

122
CHAPTER FIVE- Concluding Discussion & Future Development
5.1 Discussion
The premises underpinning the rationale for using a novel GDD in GFS are: first, that
consistent internal flow control and elimination o f external leakage will prevent early
post-operative hypotony; and second, that using a bioinert coating will minimise
modification o f internal flow resistance by biological spoliation, and minimise any
foreign body inflammatory reaction.
Experimental flow studies described in preceding chapters demonstrate that
Poiseuille’s law will accurately predict the critical dimensions for a GDD flow
restrictor based on a small bore tube. They also demonstrated that improving fit
between the external profile o f a new GDD and the incision through which it is
inserted should facilitate implantation and eliminate uncontrolled external leakage.
Our in vitro assays, designed to reflect a number o f key dimensions o f
biocompatibility in GDD implantation, suggesting that new generation bioinert
materials should improve clinical performance. Further information could be obtained
from sub-conjunctival implantation studies o f material biocompatibility and dynamic
flow performance in conditions reflecting the aqueous environment after blood
aqueous barrier breakdown using various concentrations o f serum in the flow rig.
Although limited, our initial observations o f flow performance in vivo were highly
encouraging. There were no adverse tissue reactions post-operatively. Overall, work
contained in this thesis demonstrates proof o f principle for a number o f important new
design departures in GDD development.
With current laser drilling techniques, dimensional control is too poor to make bulk
manufacture o f GDDs, or even prototype manufacture for further trials, viable. The
challenge now is to identify a more reliable means o f critical dimensional control.

123
5.2 Future Development
5.2.1 Extrusion M oulding and Hot Drawing
Extrusion is a process that can be compared to squeezing toothpaste out o f a tube.
Polymer granules are forced through a heated barrel and the fused polymer is then
squeezed through a die, which defines the profile o f the extruded component. Water
or air-cools the extruded material as it leaves the die, and is cut to the required length.
Disadvantages are that the cost o f producing a die is high and the process is limited to
shapes with a uniform cross-section. This would limit design flexibility for a new
device.
Hot drawing is similar to extrusion, but involves heating a thermoplastic polymer or
glass to its glass transition temperature, then exploiting the consistency o f length to
diameter ratios produced by stretching a heated tubular element under constant
tension. This is the process by which glass micropipettes in routine laboratory use are
fabricated. Hot drawing is also limited to a uniform cross-section; but is relatively
cheap to explore, and could be a viable route to producing a limited prototype run.
5.2.2 Photolithography
Photolithography is a relatively new micromanufacturing technique in which
polymers are exposed to selectively to light energy in order to define a three
dimensional shape. Selective exposure is either through a mask to produce a uniform
cross-sectional shape, or by scanning a focussed point o f light through the target
polymer, or “photoresist,” to produce non-uniform cross-sections. Light energy

124
defines shapes within the resist either by curing the polymer (positive photoresists) or
ablating it (negative photoresists) at the point o f exposure. Shorter wavelength light
defines shapes most accurately, and X-ray lithography is capable o f producing
complex shapes with submicron accuracy. These accurate solid representations o f
designs on a micron scale can be used either to create prototype devices individually,
or to create micro-moulds for scale up to bulk manufacture.
5.3 Conclusion
The health economic arguments for developing a fast, reliable, one-stop treatment
glaucoma are clear, particularly in the developing world, where access to regular
review and drug treatment is likely to remain limited. Laser drilling has not been
accurate enough to realise the goal o f producing a biocompatible GDD to improve
flow control and reduce operating time in routine GFS. Emerging techniques for
micro-manufacture such as X-ray lithography hold immense promise in this field.
Possibilities for fusing these techniques with improvements in material
biocompatibility and advances in the pharmacological control o f wound healing
suggest a bright future for GDDs in the new century.

