Embed Size (px)
Citation preview
.
1
Developmental
disturbances
Dr. Prajakta Barapatre
• Developmental disturbances- In the size of the TOOTH
• Developmental disturbances –In the shape of the TOOTH
• Developmental disturbances –In the number of the TOOTH
• Developmental disturbances- In the structure of the TOOTH
Developmental disturbances in size of teeth
1. Microdontia
2. Macrodontia
Microdontia:-This term is used to describe teeth which are
smaller than normal.
• Three types of microdontia are recognised1).True generalised microdontia
2).Relative generalised microdontia
3).Microdontia involving a single tooth
• True generalised microdontia:- In this all the teeth are
smaller than normal
Example:Pituatory dwarfism.This condition is extremely rare
• Relative generalised microdontia:- Normal or slightly
smaller than normal teeth are present. The jaws are some
what larger than normal and so it is an illusion of true
microdontia
• Microdontia involving only a single tooth:- It is rather
common condition and often affects maxillary lateral incisor
and third molar.
• One of the common forms is peg lateral,peg shaped OR
cone shaped crown with shorter root is noticed
• Macrodontia:-Teeth are larger than normal. It may be classified as
1. True generalised macrodontia
2. Relative generalised macrodontia
3. Macrodontia of single tooth
True generalised macrodontia:- Here all the teeth are larger than normal, has been associated with pituitory gigantism
Relative generalised macrodontia:-It is common and is a result of the presence of normal or slightly larger than normal teeth in small jaws.
Macrodontia of single tooth:-It is relatively un common. Tooth may appear normal in every respect except for its size. This sige should not be confused with the fusion of the teeth. It is occasionally seen in cases of hemi hyper trophy of the face
Developmental disturbances in shape of teeth
• Gemination
• Fusion
• Concrescence
• Dilaceration
• Taloncusp
• Dense in denty
• Dense Evaginatus
• Taurodontism
• Super numerary roots
.
2
Gemination:-
*Anomalie which arise from an attempt at division of a single tooth germ by an invagination with resultant incomplete formation of two teeth.
*Structure is usually is one with two completely or incompletely separated crowns that have a single root and root canal.
*Seen in Deciduos and permanent dentition
Fusion:-
*Anomalie arise through union of two normally separated tooth germs
*It has been thought that some physical force or pressure produces contact of the developing teeth and their subsequent fusion
*Fusion may also occur between a normal tooth and a supernumerary tooth
Clinical problems:-Appearance, spacing and periodontal conditions
Fusion
Concrescence:-
* It is actually a form of fusion which occurs after root formation has been completed
* In this condition the teeth are united by cementum only
* It could be a result of traumatic injury or crowding of teeth with resorption of inter dental bone
* Diagnosis is only by radiographs
Dialaceretion:-
* It refers to an angulation or a sharp bend or curve in the root or crown of a formed tooth.
* It could be due to trauma during the period in which the tooth is forming, with the result that the position of the calcified portion of the tooth is changed and the reminder of the tooth is formed at an angle
* This teeth frequently present a problem while extraction
Taloncusp:-
* Anomalous structure resembling an eagle’s talon,projects
lingually from the cingulum areas of a maxillary or
mandibular permanent incisor
* This cusp blends smoothly with the tooth except that there is
a deep developmental groove where the cusp blends with
the slopping lingual tooth surface
* composed of normal enamel dentin and a horn of pulp tissue
* It should be considered in terms of esthetics caries control,
Occulusal accomadation
* It appears to be more prevalent in person with Rubinsteni-
taybi syndrome
Densindente:-
* It is a result of invasination in the surface of the tooth crown before
calcification has occurred
* Maxillary lateral incisors are most frequently involved and condition is
frequently bilateral
Causes:-
1. Increased localised external pressure
2. Focal growth retardation
3. Focal growth stimulation in certain areas of tooth bud
Radiograpically it is recognised as a pear shaped invasination of enamel
and dentin with a narrow constriction at the opening on the surface of
the tooth and closely approximating the pulp in its depth
• Dense evaginatus (occlusal enamel pearl);- Developmental condition that appears clinically as an accessory cusp or globule of the enamel on the occlusal surface between the buccal and lingual cusps of pre molars unilaterally OR bilaterally
* It could be proliferation and evagination of an area of the inner enamel epithelium and subjacent odontogenic mesenchyme in to the dental organ during early tooth development
Taurodontism:-
* It is a peculiar anamoly in which the body of the tooth is enlarged at the expensive of roots
.
3
Causes include:
* When the mandelian recessive trait
* Atavastic feature
* Mutation resulting from odontoblastic deficiency during
dentinogenesis of the roots
Super numerary roots:-
* An additional root develops to the involved tooth
* Any tooth can exhibit these roots
Developmental disturbances in number of Teeth
1. Anodontia
2. Super numerary teeth
Anodontia:-Congenital absence of teeth
It is of TWO types
1.Total anodontia
2.Partial Anodontia
Total anodontia:-
All the teeth are missing,may involve both the deciduous and the permanent dentition .Example :Ectodermal Hypoplasia
Partial Anodontia:-
* Any tooth may be congenitally missing
* There is tendency for certain teeth to be missing more frequently than others being the mandible second premolar commonest
Super Numerary teeth:-
* The tooth may closely resemble the teeth of the group to which it belongs I.e Molars or pre molars or Anteriors
* Most common super numerary tooth are mesiodens followed by maxillary fourth molar
* Gardner’s syndrome consist of he multiple impacted super numerary teeth
Developmental disturbances in structure of
Teeth
1. Amelogenesis Imperfecta
2. Enamel Hypoplacia
3. Dentinogenesis imperecta
Amelogenesis Imperfecta:-
* Represents a group of hereditary defects of enamel un associated with any other generalised defects.
* It is an ectodermal diturbance classified in to
1) Hypo plastic
2) Hypo calcified
3) Hypo maturation
• Clinically the crowns of the teeth may or may not show discolouration
if present varies depending on the type of disorder, ranging from
Yellow to dark brown
• In some cases enamel may be totally absent r it may have chalky
texture or even a cheesy consistency or be relatively hard
• Sometimes the enamel is smooth or it may have numerous parallel
vertical wrinkles or grooves
• It may be chipped or show depressions in the base of which dentin
may be exposed
• Contact points between teeth are often open and occlusal surfaces
and incisal edges frequently abraded
Enamel Hypoplasia:-
* It is defined as a incomplete or defective formation of the organic matrix of teeth
* A number of different factors each capable of producing injury to the amiloblast may give rise to this condition.
Causes are:
-Nutitional deficiency (Vitamin A,D,C)
-Examthematous diseases (Measels,chicken fox,scarlet fever)
-Congenital syphilis
-Hypocalcemia
-Birth Injury,prematurity, RH Heamolytc disease
-Local Infection or Trauma
-Ingestion of chemical such as flouride
.
4
Radiographically:-
* The most striking feature is the partial or total precocious
* Obliteration of the pulp chamberand root cannals by continued formation of the dentin.
Chemical and physical features:-
• Chemical analysis shows that type-1 &2&3 increased water content as much as above while the inorganic content is less than that of normal dentin
• Dentin dysplasia(rootless teeth):- It is a rare disturbance of dentin formation characterized
• By normal enamel but atypical dentin formation with abnormal pulpal morphology.
• Transmitted as an autosomal dominant character.
Type-1(Radicular dysplasia):-
These teeth characteristically exhibit extreme mobility
&after only minor trauma as a result of their abnormally short roots.
Type-2(Coronal dysplasia) :-
-The permanent teeth how ever exhibit an abnormally
-Large pulp chamber in the coronal portion of the tooth often
described as THISTLE TUBE in shape.
Regionalodontoplasia
• They exhibit either delay or total failure in eruption.
• Show a marked reduction in radiodensity , so that the teeth assume a ghost appearance
Disturbances in the growth of the teeth:-
1. Premature eruption
2. Eruption sequestrum
3. Delayed eruption
4. Impacted teeth
5. Ankylosed teeth
1).Premature eruption:-
• Neonatal teeth are example for the premature eruption.
• The premature eruption of the permanent teeth is usually a sequelae of the loss of the deciduous teeth.
• This could be the possibility of the endocrine dysfunction.(hyperthyroidism)
2).Eruption sequestrum:-
-It is tiny irregular spicule of the bone overlying the crown of an erupting permanent molar found just prior to or immediately following the emergence of the tips of the cusps through the oral mucosa.
3).Delayed eruption:-
• Local factors: -Fibromatosis gingivae
• Systemic factors:-Rickets, cretinism,cleido cranial dysplasia
4).Impactedteeth:-
• Individual teeth which are unerupted usually because of lack of eruptive force.
Causes:-
• Lack of space
• Rotation of the tooth buds resulting in teeth which are aimed in the wrong direction
• Because their long axis is not parallel to a normal eruptive path.
5).Ankylosedteeth:-
• Most commonly mandibular second molars that have undergone
a variable degree of root resorption & then have become
ankylosed to the bone.
Causes:-
-Trauma,infection,disturbed local metabolism or a genetic influence
.
5
• Hypoplasia results only if the injury occurs during the time
the teeth developing or more specifically during the
formative stage of enamel development.Once the enamel is
calcified no such defects can be produced
E.H due to exanthmatous fever:-
• Pitting varilog and this pits tend to strain.The clinical
apearances of it mau be very unsightly.
• E.H due to congenitalsyphilis:-
-Involves the maxillary and mandibular permanent
incisors and the first molars
-The anterior teeth affected are called HUTCHINSONS TEETH
and molars are referred to as mulberry molars , moon’s
molars, fournier,s molars.
The anterior teeth will be screw driver shaped ,themesial and
distal surfaces of the crown tapering and converging towards
the cervical margin and it could be due the absence of cental
tubercle or calcification center.
-In the first molar crowns ,the enamel of the occlusal surfaces
and the occlusal third of the tooth appears to be arranged in
an agglomerate mass of the globules rather than in well
formed cusps.
The crown is narrower on the occlusal surfaces than at the
cervical margin.
E.H due to local infection or trauma
• It is occasionally seen,only a single tooth is involved ,most
commonly one of the permanent maxillary incissor or
maxillary or mandibular premolar.
• There may be any degree of hypoplasia ranging from the
mild brownish discoluration of the enamel to sever pitting or
irregularity of the tooth crown.
• This single tooth is called turners toothand the conditionis
called as Turners hypoplasia.
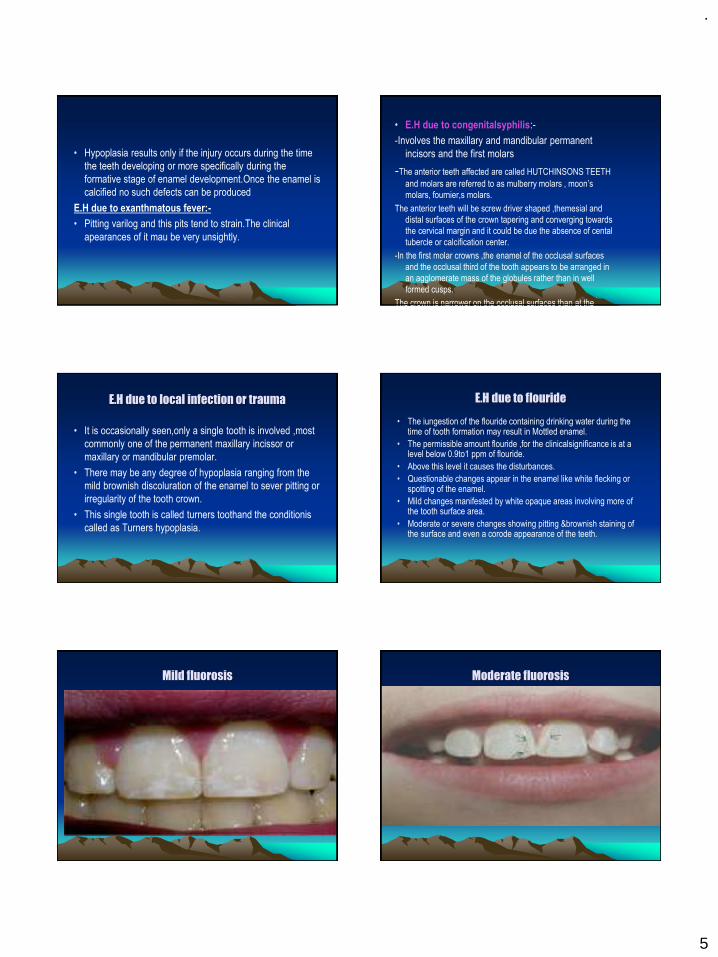
E.H due to flouride
• The iungestion of the flouride containing drinking water during the time of tooth formation may result in Mottled enamel.
• The permissible amount flouride ,for the clinicalsignificance is at a level below 0.9to1 ppm of flouride.
• Above this level it causes the disturbances.
• Questionable changes appear in the enamel like white flecking or spotting of the enamel.
• Mild changes manifested by white opaque areas involving more of the tooth surface area.
• Moderate or severe changes showing pitting &brownish staining of the surface and even a corode appearance of the teeth.
Mild fluorosis Moderate fluorosis
.
6
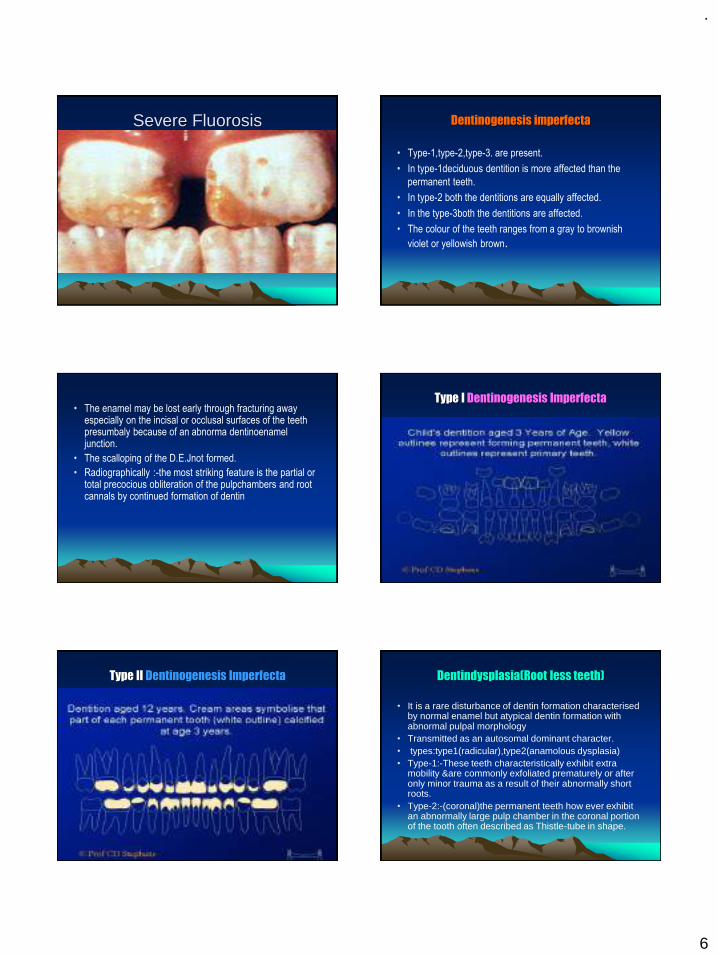
Severe Fluorosis Dentinogenesis imperfecta
• Type-1,type-2,type-3. are present.
• In type-1deciduous dentition is more affected than the
permanent teeth.
• In type-2 both the dentitions are equally affected.
• In the type-3both the dentitions are affected.
• The colour of the teeth ranges from a gray to brownish
violet or yellowish brown.
• The enamel may be lost early through fracturing away especially on the incisal or occlusal surfaces of the teeth presumbaly because of an abnorma dentinoenamel junction.
• The scalloping of the D.E.Jnot formed.
• Radiographically :-the most striking feature is the partial or total precocious obliteration of the pulpchambers and root cannals by continued formation of dentin
Type I Dentinogenesis Imperfecta
Type II Dentinogenesis Imperfecta Dentindysplasia(Root less teeth)
• It is a rare disturbance of dentin formation characterised by normal enamel but atypical dentin formation with abnormal pulpal morphology
• Transmitted as an autosomal dominant character.• types:type1(radicular),type2(anamolous dysplasia)• Type-1:-These teeth characteristically exhibit extra
mobility &are commonly exfoliated prematurely or after only minor trauma as a result of their abnormally short roots.
• Type-2:-(coronal)the permanent teeth how ever exhibit an abnormally large pulp chamber in the coronal portion of the tooth often described as Thistle-tube in shape.

.
7
Regional odontoplasia
• They exhibit either delay or a total failure in eruption.
• Radiographic features:-show a marked reduction in
radio density so that the teeth assume a Ghost
appearance.
Disturbances in the growth of the teeth
1. Premature eruption
2. Eruption sequestrum
3. Delayed eruption
4. Impacted teeth
5. Ankylosed teeth
• Premature eruption:-
• Neonatal teeth are example for the premature eruption.
• The premature eruption of the permanent teeth is usually a sequelae
of the loss of the deciduous teeth.
• This could be the possibility of the endocrine
dysfunction.(hyperthyroidism)
• Eruption sequestrum:-
• It is tiny irregular spicule of the bone overlying the crownof an
erupting permanent molar found just prior to or immediately following
the emergence of the tips of the cusps through the oral mucosa
Delayed eruption:-
Local factors: - Fibromatosis gingivae
Systemic factors:- Rickets, cretinism,cleido cranial dysplasia
Impacted teeth:-
• Individual teeth which are unerupted usually because of lack of eruptive force.
Causes:-
-Lack of space
-Rotation of the tooth buds resulting in teeth which are aimed in the wrong direction
-Because their long axis is not parallel to a normal eruptive path.
Ankylosedteeth:-
Most commonly mandibular second molars that have
undergone a variable degree of root resorption & then have
become ankylosed to the bone.
Causes:-
Trauma,infection,disturbed local metabolism or a genetic
influence
Thank you

.
1
DEVELOPMENT OF FACE, MAXILLA & MANDIBLE
Presented By :
Dr. Prajakta Barapatre
DEFINITIONS
GROWTHQuantitative aspect of biological development per unit of time
MoyersDEVELOPMENT
It refers to all the naturally occurring unidirectional changes in the life of an individual from its existence as a single cell to its elaboration as a multifunctional unit terminating in death
Moyers
DEFINITIONS
DIFFERENTIATION
It is the change from a generalized cell or
tissue to one that is more specialized. Thus
differ-entiation is the change in quality or
kind.
INTRODUCTION
◼ According to Todd, “ Growth is an increase
in size & Development is progress towards maturity
◼ Each process relies on the other, & under the influence of the morphogenetic pattern, the three-fold process works its miracles : self-multiplication, differentiation, organization –each according to its own kind.” The fourth
dimension is time
INTRODUCTION
◼ There is a 5000 fold increase in height during the prenatal period as compared to only a 3 fold increase during the entire postnatal period - Krogman
◼ The increase in weight according to Krogman, is 6.5 billion fold from ovum to birth & only 20 fold from birth to childhood. By the end of 4th month of life, birth weight is doubled
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES

.
2
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
Prenatal life is divided into three periods :
◼ The period of the ovum { from fertilization to the end of the 14th day }
◼ The period of the embryo { from 14th day to about the 56th day }
◼ The period of the fetus { from 56th day until the 270th day – birth }
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
◼ At about 21 days after conception, the developing brain & the pericardium form 2 prominent bulgings on the ventral aspect of the embryo after the formation of the head fold
◼ These bulgings are separated by the stomodeum (i.e comprising the 2 maxillary processes & the mandibular arch). The floor of the stomodeum is formed by the buccopharyngeal membrane, which separates it from the foregut
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
◼ The mesoderm covering the developing forebrain proliferates & forms a downward projection that overlaps the upper part of the stomodeum, this downward projection is known as the frontonasal process
◼ The pharyngeal arches are laid down in the lateral, & ventral wall of the cranial most part of the foregut that is in very close relationship to the stomodeum
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
◼ Between the 3rd & 8th weeks of intrauterine life a major part of the development of the face takes place
◼ The face is derived from the following structures that lie around the stomodeum
⚫ The Frontonasal Process
⚫ The 1st Pharyngeal (or Mandibular) arch of each side
◼ Each mandibular arch forms the lateral wall of the stomodeum, which gives of a bud from its dorsal end. It grows ventro-medially cranial to the main part of the arch which now is called the mandibular process
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
◼ During the 4th week, when the embryo is 5mm long, the ectoderm overlying the frontonasal process shows bilateral thickenings, a little above the stomodeum, these are called the nasal placodes
◼ These placodes sink below the surface to form nasal pits
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
◼ These pits are continuous below with the stomodeum
◼ The edges of each pit are raised above the surface, the medial raised edge is called the medial nasal process & the lateral edge is called the lateral nasal process
.
3
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PHARYNGEAL OR BRANCHIAL ARCHES
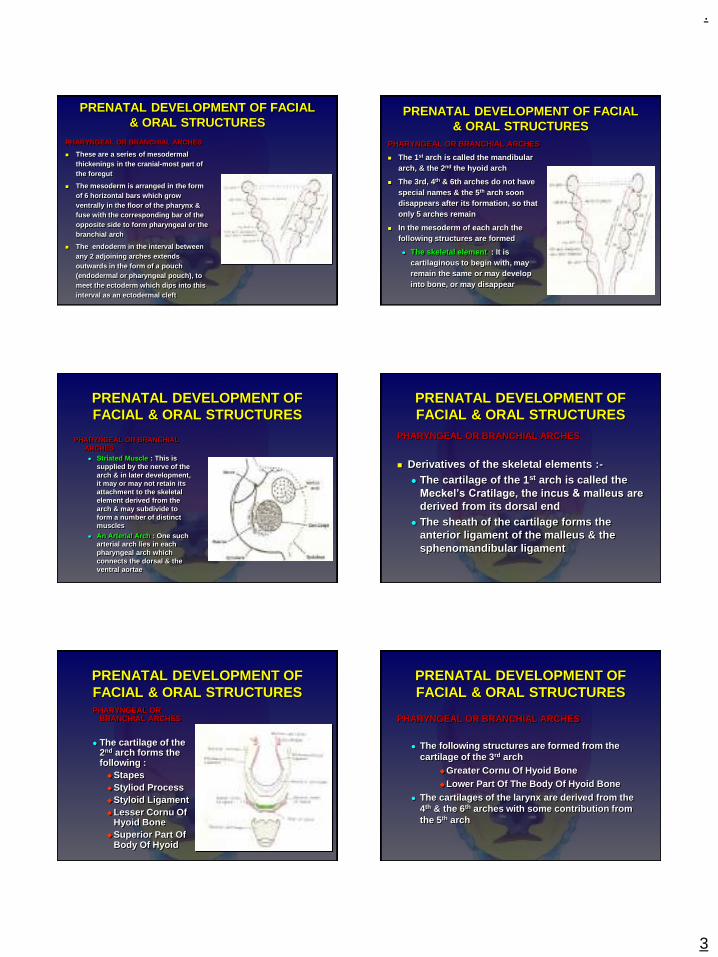
◼ These are a series of mesodermal thickenings in the cranial-most part of the foregut
◼ The mesoderm is arranged in the form of 6 horizontal bars which grow ventrally in the floor of the pharynx & fuse with the corresponding bar of the opposite side to form pharyngeal or the branchial arch
◼ The endoderm in the interval between any 2 adjoining arches extends outwards in the form of a pouch (endodermal or pharyngeal pouch), to meet the ectoderm which dips into this interval as an ectodermal cleft
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PHARYNGEAL OR BRANCHIAL ARCHES
◼ The 1st arch is called the mandibular arch, & the 2nd the hyoid arch
◼ The 3rd, 4th & 6th arches do not have special names & the 5th arch soon disappears after its formation, so that only 5 arches remain
◼ In the mesoderm of each arch the following structures are formed
⚫ The skeletal element : It is cartilaginous to begin with, may remain the same or may develop into bone, or may disappear
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PHARYNGEAL OR BRANCHIAL ARCHES⚫ Striated Muscle : This is
supplied by the nerve of the arch & in later development, it may or may not retain its attachment to the skeletal element derived from the arch & may subdivide to form a number of distinct muscles
⚫ An Arterial Arch : One such arterial arch lies in each pharyngeal arch which connects the dorsal & the ventral aortae
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PHARYNGEAL OR BRANCHIAL ARCHES
◼ Derivatives of the skeletal elements :-⚫ The cartilage of the 1st arch is called the
Meckel’s Cratilage, the incus & malleus are
derived from its dorsal end ⚫ The sheath of the cartilage forms the
anterior ligament of the malleus & the sphenomandibular ligament
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURESPHARYNGEAL OR
BRANCHIAL ARCHES
⚫ The cartilage of the 2nd arch forms the following :◆Stapes ◆Styliod Process◆Styloid Ligament◆Lesser Cornu Of
Hyoid Bone ◆Superior Part Of
Body Of Hyoid
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PHARYNGEAL OR BRANCHIAL ARCHES
⚫ The following structures are formed from the cartilage of the 3rd arch
◆Greater Cornu Of Hyoid Bone ◆Lower Part Of The Body Of Hyoid Bone
⚫ The cartilages of the larynx are derived from the 4th & the 6th arches with some contribution from the 5th arch
.
4
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
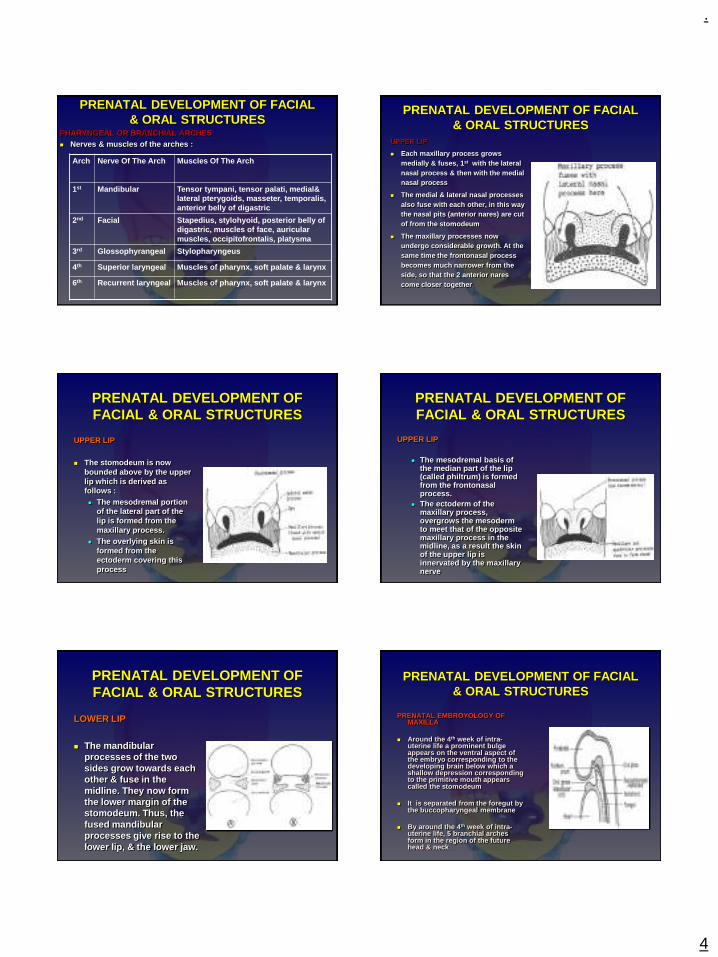
PHARYNGEAL OR BRANCHIAL ARCHES◼ Nerves & muscles of the arches :
Arch Nerve Of The Arch Muscles Of The Arch
1st Mandibular Tensor tympani, tensor palati, medial& lateral pterygoids, masseter, temporalis, anterior belly of digastric
2nd Facial Stapedius, stylohyoid, posterior belly of digastric, muscles of face, auricular muscles, occipitofrontalis, platysma
3rd Glossophyrangeal Stylopharyngeus
4th Superior laryngeal Muscles of pharynx, soft palate & larynx
6th Recurrent laryngeal Muscles of pharynx, soft palate & larynx
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
UPPER LIP
◼ Each maxillary process grows medially & fuses, 1st with the lateral nasal process & then with the medial nasal process
◼ The medial & lateral nasal processes also fuse with each other, in this way the nasal pits (anterior nares) are cut of from the stomodeum
◼ The maxillary processes now undergo considerable growth. At the same time the frontonasal process becomes much narrower from the side, so that the 2 anterior nares come closer together
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
UPPER LIP
◼ The stomodeum is now bounded above by the upper lip which is derived as follows :⚫ The mesodremal portion
of the lateral part of the lip is formed from the maxillary process.
⚫ The overlying skin is formed from the ectoderm covering this process
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
UPPER LIP
⚫ The mesodremal basis of the median part of the lip (called philtrum) is formed from the frontonasal process.
⚫ The ectoderm of the maxillary process, overgrows the mesoderm to meet that of the opposite maxillary process in the midline, as a result the skin of the upper lip is innervated by the maxillary nerve
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
LOWER LIP
◼ The mandibular processes of the two sides grow towards each other & fuse in the midline. They now form the lower margin of the stomodeum. Thus, the fused mandibular processes give rise to the lower lip, & the lower jaw.
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PRENATAL EMBROYOLOGY OF MAXILLA
◼ Around the 4th week of intra-uterine life a prominent bulge appears on the ventral aspect of the embryo corresponding to the developing brain below which a shallow depression corresponding to the primitive mouth appears called the stomodeum
◼ It is separated from the foregut by the buccopharyngeal membrane
◼ By around the 4th week of intra-uterine life, 5 branchial archesform in the region of the future head & neck

.
5
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PRENATAL EMBROYOLOGY OF MAXILLA
◼ The 1st branchial arch is called the mandibular arch –responsible for the development of the nasomaxillary region
◼ The mesoderm covering the developing forebrain proliferates to form the frontonasal process
◼ The stomodeum is overlapped superiorly by the frontonasal process & laterally by the mandibular arches of both the sides
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PRENATAL EMBROYOLOGY OF MAXILLA
◼ The ectoderm overlying the frontonasal process shows bilateral localized thickenings above the stomodeum called the nasal placodes, which soon sink to form the nasal pits
◼ The formation of nasal pits divides the frontonasal process into 2 parts :
⚫ The medial nasal process⚫ The lateral nasal process
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PRENATAL EMBROYOLOGY OF MAXILLA
◼ The mandibular arch gives off a bud from its dorsal end called the maxillary processwhich grows ventro-medio-cranial to the mandibular process
◼ At this stage the stomodeum is overlapped from above by the frontal process, below by the mandibular process & on either side by the maxillary process
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PRENATAL EMBROYOLOGY OF MAXILLA◼ The two mandibular processes grow medially & fuse
to form the lower lip & the lower jaw
◼ The maxillary process undergoes growth, the frontonasal process becomes narrower so that the 2 nasal pits come closer
◼ The line of fusion of the maxillary process & the medial nasal process corresponds to the nasolacrimal duct
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PALATE
◼ The palate is formed by the contributions of the :
⚫ Maxillary process⚫ Palatal shelves given off by the maxillary process⚫ Frontonasal process
The frontonasal process gives rise to the premaxillary regionwhile the palatal shelves form the rest of the palate
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PALATE
◼ Medial growth of the palatal shelves & their union is prevented by the presence of the tongue, thus the palatal shelves grow vertically downwards initially
◼ During the 7th week of intrauterine life, a transformation in the position of the palatal shelves occurs i.e from a vertical to a horizontal position
◼ The connective tissue of the palatal shelves intermingle with each other resulting in their fusion around the 8 ½ weeks of intra-uterine life

