Embed Size (px)
Citation preview

Development of the Building Strong
Foundations for Aboriginal Children,
Families and Communities Program
Service Standards
June 2015
LITERATURE REVIEW

NSW Ministry of Health
100 Christie Street
ST LEONARDS NSW 2065
Tel. (02) 9391 9000
Fax. (02) 9391 9101
TTY. (02) 9391 9900
www.health.nsw.gov.au
Produced by: NSW Ministry of Health
Contributors and writers:
University of Technology
Rachel Smith
Angela Dawson
Maralyn Foureur
Cathrine Fowler
Juanita Sherwood
Caroline Homer
It may be reproduced in whole or in part for study or training
purposes subject to the inclusion of an acknowledgement of
the source.
It may not be reproduced for commercial usage or sale.
Reproduction for purposes other than those indicated above
requires written permission from the NSW Ministry of Health.
Suggested citation: Smith, R., Dawson, A., Foureur, M.,
Fowler, C., Sherwood, J., Homer, CSE. 2014, Development of
the Building Strong Foundations for Aboriginal Children,
Families and Communities (BSF) Program Service Standards:
Literature Review, Faculty of Health, University of Technology
Sydney.
© NSW Ministry of Health 2019
SHPN (HSP) 190280
ISBN 978-1-76081-155-6
Further copies of this document can be downloaded from the
NSW Health website www.health.nsw.gov.au
October 2019
NSW Health 1
Table of contents
Executive Summary ___________________________________________________ 2
List of abbreviations ______________________________________________________ 4
Introduction _________________________________________________________ 5
Aims and objectives of the literature review ___________________________________ 5
Background _________________________________________________________ 5
Closing the Gap __________________________________________________________ 6
Building Strong Foundations (BSF) services __________________________________ 7
Methods ____________________________________________________________ 7
Framework used to guide the analysis of literature _____________________________ 7
Search Protocol __________________________________________________________ 8
Inclusion Criterion ________________________________________________________ 8
Findings ____________________________________________________________ 9
The National Framework for Universal Child and Family Health Services __________ 10
Service provision for Aboriginal families ____________________________________ 10
Community development and Community-led design of services __________________________ 11
Specific programs for early childhood ________________________________________________ 12
Specific programs for women during pregnancy and the first few weeks of life ________________ 13
Service Standard Principles _______________________________________________ 14
Defining service standards ________________________________________________________ 15
Justifying the use of service standards _______________________________________________ 15
Structure of service standards _____________________________________________________ 16
Other ways of describing key elements within standards _________________________________ 20
Developing and measuring service standards _________________________________________ 20
Policy and Regulation ____________________________________________________ 20
Policy frameworks _______________________________________________________________ 21
Setting targets in policy ___________________________________________________________ 21
Policy supporting child and family health in NSW _______________________________________ 21
Developing a fit-for-purpose workforce ______________________________________ 22
Influences on the workforce _______________________________________________________ 22
A health workforce that can deliver culturally safe services _______________________________ 22
Capacity building of the workforce __________________________________________________ 23
Clarity of roles, responsibilities and competencies ______________________________________ 23
Conclusion _________________________________________________________ 24
References _________________________________________________________ 25

NSW Health 2
Executive Summary
This literature review was undertaken to inform the development of service standards and workforce
strategy for the Building Strong Foundations for Aboriginal Children, Families and Communities (BSF)
programs in New South Wales. The primary aims of the review were to identify current best practice
examples of service standards and workforce and recruitment strategies for the delivery of high quality
services for Aboriginal1 children, families and communities. The review included literature on service
provision; developing, utilising and identifying effective components of service standards; implementing
and evaluating service standards; and, effective human resource processes to support the provision of
best practice health care for Aboriginal children and families.
The context of the review firstly recognises Aboriginal Peoples as the First Australians and respects
the culture of strong connection and community. The review acknowledges the Aboriginal definition of
health as incorporating a whole of life view, where health includes the physical, social, emotional and
cultural wellbeing of communities and individuals. The historical and ongoing impact of colonisation is
recognised and the importance of adopting a strengths-based approach to working with Aboriginal
families is valued.
An integrative literature review was undertaken and involved a structured search and analysis of both
peer-reviewed and grey literature. The search initially generated 148 papers and documents that met
the inclusion criteria and on closer examination 23 of these were considered not relevant. 125 papers
and documents were examined in detail and from this 84 were used to inform the review. Papers and
documents were analysed and discussed in relation to the following broad topic areas;
Service provision for Aboriginal and Torres Strait Islander families
Service standards principles and content
Implementation and evaluation
Policy and/or regulation that inform standards/services
Workforce development
The analysis of papers in relation to service provision for Aboriginal families provided the review with a
summary of evidence-based principles that should be considered when reviewing existing services or
developing new service standards. Evidence-based principles identified in the literature review are
presented in Table 1.
Table 1: Evidence-based principles identified in the literature review
Evidence-based principles that underpin Aboriginal child and family health programs
Ensure community leadership and sustained involvement in the development of the service Consistent with the principles of Primary Health Care Invest in capacity building for sustainability Provide targeted funding for Aboriginal specific services Provide locally accessible and appropriate services for all families Provide a culturally competent service Ensure flexibility in implementation and service delivery Support a strengths-based and family centred approach Provide integrated services Promote high quality communication and collaboration
1 The term ‘Aboriginal’ is not generally inclusive of Torres Strait Islander people, and reference to both Aboriginal and Torres Strait
Islander people should therefore be spelt out where necessary. Within NSW Health, the term ‘Aboriginal’ is generally used in preference to ‘Aboriginal and Torres Strait Islander’, in recognition that Aboriginal people are the original inhabitants of NSW (see NSW Health Circular No. 2003/55). When discussing or presenting national or international literature that uses the tit le Indigenous,
this terminology will be used.
NSW Health 3
Whilst not made explicit in the service standards literature, there is an assumption that all care
provided by services for Aboriginal children, families and communities will be based on evidence
where evidence is available, and if evidence is lacking, will be based on expert consensus.
There is increasing interest and use of service standards in health service delivery and health
performance measurement. Despite this, there is limited information available on what constitutes
a service standard. However, there is agreement in justifying the use of standards to monitor and
improve services and to provide standardisation and consistency in service delivery. There is also
agreement in the literature in regard to broad key components required in the development of
service standards for child and family health services and these include being based on strong
evidence, having an accepted theoretical basis, being innovative and having cultural reach.
Service standards must also be supported by strong overarching policy direction and regulation. A
number of NSW state policies were identified that should inform the development of service
standards that meet and support the strategic directions of Aboriginal maternal, child and family
health service provision. Strategies for improving Aboriginal health service provision in NSW
include building trust through partnership, ensuring integrated service planning and delivery,
strengthening the Aboriginal workforce and providing culturally safe health services. In relation to
supporting development of an Aboriginal workforce and providing culturally safe services the
evidence identifies ensuring cultural competence training is a requirement for the entire health
workforce.
An important principle in the development, implementation and evaluation of service standards and
service delivery in Aboriginal health is to ensure a grass-roots approach and sustained involvement
of Aboriginal community leaders and service users.
NSW Health 4
List of abbreviations
ACCHO Aboriginal Community Controlled Health Organisations
ACSQHC Australian Commission on Safety and Quality in Health Care
AHEO Aboriginal Health Education Officer
AHW Aboriginal Health Worker
AMIC Aboriginal Maternal and Infant Care
AMIHS Aboriginal Maternal and Infant Health Strategy
AMS Aboriginal Medical Services
BSF Building Strong Foundations
COAG Council of Australian Governments
HCQI OECD Health Care Quality Indicators Project
HPF Health Performance Framework
MGP Midwifery Group Practice
NACCHO National Aboriginal Community Controlled Health Organisation
NPA National Partnership Agreement
PHC Primary Health Care
SNAICC Secretariat of National Aboriginal and Islander Child Care
SMSBSC Strong Mothers, Strong Babies, Strong Culture Program
WHO HSPA WHO Health Systems Performance Assessment Framework
WHO World Health Organization
NSW Health 5
Introduction
A literature review was undertaken to inform the development of the Building Strong Foundations for
Aboriginal Children Families and Communities (BSF) program Service Standards. The BSF Service
Standards (BSF Standards) will assist health services, clinical stream directors, managers and BSF
staff to ensure BSF programs are delivered consistently so that they support Aboriginal families,
children and communities so that Aboriginal children have the best start to life, are healthy, and ready
for school.
The BSF Standards will set out specifications and procedures intended to ensure BSF program
systems are culturally safe, reliable and consistently perform the way they were intended to. The BSF
Standards will establish a common language that defines quality and safety criteria; they will be
practical, outline achievable goals and be based on best practice evidence where available or by
consensus of relevant clinical/content and Aboriginal family experts.
It is important that evidence informs the BSF Standards and the workforce strategy developed as part
of this project. Identifying the evidence is therefore the focus of this document.
Aims and objectives of the literature review
The aim of the literature review was:
To identify current high quality evidence and published best practice examples to assist in the
development of service standards for the delivery of high quality family centred health services
for Aboriginal children and families
To identify evidence and published best practice examples of workforce and recruitment
activities that can assist to ensure the BSF services provided are culturally safe, reliable and
consistent services for Aboriginal children and families
There were a number of specific objectives. These were:
1. Review the evidence relating to the effective provision of services for Aboriginal families
2. Identify the principles that underpin the effective provision of services to these children and
families
3. Investigate the principles that underpin best practice service standards generally, and more
specifically in relation to child and family health services
4. Examine what constitutes the most effective structure and components of service standards
5. Identify relevant policies and regulations that will inform the development and implementation
of service standards
6. Explore the processes involved in the development, implementation and evaluation of service
standards generally, and more specifically in relation to child and family health services
7. Identify factors that contribute to developing a fit-for-purpose workforce in relation to the
provision of child and family health services for Aboriginal children and their families
8. Examine the most effective human resources processes to support, develop and assess
individual and team performance against service standards
Background
Aboriginal Peoples are recognised and respected as the First Nation Peoples of Australia and as such,
like other Indigenous Peoples, have a strong affinity with the land and all that live on it. Aboriginal
Peoples had a strong, sustainable and healthy livelihood up until colonisation and this can in part be
attributed to their traditional view of health. The nationally recognised definition of Aboriginal Health
refers to health as:
‘…not just the physical wellbeing of an individual but refers to the social, emotional and
cultural wellbeing of the whole community in which each individual is able to achieve their full
potential as a human being, thereby bringing about the total wellbeing of their communities. It
is a whole of life view and includes the cyclical concept of life-death-life’ (1).