125
R eferences
Addicks EM, Quigley HA, Green WR, Robin AL. Histologic characteristics o f filtering blebs in glaucomatous eyes. Arch Ophthalmol 1983; 101: 795-798
Allan B. Closer to nature: new biomaterials and tissue engineering in ophthalmology. Br J Ophthalmol. 1999 N ov;83(l 1): 1235-40.
Allan BDS, van Saarloos PP, Cooper RL, Constable IJ. Excimer laser sclerostomy in pseudophakic patients with advanced open angle glaucoma. Br J Ophthalmol 1994;78: 199-205.
Allan BDS, van Saarloos PP, Vijayasekaran S, Cooper RL, Constable IJ. Excimer laser sclerostomy: tissue damage and dimensional reproducibility in vitro. Lasers and Light in Ophthalmology 1993; 5: 121-130.
Amon M; Menapace R; Radax U; Frey 1er H. In vivo study o f cell reactions on poly(methyl methacrylate) intraocular lenses with different surface properties. J Cataract Refract Surg, 1996, 22 Suppl 1:825-9
Ayyala RS, Michelini-Norris B, Flores A, Haller E, Margo CE. Comparason o f different biomaterials for glaucoma drainage devices: Part 2. Arch Ophthalmology 2000; 118(8): 1081-4
Baerveldt G, Chou JS, Longren B. Comparison o f the Baerveldt glaucoma implant with bioseal to the Baerveldt implant in rabbits. Invest Ophthalmol Vis Sci 1997; 38: 52
Bainbridge JW, Teimory M, Tabindeh H, Kirwan JF, Dalton R, Reid F, Rostron CK. Intraocular lens implants and risk o f endophthalmitis. British Journal o f Ophthalmology 1998; 32: 1-4
Barrett G, Constable IJ. Comeal endothelial loss with new intraocular lenes. A J Ophthalmol 1984;98:157-165
Barrett GD; Beasley H; Lorenzetti OJ; Rosenthal A. M ulticenter trial o f an intraocular hydrogel lens implant. J Cataract Refract Surg, 1987 Nov, 13:6, 621-6
Batchelor GK. An introduction to fluid dynamics. 2000. Cambriege University Press
Bayleat HD, Nordquist RE, Lemer MP, Gupta A. Comparison o f endothelial damage produced by control and surface moditfied poly(methyl methacrylate) intraocular lenses. J Cataract Refract Surg 1989; 15: 491-494
Beebe WE, Starita RJ, Fellman RL, Lynn JR, et al. The use o f Molteno implant and anterior chamber tube to encircling band for the treatment o f glaucoma in keratoplasty patients. Ophthalmology 1990;97:1414
126
Bick MW. Use o f tantalum for ocular drainage. Arch Ophth 1949; 42: 373-388
Bietti GB. The present state o f the use o f plastics in eye surgery. Acta Ophth. 1955; 33: 337-370.
Block MDW, Greve EL, Dunnebier EA. Scleral flap sutures and the development o f flat or shallow anterior chambers after trabeculectomy. Invest Ophth Vis Sci 1992; 33 (Suppl): 2898
Blondeau P, Phelps CD. Trabeculectomy vs thermosclerostomy: a randomized prospective trial. Arch Ophthalmol 1981; 99: 810-816
Britt MT, LaBree LD, Lloyd MA, Minckler DS, Heuer DK, Baerveldt G and Varma R. Randomized clinical trial o f the 350 mm^ versus 500 mm^ Baerveldt implant: longer term result: is bigger better? Ophthalmology 1999; 106(12): 2312-8
Broadway-DC; Grierson-I; O'Brien-C; Hitchings-RA. Adverse effects o f topical antiglaucoma medication. II. The outcome o f filtration surgery. Arch-Ophthalmol. 1994 Nov; 112(11): 1446-54
Brubaker RF. Flow o f aqueous-humor in humans. The Friedenwald Lecture. Investigative Ophthalmology & Visual 1991;32(13):3145-3166
Cairns JE. Trabeculectomy. Preliminary report o f a new methods. Am J Ophthalmol 1968;66:673-679
Cantor L, Burgoyne J, Sanders S, Bhavnani V, Hoop J, Brizendine E. The effect o f mitomycin C on M olteno implant surgery: a 1 -year randomized, masked, prospective study. J Glaucoma 1998 Aug;7(4):240-6
Cao W, Hench LL. Bioactive materials. Ceramics Int 1996; 22: 493-507
Cavazzani A. A. farm acol. Sperim., iv, 401, 1905 ; viii, 262, 1909
Cheung JC, Wright MW , Murali S, Pederson JE. Intermediate-term outcome o f variable dose mitomycin c filtering surgery. Ophthalmology 1997; 104: 143-149
Coleman AL, Hill R, W ilson MR, Choplin N, Kotasneumann R, Tam M, Bacharach J, Panek WC. Initial Clinical experience with the Ahmed Glaucoma Valve Implant. Am J Ophthalmol 1995; 120: 23-31
Coleman AL, Mondino BJ, et al. Clinical Experience with the Ahmed Glaucoma Valve Implant in Eyes with prior or concurrent Penetrating keratoplasties. Am J Ophthalmol. 1997; 123(1): 54-61
Coleman AL, Smyth RJ, W ilson MR, Tam M. Initial Clinical Experience with the Ahmed Glaucoma Valve Implant in Paediatrics Patients. Arch Ophthalmol. 1997;115:186-191

127
Collaborative normal tension glaucoma study group. The effectiveness o f intraocular pressure reduction in the treatment o f normal tension glaucoma Am J Ophthalmol 1998;126:498-505
Collins WE, Mosher DF, Tomasini BR, Cooper SL. A preliminary comparison o f thrombogenic activity o f vitronectin and other RGD-containing proteins when bound to surfaces. In: Leonard EF, Turitto VT, Vroman L, eds. Blood in contact with natural and artificial surfaces. Ann. N.K. Acad. Sci. 1987;516:291-299.
Costa VP, Smith M, Spaeth GL, Gandham S, Markovitz B. Loss o f visual acuity after trabeculectomy. Ophthalmology 1993; 100: 599-612.
D ’Hermies F; Korobelnik JF; Caputo G; M ashhour B; Chauvaud D; Pouliquen Y; Renard G. Encapsulation o f scleral buckling materials. A study o f sixty specimens. Ophthalmology, 1998 Jun, 105:6, 1079-86
Dankert J, Hogt AH, Feijen J. Biomedical polymers: Bacterial adhesion, colonization, and infection. CRC Cri Rev Biocompat. 1986; 2: 219-301
Derjaguin BY and Landau LD. Theory o f the stability o f strongly charged lyophobic sols and o f the adhesion o f strongly charged particles in solutions o f electrolytes. Acta Physic Chimica USSR. 1941 ; 14: 633 -62
Dilly PN, Holmes-Sellors PJ. Bacterial adhesion to intraocular lenses. J Cataract 1989;15:317-320
Drance SM. Glaucoma-changing concepts. Eye 1992; 6: 337-345
Durrani AA, Hayward JA, Chapman D. Biomembranes as models for polymer surfaces. Biomaterials 1986;7:121-125.
Egbert PR, Liebert MF. Internal suture occlusion o f the Molteno glaucoma implant for the prevention o f post operative hypotony. Ophthalmic Surg 1989; 20: 53-56
Eisenberg DL, Koo EY, Hafner G, Schuman JS In vitro flow properties o f glaucoma im^XeinX &Qv\cQS.Ophthalmic Surg Lasers 1999 Sep-Oct;30(8):662-7
Ellis RA. Reduction o f intraocular pressure using plastics in surgery. Am J Ophthalmol I960; 68: 879-883
El Sayyad F, Helal M, El Kholify H, Khalil M, El-Maghraby A. Nonpenetrating deep sclerectomy versus trabeculectomy in bilateral primary open-angle glaucoma. Ophthalmology 2000; 107:1671 -1674
Fellenbaum PS, Almeida AR, M inckler DS, Sidoti PA, Baerveldt G, Heuer DK. Krupin disk implantation for complicated glaucoma. Ophthalmology 1994; 101(7): 1178-1182

