Embed Size (px)
Citation preview

Development of the Improvement Sciences
Internationally and in Sweden… Opportunities and Challenges
A Swedish Duet by:Boel Andersson Gӓre, MD, PhD
Director, Futurum, Region Jönköping CountyProfessor, the Jönköping Academy for Improvement of
Health and WelfareJohan Thor, MD, MPH, PhD
Vinnvård Fellow of Improvement Science, The Jönköping Academy for Improvement of Health and Welfare

Development of the Improvement Sciences
Internationally and in Sweden… Opportunities and Challenges
A Swedish Duet by:Boel Andersson Gӓre, MD, PhD
Director, Futurum, Region Jönköping CountyProfessor, the Jönköping Academy for Improvement of
Health and WelfareJohan Thor, MD, MPH, PhD
Vinnvård Fellow of Improvement Science, The Jönköping Academy for Improvement of Health and Welfare

Marie Fredriksson & Per Gessle of Roxette
In this duet, we aim to: Frame the sciences of improvement in a wider context
Illustrate improvement science with examples from Sweden and our international partners
Highlight remaining questions worth pondering throughout the day (and beyond)

Framing the Science of Improvement
Improvement Knowledge
Improvement Science
Brent James, MD
Don Berwick, MD, MPP
Paul Batalden, MDMaureen Bisognano, RN
Linda Headrick, MD
W. Edwards DemingJoseph JuranWalter Shewhart
Florence Nightingale, RN
How do we best apply improvement knowledge? How does it work, and
how can we make it work better still?

Why Improvement Science?
Davidoff F, Batalden P. Toward stronger evidence on quality improvement. Draft publication guidelines: the beginning of a consensus project. Quality and Safety in Health Care. 2005;14(5):319‐25.
”In contrast to the integral role that publication plays in scientific discovery, publication in medical quality improvement has unfortunately had only a limited role to date. This lack of published reports has arguably deprived the healthcare system of rigorous scholarly evidence on improvement work and, hence, has slowed improvement of the improvement process.”
”Failure to publish improvement experiences, including negative results, slows the dissemination of known effective innovations and wastes the time, effort, and money that others spend independently rediscovering those same innovations—and making the same mistakes.”

“Improvement science is the useful knowledge for improving health care.”
A working definition:
The science of improving health care
Paul Batalden, 2013The Vin McLoughlin Symposium on the Epistemology of Improving Quality:http://ec2‐46‐51‐185‐22.eu‐west‐1.compute.amazonaws.com/areas‐of‐work/improvement‐science/the‐vin‐mcloughlin‐symposium‐on‐the‐epistemology‐of‐improving‐quality/
BMJ Quality & Safety – Supplement 2011‐04: ”Knowledge for Improvement” – Open access:http://qualitysafety.bmj.com/content/20/Suppl_1.toc

The Art and the Science
Improvement is ”a human and organizational accomplishment”.
Bate P, Mendel P, Robert G, et al. Organizing for quality: the improvement journeys of leading hospitals in Europe and the United States: Oxford ; New York: Radcliffe; 2008.

Improvement Science
Current healthcare with its
limitations
Future, much better,
healthcare
What happens in ”the black
box”?
In fact, “many quality improvement interventions are black boxes that are difficult to reproduce in new contexts. Improvement science now needs to start the difficult task of the systematic accumulation and synthesis of knowledge”.Marshall M, Pronovost P, Dixon‐Woods M. Promotion of improvement as a science. Lancet. 2013;381(9864):419‐21.

The purpose of Science?
• Truth?
• Understanding?
• Problem-solving?
Hasok ChangDepartment of History and
Philosophy of ScienceUniversity of Cambridge
ISDG 130607

To Shift Paradigms
”To proceed beyond limitations of a given level of knowledge, the researcher, as a rule, has to break down methodological taboos which condemn as ’unscientific’ or ’illogical’ the very methods or concepts which later on prove to be basic for the next major progress.”
Credit: Ann‐Christine Andersson
Kurt Lewin (1890‐1947), “the father of modern social psychology”.