.
6
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PALATE
◼ The initial palatal contact occurs in the central region of the secondary palate posterior to the premaxilla
◼ The mesial edges of the palatal processes fuse with the free lower end of the nasal septum & thus separates the 2 nasal cavities from each other & the oral cavity
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
OSSIFICATION OF THE PALATE
◼ It occurs from the 8th week of intra-uterine life
◼ Its an intramembranous type of ossification
◼ The palate ossifies from a single centre derived from the maxilla
◼ The most posterior part of the palate does not ossify & forms the soft palate
◼ The mid-palatal suture ossifies by 12-14 years
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
TONGUE
◼ During the 5th week of embryonal life, rapidly proliferating mesenchymal swellings, covered with a layer of epithelium, appear on the internal aspect of the mandibular arch known as the lateral lingual swellings
◼ Between the swellings arises a small medial projection, the tuberculum impar
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
TONGUE
◼ Caudal to the tuberculum impar, the copula unites the 2nd & the 3rd branchial arches to form a mid central elevation extending backward to the epiglottis
◼ Mesodermal tissue from the 2nd, 3rd & 4th arches grow on either side of the copula & form the tongue structure
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
TONGUE
◼ The point at which the 2nd & 3rd branchial arches merge is marked by the foramen caecum just behind the sulcus terminalis, which marks a boundary between root of the tongue and its active portion.
◼ Mucosal sac or covering of the body of the tongue originates from 1st lateral lingual swelling of the mandibular arch.
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
TONGUE
◼ The papillae of the tongue are seen in the 11th weekof fetal age
◼ By 14 weeks the taste buds can be observed in the fungiform papillae, & they appear in circumvallate papillae at about 12 weeks
.
7
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
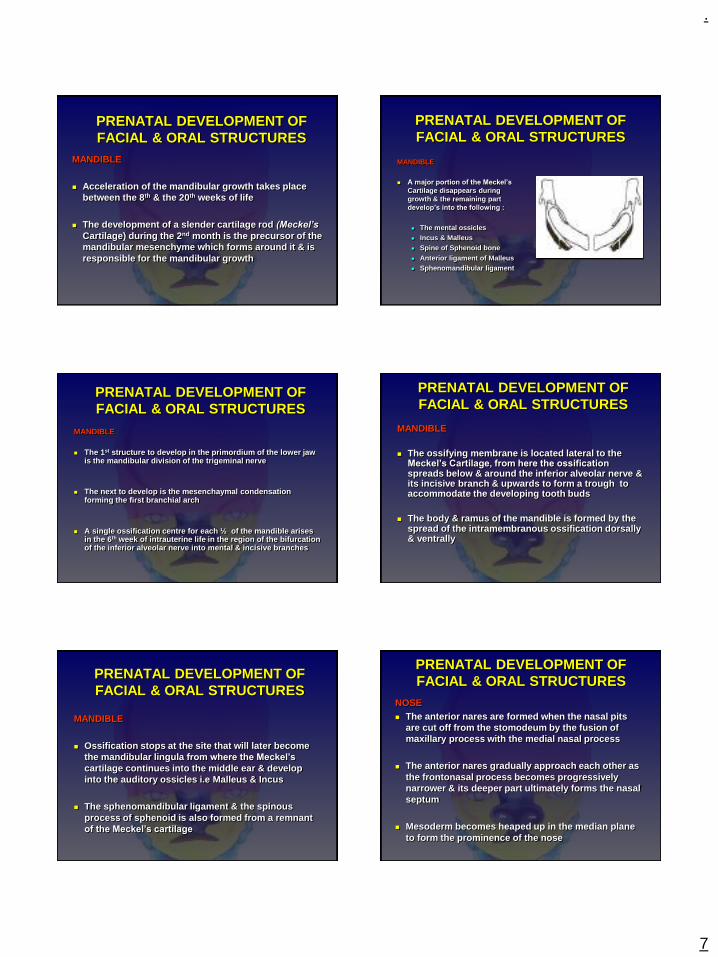
◼ Acceleration of the mandibular growth takes place between the 8th & the 20th weeks of life
◼ The development of a slender cartilage rod (Meckel’s
Cartilage) during the 2nd month is the precursor of the mandibular mesenchyme which forms around it & is responsible for the mandibular growth
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ A major portion of the Meckel’s
Cartilage disappears during growth & the remaining part develop’s into the following :
⚫ The mental ossicles⚫ Incus & Malleus⚫ Spine of Sphenoid bone⚫ Anterior ligament of Malleus⚫ Sphenomandibular ligament
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ The 1st structure to develop in the primordium of the lower jaw is the mandibular division of the trigeminal nerve
◼ The next to develop is the mesenchaymal condensation forming the first branchial arch
◼ A single ossification centre for each ½ of the mandible arises in the 6th week of intrauterine life in the region of the bifurcation of the inferior alveolar nerve into mental & incisive branches
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ The ossifying membrane is located lateral to the Meckel’s Cartilage, from here the ossification spreads below & around the inferior alveolar nerve & its incisive branch & upwards to form a trough to accommodate the developing tooth buds
◼ The body & ramus of the mandible is formed by the spread of the intramembranous ossification dorsally & ventrally
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ Ossification stops at the site that will later become the mandibular lingula from where the Meckel’s
cartilage continues into the middle ear & develop into the auditory ossicles i.e Malleus & Incus
◼ The sphenomandibular ligament & the spinous process of sphenoid is also formed from a remnant of the Meckel’s cartilage
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
NOSE◼ The anterior nares are formed when the nasal pits
are cut off from the stomodeum by the fusion of maxillary process with the medial nasal process
◼ The anterior nares gradually approach each other as the frontonasal process becomes progressively narrower & its deeper part ultimately forms the nasal septum
◼ Mesoderm becomes heaped up in the median plane to form the prominence of the nose
.
8
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
NOSE
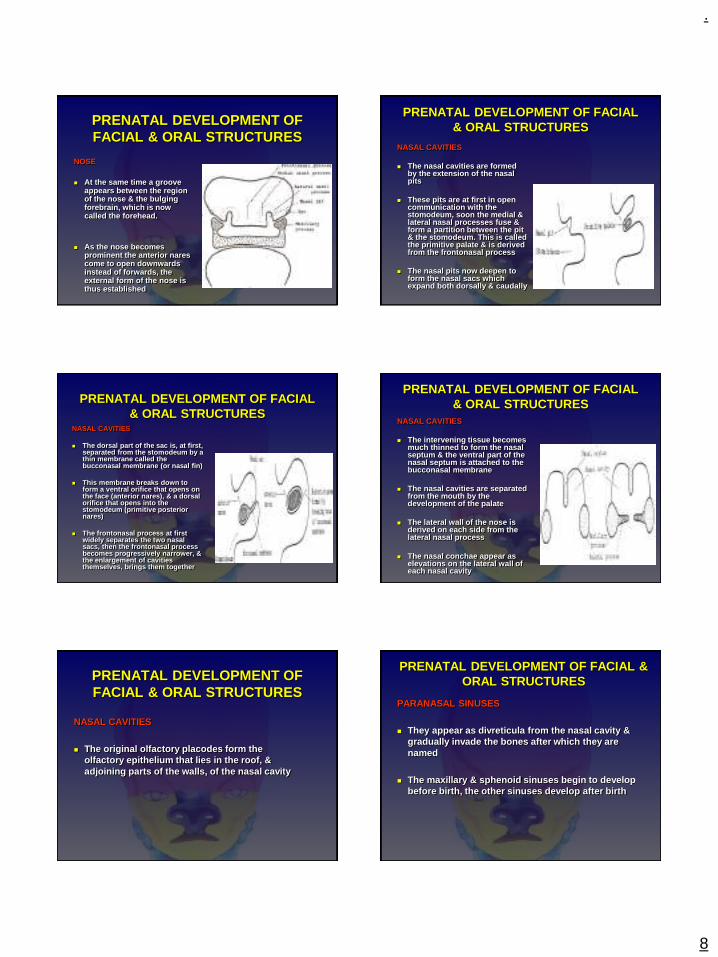
◼ At the same time a groove appears between the region of the nose & the bulging forebrain, which is now called the forehead.
◼ As the nose becomes prominent the anterior nares come to open downwards instead of forwards, the external form of the nose is thus established
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
NASAL CAVITIES
◼ The nasal cavities are formed by the extension of the nasal pits
◼ These pits are at first in open communication with the stomodeum, soon the medial & lateral nasal processes fuse & form a partition between the pit & the stomodeum. This is called the primitive palate & is derived from the frontonasal process
◼ The nasal pits now deepen to form the nasal sacs which expand both dorsally & caudally
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
NASAL CAVITIES
◼ The dorsal part of the sac is, at first, separated from the stomodeum by a thin membrane called the bucconasal membrane (or nasal fin)
◼ This membrane breaks down to form a ventral orifice that opens on the face (anterior nares), & a dorsal orifice that opens into the stomodeum (primitive posterior nares)
◼ The frontonasal process at first widely separates the two nasal sacs, then the frontonasal process becomes progressively narrower, & the enlargement of cavities themselves, brings them together
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
NASAL CAVITIES
◼ The intervening tissue becomes much thinned to form the nasal septum & the ventral part of the nasal septum is attached to the bucconasal membrane
◼ The nasal cavities are separated from the mouth by the development of the palate
◼ The lateral wall of the nose is derived on each side from the lateral nasal process
◼ The nasal conchae appear as elevations on the lateral wall of each nasal cavity
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
NASAL CAVITIES
◼ The original olfactory placodes form the olfactory epithelium that lies in the roof, & adjoining parts of the walls, of the nasal cavity
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
PARANASAL SINUSES
◼ They appear as divreticula from the nasal cavity & gradually invade the bones after which they are named
◼ The maxillary & sphenoid sinuses begin to develop before birth, the other sinuses develop after birth
.
9
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
CHEEKS
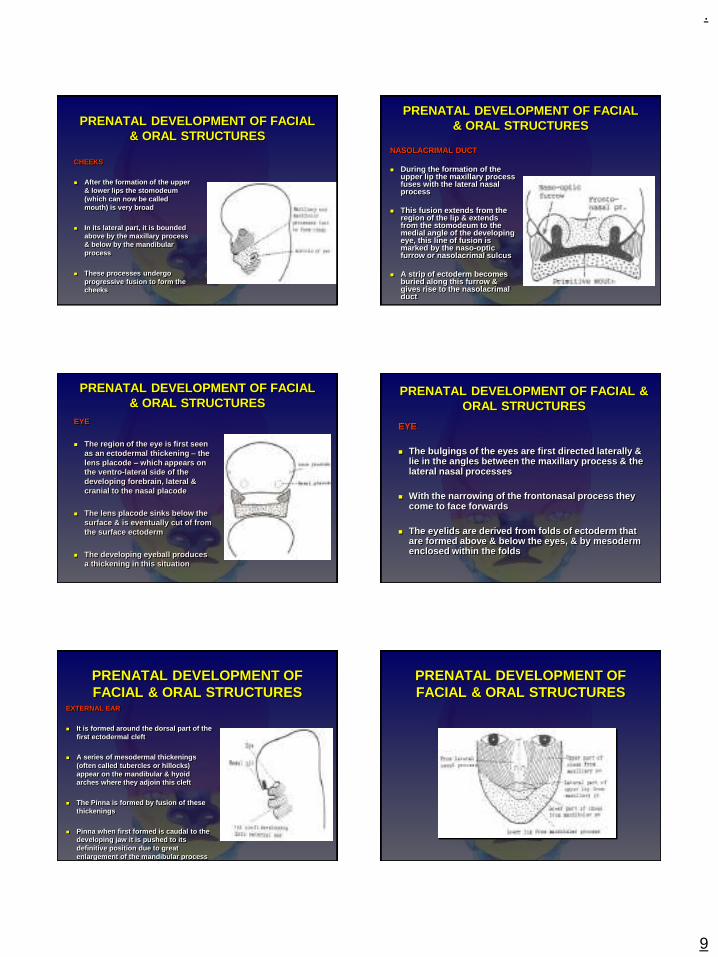
◼ After the formation of the upper & lower lips the stomodeum (which can now be called mouth) is very broad
◼ In its lateral part, it is bounded above by the maxillary process & below by the mandibular process
◼ These processes undergo progressive fusion to form the cheeks
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
NASOLACRIMAL DUCT
◼ During the formation of the upper lip the maxillary process fuses with the lateral nasal process
◼ This fusion extends from the region of the lip & extends from the stomodeum to the medial angle of the developing eye, this line of fusion is marked by the naso-optic furrow or nasolacrimal sulcus
◼ A strip of ectoderm becomes buried along this furrow & gives rise to the nasolacrimal duct
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
EYE
◼ The region of the eye is first seen as an ectodermal thickening – the lens placode – which appears on the ventro-lateral side of the developing forebrain, lateral & cranial to the nasal placode
◼ The lens placode sinks below the surface & is eventually cut of from the surface ectoderm
◼ The developing eyeball produces a thickening in this situation
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
EYE
◼ The bulgings of the eyes are first directed laterally & lie in the angles between the maxillary process & the lateral nasal processes
◼ With the narrowing of the frontonasal process they come to face forwards
◼ The eyelids are derived from folds of ectoderm that are formed above & below the eyes, & by mesoderm enclosed within the folds
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
EXTERNAL EAR
◼ It is formed around the dorsal part of the first ectodermal cleft
◼ A series of mesodermal thickenings (often called tubercles or hillocks)appear on the mandibular & hyoid arches where they adjoin this cleft
◼ The Pinna is formed by fusion of these thickenings
◼ Pinna when first formed is caudal to the developing jaw it is pushed to its definitive position due to great enlargement of the mandibular process
PRENATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES

.
10
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ The maxillary complex is attached to the cranial base, hence it influences the development of this region
◼ The growth of the maxilla is dependent on the sphenooccipital & sphenoethmoidal synchondroses
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ The growth of the nasomaxillary complex is produced by the following mechanisms
⚫ Displacement⚫ Growth at Sutures⚫ Surface Remodeling
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ Displacement
⚫ Growth of the cranial base leads to a passive or secondry displacement of the nasomaxillary complex in a downward & forward direction
⚫ As the middle cranial fossa grows it moves the nasomaxillary complex to a more anterior position
⚫ This passive displacement of maxilla is an important growth mechanism during the primary dentition years
⚫ Also, growth of the maxillary tuberosity results in a primary type of displacement in a forward direction, which is due to the enlargement of the bone itself
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ Growth At Sutures
⚫ The maxilla is connected to the carnium & cranial base by a number of sutures which include :
◆The fronto-nasal suture
◆The fronto-maxillary suture
◆The zygomatico-temporal suture
◆The zygomatico-maxillary sututre
◆The pterygo-palatine suture
.
11
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ Growth At Sutures
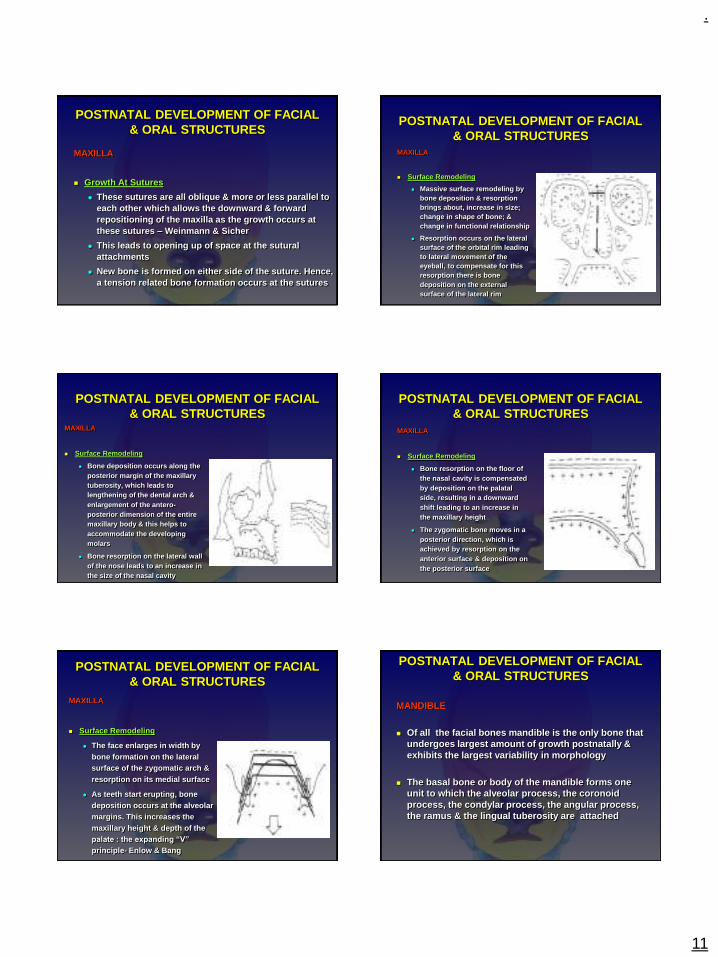
⚫ These sutures are all oblique & more or less parallel to each other which allows the downward & forward repositioning of the maxilla as the growth occurs at these sutures – Weinmann & Sicher
⚫ This leads to opening up of space at the sutural attachments
⚫ New bone is formed on either side of the suture. Hence, a tension related bone formation occurs at the sutures
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ Surface Remodeling
⚫ Massive surface remodeling by bone deposition & resorption brings about, increase in size; change in shape of bone; & change in functional relationship
⚫ Resorption occurs on the lateral surface of the orbital rim leading to lateral movement of the eyeball, to compensate for this resorption there is bone deposition on the external surface of the lateral rim
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ Surface Remodeling
⚫ Bone deposition occurs along the posterior margin of the maxillary tuberosity, which leads to lengthening of the dental arch & enlargement of the antero-posterior dimension of the entire maxillary body & this helps to accommodate the developing molars
⚫ Bone resorption on the lateral wall of the nose leads to an increase in the size of the nasal cavity
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ Surface Remodeling
⚫ Bone resorption on the floor of the nasal cavity is compensated by deposition on the palatal side, resulting in a downward shift leading to an increase in the maxillary height
⚫ The zygomatic bone moves in a posterior direction, which is achieved by resorption on the anterior surface & deposition on the posterior surface
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MAXILLA
◼ Surface Remodeling
⚫ The face enlarges in width by bone formation on the lateral surface of the zygomatic arch & resorption on its medial surface
⚫ As teeth start erupting, bone deposition occurs at the alveolar margins. This increases the maxillary height & depth of the palate : the expanding “V”
principle- Enlow & Bang
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ Of all the facial bones mandible is the only bone that undergoes largest amount of growth postnatally & exhibits the largest variability in morphology
◼ The basal bone or body of the mandible forms one unit to which the alveolar process, the coronoid process, the condylar process, the angular process, the ramus & the lingual tuberosity are attached
.
12
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ Ramus
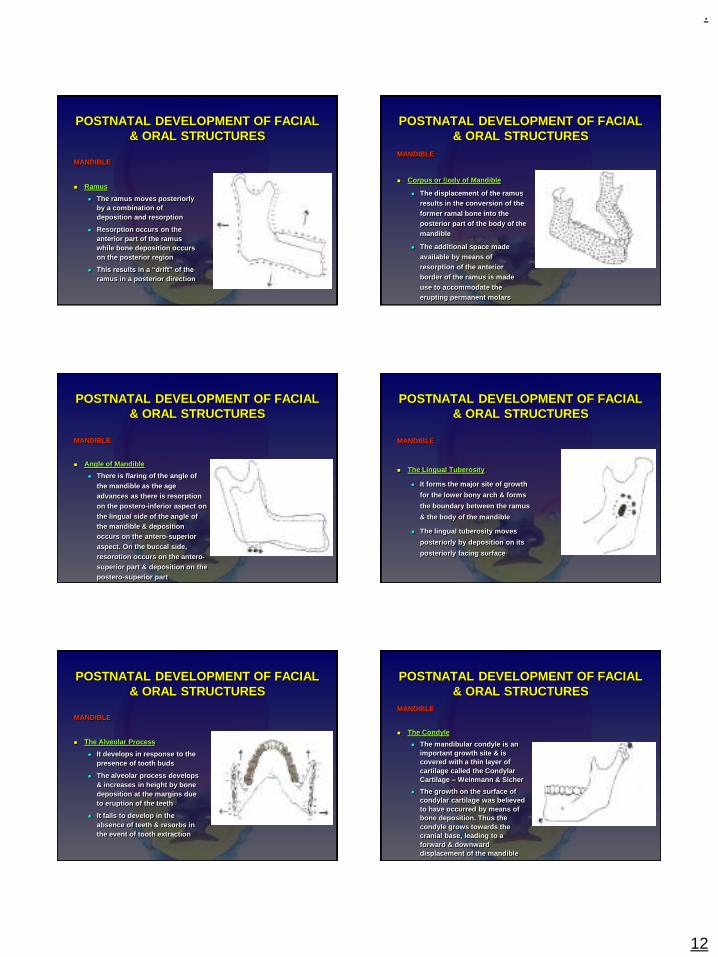
⚫ The ramus moves posteriorly by a combination of deposition and resorption
⚫ Resorption occurs on the anterior part of the ramus while bone deposition occurs on the posterior region
⚫ This results in a “drift” of the
ramus in a posterior direction
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ Corpus or Body of Mandible
⚫ The displacement of the ramus results in the conversion of the former ramal bone into the posterior part of the body of the mandible
⚫ The additional space made available by means of resorption of the anterior border of the ramus is made use to accommodate the erupting permanent molars
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ Angle of Mandible
⚫ There is flaring of the angle of the mandible as the age advances as there is resorption on the postero-inferior aspect on the lingual side of the angle of the mandible & deposition occurs on the antero-superior aspect. On the buccal side, resorotion occurs on the antero-superior part & deposition on the postero-superior part
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ The Lingual Tuberosity
⚫ It forms the major site of growth
for the lower bony arch & forms
the boundary between the ramus
& the body of the mandible
⚫ The lingual tuberosity moves
posteriorly by deposition on its
posteriorly facing surface
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ The Alveolar Process
⚫ It develops in response to the presence of tooth buds
⚫ The alveolar process develops & increases in height by bone deposition at the margins due to eruption of the teeth
⚫ It fails to develop in the absence of teeth & resorbs in the event of tooth extraction
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ The Condyle
⚫ The mandibular condyle is an important growth site & is covered with a thin layer of cartilage called the Condylar Cartilage – Weinmann & Sicher
⚫ The growth on the surface of condylar cartilage was believed to have occurred by means of bone deposition. Thus the condyle grows towards the cranial base, leading to a forward & downward displacement of the mandible
.
13
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ The Condyle
⚫ It is now believed that the growth of the soft tissues including the muscles & connective tissues caries the mandible forwards away from the cranial base
⚫ The growth rate increases at puberty reaching a peak between 12 ½ - 14 years & it ceases around 20 years of age
POSTNATAL DEVELOPMENT OF FACIAL & ORAL STRUCTURES
MANDIBLE
◼ The Coronoid Process
⚫ The growth here follows the enlarging “V” principle – Enlow & Bang
⚫ The depositon ocuurs on the lingual (medial) surface of the left & right coronoid process, there is an increase in the vertical dimension as well
⚫ The deposition on the lingual side of the coronoid process brings about a posterior growth movement in a “V”
pattern
THE HUMAN EMBRYOLOGY
REFRENCES
◼ Graber TM. Orthodontics principles & practice. 3rd ed. Philedelphia. W B Saunders Co. – 2001. p.1-128
◼ Profit WR. Contemporary orthodontics. 3rd
ed. Missouri. Mosby Inc – 2001 ◼ Arey LB. Develeopmental anatomy. 7th ed.
Philedelphia. WB Saunders Co.-1965◼ Orban B. Oral histology & embryology. 7th ed.
St. Louis. Mosby Inc – 1972
.
1
DIAGNOSIS AND
TREATMENT PLANING
DR PRAJAKTA BARAPATRE
CONTENTS
INTRODUCTION
HISTORY
EXAMINATION
DIAGNOSTIC IMPRESSIONS AND CASTS
DIFFERENTIAL DIAGNOSIS
TREATMENT PLANING
SUMMARY
INTRODUCTION
Diagnosis : The determination of the nature of a disease after thorough examination.
Diagnosis for prosthodontic care requires the use of general diagnostic skills & accumulated knowledge from other aspects of dentistry & its supporting science
Purpose of dental treatment:
a) To respond to a patient’s need
b) Relating the patient’s desires or wants to need
c) Developing a plan relevant to these wants & needs
d) Executing the treatment
HISTORY
A consistent, methodical approach
to examining patients is required
The general, medical and dental history is
obtained
GENERAL HISTORY
AGE :
Provides a reference for the physiological status of patient.
Neuromuscular skills diminishes with age and ability to adapt to new situations is decreased.
With age, oral epithelium becomes dehydrated and loses its elasticity resulting in decreased resistance to trauma.
Salivary flow decreases with age leading to greater risk of caries
GENERAL HISTORY
SEX:
In females, menopause may be associated with
hormonal imbalance which can cause osteoporosis
and atrophy of oral epithelium.
Pregnancy can have a bearing on the type of
prosthesis.
.
2
GENERAL HISTORY
OCCUPATION:
Interim and immediate partial denture may need to
be considered depending on the occupation
GENERAL HISTORY
MENTAL ATTITUDE:
Dr.MM House classification(1950)
He classified patient’s psychology into 4 types:
Philosophical (excellent prognosis)
Exacting (reluctant to dentists advice)
Hysterical (emotionally unstable with unrealistic
expectation)
Indifferent (uncooperative)
MEDICAL HISTORY
Systemic health and the drugs taken by patient may
affect removable partial denture treatment.
MEDICAL HISTORY (Systemic diseases)
DIABETES:
Uncontrolled diabetes is characterized by
xerostomia, which significantly reduces the ability of
patient to wear a prosthosis with comfort and
increases the possibility of caries.
MEDICAL HISTORY (Systemic diseases)
ARTHERITIS:
If arthritic changes occur in the TMJ, recording jaw
relation can be difficult and changes in the occlusion
may occur.
MEDICAL HISTORY (Systemic diseases)
ANEMIA:
These patients have a pale mucosa, sore tongue,
xerostomia, and gingival bleeding. Wearing a RPD
will be more difficult for them.
.
3
MEDICAL HISTORY (Systemic diseases)
EPILEPSY:
Any seizure may result in fracture and aspiration of the prosthesis, and possibly the loss of additional teeth.
All material used in the construction of a prosthesis must be radiopaque.
If the patient’s medication includes diphenlyhydantoin, one must take particular care not to irritate gingival tissue else hypertrophy may occur.
MEDICAL HISTORY (Systemic diseases)
CVS DISEASE:
Patients with the following symptoms require
medical approval before any dental procedures:
Acute myocardial infarction
Angina pectoris
Congestive heart failure
Uncontrolled hypertension
MEDICAL HISTORY (Systemic diseases)
CANCER:
Oral complications are also common side effects of
radiation and chemotherapy for malignancies.
The most common are mucosal irritation, xerostomia,
bacterial and fungal infection.
MEDICAL HISTORY (Systemic diseases)
TRANSMISSIBLE DISEASE:
Hepatitis, tuberculosis, influenza and other
transmissible disease pose a particular hazard for
the dentist, patients and auxiliaries by
contaminated aerosol.
MEDICAL HISTORY ( Drugs )
Some of the frequently prescribed drugs that can
affect prosthodontic treatment.
ANTICOAGULANTS:
Post surgical bleeding could be a problem for
patients receiving anticoagulants who undergo
extraction or soft tissue surgery.
MEDICAL HISTORY ( Drugs )
ANTIHYPERTENSIVE AGENTS:
The most significant side effect of the
antihypertensive drug is postural hypotension, which
may result in syncope when the patient suddenly
assume the upright position.
Therefore care must be taken when the patient gets
up from the dental chair
.
4
MEDICAL HISTORY ( Drugs )
ENDOCRINE THERAPY:
Patient receiving endocrine therapy may develop
an extremely sore mouth. If the patient is wearing a
prosthesis, it could incorrectly be blamed for causing
the discomfort.
MEDICAL HISTORY ( Drugs )
SALIVA INHIBITING DRUGS:
Atropine and their derivatives are sometimes used
to control excessive salivary secretion, particularly
when it is necessary to make accurate impression.
The are generally contraindicated for use in patient
with cardiac disease.
DENTAL HISTORY
Dental history provides the following information:
Reason for tooth loss
Details of previous prosthesis
Patient expectation
EXAMINATION
ORAL EXAMINATION
RADIOGRAPHIC EXAMINATION
ORAL EXAMINATION
Preliminary oral examination :
This is performed in the first appointment. It helps
determine the need for management of acute
condition and whether a prophylaxis is required to
conduct a thorough oral examination.
ORAL EXAMINATION
Definitive oral examination
This is performed in the second appointment with
the aid of radiographs and mounted diagnostic
casts. The following should be clinically evaluated :-
CARIES EVALUATION:
The remaining natural teeth are evaluated for
presence of any caries and restored teeth for signs
of decalcification or recurrent caries.
.
5
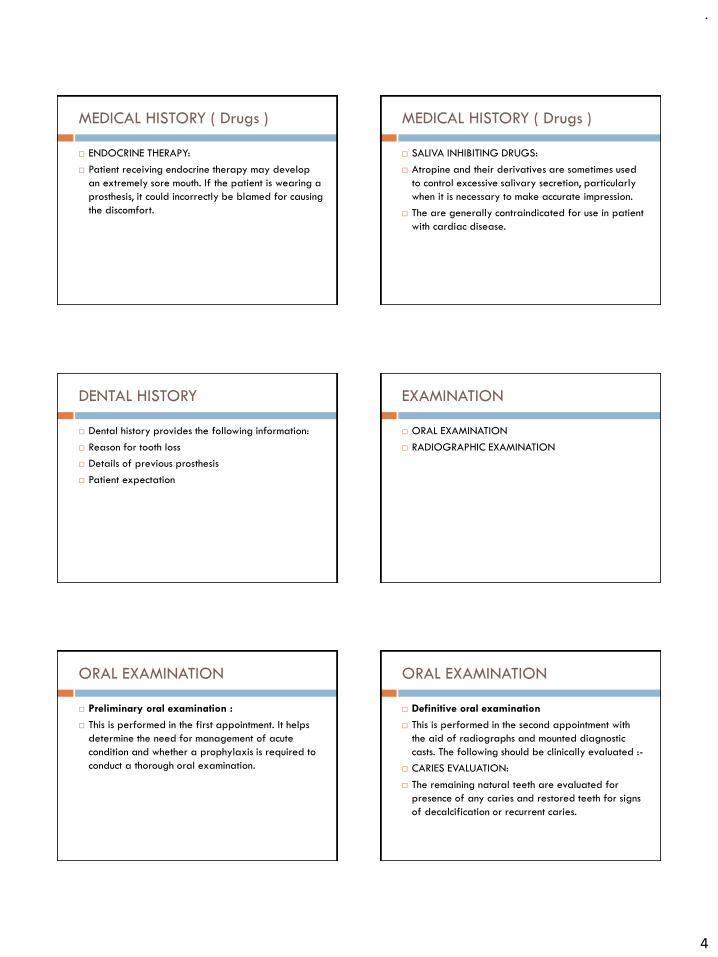
ORAL EXAMINATION
Definitive oral examination
PERIODONTAL EVALUATION:
To assess pocket depths, attachment levels, furcation
involvement, and tooth mobility.
Mobility may be due to trauma from occlusion,
periodontitis and loss of support. Mobility due to
trauma from occlusion can be reversed if the
occlusion is corrected.
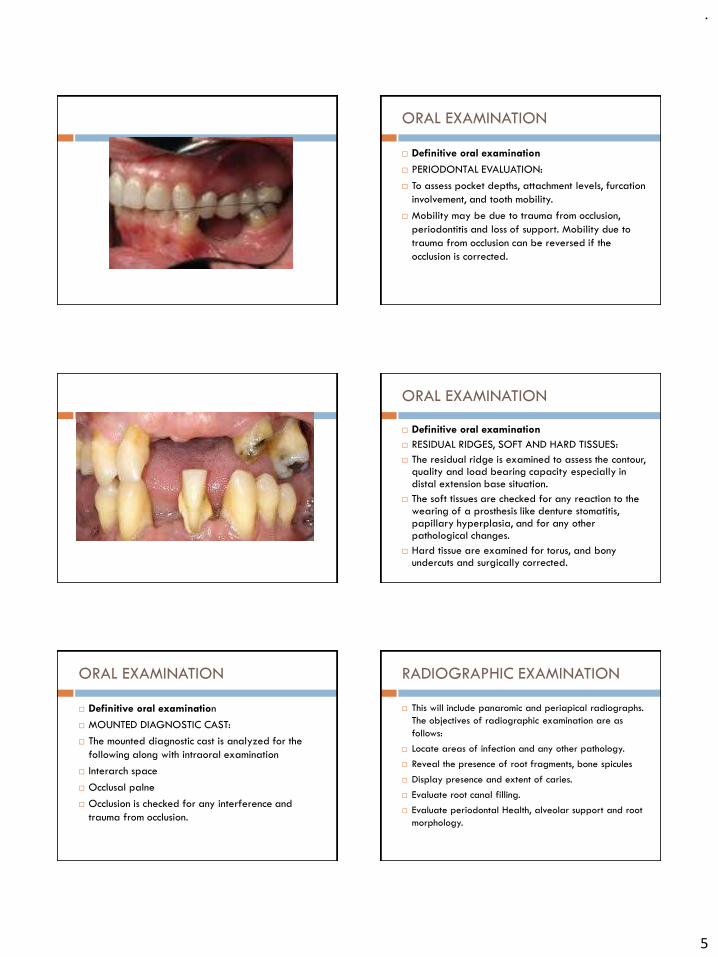
ORAL EXAMINATION
Definitive oral examination
RESIDUAL RIDGES, SOFT AND HARD TISSUES:
The residual ridge is examined to assess the contour, quality and load bearing capacity especially in distal extension base situation.
The soft tissues are checked for any reaction to the wearing of a prosthesis like denture stomatitis, papillary hyperplasia, and for any other pathological changes.
Hard tissue are examined for torus, and bony undercuts and surgically corrected.
ORAL EXAMINATION
Definitive oral examination
MOUNTED DIAGNOSTIC CAST:
The mounted diagnostic cast is analyzed for the
following along with intraoral examination
Interarch space
Occlusal palne
Occlusion is checked for any interference and
trauma from occlusion.
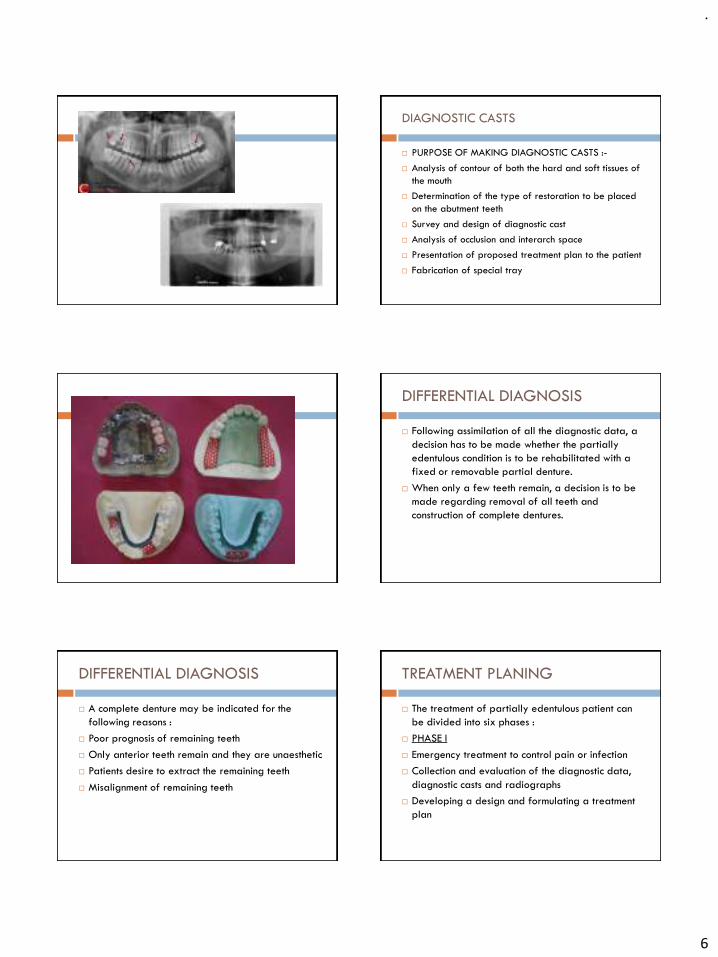
RADIOGRAPHIC EXAMINATION
This will include panaromic and periapical radiographs.
The objectives of radiographic examination are as
follows:
Locate areas of infection and any other pathology.
Reveal the presence of root fragments, bone spicules
Display presence and extent of caries.
Evaluate root canal filling.
Evaluate periodontal Health, alveolar support and root
morphology.
.
6
DIAGNOSTIC CASTS
PURPOSE OF MAKING DIAGNOSTIC CASTS :-
Analysis of contour of both the hard and soft tissues of
the mouth
Determination of the type of restoration to be placed
on the abutment teeth
Survey and design of diagnostic cast
Analysis of occlusion and interarch space
Presentation of proposed treatment plan to the patient
Fabrication of special tray
DIFFERENTIAL DIAGNOSIS
Following assimilation of all the diagnostic data, a
decision has to be made whether the partially
edentulous condition is to be rehabilitated with a
fixed or removable partial denture.
When only a few teeth remain, a decision is to be
made regarding removal of all teeth and
construction of complete dentures.
DIFFERENTIAL DIAGNOSIS
A complete denture may be indicated for the
following reasons :
Poor prognosis of remaining teeth
Only anterior teeth remain and they are unaesthetic
Patients desire to extract the remaining teeth
Misalignment of remaining teeth
TREATMENT PLANING
The treatment of partially edentulous patient can
be divided into six phases :
PHASE I
Emergency treatment to control pain or infection
Collection and evaluation of the diagnostic data,
diagnostic casts and radiographs
Developing a design and formulating a treatment
plan