128
Fluorouracil filtering surgery study group. One year follow-up. Am J Ophthalmol 1989; 108:625-635
Francis BA, Cortes A, Chen J, Alvarado JA. Characteristics o f glaucoma drainage implants during dynamic and steady-state flow conditions. Ophthalmology 1998;105:1708-1714
Freeman J. Clinical experience with the Molteno dual chamber single plate implant. Ophthalmic Surg 1992; 23: 238-241
Gandolfl S.A. Cimino L. Deep sclerectomy without absorbable implants and with unsutured scleral flap: Prospective, randomised 2-year clinical trial vs trabeculectomy with releasable sutures. Inves Ophthalmol Vis Sci Suppl 2000; 436
Garbassi F, Morra M, Occhiello E eds. Polymer surfaces: From physics to technology. Willey 1998
Gibson G. Transcleral lacrimal canaliculus transplants. Tr Am Ophth Soc. 1942; 40: 499-515
Glovinsky Y, Belkin M. Evaluation o f the “G -Planf ’ glaucoma shunt in rabbit eyes. Invest Ophthalmol Vis Sci 1997: 38;53
Grant W M, Burke JF. Why do some people go blind from glaucoma? Ophthalmology 1982;89:991-998
Gressel MG, Parrish RK, Heuer DK. Delayed non-expulsive suprachoroidal ]\2iQmorxl\dig&. Arch Ophthalmol 1984; 102: 1257-1761
Greve EL, Drake CL. Four year follow-up o f glaucoma operation. Int Ophthalmol
1979;1:139-145
Grey RHB, Bums-Cox CJ, Hughes A. Blind and partially sight registration in Avon. Br J Ophthalmol 1989; 73: 88-94
Gristina AG & Naylor PT. Implant-associated infection. In; Ratner BD, Hoffman AS, Schoen FJ, Lemons JF, eds. Biomaterials science. San Diego:Academic Press, 1996;4:205-214
Gristina AG. Biomaterial-centred infection:microbial adhesion versus tissue integration. Science 1987;237:1588-95
Hall B, Bird R, Kojima M, Chapman D. Biomembranes as models for polymer surfaces. Biomaterials 1989; 10: 219-224
129
Hart WM. The epidemiology o f primary open angle glaueoma. In Ritch R, Shields MB, Krupin T eds. The glaucomas, St Louis: CV Mosby 1989: 789-798.
Hayward JA, Chapman D. Biomembrane surfaces as models for polymer design: the potential for haemoeompatibility. Biomatehals\9% A\A\l3S-\A2.
Helies P, Savoldelli M, Legeais JM, Parel JM, Renard GJ. Artificial MESHW ORK (MESH). Clinical and histological study in the rabbit with a six months follow up. Invest Ophthalmol Vis Sci 1997: 38; 1246
Heuer DK, Lloyd MA, Abrams DA, Baerveldt G, M inckler DS, Lee MB, et al. W hich is better? One or two? A randomized clinical trial o f Single plate versus Double plate Molteno Implantation for glaucomas in Aphakia and pseudophakia. Ophthalmology 1992; 99(10): 1512-1519
Hitchings-RA. Low tension glaucoma—its place in modem glaueoma practice. Br-J- Ophthalmol. 1992 Aug; 76(8): 494-6
Honrubia EM, Grijalbo MP, Gomez ML, Lopez A. Surgical treatment o f neovascular glaucoma. Trans Ophthalmol Soc UK 1979; 99: 89-91.
Hunter S, Angelini GD. Phosphatidylcholine-coated chest tubes improve drainage after open heart operation. The Society o f Thoracic Surgeons. 1993; 1329-1342.
Ikada Y. Surface modification o f polymers for medical applications . Biomaterials 1994; 15(10): 725-736
Ishihara K, Ziats NP, Tierney BP, et al. Protein adsorption from human plasm a is reduced on phospholipid polymers. J Biomed Mater Res 1991; 25: 1397-1407
Iwach AG, Hoskins HD Jr, M ora JS, Dickens CJ, Drake MV, Gaffney MM, Nguyen N, Wong PC, Tran H, Ma AS. Update on the subconjunctival THC:YAG (holmium) laser sclerostomy Ab extemo clinical trial: a 4-year report. Ophthalmic Surg Lasers 1996 Oct;27(10):823-31
Jacob-labarre JT, McKinnon SJ, Tanji T. Biocompatibility response to modified Baerveldt glaucoma drains. Invest Ophthalmol Vis Sci 1996; 37 (Suppl): 1164
Jampel HD, Leong KW, Dunkelburger GR, Quigley HA. Glaucoma filtration surgery in monkeys using 5-fluorouridine in polyanhydride disks. Arch Ophthalmol 1990; 108: 430-435
Jay JL, Allan D. The benefit o f early trabeculectomy versus conventional management in primary open angle glaucoma relative to the severity o f the disease.
1989; 3: 528-535
Jay JL. Rational choice o f therapy in primary open angle glaucom. Eye 1992; 6: 243- 247