Development of a Research Paradigm
Marshall M, Pronovost P, Dixon‐Woods M. Promotion of improvement as a science. Lancet. 2013;381(9864):419‐21.
“We believe that the science of improvement is in what Kuhn calls the pre‐paradigm phase of
the emergence of a new discipline, one of the
characteristics of which is the absence of an agreed definition”

Realist Evaluation of Improvement
Greenhalgh T, Humphrey C, Hughes J, et al. How do you modernize a health service? A realist evaluation of whole‐scale transformation in London. Milbank Q. 2009;87:391‐416.
“Realist evaluation can draw useful lessons about how particular preconditions make particular
outcomes more likely, even though it cannot produce predictive guidance
or a simple recipe for success”
Professor Trisha Greenhalgh

Engaged Scholarship
• The gap between theory and practice: a problem of knowledge production rather than of transfer
• Engaged scholarship, an approach to generating knowledge that advances both science and practice: “a participative form of research for obtaining the different perspectives of key stakeholders (researchers, users, clients, sponsors, and practitioners) in studying complex problems.”
Van de Ven, AH. Engaged scholarship: a guide for organizational and social research. Oxford; New York: Oxford University Press; 2007.

Map of Improvement Science Centres http://tinyurl.com/ISCworld
Improvement Science Environmental Scan
Commissioned by the Health Foundation Carried out by:
Ross Baker, Kaveh ShojaniaLisha Lo
Naomi FulopAngus Ramsay 82 Centers met critera

Core findings• Centres quite heterogeneous in focus & activities• Foci often linked to
– interests of lead faculty–patterns of funding from research councils and similar bodies
• Current funding sources are not secure for many centres, although some centres have prospered on large endowments

Contrasting Research ThemesUK centres– Evaluation– Innovation– Patient Safety– Measurement– Organization and
delivery of care– Public health– Implementation– Knowledge translation
North American centres– Informatics– Patient safety (broadly)– Medication safety– Safety in specific settings (e.g., primary
care)– Policy– Hospital-acquired infection prevention– Design– Measurement of outcomes,
performance, quality and safety– Team work and communications

Forskning för ständiga förbättringar i vård och omsorg
The Vinnvård Research ProgrammeVårdalstiftelsen, Vinnova, SALAR and the Ministry of Health and Social Affairs, 2008
Four major goals:
1. To increase the use of research‐based knowledge in health and social care (bridge research and practice).
2. To develop innovative ways of organizing work in health and social care
3. To stimulate the development of institutional learning structures with a focus on how to lead, manage and develop practices in health and social care organizations
4. To establish research regarding how to lead, manage and develop practices in health and social care organizations at Swedish universities
Improvement Science in Sweden

Doctoral theses in ImprovementScience in Sweden the last years
Some results from the Vinnvård program3 University centers > 30 PhD theses> 200 publicationsInternational collaboration8 fellows in improvement scienceArenas for learning, sharing and collaboration in practice and academiaNew programs in education

”Bridging the Gaps”A Vinnvård Program
What we do What we know
Deeper understanding of some perspectives of QI; Learning in the microsystem, team development in QI,
coaching, measurement, co-production, leadership, canwe show results?

Lesson Learned: Jönköping Academy
1. Start small with entreprenerial, boundary spanning, curious people from different scientic fields
2. Leadership engagement from both practice and academia, joined ownership, agree on values to be created
3. Infrastructure for close and continous contact betweenacademia, practice and patients/clients
4. Close link researchers, PhD program and education tobuild capacity and interest
5. Strategic networking, networkning, networkning…
ISDG, Andersson Gäre, 2013

Characteristics of Improvement Sciences Approaches/Designs/Methods
• Participative research; Action, Interactive… • ”Pragmatic worldview”• Dynamic, Iterative, cyclic, over time• Evaluation; Learning, Realistic, Developmental...• Multidiscliplinary• Multiprofessional• Case methodology• Mixed methods

A Model for Knowledge Creation through Interactive Research“Research With”
P-E Ellström, 2007
A research approach with a threefold task;
1. the scientific task
2. the practice‐oriented task
3. the educative task

Current Improvement ResearchWhile quality
measurement – e.g. through registries – is essential for guiding,
and evaluating, improvement efforts,
it does not automatically yield improvement. How can stakeholders get the most of out their measurements?
Anette Peterson aimed “to examine if and how Quality Improvement
Collaboratives (QICs), supported by quality registries, can contribute to
quality improvement in healthcare, and to examine how QICs differ between
different types of care.”
Apply quality improvement principles!