.
7
TREATMENT PLANING
PHASE II
Preparation of mouth
PHASE III
Preparation of abutment teeth
Final impression and fabrication of master cast
TREATMENT PLANING
PHASE IV
Fabrication of removable partial denture
PHASE V
Denture insertion
Post insertion instructions
TREATMENT PLANING
PHASE VI
Maintenance and recall
Patient education and motivation is a very important
part of treatment planning and should be included in
every phase
SUMMARY
The actual construction of the removable partial
denture is only the last of many complex
procedures, all requiring the dentist to have
knowledge and skill in almost every phase of dental
practice.
Many failure in RPD can be traced to an
inadequate diagnosis leading to an inappropriate
or incomplete treatment plan.
SUMMARY
Hence the time spent on patient interview to record
history, ascertaining patient psychology and
expectation and collecting the diagnostic data, is
invaluable and forms the most important phase in
the construction of a removable partial denture.
.
1
DISTAL EXTENSION REMOVABLE
PARTIAL DENTURE PROSTHESIS.
DR PRAJAKTA BARAPATRE
CONTENTS:
➢Introduction
➢Movements of a distal extension Rpd
➢Nature of load acting in distal extension partial denture
➢Treatment of distal extension partial denture
➢Altered cast impression procedure
➢Review of literature
➢Summary and Conclusion
➢References
INTRODUCTION
A removable partial denture prosthesis as its name
implies is a prosthodontic restoration that supplies teeth
and its associated structures to a partial edentulous arch
and can be removed and inserted by the patient.
Removable partial dentures can be classified
according to the support they derive from the remaining
dentition and associated soft tissues.
Many RPD’s derive all their support from the
remaining natural teeth and are referred to as tooth-
borne RPD’s.
RPD’s that derive their support from both the
teeth and associated residual ridge tissues are termed as
tooth-tissue borne RPD’s or distal extension RPD’
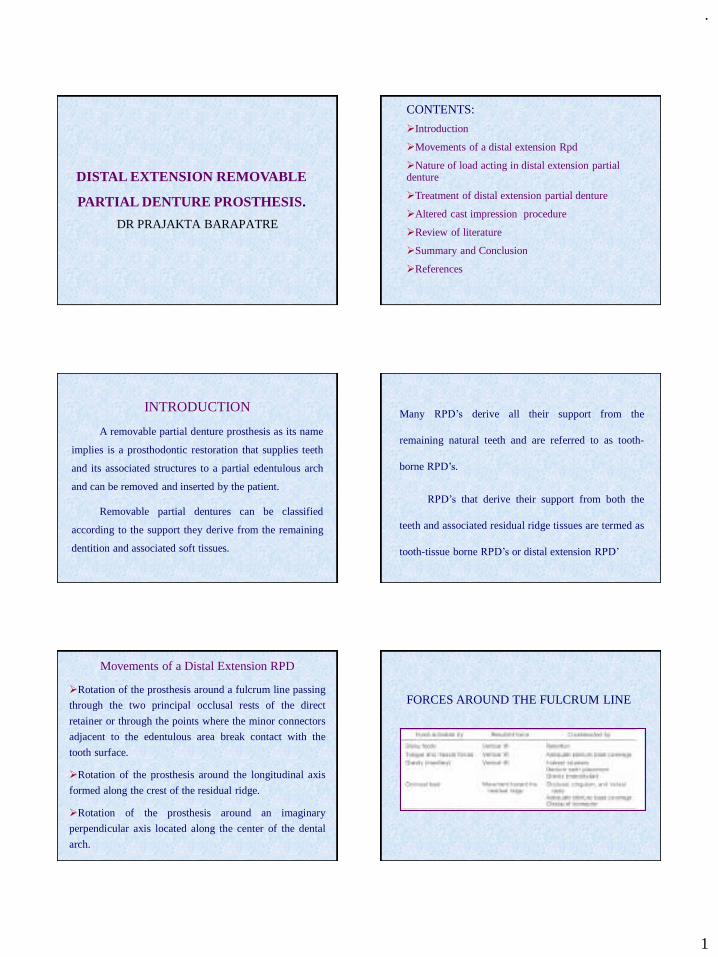
Movements of a Distal Extension RPD
➢Rotation of the prosthesis around a fulcrum line passing
through the two principal occlusal rests of the direct
retainer or through the points where the minor connectors
adjacent to the edentulous area break contact with the
tooth surface.
➢Rotation of the prosthesis around the longitudinal axis
formed along the crest of the residual ridge.
➢Rotation of the prosthesis around an imaginary
perpendicular axis located along the center of the dental
arch.
FORCES AROUND THE FULCRUM LINE
.
2
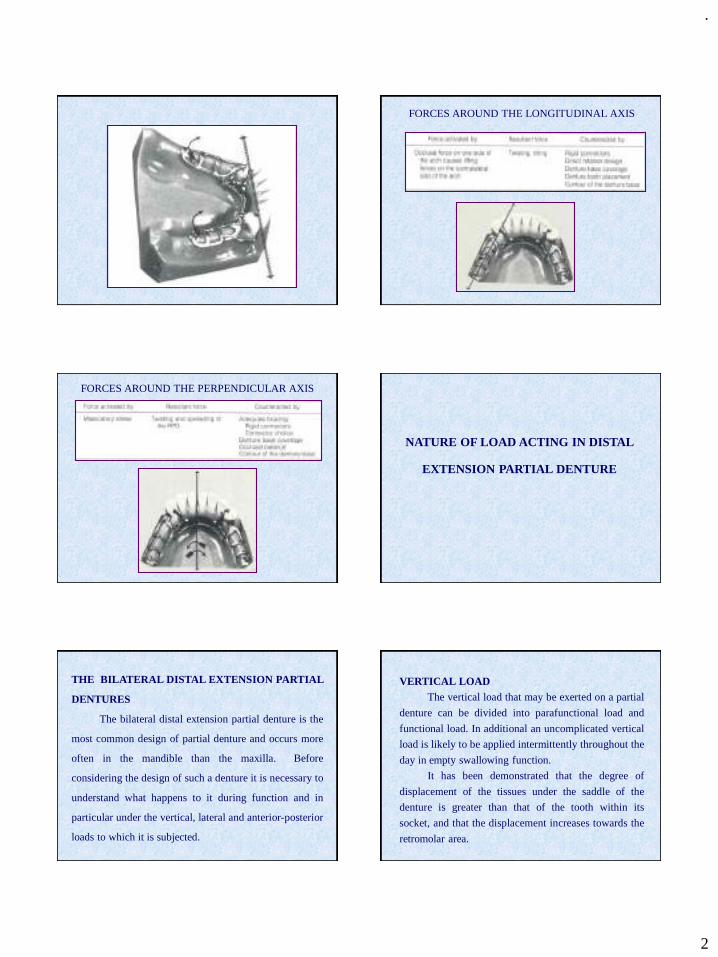
FORCES AROUND THE LONGITUDINAL AXIS
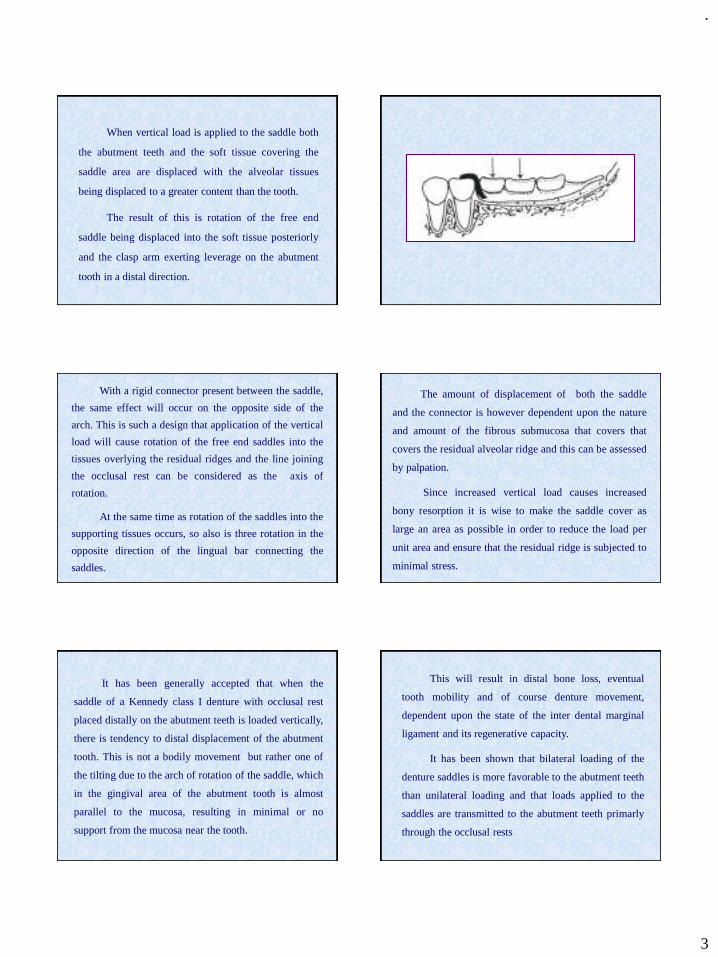
FORCES AROUND THE PERPENDICULAR AXIS
NATURE OF LOAD ACTING IN DISTAL
EXTENSION PARTIAL DENTURE
THE BILATERAL DISTAL EXTENSION PARTIAL
DENTURES
The bilateral distal extension partial denture is the
most common design of partial denture and occurs more
often in the mandible than the maxilla. Before
considering the design of such a denture it is necessary to
understand what happens to it during function and in
particular under the vertical, lateral and anterior-posterior
loads to which it is subjected.
VERTICAL LOADThe vertical load that may be exerted on a partial
denture can be divided into parafunctional load and
functional load. In additional an uncomplicated vertical
load is likely to be applied intermittently throughout the
day in empty swallowing function.
It has been demonstrated that the degree of
displacement of the tissues under the saddle of the
denture is greater than that of the tooth within its
socket, and that the displacement increases towards the
retromolar area.
.
3
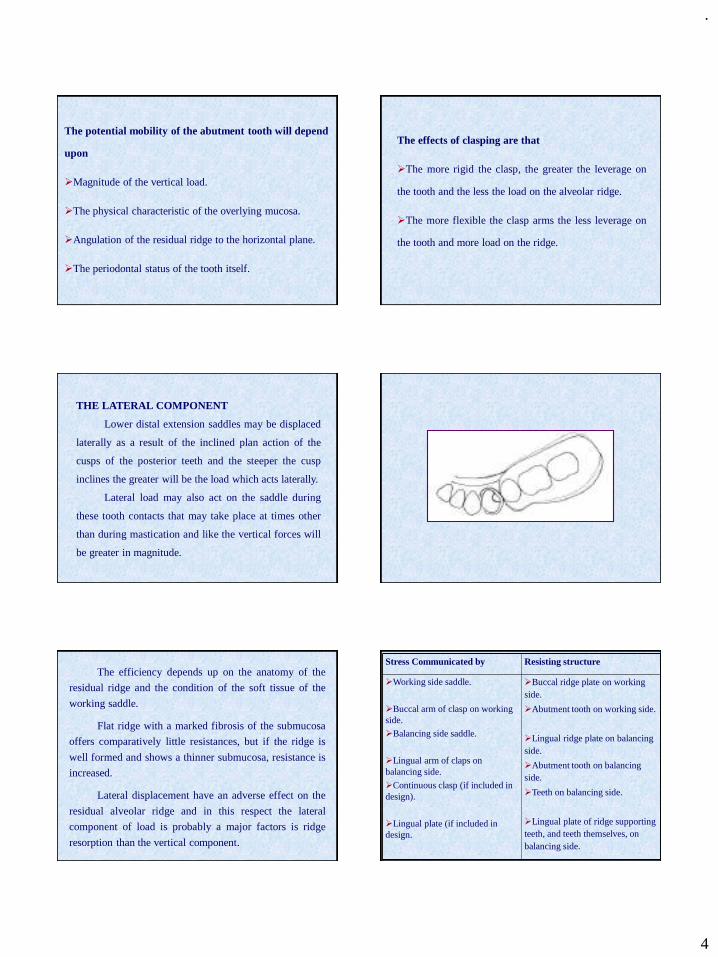
When vertical load is applied to the saddle both
the abutment teeth and the soft tissue covering the
saddle area are displaced with the alveolar tissues
being displaced to a greater content than the tooth.
The result of this is rotation of the free end
saddle being displaced into the soft tissue posteriorly
and the clasp arm exerting leverage on the abutment
tooth in a distal direction.
With a rigid connector present between the saddle,
the same effect will occur on the opposite side of the
arch. This is such a design that application of the vertical
load will cause rotation of the free end saddles into the
tissues overlying the residual ridges and the line joining
the occlusal rest can be considered as the axis of
rotation.
At the same time as rotation of the saddles into the
supporting tissues occurs, so also is three rotation in the
opposite direction of the lingual bar connecting the
saddles.
The amount of displacement of both the saddle
and the connector is however dependent upon the nature
and amount of the fibrous submucosa that covers that
covers the residual alveolar ridge and this can be assessed
by palpation.
Since increased vertical load causes increased
bony resorption it is wise to make the saddle cover as
large an area as possible in order to reduce the load per
unit area and ensure that the residual ridge is subjected to
minimal stress.
It has been generally accepted that when the
saddle of a Kennedy class I denture with occlusal rest
placed distally on the abutment teeth is loaded vertically,
there is tendency to distal displacement of the abutment
tooth. This is not a bodily movement but rather one of
the tilting due to the arch of rotation of the saddle, which
in the gingival area of the abutment tooth is almost
parallel to the mucosa, resulting in minimal or no
support from the mucosa near the tooth.
This will result in distal bone loss, eventual
tooth mobility and of course denture movement,
dependent upon the state of the inter dental marginal
ligament and its regenerative capacity.
It has been shown that bilateral loading of the
denture saddles is more favorable to the abutment teeth
than unilateral loading and that loads applied to the
saddles are transmitted to the abutment teeth primarly
through the occlusal rests
.
4
The potential mobility of the abutment tooth will depend
upon
➢Magnitude of the vertical load.
➢The physical characteristic of the overlying mucosa.
➢Angulation of the residual ridge to the horizontal plane.
➢The periodontal status of the tooth itself.
The effects of clasping are that
➢The more rigid the clasp, the greater the leverage on
the tooth and the less the load on the alveolar ridge.
➢The more flexible the clasp arms the less leverage on
the tooth and more load on the ridge.
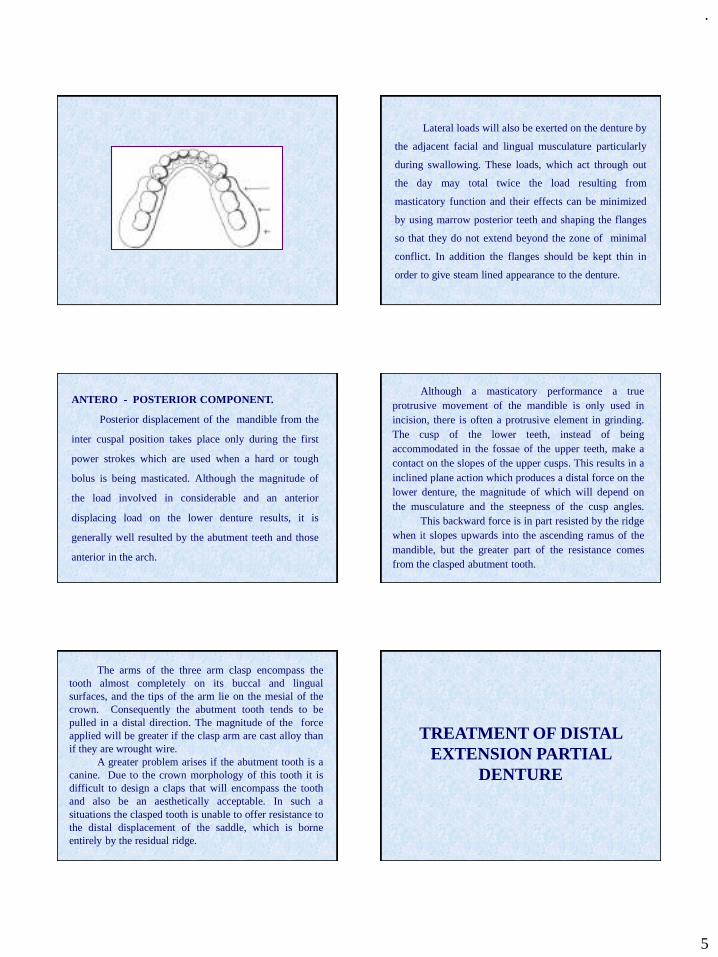
THE LATERAL COMPONENT
Lower distal extension saddles may be displaced
laterally as a result of the inclined plan action of the
cusps of the posterior teeth and the steeper the cusp
inclines the greater will be the load which acts laterally.
Lateral load may also act on the saddle during
these tooth contacts that may take place at times other
than during mastication and like the vertical forces will
be greater in magnitude.
The efficiency depends up on the anatomy of the
residual ridge and the condition of the soft tissue of the
working saddle.
Flat ridge with a marked fibrosis of the submucosa
offers comparatively little resistances, but if the ridge is
well formed and shows a thinner submucosa, resistance is
increased.
Lateral displacement have an adverse effect on the
residual alveolar ridge and in this respect the lateral
component of load is probably a major factors is ridge
resorption than the vertical component.
Stress Communicated by Resisting structure
➢Working side saddle.
➢Buccal arm of clasp on working side.
➢Balancing side saddle.
➢Lingual arm of claps on balancing side.
➢Continuous clasp (if included in design).
➢Lingual plate (if included in design.
➢Buccal ridge plate on working side.
➢Abutment tooth on working side.
➢Lingual ridge plate on balancing side.
➢Abutment tooth on balancing side.
➢Teeth on balancing side.
➢Lingual plate of ridge supporting teeth, and teeth themselves, on balancing side.
.
5
Lateral loads will also be exerted on the denture by
the adjacent facial and lingual musculature particularly
during swallowing. These loads, which act through out
the day may total twice the load resulting from
masticatory function and their effects can be minimized
by using marrow posterior teeth and shaping the flanges
so that they do not extend beyond the zone of minimal
conflict. In addition the flanges should be kept thin in
order to give steam lined appearance to the denture.
ANTERO - POSTERIOR COMPONENT.
Posterior displacement of the mandible from the
inter cuspal position takes place only during the first
power strokes which are used when a hard or tough
bolus is being masticated. Although the magnitude of
the load involved in considerable and an anterior
displacing load on the lower denture results, it is
generally well resulted by the abutment teeth and those
anterior in the arch.
Although a masticatory performance a trueprotrusive movement of the mandible is only used inincision, there is often a protrusive element in grinding.The cusp of the lower teeth, instead of beingaccommodated in the fossae of the upper teeth, make acontact on the slopes of the upper cusps. This results in ainclined plane action which produces a distal force on thelower denture, the magnitude of which will depend onthe musculature and the steepness of the cusp angles.
This backward force is in part resisted by the ridgewhen it slopes upwards into the ascending ramus of themandible, but the greater part of the resistance comesfrom the clasped abutment tooth.
The arms of the three arm clasp encompass thetooth almost completely on its buccal and lingualsurfaces, and the tips of the arm lie on the mesial of thecrown. Consequently the abutment tooth tends to bepulled in a distal direction. The magnitude of the forceapplied will be greater if the clasp arm are cast alloy thanif they are wrought wire.
A greater problem arises if the abutment tooth is acanine. Due to the crown morphology of this tooth it isdifficult to design a claps that will encompass the toothand also be an aesthetically acceptable. In such asituations the clasped tooth is unable to offer resistance tothe distal displacement of the saddle, which is borneentirely by the residual ridge.
TREATMENT OF DISTAL EXTENSION PARTIAL
DENTURE
.
6
KENNEDY CLASS I The suggested methods of restoring the bilateral free end
saddle may be achieved by
1.Reducing the load
2.Distributing the load between teeth and residual ridges.
i) By varying the connector between clasp and saddle.
a) Stress breaking.
b) Combining rigid connection and gingivally
approaching clasp.
c) Combining rigid connection and occlusal
approaching clasp
d) The disjunct denture
ii) By anterior placement of the occlusal rest :
a) The RPI system.
b) The balance of force system.
iii) By mucocompression
3. Distributing the load widely
i) Over more than one abutment tooth on each
side.
ii) Over the maximal area of edentulous ridge.
Reducing the load
The vertical load on the saddle in mastication may be
reduced by decreasing the size of the occlusal table and also
by ensuring as wide a coverage of the residual ridge area by
the base of the saddle as is compatible with function.
➢Using canines and premolars instead of premolars
and Molars.
➢Using narrow teeth or reducing the width of
selected teeth by removing the lingual cusp (s).
➢Leaving a tooth off a saddle.
DISTRIBUTION OF THE LOAD BETWEEN TEETHAND RIDGESi) By varying the connection between clasp and saddle.
a. Stress breakingThe principle of stress breaking in partial denture
design is the provision of some degree of movement orflexibility between the clasp unit and the distal extensionsaddle. The stress transmitted by the denture to the tissuesis distributed differently therefore and also reduced by theenergy absorbed in deformation than if the connection hadbeen rigid. Any device which allows movement betweenthe saddle unit and the retaining unit is known as a stressbreaker.
Stress Breakers can be divided into two groups.
➢ Those having a movable joint between the direct
retainer and the saddle.
➢ Those having a flexible connection between the
direct retainer and the saddle.
The first group is necessary when a precision
attachment is used, but can also be used when a claps
is preferred. They vary in their range of movement,
some allowing only up and down and side to side
movements, whereas others also permit a vertical
hinge action.
Construction of a flexible or semi-flexible connector
between the direct retainer and tooth supported part of the
denture and the mucosally supported saddle is achieved
with a distally extended flexible bar connected to the rigid
connector.
The degree of flexibility will depend upon in its
length and cross sectional form.
Where a lingual bar connector has been used to join
the two saddles it should be distally extended on each side
and then re-curved along the residual ridge to allow
attachment into the matrix resin of the saddle.
.
7
Alternatively if a lingual plate connector is used a
split of an appropriate length can be made at its inferior
border. The saddle is attached to the more flexible bar
while the clasp units are attached to the rigid part of the
framework.
The use of such designs allows the mucosa
supported saddle a degree of movement which is
independent of the rigid tooth supported part of the denture
and therefore lessens the stress of the abutment teeth.
When a vertical load is applied the saddle is
displaced downward into the soft tissue covering the ridge
to a greater extend than where the retainer and occlusal
rest have direct connection with a saddle. This means that
the ridge bone has to withstand an increased vertical load
which is more evenly spread over the whole ridge rather
than concentrated at the free end of the saddle. Although
not quite accurate it may be assumed that the centre of
saddle rotation is at the portion of the connector lying
anterior to it.
The net result of the stress breaking action as far
as the vertical component is concerned is a greater
assignment of load to the edentulous ridge and less to
the abutment tooth.
The torque on the abutment is reduced markedly
in magnitude and is favorable in direction.
When a lateral component acts on the stress broken
saddle a greatly increased lateral stress is placed on the
alveolar bone. Less of the load falls on the abutment teeth
and consequently the magnitude of the damaging lateral
torque is reduced.
If a continuous clasp or lingual plate is included in
the design it is incorporated in the retainer unit and thus
plays less part in the distribution of lateral load.
Stress breaking has little effect on the anteriorcomponent of force acting on the denture saddle duringthe power strokes ; uninterrupted contact between toothand retainer and retainer and saddle ensures no saddlemovement in an anterior direction and load distribution isaccordingly not altered.
The dangerous horizontal torques acting on theabutment teeth are reduced by stress breaking and that, inconsequence, their supporting structures are less liable tobreak down.
However, the edentulous ridge is called upon toaccept more vertical and horizontal stress and as a resulttends to resorb more quickly.
.
8
B. COMBINING RIGID CONNECTION AND
GINGIVALLY APPRAOCHING CLASPING
When rigid connection between retainers and
saddles is used, with gingivally approaching clasps, a
condition may exist which is similar in principle to stress
breaking. The portion of this type of claps that is in
contact with the abutment tooth is at the end of a bar that
is resilient to a degree which depends upon its length and
cross section and the alloy used.
If the occlusal rest is allowed to move over the
occlusal surfaces of the tooth to a small degree in lateral
and antero-posterior directions (and this may occur when
saucer-shaped rest seat preparation are used), the action
of the clasp bar resembles a stress breaker, since its
resilience reduces the horizontal forces on the abutment
tooth. The effectiveness of the stress breaking actions of
these clasps may be increased by increasing the
resilience of the bar.
C. COMBINING RIGID CONNECTION ANDOCCLUSALLY APPROAHING CLASPING.
A combination of rigid connection andocclusally approaching clasps is the opposite extreme tostress breaking. In this condition more load is placed onthe abutment tooth and ridge is capable of variation anddepends on the ridge.
When the arm is resilient, a certain amount ofmovement of the clasp over the surface of the tooth ispermitted. At one extreme a wrought gold wire claspallows most movement of the clasp over the enamel.Whereas a cast cobalt chromium clasp permits leastmovement.
The extent of these clasp movements is small but
they may, however, be sufficient to reduce the torque acting
on the abutment and keep them within the physiologic
limit.
If the mucosal tissues covering the ridge areas are
highly displaceable and mobile, then there may be an
indication for some type of movable or flexible connection
between the saddles and the retainer units.
d. THE DISJUNCT DENTUREIn the older patient it is not uncommon to find a
situation, particularly in the lower jaw, where the few
remaining teeth are anterior teeth with considerable
gingival recession and a generally poor periodontal
condition.
It has been suggested that such a problems may be
overcome by the construction of a two part denture,
composed separately of tooth borne and mucosa borne
sections each acting independently of each other on its
supporting tissues.
The tooth borne part comprises a lingual plate
which acts to protect the teeth and the gingivae from the
connector of the mucosa borne part, and which also
carries retention elements. In addition, it is constructed
with distally extending buccal bars which are designed
to engage a slot in the saddle of the mucosa borne part.
These are known as disjunct bars as they are not
attached directly and rigidly to the mucosa borne saddle
but allow some movement. They are however, necessary
for its retention.
.
9
The mucosa borne section of the denture are
essentially separate, there is no transfer of the vertical
masticatory load from the mucosa borne saddle to the
tooth borne section. In addition because of the absence of
a rigid connection between the two separate parts there is
little transfer of load by means of the disjunct bars. The
mucosa borne part can therefore move independently
according to the compressibility of the mucosa.
This technique has been suggested as particularly
useful in the treatment of the bilateral free end saddle,
where the support contribution of the remaining
standing teeth is poor and their periodontal health also
might be further compromised by a totally mucosally
borne designed denture.
The disadvantage of the denture is that is
technically difficult to construct and also that patients
occasionally complain it ‘rattling’ during function which
is of course due to the principles inherent in its design.
II. BY ANTERIOR PLACEMENT OF THEOCCLUSAL REST
The distribution of load between the abutment
teeth and residual ridge can sometimes be altered
favorably by anterior placement of the occlusal rest. This
has the effect of altering stresses on the saddle from a
Class I lever situation where the resistance to the applied
load lies on the opposite side of the fulcrum, to a Class
II lever where the resistance lies between the applied
load and the fulcrum. This permits more even
distribution of load and less stress on the abutment teeth
a. THE RPI SYSTEMThis system of partial denture design involving a
clasp unit comprised of a rest, proximal plate and “I” bar
retainer
An important consideration of this system is the
positioning of the occlusal rest to provide the element of
tooth support. If the rest is placed distally on the
abutment tooth and applied to the saddle, it has been
demonstrated that the arc of movement of the denture
base tends to the mainly perpendicular to the residual
ridge in the posterior region.
.
10
On moving anteriorly, however, the region near
the abutment tooth the saddle movement is almost
parallel to the ridge in an anterior direction. It is clear
that in this situations the mucosa adjacent to the tooth
can offer little resistance to the applied load, it and the
gingival margin being likely to be traumatized by the
horizontal movement of the denture against the abutment
tooth. This area, where tooth support ends and mucosa
support begins, should therefore be protected.
If the occlusal rest is placed mesially on the
abutment teeth, it has been shown that the arc of
movement of the saddle under applied load will alter and
be more perpendicular to the mucosa throughout its
length, due to the presence of a mesial rather than a distal
fulcrum.
This will increase the support provided by the
mucosa whilst reducing the anterior movement of the
saddle under applied load.
If the rest is placed distally then the tooth will tend
to tilt distally, where it has little support. If it is placed
mesially however, although there will be a tendency of
mesial tilting of the abutment tooth, this will be resisted
by other teeth in the arch anterior to it.
Potential damage to the gingival tissues distal to
the abutment tooth can be lessened if the distal surface of
the tooth is covered by a thin plate of cast metal (the
proximal plate) which extends on to the soft tissues. This
is relieved at the gingival margin.
Wear and damage will also be limited and the metal
will maintain a close adaptation so protecting the tissues
from food packing and preventing gingival hypertrophy.
In addition the plate should extend lingually on the
proximal surfaces of the tooth in order to provide some
reciprocation for the “I” bar clasp.
It has been argued that by constructing a
conventional occlusally approaching clasp the external
contour of the tooth is altered adversely, particularly in
relation to natural stimulation of the gingivae and in food
shedding.
If its tip is placed towards the mesial portion of the
tooth it also serves to bring the proximal plate into tight
contact with the distal surface. As the denture is
depressed on to its basal seat the clasp will move towards
and downwards and out of contact with the tooth so
removing any possibility of leverage.
The mesial rest is linked to a minor connector
which also provides some reciprocation and is placed in
the mesio lingual embrasure but free of the adjacent tooth
anterior to it. With applied load to the saddle the rest acts
as a fulcrum point, ensuring mesial rather than distal
loading of the abutment tooth.