NSW Health 6
It is neither possible nor respectful to discuss Aboriginal health without firstly recognising the positive
impact that Aboriginal Community Controlled Health Organisations have had on Aboriginal health
outcomes since their advent in the early seventies. Local Community control of health is important for
Aboriginal Peoples as it promotes an Aboriginal model of health and wellbeing and promotes self-
determination. Aboriginal Community Controlled Health Organisations are exemplars of a primary
health care model and are administered by Communities, in Communities and for Communities. They
ensure a grass-roots approach to planning, delivering and evaluating health services and promote
community engagement and integrated service delivery that is effective and culturally competent for
that particular Community (2).
The Australian Government recognises that ‘dispossession, interruption of culture and
intergenerational trauma have significantly impacted on the health and wellbeing of Aboriginal and
Torres Strait Islander people’ (3p10). Previous failure to recognise the impact colonisation has had on
Aboriginal peoples has contributed to the myth that Aboriginal Peoples are somehow responsible for
the poor states of health found in some Communities. A continued focus on poor states of health and
disease has in turn created a ‘problem to be solved’ and has led to a deficit-based approach to
improving Aboriginal health outcomes (4). A focus on deficits in relation to health and wellbeing of
Aboriginal Peoples has prevented developing an understanding of cultural and community practices
that support and strengthen Aboriginal health. In relation to Aboriginal child and family health, a deficit-
based approach has pervaded health interventions and historically there has been little recognition of
the strengths and resilience of Aboriginal childrearing practices. The interventionist approach has failed
to recognise the importance of community engagement, cultural respect and community partnership in
effecting positive health and wellbeing (5).
Closing the Gap
In relation to improving health outcomes the terms ‘closing the gap’ and ‘close the gap’ are now
synonymous with Aboriginal Health and despite popular belief, the closing the gap strategy was not
developed by the Government. In 2006, the National Indigenous Health Equality Campaign which
comprised of a number of organisations including the National Aboriginal Community Controlled Health
Organisation (NACCHO) and Oxfam Australia used the phrase ‘close the gap’ for its publicity campaign
in regard to the inequality in life expectancy (6). This bringing together of prominent organisations
committed to addressing inequalities in Aboriginal life expectancy prompted the Council of Australian
Governments (COAG) to commit to and be accountable for ‘closing the gap’ within a specific
timeframe. In addition to addressing inequality in life expectancy in one generation COAG also
publically committed to increasing access to early childhood education, halving the gap in infant
mortality and reading, writing and numeracy achievement by 2018, and halving the gap in year 12
achievements by 2020 (7).
Since the Closing the Gap awareness campaign in 2006 and the COAG adoption of targets in 2008,
numerous strategies and actions have been implemented in an attempt to address the gap. One of
these strategies is a National Partnership (NP) between State and Territory Governments aimed at
improving Indigenous early childhood development services and outcomes (8). The Indigenous Early
Childhood Development (IECD NP) has direct relevance to the Building Strong Foundations (BSF)
program in New South Wales. The BSF program is entirely funded by the NSW government. Funding
for the program contributes to commitments made by the NSW Government under element three of the
IECD NP.
The Indigenous Early Childhood NPA has three priority areas (also known as elements). These are:
1. Integration of early childhood services through children and family centres;
2. Increased access to antenatal care, pre-pregnancy and teenage sexual and reproductive health;
3. Increased access to, and use of, maternal child health services by Indigenous families.
The IECD NP ceased on 30 June 2014, however the Commonwealth government has made
commitments in the 2014-15 budget to continue funding for the element three ‘New Directions program’
and extend funding for 12 months to element two priority area.
NSW Health 7
Building Strong Foundations (BSF) services
NSW Health has designed, developed and implemented BSF services. BSF is a primary health care
model of care, with Aboriginal Health Workers and Child and Family Health Nurses working in
partnership to provide a strengths-based approach to early childhood health for children from 0–school
entry and their families. The program aims to promote health and wellbeing, support parenting,
enhance community development, identify health, development and wellbeing concerns, and provide or
refer children and families for early intervention to ensure children have the best possible start in life
and are school ready (9-11).
This model is consistent with the Supporting Families Early policy suite, Aboriginal Maternal and Infant
Health Services (AMIHS) and Families NSW principles and is based on the ecological systems theory
of child development (11). The BSF Program promotes culturally appropriate and safe clinical practice
based on sound evidence, knowledge and skills. It closely interfaces with Aboriginal maternity
programs especially the NSW Health Aboriginal Maternal and Infant Health Services (AMIHS) (9-11).
The BSF services are delivered by Local Health Districts and an Aboriginal Community Controlled
Health Service (Albury Wodonga) and are overseen by NSW Kids and Families (NSW K+F).
This literature review was undertaken to seek evidence to support and inform the development of
service standards for the Building Strong Foundations for Aboriginal Children, Families and
Communities programs in New South Wales. The BSF Standards will set out specifications and
procedures to ensure BSF systems are culturally safe, provide high quality evidence based clinical
care that is reliable and provided consistently the way they were intended. The BSF Standards will
support the establishment of a common language that defines high quality and safe service provision.
The BSF Standards need to be practical, outline achievable goals and based on best available
evidence or by consensus of relevant experts where there is no clear evidence available.
Methods
An integrative literature review was undertaken and involved a structured search and analysis of both
peer-reviewed and grey literature. Although there is no standardised format for integrative literature
reviews it is recognised that results of the search are arranged and critically discussed by relationships
and not by chronological order. An integrative review commences with a conceptualised structuring of
the topic so that literature relationships can be identified prior to the review and these serve to provide
a framework for the review (12).
Framework used to guide the analysis of literature
The development of relevant, evidence-based and practical service standards for BSF programs
necessitated a review of a broad range of literature. To ensure the review was undertaken in a
systematic way a framework was developed to guide the literature search and the analysis of the
retrieved documents. This enabled the findings to be presented in a coherent manner.
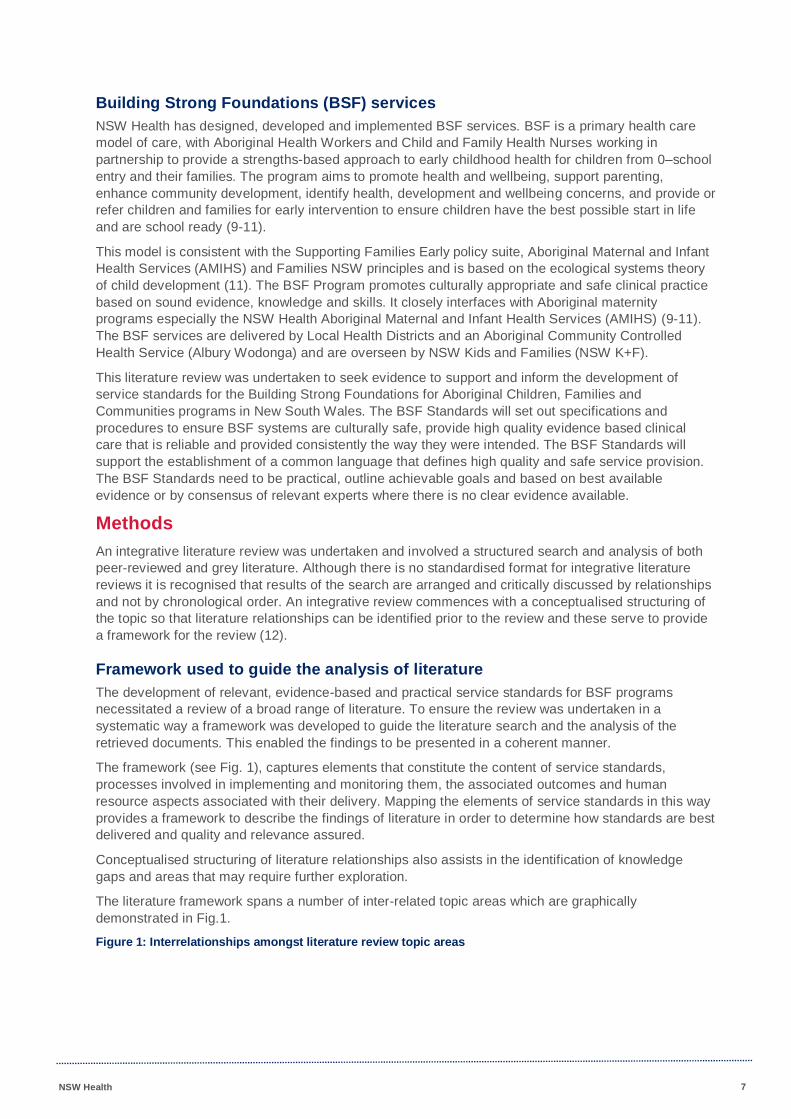
The framework (see Fig. 1), captures elements that constitute the content of service standards,
processes involved in implementing and monitoring them, the associated outcomes and human
resource aspects associated with their delivery. Mapping the elements of service standards in this way
provides a framework to describe the findings of literature in order to determine how standards are best
delivered and quality and relevance assured.
Conceptualised structuring of literature relationships also assists in the identification of knowledge
gaps and areas that may require further exploration.
The literature framework spans a number of inter-related topic areas which are graphically
demonstrated in Fig.1.
Figure 1: Interrelationships amongst literature review topic areas
NSW Health 8
Search Protocol
A systematic search of the literature was undertaken using 6 bibliographic databases (Indigenous
Collection (Informit), MEDLINE, Academic Search Complete (EBESCO), SCOPUS (Elsevier),
PubMED, and Health Business Full Text Elite (EBESCO)) between 2004 and 2014. In addition, Google
Scholar was used to search for grey literature such as Government and non-Government reports,
evaluations, policies and regulatory documents. In an effort to identify key Aboriginal health
publications and resources websites such as SNAICC (Secretariat of National Aboriginal and Islander
Child Care) and the Closing the Gap Clearinghouse were searched. A further hand search of
references used to inform the grey literature was undertaken.
The following search terms were used in bibliographic databases to locate relevant documents:
‘service standards’, ‘health service’, ‘early childhood’, ‘Aboriginal’, ‘Aboriginal and Torres Strait
Islander’, ‘Australian Indigenous’, ‘quality indicators’, and, ‘service delivery’. The systematic
bibliographic database searches where possible utilised MeSH medical subject headings. MeSH
provides descriptors in a hierarchical structure that permits searching at various levels of specificity.
The following MeSH subject headings were used; ‘service standards’, ‘workforce development’
‘Indigenous’ and ‘Aboriginal Health’. Subject terms of key words for the Google Scholar search
included combinations of the terms above. The terms were agreed prior to undertaking the integrative
review.
All search results were reviewed and relevant publications were imported and manually entered into an
Endnote bibliographic software program, broadly categorised into type of document and analysed in
relation to the topic and focus area. Given the broad nature of the search topic and the reliance on grey
literature to identify relevant documents the search continued as the review progressed.
