Embed Size (px)
Citation preview
Diabetes Mellitus
Barbara S. HaysWinter, 2006
Blood Glucose(normal serum level 65 – 105
mg)
• Inside CNS– Brain uses glucose as primary fuel– Brain cannot store/produce glucose
• Outside CNS– Fatty acids: stored as
• Glycogen (liver/muscles)• Triglycerides (fat cells)
Blood glucose, cont.
• Outside CNS, continued– Endocrine portion of pancreas: Islets of
Langerhans• Alpha cells make glucagon
– “counterregulatory”, acts opposite of insulin
• Beta cells make insulin– Allows body cells to store and use carbohydrate,
fats, and protein
Hyperglycemia
• When blood glucose becomes high– INSULIN allows glucose to enter cells
• Liver– Production /storage of glycogen– Inhibits glycogen breakdown– Increased protein & fat synthesis (VLDL
formation)
• Muscles– Promotes protein and glycogen synthesis
• Fat cells– Promotes storage of triglycerides
Hyperglycemia
• Drowsy• Flushed• Thirsty
Hypoglycemia
• Glucagon: causes release of glucose from liver– “glycogenolysis (breakdown of glycogen
to glucose)– “glyconeogenesis of glucose not
available• Lipolysis (breakdown of fat)• Proteolysis (breakdown of amino acids)
Hypoglycemia
• Weak, sweaty• Confused/irritable/
disoriented
Diabetes Mellitus(problem with glucose
metabolism)• Major health problem US/worldwide• Complications [lousy blood vessels]
– Blindness– Renal failure– Amputations– [heart attacks and strokes]– [OB/neonatal complications]
Diabetes Mellitus
The good news:– Blood glucose control reduces
complications of Diabetes!
Diabetes Mellitus
• Absence (or ineffectiveness of ) insulin
• Cellular resistance• Cells can’t use glucose for energy
– Starvation mode• Compensatory breakdown of body
fat/protein• Ketone bodies from faulty fat breakdown
» Metabolic acidosis, compensatory breathing (Kussmal’s breathing)
Diabetes Mellitus
• HYPERGLYCEMIA: fluid/electrolyte imbalance.– Polyuria
• Sodium, chloride, potassium excreted
– Polydipsia from dehydration– Polyphagia: cells are starving, so
person feels hungry despite eating huge amounts of food. Starvation state remains until insulin is available.
Diabetes Mellitus
• Complications of chronic hyperglycemia– Macrovascular complications
• Cardiovascular disease (heart attack)• Cerebrovascular disease (strokes)
– Microvascular• Blindness (retinal proliferation, macular
degeneration)• Amputations• Diabetic neuropathy (diffuse, generalized, or focal)• Erectile dysfunction
Classifying Diabetes Mellitus
• Type I Diabetes: autoimmune– Beta cell destruction in genetically
susceptible person
– Some viral infections
Classifying Diabetes Mellitus
• Type II Diabetes– Reduction in ability of most cells to
respond to insulin– Poor control of liver glucose output– Decreased beta-cell function (eventual
failure)
Diabetes Mellitus
• Major risk factors– Family history– Obesity– Origin (Afro-American, Hispanic, Native
American, Asian-American)– Age (older than 45)– History of gestational diabetes– High cholesterol– Hypertension
Diabetes Mellitus
• Prevention of effects: combination approach– Increased exercise
• Decreases need for insulin
– Reduce calorie intake• Improves insulin sensitivity
– Weight reduction• Improves insulin action
Triad of Treatment
• Diet
• Medication– Oral hypoglycemics– Insulins
• Exercise
Diabetes treatment
• Exercise– Under physician supervision– Check glucose prior
Diabetes treatment
• Diet– Lower calorie– Fewer foods of “high glycemic index”– Spread meals evenly
Diabetes treatment
• Anti-Diabetic medications– Oral hypoglycemic agents (“Easy” p
297)• Sulfonylureas• Thiazolidinediones• Biguanides• Alpha-glucosidase inhibitors• D-phenylalinine derivatives• Combinations