.
11
Under load it will be depressed tissue wards
further into the undercut area without exerting torque
or leverage on the abutment tooth.
The “I” bar crosses the gingival margin at right
angles and contacts the tooth in its gingival third and
at the greatest mesiodistal prominence of the tooth, its
precise position of contact immediately below and
above the survey line.
Besides being retentive, it will move mesio
gingivally away from the tooth under applied load.
The RPI system will result in a denture with
➢ Enhanced mucosal support due to perpendicularloading.
➢Reinforcement against mesial tilting of the abutmenttooth.
➢Adequate retention with minimal effect on natural toothcontour.
➢No adverse stress on the abutment tooth duringmasticatory loading.
➢Protection of the transitional region between the toothand the mucosal area of the edentulous saddle.
b. Balance of force system
The balance of force system, canbe considered as a
further refinement of the RPI system being based on the
mechanical principles of a class II lever. As the magnitude
of masticatory loads on the abutment teeth are much
greater than those of the forces of displacement and as the
tooth is less able to withstand this, the design has been
developed to ensure that loads during masticatory
performance are directed vertically along the long axis of
the tooth so avoiding torque and leverage.
A rest seat must be provided on the part of the
occlusal surface of the abutment tooth that is distant from
the saddle. This will act as the fulcrum point and ensure
vertical loading on the tooth during function. In distal
extension partial dentures this would be a mesially
placed support unit.
In addition to rest seat preparation an
interproximal access area of about 1 mm must be created
between the abutment tooth and the anterior tooth
adjacent. It is in this area that reciprocation for the clasp
arm will be positioned together with the minor connector.
The clasp unit is designed so that retentive tip of the
claps arm is positioned on the interproximal surface of the
abutment tooth adjacent to the edentulous saddle. It should
lie below the maximum convexity of this surface engaging
a degree of undercut according to the physical properties
of the material.
The reciprocation for the retentive force of the clasp
arm in resisting displacement is provided by a vertical
plate in the prepared access area on the abutment tooth
above its maximum convexity. The vertical plate is joined
to the major connector.
.
12
The unit should be so designed that the flexible tip
of the clasp arm, the occlusal rest and the contact surface
of the vertical reciprocating plate are in line with the
crest of the edentulous ridge. Retention is therefore
achieved mesiodistally as opposed to bucco-lingually and
the design ensures that the greatest loads on the tooth are
applied mesio-distally where it is well supported.
When masticatory load is applied to the distal
extension saddle its downward movement towards the
underlying tissue is accompanied by a similar movement
of the retentive tip of the clasp arm. This allows the
clasp to disengage the tooth as it moves into an area of
increased undercut, this eliminating horizontal tooth
loading. The mesial occlusal rests will direct loads
vertically along the long axis of the tooth hence it is
better able to withstand them.
If a displacing force is applied to the denture, the
saddle and clasp tip once again move in the same
direction occlusally. The clasp tip will now engage the
proximal surface of the tooth below its maximum
convexity thus providing resistance to further
displacement. Reciprocation during this action is
provided by the vertical interproximal plate on the
opposite side of the tooth.
III. BY MUCOCOMPRESSION
➢Mucostasis➢Mucocompression.
The greater the amount of displacement the less isthe magnitude of the torque and load on the abutment,when a vertical load is placed on the saddle.
Different impression materials give varyingdegrees of mucosal displacement
The saddle base fitted accurately against themucosa from which tissue fluid has already beendisplaced sinks less under the masticatory load than iffitted against an undisturbed mucosa.
The amount of displacement affects the
distribution of load between abutment and ridge bone.
The greater the displacement the more evenly is
the stress distributed between the abutment and the
edentulous ridge.
However, the mucosa cannot be continuously
subjected to such heavy pressure since this will result in
decreased blood supply to, and drainage from, the soft
tissues. Coupled with the fact that the tissue fluid is also
reduced, this may result in a tropic disturbance
The natural tendency of the displaced tissue is torecoil in a visco-elastic manner. In assuming that thesaddle is maintained in the closest approximation with thedisplaced mucosa, the presence of some force to hold it inthis position is also assumed.
This force can only come from rigid clasping of theabutment tooth and results in a continuous force acting onthe abutment.
It is thus seen that the use of rigid connection andclasping together with mixture displacement leads to anunacceptable situation in respect of potential damage tothe abutment and covering mucosa.

.
13
If maximum displacement is to be used,
arrangement must be made to allow some recoil of the
mucosal tissues.
This can be achieved either by very light
clasping, generally wrought gold wires of thin gauge,
or by a stress breaker giving flexible connection
between the saddles and retainer units.
The method of maximum displacement coupled with
light clasping directly attached to the saddles is not used
➢ Retention of such a denture is inadequate because of
the light clasping and poor adhesion, the latter being due to
the uneven thickness of saliva film between the mucosa and
the fitting surface of the denture after recoil of the tissues.
➢ Lateral stresses are resisted largely by the edentulous
ridge, which is, therefore, liable to resorb.
With mucostasis, even when cast clasps are
directly attached to the saddles, no forces act either on
the ridge or abutment when the saddle is not under load.
In the resting stage, too, adhesion is maximal.
With this type of impression too, the bone is not
evently stressed, the areas underlying thinner mucosa
receiving an increased share of the load.
With such a technique and where rigid clasping
directly attached to the saddle is used, maximal leverage
and torque is placed on the abutment teeth, which are,
therefore, predisposed to periodontal breakdown.
With this type of impression too, the bone is not
evenly stressed, the areas underlying thinner mucosa
receiving an increased share of the load.
There is however, a condition intermediate between
maximum displacement and mucostasis that has
considerable advantages
Thus a compromise between stasis and maximum
displacement seems to give a result with the advantages
of each present to some degree.
3. WIDE DISTRIBUTION OF LOAD
I)WIDE DISTRIBUTION OF LOAD OVER THE
TEETH
When clinically circumstances permit, the procedure
is to move the occlusal rest anteriorly so that it lies not
on the tooth that immediately bound the saddle, but on
the occlusal surface of the tooth that lies immediately
anterior.
If a rest is placed on this tooth some of the vertical
load is placed upon it and its marginal ridge becomes
the fulcrum point.
If two flexible arms now arise from this and its
encompass the buccal and lingual surfaces of the
posterior tooth and if these arms lie above the survey
lines then some of the vertical load is dispersed.
Part is dissipated in opening the clasp arms and
part is directed down the long axis of the tooth.
The retaining clasp is on the rested tooth. Which
accepts vertical load through the occlusal rest. Lateral
load is distributed to the two teeth by the clasp arms.

.
14
II.) WIDE DISTRIBUTION OF LOAD OVER THE
RIDGE
The saddles of the denture should always cover the
largest possible area, so that the pressure falling on any
unit area of the edentulous ridge is reduced under vertical
and horizontal loading. While full coverage over the
retromolar area and the buttress bone both buccally and
lingually is desirable for load distribution it may not
always be acceptable to the patient.
Modification of the bilateral free end saddle lower
denture
Modification of the bilateral free end saddle lower denture
1) An anterior saddle present in addition to 2 free end saddle
2) Long free end saddle interrupted by a single standing
An anterior saddle present in addition to 2 free end saddle
The stress on the abutment tooth depends on
• saddle length and shape
•Displaceability of mucosa
A rigid construction is advisable
By clasping the 4 abutment teeth , vertical and horizontal forces are resisted by 2 teeth on each side . This facilitates wide distribution of load
a)If only 2 premolars remain bilaterally
• Lingual bars and continuous clasps
The clasps are constructed in wrought wire but if ridges are well formed they may be constructed in cast metal
b)if premolars are severely inclined lingually
• Buccal bar
• Back action clasp
c)Only 2 canine remain
•Simple acrylic resin mucosa supported denture
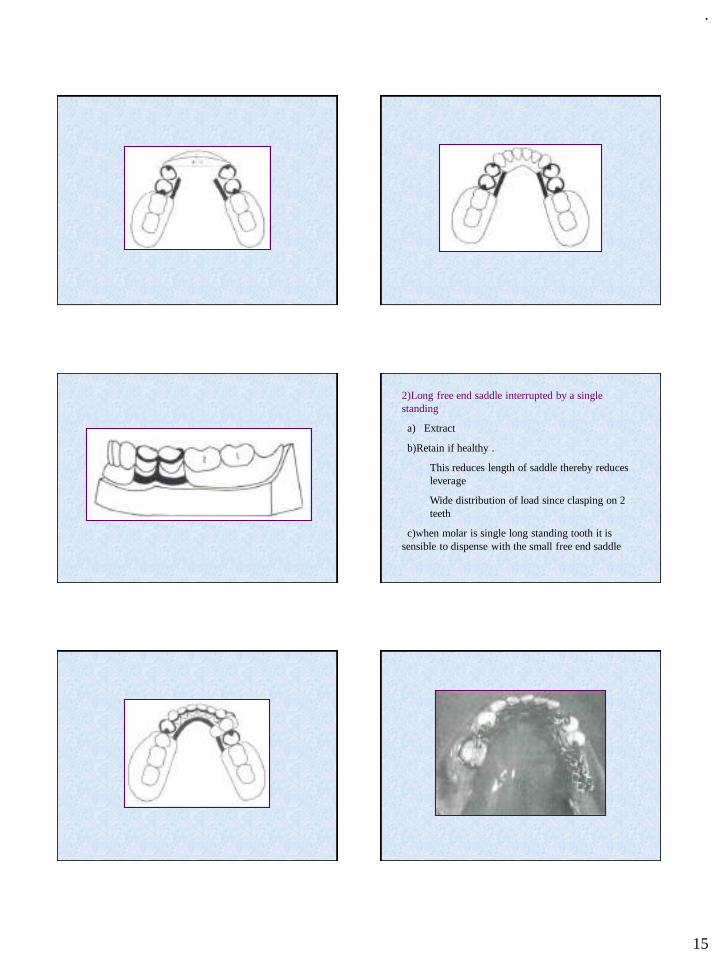
.
15
2)Long free end saddle interrupted by a single standing
a) Extract
b)Retain if healthy .
This reduces length of saddle thereby reduces leverage
Wide distribution of load since clasping on 2 teeth
c)when molar is single long standing tooth it is sensible to dispense with the small free end saddle
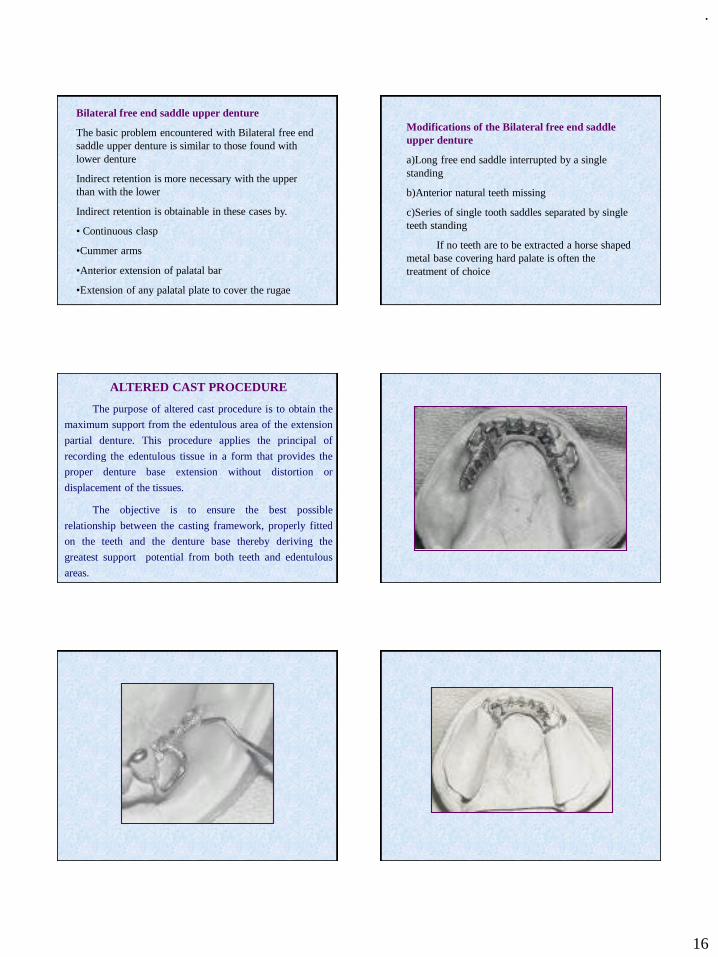
.
16
Bilateral free end saddle upper denture
The basic problem encountered with Bilateral free end saddle upper denture is similar to those found with lower denture
Indirect retention is more necessary with the upper than with the lower
Indirect retention is obtainable in these cases by.
• Continuous clasp
•Cummer arms
•Anterior extension of palatal bar
•Extension of any palatal plate to cover the rugae
Modifications of the Bilateral free end saddle upper denture
a)Long free end saddle interrupted by a single standing
b)Anterior natural teeth missing
c)Series of single tooth saddles separated by single teeth standing
If no teeth are to be extracted a horse shaped metal base covering hard palate is often the treatment of choice
ALTERED CAST PROCEDURE
The purpose of altered cast procedure is to obtain the
maximum support from the edentulous area of the extension
partial denture. This procedure applies the principal of
recording the edentulous tissue in a form that provides the
proper denture base extension without distortion or
displacement of the tissues.
The objective is to ensure the best possible
relationship between the casting framework, properly fitted
on the teeth and the denture base thereby deriving the
greatest support potential from both teeth and edentulous
areas.
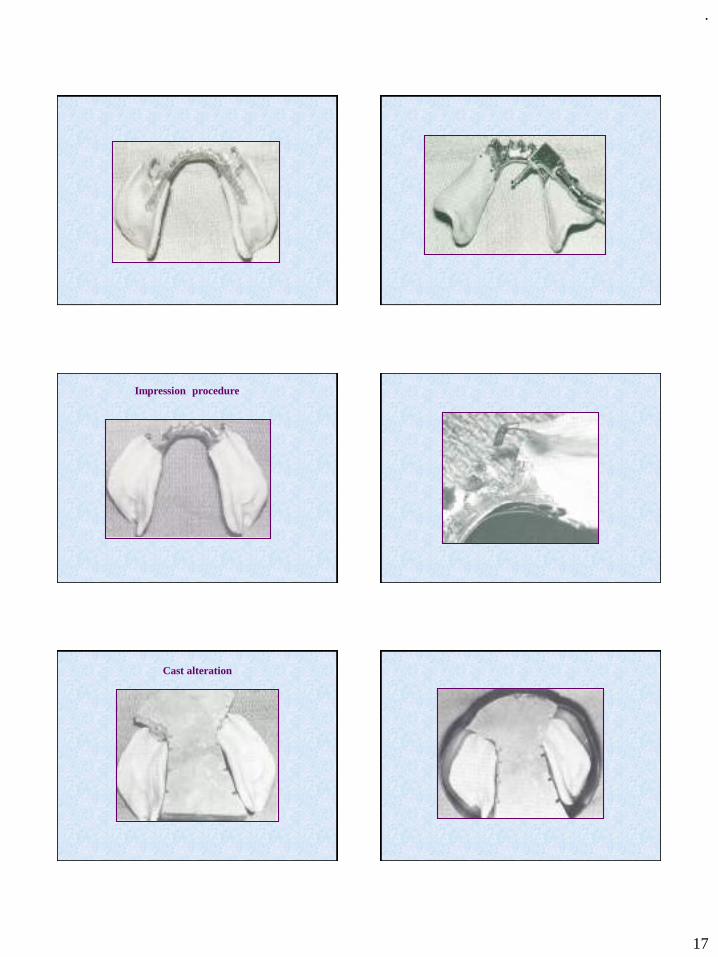
.
17
Impression procedure
Cast alteration
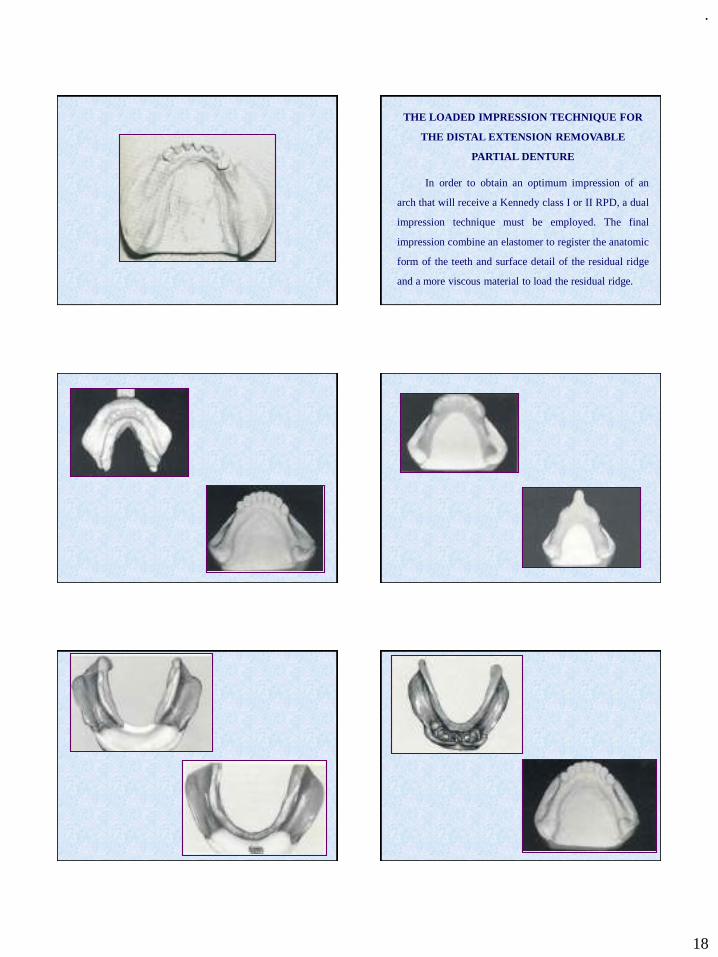
.
18
THE LOADED IMPRESSION TECHNIQUE FOR
THE DISTAL EXTENSION REMOVABLE
PARTIAL DENTURE
In order to obtain an optimum impression of an
arch that will receive a Kennedy class I or II RPD, a dual
impression technique must be employed. The final
impression combine an elastomer to register the anatomic
form of the teeth and surface detail of the residual ridge
and a more viscous material to load the residual ridge.
.
19
Review of Literature
Stress analysis is distal extension partial dentures.
George W. Hindels J. Prosthet Dent. 7; 197 – 205, 1952.
He described the load distribution in extension saddle partial
dentures. He said that the method used to make impression of
the supporting and retaining anatomic status of the mouth is of
basic importance for obtaining optimum distribution of the
masticatory load in the construction of remarkable partial
denture, especially those of the lower extension saddle type.
His opinion is that there are three definite requirement that
must be fulfilled to assure proper load distribution in extension
saddle partial denture.
They are
➢The tissue surface of the saddle should be negative reproduction
of the anatomic, undisturbed surface of the alveolar mucosa.
➢The masticatory load should be distributed between the ridge and
the abutment teeth during function and cannot be left to be carried
by alveolar ridge alone.
➢The denture saddle should be related to the metal frame work in
such a way as to be similar to the relationship existing between the
supporting teeth and the supporting mucosa when latter is a
masticatory load.
The Bilateral free end saddle lower denture.
Lamme G.A. and John Osborne
J. Prosthet Dent 4 : 640 – 652, 1954.
They stated that the bilateral free end saddle lower denture (class I
lower denture of the kennedy’s classification) always presents a
treatment problem. A free end saddle can have tooth support at only
one extremity and this at least part of lead falling upon it must be
resisted by the edentulous alveolar bone. This is in contra distinction
to the bounded saddle, which has anteriorly and posteriorly placed
abutment teeth. in this he given following methods for the treatment
of the free and saddle. The following method of attempting to control
the vertical load are designed to give the optimal reaction in both
teeth and alveolar
1.Reducing the load directly.
2.Distributing the load between teeth and alveolar
i) By varying the nature of the connection between
clasp and saddle.
a)Stress breaking
b)Combining rigid connection and gingivally
approaching clasping.
c)Combining rigid connection and occlusal
approaching clasping.
ii) By anterior placement of the occlusal rest.
iii) By mucocompression.
3. Distributing the load widely
i) Over more than one abutment tooth on each side.
ii) Over the maximal area of edentulous alveolar
Stress analysis is distal extension partial dentures.
George W. Hindels J. Prosthet Dent. 7; 197 – 205, 1957.
He did a stress analysis in distal extension partial dentures, he
said that masticatory stresses exerted on the base of a distal
extension partial denture are transmitted to the supporting
anatomic structures through contacting parts of the appliance.
If the parts are incorrectly designed or constructed, they will
alter the direction and force of these masticatory stresses and
may create stresses which are not within the physiologic limits
of tissue tolerance. The partial denture should be constructed.
So this movement is vertical is relation to the supporting bone.
.
20
Clasp and rest should be designed to allow for this vertical
movement of the denture base. Stress other than those vertical to
the abutment teeth should be reciprocated. Reciprocation is best
obtained by contact of rigid parts of the partial denture with
modified axial surface of the abutment teeth which are made
parallel to each other and the path of insertion
A study of partial denture design and masticatory pressure
in the mandibular bilateral distal extension case.Anthony K. Karies : J. Prosthet dent. 8: 340-350, 1958
In a study of masticatory performance, he found out that the
followings;
➢ The reduction of the size of the occlusal table reduces the forcesacting on the partial denture and lessens the stresses on theabutment teeth and supporting tissues.
➢ The effect of the partial denture on masticatory performance didnot reveal any significant relationship.
➢ The rigid design of the partial denture were more desirable thanthe flexible are specifically the rigid lingual bar is moredesirable than a flexible bar in withstanding horizontal stresses.
Preparation of abutment teeth for removable partial
dentures.
Holmes J.B. J. Prosthet Dent. 20: 396 – 406, 1968.
He mentioned about the preparation of abutment teeth for
dentures, he says that the preparation of spoon shaped or
rounded rest seat areas that direct forces towards the long axes
at abutment teeth provides positive support for the partial
denture. The location of rest areas affects the movements of
abutment teeth by changing the direction of force applied to the
teeth and to the denture base.
Metal guiding planes that contact the proximal surface of the
abutment teeth and extend 1 to 2 mm onto the residual ridge
lessen the possibility that debris will collected around the denture
the residual ridge and the abutment. The development of adequate
support for partial denture without applying under torquing force
to the abutment and the maintenance of the health of the
periodontal supporting structure pre vital to the success of partial
denture treatment.
Clasp design for extension base removable partialdentures.
Arthur J. Krol J. Prosthet Dent. 29:408-416, 1973.
He mentioned that clasp design for extension base partial
dentures is one of the more fascinating and thought provoking
subject in dentistry. Many types of clasp for unilateral and
bilateral distal extension base partial dentures are consult
being and by dentist and dental laboratories throughout the
work in an attempt to prolong the life of the remaining teeth.
The clasp returd to as an R.P.I. clasp is introduced which
minimizes tooth coverage and reduces stress on the abutment
tooth.
RICHARD P. FRANK in 1986 in his clinical observation indicated
that the wrought wire clasp assembly. The I-bar clasp assembly and
the L-bar clasp assembly yield similar results. Several thousand
observations have been made by the faculty and no special trend of
problems has been noted that would cause one clasp assembly to be
favoured over another. These three types of clasp assemblies work
satisfactorily when properly chosen and carefully applied.
.
21
RONALD E. MYERS in 1986 in his photoelastic study of rests
found out that with a distal extension removable partial denture,
maximum use of existing oral structure can aid in the total support
of the prostheses and reduce the force on the solitary abutment.
Four rests with relieved and unrelieved guide plates were
evaluated for optimum stress distribution around the root of a
solitary premolar abutment. The rest were the mesial, the distal.
The mesial and distal and the continuous rest.
The findings demonstrated that :
1.The continuous rest had the most favourable stress
concentrations.
2.All other rest design demonstrated more lateral stress than the
continuous rest.
3.Relieved guide planes demonstrated 58% less maximum shear
stress in the apical portion than unrelieved guide planes.
An analysis of rotational movements of asymmetricaldestal extension removable partial dentures.
Aviv I. Et al J. Prosthet Dent 61; 211 - 214, 1989.
He states that an axis of rotation is created through the most
distally placed occlusal rest. When a distal extension removable
partial denture is loaded. If the residual ridges are of unequal
length, the axis of rotation may not be perpendicular to the
residual ridge. Movements of I bar retainers loaded on the
mesiobuccal aspect of asymmetrical abutment teeth may torque
the abutment teeth as the denture base moves tissues wards. Use
of L shaped direct retainer on the distobuccal surveyed undercut
will create a more favourable class II lesser effect on the
abutment tooth
Comparison of vertical movements occurring during loading of distal extension RPD bases made by three impression techniques.
Richard J Leupold, Robert J Flinton, David L Pfiefer
JPD 1992;68:290-293
The study clinically compared the vertical displacement
of the distal extension RPD made from altered cast
impression, an impression from border molded custom
tray. Stock tray irreversible hydrocolloid was used as a
control. Although statistically significant 0.19mm
difference between impression techniques may or may
not be clinically significant.
Sectional impression for mandibular distal extension RPD
Hanaa Al Shiekh, Adel M Abdul Hakim
JPD1998;80:216-219
The final impressions made in border molded full
arch custom tray clinically comparable to sectional
impression for distal extension mandibular RPD.
Sectional impressions demonstrated significant
reduction in vertical movement when analyzed
statistically. However this finding maybe clinically
insignificant.
Clinical outcome of altered cast impression procedures compared with the use of a one piece cast.
Richard P Frank , James S Brudvik, Karleen G Noonan
JPD 2004;91:468-476
The altered cast impression procedure does not have
significant advantages over the one piece cast provided
standards in this study are met. These include completely
extended impression, use of a magnification to ensure
complete seating of the frame work and coverage of the
retromolar pad and buccal shelf by the base.
.
22