Inclusion Criterion
Publications from 2004 to (March) 2014 were included in the review. The search included:
Original research papers
Peer reviewed opinion papers
Service or service standards evaluation reports
Policy documents
Regulatory documents
Australian and international documents were included in the review. As described previously, the
reference lists of published papers, policy documents and evaluation reports were also examined to
determine whether there were any additional resources which would be valuable to include.
NSW Health 9
Findings
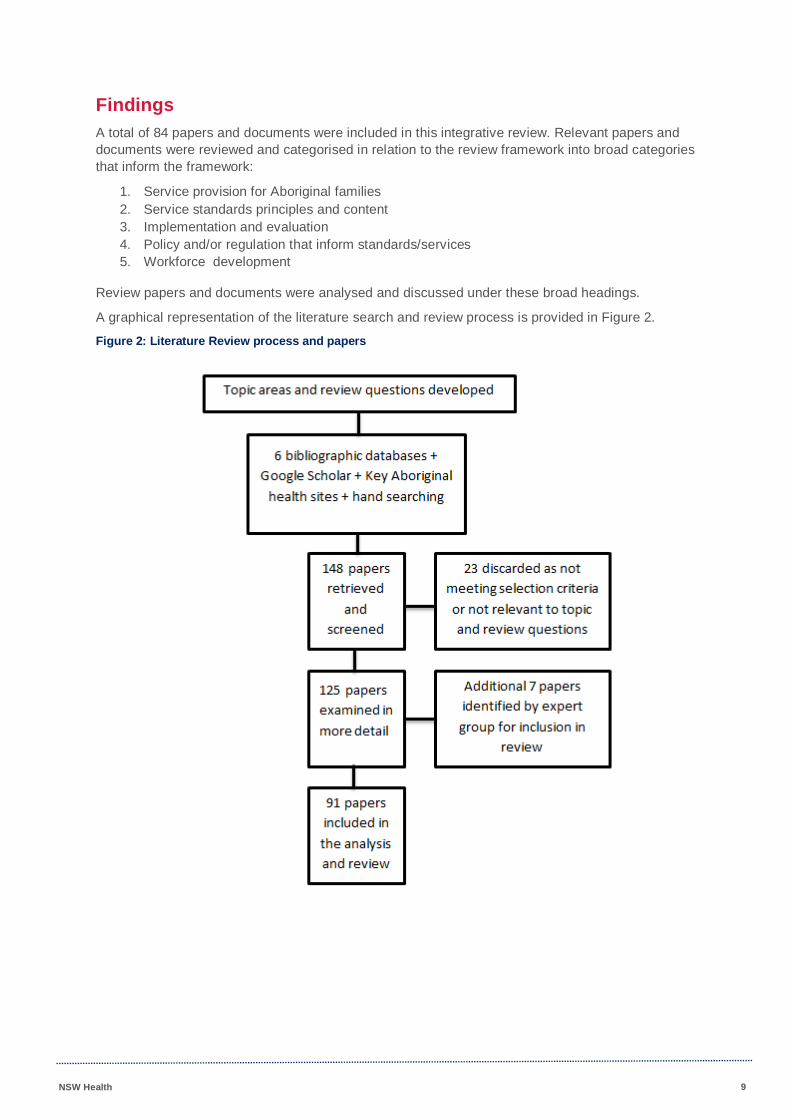
A total of 84 papers and documents were included in this integrative review. Relevant papers and
documents were reviewed and categorised in relation to the review framework into broad categories
that inform the framework:
1. Service provision for Aboriginal families
2. Service standards principles and content
3. Implementation and evaluation
4. Policy and/or regulation that inform standards/services
5. Workforce development
Review papers and documents were analysed and discussed under these broad headings.
A graphical representation of the literature search and review process is provided in Figure 2.
Figure 2: Literature Review process and papers
NSW Health 10
The National Framework for Universal Child and Family Health Services
The National Framework for Universal Child and Family Health Services (The Framework) sets out a
vision for the provision of health services for all Australian children that states ‘All Australian children
benefit from quality universal child and family health services that support their optimal health and
development’ (13. p2.) . The Framework outlines service principles to achieve the vision and these
include access; equity; focus on promotion and prevention; partnership with families; recognising and
respecting diversity; collaboration and continuity; and evidence-based service provision. The service
principles identified in the Framework also appear alongside others as essential principles that should
underpin Aboriginal child and family health services (see Table 1.).
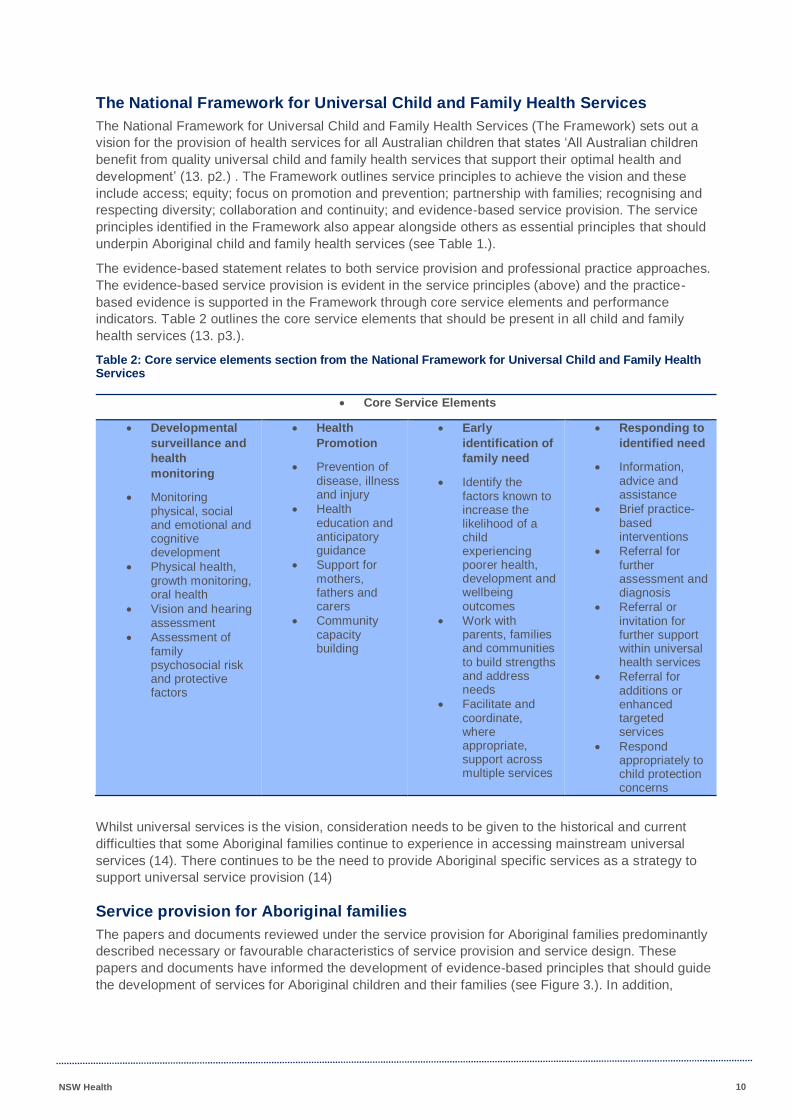
The evidence-based statement relates to both service provision and professional practice approaches.
The evidence-based service provision is evident in the service principles (above) and the practice-
based evidence is supported in the Framework through core service elements and performance
indicators. Table 2 outlines the core service elements that should be present in all child and family
health services (13. p3.).
Table 2: Core service elements section from the National Framework for Universal Child and Family Health Services
Core Service Elements
Developmental
surveillance and
health
monitoring
Monitoring physical, social and emotional and cognitive development
Physical health, growth monitoring, oral health
Vision and hearing assessment
Assessment of family psychosocial risk and protective factors
Health
Promotion
Prevention of disease, illness and injury
Health education and anticipatory guidance
Support for mothers, fathers and carers
Community capacity building
Early
identification of
family need
Identify the factors known to increase the likelihood of a child experiencing poorer health, development and wellbeing outcomes
Work with parents, families and communities to build strengths and address needs
Facilitate and coordinate, where appropriate, support across multiple services
Responding to
identified need
Information, advice and assistance
Brief practice-based interventions
Referral for further assessment and diagnosis
Referral or invitation for further support within universal health services
Referral for additions or enhanced targeted services
Respond appropriately to child protection concerns
Whilst universal services is the vision, consideration needs to be given to the historical and current
difficulties that some Aboriginal families continue to experience in accessing mainstream universal
services (14). There continues to be the need to provide Aboriginal specific services as a strategy to
support universal service provision (14)
Service provision for Aboriginal families
The papers and documents reviewed under the service provision for Aboriginal families predominantly
described necessary or favourable characteristics of service provision and service design. These
papers and documents have informed the development of evidence-based principles that should guide
the development of services for Aboriginal children and their families (see Figure 3.). In addition,

NSW Health 11
included in this broad category were papers and documents that examined and/or evaluated specific
programs for Aboriginal families.
Despite efforts to ‘close the gap’ disparity remains between Aboriginal and non-Aboriginal Australians
in terms of Aboriginal disease burden and common health indicators and measures (15, 16). It is now
widely accepted that colonisation had, and continues to have, a negative impact on the health and
wellbeing of the First Nation Peoples in Australia (4). In recognition of this, colonisation is now well
accepted as a social determinant of Indigenous health (17). In an attempt to address the burden of
disease that exists for Aboriginal Peoples various interventions and strategies have been introduced
with varying rates of success.
The Commonwealth Department of Health aims to improve services for Aboriginal Peoples through
three targeted approaches to service delivery. Firstly, through improving access and responsiveness of
existing mainstream health services, then by providing Aboriginal specific services and lastly through
improving service delivery by increasing cross government collaboration (18). One aspect of this cross-
government collaboration is the National Partnership Agreements between the Commonwealth and
state and territory governments. These agreements ensure governments are working towards a
common framework, using common indicators and measures, and policies. There are six National
Partnership Agreements in relation to the Closing the Gap policy and the first of these is Indigenous
Early Childhood Development (8, 19).
Community development and Community-led design of services
Although many programs developed or applied to Aboriginal health claim to use a ‘community
development’ approach, in reality there is contention as to what this actually means and how it
translates into service provision (20). Much of the published evidence in regard to community
development describes the process but fails to measure or discuss the outcomes (20) This is not to
say that community development is not successful, but historically there has been a lack of evaluation
on the process and outcomes and as such, the process is not well represented in the literature (20).