130
Joo CK, Kim JH. Compatibility o f intraocular lenses with blood and connective tissue cells measured by cellular deposition and inflammatory response in vitro. J Cataract Refract Surg. 1992 May; 18(3):240-6
Joseph JP, Grierson I, Hitchings RA. Partial charaeterization o f the fibroblast chemotaetie eonstituents o f human aqueous humour. Int Ophthalmol 1989; 13: 125- 130
Joseph NJ, Sherwood MB, Trantas G, Hitchings RA. A one piece drainage system for glaueoma surgery. Trans Ophthalmol Soc UK 1986; 105: 657-664.
Karlen ME, Sanehez E, Schnyder CC, Sickenberg M, Mermoud A. Deep sclerectomy with collegen implant: medium term results. Br J Ophthalmol 1999;83:6-11
Kassar BS, Vam ell ED. Effects o f PMMA and silicone lens materials on normal rabbit comeal endothelium: An in vitro study. Am Intra-Ocular Implant Soc J 1980;6: 344
Katz GJ, Higginbotham EJ, Liehter PR, Skuta GL, Museh DC, Bergstrom TJ,Johnson AT. Mitomycin C versus 5-fluorouracil in high-risk glaucoma filtering surgery. Extended follow-up. Ophthalmology 1995 Sep; 102(9): 1263-9
Kaufman HE, Katz J, Valenti J, Sheets JW, Goldberg EP.Corneal endothelium damage with intraocular lenses: contact adhesion between surgical materials and tissue. Science. 1977 Nov 4; 198(4316):525-7
Kee C, Youn DH. Experimental designed glaucoma implant surgery with mitomyein- C in rabbits. Korean Journal o f Ophthalmology 1995; 9(2): 89-95.
Khaw PT, Tsai JC, Constable PH, Cordeiro F, Oeeleston NL. Preventing searring after glaueoma filtration surgery with single applieation agents: A praetical approaeh. Asia-Pacific Journal o f Ophthalmology 1995;&(1); 6-13
Kidd MN, O ’Connor M. Progression o f field loss after trabeeulectomy: a five year follow-up. Br J Ophthalmol 1985; 69: 827-831.
Kim DD, Menmen JE. Spontaneous disengagement o f the OptiMed implant. Arch Ophthalmol 1996: 114(11); 1420-1421
Kim SW. nonthrombogenic treatments and startegies. In; Ratner BD, Hoffman AS, Schoen FJ, Lemons JF, eds. Biomaterials science. San Diego:Academie Press, 1996;22:493-507
Knight-PM; Link-WJ. Surface modifieation o f intraocular lenses to reduce comeal endothelial damage. J-Am-Intraoeul-Implant-Soe. 1979 Apr; 5(2): 123-30
Knzler, J.F. & MeGee, J.A. Contaet Lens Materials. In: Juniper, R. & Reid, P. eds. Chemistry & Industry Biomedical Materials. London, Elsevier, 1994;16:651-655.

131
Kochounian HH; Maxwell WA; Gupta A. Complement activation by surface modified poly(methyl methacrylate) intraocular lenses. J Cataract Refract Surg, 1991 Mar, 17:2, 139-42
Kojima M, Ishihara K, Watanabe A, Nakabayashi N. Interaction between phospholipids and biocompatible polymers containing a phosohorylcholine moiety. Biomaterials 1991;12:121-124.
KolkerAE. Visual prognosis in advanced glaucoma. A comparison o f medical and surgical therapy for retention o f vision in 101 eyes with advanced glaucoma. Trans Am Ophthalmol Soc 1977;75:539-555
Kottke-M archant K, Anderson JM, Umemura Y, Marchant. Effect o f albumin coating on the in vitro blood compatibility o f Dacron arterial prosteses. Biomaterials 1989;10:147-150.
Krawczyk CH. Glaueoma drainage devices and the FDA. Ophthalmology 1995; 102(11): 1581-2
Krupin Eye Valve Filtering Surgery Study Group. Krupin Eye Valve with Disk for Filtration Surgery. Ophthalmology 1994; 101(4): 651-658
Krupin T, Podos SM, Becker B, Newkirk JB. Valve implants in filtering surgery. A preliminary report. Am J Ophthalmol 1976; 81: 232-235
La Rocca V. Internat Cong Ophth. (Brussels) 1958.
Larsson R, Selen G, Bjordklund H, Fagerholm P. Intraocular PM MA lenses modified with surfaee-immobilised heparin: evaluation o f bioeompatibility in vitro and in vivo. Biomaterials. 1989; 10(8):511 -6
Latina MA, Melamed S, March WF, Kass MA, Kolker AE. Gonioscopic ab intemo laser sclerostomy. A pilot study in glaucoma patients. Ophthalmology 1992 N ov ;99(ll): 1736-44
Lavin MJ, W ormold RPL, Migdal CS, Hitchings RA. The influence o f prior therapy on the success o f trabeculectomy. Arch Ophthalmol 1990; 108: 1543-1548
Lawin-Brussel CA, Refojo MF, Kenyon KR. In vitro adhesion o f Pseudomonas aeruginosa and Staphhylococcus aureus to surface passivated poly(methhyl methacrylate) intraocular lenses. J Cataract Refract Surg, 1992;18:598-601
Lee D, Shin DH, Birt CM, Kim C, Kupin TH, Olivier MM, Khatana AK, Reed SY. The effect o f adjunctive mitomycin C in Molteno implant surgery. Ophthalmology 1997 Dec;104(12):2126-35
Lee P-F, W ong W-T: Aqueous-venous shunt for glaucoma: Report on 15 cases. Ann Ophthalmol 1974; 6: 1083-1088.