.
1
Good MorningTHE ENDOCRINE SYSTEM
Presented by:
Dr. PRAJAKTA BARAPATRE
Introduction
The body functions are regulated by nervous and endocrine systems aiming
for homeostasis.
Both systems represent two parts of control systems.
The difference between the two systems is in their speed and time needed to
exert their action.
The nervous system responds within a fraction of seconds whereas the
endocrine system responds from a fraction of second up to over cycles of
days, months or even years.
The difference in time factor because the nervous system depends upon an action potential as a conductor of its signal, which travel along the nerve fibers within a fraction of seconds while the endocrine system depends upon a chemical substance called hormone which travel allover the body with blood to exert the signal which it carries.
Both systems are integrated to control homeostasis and this principle is clearly seen in the hypothalamus and pituitary gland where the two systems are linked
The nervous system mediate its activity through nerves that directly innervate the cells being controlled, by releasing regulatory molecules known as neurotransmitters to achieve the desired effect.
Both systems enable the body to respond to a wide range of internal and external stimuli by electing appropriate responses to these stimuli that ensure that the physiological functioning of the body is done to achieve homeostasis.
HOMEOSTASIS
keeping the parameters of the body in a steady, same state.
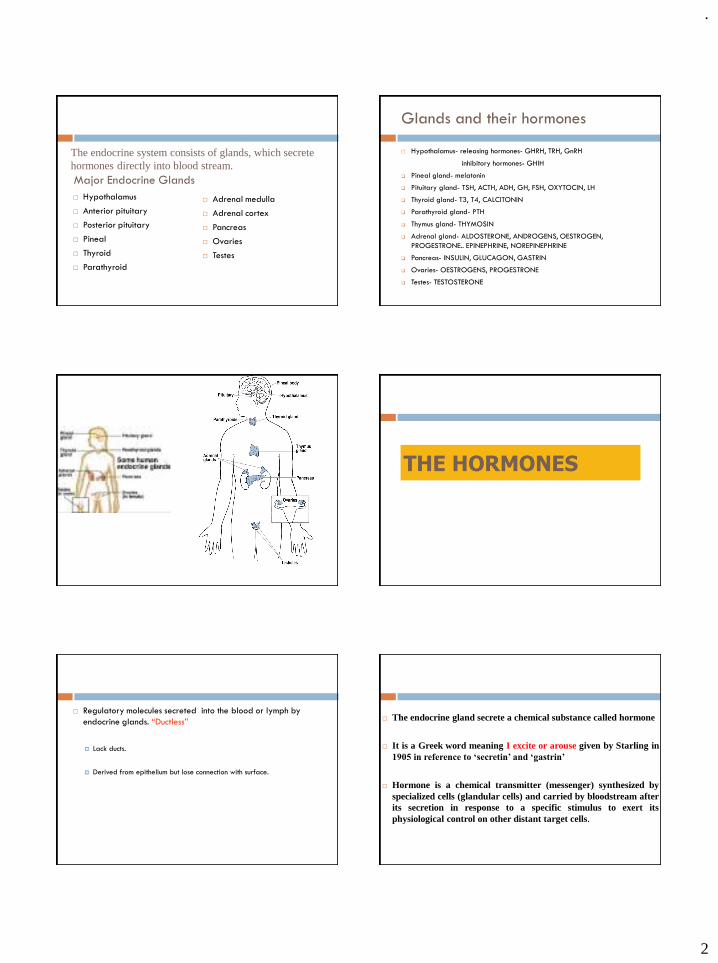
.
2
The endocrine system consists of glands, which secrete hormones directly into blood stream.Major Endocrine Glands
Hypothalamus
Anterior pituitary
Posterior pituitary
Pineal
Thyroid
Parathyroid
Adrenal medulla
Adrenal cortex
Pancreas
Ovaries
Testes
Glands and their hormones
Hypothalamus- releasing hormones- GHRH, TRH, GnRH
inhibitory hormones- GHIH
❑ Pineal gland- melatonin
❑ Pituitary gland- TSH, ACTH, ADH, GH, FSH, OXYTOCIN, LH
❑ Thyroid gland- T3, T4, CALCITONIN
❑ Parathyroid gland- PTH
❑ Thymus gland- THYMOSIN
❑ Adrenal gland- ALDOSTERONE, ANDROGENS, OESTROGEN,
PROGESTRONE.. EPINEPHRINE, NOREPINEPHRINE
❑ Pancreas- INSULIN, GLUCAGON, GASTRIN
❑ Ovaries- OESTROGENS, PROGESTRONE
❑ Testes- TESTOSTERONE
THE HORMONES
Regulatory molecules secreted into the blood or lymph by
endocrine glands. “Ductless”
Lack ducts.
Derived from epithelium but lose connection with surface.
The endocrine gland secrete a chemical substance called hormone
It is a Greek word meaning I excite or arouse given by Starling in 1905 in reference to ‘secretin’ and ‘gastrin’
Hormone is a chemical transmitter (messenger) synthesized by specialized cells (glandular cells) and carried by bloodstream after its secretion in response to a specific stimulus to exert its physiological control on other distant target cells.
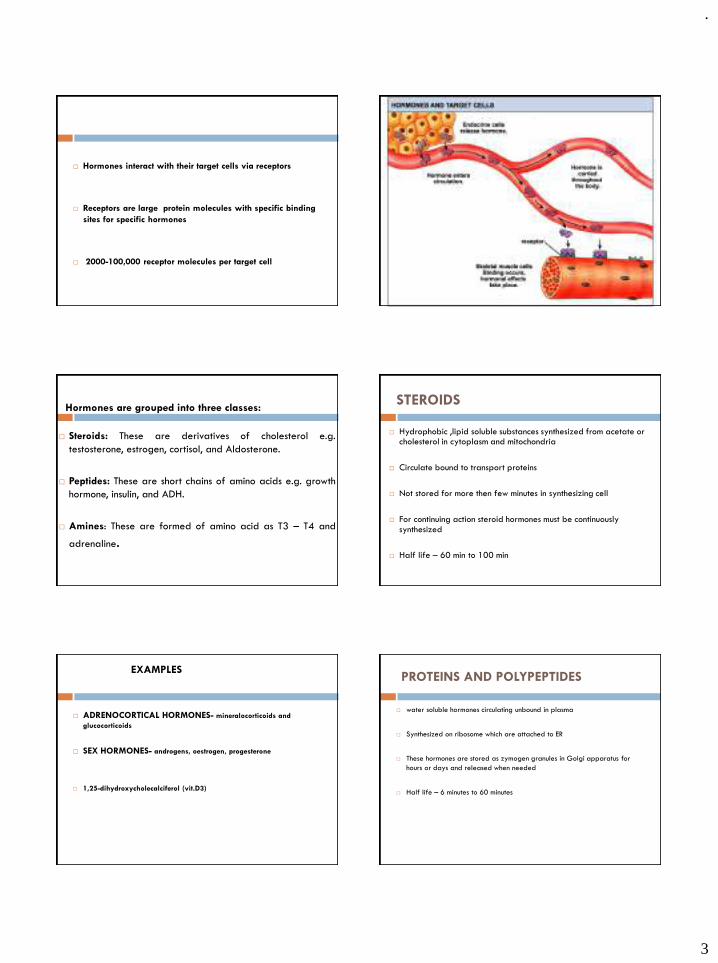
.
3
Hormones interact with their target cells via receptors
Receptors are large protein molecules with specific binding
sites for specific hormones
2000-100,000 receptor molecules per target cell
Hormones are grouped into three classes:
Steroids: These are derivatives of cholesterol e.g.
testosterone, estrogen, cortisol, and Aldosterone.
Peptides: These are short chains of amino acids e.g. growth
hormone, insulin, and ADH.
Amines: These are formed of amino acid as T3 – T4 and
adrenaline.
STEROIDS
Hydrophobic ,lipid soluble substances synthesized from acetate or cholesterol in cytoplasm and mitochondria
Circulate bound to transport proteins
Not stored for more then few minutes in synthesizing cell
For continuing action steroid hormones must be continuously synthesized
Half life – 60 min to 100 min
EXAMPLES
ADRENOCORTICAL HORMONES- mineralocorticoids and
glucocorticoids
SEX HORMONES- androgens, oestrogen, progesterone
1,25-dihydroxycholecalciferol (vit.D3)
PROTEINS AND POLYPEPTIDES
water soluble hormones circulating unbound in plasma
Synthesized on ribosome which are attached to ER
These hormones are stored as zymogen granules in Golgi apparatus for
hours or days and released when needed
Half life – 6 minutes to 60 minutes
.
4
EXAMPLES
Anterior and posterior pituitary hormones
Hypothalamic hormones
Parathyroid hormones, calcitonin, insulin, glucagon, gastrin, secretin and
angiotensin
AMINES
Hormones derived from tyrosine and tryptophan.
Most of thyroid hormones are bound to transport proteins
Half life- 7 to 9 days
Examples include hormones secreted by adrenal medulla, thyroid, and
pineal glands.
HORMONAL INTERACTIONS
SYNERGISM:
Two hormones work together to produce a result.
Additive:
◼ Each hormone separately produces response, together at same
concentrations stimulate even greater effect.
◼ Epinephrine and nor epinephrine.
Complementary:
◼ Each hormone stimulates different step in the process.
◼ FSH and testosterone.
PERMISSIVE EFFECTS:
Hormone enhances the responsiveness of a target
organ to second hormone.
Increases the activity of a second hormone.
◼ Prior exposure of uterus to estrogen induces formation of
receptors for progesterone.
ANTAGONISTIC EFFECTS:
Action of one hormone antagonizes the effects of
another.
Insulin and glucagon.
HORMONE CONCENTRATION
Concentration of hormones in blood reflects the rate of
secretion.
Half-life:
Time required for the plasma concentration is reduced to ½ reference
level.
Physiological range of concentration produces normal tissue
response.
.
5
Effects of Hormone Concentration
Varying hormone concentration within normal, physiological
range can affect the responsiveness of target cells.
Priming effects (up regulation)
Increase number of receptors formed on target cells.
Greater response by the target cell.
Desensitization (down regulation):
Decrease in number of receptors on target cells.
Produces less of a target cell response.
Receptor Down-regulation
After hormone binding receptors may be
internalized
Leads to reduced responsiveness of target cell
(usually temporary)
Receptor may be recycled to cell surface or
degraded
Mechanisms of Hormone Action
Hormones of same chemical class have similar mechanisms of action.
Target cell must have specific receptors for that hormone (specificity).
Hormones bind to receptors with high bond strength (affinity).
Low capacity of receptors (saturation).
Hormones That Bind to Nuclear Receptor
Proteins
Lipophilic steroid and thyroid hormones bound to plasma carrier
proteins.
Hormones dissociate from carrier proteins to pass through lipid component of the target cell membrane.
Receptors for the lipophilic hormones are known as nuclear hormone receptors.
Nuclear Hormone Receptors
Function within cell to activate genetic transcription.
mRNA directs synthesis of specific enzyme proteins that change metabolism (translation).
Receptor must be activated by binding to hormone before binding to specific region of DNA called HRE (hormone responsive element).
Located adjacent to gene that will be transcribed.
Mechanisms of Steroid Hormone Action
Steroid receptors located in
cytoplasm.
Bind to steroid hormone.
Translocates to nucleus.
DNA-binding domain binds to specific HRE of the DNA.
Dimerization occurs.
Stimulates transcription.
.
6
Intracellular Receptors
Steroid and thyroid hormones act via intracellular receptors
Hormone-receptor complex interacts directly with DNA in chromatin fiber at the promoter of specific genes
H-R complex acts as a transcription factor to enhance (or decrease) rate of transcription
Intracellular Receptors
Hormones That Use 2nd Messengers
Cannot pass through plasma membrane.
Catecholamine's, polypeptides, and glycoprotein's bind to receptor proteins on the target cell membrane.
This activates the enzyme adenylyl cyclase on the inner surface of the
membrane
This increases formation of intracellular cAMP from ATP , which acts as a
second messenger
Second messenger is a basic regulator of cell metabolism.. Acting by
converting inactive protein kinases to their active form
Phosphorylation of proteins occurs causing activation or inactivation of
specific enzymes- altered cell activity
.
7
cAMP as second messenger
Biological effects
Second messengers create phenotypic changes in
target cells
Alter phosphorylation (activity) of proteins
Alter permeability of membranes
Indirectly influence gene expression
G protein –linked receptors
Non-G protein Receptors Regulation of endocrine system
DIRECT NEGATIVE FEEDBACK:
There is direct interaction between the controlling hormone and the controlled
metabolite: - e.g.:- Plasma calcium level.
E.g. In case of decreased plasma calcium level → this is detected directly by
parathyroid cells lead to synthesis of parathormone hormone leads to increase
calcium level by increased secretion.
.
8
INDIRECT NEGATIVE FEEDBACK:
Some peripheral endocrine glands (thyroid, adrenal cortex and gonads) are dependent on the regulation provided by hormones released from the anterior pituitary, whose release is in turn dependent on the endocrine activity of
hypothalamus.
That is why hypothalamus is also known as ‘MASTER OF ENDOCRINE ORCHESTRA’
In this situation, the hypothalamic neuroendocrine cells are frequently integrating information from a variety of sources, including the circulating levels of the hormone secreted by the peripheral endocrine gland.
Negative Feedback:
A self-correcting system
normal
Upper limit
Lower limit
Blglu
A Negative Feedback System Positive Feedback:
Positive feedback exists when a hormone is able to stimulate its own production.
Such situations are rare and the only example that is well documented, relates to ovulation and 17 b-oestradiol, which achieves positive feedback by stimulating the release of hypothalamic GnRH; this causes the release of pituitary FSH and LH, which in turn stimulates the production of more 17 b-oestradiol by the ovary.
Positive Feedback?
This is a NON-correcting system. A little becomes more. Less becomes a lot less.
Examples: Oxytocin and Prolactin hormones
.
Properties of Hormones
1- Hormones are synthesized continuously.
2- Hormones may be stored within the cytoplasm of the cells as inactive granule e.g.
pituitary hormones or in the form of colloid mass as in thyroid acini.
3- Some hormones are secreted by more than one gland e.g. estrogenic hormones are
secreted by (ovary, placenta and adrenal cortex).
4 -Most hormones are released from their glands in short burst (pulses) that maintain
basal definite level for each hormone in blood.
.
9
5- The hormone secretion show diurnal variation (circadian rhythm) e.g. growth hormone secretion is markedly increased in early hours of sleep, while plasma cortisol rise in early morning.
6- Reciprocal chemical regulation: The stimuli which produce secretion of one hormone inhibits the release of its antagonistic e.g. fall in plasma calcium stimulate secretion of parathormone and inhibit the secretion of thyrocalcitonin hormone.
7- Hormones produce their physiological effect by a very low concentration in blood.
8- Hormones act on a very specific receptors.
9- Hormones act as trigger substances, which initiate biochemical reactions that persist
after disappearance of hormone from blood.
10- Hormones may affect many cells of the body e.g. insulin & thyroxine.
11- Hormones may produce specific action e.g. insulin lowers blood glucose.
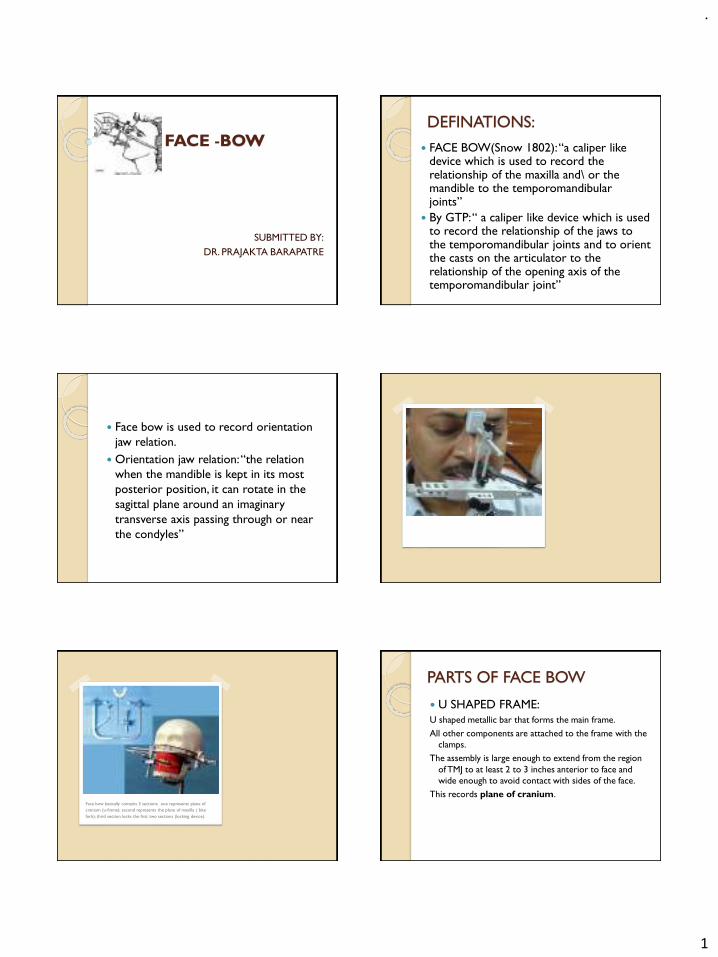
.
1
FACE -BOW
SUBMITTED BY:
DR. PRAJAKTA BARAPATRE
DEFINATIONS:
FACE BOW(Snow 1802): “a caliper like device which is used to record the relationship of the maxilla and\ or the mandible to the temporomandibularjoints”
By GTP: “ a caliper like device which is used to record the relationship of the jaws to the temporomandibular joints and to orient the casts on the articulator to the relationship of the opening axis of the temporomandibular joint”
Face bow is used to record orientation
jaw relation.
Orientation jaw relation: “the relation
when the mandible is kept in its most
posterior position, it can rotate in the
sagittal plane around an imaginary
transverse axis passing through or near
the condyles”
Face bow basically contains 3 sections: one represents plane of
cranium (u-frame); second represents the plane of maxilla ( bite
fork); third section locks the first two sections (locking device).
PARTS OF FACE BOW
U SHAPED FRAME:
U shaped metallic bar that forms the main frame.
All other components are attached to the frame with the
clamps.
The assembly is large enough to extend from the region
of TMJ to at least 2 to 3 inches anterior to face and
wide enough to avoid contact with sides of the face.
This records plane of cranium.
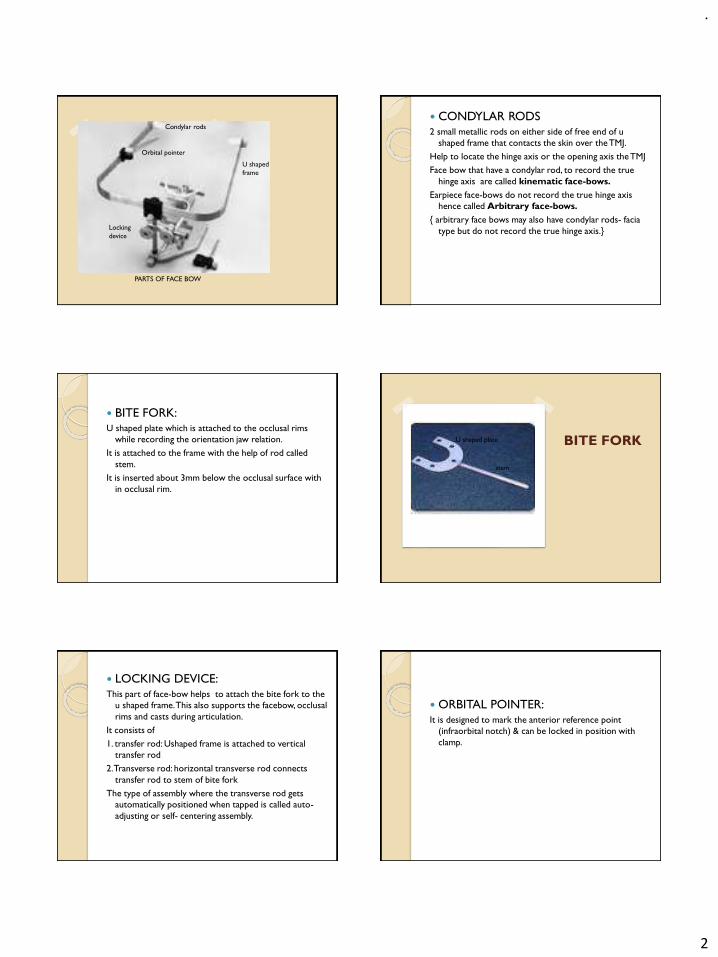
.
2
Condylar rods
Orbital pointer
U shaped
frame
Locking
device
PARTS OF FACE BOW
CONDYLAR RODS
2 small metallic rods on either side of free end of u
shaped frame that contacts the skin over the TMJ.
Help to locate the hinge axis or the opening axis the TMJ
Face bow that have a condylar rod, to record the true
hinge axis are called kinematic face-bows.
Earpiece face-bows do not record the true hinge axis
hence called Arbitrary face-bows.
{ arbitrary face bows may also have condylar rods- facia
type but do not record the true hinge axis.}
BITE FORK:
U shaped plate which is attached to the occlusal rims
while recording the orientation jaw relation.
It is attached to the frame with the help of rod called
stem.
It is inserted about 3mm below the occlusal surface with
in occlusal rim.
BITE FORK
stem
U shaped plate
LOCKING DEVICE:
This part of face-bow helps to attach the bite fork to the
u shaped frame. This also supports the facebow, occlusal
rims and casts during articulation.
It consists of
1. transfer rod: Ushaped frame is attached to vertical
transfer rod
2. Transverse rod: horizontal transverse rod connects
transfer rod to stem of bite fork
The type of assembly where the transverse rod gets
automatically positioned when tapped is called auto-
adjusting or self- centering assembly.
ORBITAL POINTER:
It is designed to mark the anterior reference point
(infraorbital notch) & can be locked in position with
clamp.
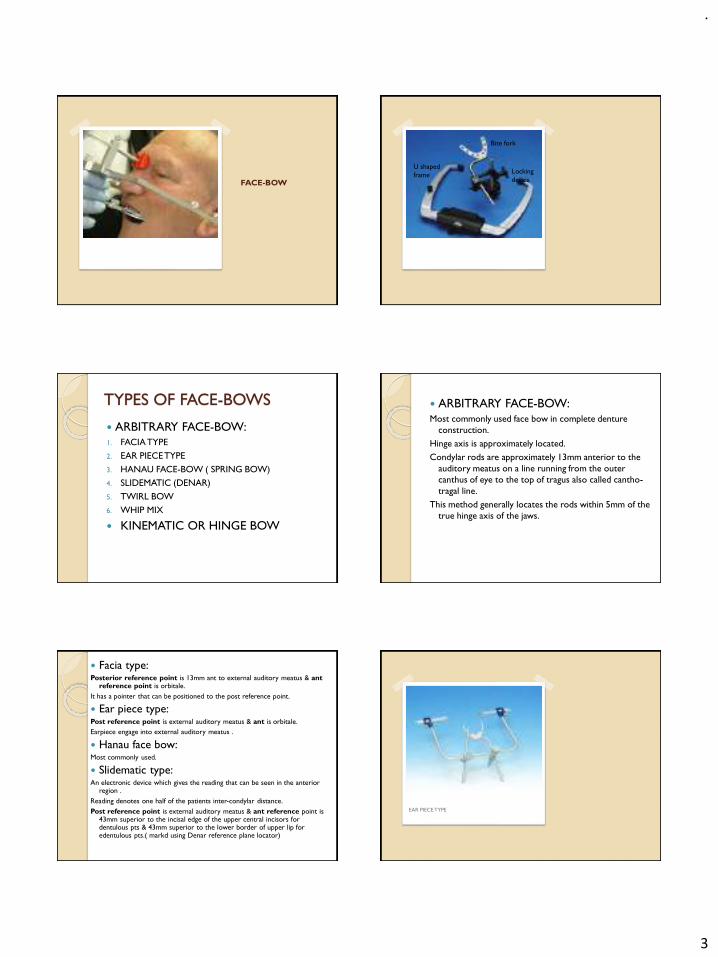
.
3
FACE-BOW
Bite fork
Locking
device
U shaped
frame
TYPES OF FACE-BOWS
ARBITRARY FACE-BOW:
1. FACIA TYPE
2. EAR PIECE TYPE
3. HANAU FACE-BOW ( SPRING BOW)
4. SLIDEMATIC (DENAR)
5. TWIRL BOW
6. WHIP MIX
KINEMATIC OR HINGE BOW
ARBITRARY FACE-BOW:
Most commonly used face bow in complete denture
construction.
Hinge axis is approximately located.
Condylar rods are approximately 13mm anterior to the
auditory meatus on a line running from the outer
canthus of eye to the top of tragus also called cantho-
tragal line.
This method generally locates the rods within 5mm of the
true hinge axis of the jaws.
Facia type:Posterior reference point is 13mm ant to external auditory meatus & ant
reference point is orbitale.
It has a pointer that can be positioned to the post reference point.
Ear piece type:Post reference point is external auditory meatus & ant is orbitale.
Earpiece engage into external auditory meatus .
Hanau face bow:Most commonly used.
Slidematic type:An electronic device which gives the reading that can be seen in the anterior
region .
Reading denotes one half of the patients inter-condylar distance.
Post reference point is external auditory meatus & ant reference point is 43mm superior to the incisal edge of the upper central incisors for dentulous pts & 43mm superior to the lower border of upper lip for edentulous pts.( markd using Denar reference plane locator)
EAR PIECE TYPE

.
4
Twirl bow:Doesn’t require any physical attachment to articulator.
Not commonly used for CD construction.
Mounting guide is used to mount the transfer rod to the articulator.
Easy to manipulate as no need to mount maxillary cast in articulator
Whip mix:In built hinge axis locator . Automatically locates hinge axis when ear piece
placed in external auditory meatus .
It has nasion relater assembly with a plastic nose piece , this determines ant
reference point.
KINEMATIC FACE BOW:Used for fabrication of FPD & full mouth rehabilitation, generally not for
CD.
Action of face bow:It helps to orient the cast in pts terminal hinge axis.
The terminal hinge position is most retruded hinge position & is
learnable, repeatable & recordable.
It coincides with centric relation n 12-15 degree pure rotational
movement of joint is possible.
.
1
Geriatrics jag
Dr. Prajakta Barapatre
• Introduction• Definitions• Aging• Sequelae of aging• Oral changes in aging• Geropsychiatric disorders• Nutritional deficiencies• Pharmacology and aging• Drugs in dental practice• Prosthetic considerations• Conclusions
DEFINITIONS :
GERIATRICS :
The branch of medicine or dentistry that treats the problemspeculiar to the aging patient, including the clinical problems ofsenescence and senility.
GERODONTICS :
The treatment of dental problems of aging persons orproblems peculiar to advanced age.
GERODONTOLOGY :
The study of the dentition and dental problems in aged oraging persons.
People who are above the age of 65 years are termed asgeriatric persons.
AGING :
The aging process may be defined as “the sum of allmorphologic and functional alterations that occur in anorganism, and lead to functional impairment, which decreasesthe ability to survive stress.”
• Aging is manifested at all levels.
• The changes seen are not dramatic, but with time leads toexponentially increasing mortality rate at the populationlevels.
THE BIOLOGY OF AGING :
It is difficult to delineate where the normal aging process endsand the disease process begins.
FACTORS INFLUENCING AGING :
Genetic factors :
▪ Mutations
▪ Species specific life spans
▪ Sex
▪ Parental age
▪ Premature aging syndrome
▪ Cells in culture
ENVIRONMENTAL FACTORS :
▪ Physical and chemical components – radiation
▪ Biologic factors – nutrition
▪ Pathogens and parasites
▪ Tropical countries
▪ Socio-economic factors
➢ Low income groups
➢ Bad housing
➢ Poor working condition
➢ Stresses of life
.
2
BIOLOGIC THEORIES OF AGING :
Genetic theories Non genetic theories
Error theories Immunologic theories
Somatic mutations Free-radical theory
Reduncies Cross linking theory
Genetically programmed senescence
Metabolic rate or wear and tear theory
Disposable soma theory
PHYSIOLOGY OF AGING :
Physiological deterioration – increases with age
It reduces physiological capacity and the ability to meetchallenges. It is progressive. Major contributing factor to death ofthe extremely old.
CENTRAL NERVOUS SYSTEM :
▪ Impairment of learning and memory after 70 yrs.
▪ Slowing of central processing
▪ Decrease in the brain size and weight
▪ Deterioration of the motor systems
➢ Decrease function of the extrapyramidal system
✓ Cerebellar function
✓ Muscular strength
➢ Increase in the
✓ Movement time
✓ Reaction time
➢ Sensory systems
Loss of
▪ Vibratory perceptions in lower extremities
▪ Touch
▪ Taste
▪ Smell
▪ Hearing
▪ Vision
➢ Sleep
▪ Shortening of sleep time
▪ Increased multiple brief awakening
Special senses
➢ Neuro-muscular system
▪ Loss of muscle mass
▪ Loss of muscle strength
▪ Loss of muscle performance
CARDIO-VASCULAR SYSTEM :
Decrease in
▪ Intrinsic heart rate
▪ Mean maximum HR during exercise
▪ Cardiac output
▪ Oxygen consumption
Increase in
▪ Peripheral resistance
▪ Muscle stiffness
▪ Contraction period
▪ Thickness of walls of aorta
RESPIRATORY SYSTEM :
▪ Increase in residual volume
▪ Decrease in expiratory reserve volume
▪ No change in total lung capacity
▪ Marked changes in airflow
KIDNEY AND BODY FLUIDS :
Loss of
▪ Weight of kidney
▪ Glomeruli
Deterioration of function
▪ Progressive declination in renal blood flow
▪ GFR (glomerular filtration rate)
GASTROINTESTINAL SYSTEM :
▪ Disordered contractions
▪ Spontaneous gastro-oesophageal reflex
▪ Slow gastric emptying
▪ Loss fat absorption
▪ Very slight impairment of protein digestion
.
3
▪ Reduction in calcium absorption
▪ Decreased secretion by gastric glands – less volume andconc. of
✓ HCl
✓ Intrinsic factor
✓ Pepsin
ENDOCRINES :
➢ Adenohypophysis – secretion of thyrotropin is blunted
➢ Neurohypophysis – greater release of antidiuretic hormone
➢ Thyroid - Slight decrease in T4 (thyroxine)
- Cortisol secretion is decreased
Aldosterone – decreased
➢ Insulin – decreased sensitivity of the target tissues to the actionof insulin – glucose intolerance.
REPRODUCTION :
Men
➢ Decline in sexual interest, drive and vigor
➢ Increase in plasma conc. of LH (leutenizing hormone) and FSH(follicle stimulating hormone)
Women
➢ Marked decline in estrogen concentration after menopause
MISCELLANEOUS :
➢ Loss of lean body mass
➢ Body fat increase with age
➢ Decrease in BMR
➢ Reduced ability to maintain body temperature
➢ Immune system.
ORAL CHANGES IN AGING :
Oral mucosa : The clinical picture is one that of atrophy
• Loss of elasticity and stippling
• More susceptible to injury
• Decreased repair potential
• Frequent application of soft liners.
Skin changes :
• Wrinkled, dry, patchy pigmentation
• Loss of elasticity and fine pattern.
• Diminished bulk of muscles, fat and connective tissue –
drooping of skin into folds and creases.
Gingiva :
• Loss of stippling
• Oedematous appearance
• Thin keratinized layer
• Tissue is easily injured
Lips :
• Angular cheilitis
➢ Vit B deficiency
➢ Dehydration
Teeth :
Enamel
➢ Attrition
➢ Erosion
➢ Abrasion
➢ Fluoride content is increases
➢ Enamel cracks – increases
➢ Enamel lamellae – increases
➢ Cementum – increase in thickness
➢ Dentin - Secondary dentin formation
Obturation of dentinal tubules
Pulp : Fibre - Increased
- Blood supply – reduces
- Pulpstones – increases
SALIVARY CHANGES :
Salivary flow reduces
Medication - Depression
- Insomnia
Salivary gland atrophy
PHYSICAL CHANGES :
Viscous ropy
• Plaque formation and growth of cariogenic bacteria
TREATMENT OF XEROSTOMIA :
Increase intake of water
• Frequent mouth rinses
• Lubricating jelly
• Silicone fluid
• Semisolid denture adhesives – decrease irritation of the tissues.
• Temporarily increases denture retention
• Use of silogogues – pylocarpine hydrochloride or nitrate, 5mgbefore meals.
.
4
• Sucking on sour candy
• Nicotinamide 250 to 400mg tid for 2 weeks.
EFFECTS OF AGING :
• Thinning of cortical bone
• Increase in porosity
• Loss of trabecular
• Cellular atrophy
• Sclerosis
Maxilla – narrower
Mandible – wider posteriorly
TONGUE AND TASTE :
• Smooth, glossy or red and inflamed in appearance
• Disturbed sensation – taste
• Soreness, burning (post menopausal women)
• Varicose veins on the ventral surface
TONGUE SIZE :
Does not vary with age but over development of intrinsic muscles,hence larger tongue (loss of teeth mastication and to keep theloose denture).
IMPACT OF ENVIRONMENTAL AND SOCIAL FORCES ONAGING :
An older person’s life is basically roleless, unstructured by thesociety, and conspicuously lacking in norms. Rosow (1974).
GENERAL MEDICAL ASPECTS OF AGING
• CARDIOPULMONARY DISORDERS :
➢ Valvular heart disease
➢ Cardiac arrhythmias
➢ Coronary artery disease / ischemic heart disease.
➢ Hypertension
➢ Congestive heart failure
➢ Chronic bronchitis/emphysema.
• NERVOUS SYSTEM DISORDERS :
➢ CVA (cerebrovascular accidents) or strokes
➢ Parkinson’s disease
• RHEUMATOLOGIC DISORDERS :
➢ Temporal arthritis
➢ Osteoporosis
➢ Osteoarthritis
• MISCELLANEOUS DISORDERS :
➢ Leukemia
➢ Iron deficiency anemia
➢ Diabetes mellitus
➢ Thyroid disorders
➢ Urinary incontinence
GEROPSYCHIATRIC DISORDERS :
• Situational disorders :
Associated with emotional crisis or prolonged situational stress.
• Improper oral hygiene
• Sustained muscular tension.
✓ Bruxism
✓ Atypical facial pain
• Burning mouth and/or tongue.
Such patients should be treated with compassion, respect and
willingness to comfort them.
AFFECTIVE DISORDERS :
Depression :
Usually co-operative
▪ Appear to forget clear instructions.
▪ Fatigue easily and require several short appointments
▪ Side effects of anti-depressants :
▪ Burning mouth
▪ Postural dizziness
▪ Excitement
▪ Tachycardia
▪ Overactivity
▪ Rapid speech
▪ Confusion.