Acute care for myocardial infarction
– substantial improvement in process and outcomes.
Care for children and youth with diabetes;
included team coaches –improvement in HbA1c at all centers in Sweden.
Care for adults with diabetes – chronic care and life‐style change. Harder to achieve HbA1c‐improvement.
Improvement collaboratives can have different
impact depending on the kind of care
involved.
Peterson A. Learning and understanding for quality improvement under different conditions: An analysis of quality registry‐based collaboratives in acute and chronic care. [PhD Thesis] Jönköping: Jönköping University, School of Health and Welfare; 2015.
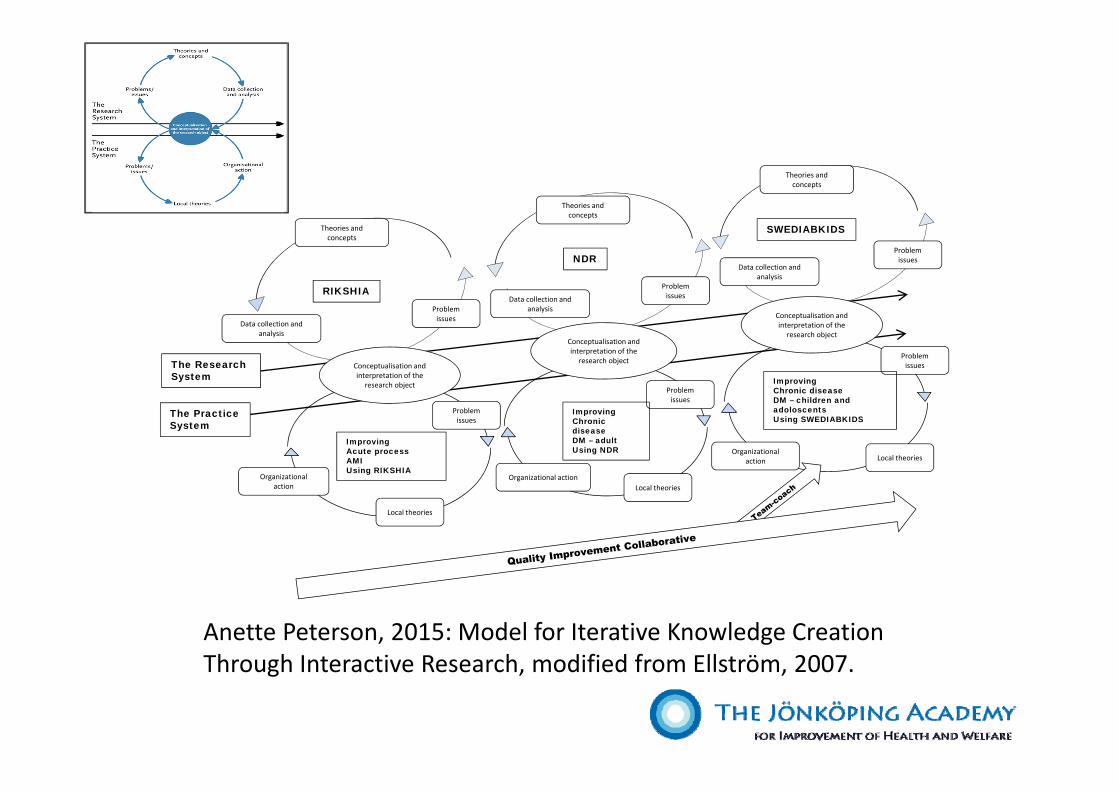
Anette Peterson, 2015: Model for Iterative Knowledge Creation Through Interactive Research, modified from Ellström, 2007.
Problem issues
Problem issues
Problem issues
Local theories
Local theories
Local theories
Organizationalaction
Organizational action
Organizationalaction
RIKSHIA
NDR
SWEDIABKIDS
ImprovingAcute process AMIUsing RIKSHIA
ImprovingChronicdiseaseDM – adultUsing NDR
ImprovingChronic diseaseDM – children and adoloscentsUsing SWEDIABKIDS
The Research System
The PracticeSystem
Theories and concepts
Problem issues
Data collection and analysis
Conceptualisation and interpretation of the
research object
Theories and concepts
Problem issuesData collection and
analysis
Theories and concepts
Problem issues
Data collection and analysis
Conceptualisation and interpretation of the
research object
Conceptualisation and interpretation of the
research object