132
Lee VW. Glaucoma “valves” - truth versus myth. Ophthalmology 1998;105(4);567-8.
Liebmann JM, Sokol J, Ritch R. Management o f chronic hypotony after glaucoma filtration surgery. J Glaucoma 1996; 5: 210-220
Lim KS, Allan B, Muir A, Lloyd AW, Khaw PT. Glaucoma filtration implants. Past, present and future. British Journal o f Ophthalmology 1998;82(9): 1083-1089
Lloyd MA, Baerveldt G, Fellenbaum PS, Sidoti PA, M inckler DS, Martone JF, et al. Intermediate-term Results o f a Randomized Clinical Trial o f the 350 versus the 500
mm^ Baerveldt Implant. Ophthalmology 1994; 101(8): 1456-1463
Lloyd MA, Baerveldt G, Heuer DK, M artone JF, M inckler DS, Zhau JL, Nguyen QH. The Baerveldt glaucoma implant- long-term histologic studies in rabbits and clinical experience in humans. Investigative Ophthalmology & Visual Science 1991: 32(4); 746-746 (Meeting Abstract)
Lloyd MA, Sedlak T, Heuer DK, M inckler DS, Baerveldt G, Lee MB. Clinical experience with the single plate Molteno implant in complicated glaucomas: update o f a pilot study. Ophthalmology 1992; 99: 679-687
Losche W. Vorschlage zur Verbesserung der Zyklodialyse. Klin Monatsbl f Augenh. 1952; 121:715-716
M ajima K. An evaluation o f the biocompatibility o f intraocular lenses. Ophthalmic Surg Lasers, 1996 Nov, 27:11, 946-51
Mao LK, Stewart WC, Shields MB. Correlation between intraocular pressure control and progressive glaucomatous damage in primary open angle glaucoma. Am J Ophthalmol 1991 ; 111: 51 -60
Mascati NT. A new surgical approach for the control o f a class o f glaucomas. Int Surg 1967; 47: 10-15
Mateo NB, Ratner BD. Relating the surface properties o f intraocular lens materials to endothelial cell adhesion damage. Invest Ophthalmol & Vis Scienc 1989;30(5): 853- 860
Maumenee AE. Causes o f optic nerve damage in glaucoma. Ophthalmology 1983; 90: 741-757
McDonnell PJ, Robin JB, Schanzlin DJ, et al. Molteno implant for control o f glaucoma in eyes after penetrating keratoplasty. Ophthalmology 1988;95: 364
McEwen WK. Application o f Poiseuille’s law to aqueous outflow. Archives o f Ophthalmology 1958;60:290-294
133
Melamed S, David R. Ongoing clinical assessment o f the safety profile and efficacy o f brimonidine compared with timolol: year-three results. Brimonidine Study Group II. Clin Ther 2000 Jan;22(I):103-l 1
Melamed S. M olteno implant surgery in refractory glaucoma. Surv o f Ophthalmol 1990;34: 441-448
Membrey WL, Poinoosawmy DP, Bunce C, Fitzke FW, Hitchings RA. The effect o f intraocular pressure reduction on the risk o f visual field progression in normal pressure glaucoma patients following trabeculectomy. Inves Ophthalmol Vis Sci Suppl 2000;2981
Mermoud A, Salmon JF, Alexander P, Straker C, Murray AND. Molteno tube implantation for neo vascular glaucoma. Long term results and factors influencing the outcome. Ophthalmology 1993; 100: 897-902
Migdal CS, Hitchings RA. Morbidity following prolonged hypotony after trabeculectomy. Ophthalmic Surg 1988; 19: 865-867
Migdal CS. Rational choice o f therapy in established primary open angle glaucoma. 1992; 6: 346-347
Miller MH, Grierson 1, Unger W l, Hitchings RA. W ound healing in an animal model o f glaucoma fistulizing surgery in the rabbit. Ophthalmic Surg 1989; 20: 350-357
Mills RP, Reynolds A, Emond MJ, Barlow WE, Leen MM. Long-term survival o f Molteno glaucoma drainage devices. Ophthalmology 1996; 103(2): 299-305
Minckler DS, Heuer DK, Hasty B, Baerveldt G, Cutting RC, Barlow WE. Clinical experience with the single plate Molteno implant in complicated glaucomas. Ophthalmology 1988; 95: 1181-1188.
Minckler DS, Shammas A, Wilcox M, Ogden T: Experimental studies o f aqueous filtration using the Molteno implant. Trans Am Ophthalmol Soc 1987; 84: 368-392.
Molteno ACB, Strachan J, Ancker E. Long tube implants in the management o f glaucoma. S A fr M ed 1976; 50: 1062-1066.
Molteno ACB, Von Rooyen MMB, Bartholomew RS. Implants for draining neovascular glaucoma. Br J Ophthalmol 1977; 61: 120-125
Molteno ACB. New implant for drainage in glaucoma. Animal trial. B r itJ Ophthalmol 1969; 53: 161-168
Molteno ACB. The optimal design o f drainage implants for glaucoma. Trans Ophthalmol Soc N Z 1981; 33: 39-41
Molteno ACB. The use o f drainage implants in resistant cases o f glaucoma. Trans Ophthalmol Soc NZ. 1983; 35: 94-97