.
5
ANXIETY DISORDERS :
• Apprehensiveness
• Worry
• Agitation
• Tachycardia
• Dizziness
• Weakness
• Visual and gastro intestinal disturbance
• Fatigue and headache
• Insomnia
• Sometimes depressive mood elements.
TREATMENT :
• Benzodiazepines
• Tricyclic antidepressants.
• Disorders of cognitive function :
• Dementia, deliria and toxic confusional states.
PREMEDICATION :
• Aggressive, confused or frightened patients.
• Haloperidol 1-2 mg
• Thiothixine 2-5 mg. one hour before the treatment.
• Thioridazine 25-50 mg the night before the procedure.
PARANOID STATES :
Paranoid is a group of symptoms involving irrationalsuspiciousness on others.
CHRONIC MENTAL DISORDER PERSISTING INTOLATE LIFE :
Chronic schizophrenics who survive into their 60’s or 70’soften display no florid psychotic symptoms, showing only passivity,impoverishment of social, intellectual and emotional life, social andfinancial dependency and occasional odd habits.
They neglect even an extensive oral disease.
AGING AND NUTRITION :
The diagnosis of a nutritional deficiency-stomatitis mustalways be consistent with a background of nutritional impairmentand substantiated by a conservative interpretation of the dataderived from a careful and complete diet survey, a probing medicalhistory and physical examination, and appropriate laboratory androentogenographic determination.
ETIOLOGY OF DIETARY DEFICIENCY :
• Lack of proper food intake
➢ Low income and lack of knowledge on how to spend themoney available for food to the best advantage.
➢ Physical handicaps, debility, lack of mobility which makespreparation of food difficult
➢ Poor facility.
➢ Poor dentitions, or improper dentures
➢ Depression boredom, anxiety and loneliness.
• Disease which interfere with
➢ Digestion
➢ Absorption
➢ Utilization of foods.
Eg: Oral cancers
• Chronic ulcerative lesions
• Diverticulosis → presented by constipation
• Atrophic gastritis
• Liver dysfunction
ORAL SYMPTOMS OF NUTRITIONAL DEFICIENCIES :
The symptoms may antidate, coincide, with, or follow theappearance of deficiency induced signs.
They are represented by
• Burning
• Soreness
• Tenderness
• Dryness
Loss of diminution of taste (Ageusia or dysgausia)
SORENESS AND BURNING OF TONGUE :
• Iron deficiency anemia
• Vit B12 responsive pernicious anemia.
STOMATODYNIA :
• Pellagra
• Sprue
• Kwashiorkor
• Scurvy
• Nutritional microcytic anemia
XEROSTOMIA :
• Vit A deficiency
• Ariboflavinosis
• Pellagra pernicious anemia
.
6
• Iron – deficiency anemia
• Sprue
• Dehydration
• Sialorrhea
▪ Acute nutritional deficiency stomatitis
▪ Acute pellagra
• Impairment of taste sense :
▪ Pellagra
▪ Pernicious anemia
ORAL SIGNS OF NUTRITIONAL DEFICIENCY :
▪ Cheilosis
▪ Gingivitis
▪ Glossitis.
C.
ORIGINATE AS :
Gingivitis :
Deficiencies of niacin, tryptophan, and vitamin C.
Glossitis :
Niacin, folic acid, vit B12, pyridoxine, protein and irondeficiency.
TREATMENT OF NUTRITIONAL DEFICIENCIES :
General principles :
1. A well-balanced high protein (120 to 150 gm) diet should beadministered with adequate calories, vitamins, and minerals.
2. Therapeutic amounts of specific nutrients should be added as asupplement to the daily diet.
DAILY THERAPEUTIC DOSE :
• Folic acid 5 to 10mg
• Niacin amide 150 to 250 mg
• Riboflavin 10 – 15 mg
• Ascorbic acid 150-300 mg
• Vit- A 25,000 – 50,000 units.
• Vit-D 3,000 – 5,000 units
• Medicinal iron 200 – 400 mg (1.2 gm of ferrous sulfate)
• Vit B12 10-15 g (micrograms)
PHARMACOLOGYAND AGING :
General consideration :
• In general, elderly people use 30% of all prescribed medications(Nielsen et al 1981). Thus, it is important to know if drug dosagehas to be changed when older persons are considered.
• Significant changes in pharmacokinetics and pharmacodynamicsdo occur with increasing age.
Compliance :
1) The number of different drugs prescribed, and
2) The number of doses given per day of each drug.
• More than three different drugs and more than two doses forday of each drug decrease compliance significantly.
• Elderly patients are not necessarily more prone to non-compliance than younger patients.
ABSORPTION :
A series of physiologic functions in the gastrointestinal tractchange with age.
There is decrease in
▪ Gastric emptying rate
▪ Secretion of hydrochloric acid
▪ Gastrointestinal mobility
▪ Intestinal blood flow
▪ Efficiency of many active transport systems.
As a result, a higher plasma drug levels is found in elderly.
VOLUME OF DISTRIBUTION :
The total body weight declines steadily after the age of 50 years,because of loss of intracellular water and of lean body mass,while adipose tissue mass is increased.
CONSEQUENCES :
▪ Diminished functions like mastication
▪ Digestive problems
▪ Poor retention of dentures
▪ Susceptibility of mucosa to frictional irritation from denture
movement.
▪ Interference with patients ability to wear dentures.
EXCESSIVE SALIVA :
Transient – on insertion of denture. No reduction in salivary
output from the parotid gland whereas that of submandibular
gland is reduced.
Submandibular gland : 45% of total output
.
7
CLINICAL SIGNIFICANCE :
The volume distribution of lipid soluble drugs is higher,whereas that of water soluble drugs is decreased.
PROTEIN BINDING :
The concentration of serum albumin decreased withadvancing age.
In aged → 3.5 g/dl.
Young adults → 4-4.5 g/dl.
This causes on increased unbound fraction of drugs andinfluence the distribution of drugs.
METABOLISM :
The hepatic blood flow decreases with age and the rate ofmetabolism of high clearance drugs such as propranolol andlidocain whose elimination are highly flow dependent, is reduced inthe elderly.
The elimination of low clearance drugs depends primarily
on the activity of the hepatic microsomal drug metabolizing
enzymes. The enzyme activity per unit liver also decreased with
advancing age.
RENAL EXCRETION :
Renal function evaluated an the basis of insulin clearance or
by endogenous creatinine decreases considerably with age.
Young→ 20-22 mg/kg/24hr
Old → 10 mg/kg/24hr.
Dosage modifications are necessary primarily to drugs for which
the renal excretion of the parent compound or the active
metabolites is the major mechanism of elimination.
PHARMACODYNAMICS :
• Reduced hepatic synthesis of blood clotting factors with a
resulting greater sensitivity to the action of oral anticoagulants.
• Diazepam and nitrazepam (10mg) appear to result in greater
depression of the central nervous system.
ADVERSE REACTIONS :
Frequency of adverse drug reactions is greater in the elderly.
However, older persons take more medications and this must be
taken into consideration.
DRUGS IN DENTAL PRACTICE
ANTIBIOTICS :
• Water soluble antibiotics like penicillins, cephalosporins,aminoglycosides, tetracycline will be affected by the age –
dependent decrease in renal function.
• In contrast, lipid-soluble antibiotics like erythromycin,chloramphenicol are primarily metabolized in liver resulting inmore hydrophilic metabolites which are subsequently excretedby the kidneys.
PENICILLINS :
• Excretion of these drugs is much reduced in the elderlycompared to younger subjects.
• Because of high therapeutic index the modification of dosage tocompensate for reduced renal clearance is not necessary.
In general, normal doses of all penicillins can be safely
prescribed to all elderly patients regardless of age.
ERYTHROMYCIN :
• High therapeutic index.
• Therefore, normal dosages should be prescribed to all patients
irrespective of age.
METRONIDAZOLE AND TINIDAZOLE :
• It is advisable to use lower dosages of metronidazole in this age
group to avoid accumulation of active water soluble
metabolites when kidneys function is reduced.
• The excretion of tinidazole is unchanged in renal failure.
Aspirin (acetylsalicylic acid) : Clinically, normal dosages upto3gm/day can be prescribed, but they should be monitored forchronic salicylate toxicity which causes mental confusion andhyperventilation, which can be mistaken for a result of age itselfor a disease.
BENZODIAZEPINES :
Diazepam :
• The clearance of diazepam is unaffected by increasing age, butthe elimination of desmythyldiazepam is reduced in elderly.
• Short acting benzodiazepines like temazepam and triazolam havedecreased tendency to hang over symptoms and used in elderly.
• In general, moderation of doses should be exercised consideringhow easily elderly patients develop mental confusion and loss ofmemory.
.
8
LOCALANALGESICS :
• The clearance of lidocaine is reduced in elderly males, whilefemales donot exhibit significant difference from younger subjects.
• Concentrations greater than 5% are rarely required for infiltrationanalgesics.
• It is important to consider the interactions which may take placebetween the pressor amines in the analgesics and manyantihypertensives and antidepressants.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) :
• No significant age-dependent differences in the kinetics is found.
• Despite few and small alterations with advancing age, it seemsprudent to administer smaller dosage to the elderly, because theyare prone to adverse reactions such as gastric and intestinalhemorrhages, and edemas than younger subjects.
• Many NSAIDs decrease the action of diuretics, probably due tointeraction with the mechanisms of renal excretion.
ANTICOAGULANTS :
Age itself is not a contraindication for the use of anticoagulants.It is difficult to treat on an outpatient basis. The patients shouldbe monitored carefully and closely watched for the risk ofpotential drug interactions.
ORAL DISEASES CAUSED BY DRUGS :
Ulcerations of mucosa
• Salicylates
• Potassium
• Corticosteroids
• Pancreatic enzymes
• Emepronium
• Tetracycline
• Clindamycin
Stevens-Johnson syndrome• Sulfonamides
• Penicillins
Herpes• Immunosuppressive therapy
Candida infection• Corticosteroids
• Antibiotics
Xerostomia• Anticholinergics
• Antihistamines
• Cyclic antidepressants
• High doses of neuroleptics
• Opioids and
• Disopyramide
PROSTHETIC CONSIDERATIONS IN GERIATRICDENTISTRY :
Oral status and treatment needs :
In elderly populations the pattern of use of dental services
and the need and demand for dental treatment are clearly different
from that of younger populations.
Diagnosis and treatment planning :
A careful history and clinical examination of the elderly
patient are essential in attempting to clarify the patients demand and
need for prosthetic treatment.
SYSTEMIC FACTORS
NUTRITION :
• The elderly patients are very often deficient in one or severalnutrient or minerals.
• A decreased plasma concentration of thiamine, riboflavin, orfolic acid in elderly patients may be associated with reducedtolerance to removable dentures.
• Dietary supplements of proteins and minerals will increasetolerance to dentures.
DEBILITATING DISEASES :
• Systemic diseases, such as gastrointestinal disorders, diabetesmellitus, or arteriosclerosis, may enhance the symptoms andsigns of debility.
• As a consequence patients will often totally neglect oral and
prosthetic care. Any treatment should be postponed until the
patients general health is restored.
• For chronically ill patients, a professional oral hygiene care
must be scheduled to control caries and periodontal disease.
NEUROPHYSIOLOGICAL CHANGES :
• With advancing age there is degeneration of functional
elements in the central nervous system.
• Adaptation and learning becomes slow. The patients existing
dentures can be used as a template for the design of new
dentures, to make adaptation to new dentures more easy.
.
9
PSYCHIC CHANGES :
• Progressive cerebral involution in the elderly patient may resultin psychic changes which complicate the outcome of prosthetictreatment.
• Elderly patients often feel neglected and rejected.
• To receive some attention some mentally ill patients maycomplain of soreness produced by the dentures where no evidentsymptoms exist and may try to damage the dentures.
• When mental diseases are suspected, the patients physicianshould be consulted regarding an appropriate time for prosthetictreatment.
LOCAL FACTORS :
• Some diseases such as nutritional disorders, skin diseases orblood dyscrasias, may manifest themselves initially in the oralcavity and dentist may be the first person to evaluate the signsand symptoms.
FACTORS TO BE CONSIDERED DURING THE CLINICAL EXAMINATION
• Function of temporomandibular joint
• Size and tone of musculature
• Quantity and quality of saliva
• Tissue tone
• Health of the oral mucosa
• Dental and periodontal health
• Oral and denture hygiene
• Size and shape of alveolar ridges
• Interridge space and ridge relations
• Occlusal conditions
• Fit and extension of existing denture
ORAL PHYSIOLOGIC CHANGES :
• Progressive atrophy of the masticatory, the buccal, and the
labial musculature is a sign of aging. This may cause severe
reduction of chewing efficiency. Patient should be advised to
take adequate diet, which is easy to chew.
• Atrophy of buccal musculature may result in accumulation of
food especially on buccal denture flanges. The placement of
denture teeth buccal to the alveolar ridges may help establish
contact between the denture flanges and cheeks. However, this
may compromise the stability of the dentures.
• Reduced salivary secretion or xerostomia. Frequently, a
complication debilitating diseases e.g. diabetes, or treatment
with psychopharmacologic drugs.
This will result in
• Rampant caries
• Loss of denture retention
• Traumatic lesions
• Infections of oral mcuosa
Meticulous oral hygiene supplemented by mouth washes with
chlorhexidine and daily use of artificial saliva substitutes are
important means to reduce complications.
The regular use of removable dentures should be restricted in
patients with xerostomia.
ALVEOLAR RIDGE ATROPHY :
• Alveolar ridge atrophy is a continuing process of reduction of
the edentulous alveolar ridge which takes place at varying rates
in different individuals.
• Various anatomic, metabolic or mechanical factors are involved
in this process (Atwood 1979).
• There is no reliable way of reducing alveolar ridge atrophy but
the correction of metabolic alterations and meticulous denture
care may have a positive effect.
• The best way of preventing alveolar ridge atrophy is to maintain
some teeth or roots in the jaws for support of a removable
denture.
ORAL HYGIENE :
SALIVA
.
10
EXISTING DENTURES :
The design of existing dentures should be carefully evaluatedand related to the patient’s complaints. Obviously, the new denturesmust correct faults of the existing dentures. However, in order tofacilitate neuromuscular adaptation the new dentures should bedesigned with careful consideration to the design of existingdentures.
GUIDELINES FOR REHABILITATION WITH REMOVABLEPARTIAL DENTURES :
Functional aspects :
Removable partial dentures may be indicated in elderlypatients in order 1) to restore function of the masticatory system byproviding adequate occlusal support and mastication, 2) to preventdevelopment of occlusal disturbances and TMJ-dysfunction.Furthermore, the patient’s demand for improved esthetics andphonetics may be achieved by placement of a removable partialdenture.
In elderly patients distal extension removable partial denturesmay be indicated.
1. To restore esthetics or phonetics
2. To improve mastication
3. In Patients with significant signs and symptoms of TMJ-disturbances and extensive loss of teeth.
4. In a jaw opposing a complete denture to increase functionalstability of the complete denture
DESIGN OF REMOVABLE PARTIAL DENTURES INELDERLY PATIENTS :
THESE GUIDELINES COULD BE SUMMARIZED ASFOLLOWS :
• The design should be as simple as possible with saddles, majorconnectors and minor connectors avoiding contact with the freegingiva and contacting the alveolar ridge or the palateapproximately 3 mm from the teeth surfaces in order to reduce thenegative effect on oral hygiene.
• Saddles should be tooth supported, if possible; in distal extensionremovable partial dentures occlusal rests should be placed in sucha way that tilting of abutment teeth will not take place.
• Major connectors, minor connectors, reciprocating clasp arms,and occlusal rests should be rigid in order to withstand anddistribute occlusal forces.
In elderly patients excessive occlusal wear of the naturalteeth may be seen frequently which makes restoration of theocclusion mandatory. This is both clinically and technically acomplicated treatment. Placement of removable partial dentureswith onlays on the abutments teeth to obtain a harmoniousocclusion is a solution to the problem that is relatively inexpensivebut which requires excellent oral hygiene.
GUIDELINES FOR REHABILITATION WITH COMPLETEDENTURES :
Complete denture prosthodontics involves the replacementof the lost natural dentition and associated structures of the maxillaand the mandible in patients who have lost their remaining teeth orare soon to loose them.
OVERLAY DENTURE :
Today, with the stress on preventive measures inprosthodontics, this type of treatment is a realistic alternative toconventional complete dentures in most patients with someremaining teeth.
The advantages of treatment with overdentures in elderlypatients are the following:
• provide support for the dentureThe roots and periodontalligament membrane will aid in minimizing future loss of thealveolar ridge.
• pro-prioceptive response
• retention to the removable denture.
of the lips.
In geriatric dentistry treatment with overlay dentures isparticularly relevant in the following situations:
• In patients with clinical signs of muscular hyperfunction of themasticatory apparatus, e.g. severe attrition, bruxism.
• In patients where there are no overt signs of a decreased verticaldimension of occlusion but where an increase of the verticaldimension of occlusion is indicated to create sufficient space for adenture.
.
11
THE CLINICAL TREATMENT PLAN INCLUDES :
1. Removal of posterior teeth 3-4 weeks prior to dentureconstruction. It is important to maintain one or two occlusalcontacts in the premolar region to maintain the verticaldimension of occlusion.
2. Primary impression
3. Functional secondary impression in an individual tray
4. Recording of the jaw relationship in centric relation and at anacceptable vertical dimension of occlusion.
5. Arrangement of posterior teeth
6. Arrangement of anterior teeth which are usually placed in thesame position as the natural teeth to support neuromuscular andpsychologic adaptation to the dentures.
6. Alteration of the cast to compensate for soft tissue changes.Alterations for soft tissue changes. Alterations to compensatefor bone changes are only indicated for esthetic reasons andwhen there are severe bony undercuts.
7. After extraction and adjustment of the alveolar ridge thedenture is inserted, the occlusion correction and the patientinstructed to return the following morning.
Postoperative care includes instruction in oral and denturehygiene and regular control of occlusion and fit of the dentures.Soft relining materials, and tissue conditioning material may beused as an effort to keep the occlusion of the teeth, the fit of thedenture and the tissue changes in harmony. Gross tissuechanges are usually completed 3-6 months after extraction. Atthat time a permanent denture is constructed or the immediatedenture is relined or rebased.
PROGNOSIS: DENTALAND PROSTHETIC CARE :
Regular recall of denture wearers should take place for the
following reasons :
• In order to control development of microbial plaque on tooth
surfaces and on dentures. A denture is a predisposing condition
to caries, periodontal disease and denture-induced stomatitis .
• In order to control development of functional disorders of the
masticatory system resulting from changes of occlusal
relationships. Such changes may occur due to breakage of clasps
and rests, wear of denture teeth and atrophy of the alveolar ridge.
• In order prevent mechanical injury to periodontal and denture-
supporting tissues.
FIXED PROSTHODONTICS IN GERIATRIC DENTISTRY :
Patients with advanced oral diseases and multiple missing
teeth jeopardizing an optimal masticatory function can now be
treated successfully irrespective of age. Furthermore, treatment
success can be maintained for many years provided an adequate
maintenance care program is established.
CAUSE-RELATED THERAPY :
Besides improving chewing comfort fixed reconstructions
generally offer better accessibility for oral hygiene than do
removable prosthetic appliances.
It is important to gain a clear perception of the patient’s
motivation for dental treatment and desire to maintain teeth, as wellas his/her ideas of chewing comfort and the need for improvedesthetics. Also, information about the willingness to maintain ahealthy dentition is of utmost importance. Every single toothshould be diagnosed for caries, periodontal and pulp disease as wellas for masticatory function.
A comprehensive treatment plan for the elderly patientencompasses four distinct phases:
1. SYSTEMIC PHASE :
Due consideration is given to the medically compromisedpatient. The risks for the patient and for the operator are identified.If necessary , the patient’s physician is consulted and possiblemedication administered.
2. HYGIENIC PHASE :
The goal of this treatment phase is the establishment ofoptimal oral hygiene. Instruction of oral hygiene is accompanied bymotivation of the patient and by thorough scaling and root planing.“Hopeless” teeth are extracted.
3. CORRECTIVE PHASE :
This includes further periodontal treatment, endodontictherapy, restoration of teeth with alloplastic material and theincorporation of fixed or removable partial restorations.Occasionally, occlusal therapy, such as the application of a bitesplint followed by occlusal adjustment, or orthodontic therapy mayalso be performed during this phase. Prior to reconstructing thepartially edentulous patient retained and/or impacted teeth/rootsshould be removed, if indicated. During the entire corrective phaseoral hygiene is monitored.
.
12
4. MAINTENANCE PHASE :
A maintenance care program with regular recall visits atfrequent intervals (3-4 months) should be established in order toassure a favorable prognosis. During this phase attention shouldalso be given to possible technical failures in the reconstruction.
The necessity of a complete dentition with 14 antagonisticocclusal units for maintaining adequate function of the masticatorysystem is important as a shortened dental arch may act as anetiologic factor for functional disturbances in the masticatorysystem. This is necessary for providing a subjective chewingcomfort.
The need for replacing lost teeth beyond the secondpremolar might not be indicated as previously thought, and solimited and individual treatment planning should be givenpreference over ‘ideal’ professional concepts of optimal function.
POST THERAPEUTICAL MAINTENANCE :
Maintenance care should include the continuous monitoring
of the bridge work, assessment of pulp vitality and patients need for
fluoride treatment.
Recall visits will reemphasize the necessity for good home
care and correct any irregularities in optimal plaque control. Topical
fluorides should be applied at each recall.
ORAL IMPLANTS IN THE AGED :
An implant can be defined as an alloplastic device placed in
the body for a specific functional purpose. The purpose of the oral
implant is to create stable retention of prosthetic appliances.
SURGICALAND MEDICALASPECTS :
Pre operative measures for improving the prognosis ofimplant therapy should be undertaken, the nutritional status shouldbe improved, anti coagulation therapy stopped and antibioticsadministered for the prevention of infections.
Surgical procedures can be done under local anaesthesia.Nervous patients should be sedated with an appropriatepreparation, for example a benzodiazepine.
Surgery must be performed as quickly and as atraumaticallyas possible to reduce strain on the aged patient and tissues inquestion. Asceptic surgical procedures should be followed toprevent postoperative complications. When the osseous implantsites are being prepared, heat due to friction has to be reduced to aminimum by continuous irrigation with sterile saline and byminimizing drill speed.
In aged patients susceptible to local infections, the area of
surgery should be protected by antibiotics.
During healing an optimal diet containing enough
calories, protein, vitamins and supplementary calcium is
essential.
It is also important to give the patient or his next kin
careful and detailed instructions to be followed during the post
operative period.
If all the above said principles are followed, implant
surgery seems to be successful.
INDICATIONS :
Indications for treatment with implants in the aged are as follows :
• A. Insufficient retention of prosthetic devices due to,
• Extensive resorption of the alveolar bone.
• Hypersensitive and highly vulnerable mucosal conditions.
• Defects of the jaw after trauma or tumour resection.
• Disturbed innervation of the oral and perioral muscles followingtrauma of cerebrovascular diseases.
B. Functional disturbances, preventing the patient from wearingprosthetic devices due to,
• Age related adaptation difficulties to dentures.
• Severe nausea and vomiting reflexes
C. Psycho-social inability to accept a prosthetic device in spite ofadequate morphological and functional prerequisites.
CONTRA INDICATIONS : These are
• Oral rehabilitation with conventional prosthetic devices whichhas already been accepted.
• Insufficient residual bone volume with poor quality.
• Lack of motivation for treatment with implants.
• Lack of motivation for sufficient oral hygiene measures
• General medical conditions. Eg: diabetes and severeosteoporosis.
• Alcoholic and / or narcotic misuse.
• Special oral conditions as seen after radiation therapy.
• Certain psychological conditions and other mental conditionsthat might indicate negative psychological outcome.
• Inability to perform meticulous postoperative care and long standing maintenance programs.
.
13
IMPLANT PROCEDURES :
There are at present two different, well-documented implant
designs which are shown to be successful in the aged patients.
They are,
1. Osseointegrated titanium implants ad modum Branemark
especially suitable for edentulous cases.
2. Enosseous implants of aluminium oxide ceramics ad modum
Schulte for single tooth loss.
IMPLANTS AD MODUM BRANEMARK :
After a careful pre operative analysis regarding the patientsgeneral, physical and psychological health including an evaluationof the oral condition from a prosthodontic surgical and radiographicpoint of view, the treatment is performed in three stages.
Stage I : titanium threaded implants are installed according to anelaborate surgical procedure.
An undisturbed and relatively long period (5-6 months) ofhealing and osseointegration of the implants is necessary in thetreatment of the aged.
Stage II : after the healing period the abutment connection issurgically achieved.
Stage III : about 2 weeks later, the prosthetic procedures should befinished.
IMPLANTS AD MODUM SCHULTE :
These implants are made of aluminium oxide and produced
in different sizes.
The implants are inserted according to the surgical principles
to achieve osseointegration. During healing the implant is not
protected by covering mucosa. After a healing period of about 3
months, treatment is completed by application of a prosthetic
reconstruction on the implant.
The frequency of successful cases is about the same as for
titanium implants and covers a period of 8 years. Both systems have
their special advantages and indications.
CONCLUSION :
The outcome of prosthetic treatment in geriatric dentistry is
determined by several factors such as the general and oral health
status of the patient, the patient’s degree of cooperation, economic
resources, biologic and technical quality of prosthetic materials,
and the prosthodontist’s knowledge, judgment and technical
abilities. Thus, insight in clinical and technical aspects of prosthetic
treatment is important in order to be able to successfully treat
elderly patients who are partially or totally edentulous. However,
the greatest challenge to the clinician is to make a choice between
treating the patient, with the risk of producing iatrogenic disease, or
not treating the patient, with the risk of more damage occurring to
the masticatory system.
.
1
GINGIVAL RETRACTION
Dr Prajakta Barapatre
Definition
⚫ Gingival displacement/Gingival retraction:The deflection of the marginal gingiva away from a tooth
⚫ The gingiva must be displaced to make a complete impression and some time even to permit completion of the preparation and cementation of the restoration
Finish Line Exposure
The marginal fit of a restoration is essential in preventing the recurrent caries and gingival irritation, hence the finish line of the tooth preparation must be reproduced in the impression
Obtaining a complete impression is complicated when some or all of the preparation finish line lies at or apical to the crest of the free gingiva .
Control of fluid in the sulcus , particularly when a hydrophobic impression material is used ,is also necessary , because liquids can cause an incomplete impression of the critical finish line area .
Objectives of gingival retraction
To widen the gingival sulcus to provide access for the impression materials to reach the sub-gingival margins and to record accurately the finished margins
Recording the contour beyond the finish line helps to correctly contour the restoration and smoothly blend the margins of the restorations with the unprepared tooth structure.
While cementing a restoration ,it helps in removal of excess cement without injuring the gingival tissue.
In case of sub-gingival preparation ,it prevents injury to the crest of the gingiva.
Methods for gingival retraction
➢ Mechanical method
• rubber dam
• cotton twills with ZnoE cement
• copper band impression
• temporary acrylic resin copings
➢ Mechanico-chemical methods
• Various chemicals used
• Advantages and Disadvantages
• Classification of retraction cords
• Technique for Gingival cord retraction
Methods for gingival retraction
➢ Rotary Gingival curettage
• Criteria
• Technique➢ Electro surgery
• History• Mechanism of Action• Types of current• Tissue considerations• Advantages and disadvantages• Contraindications• Technique
➢ Recent Advances in Gingival Retraction material• Muracil retraction strips• Magic foam.• Expysyl retraction paste.

.
2
Mechanical Method
First to be developed.
Physical displacement of gingival tissue.
Used alone or in conjunction with other methods
a.Rubber dam• Heavy and extra heavy rubber dams were used.
• Retraction is done by rubber dam or clamp.
• Produced retraction by compression.
• Generally it is used when a limited number of teeth in one quadrant are being restored and in situations in which preparations do not have to be extended very far subgingivally
• Advantages
control of seepage and hemorrhage.
ease of application.
• Disadvantages
full arch models cannot be made.
cannot be used with polyvinyl siloxane material.
b.Cotton twills with ZnoE cement
• Employs gentle pressure over a period of time.
• ZnoE mixed into creamy consistency,
• Cotton twills rolled into this mass and then on a towel to gain compactness.
• Prevents sticking of pack to the instruments and gives ease in handling.
• Should reflect the tissue laterally.
• Pack held in place with fast setting Znoe cement.
• Min.48 hrs but not >7 days.
c.Copper Band impressions
Physically displacing the gingiva was one of the first methods used for insuring adequate reproduction of the preparation finish lines
a copper tube can serve as a mean of carrying the impression material as well as to displace the gingiva to expose the finish line.
TECHNIQUE A copper band is welded
to form a tube corresponding to the size of the prepared tooth . one end of the tube is festooned ,or trimmed to follow the profile of the finish line. After positioning and contouring the tube over the prepared tooth, it is filled with modelling compound and then it is seated carefully in place along the path of insertion of the tooth preparation and the impression is made .
Disadvantag:It can cause injury to the gingival tissues.
Chemico mechanical method
It is a method of combining a chemicalwith pressure packing ,which leads toenlargement of the gingival sulcus as wellas control of fluids seeping from thesulcus .
gingival retraction cord soaked in achemical (which promote gingivalcontraction) will provide better gingivalretraction compared to a plain retractioncord .
CHEMICAL USED
These are generally localvasoconstrictors which causestransient gingival shrinkage
(A) 8% racemic epinephrine
(B) Aluminium chloride
(C) Alum(aluminium potassium sulphate )
(D) Aluminium sulphate
(E) Ferric sulphate

.
3
Ideal requirement for chemical used with gingival retraction cords
❖ It should produce effective gingivaldisplacement and haemostasis.❖ It should not produce anyirreversible damage to the gingiva .❖ it should not have any systemic sideeffect .
contraindications for epinephrine
❖ CVS disease❖ Diabetes❖ Hyperthyroidism❖ Known hypersensitivity to epinephrine❖ patient taking ganglionic blocker ,orepinephrine potentiating drug
Newer gingival retraction agents are
❖ Phenylephrine hydrochloride 0.25 %❖ Oxymetazoline hydrochloride 0.05 %❖ Tetrahydrozoline hydrochloride 0.05 %
❖ The amount of epinephrine absorbed is highly variable,depending on the degree of exposure of the vascular bed as well as thetime of contact and the amount of medication in the cord .
❖ The amount of epinephrine absorbed from 2.5 cm of typicalretraction cord during 5 to 15 minutes in the gingival sulcus is 71 µg .It isapproximately 1/3 rd the maximum dose of 0.2 mg (200 µg ) for a healthyadult and nearly twice the recommended amount of 0.04 mg (40 µg ) fora cardiac patient .
❖ If cord is placed around more than one tooth ,if more than oneimpression is made of a single tooth , and /or if the epinephrine-containing anesthetic is used , a patient could easily exceed therecommended maximum dose of epinephrine .
❖ WEIR and WILLIAMS (1984) ,in an in vivo study of 120 humanteeth ,found no significant difference between the hemorrhage controloffered by cords impregnated with aluminum sulphate ,and thoseimpregnated with epinephrine
Some silent point about epinephrine
TECHNIQUECORD PLACEMENT IS A GENTLE MOVE , NOT A POWERPLAY .❖ The operating area should be dry. Fluid control should be done with anevacuating device and the quadrant containing the prepared tooth is isolatedwith cotton rolls.
❖ Hemorrhage can be controlled by using haemostatic agent likehemodent liquid (aluminium chloride)
Retraction cord is looped around thetooth and held tightly with the thumband forefinger and apply slighttension in an apical direction
Cord is twisted to make ittight and small
Placement of cord isbegun by pushing it intothe gingival sulcus onthe mesial surface of thetooth .It should be tackedlightly into the distalcrevice .
As the cord is being placedsubgingivally ,the instrumentmust be pushed slightly towardsthe area already tucked intoplace .If the force of theinstrument is directed away fromthe area previously packed, thecord already packed will bepulled out .
Occasionally it isnecessary to hold the cordwith one instrument whilepacking with the second .
The instrument used forpacking should be angledslightly towards the root tofacilitate the sub-gingivalplacement of the cord
If it is held parallel to the long axis of thetooth , the cord will be pushed against thewall of the gingival crevice ,and willrebounce .
Excess cord is cut off near the interproximal area such that a slight overlapof the cord occur in this region . if theoverlap occur on the facial and lingualsurfaces , the gingival finish line in thatarea may not be replicated properly in theimpression .At least 2-3 mm of cord is left protrudingout-side the sulcus so that it can begrasped for easy removal .
After cutting off the excessat the mesial end ,thedistal end of the cord is atucked in until it overlapsthe tucked mesial end .

.
4
TECHNIQUE (contd)
The cord can be packed with specialinstrument like Fischer packing instrument.It is a double ended, serrated or smoothedges stainless steel instrument facilitatesplacing of retraction cord around the tooth.Both ends of the retraction cord packers areshaped at an angle which allows the cord tobe packed swiftly right around the tooth.
.Retraction cord scissors
Blunt-tipped retraction cord scissorswith less risk to tissue. 1/2" long springsteel blades flex for a consistent cut tothe tip and a longer service life.Uniband spring handle provides forsmooth control.
❖ After 4-6 minutes , the cord should beremoved slowly in order to avoid bleeding .If activebleeding persists , a cord soaked in ferric sulphateshould be placed in the sulcus and removed after 3minutes
❖ The impression should be made onlyafter cessation of bleeding .
❖ The retraction cord must be slightlymoist before removal . removing dry cord from thecrevice can injure the delicate epithelial lining of thegingiva .
Classification of retraction cords
a. Depending on the configuration TwistedKnittedPlain
b. Depending on surface finishwaxedunwaxed
c. Depending on the chemical treatment
plain impregnated
d. Depending on number strandssingle double-string
e. Depending on the thickness (color
coded)
black 000
yellow 00
purple 0
blue 1
green 2
red 3
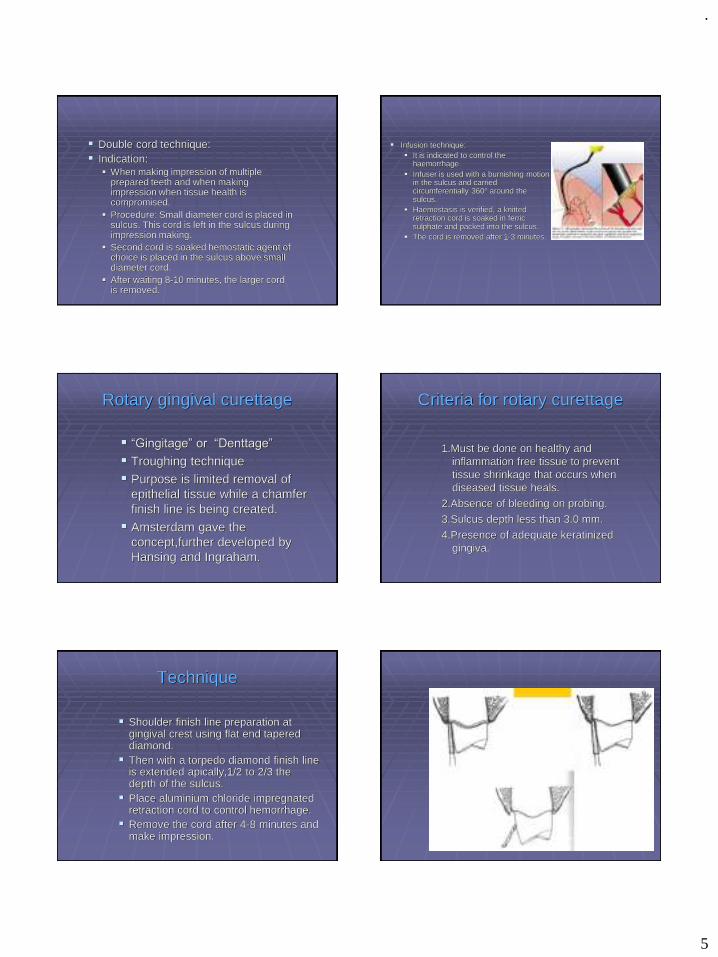
.
5
▪ Double cord technique:▪ Indication:
▪ When making impression of multiple prepared teeth and when making impression when tissue health is compromised.
▪ Procedure: Small diameter cord is placed in sulcus. This cord is left in the sulcus during impression making.
▪ Second cord is soaked hemostatic agent of choice is placed in the sulcus above small diameter cord.
▪ After waiting 8-10 minutes, the larger cord is removed.
▪ Infusion technique:▪ It is indicated to control the
haemorrhage.▪ Infuser is used with a burnishing motion
in the sulcus and carried circumferentially 360° around the sulcus.
▪ Haemostasis is verified, a knitted retraction cord is soaked in ferric sulphate and packed into the sulcus.
▪ The cord is removed after 1-3 minutes.
Rotary gingival curettage
▪ “Gingitage” or “Denttage”
▪ Troughing technique▪ Purpose is limited removal of
epithelial tissue while a chamfer finish line is being created.
▪ Amsterdam gave the concept,further developed by Hansing and Ingraham.
Criteria for rotary curettage
1.Must be done on healthy and inflammation free tissue to prevent tissue shrinkage that occurs when diseased tissue heals.
2.Absence of bleeding on probing.3.Sulcus depth less than 3.0 mm.
4.Presence of adequate keratinized gingiva.
Technique
▪ Shoulder finish line preparation at gingival crest using flat end tapered diamond.
▪ Then with a torpedo diamond finish line is extended apically,1/2 to 2/3 the depth of the sulcus.
▪ Place aluminium chloride impregnated retraction cord to control hemorrhage.
▪ Remove the cord after 4-8 minutes and make impression.