Despite the lack of formal evaluation, there exists much report-based and anecdotal evidence of the
success of various community development programs and it continues to be an important underpinning
principle of service delivery in Aboriginal health.
Evidence from Australia and overseas demonstrates that for services to be accepted by those they are
designed for, a grass-roots approach is needed with community leadership and sustained involvement
in the development of the service. In Australia, the National Aboriginal Community Controlled Health
Organisation (NACCHO) claims that Aboriginal Community Controlled Health Organisations (ACCHO)
have been responsible for many of the health gains achieved in the past 50 years. NACCHO assert
that it is the grass-roots model of Aboriginal communities working with, and for, Aboriginal communities
that allows communities to reclaim control of health and self-determination (16). The NACCHO 10
Point Plan 2013-2023 lists key steps that they consider will support progress to closing the gap and
reaching health equality targets. These key steps include developing service models and workforce
strategies to build and sustain capacity and provide primary health care services where most needed
(16). In support of NACCHOs vision in relation to primary health care services for Aboriginal
communities the Australian Government has committed to working in partnership to improve delivery of
coordinated and culturally respectful care (18).
Despite widespread acceptance that programs developed for Aboriginal families should be led by, and
situated within Aboriginal communities, this is often not the case. Many programs designed and
delivered in mainstream child health are then ‘adapted’ for Aboriginal families. When programs are not
developed in respectful and inclusive ways, by involving the communities and families from the outset,
then often the programs are not suited to the needs of the communities (21). Aboriginal Peoples are
not a homogenous group and their cultures are complex and diverse. This diversity creates the need to
ensure any program developed has the flexibility to be adapted to the local context or Country where it
is to be offered (22).
NSW Health 12
Specific programs for early childhood
Although the need for Aboriginal specific, early intervention, early childhood programs is widely
accepted there is limited rigorous research evaluating these programs (14, 23). In relation to
mainstream early childhood health services, there is extensive research to support provision of
accessible and appropriate universal services for all families (24) and much support exists around the
importance of ensuring best possible environments in the early years as these years have significant
impact on ensuring long-term health (23).
It is important to remember that much of the research into Aboriginal early childhood health services
has been conducted using western approaches to research and that Indigenous research
methodologies have not previously been widely utilised (25). In addition, much of the research into
early childhood health focuses on the physical aspect of health and largely ignores the social,
emotional and spiritual aspects of the child, the family and the community that they live in and to which
they belong. This approach disregards the whole of life view that is Aboriginal health and therefore
limits the research (4, 25-27). Historically, research into Aboriginal health has examined issues or gaps
and as such has taken a deficit approach to Aboriginal child health and fails to recognise and celebrate
the strength and resilience of individuals, families and communities (21). In an exploration of Australian
Aboriginal childrearing practices (5) Geia found that using a strengths-based approach shifts the focus
away from problems and focusses on community and family strengths. This and other research also
identified essential components required when preparing health practitioners to work in Aboriginal
communities. Essential components included community engagement, cultural respect and working in
partnership with communities (5, 27-31).
In a review of the literature regarding effective early intervention strategies for Indigenous children and
their families, Munro (14) set out to answer questions in regard to the provision of specifically designed
services for Aboriginal children and families and early intervention programs (with a focus on child
protection). The review investigated the effectiveness of these services, and if effective, what factors
may have contributed to positive outcomes. They found only one specifically designed program that
met the methodological selection criteria, the Aboriginal Maternal and Infant Health Strategy (AMIHS).
The other programs examined in the review were adapted from mainstream programs (14). The review
outlines three Australian programs that examined early intervention strategies and two of these used
the Positive Parenting Program (Triple P) as an intervention. One was a randomised clinical trial
testing the adaptation of the evidence-based Positive Parenting Program (Triple P) with Aboriginal
families. Results indicated that the response to the program was generally positive and the authors
claim that the results provide evidence that an effective program can be made to fit the needs of
Aboriginal people and can be delivered by Aboriginal Health Workers in a community setting (14). The
other two studies were mainstream programs with some Aboriginal families identified as participants.
A commonly identified effective strategy or underlying principle of early childhood health services for
Aboriginal children and families is the provision of a culturally competent service (14, 23, 30-33). Other
strategies include supporting equitable access through assistance with transport or providing an ‘in-
home’ service to negate the need for transport to access care; providing a flexible service delivery
mode; and, ensuring community consultation occurs at all levels of planning and service delivery (14).
Other characteristics in addition to program flexibility have been identified in the research regarding
successful prevention and early intervention programs for Indigenous children in the early childhood
years. In their review of the literature on health intervention programs for Australian Indigenous
children and families Bowes and Grace (21) present evidence around what works. This includes
programs that adopt a strengths-based approach; are family centred; involve communities in
development and implementation; adapt to suit local need so are therefore flexible; and, provide
integrative and collaborative services. In addition to these characteristics, the evidence supports
allowing longer lead in times to ensure appropriate and respectful engagement with communities and
high-quality cultural competence training for all non-Aboriginal staff (14, 21, 23).

NSW Health 13
Specific programs for women during pregnancy and the first few weeks of life
Due to the lack of available published research literature on Indigenous specific early childhood health
programs a number of Indigenous specific maternal child health programs that are more pregnancy
and early weeks related are presented below.
A small number of specific services have been developed in Australia and Canada for Indigenous
women. In NSW, the goal of the NSW Aboriginal Maternal and Infant Health Service (AMIHS) is to
improve the health of Aboriginal mothers and babies. Midwives and Aboriginal Health Workers (AHWs)
or Aboriginal Health Education Officers (AHEOs) work together in small teams to provide a high quality
service that is culturally respectful, woman centred, based on primary health care principles and
provided in partnership with Aboriginal Peoples. AMIHS builds on the universal maternity services that
are available in NSW and has demonstrated improved outcomes for women and babies (34).
Evaluation of AMIHS programs demonstrated the following outcomes (34);
increase in the number of women accessing pregnancy care before 20 weeks gestation
decrease in the number of low-birth weight babies
decrease in the number of babies born prematurely
decrease in perinatal mortality
increase in initiation and continuation of breastfeeding, and
increase in rates of satisfaction for women accessing the service.
In addition to these results, an evaluation of an extended AMIHS program (including the provision of
labour and birth support) demonstrated a decrease in the rates of smoking and satisfaction with care
particularly in the areas of ease of access, having a known carer and being able to form trusting
relationships with caregivers (31, 35).
In northern Australia, the “Strong Mothers, Strong Babies, Strong Culture” Program (SMSBSC), was
developed in the 1990s as a community-based intervention program to address the discrepancy in
perinatal health outcomes for Aboriginal women in the Northern Territory. The intervention, involving
senior women in the Aboriginal communities aimed at helping younger women prepare for pregnancy,
support them during pregnancy by encouraging them to attend antenatal clinics early in their
pregnancy, and provide useful advice regarding healthy practices during pregnancy such as ceasing
alcohol consumption and smoking, maintaining a healthy diet including increasing “bush tucker” intake
and reinforcing the importance of seeking appropriate medical advice and adhering to treatment. An
evaluation of the program demonstrated a significant increase in birth weight of the babies of women in
the intervention group (36).
In Queensland, the “Mums and Babies” program is an integrated model of shared antenatal care
delivered by the Townsville Aboriginal and Islanders Health Service. An evaluation of the program
demonstrated a significant increase in the number of antenatal visits and the women were at an earlier
stage in their pregnancy at their first antenatal visit. Quality of antenatal care was improved and
perinatal outcomes improved in all areas, with a reduction in pre-term birth, and an increase in mean
birth-weight. Perinatal mortality was reduced from 60 per 1000 to 14 per 1000 (37).
Similarly, in the southern part of Australia, The Anangu Bibi Family Birthing program, staffed by
Aboriginal Maternal and Infant Care (AMIC) workers and midwives was established to provide care to
Aboriginal mothers and families in two sites in regional South Australia. Both the AMIC workers and the
midwives reported benefits from working together, the AMIC workers bringing the cultural knowledge to
the partnership and the midwives bringing the clinical knowledge. Whilst this study did not address
improved outcomes for mothers and babies, anecdotal evidence shows an increase in the use of
services by Aboriginal women and families (38).
In Victoria, the Women’s Business Service was implemented as a primary health care service. This
program provides holistic, personalised care by a midwife and an Aboriginal Maternal Health Worker
and was also evaluated favourably from the perspective of the women (39). Women who experience
care at the Woman’s Business Service were significantly more likely to feel positive about aspects of
their antenatal care such as feeling well informed, not feeling rushed and being happy with the care
NSW Health 14
than other women attending the rural public antenatal service. In addition, these women were
significantly more confident in caring for their babies and less likely to want additional help or advice in
their first week at home (39).
More recently in the Northern Territory, The Darwin Midwifery Group Practice (MGP) has been
established to provide continuity of care/carer for remote-dwelling Aboriginal women from seven Top
End remote communities, who travel to Darwin for birth (40, 41). A costs analysis of this model of
service provision for remote dwelling Aboriginal women who travelled to Darwin to give birth, showed
MGP was cost effective, and women received better care and experienced equivalent birth outcomes
compared with the baseline maternity care (40).
There are also international examples of primary health services for Indigenous women and families.
For example, the Inuulitsivik Midwifery Service and education program integrates both traditional and
modern approaches to care and education and has returned childbirth to the remote communities of
Nunavik, one of the Inuit regions of Quebec, Canada. This service provides care for seven
communities in the Hudson Bay and Hudson Straits areas with a population of around 5500. All the
communities are accessed by ‘fly-in’ and the tertiary referral centre is more than 1000 miles away in
Montreal. Previously, women were evacuated from their homes and flown to southern Canada four or
more weeks before the due date to give birth, and they stayed one or two weeks after the birth, thus
isolating them from their families for 5-8 weeks (42). The Inuulitsivik model provides midwifery-led
antenatal and postnatal care and birthing services for women of “low-risk” in the larger villages of the
Hudson Coast. The smaller villages receive onsite antenatal care but are transferred to give birth. This
comprises around 25% of the women in this area, however they are receiving antenatal care in their
own language, in their home region, by Inuit midwives (43). Evaluations of the model demonstrate
improvements in perinatal mortality, increase in birth weight, decrease in preterm birth and increase in
breastfeeding rates (44).
Review and analysis of literature related to service provision for Aboriginal families provides direction in
terms of characteristics or components required of such services. Evaluation of Aboriginal maternal,
child and family specific services for the purpose of this review has informed the development of
evidence-based principles that should be incorporated into existing services or used when developing
services for Aboriginal women and families. The evidenced based principles are listed in Table 3.
