Embed Size (px)
DESCRIPTION
Developments in supportive care of the haematology patient. Nick Duncan Haematology pharmacist QE Hospital, Birmingham. Outline of session. Stem cell stimulation Plerixafor Pegfilgrastim Anti-infectives Maribavir Symptom control Aprepitant Palifermin New agents for GVHD. - PowerPoint PPT Presentation
Citation preview

Developments in supportive care of the
haematology patient
Nick Duncan
Haematology pharmacist
QE Hospital, Birmingham

Outline of session
Stem cell stimulation Plerixafor Pegfilgrastim
Anti-infectives Maribavir
Symptom control Aprepitant Palifermin New agents for GVHD

Stem cell stimulation

Current Mobilization Strategies for Autologous Haematopoietic Stem Cell Transplantation
Growth factor alone - Filgrastim, Lenograstim
Growth factor + Chemotherapy
No agreed front-line choice – current failure rate 15-20%

Consequences of Sub-optimal Mobilisation
Failure to mobilise a sufficient number of CD34+ cells may result in: Increased number of days of apheresis Need for bone marrow harvest Ineligibility for transplantation Additional burden on patients
Use of sub-optimal apheresis product may lead to: Delayed, partial, or failed stem cell engraftment Potential for increased risk of opportunistic infections
and/or bleeding

Limitations of Salvage Mobilisation Strategies
Strategy Complications
Repeat Mobilization High product volume when combined with previous collection
Higher cost & morbidity Associated with high failure rate
Alternative Cytokines Higher dose of G-
CSF Combine G-CSF with
GM-CSF
Associated with added toxicity or lack of efficacy
Addition of Chemotherapy
Toxicity, neutropenic fever, admission costs
Traditional Bone Marrow Harvest
Slower engraftment Increased cost, risk (due to anesthesia) and
pain for patient

Plerixafor
Recently approved by EMEARecently approved by EMEA In combination with G-CSF to enhance mobilisation of
haematopoietic stem cells to the peripheral blood for collection and subsequent autologous transplantation in patients with lymphoma and multiple myeloma whose cells mobilise poorly.
Novel mechanism of action A CXCR4 receptor antagonist

SDF-1CXCR4
stem cell
bone marrow
Mechanism of Action of Plerixafor
SDF-1 and CXCR4 play key regulatory roles in stem cell trafficking to, and retention by the bone marrow.
Plerixafor blocks the CXCR4-SDF-1a interaction, releasing stem cells from the bone marrow into the circulating blood
Lapidot T and Petit I. Exp Hematol. 2002;30:973


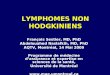
27.9%
49.1%
57.7%
65.6%
4.2%
14.2%
21.6%24.2%
0
10
20
30
40
50
60
70
1 2 3 4
Apheresis Day
HR = 3.64, 95%CI (2.39, 5.45), P < 0.0001
Kap
lan
-Mei
er e
stim
ate
of
pro
po
rtio
n o
f p
atie
nts
rea
chin
g ≥
5 ×
106
CD
34+
cel
ls/k
g
Plerixafor + G-CSF
Placebo + G-CSF
NHL Patients (%) achieving ≥ 5 million CD34+ cells/kg by apheresis day
DiPersio JF et al JCO 2009; Epub ahead of print

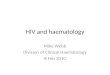
Myeloma patients (%) achieving ≥ 6 x 106 CD34+ Cells/kg by apheresis day
54.2
77.986.8 86.8
17.3
35.3
49.056.0
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4
Apheresis Day
HR = 2.54, P < .0001
Kap
lan
-Mei
er E
stim
ate
of
Pro
po
rtio
n o
f P
atie
nts
Rea
chin
g ≥
6 x
106
CD
34+
cel
ls/k
g
Plerixafor + G-CSF
Placebo + G-CSF
DiPersio JF et al Blood 2009; 113: 5720-5726

Transplant Outcomes: Number of Days to Neutrophil & Platelet Engraftment
PLERIXAFOR PLACEBO
Median time to neutrophil engraftment (days)
NHL: 10
Myeloma: 11
NHL: 10
Myeloma: 11
Median time to platelet engraftment (days)
NHL: 20
Myeloma: 18
NHL: 20
Myeloma: 18
DiPersio JF et al JCO 2009; Epub ahead of printDiPersio JF et al Blood 2009; 113: 5720-5726

Safety of Plerixafor – myeloma study
DiPersio JF et al Blood 2009; 113: 5720-5726