– Insulins (“Easy” Prototype Pro p 393)
Sulfonylureas
• Stimulate pancreas to secrete insulin– Glyburide (Diabeta) [Prototype Pro p 393]
• Glucotrol (Glipizide)• Diabenese (chlorpropamide)
• Adverse reactions– Hypoglycemia– Water retention/edema– Photosensitivity
• May need to add insulin in times of stress
Biguanides
• Decreases liver production of glucose• Decreases intestinal absorption of
glucose• Improves cell sensitivity to insulin
• Example: Metformin– GI upset, flatulence– Cardiac (CHF, MI)
Thiazolidinediones
• Increase cellular sensitivity to insulin– Pioglitazone (Actos)– Rosiglitazone (Avandia)
Client should have liver enzymes checked periodically
D-Phenylalanine derivatives
• Nateglinide (Starlix)
• Rapid onset, short half-life– Good for those with rapid post prandial
rise in blood glucose
Combinations
• Glucovance– Glyburide and Metformin
• Avandamet– Avandia and Metformin
[come tell me when you run into this question…]
Insulin
• Made in beta cells of the pancreas• Moves glucose into cells (thus acts
like growth hormone in a way)• Moves potassium into cells (can buy
time in emergencies)
Insulin preparations (“Easy” p 390)
given ONLY with syringes marked in “units”
• Rapid acting (lispro, asparte)
• Short acting (regular)
• Intermediate acting (NPH)
• Long acting– Ultralente– [Glargine/Lantus]
Your learning
• Onset of action
• Peak (blood glucose will be lowest then)
• Duration
Rapid acting insulin
• Lispro (Humolog, Novolog Aspart)– Onset of action
• “15-30” minutes [may come on in 5 minutes…]
– Peak of action• 1 - 2 hours
– Duration• 3 – 4 hours
Short acting insulins
• Regular (clear so can be given IV)– Onset of action
• 0.5 to 1 hour
– Peak of action• 2 – 4 hours
– Duration of action• 6 – 8 hours
Intermediate acting insulins
• NPH, Lente (chemicals added. Cloudy)– Onset of action
• 1 – 4 hours
– Peak of action• 4 – 12 hours
– Duration of action• 18 – 24 hours
Long acting insulins
• Ultralente– Onset of action
• 4 – 8 hours
– Peak of action• 18 hours
– Duration of action• 24 – 36 hours
Once a day insulin
• Glargine/Lantus– Cannot be diluted or mixed in syringe
with any other insulin– Slow, steady release– Daily dosing [usually at bedtime]– Refrigerated or tosses every 14 days
Combination insulins
• 70/30 (70% NPH and 30% regular)• Humolog 70/30 (Humolog and
regular)
• Fewer injections• Rotate sites to decrease
lipodystrophy
Miscellaneous
• Byetta for type II Diabetics taking sulfonylureas or combination– Mimics physiologic glucose control
• Inhances insulin secretion only in presence of hyperglycemia
• Insulin secretion decreases as blood glucose approaches normal
• Neutontin for Diabetic nerve pain
Some things to know
• Insulin moves potassium into cells– Good for emergency situations– Dangerous if potassium level already
low
Some things to know…
• HHNK (Hyperglycemic Hyperosmolar Non-Ketotic Coma). Also called– HHNK– HNKS [syndrome]
• Like dibetic ketoacidosis, without the ketones
• Type II diabetic, makes enough insulin to avoid ketones, but sugar guilds up to dangerous levels -> cellular dehydration
Some things to know…
• Dawn Phenomenon vs Somogi’s effect– Dawn phenomenon
• Blood sugar rises in early morning
– Somogi’s (rebound) effect• Blood sugar rise in morning as reaction to
hypoglycemic time during the night
Some things to know…
• Diabetic foot care– Dry, cracked skin + poor circulation
could = loss of a limb
– For the most part nurses don’t trim nails of diabetic clients. Refer to Podiatrist.
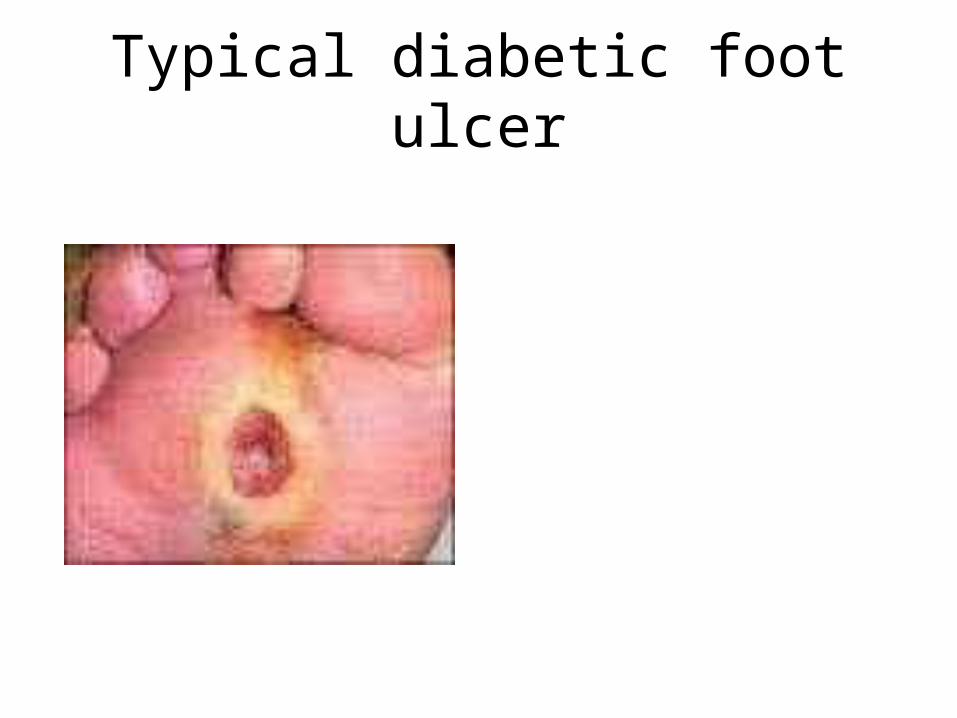
Typical diabetic foot ulcer