Table 3: Summary of the evidence in relation to service provision
Evidenced based principles that underpin Aboriginal child and family health programs
1. Ensure community leadership and sustained involvement in the development of the service 2. Consistent with the principles of Primary Health Care 3. Invest in capacity building for sustainability 4. Provide targeted funding for Aboriginal specific services 5. Provide locally accessible and appropriate services for all families 6. Provide a culturally competent service 7. Ensure flexibility in implementation and service delivery 8. Support a strengths-based and family centred approach 9. Provide integrated services 10. Promote high quality communication and collaboration
Whilst not made explicit in the service standards literature, there is an assumption that all care
provided by services for Aboriginal children, families and communities will be evidence based where
evidence is available and if evidence is lacking will be based on expert consensus.
Service Standard Principles
Relevant papers reviewed in regard to service standards or the principles that underpin service
standards included papers that defined or provided information on what a service standard is and what
they are commonly used for. Whilst a number of papers described or presented service standards
there was a dearth of information regarding the evaluation of or results from implementing service
standards.

NSW Health 15
Although evidence of health related service standards or service delivery standards have been present
in the literature from more than three decades ago (45), in the past ten years there has been a
significant increase in the number of service standards developed and produced. Since the advent and
acceptance of national and international health accreditation processes such as the WHO Health
Systems Performance Assessment Framework (WHO HSPA), the OECD Health Care Quality
Indicators Project (HCQI) and the Australian National Health Performance Framework (46, 47), the
development and subsequent use of service standards or service delivery standards has increased.
Service standards should be linked with national policies and best practice frameworks (48-52). In the
area of child and family health services and in particular services for Aboriginal children and families,
service standards should therefore be informed by:
Respecting the Difference An Aboriginal Cultural Training Framework for NSW Health
PD2011_069;
the National Framework for Universal Child and Family Health Services;
the Aboriginal and Torres Strait Islander Health Performance Framework; and
the proposed National Framework for Aboriginal and Torres Strait Islander Child and Family
Health Services (1, 13, 15, 23, 53, 54).
In relation to the BSF service standards, these will also be informed by relevant NSW state policies
and frameworks. The Standards will also be informed by the experiences and expertise of those
currently working within BSF services across the state.
Defining service standards
Health performance measurement systems and processes are becoming widely accepted and
increasingly important in health service provision across Australia (55). In particular, health
performance measurement in relation to Aboriginal and Torres Strait Islander health outcomes has
become more focussed since the introduction of the Aboriginal and Torres Strait Islander Health
Performance Framework (HPF) (56). Crucially, there are no clear, agreed definitions of a service
standard or quality indicator. At times, the literature uses these terms interchangeably. However,
agreement does exist that both should provide a target and a measure of services or care provided.
Despite all the interest in service standards, definitions or descriptions of what constitutes service
standards are lacking. Examination of the service standard literature provides limited information on
what service (delivery) standards are. The Department of Education and Children’s Services (49p.3)
state that service standards are:
‘…a set of clear and public criteria with explicit indicators that define the service delivery
performance by which Support Services can be monitored and reviewed.’
Furthermore, they go on to say that service standards are used to define the quality of service provided
by the organisation and therefore should be at a level that is clear, measurable and achievable (49p.3).
Similarly, the Institute for Citizen Services state that service standards:
‘…outline the specific delivery targets established by an organization [sic], and are made up of
a set of commitments that an organization [sic] promises to honour when delivering a service.’
While the stated definitions of service standards are similar and succinct, many of the reviewed
standards provided further detail when justifying the use or the purpose of service standards.
Justifying the use of service standards
There is a range of reasons given to justify the use of service standards in health care service delivery.
The Australian Commission on Safety and Quality in Health Care (ACSQHC) developed standards to
introduce safety and quality systems to ensure high levels of health care provision (48). The
ACSQHC’s primary and overarching standard from the National Safety and Quality Health Service
Standards document concerns governance. The ACSQHC assert that Standard 1 provides a safety
and quality governance framework and informs all other ACSQHC standards. The governance

NSW Health 16
framework is designed to create a health system where performance can be monitored and continually
improved (48).
Provision of a system to monitor and improve service delivery and service quality is a common
justification for, or stated purpose of, service standards. Swersey (57), when discussing the use of
standards in health care, asserts that quality cannot be improved if it is not being measured. The
Queensland Government, in their Standards for Community Services state that setting service
standards is important to ensure community service provision is safe and able to be continuously
improved (58). The Victorian Government’s Human Service Standards were, in part, produced to try to
reduce ‘red tape’ so as to streamline monitoring and evaluation processes (59).
Whilst the majority of producers of service standards include quality improvement and monitoring
processes as a justification for the need for standards, there is some confusion regarding the
terminology used. There exists an undeniable relationship between service standards and quality
standards with the terminology being used interchangeably in some of the literature (48, 49, 59). In
addition, many of the standards reviewed included quality and/or performance indicators within their
respective frameworks.
Each service standards document reviewed uses some form of quality provision or measuring in
discussions around the purpose of the standards, but provision of quality or measures of quality is not
the sole purpose of standards. Another justification for the production and the increasingly widespread
use of service standards is the identification of evidence to support best practice. When the reviewed
standards documents provide information on the development of the standards, best practice and
evidence-based framework claims feature regularly (50, 60). Given the focus on high quality service
provision and quality care service, standards must be based on best practice care (50).
Further justification for the use of service standards is the expectation that there should be
standardisation or consistency in service provision or delivery so that each client or service user
experiences the same high level of quality care (48, 51, 61). Inconsistencies in service delivery may
affect the organisation’s ability to meet expected standards (best practice) in care provision. Many
services are underpinned by a vision, mission and/or guiding principles and inconsistencies in services
will impact on the organisation’s ability to ensure these are met. The service standards reviewed for the
purpose of this review covered a variety of services such as disability and juvenile justice services,
therefore each set of standards should include service specific information and service standards
developed for Aboriginal child health services will contain information on child health development and
wellbeing outcomes and cultural care.
Structure of service standards
Although the structure of the reviewed service standards differs, essentially the content of the
standards is similar. Many standards documents have a small number (4-12) of overarching ‘standard’
statements and within each standard there are elements/components/outcomes and performance
criteria, evidence or measures (48, 50, 59, 60, 62, 63). Alternate structures include statement of a
standard and explanation points with practice tips and the provision of a separate tool for auditing or
measuring (61, 64). The Community Relations Commission for a Multicultural NSW used an alternate
approach in format whereby they identified three activity areas. Each activity area is comprised of
outcomes, which when compared with similar service standards or service standard frameworks, the
outcomes could be identified as service standards (52).
Regardless of the differing structure and nomenclature used in standards documents, most of the
standards provide information on the development process. This includes advocacy for a systematic
approach to development that includes defining quality services, stakeholder engagement,
development of quality indicators and a plan for implementation (45, 48, 49, 57, 60, 65). Swersey (57)
proposes a detailed development framework that includes determining the needs of customers;
defining what quality is and developing a quality statement; measuring satisfaction; being specific
about the expected standards of service; and, developing key quality measures.
NSW Health 17
The Department of Education and Children’s Services (49) provide further detail on a framework for
development that includes additional considerations such as consideration of existing policies or
standards and consideration of the roles and responsibilities of staff within the services. Others
advocate the creation of a mission statement to provide clarity (51) comprehensive consultation and
consensus (66) and, ensuring standards are developed within an evidence-based best practice model
of service provision (48, 50, 60, 62, 67, 68).
Regardless of the process for development of service frameworks or standards identified, broad key
components for best practice service provision include an effective evaluation process and assessment
of hard to produce proof of the effectiveness of the program. In relation to maternal, child and family
health, programs must also be based on strong evidence and supported by accepted theories of
child/family health and development. It is also recommended that programs be replicable in that a
program is able to be implemented and provide consistent outcomes in varying locations and this is
only possible when the program has identified core components, values and service delivery models or
service standards. Other key components are that programs are innovative and have cultural reach
and are culturally competent (69).

Table 4: Matrix of key features or principles presented in Service Standards documents
Service Standard Document Title
Key features or principles presented as standards (shaded indicates present)
Relationship/
Partnerships
Participation Acces
s
Communication
/Collaboration
Cultural
relevance
Wellbeing System
processes (HR,
complaints)
Organisational
Management
Workforce/
Recruitment
Support Services Service Delivery
Standards (Dept. of Education and
Children’s Services South Australia)
(49)
Standards Evidence Guide
(Department of Human Services Victoria)
(59)
Guide to the National Quality
Standard (Australian Children's
Education & Care Quality Authority)
(60)
Maternal and Child Health Service
Program Standards (Department of
Education and Early Childhood
Development Victoria)
(50)
Service Delivery Standards:
Indigenous Justice Program (Attorney
General's Department)
(62)
National Standards for Disability
Services (New South Wales
Government Family and Community
Services)
(66)
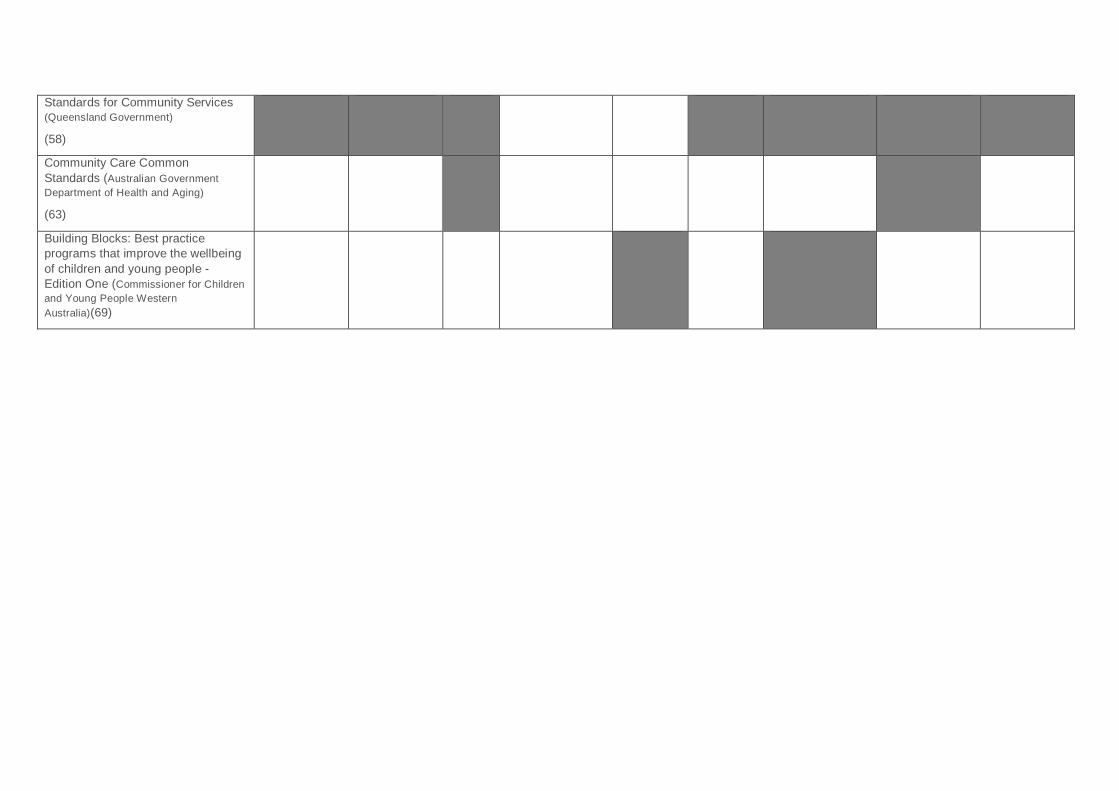
Standards for Community Services
(Queensland Government)
(58)
Community Care Common
Standards (Australian Government
Department of Health and Aging)
(63)
Building Blocks: Best practice
programs that improve the wellbeing
of children and young people -
Edition One (Commissioner for Children
and Young People Western
Australia)(69)
NSW Health 20
Other ways of describing key elements within standards
In addition to the standards identified in this systematic review, the search identified further literature
that related to service standard content but were not actual service standards. Again, due to a lack of
published literature specifically addressing Aboriginal early childhood health services the following
information is based on maternal and early weeks programs. A rapid review of the literature in relation
to maternity service requirements for Indigenous mothers and babies in Australia, Canada, New
Zealand and the United States of America by Kildea and Van Wagner (32) identified the key service
elements that could translate into service standards in a broad sense. The elements are:
governance and ownership;
having an identified philosophy and service characteristics;
provision of appropriate training and education; and,
monitoring and evaluation mechanisms.