134
Molteno CB, Polkinghorne J, Bowbyes A. The vicryl tie technique for inserting a draining implant in the treatment o f secondary glaucoma. Aust N Z J Ophthalmol 1986: 14:343-354
Moroudas NG. Chemistry and mechanical requirements for fibroblast adhesion.Nature 1973; 244:353
M uldoon WE, Ripple PH, Wilder HC. Platinum implant in glaucoma surgery. Arch Ophthal. 1951; 45: 666-672
Mulvihill JN; Faradji A; Oberling F; Cazenave JP. Surface passivation by human albumin o f plasmapheresis circuits reduces platelet accumulation and thrombus formation. Experimental and clinical studies. J Biomed M ater Res, 1990 Feb, 24:2, 155-63
Nordmann JP, Soderstrom M, Rouland JF, Malecaze F. Comparison o f the intraocular pressure lowering effect o f latanoprost and a fixed combination o f timolol-pilocarpine eye drops in patients insufficiently controlled with beta adrenergic antagonists. French Latanoprost Study Group, and the Swedish Latanoprost Study Group. Br J Ophthalmol 2000 Feb;84(2):181-5
Oga M, Sugioka Y, Hobgood CD, Gristina AG, M yrvik QN. Surgical biomaterials and differential colonization by Staphhylococcus epidermis. Biomaterials 1988; 9: 285-289
Pandya AD: Experimental evaluation o f a hydroxylapatite reservoir tube shunt in rabbits. Ophthalmic Surgery & Laser 1996 : 27 (4) : 308-314
Paysee E, Lee PP, Lloyd MA, Sidoti PA, Fellenbaum PS, Baerveldt G, M inckler DS, Heuer DK. Suprachoroidal haemorrhage after Molteno implantation. J Glaucoma 1996; 5: 170-175
Perkins TW, Cardakli F, et al. Adjunctive M itomycin C in Molteno Implant Surgery. Ophthalmology 1995; 102(1): 91-97
Pitt WG, Park K, Cooper SL. Sequential protein adsorption and thrombus deposition on polymeric biomaterials. Journal o f Colloid and Interface Science 1986; 111: 343- 362
Porter JM, Krawczyk CH, Carey RF. In vitro flow testing o f glaucoma drainage devices. Ophthalmology 1997; 104: 1701-1707
Portoles M, Refojo MF and Leong FL. Reduce bacterial adhesion to hearin-surface- modified intraocular J Cataract Refrac Surg.X992\ 19(6): 755-759.
Prata JA, Mermoud A, LaBree L, Minckler DS. In vitro and in vivo flow characteristics o f glaucoma drainage implants. Ophthalmology 1995; 102: 894-904