Iterative Cycles of Learning
Generalizable scientific evidence or best practiceNational guidelines
Particular context Acute setting Primary care unit
Measured performance inRIKS‐HIANDRSWEDIABKIDS
Execution of planned changesPlans for change
Learning
Anette Peterson, Thesis 2015
Batalden PB,Davidoff F. What is "quality improvement" and how can it transform healthcare? Qual Saf Health Care. 2007;16:2‐3.

SQUIRE 2.0
SQUIRE stands for Standards for QUality Improvement Reporting Excellence. The SQUIRE guidelines provide a framework for reporting new knowledge about how to improve healthcare.
http://www.squire‐statement.org/
Distinctive consideration: Be explicit about BOTH how you acted to improve AND how you studied the
improvement efforts.

‘Doing’ an improvement project is fundamentally different from ‘studying’ it. The primary purpose of ‘doing’
improvement is to produce better local processes and outcomes rather than contribute to new generalisable knowledge. In contrast, the reason for ‘studying’ the intervention is mainly to contribute to the body of knowledge about the efficacy and generalisability of efforts for improving healthcare. Both ‘doing’ and
‘studying’ are required for a deep understanding of the nature and impact of the intervention(s) as well as the
possible underlying mechanisms.
Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus process. BMJ Qual Saf. 2015.
P
S D
A

The improvement project and the study of the project
IMPROVEMENT
PROJECT
Improvementleader/author
•planning•organizing
Patients•interviews•feedback
•touch points
Staff•interviews•feedback
•touch points
Co-designgroup•meeting
•touch points•planning
improvements
Co-designteam
•follow-upmeetings
Co-designteam
follow-upmeetings
Co-designgroup•reunion
•reporting•celebration
The
STUDY
ofthe
IMPROVEMENT
Experiencequestionnaires
Experiencequestionnaires
Experiencequestionnaires
Experiencequestionnaires
Experiencequestionnaires
Focus group interview
Concludingquestionnaire
Carolina Bergerum, 2012

A trap for many
• For people with a medical background, a common “trap” is to assume that the effectiveness of methods for improvement can be studied using the same principles as are used for clinical epidemiology.
• The answer, typically is: the evidence is mixed but shows that these methods CAN be applied successfully to yield measurable improvement of health and healthcare, but that their success is contingent on adaptation to a particular context. This is traditionally not welcome in the RCT paradigm, since “adaptation of the intervention” is contradictory of good research design and conduct.
“What is the evidence for the effectiveness of quality improvement?”

A trap for many
• For people with a medical background, a common “trap” is to assume that the effectiveness of methods for improvement can be studied using the same principles as are used for clinical epidemiology.
• The answer, typically, is: the evidence is mixed but shows that these methods CAN be applied successfully to yield measurable improvement of health and healthcare, but that their success is contingent on adaptation to a particular context. This is traditionally not welcome in the RCT paradigm, since “adaptation of the intervention” is contradictory of good research design and conduct.

The solution?
• Recognize that quality improvement, fundamentally, constitutes complex social change, when multiple human actors try to improve their work and their joint performance.
• Design research accordingly!Improvement is ”a human
and organizational accomplishment”.

What are we still trying to figure out?
• Turn to your neighbor and discuss: What brought you to this Symposium today?
• What are you curious about regarding the improvement of health and care?
• What do we need to understand better than we do today?
• How do we build, convey and apply the scientific basis for improvement?
Batalden PB, Cronenwett LR, Brown LL, et al. Collaboration in improving care for patients: how can we find out what we haven't been able to figure out yet? Jt Comm J Qual Improv. 1998;24:609‐18.





