The consultation paper on the proposed National Framework for Aboriginal and Torres Strait Islander
Child and Family Health Services (53) also includes key elements that services should incorporate and
these include:
being culturally competent and safe;
understanding and responding to community and population needs;
maximising service access; and,
collaboration, coordination and integration with relevant services.
This consultation paper relates specifically to Aboriginal and Torres Strait Islander child and family
health service provision and as such the suggested key elements should be utilised in both the
development of service standards and the provision of services for Aboriginal and Torres Strait Islander
families.
Developing and measuring service standards
Limited information is available for a best practice model in regard to developing service standards.
Swersey (57) advocates for a structured approach that involves defining quality, stakeholder
engagement, having specific standards that have indicators or measures. Other development
processes advocate a similar approach but include using a systematic approach and basing the
standards on current best practice (48, 51). The majority of service standards documents identify the
importance of being able to measure against the standards.
The NSW Disability Service Standards provide and recommend the use of key performance indicators
(KPI) drawn from the standards and have developed a KPI guidance document to support the service
standards (64). Using the KPIs is encouraged and it is claimed that this will assist organisations in
evaluating activities and outcomes. In addition, it is suggested that measuring activity against the KPIs
will allow organisations to identify service improvement opportunities (64). Other measures advocated
in the literature include the development of evidence-based quality indicators so that benchmarking of
services can occur (70). Stelfox and Straus (70) provide a framework for developing quality indicators
that is similar to frameworks for developing service standards. The framework suggests that quality
indicators should be important to the audience, scientifically sound, feasible and usable. They advocate
a consensus approach to the development of these indicators.
Policy and Regulation
Development and implementation of appropriate and workable service standards must incorporate
relevant policy and regulatory requirements. Policies that are applicable to the BSF service standards
development include the following three broad areas:
NSW Health 21
1. Maternal, child and family health
2. Aboriginal and Torres Strait Islander health
3. Community development to improve child health development and wellbeing.
Five main documents provided insight into policy and regulation areas with respect to service
standards. These included policy frameworks and targets. Policy is however referred to in many other
areas in a more general sense.
Policy frameworks
A national review of state and territory maternal and child health policies identified differences in policy
frameworks across jurisdictions in Australia (33). Although informed by national policies, each state and
territory have developed and refer to separate policy frameworks. Fortunately commonalities include
alignment with international research and policy directions; a focus on prevention and early
intervention; emphasis on continuity of care and collaboration; and, integrating of services (33). The
review also identified the inclusion of distinct statements in regard to the importance of delivering
culturally appropriate services for Aboriginal and Torres Strait Islander children and families and this
included the promotion of linkages with Aboriginal Community Controlled Health Organisations (33).
Setting targets in policy
The National Aboriginal Community Controlled Health Organisation (NACCHO) in their 10-point plan to
achieve a healthy future for generational change, advocate for governments and policy makers to adopt
the targets and actions in the 10-point plan. The Healthy Futures 2013-2030 10-Point Plan states that
healthy futures and generational change will be achieved through investing in the Aboriginal
Community Controlled health sector so that innovative models of primary health care can be delivered.
This will be driven by Aboriginal health leaders and partnerships with other health services, and also
through health system reform. These actions will be underpinned by appropriate health financing, well-
prepared health workforce, strong health infrastructure, rigorous research and data collection and
processes that are accountable and report, monitor and evaluate services (16).
Policy supporting child and family health in NSW
In NSW, there are a number of policies that support both the provision of child and family health and
the provision of health services for Aboriginal and Torres Strait Islander families. The NSW Aboriginal
Health Plan’s strategic directions are particularly important when considering service standards and
service provision. The strategic directions (71) are:
1. Building trust through partnerships
2. Implementing what works and building the evidence
3. Ensuring integrated planning and service delivery
4. Strengthening the Aboriginal workforce
5. Providing culturally safe work environments and health services
6. Strengthening performance monitoring, management and accountability.
In addition, the New South Wales Government Plan NSW 2021 includes a child wellbeing section that
primarily focuses on prevention and early intervention for child health services.
The NSW Government’s policy suite Supporting Families Early package includes policy in regard to the
provision of maternal and child primary health care services and the Safe Start strategic policy with a
focus on coordinated services for families with psychosocial risk likely to impact on their parenting. The
Supporting Families Early package also provides overarching strategies for service provision similar to
the NSW Aboriginal Health Plan in that they highlight planning and partnership, ensuring a skilled and
supported workforce and implementation as key strategies to ensure appropriate service provision (72).
NSW Health 22
Developing a fit-for-purpose workforce
A number of documents and reviews were examined to determine the most effective factors that
contribute to developing a fit-for-purpose workforce in relation to the provision of child and family health
services for Aboriginal children and their families; and, the most effective human resources processes
to support, develop and assess individual and team performance against service standards.
Developing, supporting and sustaining a fit-for-purpose workforce are integral to the effective delivery
of the BSF programs and therefore the standards must acknowledge and incorporate workforce
development (73).
Influences on the workforce
Patient (or more relevant in this context communities, families, children), practitioner (nurse, Aboriginal
Health Worker, doctor, allied health ), and institutional outcomes are affected by current work
environments (74). Work environment includes staffing, leadership and management, commitment to
professional development and quality care, and relationships between staff members (75). There is a
well-established link between satisfied nurses, satisfied patients, and better quality of care and the
work environment affects satisfaction and turnover, that is, the propensity to leave the workforce or
workplace (76-78). Turnover is expensive as recruitment and replacement is costly, as is up-skilling
and orientation of new staff and high turnover is related to burnout, poorer mental health outcomes and
an increased likelihood of medical error (79-82). Therefore, attracting and keeping the health workforce
is important, no matter what the specific context area.
A health workforce that can deliver culturally safe services
Cultural competence is a critical component of a fit-for-purpose workforce and high quality cultural
competence training is required (21, 54). Cultural competence is defined as having the capacity to work
effectively with people from diverse backgrounds and being respectful while also recognising how the
individual’s culture influences the care given or received (14) .
It is essential that non-Aboriginal health professionals are supported in gaining an understanding of
Aboriginal ‘women’s business’ (83). The NSW Aboriginal Health Plan 2013-2023 (3) highlights the need
to develop structures, policies and processes required for culturally safe work environments. Aboriginal
people continue to experience institutional and interpersonal racism and this is relevant for both staff
and clients.
Health Workforce Australia (HWA) (84) is developing a curriculum framework as a necessary step in
creating a health workforce better able to respond to the needs of Aboriginal and Torres Strait Islander
peoples and communities and deliver culturally safe services. This national Aboriginal and Torres Strait
Islander health curriculum framework was developed in recognition of a lack of culturally competent
skills across all health professions and that Aboriginal and Torres Strait Islander Peoples are more
likely to access care when there is respectful communication and understanding or acknowledgement
of culture. It is hoped that this curriculum framework will play an important role in the future in ensuring
that pre-registration education of professionals, including nurses, midwives and doctors, and will
develop a workforce that can more readily deliver culturally safe and respectful services from the
outset. As a result of the 2014-2015 Federal Government budget announcement Health Workforce
Australia’s program functions are to be transferred to the Commonwealth Department, Health
Workforce Division. Health Workforce Australia have informed all stakeholders that the Implementing
an Aboriginal and Torres Strait Islander Health Curriculum Project with the Curtin University project
team will continue until the end of the project with accountability to the Commonwealth Department,
Health Workforce Division (Personal Communication).
In addition to the proposed introduction of the HWA curriculum project, there are a number of other
resources available to assist in developing a culturally respectful and competent workforce. All New
South Wales Health employees are mandated to complete both online and face-to-face cultural respect
training through the completion of the cultural training framework Respecting the Difference (54).

NSW Health 23
A structured literature review on early childhood interventions for Indigenous families identified that
workforce development in Indigenous health programs must incorporate employment and building
capacity of local Indigenous people (21). This requires community leadership and endorsement and a
commitment to being strengths-based, not only for the clients but also for the workforce. An effective
workforce, whether Aboriginal or Non-Aboriginal, needs to depend on trust and relationship building.
Non-Aboriginal staff need particular attention to being the ‘right kind of person’, that is, being able to
work effectively in a cross-cultural, flexible and collaborative manner. Training and supportive
supervision needs to be built into a workforce development strategy to ensure that staff with these
qualities are recruited into the programs (21). A review undertaken to develop the framework for
Universal Child Health Services highlighted that attention is needed in initial and ongoing training,
cultural competencies, staff support and mentoring (13).
Capacity building of the workforce
Capacity building has been identified in a number of policy documents as being critical to the
development of the workforce, especially, the support of Aboriginal and Torres Strait Islander peoples.
In NSW, the Aboriginal Health Plan 2013-2023 (3) focuses on developing and nurturing the Aboriginal
health workforce, in particular the unique role of the AHW. The Plan includes a number of strategies to
improve recruitment, retention, education and training. These include Aboriginal health cadetships for
student nurses and midwives which are currently being evaluated.