135
Prata JA, Minckler DS, Mermoud A, Baerveldt G. Effeets o f intraoperative Mitomyein-C on the function o f Baerveldt glaucoma implants in rabbits. J o f Glaucoma 1996; 5: 29-38
Price FW, W hitson WE. Polypropylene ligatures as a means o f controlling intraocular pressure with Molteno implants. Ophthalmic Surg 1989; 20(11): 781-783
R.G.A. Faragher, S. Nagri, S. Dropeova, S.V. Mikalovsky, A.W. Lloyd, G.W. Hanlon, C.J. O lliff and S.P. Denyer. In: Fundamentals o f Adsorption, (LeVAn, M.D. ed.) Kluwar Academic Publishers, Boston, 1996, p. 285-292.
Raina UK, Tuli D. Trabeculectomy with releasable sutures: a prospective, randomized pilot study. Arch Ophthalmol 1998 Oct;l 16(10):1288-93
Rapuano CJ, Schmidt CM, Cohen EJ, Rajpal RK, Raber IM, Katz LJ, Wilson RP, Laibson PR, Kremer I. Results o f alloplastic tube shunt procedures before, during, or after penetrating keratoplasty. Cornea 1995; 14(1): 26-32
Raskin EM, Speaaker MG, McCormick SA, et al. Influence o f haaptic materials on the adherence o f staphylococci to intraocular lenses. Arch Opthalmol 1993;! 11:250- 253
Ratner BD. ESCA and SEM studies on polyurethanes for biomedical applications. In Advances in Chemistry Series No. 162, Dwight DW, Fabish TJ, and Thomas HR, editors. Washington, DC, American Chemistry Society, 1981, pp. 371-382.
Ravalico G; Baccara F; Lovisato A; Tognetto D.Postoperative eellular reaction on various intraocular lens materials. Ophthalmology, 1997 Jul, 104:7, 1084-91
Reiss GR, Lee DA, Topper JE, Brubaker RF. Aqueous humor flow during sleep.Invest Ophthalmol Vis Sci 1984;25:776
Rollett M, Moreau M. Le drainage au crin de la chambre antérieure contre F hypertonie et la douleur. Rev Gen Ophtal. 1907; 26: 289-292
Rollett M, Moreau M. Traitement de phypopyon par le drainage capillary de la chambre antérieure. Rev Gen Ophtal. 1906; 25: 481-489Rollins DF, Drance SM. Five year follow-up o f trabeculectomy in the management o f chronic open angle glaucoma. In: Mosby CV, ed. Symposium on glaucomas: Trans New Orleans A cad Ophthalmol. 1981;295-300
Roth SM, Starita RJ, Spaeth GL, Steinmann WC, Paryzees EM. The effeets o f postoperative corticosteroids on trabeculectomy: long-term follow-up. Invest Ophthalmol Vis Sci. Suppl. 1988;367
Row H. Operation to control glaucoma: Preliminary report. Arch Ophthal. 1934; 12: 325-329.
136
Schocket SS, Lakhanpal V, Richards RD. Anterior chamber tube shunt to an encircling band in the treatment o f neovascular glaucoma. Ophthalmology 1982; 89: 1188-1194.
Schoen FJ. Host reaction to biomaterials and their evaluation. In; Ratner BD, Hoffman AS, Schoen FJ, Lemons JF, eds. Biomaterials science. San Diego:Academic Press, 1996;4:165-173
Schottenstein EM. The epidemiology o f primary open angle glaucoma. In Ritch R, Shields MB, Krupin T eds. The glaucomas, St Louis: CV M osby 1989: 301-317.
Schulzer M, Drance SM, Carter CJ et al. Biostatistieal evidence for two distinct chronic open angle glaucoma populations. Br J Ophthalmol 1990; 74: 196-201
Shahinian L, Egbert PR, Williams AS. Histological study o f healing after ab intemo laser sclerotomy. Am J Ophthalmol 1992; 114:216-219.
Sidoti PA, Dunphy TR, Baerveldt G, Labree L, Minckler DS, Lee PP, Heuer DK. Experienee with the Baerveldt Glaucoma Implant in Treating Neovascular Glaucoma. Ophthalmology, !995: 102: 1107-1118
Siegner SW, Netland PA, Urban RC, Williams AS, Richards DW, Latina MA, Brandt JD. Clinical experience with the Baerveldt glaucoma drainage implant.Ophthalmology 1995; 102(9): 1298-1307
Singh J, Bell RW, Adams A, O'Brien C. Enhancement o f post trabeculectomy bleb formation by laser suture lysis. Br J Ophthalmol 1996 Jul;80(7):624-7
Skuta GL, Beeson CC, Higginbotham EJ, et al. Intraoperative mitomycin versus postoperative 5-fluorouracil in high-risk glaucoma filtering surgery. Ophthalmology. 1992; 99:438-444
Smetana K, Lukas J, Paleckova V, Bartunkova J, Liu FT, Vacik J, Gabius HJ. Effect o f structure o f hydrogels on the adhesion and phenotypic characteristics o f human monocytes. Biomaterials 1997, 18, 1009 - 14.
Smith SG, Galanis JC. One-year results o f the intrascleral glaucoma implant. J Cataract Refract Surg. 1995; 21: 453-456
Smith SL, Starita RJ, Fellman RL, Lynn JR. Early clinical experience with the 2
Baerveldt 350 mm glaucoma implan Ophthalmology 1993; 100: 914-918.
2Baerveldt 350 mm glaucoma implant and associated extraocular muscle imbalance.
Stamper RL, McMenemy MG, Lieberman ME. Hypotonous maeulopathy after
trabeculectomy with subconjunctival 5-fluorouracil. American Journal o f Ophthalmology 1992; 114: 544-553

137
Stavrou P, Murray PI. Heparin surface modified intraocular lenses in uveitis. Ocul Immunol Inflamm 1994;2:161-8
Stefansson, J. An operation for glaucoma. Am J Ophthal. 1925; 8: 681-693
Susanna R, Nieolela MT, Takahashi WY. Mitomycin C as Adjunctive Therapy with Glaueoma Implant Surgery. Ophthalmic Surgery 1994; 25(7): 458-462
Tang L, Eaton JW. Fibrin(ogen) mediates acute inflammatory responses to biomaterials. J Exp M ed 1993; 178: 2147-2156
Tang L, Eaton JW. Inflammatory Responses to Biomaterials. Am J Clin Pathol 1995; 466-471.
Tang L, Lucas AH, Eaton JW. Inflammatory responses to implanted polymeric biomaterials: role o f surface adsorbed IgG. J. Lab. Clin. Med. 1993; 122:292
Tang L; Eaton JW. Fibrin(ogen) mediates acute inflammatory responses to biomaterials. J Exp Med, 1993 Dee, 178:6, 2147-56
Traneosco MU, Use o f tantalum implants for inducing a permanent hypotony in rabbits’ eye. Am J Ophthalmol 1949; 32: 499-508
Trocme SD, Li H. Effect o f heparin-surface-modified intraocular lenses on postoperative inflammation after phacoemulsification: a randomized trial in a United States patient population. Heparin-Surfaee-Modified Lens Study Group. Ophthalmology. 2000 Jun; 107(6): 1031-7
Tromp RM, Hamers RJ, Demuth JE. Quantum states and atomic structure o f silicone surfaces. Science 1986;234:304-390
Umezawa S; Shimizu K. Bioeompatibility o f surface-modified intraocular lenses. J Cataract Refract Surg, 1993 May, 19:3, 371-4
Versura P; Torreggiani A; Cellini M; Caramazza R. Adhesion mechanisms o f human lens epithelial cells on 4 intraocular lens materials. J Cataract Refract Surg, 1999 Apr, 25:4, 527-33
Verwey EJW and Overbeek JHG. Theory o f Stability o f Lyophobic Colloids. 1948. Elsevier, Amsterdam.
Werner EB, Drance SM, Schulzer M. Trabeeulectomy and the progression o f glaucomatous visual field loss. Arch Ophthalmol 1977; 95: 1374- 1380
Wetzel W, Haring G, Brinkmann R, Bimgruber R. Laser sclerostomy ab extemo using the erbium: Y AG laser. First results o f a clinical study. Ger J Ophthalmol 1994 Mar;3(2):112-5
White TC. A new implantable ocular pressure relief device. A preliminary report. Glaucoma 1985; 7: 289-294
138
Yasuda H, Yamanashi BS, Devito DP. The rate o f adhesion o f melanoma cells onto nonionic polymer surfaces. J Biomed Mater Res 1978; 12:701
Zorab A. The reduction o f tension in chronic glaucoma. Ophthalmoscope 1912; 10: 258-261