.
6
Electrosurgery
HistorySchillinburg stated that the use of heat as
surgical tool was known to Egyptians about 3000BC.
Experiments of d’Arsonvol (1891) demonstrated that electricity at high frequency will pass through a body without producing a shock (pain or muscle spasm), producing instead an increase in the internal temperature of the tissue.
This discovery was used as the basis for eventual development of electrosurgery.
Mechanism of action
► Controlled tissue destruction.
► Current flows through a small cutting electrode.
► Producing high current density and rapid temperature rise .
► Cells directly adjacent to the electrode are destroyed due to this temperature increase.
Types of current
1.Fully Rectified current (modulated)▪ continuous flow of current
▪ good cutting characteristics
▪ enlargement of gingival sulcus
2.Fully Rectified current (filtered)▪ continuous current wave
▪ excellent cutting characteristics
▪ less injury than modulated current
2.Partially rectified current (damped)
• Considerable tissue destruction.
• Slow healing.
• Used for spot coagulation.
3.Unrectified current (damped)
►Recurring peaks of current that rapidly diminish.
►Causes intrinsic dehydration and necrosis.
►Slow and painful healing.
►Not used in dental surgery.
.
7
Tissue considerations
► Keep electrode in motion.
► Appropriate current setting.
► Larger the electrode ,greater the current required.
► 5-10 seconds between applications.
► Patient should be properly grounded.
► Tissue must be moist.
► Electrode must remain free of tissue fragments.
► Electrode must not touch any metallic restorations.
Advantages
►Clear operating area without or no bleeding.
►Healing by primary intension.
►Lack of pressure to incise tissue.
►Electroplaining of tissue.
►less tissue loss after healing
Disadvantages
► Unpleasant odour.
► Slight loss of crestal bone (Kamansky F.W. et al)
► Burn mark on the root surface.
► Not suitable for thin gingiva.
Contraindications
Patients with cardiac pace maker.
Patients with delayed wound healing.
Technique
► Anesthesia
► A drop of aromatic smelling oil.
► Complete seating of electrodes in handpiece.
► Light pressure and quick ,deft stokes.
► 7mm per second
► 5-10 seconds between each stroke.
► Power selector dial ,as recommended.
.
8
Lasers
► Lasers helps in exposure of subgingival finish lines, controls the hemorrhage, and removes just enough epithelial attachment and periodontal ligament to facilitate the placement of retraction cord.
► Minimum gingival recession.
► Laser tips 400-600 micron in diameter.
► A feather light stroke should be used.
► The laser handpiece should be kept moving.
► Along with the attached gingiva, approximately 1mm of epithelial attachment should be removed and coagulated to achieve hemostasis and to expose the crown margins.
Advantages
► Minimum pain, inconvenience discomfort
► Less fear anxiety, stress
► Minimum or no anaesthesia
► No drill sounds
► Less chair time
► Reduced post operative complications
► Minimum or no bleeding
Recent Advances Mechanical retraction
Expasyl retraction paste
• In 1978, Van der Velden and De Vries studied the forces applied to the sulcus during various dental procedures. They observed a tearing of the epithelial attachment as soon as pressure of 1N/mm2 was applied to the marginal gingiva. This attachment was destroyed when the pressure exceeded 2.5N/mm2. The pressure applied by a retraction cord in this region is between 5 and 10N/mm2 (depending on the number of cords inserted into the sulcus). A simple periodontal probe exerts a pressure between 1 and 2N/mm2. To separate the marginal gingiva from the human tooth at a distance of 1.5 mm, it is necessary to apply a pressure of 0.1N/mm2. The conclusion of these studies was that gingival retraction should be accomplished under a pressure of between 0.1 and 1N/mm2 to avoid tearing of the epithelial attachment.

.
9
Magic foam
►Marco Ferrari et al in 1996 they found merocel a synthetic material that is specifically chemically extracted by a biocompatible polymer (hydroxylate polyvinyl acetate)
Matrix impression system
►Gus J. Livaditis (1998) in this system a matrix of polyether occlusal registration elastomeric material is made over the tooth preparation.
.
10
summary
► Technicians generally agree that impressions for crowns and fixed prostheses could be better. There are numerous clinical procedures that can assist dentists in making better impressions. Some of these procedures are performing adequate periodontal therapy before starting fixed-prosthodontic procedures; using preoperative chlorhexidine mouthrinses; protecting gingiva during tooth preparations; using a proper cord placement technique, preferably a two-cord procedure; judiciously using electro-surgery or laser for tissue management; and leaving some margins supragingival. Practitioners are advised to evaluate their impressions carefully and make changes in technique if the impressions could be better.
References
► Shillingburg H.T etal. Fundamentals of fixed Prosthodontics.3r edi.quintessence pub.co
► Rosenstiel,Land,Fugimoto - Contemporary Fixed Prosthodontics 3rd edi. The mosby co.
► Marco Ferrari et al 1996, JPD 75; 242-7.
► Asbjorn Jokstad, JPD 1999, 81; 258-61.
► .W.D.Mello,V.Chitre et al:Gingival retraction cords-their role in tissue displacement:A Review JIPS2003,vol.3,pg.16
► Livaditis G.J. Comparison of the new matrix system with traditional fixed prosthodontic impression procedures, J Prosthet Dent 1998;79:200-7
► Christensen G.J. Laboratories want better impressions, JADA 2007, 138; 527-529
► Nazarian A, Tissue Management with Expasyl; A Keyto Restorative Success, Continuing education, 2007. dentaltown.com
.
1
Growth and Development of MAXILLA AND MANDIBLE
DR. PRAJAKTA BARAPATRE
2
CONTENTS
INTRODUCTIONBASIC CONCEPTSDefinitionsFactors affecting growthGrowth spurtsMethods of studying growthCephalo caudal gradient of growthTypes of bone ossificationGrowth movementsTheories PRE NATAL GROWTHNATALPOST NATAL GROWTHDEVELOPMENTAL ANOMALIESCONCLUSIONREFERENCES
3
Introduction
◼ “Growth was concieved by an anatomist born to a biologist, delivered by a physician, left on a chemists door steps, adopted by a physiologist.
◼ At an early age she eloped with a statician, divorced him for a physcologist and is now being wooed alternately by an endocrinologist, a paediatrician, a physical anthropologist, an educationalist, bio-chemist, physicist, mathematician, dentist, ugenicist and the childrens beauraue”
» Quoted by Krogman.(5)
Source: JCO on CD-ROM (Copyright © 1998 JCO, Inc.), Volume 1983 Oct(669 - 679): JCO/lnterviews: Dr. Donald H. Enlow on Craniofacial Growth
▪ DR. GOTTLIEB
Is there good growth and bad growth?
▪ DR. ENLOW
Well, no. Growth for any individual is "normal", given the circumstances that exist for that individual. Growth is a process striving toward a state of functional equilibrium, and it is always responsive to the conditions that occur, unless pathology is involved. Most structural dysplasias, of course, are in "equilibrium".
5
Basic Concepts of Growth & Development
DEFINITIONS(6)GROWTH1.Acc. to Stewart,(1982)
Developmental increase in mass.2.Acc. To proffit(1986),
Increase in size or number.3.Acc. to Moyer (1988),
Normal changes in the amount of living substance.
6
4.Acc. to Stedman, (1990)
Increase in size of a living being or any of its parts occuring in the process of development.
5.Acc. to Pinkham, (1994)
An increased expansion or extension of any living tissue.
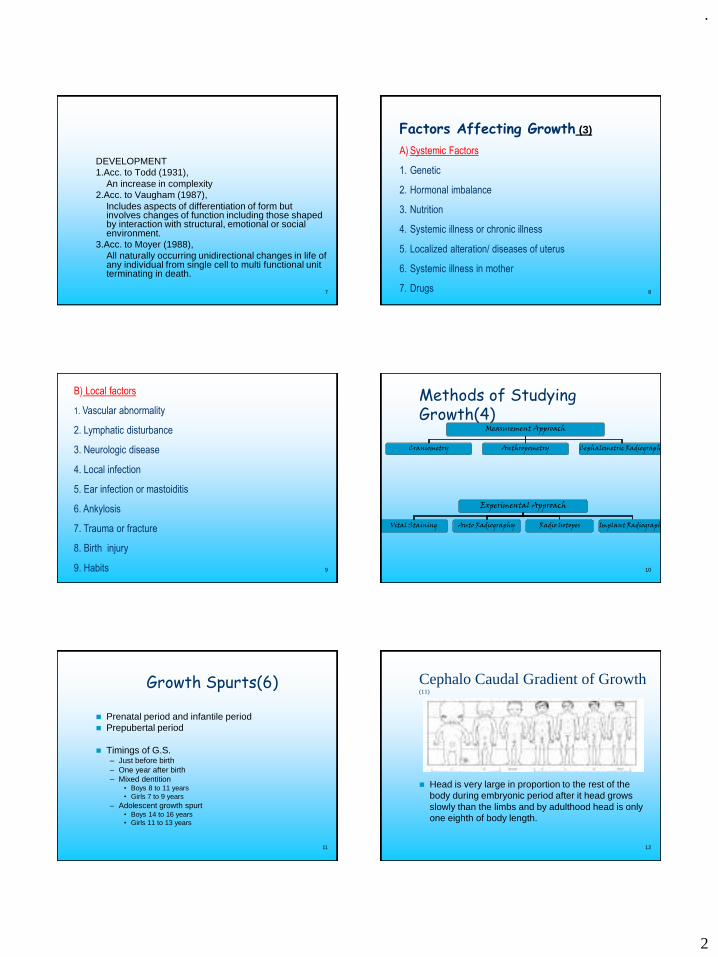
.
2
7
DEVELOPMENT1.Acc. to Todd (1931),
An increase in complexity2.Acc. to Vaugham (1987),
Includes aspects of differentiation of form but involves changes of function including those shaped by interaction with structural, emotional or social environment.
3.Acc. to Moyer (1988),All naturally occurring unidirectional changes in life of any individual from single cell to multi functional unit terminating in death.
8
Factors Affecting Growth (3)
A) Systemic Factors
1. Genetic
2. Hormonal imbalance
3. Nutrition
4. Systemic illness or chronic illness
5. Localized alteration/ diseases of uterus
6. Systemic illness in mother
7. Drugs
9
B) Local factors
1. Vascular abnormality
2. Lymphatic disturbance
3. Neurologic disease
4. Local infection
5. Ear infection or mastoiditis
6. Ankylosis
7. Trauma or fracture
8. Birth injury
9. Habits 10
Methods of Studying Growth(4)
Measurement Approach
Craniometry Anthropometry Cephalometric Radiography
Experimental Approach
Vital Staining Auto Radiography Radio Isotopes Implant Radiography
11
Growth Spurts(6)
◼ Prenatal period and infantile period◼ Prepubertal period
◼ Timings of G.S.– Just before birth– One year after birth– Mixed dentition
• Boys 8 to 11 years• Girls 7 to 9 years
– Adolescent growth spurt• Boys 14 to 16 years• Girls 11 to 13 years
12
Cephalo Caudal Gradient of Growth(11)
◼ Head is very large in proportion to the rest of the body during embryonic period after it head grows slowly than the limbs and by adulthood head is only one eighth of body length.
.
3
Scammons Curve(13)
14
Types of bone growth
◼ Mandible is the second bone in the body to ossify,
◼ Bone growth can be of two types;
◼ INTRA MEMBRANOUS
◼ ENDOCHONDRAL
15
IntramembranousEctomesenchyme Epithelium
Osteogenic membrane
Osteoblast
Osteoid matrix
Blood vessels
16
Intramembranous
17
Intramembranous
18
Endochondral
Mesenchymal cells Cart. Matrix of glycoproteins
Cart. templateosteoblast
Osteoid matrix mineralized
Blood vessels
.
4
19
Endochondral
20
Endochondral
21
Clinical significance
◼ In postnatal life distinction b/w two is of no
significance:-
◼ # of intramembranous bone
◼ Surface remodelling of endochondral bone
◼ Prenatal life – congenital defects
◼ Achondroplasia – Endochondral bone
◼ Cleidocranial dysostosis – Intramembranous bone
◼ Osteogenesis Imperfecta – both type22
Mechanisms Of Bone Growth(2,12,13)
1. Bone remodelling
Process Of Bone Deposition And Resorption
2. Cortical drift
Combination of bone deposition and resorption resulting in growth movement
towards deposition surface
3. Displacement
Movement of whole bone as a unit
I) Primary displacement
II) Secondary displacement
23 24
Theories Of Growth
.
5
25
Theories Of Growth
26
Other Theories
◼ ENLOW’S “V”
PRINCIPLE
◼ The growth and
enlargement of bones
occur towards wide
end of ‘v’ due to
differential deposition
and resorption
27
Enlow’s Counterpart Principle
◼ ‘The growth of any given facial or cranial part
relates specifically to other structural and geometric
“counter” parts in the face and cranium’.
◼ Eg. Maxillary arch is counter part of mandibular
arch.Regional part counter part
Balanced growth28
Growth and DevelopmentPrenatal Natal Post Natal
Period of Ovum Period of Embryo Period of Foetus
Period of ovum(3,11,12)
• From fertilization to end of fourteenth day• Ovum Zygote Blastocyst Gastrula
Neurulation
30
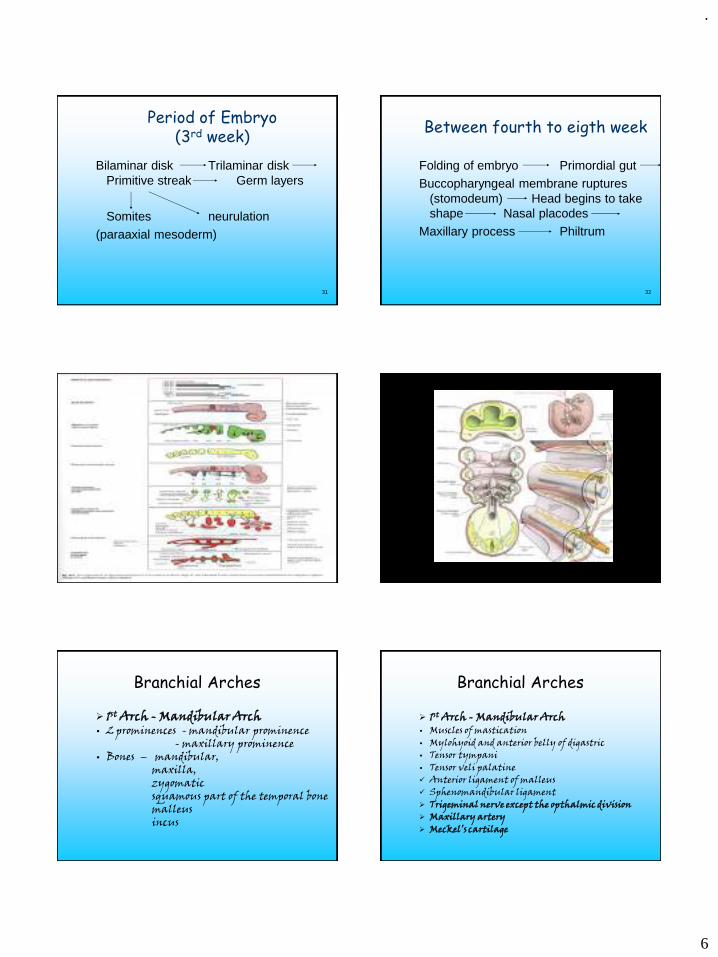
.
6
31
Period of Embryo(3rd week)
Bilaminar disk Trilaminar disk Primitive streak Germ layers
Somites neurulation
(paraaxial mesoderm)
32
Between fourth to eigth week
Folding of embryo Primordial gut
Buccopharyngeal membrane ruptures (stomodeum) Head begins to take shape Nasal placodes
Maxillary process Philtrum
33
Branchial Arches
➢ 1st Arch - Mandibular Arch• 2 prominences - mandibular prominence
- maxillary prominence• Bones – mandibular,
maxilla, zygomatic squamous part of the temporal bonemalleusincus
Branchial Arches
➢ 1st Arch - Mandibular Arch• Muscles of mastication• Mylohyoid and anterior belly of digastric• Tensor tympani• Tensor veli palatine✓ Anterior ligament of malleus✓ Sphenomandibular ligament➢ Trigeminal nerve except the opthalmic division➢ Maxillary artery➢ Meckel’s cartilage
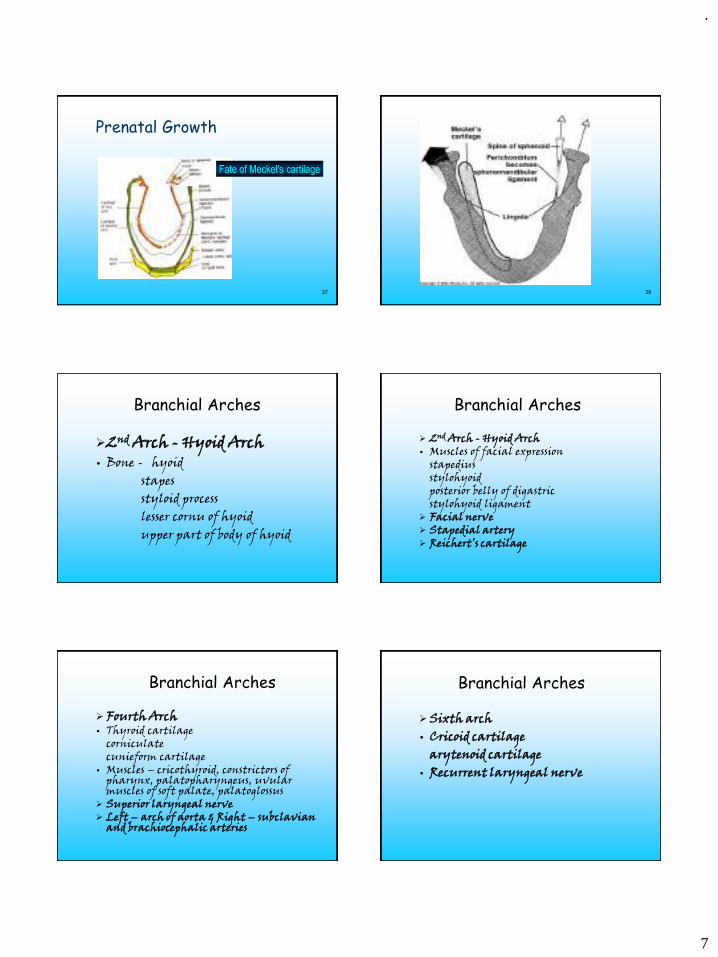
.
7
37
Prenatal Growth
Fate of Meckel’s cartilage
38
Branchial Arches
➢2nd Arch - Hyoid Arch• Bone - hyoid
stapesstyloid processlesser cornu of hyoidupper part of body of hyoid
Branchial Arches
➢ 2nd Arch - Hyoid Arch• Muscles of facial expression
stapedius stylohyoidposterior belly of digastricstylohyoid ligament
➢ Facial nerve➢ Stapedial artery➢ Reichert’s cartilage
Branchial Arches
➢ Fourth Arch• Thyroid cartilage
corniculatecunieform cartilage
• Muscles – cricothyroid, constrictors of pharynx, palatopharyngeus, uvular muscles of soft palate, palatoglossus
➢ Superior laryngeal nerve➢ Left – arch of aorta & Right – subclavian
and brachiocephalic arteries
Branchial Arches
➢ Sixth arch• Cricoid cartilage
arytenoid cartilage• Recurrent laryngeal nerve

.
8
Branchial Arches
➢ Third Arch• Bone – greater cornu and the inferior part of
the body of the hyoid bone• Stylopharyngeus➢ Glossopharyngeal nerve➢ Common carotid artery
Internal carotid artery➢ Carotid body
Prenatal embryology
• Face - Upper - Frontonasal- Middle - Maxillary- Lower - Mandibular
Organizing centersProsencephalic - Upper third of faceRhombencephalic - Middle third of face
1/3rd Prominence
45
Pre-natal growth
◼At fourth week of of IUL-1.migration of neural crest cells2.formation of brachial arches
STOMODEUM
FRONTONASAL MAXILLARYMAXILLARY
MANDIBULAR MANDIBULAR
47
Medial nasal process
Lateral nasal process
Maxillary process
Mandibular process