Building capacity of an Aboriginal health workforce is one of the key outcomes of the Aboriginal
Workforce Strategic Framework. The key outcomes include increasing the Aboriginal workforce to 2.6%
of the health workforce by end 2015; having targeted positions and specifically designed recruitment
and retention processes; provision of strong leadership; supported access to continuing professional
development opportunities; strengthen Aboriginal workforce data collection; and, ensuring all NSW
Health staff complete the mandated Aboriginal Cultural Training (73).
In addition to strengthening and building capacity in the Aboriginal workforce, it is important to consider
actively building the capacity of non-Aboriginal staff who work in Aboriginal health. In part, this is
supported in the BSF programs by ensuring all Child and Family Health Nurses work in partnership with
Aboriginal Health Workers when working with families and in communities. As discussed previously this
also should include recruitment of the ‘right’ person for the position and ensure adequate mentorship
and training is available so staff can deliver culturally respectful, flexible and collaborative care (21). It
is believed that supporting all staff to improve understanding and develop respect for Aboriginal people,
families and communities will enable staff to form meaningful and respectful professional relationships
which in turn will improve health outcomes (54).
Clarity of roles, responsibilities and competencies
Clarity about the roles, responsibilities and competencies is required to ensure that services can
function efficiently and effectively (31, 85). This clarity will inform workforce and recruitment and
continuing professional development (85, 86).
According to the NSW Health Child and Family Health Nursing Professional Practice Framework 2011-
2016 a Child and Family Health Nurse (CFHN) works within a primary health care model in a variety of
settings and the foundation of their practice is working in partnership with parents (87). In addition to
documenting core skills and knowledge required for the profession the CFHN also define their scope of
practice under three areas of practice;
1. Infant child health surveillance and screening
2. Family assessment and surveillance for emotional health and wellbeing
3. Infant, child and family care
Child and Family Health Nurses’ practice is guided by the ANMC Competency Framework for
Registered Nurses and NSW CFHN Professional Practice Framework.
NSW Health 24
The Aboriginal Health Worker’s practice, in NSW is guided by the Definition of an Aboriginal Health
Worker Information Bulletin (88). There is recognition that there has been inconsistency in the definition
and understanding of the role of Aboriginal Health Workers both in NSW and nationally. Changes in
national regulation in regard to the advent of the Aboriginal and Torres Strait Islander Health
Practitioner Board of Australia and new National Skills Council qualification standards for Aboriginal
Health Workers has supported the need for clarity in defining the role and scope of practice of
Aboriginal Health Workers (89, 90). Although there is recognition of role diversity the following
characteristics were universally present in all Aboriginal Health Workers (91);
Aboriginal primary health care provision
Cultural security and safety
Health promotion
Local Community knowledge
Holistic health care approach
The recognition of an equal partnership between Aboriginal Health Workers and Child and Family
Health Nurses and respect for the skills, knowledge and attributes each partner brings to their role is
vital to ensure the BSF programs provide safe and effective care to Aboriginal children, families and
communities.
Clarity about roles and responsibilities assists effective team building which was critical to the success
of the AMIHS programs (85). This is also important for job satisfaction and retention. Workforce
strategies identified in relation to the AMIHS programs, especially to support retention, included;
adequate orientation to the program and the community
prompt and effective conflict resolution if this is required
effective management and leadership with clear lines of accountability, performance
management, clinical supervision and support for education and training
clear strategic direction
respectful relationships within the team, and
occupational autonomy and flexibility.
Conclusion
This integrative literature review will inform the development of the BSF Standards and workforce
strategy documents. The review has highlighted key components and principles that should be present
in service delivery and development of service standards for Aboriginal specific child and family health
programs. Service standards must be supported by policy direction and regulation and informed by
evidence and best practice principles.
Workforce development strategies and capacity building must ensure that those who work in programs
that provide services for Aboriginal children, families and communities can demonstrate cultural
competence relevant to the community they work with. Training and supervision needs to be provided
on an ongoing basis and those working in the programs benefit from high levels of occupational
autonomy and flexible work practices and service delivery.
NSW Health 25
References
1. National Aboriginal Community Controlled Health Organisation. Definitions: Aboriginal Health 2006 [cited 2014 27 March]. Available from: http://www.naccho.org.au/aboriginal-health/definitions/. 2. Aboriginal Health & Medical Research Council of New South Wales. Primary, Secondary and Tertiary Health Care Services to Aboriginal Communities: Core Functions of Primary Health Care in Aboriginal Community Controlled Health Services (ACCHS): AH&MRC Monograph Series. Strawberry Hills: Aboriginal Health & Medical Research Council of New South Wales, 1999. 3. Australian Government. National Aboriginal and Torres Strait Islander Health Plan 2013-2023. Canberra: Department of Health and Aging, 2013. 4. Sherwood J. Colonisation - It's bad for your health: The context of Aboriginal health. Contemporary Nurse: A Journal for the Australian Nursing Profession. 2013;46(1):28-40. 5. Geia L. A strengths based approach to Australian Aboriginal childrearing practices is the answer to better health outcomes in Aboriginal family and child health Collegian. 2011;18:99-100. 6. Australian Indigenous Health Infonet. What is the History of Closing the Gap Western Australia: Edith Cowan University; 2014 [cited 2014 6 May]. Available from: http://www.healthinfonet.ecu.edu.au/closing-the-gap/key-facts/what-is-the-history-of-closing-the-gap. 7. Council of Australian Governments (COAG). Closing the Gap in Indigenous Disadvantage Canberra: Council of Australian Governments; 2008 [cited 2014 6 May]. Available from: https://www.coag.gov.au/closing_the_gap_in_indigenous_disadvantage. 8. Australian Government. National Partnership Agreement between the Commonwealth of Australi and the State and Territory Governments regarding Indigenous Early Childhood Development. Canberra: Council of Australian Governments, 2008. 9. New South Wales Health. Supporting families early: SAFE START strategic policy. Sydney: New South Wales Department of Health, 2009. 10. New South Wales Department of Health. Workforce & Recruitment: Aboriginal Maternal and Infant Health Service. Sydney: New South Wales Department of Health, no date. 11. New South Wales Health. Service delivery model: Aboriginal Maternal and Infant Health Service. Sydney: New South Wales Health, no date. 12. Torraco R. Writing Integrative Literature Reviews: Guidelines and Examples. Human Resource Development Review. 2005;4(3):356-67. 13. Australian Health Ministers' Advisory Council. National Framework for Universal Child and Family Health Services. Canberra: Australian Government Department of Health and Aging, 2011. 14. Munro H. Effective early intervention strategies for Indigenous children and their families. Sydney: New South Wales Government Family and Community Services Research Centre, 2012. 15. Australian Health Ministers' Advisory Council. Aboriginal and Torres Strait Islander Health Performance Framework 2012 Report. Canberra: Australian Government Department of Health and Aging, 2012. 16. National Aboriginal Community Controlled Health Organisation. Investing in healthy futures for generational change. Unknown: National Aboriginal Community Controlled Health Organisation, 2013. 17. Commission on Social Determinants of Health (CSDH), editor Social determinants and Indigenous health: The International experience and its policy implications. International Symposium on the Social Determinants of Indigenous Health 2007; Adelaide, 29-30 April 2007: Commission on Social Determinants of Health (CSDH). 18. Australian Government Department of Health. Aboriginal and Torres Strait Islander Health: Australian Government Department of Health; 2013 [cited 2014 7 April]. Available from: https://www.health.gov.au/internet/main/publishing.nsf/Content/Aboriginal+and+Torres+Strait+Islander+Health-1lp. 19. Australian Government. Indigenous Early Childhood Development National Partnership Agreement: First annual report on health performance indicators. Canberra: Australian Institute of Health and Welfare, 2013.
NSW Health 26
20. Campbell D, Pyett P, McCarthy L. Community Development interventions to improve Aboriginal health: Building and evidence base. Health Sociology Review. 2007;16(3-4):304-14. 21. Bowes J, Grace R. Review of early childhood parenting, education and health intervention programs for Indigenous children and families in Australia. Canberra: Closing the Gap ClearingHouse, 2014. 22. University of Technology Sydney Faculty of Health. Heterogeneity of Indigenous Australians Sydney: Faculty of Health University of Technology Sydney; 2013. Available from: http://utsindigenoushealth.com/heterogeneity-of-indigenous-australians/. 23. KCB Australia for the Department of Health and Aging. National Framework for Aboriginal and Torres Strait Islander Child and Family Health Services: Policy and Program Context Scoping Paper. Orange: Department of Health and Aging, 2013. 24. 0u L, Garrett P, Hillman K. Ethnic and Indigenous access to early childhood healthcare services in Australia: parents' perceived unmet needs and related barriers. Australian & New Zealand Journal of Public Health.35(1):30-7. 25. Priest N, Mackean T, Waters E, Davis E, Riggs E. Indigenous child health research: a critical analysis of Australian studies. Australian And New Zealand Journal Of Public Health. 2009;33(1):55-63. 26. Geia LK, Hayes B, Usher K. Yarning/Aboriginal storytelling: Towards an understanding of an Indigenous perspective and its implications for research practice. Contemporary Nurse: A Journal for the Australian Nursing Profession. 2013;46(1):13-7. 27. Secretariat of National Aboriginal and Islander Child Care. Growing up our way: Aboriginal and Torres Strait Islander child rearing practices matrix. Melbourne: Secretariat of National Aboriginal and Islander Child Care,, 2011. 28. Geia L. First steps, making footprints: intergenerational Palm Island families' Indigenous stories (narratives) of childrearing practice strengths. Townsville: James Cook University; 2012. 29. Geia LK, Hayes B, Usher K. A strengths based approach to Australian Aboriginal childrearing practices is the answer to better outcomes in Aboriginal family and child health. Collegian (Royal College of Nursing, Australia). 2011;18(3):99-100. 30. Kildea S, Stapleton H, Murphy R, Low N, Gibbons K. The Murri clinic: a comparative retrospective study of an antenatal clinic developed for Aboriginal and Torres Strait Islander women. BMC Pregnancy and Childbirth. 2012;12:159. 31. Homer C, Foureur M, Allende T. Evaluation of the Malabar Community Midwifery link service. Sydney: accessUTS, 2009. 32. Kildea S, Van Wagner V. 'Birthing on Country' maternity service delivery models: a rapid review: an Evidence Check rapid review. Sax Institute on behalf of the Maternity Services Inter-Jurisdictional Committee for the Australian Health Ministers Advisory Council, 2012. 33. Schmied V, Donovan J, Kruske SUE, Kemp L, Homer C, Fowler C. Commonalities and challenges: A review of Australian state and territory maternity and child health policies. Contemporary Nurse: A Journal for the Australian Nursing Profession. 2011;40(1):106-17. 34. Murphy E, Best E. The Aboriginal Maternal Infant Health Service: A Decade of Achievement in the Health of Women and Babies in NSW. New South Wales Public Health Bulletin 2012;23(3-4):68-72. 35. Homer CSE, Foureur MJ, Allende T, Pekin F, Caplice S, Catling-Paull C. ‘It's more than just having a baby’ women's experiences of a maternity service for Australian Aboriginal and Torres Strait Islander families. Midwifery. 2012;28(4):e509-e15. 36. Tursan d’Espaignet E, Measey M, Carnegie M, Mackerras D. Monitoring the ‘Strong Women, Strong Babies, Strong Culture Program’: The first eight years. Journal of paediatrics and child health. 2003;39(9):668-72. 37. Panaretto KS, Mitchell MR, Anderson L, Larkins SL, Manessis V, Buettner PG, et al. Sustainable antenatal care services in an urban Indigenous community: the Townsville experience. Medical Journal of Australia. 2007;187(1):18.