139
A ppendix 1
Glaueoma valves: Truth versus myth II
Dear Editor:
Lee' has recently exposed the theoretical flaws in the designs o f both the Ahmed and
Krupin Valves, leading marketed glaucoma drainage devices (GDD). Theoretical
flaws may also exist for the OptiMed GDD (Model 1014, Tecfen Corporation, Santa
Barbara, California, USA).
The flow resistance mechanism for the OptiMed device consists o f a small block o f
parallel tubules. No quoted diameter or range o f diameters is either given on the
company web site (www.tecfen.com/medical/ophthal/optimed.html) or published.
We examined a sample OptiMed device, using a field emission scanning electron
microscope (JEOL, Akishima, Japan) and a image analysis software (Scion Corp.,
Maryland, USA). 392 tubules were identified in a PMMA block measuring 3x2.2x0.7
mm. The average diameter o f the tubules was 47.5pm (Figure 1). With a series o f
tubules in parallel, the pressure drop across the device would vary in accordance with
a modification o f Poiseuille's formula^: -
Pressure drop = 128plQ / \36nd"^ N
Where
n = aqueous viscosity I = length o f tube Q = aqueous flow rate d = diameter o f tube N = Number o f tubes in parallel
When applied to glaucoma drainage device, the average aqueous flow rate (Q) can be
assumed" to be 2 pl/min with a viscosity (p) o f 0.001 Nsec/m^. This gives a pressure
drop across the sample device o f only 0.01 mmHg. Even in a patient with an aqueous
flow rate o f 3.1 pl/min% and aqueous viscosity ten times that o f normal, the pressure
drop across the device would still only be 0.169 mmHg.
Recent flow studies'*^ have shown that OptiMed devices did not function as claimed,
this is not surprising in view o f the simple flow analysis given above. No clinical
140
results have been published. Even in the absence o f leakage around the device, a
common problem in GDD implantation, it seems unlikely that the OptiMed device
would offer effective protection from early post-operative hypotony.
References
1. Lee VW. Glaucoma “valves” - truth versus myth, [letter] Ophthalmology
1998;105(4):567-8
2. McEwen WK. Application o f Poiseuille’s law to aqueous outflow. Archives o f
Ophthalmology 1958;60:290-294
3. Brubaker RE. Flow o f aqueous-humor in humans. The Friedenwald Lecture.
Investigative Ophthalmology & Visual Sciencel991;32(13):3145-3166
4. Prata JA, Mermoud A, LaBree L, Minckler DS. In vitro and in vivo flow
characteristics o f glaucoma drainage implants. Ophthalmology 1995; 102: 894-
904
5. Francis BA, Cortes A, Chen J, Alvarado JA. Characteristics o f glaucoma drainage
implants during dynamic and steady-state flow conditions. Ophthalmology
1998;105:1708-1714

141
Figure 1. Scanning electron microscopy image o f a sample Optimed device How restrictor.
^ A.4S G ^
t» .

142
Appendix 2
Rabbit Study Protocol Forms

143
Cage Label
AGFID ANIMAL Study 1
Adyerse Reaction Form Date: / /
Eye
Date o f Operation; Days Post-Op:___
OD/OS
/ /
lOP: OD
Complications:
Systemic illness
Comeal Abrasion
Corneal Oedema
Hypopyon
Deyice Extrusion
Others:
mmHg OS mmHg
Yes No Comments
TREATMENTS
OUTCOME
Inyestigator Signature Date Co-ordinator Signature

144
Cage Label
AGFID ANIMAL Study 1
Operation Records Date: / /
Eye OD/OSAGFID Device Lot #:
Operator:Assistant:Time: Starting Completion
MMC: Concentration Time Area
AC Reform: □ Yes □ No
Drues injected into AC
Complications: Yes No
Excessive sub-conjunctival haem orrhaee [ 1 nConjuctival damaee n nHvnhaema n nPoor anaesthesia n nOthers
Comments:
Investigator Signature Date Co-ordinator Signature

145
Cage Label
AGFID ANIM AL Study 1
Post-operative 10? monitoring study Date: / /
Eye GD/GS
Lot #
IO P:Pre-opGD GS
Post-op
IGF Monitoring
Device: AGFID/Standard
Agent injected into AC DHeparin DTP A DNone
Position of AC tube: DVisible DNot Visible
Cornea:______ DCiear______________ DHazv DVerv Hazv
AC Depth: DFlat DShallow DFormed
Hyphaema: 0100% O>50% D>25% 0<25% GNone
Pre-Clamping IGF: mmHg
Maximum IGF: ____ mmHg
Time Taken to Reach:____ Minutes
Comments:
Investigator Signature Date Co-ordinator Signature

146
Cage Label
AGFID ANIMAL Study 1
Post-Operative Assessment Date: / /
Slit Lamp ExaminationOperated Eye OD/OS
Date o f Operation: / /Davs Post-Op:
IGF: OD mmHg OS mmHg
AC Depth: DFlat
AC Inflammation: □++++
□Shallow DFormed
D+++ D++ D+ D-
Bleb Appearance: DVascular DAvascularHeight_____Area
Comments:
Investigator Signature Date Co-ordinator Signature