.
9
◼ Maxillary and Mandibular processes-first branchial arch
◼ Frontonasal processes- downward proliferation of mesenchyme of developing brain
Medial nasal Lateral nasal
Mesenchyme of first arch
maxilla
palatine
mandible
zygomatic
Part of temporal
Nasal process
Median nasal process
Lateral nasal process
◼At Seventh Week IUL-1.Formation of upper lip2.Intramembranous Bone
ossification Takes Place3.Formation of Nasal Septum4.Nasolacrimal Duct5.Formation of Primary Palate
At Seventh Week IUL◼ Primary ossification center -for each
maxilla at termination of infraorbital nerve above canine tooth dental lamina.
◼ Secondary centerzygomatic
orbitonasal
intermaxillarynasopalatine
53
Prenatal Growth
Ectomesenchymal cells
Epi. Of 1st arch
Osteogenic Memb.
36-38 day Iul
54
Prenatal Growth
1°centre of ossification
Infr alv. Nerve &
Incisive branch
Trough for dev. teeth
below around
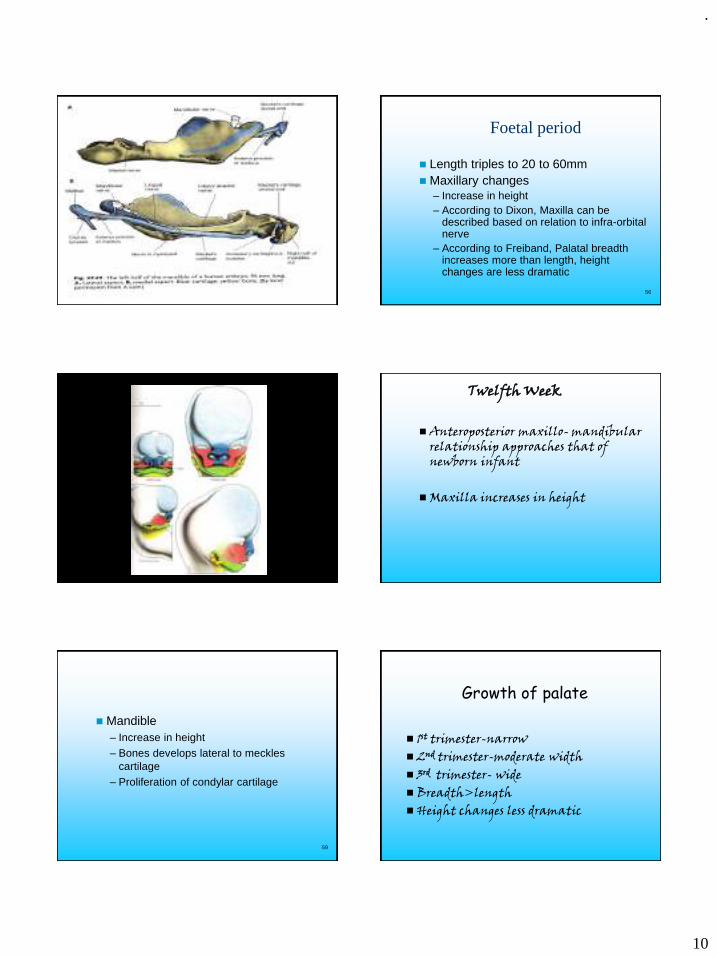
.
10
55 56
Foetal period
◼ Length triples to 20 to 60mm◼ Maxillary changes
– Increase in height– According to Dixon, Maxilla can be
described based on relation to infra-orbital nerve
– According to Freiband, Palatal breadth increases more than length, height changes are less dramatic
◼ Anteroposterior maxillo- mandibular relationship approaches that of newborn infant
◼ Maxilla increases in height
Twelfth Week
59
◼ Mandible– Increase in height– Bones develops lateral to meckles
cartilage– Proliferation of condylar cartilage
Growth of palate
◼ 1st trimester-narrow◼ 2nd trimester-moderate width◼ 3rd trimester- wide◼ Breadth>length◼ Height changes less dramatic
.
11
Growth of palate
• Two primordia, primary palate and secondary palate
◼ Formation of primary and secondary palate
◼ Elevation of palatal shelves
◼ Fusion of palatal shelves
Early palate formation
◼ 28th day of IUL◼ -disintegration of buccopharangeal
membrane◼ stomadeal chamber
◼ Horizontal extensions
Oral cavity
Nasal cavity
2 palatal shelves
Single primary palate
◼ Structure of palate
◼ PALATOGENESIS
Secondary palatePrimary palate
5 TH week IUL
12 TH week IUL6 9
CRITICAL PERIOD
Primary palate
Frontonasal process
Medial nasal
Mesenchyme
Wedge shaped mass between internal surface of maxillary prominence
Primary palatePre-maxilla
Primary palate
Primary palate
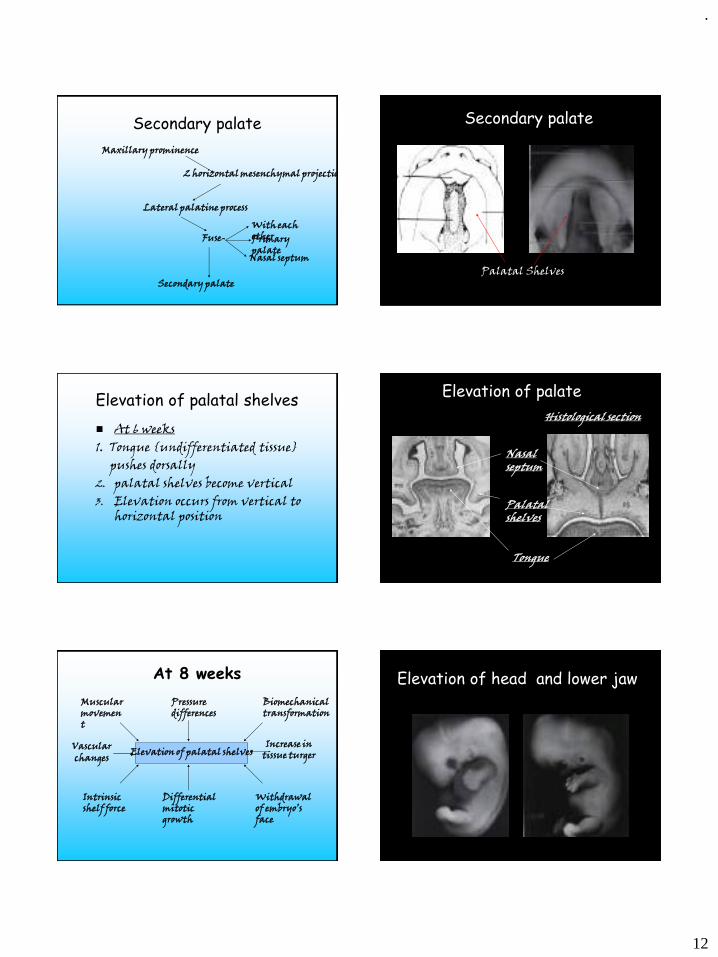
.
12
Secondary palate
2 horizontal mesenchymal projections
Maxillary prominence
Lateral palatine process
Fuse-With each otherPrimary palate
Nasal septum
Secondary palate
Secondary palate
Palatal Shelves
Elevation of palatal shelves
◼ At 6 weeks1. Tongue {undifferentiated tissue}
pushes dorsally2. palatal shelves become vertical3. Elevation occurs from vertical to
horizontal position
Elevation of palate
Nasal septum
Palatal shelves
Tongue
Histological section
At 8 weeks
Elevation of palatal shelves
Muscular movement
Pressure differences
Biomechanical transformation
Intrinsic shelf force
Differential mitotic growth
Withdrawal of embryo’s face
Vascular changes
Increase in tissue turger
Elevation of head and lower jaw
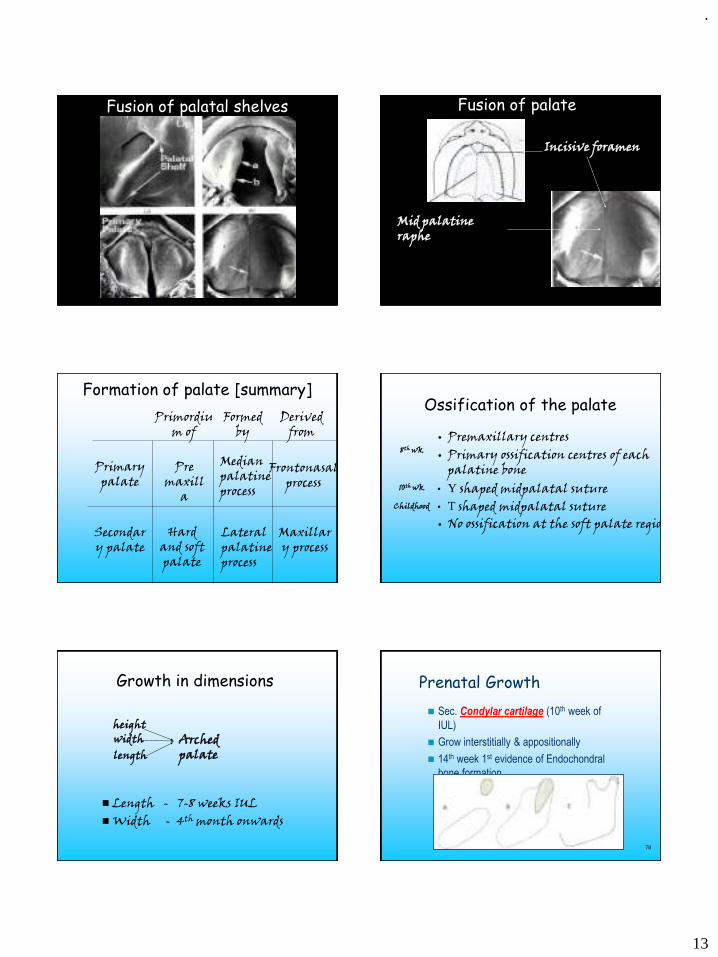
.
13
Fusion of palatal shelves Fusion of palate
Incisive foramen
Mid palatine raphe
Formation of palate [summary]
Primordium of
Formed by
Derived from
Primary palate
Secondary palate
Pre maxill
a
Hard and soft palate
Median palatine process
Lateral palatine process
Frontonasal process
Maxillary process
Ossification of the palate
• Premaxillary centres• Primary ossification centres of each
palatine bone• Y shaped midpalatal suture• T shaped midpalatal suture• No ossification at the soft palate region
8th wk
10th wk
Childhood
Growth in dimensions
◼ Length - 7-8 weeks IUL◼ Width - 4th month onwards
heightwidthlength
Arched palate
78
Prenatal Growth
◼ Sec. Condylar cartilage (10th week of
IUL)
◼ Grow interstitially & appositionally
◼ 14th week 1st evidence of Endochondral
bone formation
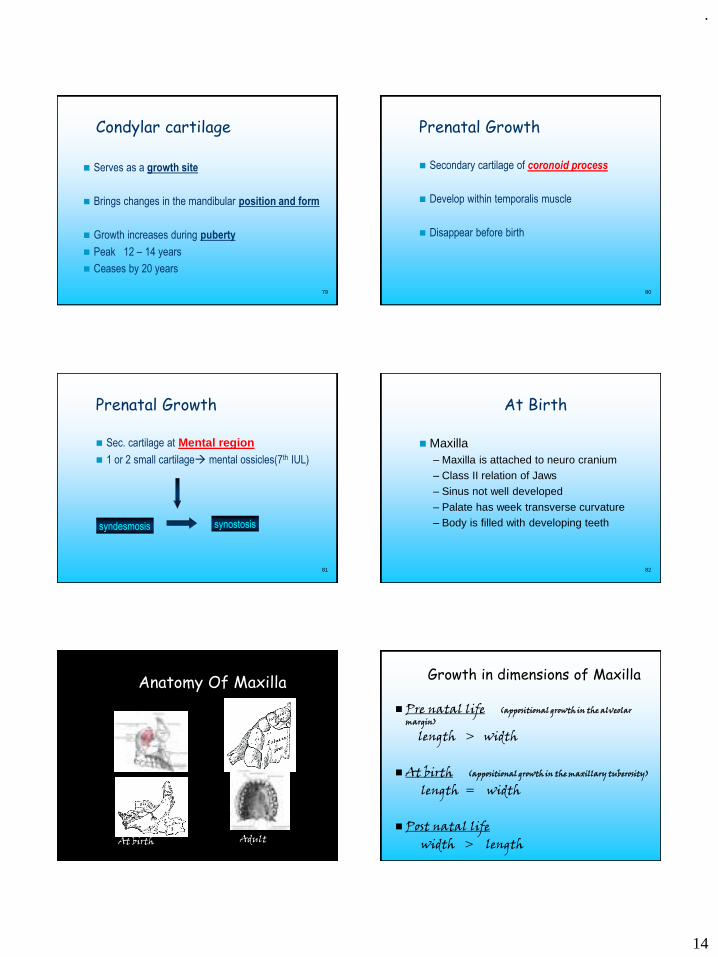
.
14
79
Condylar cartilage
◼ Serves as a growth site
◼ Brings changes in the mandibular position and form
◼ Growth increases during puberty
◼ Peak 12 – 14 years
◼ Ceases by 20 years
80
Prenatal Growth
◼ Secondary cartilage of coronoid process
◼ Develop within temporalis muscle
◼ Disappear before birth
81
Prenatal Growth
◼ Sec. cartilage at Mental region◼ 1 or 2 small cartilage→ mental ossicles(7th IUL)
syndesmosis synostosis
82
At Birth
◼ Maxilla– Maxilla is attached to neuro cranium– Class II relation of Jaws
– Sinus not well developed
– Palate has week transverse curvature– Body is filled with developing teeth
Anatomy Of Maxilla
At birth Adult
Growth in dimensions of Maxilla
◼ Pre natal life (appositional growth in the alveolar margin)
length > width
◼ At birth (appositional growth in the maxillary tuberosity)
length = width
◼ Post natal lifewidth > length
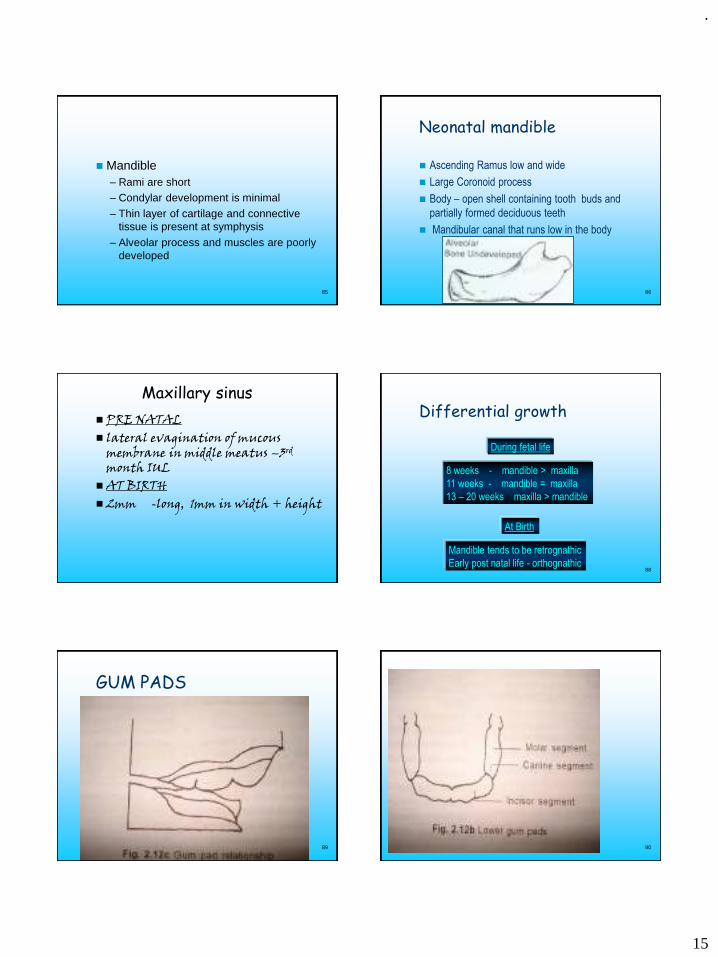
.
15
85
◼ Mandible– Rami are short – Condylar development is minimal
– Thin layer of cartilage and connective tissue is present at symphysis
– Alveolar process and muscles are poorly developed
86
Neonatal mandible
◼ Ascending Ramus low and wide
◼ Large Coronoid process
◼ Body – open shell containing tooth buds and
partially formed deciduous teeth
◼ Mandibular canal that runs low in the body
Maxillary sinus
◼ PRE NATAL◼ lateral evagination of mucous
membrane in middle meatus –3rd
month IUL◼ AT BIRTH ◼ 2mm -long, 1mm in width + height
88
Differential growth
8 weeks - mandible > maxilla
11 weeks - mandible = maxilla
13 – 20 weeks maxilla > mandible
During fetal life
At Birth
Mandible tends to be retrognathic
Early post natal life - orthognathic
89
GUM PADS
90
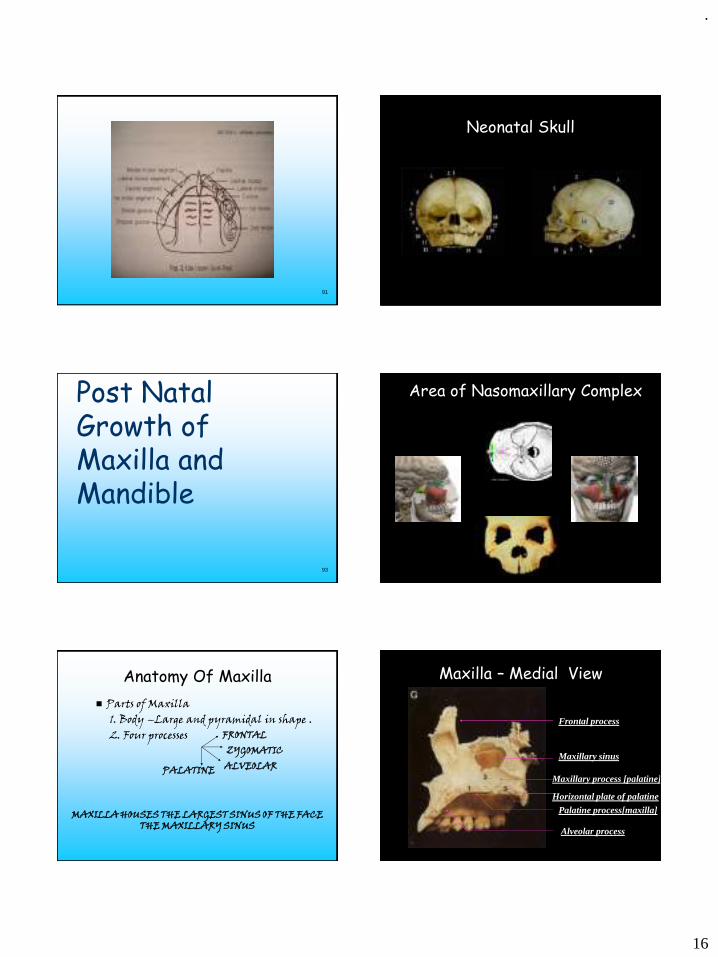
.
16
91
Neonatal Skull
93
Post Natal Growth of Maxilla and Mandible
Area of Nasomaxillary Complex
Anatomy Of Maxilla
◼ Parts of Maxilla 1. Body –Large and pyramidal in shape . 2. Four processes FRONTAL
ZYGOMATICALVEOLARPALATINE
MAXILLA HOUSES THE LARGEST SINUS OF THE FACE THE MAXILLARY SINUS
Palatine process[maxilla]
Maxillary sinus
Frontal process
Maxillary process [palatine]
Alveolar process
Maxilla – Medial View
Horizontal plate of palatine
.
17
Nasal notch
Zygomatic process
ANS
Alveolar process
Maxilla - Lateral View
Frontal process
• General features• Three dimensional growth of maxilla
Height (Vertical)Width (Transverse)Length (Ant-Post)
• Key factors in Nasomaxillary remodelling
Displacement
• Primary displacement
• Secondary displacement
Reversal line• Directions of growth
sequentially undergo reversals
• A reversal line showing the crossover between resorptive and depository growth fields seen in microscope
• Factors affecting reversalshape of bonemuscle attachmentsrotationsgrowthfeilds
Post natal growth of maxilla◼ Surface remodeling
◼ Displacement
◼ CRANIAL BASE MAXILLA
apposition resorption
MOSS
Transformation
Translation
SUTURES
Post natal growth of maxilla◼ Mechanism of growth
• Sutural
•• Surface apposition and resorption on periosteal
and endosteal surfaces
• Alveolar process
.
18
• In contrast to cranial base maxilla is dominated by intra membranous ossification
Surface apposition
Post natal growthAt Birth
Hard palate : length = width
maxillary sinus : not visible radiographically
1 – 2 years
Extensive remodeling descent of palate /enlargement of nasal cavity
Mid palatine suture growth ceases
No synostosis
Post natal growth
Mid palatine suture starts closing at 9- 10 years
RME Best done between 9-14 yrs
THE MIXED DENTITION YEARS
Growth in width of the dental arch anterior to the first molar
Ceases by 5-6 yrs
Inter canine width completed
12 yrs - females
18 yrs - males
Post natal growth
◼ The depository growth potential of the tuberosity allows for arch expansion by moving the teeth posteriorly into the area of bone deposition
◼ Extensive scope for growth modification before adolscent growth spurt
THE MIXED DENTITION YEARS THE EARLY PERMANENT DENTITION YEARS
•Growth modification still possible in boys
•RME can still be tried till 12 -15 yrs
•>15 years complete closure[synostosis]
Orthognatic surgery
.
19
Age changes◼ All para nasal sinuses increase in
size◼ Vertical height decreases
◼ Vertical changes > AP > width◼ Soft tissue changes > skeletal◼ Nose growth continues till 25 years◼ Inclination of palatal plane
increases[post downwards]
Alveolar process resorbed
Tooth loss
Post natal growth of maxilla
◼ Growth in height vertical
◼ Growth in width transverse
◼ Growth in length A - P
Vertical growth• Bjork and Skieller implant
studies - height increases because of sutural growth toward the frontal and zygomatic bones- appositional growth in the alveolar bone, floor of orbit, on hard palate and resorption on nasal floor
HEIGHT
◼ Deposition on the oral side
◼ Resorption on the nasal side
ENLOW AND BANG ‘V’ PRINCIPLE
V principle of Bang and Enlow
◼ Entire ‘v’ shaped structure moves in a direction towards the wide end of the ‘v’
Remodeling of palateH EIGHT
APPOSITION IN THE ALVEOLAR PROCESS
ERUPTION OF TEETH
.
20
Sagittal view Coronal view
HEIGHT - V’ PRINCIPLEPrimary displacement
HEIGHT
WIDTH◼ Finished earlier in postnatal life
◼ WIDTH GROWTH IN MID PALATINE SUTURE
REMODELING IN THE LATERAL SURFACE OF ALVEOLAR PROCESS
Mutual transverse rotations of maxillary halves give palate ‘u’ shape
WIDTH
• This growth mimics the general growth curve
• Mutual transverse rotation of the two maxillae results in more separation of the halves in the posterior than the anterior segment
LENGTH◼ Begins rapidly in the 2 nd year of life
Maxillary tuberosity
Palato maxillary suture
primary secondary
displacement
• Resorption in the anterior region of the maxilla
• Maxilla rotates in relation to the anterior cranial base
• Bjork and Skieller implant studies have shown that anterior surface is stable sagittally
.
21
The MAXILLARY Remodeling
• The Lacrimal Suture• The Maxillary tuberosity • Key ridge• Vertical drift of teeth• Palatal remodelling• Downward maxillary displacement• Maxillary sutures• The paranasal sinuses
Lacrimal bone• Bounded by sutural connective tissue• Undergoes remodelling rotation – medial superior
part remains with the nasal bridge, - inferior part moves outwardly with the ethmoidal sinuses
• Provides slippage of multiple bones along sutural interfaces ‘ perilacrimal sutural system’
• Maxilla slides downwards along its orbital contacts
• Developmental gridlock would develop without this system
Maxillary tuberosity◼ Established by the posterior boundary
of anterior cranial fossa◼ Helps in posterior and horizontal
lengthening of archAnterior displacement= posterior lengthening
lateral widening
downward deposition
Contributes to
maxillary sinus enlargement
Key ridge
Vertical crest below the malar protuberence’
‘Reversal occurs at the key ridge
Posterior - appositionAnterior - resorption
Vertical drift of teeth• Vertical drift – significant intrinsic growth
factor• Thus,periodontal connective tissue provides
intramembranous bone remodelling • mesial drift well known process – ‘Vertical
drift’ not a part of everyday vocubulary
Palatal remodelling
• V principle• Bone deposition on the inside of the
arch• Growth along the mid palatal suture• Grows inferiorly exchange of old palate
for new hard and soft tissues occurs
.
22
Downward maxillary displacement• Primary displacement of the
ethmomaxillary complex inferiorly
• New bone is added at all sutures and these sutures accompany displacement produced by the soft tissues
Maxillary sutures
• Sutures slide or slippage of bones along the interface
• Remodelling and relinkage of the collagenous fiber connections within the sutural connective tissue causes the displacement process
Maxillary sinus
◼Age changesExpands - 2mm vertically 3mm A-P - every year> in size -resorption in walls + alveolus
Maxillary sinus
◼ POST NATAL◼ All internal
surfaces resorption
[expect medial]
◼ Rapid continuous downward growth
close proximity to buccal maxillary teeth
131DR. ASHISH SINGH
132
Anatomy
.
23
133
Parts Of Mandible Derived From
1. INTRAMEMBRANOUS OSSIFICATION
i) Whole body of mandible except the anterior part
ii) Ramus of mandible as far as mandibular foramen
2 . ENDOCHONDRAL OSSIFICATION
i) Anterior portion of the mandible (symphysis)
ii) Part of ramus above the mandibular foramen
iii) Coronoid process
iv) Condylar process 134
Post Natal Growth And Development
GROWTH TIMING
Growth of width of mandible is completed first, then
growth in length and finally growth in height
135
Post Natal Growth And Development
WIDTH OF MANDIBLE
▪ Growth in width is completed before adolescent growth
spurt
▪ Intercanine width does increase after 12 years
▪ Both molar and bicondylar width shows small increase
until growth in length ends
136
Post Natal Growth And Development
GROWTH IN LENGTH
◼ Growth in length continues through puberty
◼ Girls—14-15 years
◼ boys---18-19 years
137
Post Natal Growth And Development
◼ Main sites of post natal growth in the Mandible
◼ Condylar cartilage
◼ Posterior border of the Rami
◼ Alveolar ridges
138
Condylar cartilage
Secondary cartilage
Dual function articular
growth
Not a pri. Centre of growth but rather
2° in evolution
2° in embryonic origin
2°in adaptive responses to changing dev.
.
24
139
Is the Condylar cartilage the principle force that produces the displacement of the mandible ?
For many years considered primary growth center
FMH - Condyle absent yet mandible positioned normally
Considered secondary cartilage -no intrinsic growth
potential
140
Petrovic et al - Role of hormones
Experiments involving transplantation of the condyle
Johnston et al - Detached condyle from the body of
mandible in guinea pigs
Injection of papain - Inhibition of chondrogenesis
Koski et al - Periosteal tension in condylar neck-lateral
pterygoid- controls condylar growth
141
◼ Condylar cartilage and functioning muscles translate
the mandible and in the absence of one the other
does best to compensate
◼ When environment is changed compensatory
contributions are enhanced
142
Current Concept
◼ Condylar cartilage does have a measure of intrinsic
genetic programming
◼ But extra condylar factors are needed to sustain this
activity
Physiologic
inductorsIntrinsic and extrinsic
biomechanical forces
ENLOW :
Increase pressure – growth inhibition
Decrease pressure – stimulates growth
based mainly on animal
experiments
143
Ramus
◼ Moves progressively
posterior by:-
◼ Deposition
◼ ResorptionANTERIOR PART
POSTERIOR PART
144
Ramus
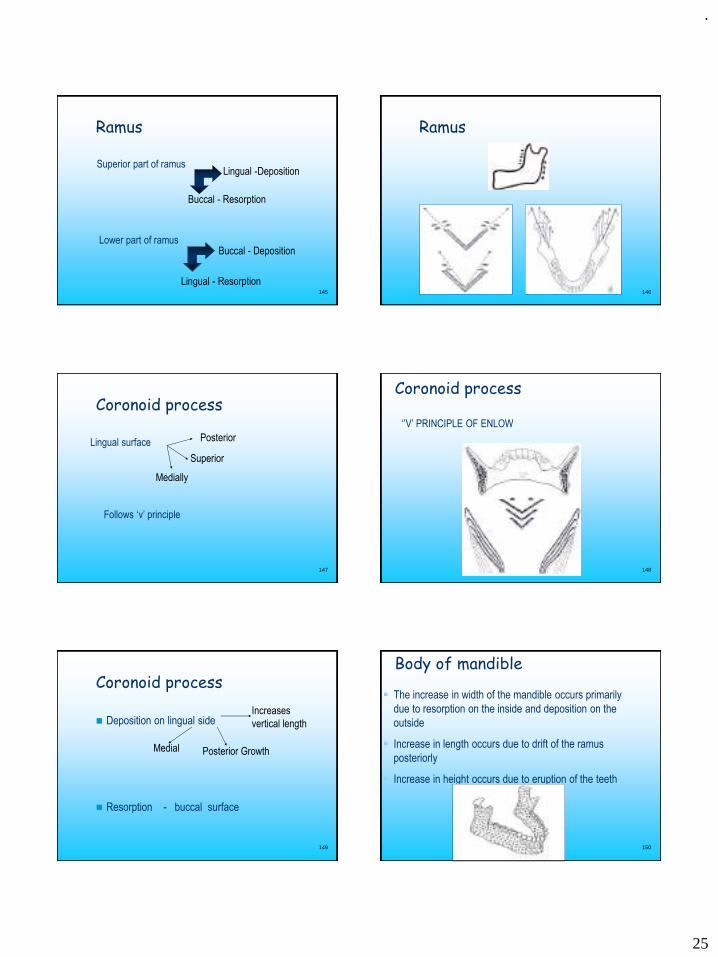
.
25
145
Ramus
Superior part of ramus
Buccal - Resorption
Lingual -Deposition
Lower part of ramusBuccal - Deposition
Lingual - Resorption146
Ramus
147
Coronoid process
Superior
Medially
Follows ‘v’ principle
Lingual surface Posterior
148
Coronoid process
‘’V’ PRINCIPLE OF ENLOW
149
Coronoid process
◼ Deposition on lingual side
◼ Resorption - buccal surface
Increases
vertical length
Posterior GrowthMedial
150
Body of mandible
▪ The increase in width of the mandible occurs primarily
due to resorption on the inside and deposition on the
outside
▪ Increase in length occurs due to drift of the ramus
posteriorly
▪ Increase in height occurs due to eruption of the teeth
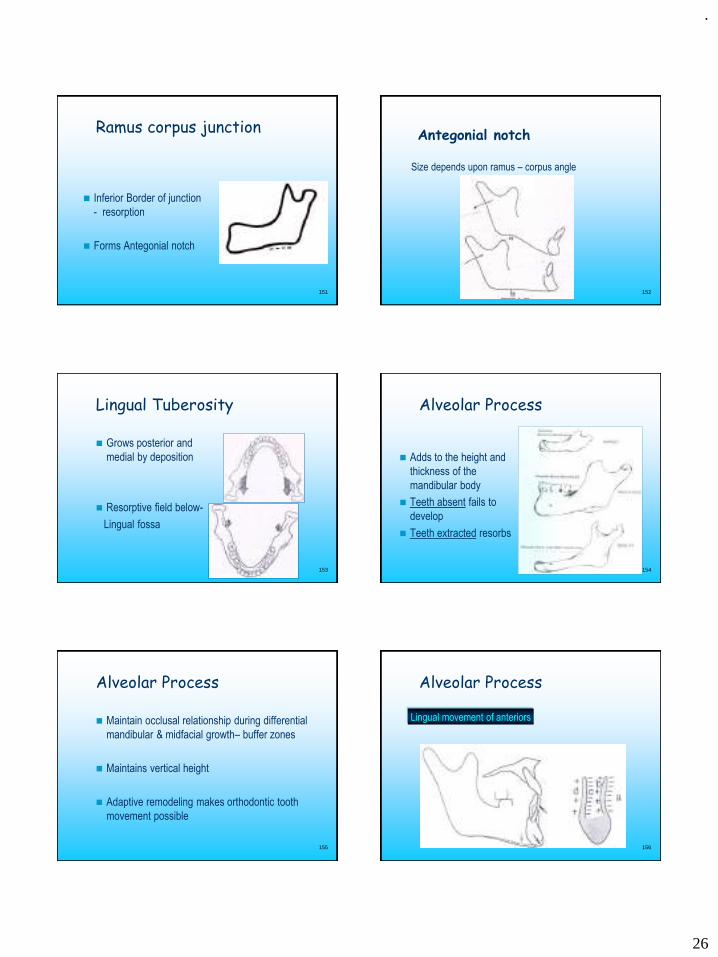
.
26
151
Ramus corpus junction
◼ Inferior Border of junction
- resorption
◼ Forms Antegonial notch
152
Antegonial notch
Size depends upon ramus – corpus angle
153
Lingual Tuberosity
◼ Grows posterior and
medial by deposition
◼ Resorptive field below-
Lingual fossa
154
Alveolar Process
◼ Adds to the height and
thickness of the
mandibular body
◼ Teeth absent fails to
develop
◼ Teeth extracted resorbs
155
Alveolar Process
◼ Maintain occlusal relationship during differential
mandibular & midfacial growth– buffer zones
◼ Maintains vertical height
◼ Adaptive remodeling makes orthodontic tooth
movement possible
156
Alveolar Process
Lingual movement of anteriors
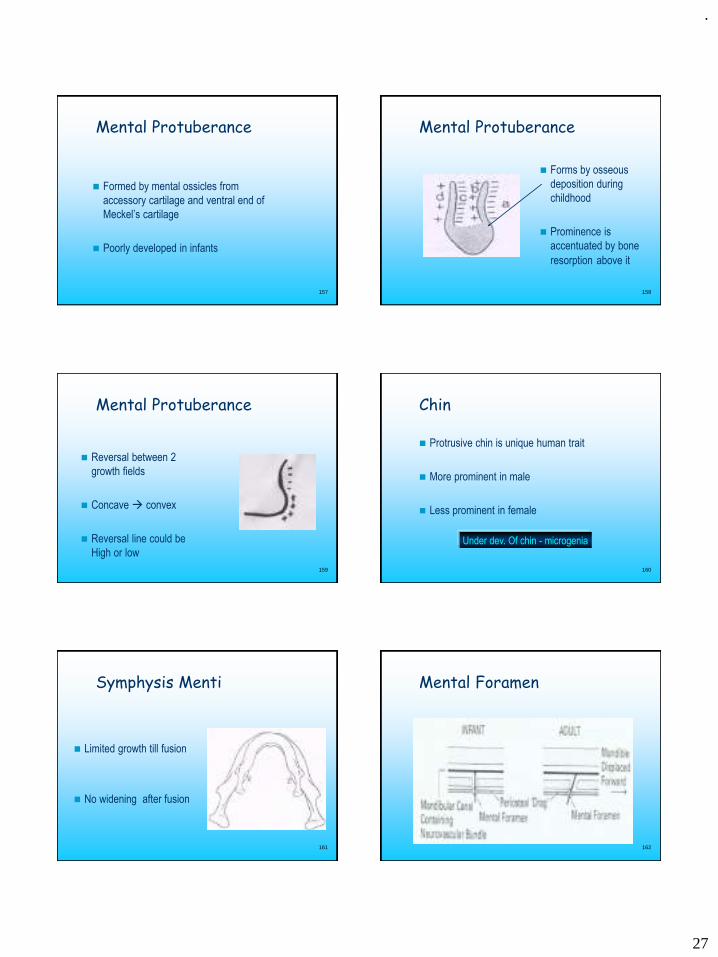
.
27
157
Mental Protuberance
◼ Formed by mental ossicles from
accessory cartilage and ventral end of
Meckel’s cartilage
◼ Poorly developed in infants
158
Mental Protuberance
◼ Forms by osseous
deposition during
childhood
◼ Prominence is
accentuated by bone
resorption above it
159
Mental Protuberance
◼ Reversal between 2
growth fields
◼ Concave → convex
◼ Reversal line could be
High or low
160
Chin
◼ Protrusive chin is unique human trait
◼ More prominent in male
◼ Less prominent in female
Under dev. Of chin - microgenia
161
Symphysis Menti
◼ Limited growth till fusion
◼ No widening after fusion
162
Mental Foramen
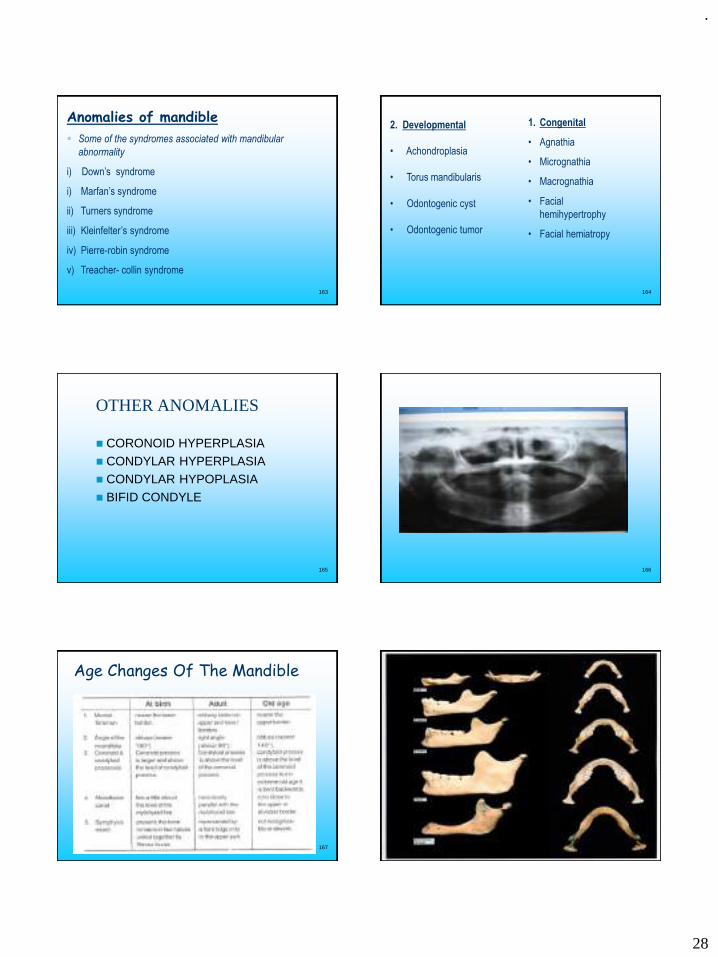
.
28
163
Anomalies of mandible
▪ Some of the syndromes associated with mandibular
abnormality
i) Down’s syndrome
i) Marfan’s syndrome
ii) Turners syndrome
iii) Kleinfelter’s syndrome
iv) Pierre-robin syndrome
v) Treacher- collin syndrome
164
1. Congenital
• Agnathia
• Micrognathia
• Macrognathia
• Facial
hemihypertrophy
• Facial hemiatropy
2. Developmental
• Achondroplasia
• Torus mandibularis
• Odontogenic cyst
• Odontogenic tumor
165
OTHER ANOMALIES
◼ CORONOID HYPERPLASIA
◼ CONDYLAR HYPERPLASIA◼ CONDYLAR HYPOPLASIA
◼ BIFID CONDYLE
166
167
Age Changes Of The Mandible
168
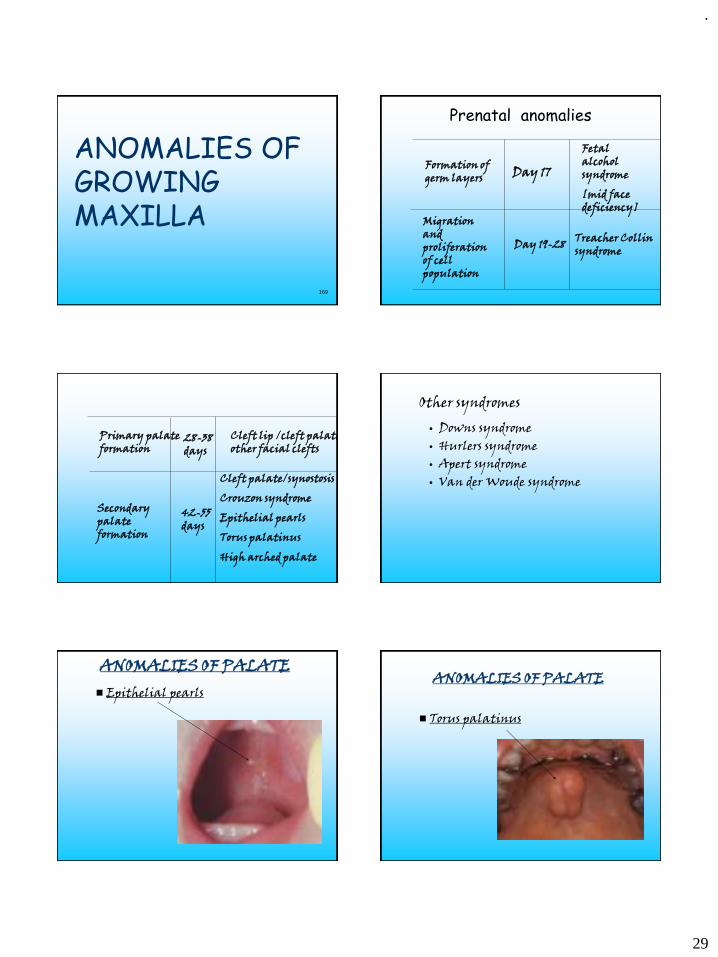
.
29
169
ANOMALIES OF GROWING MAXILLA
Prenatal anomalies
Formation of germ layers Day 17
Fetal alcohol syndrome
[mid face deficiency]
Migration and proliferation of cell population
Day 19-28 Treacher Collin syndrome
Primary palate formation
28-38 days
Cleft lip /cleft palate other facial clefts
Secondary palate formation
42-55 days
Cleft palate/synostosis
Crouzon syndrome
Epithelial pearls
Torus palatinus
High arched palate
Other syndromes
• Downs syndrome• Hurlers syndrome• Apert syndrome• Van der Woude syndrome
ANOMALIES OF PALATE◼ Epithelial pearls
ANOMALIES OF PALATE
◼ Torus palatinus
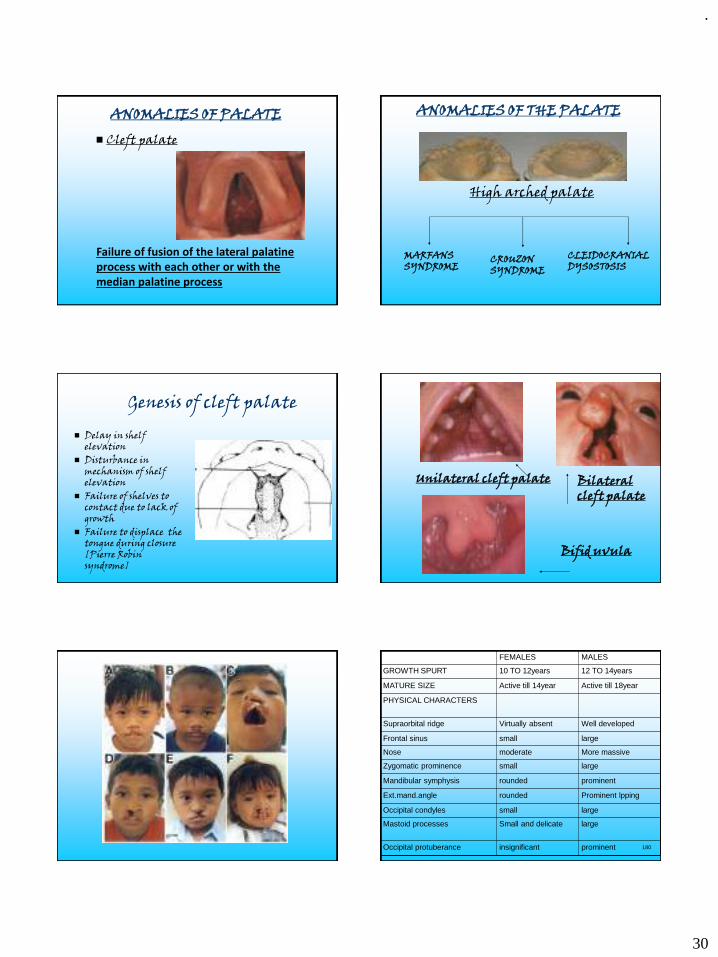
.
30
ANOMALIES OF PALATE
◼ Cleft palate
Failure of fusion of the lateral palatine process with each other or with the median palatine process
ANOMALIES OF THE PALATE
High arched palate
MARFANS SYNDROME
CROUZON SYNDROME
CLEIDOCRANIAL DYSOSTOSIS
Genesis of cleft palate
◼ Delay in shelf elevation
◼ Disturbance in mechanism of shelf elevation
◼ Failure of shelves to contact due to lack of growth
◼ Failure to displace the tongue during closure [Pierre Robin syndrome]
Bilateral cleft palate
Bifid uvula
Unilateral cleft palate
180
FEMALES MALES
GROWTH SPURT 10 TO 12years 12 TO 14years
MATURE SIZE Active till 14year Active till 18year
PHYSICAL CHARACTERS
Supraorbital ridge Virtually absent Well developed
Frontal sinus small large
Nose moderate More massive
Zygomatic prominence small large
Mandibular symphysis rounded prominent
Ext.mand.angle rounded Prominent lpping
Occipital condyles small large
Mastoid processes Small and delicate large
Occipital protuberance insignificant prominent
.
31
181
conclusion
◼ Thorough knowledge is must for a dentist to carry out the treatment procedures in effective and precise manner.
◼ Clinically diff. between an acquired and congenital anomaly should be made
◼ Importance of pre natal period and growth spurts must be understood.
◼ Since much of the knowledge is still on the level of working hpothesis, synthesis of concepts is a current state of affairs.
182
◼ “life is a change;for when you are through changing you are through.”
183
References
1. Essentials of orthodontics-william profitt. 2. ESSENTIALS OF FACIAL GROWTH-Enlow and Hans.3. TEXTBOOK OF ORTHODONTICS-Samir.E.Bishara4. TEXTBOOK OF ORTHODONTICS-Gurkeerat singh5. ORTHODONTICS (Principles and Practice)3rd Edition-Graber6. TEXTBOOK OF PEDODONTICS –Shobha Tandon7. Shafers,TEXTBOOK OF ORAL PATHOLOGY 5th EDITON8. ORAL AND MAXILLOFACIAL PATHOLOGY- Neville,Damn,Allen,Bouquot9. Age related changes in maxilla and mandible. Christopher J.Lux, Donald B
urden. Christian Conradt. European journal of orthodontics Vol27. no.6 10. Textook of histology-Tencate11. GRAYS ANATOMY 38TH EDITION12. Textbook of orthodontics-balaji13. Essential paediatrics-nelson
184
185