NSW Health 27
38. Stamp GE, Champion S, Anderson G, Warren B, Stuart-Butler D, Doolan J, et al. Aboriginal maternal and infant care workers: partners in caring for Aboriginal mothers and babies. Rural and remote health. 2008;8(883):6-8. 39. Campbell S, Brown S. Maternity care with the Women's Business Service at the Mildura Aboriginal Health Service. Australian and New Zealand Journal of Public Health. 2004;28(4):376-82. 40. Gao Y, Gold L, Josif C, Bar-Zeev S, Steenkamp M, Barclay L, et al. A cost-consequences analysis of a Midwifery Group Practice for Aboriginal mothers and infants in the Top End of the Northern Territory, Australia. Midwifery. 2014;30(4):447-55. 41. Josif C, Barclay L, Bar-Zeev S, Kildea S, Brittin M. How participatory action research supported improvements to the postnatal discharge summary system used for remote dwelling Aboriginal mothers and infants in the Top End of Australia. Action Research. 2012;10(4):387-405. 42. Houd S, Qinuajuak J, Epoo B. The outcome of perinatal care in Inukjuak, Nunavik, Canada 1998-2002. International Journal of Circumpolar Health. 2004;63. 43. Van Wagner V, Epoo B, Nastapoka J, Harney E. Reclaiming Birth, Health, and Community: Midwifery in the Inuit Villages of Nunavik, Canada. The Journal of Midwifery & Women’s Health. 2007;52(4):384-91. 44. Wagner V, Osepchook C, Harney E, Crosbie C, Tulugak M. Remote Midwifery in Nunavik, Québec, Canada: Outcomes of Perinatal Care for the Inuulitsivik Health Centre, 2000-2007. Birth: Issues in Perinatal Care. 2012;39(3):230-7. 45. Tilson HH. Standards-A Model for the Nation. American Journal of Public Health. 1982. 46. Australian Government. National Health Performance Framework. Canberra: Australian Institute of Health and Welfare, 2009. 47. Nolte. E. International Benchmarking of Healthcare Quality: a review of the literature. Cambridge: RAND Corporation, 2010. 48. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. Sydney: Australian Commission on Safety and Quality in Health Care (ACSQHC), 2011. 49. Department of Education and Children's Services. Support Services Service Delivery Standards. South Australia: Department of Education and Children's Services, 2011. 50. Department of Education and Early Childhood Development. Maternal and Child Health Service: Maternal and Child Health Service Program Standards. Melbourne: Department of Education and Early Childhood Development, 2009. 51. Institute for Citizen Centred Service. Service Standards 2014 [cited 2014 27 March]. Available from: http://www.iccs-isac.org/?lang=en. 52. New South Wales Government Community Relations Commission. Multicultural planning: a resource for practitioners. Sydney South: New South Wales Government, No date. 53. KBC Australia for the Department of Health. National Framework for Aboriginal and Torres Strait Islander Child and Family Health Services: Consultation paper. Orange NSW: KBC Australia, 2013. 54. New South Wales Ministry of Health. Respecting the Difference: An Aboriginal Cultural Training Framework for NSW Health. Sydney: New South Wales Health Workforce Development and Innovation Branch, 2011. 55. Anderson IP, Anderson M, Smylie J. The national indigenous health performance measurement system. Australian Health Review. 2008;32(4):626-38. 56. Australian Government Department of Health and Aging. Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: Department of Health and Aging, 2011. 57. Swersey AJ. The Service Quality PLATFORM. Quality Progress. 2013;46(12):56-61. 58. Queensland Government. Standards for community services. Brisbane: Department of Communities, 2007. 59. Department of Human Services. Department of Human Services standards evidence guide. Victoria: Department of Human Services, 2011.

NSW Health 28
60. Australian Children's Education & Care Quality Authority. Guide to the National Quality Standard. Australian Children's Education & Care Quality Authority,, 2013. 61. National Standards for Disability Services. National Standards for Disability Services. Australa: National Standards for Disability Services, No Date. 62. Attorney General's Department. Service Delivery Standards: Indigenous Justice Program. Canberra: Indigenous Justice and Community Safety Branch, 2013. 63. Australian Government Department of Health and Aging. Community Care Common Standards. Australian Government Department of Health and Aging, 2010. 64. New South Wales Government. Key Performance Indicator (KPI) Guide, Measuring performance against the NSW Disability Services Standards. Sydney: Ageing, Disability and Home Care, Department of Family and Community Services NSW 2012. 65. Davies P, Wye L, Horrocks S, Salisbury C, Sharp D. Developing quality indicators for community services: the case of district nursing. Quality in Primary Care. 2011;19(3):155-66. 66. New South Wales Government Family and Community Services. National Standards for Disability Services. Sydney: New South Wales Government Family and Community Services 2012. 67. Aboriginal Health and Medical Research Council of New South Wales. A literature review about indicators and their uses. Sydney: Aboriginal Health and Medical Council, 2013. 68. New South Wales Government. Standards in action. Sydney: Ageing, Disability and Home Care, Department of Family and Community Services NSW, 2012. 69. Commissioner for Children and Young People Western Australia. Building Blocks: Best practice programs that improve the wellbeing of children and young people - Edition One. Subiaco: Commissioner for Children and Young People Western Australia, 2012. 70. Stelfox HT, Straus SE. Measuring quality of care: considering conceptual approaches to quality indicator development and evaluation. Journal of Clinical Epidemiology. 2013;66(12):1328-37. 71. New South Wales Ministry of Health. NSW Aboriginal Health Plan 2013-2023. Sydney: New South Wales Ministry of Health, 2013. 72. New South Wales Health. NSW Health/Families NSW Supporting Families Early Package: Maternal and Child Health Primary Health Care Policy. Sydney: New South Wales Health, 2009. 73. New South Wales Ministry of Health. Good Health - Great Jobs: Aboriginal Workforce Strategic Framework 2011-2015. Sydney: NSW Ministry of Health, 2013. 74. Kane R, Shamliyan T, Mueller C, Duval S, Wilt T. The association of registered nurse staffing levels and patient outcomes: Systematic review and meta-analysis. Medical Care. 2007;45(12):1195-204. 75. Schalk D, Bijl M, Halfens R, Hollands L, Cummings GG. Interventions aimed at improving the nursing work environment: a systematic review. Implementation Science. 2010;5(34):doi:10.1186/748-5908-5-34. 76. Duffield C, Roche M, O'Brien-Pallas L, Catling-Paull C, King M. Staff satisfaction and retention and the role of the Nursing Unit Manager. Collegian. 2009;16(1):11-7. 77. Duffield C, Roche M, O’Brien-Pallas L, Diers D, Aisbett C, King M, et al. Glueing It Together: Nurses, their Work Environment & Patient Safety. Sydney: Univeristy of Technology Sydney; 2007. 78. Duffield C, Roche M, Diers D, Catling-Paull C, Blay N. Staffing, skill mix and the model of care. Journal Of Clinical Nursing. 2010;19(15-16):2242-51. 79. Waldman J, Kelly F, Arora S, Smith H. The shocking cost of turnover in health care. Health Care Management Review. 2004;29(1):2-7. 80. O'Brien-Pallas L, Murphy G, Shamian J, Li X, Hayes L. Impact and determinates of nurse turnover: A pan-Canadian study. Journal of Nursing Management. 2010;18:1073-86. 81. O’Brien-Pallas L, Griffin P, Shamian J, Buchan J, Duffield C, Hughes F, et al. The Impact of Nurse Turnover on Patient, Nurse, and System Outcomes: A Pilot Study and Focus for a Multicenter International Study Policy, Politics & Nursing Practice. 2006;7(169 - 179). 82. Hayes LJ, O'Brien-Pallas L, Duffield C, Shamian J, Buchan J, Hughes F, et al. Nurse turnover: a literature review. International Journal of Nursing Studies 2006;43(2):237-63
NSW Health 29
83. Australian Health Ministers' Advisory Council. Clinical Practice Guidelines: Antenatal Care - Module One. Canberra: Australian Government Department of Health and Aging, 2012. 84. Health Workforce Australia. Implementing the Aboriginal and Torres Strait Islander health curriculum framework: Consultation paper. Adelaide: Health Workforce Australia, An Australian Government Initiative, 2014. 85. Homer C. AMIHS Workforce strategy. Sydney: accessUTS for Health Administration Cooperation NSW, 2008. 86. New South Wales Health. Aboriginal Family Health Workers - operational Guidelines. North Sydney: New South Wales Health, 2009. 87. New South Wales Department of Health. Child and Family Health Nursing Professional Practice Framework 2011-2016. Sydney: New South Wales Health, 2011. 88. New South Wales Ministry of Health. Definition of an Aboriginal Health Worker. Sydney: New South Wales Ministry of Health, 2014. 89. Australian Health Practitioners Regulation Authority. Aboriginal and Torres Strait Islander Health Practice Board: Australian Health Practitioners Regulation Authority; 2014 [cited 2014 18 July]. Available from: http://www.atsihealthpracticeboard.gov.au/. 90. Community Services and Health Industries Skills Council. Aboriginal and Torres Strait Islander Health Workers: Community Services and Health Industries Skills Council; 2013 [cited 2014 18 July]. Available from: http://www.cshisc.com.au/develop/training-packages/qualifications-under-review/aboriginal-torres-strait-islander-health-workers/. 91. Health Workforce Australia. Growing Our Future: Final Report of the Aboriginal and Torres Strait Islander Health Worker Project. Canberra: Health Workforce Australia, 2011.





