Plerixafor – practical issues
Which patients to target?
Needs to be given 6-11 hours pre-apheresis Admission required?
Recommended to be given at a dose of 0.24mg/kg/day for 2-4 days Costs £4,900 + VAT for a 24mg vial

Pegfilgrastim
Currently licensed for FNE prophylaxis post conventional chemotherapy. Interest in using it for: PBSC mobilisation Post SCT

Pegfilgrastim for stem cell mobilisation
Has been used alone (usually 12mg) or post-chemo (usually 6mg) for autologous stem cell mobilisation in myeloma and lymphoma patients
Appears comparable to conventional G-CSF but studies all small
Pegfilgrastim mobilised stem cells may result in faster count recovery – Tricot G et al. Haematologica 2008; 93: 1739-42

Pegfilgrastim post SCT Number of small studies in autologous SCT
comparing pegfilgrastim (6mg on d+1 or d+5) with conventional G-CSF. Equivalence demonstrated wrt count recovery Some studies demonstrated superiority wrt incidence and
duration of FN - (e.g. Martino M et al. Eur J Haematol 2006; 77: 410-5)
One fully published study in allograft recipients – Ocheni S et al. Leuk Lymphoma 2009; 50: 612-8 Neutrophil recovery slightly faster (15 vs 16 days) with
pegfilgrastim vs lenograstim No difference wrt incidence and duration of FN.
In conclusion, drug cost likely to impact on choice of agent

Anti-infectives

CMV infection
CMV reactivation a major issue post allogeneic SCT
Pre-emptive ganciclovir mainstay of management but toxicity concerns
Lack of gold-standard prophylaxis – aciclovir, valaciclovir, ganciclovir?
Interest in new agents

Maribavir (1)
Maribavir is an oral agent with anti-CMV activity Inhibits viral DNA assembly and egress of viral
particles from infected cells Favourable toxicity profile – no renal or BM
effects Interest in using for CMV prophylaxis Promising data published 2008

Maribavir (2)
Winston et al. Blood 2008; 111:5403
111 allograft recipients randomised to maribavir (200-800mg/day) or placebo
At 100 days incidence of CMV infection was 15-19% vs. 39%
Significant reduction in need for pre-emptive ganciclovir
Toxicity – N+V, taste disturbances

Maribavir (3)
Large phase III trial (681 patients) not yet published but results released earlier this year
Maribavir prophylaxis (100mg bd) failed to meet 1ry and 2ry endpoints vs. placebo: Rate of CMV disease: 4.4% vs. 4.8% Need for anti-CMV therapies: 38% vs. 40.5% GVHD incidence and mortality comparable
Not sure what the future holds for this drug…….

Symptom control

Aprepitant
An oral neurokinin-1 antagonist
Licensed for prevention of N+V associated with moderately and highly emetogenic chemo (+5HT3 antagonist and corticosteroid)
Increasingly used in oncology
High-dose chemotherapy is highly emetogenic so should we be using aprepitant in haematology?

What do the guidelines say?
ESMO guidelines 2008 Highly emetogenic chemo
5-HT3 antagonist + steroid + aprepitant to prevent acute N+V.
Steroid + aprepitant to prevent delayed N+V
NCCN guidelines 2008 As per ESMO for highly emetogenic chemo. An option for
some patients receiving moderately emetogenic chemo. TBI - 5-HT3 antagonist + steroid For multiple-day chemotherapy advises that can give
aprepitant 125mg day 1 then 80mg days 2-5.

What do the guidelines say?
ASCO guidelines 2006 As per ESMO for highly emetogenic chemo Consider aprepitant with high-dose chemo
although lack of evidence in this group

Any data in haematology patients?
Bubalo JS et al. ASCO 2007, abstract 9112 30 patients receiving Cyclo/TBI or Bu/Cy allograft Randomised to aprepitant or placebo (plus
ondansetron +/- dex) Received aprepitant from d-7 to d+4 Complete or major response rate: 14/15 vs 7/15
(p=0.014) No emesis seen in 10/15 vs. 5/15 (p = ns) No difference wrt cyclophosphamide kinetics or
toxicity

Any data in haematology patients?
Mittaine et al. EBMT 2007, Abstract 1026 Aprepitant (3/7) + ondansetron in 5 patients
receiving Bu/Cy. No vomiting and 2 patients had 1 episode of nausea.
Domingues et al. EBMT 2008, Abstract 1235 Domingues et al. EBMT 2009, Abstract 1202
Aprepitant (days -5, -2, +1) + ondansetron in 8 patients receiving BEAM. Concluded that highly effective.

Current issues with aprepitant
Lack of data in BMT population but may be worth considering
How to deal with multiple-day chemotherapy
Little use of cisplatin in haematology
Can it replace dexamethasone?
Cost issues……

Cost issues
Comparative costs of antiemetics (BNF 2008)
02468
1012141618
Co
st
(£)
Cost/day (£)
Data misleading due to NHS contract prices for 5-HT3 antagonists – large differential between aprepitant and other agents

Mucositis as a complication of SCT
Incidence of mucositis with SCT conditioning regimens 70-80%
Consequences include pain, infection risk, inadequate nutrition, prolonged hospitalisation
Management mainly supportive Now have option of palifermin (recombinant
human keratinocyte growth factor)

Benefits of palifermin
Pivotal trial – Spielberger R et al. NEngl J Med 2004; 351: 2590-8
212 autograft patients receiving high dose chemo + TBI randomised to palifermin (60mcg/kg) or placebo
Incidence of mucositis (grade 4) – 20% vs 62% (p<0.001) Duration of mucositis (grade 3/4) – 3 vs 9 days (p<0.001)
Significant reduction in opioid and TPN requirements
Recent allograft study reported similar findings
Langer et al. BMT 2008; 42: 275-9

Can palifermin influence GVHD
Prevention of GI injury important in minimising aGVHD
Animal models demonstrated benefits of palifermin in incidence and severity of GVHD
Blazer B et al. Blood 2006; 108: 3216-22 Palifermin vs. placebo in 100 allograft recipients No difference wrt GVHD, relapse or survival Longer follow up failed to demonstrate any
differences between arms (Levine et al. Biol Blood Marrow Transplant 2008; 14: 1017-21)

Is there a role for palifermin? Trial data is reasonably strong but………..
The drug is very expensive - >£700/dose
Practice at QEH has been to give it to private patients undergoing SCT. About 25 patients treated to date Collected data on first 13 patients and demonstrated no clear
benefits compared to matched control-group (Khan, Duncan BOPA 2007). Lower-risk population?
Majority of patients developed a rash
Conclusion - may have a role with TBI-based schedules but too expensive for routine use

Management of GVHD
GVHD is the most frequent complication after allogeneic SCT.
Steroids the mainstay of treatment but steroid refractory GVHD has a mortality of 70% so need for effective 2nd line/alternative therapies
Lots of treatment options……. ATG, alemtuzumab, daclizumab,etanercept,
infliximab, pentostatin, MMF, budesonide, ECP, thalidomide, imatinib, rituximab

Recent trials in GVHD- budesonide
Andree H et al. BMT 2008; 42: 541-6 13 patients with cGVHD affecting the gut Some had received systemic steroid previously Received budesonide 3mg tds for median 5/12 7 patients achieved CR and 1 PR. Consider as alternative to systemic steroid in mild-
moderate cGVHD but caution re recurrence when treatment stopped.
Also shown efficacy in combination with systemic steroids in aGVHD of the gut – Bertz H et al. BMT 1999; 24: 1185-9

Recent trials in GVHD - imatinib
Magro L et al. BMT 2008; 42: 757-60 Sclerodermatous cGVHD historically difficult to treat
– incidence of about 11% Imatinib’s inihibition of PDGF and TGF pathways
may be of benefit – inhibits fibroblasts growth and collagen production
2 patients with refractory sclerodermatous GVHD treated with imatinib 400mg/day
Both had very good response with no tolerability issues
AT QEH, one patient with severe ocular cGVHD received imatinib for relapsed CML. GVHD improved dramatically.

Recent trials in GVHD – anti-TNF agents (1)
Infliximab drug of choice at QEH for steroid-refractory gut aGVHD – Italian study showed 59% RR in 32 patients (mainly gut +/- liverGVHD) – Patriarca F et al. Haematologica 2004; 89: 1352
Potential issues: 72% developed infection and 2 responding
patients died of fungal infection 10mg/kg/week for 4 weeks - £13,500 for 70kg
patient

Recent trials in GVHD – anti-TNF agents (2)
Etanercept has also shown promise against GVHD. Busca A et al. Am J Haematol 2007; 82: 45-52 21 patients with steroid-refractory GVHD 52% RR (64% in gut GVHD) High-rate of CMV reactivation and bacterial and fungal
infection
Also been used 1st line (+ steroids) - 69% CR rate vs 33% with steroid alone – Levine J et al. Blood 2008; 111: 2470-2475
25mg SC bw for 4/52, then weekly for 4/52 cost = £1200.

Conclusions
A number of interesting and novel recent developments in supportive care
Concerns: Affordability Quality of the trial data especially in setting of
GVHD