Embed Size (px)
Citation preview
Diabetes UpdateDiabetes Update
Division of EndocrinologyDivision of EndocrinologyDepartment of MedicineDepartment of Medicine
Wayne State University Medical SchoolWayne State University Medical SchoolDetroit, Michigan Detroit, Michigan
Part 1 of 3

DiabeticRetinopathy
Leading causeof blindnessin adults
DiabeticNephropathy
Major cause of kidney failure
CardiovascularDisease
Stroke
DiabeticNeuropathy
Major cause of lower extremity amputations
CV Disease & Stroke account for ~65% of deaths in T2D patients
Type 2 Diabetes Associated with Serious Complications
CV = cardiovascular.National Institute of Diabetes and Digestive and Kidney Diseases. National Diabetes Statistics fact sheet: general information and national estimates on diabetes in the United States, 2005. Bethesda, MD: U.S. Department of Health and Human Services, National Institute of Health, 2005.

33
Cost ($ billions)
42% Of Diabetes Costs Related To Hospitalization 42% Of Diabetes Costs Related To Hospitalization And Long-Term CareAnd Long-Term Care
$200 Billion $200 Billion Total!Total!
2010 US Total Healthcare Costs Attributable To Diabetes
5050
4040
3030
2020
1010
00Direct CostsDirect Costs Indirect CostsIndirect Costs‡‡
Oral AntidiabeticsInsulin and SuppliesOutpatient Medication*Outpatient Services†
Physician Office VisitsNursing Home Care (11%)Inpatient Care (31%)

ADA and AACE/ACE Guidelines:Treatment Goals for A1C, FPG, and PPG
ParameterNormal1,2
LevelADA3 Goal
AACE/ACE2
Goal
FPG, mg/dL <100 90–130 <110
PPG, mg/dL <140 <180 <140
A1C, % 4–6 <7a ≤6.5
FPG=fasting plasma glucose; PPG=postprandial glucose; ADA=American Diabetes Association; AACE=American Association of Clinical Endocrinologists; ACE=American College of Endocrinology.
1. Adapted from Buse J et al. In: Williams Textbook of Endocrinology. 10th ed. 2003. Permission requested.2. AACE Diabetes Mellitus Clinical Practice Guidelines Task Force. Endocr Pract. 2007;13:(suppl 1)3–68. 3. ADA. Diabetes Care. 2007;30:S4–S41.
aThe goal for an individual patient is to achieve an A1C as close to normal (<6%) as possible without significant hypoglycemia.aThe goal for an individual patient is to achieve an A1C as close to normal (<6%) as possible without significant hypoglycemia.
5
Components of HbA1cComponents of HbA1c
HbA1c = FBS + PPBS
6
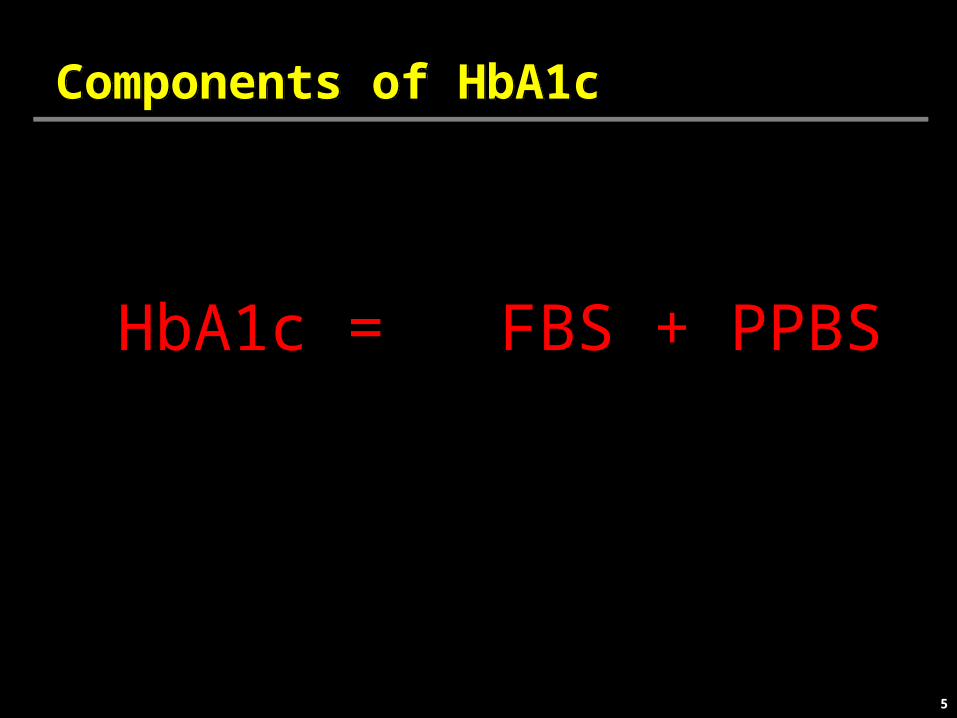
Both Fasting and Postprandial Hyperglycemia Contribute to A1CBoth Fasting and Postprandial Hyperglycemia Contribute to A1C
Plasma Glucose (mg/dL)
Adapted from Riddle MC. Diabetes Care. 1990;13:676-686
300
200
100
0
Time of Day
6 AM 12 PM 6 PM 12 AM 6 AM
Normal glycemic exposure
A1C ~5%
Uncontrolled DiabetesWith A1C ~8%
PostprandialHyperglycemia
Fasting Hyperglycemia

Normal Physiology
DEMAND SUPPLY
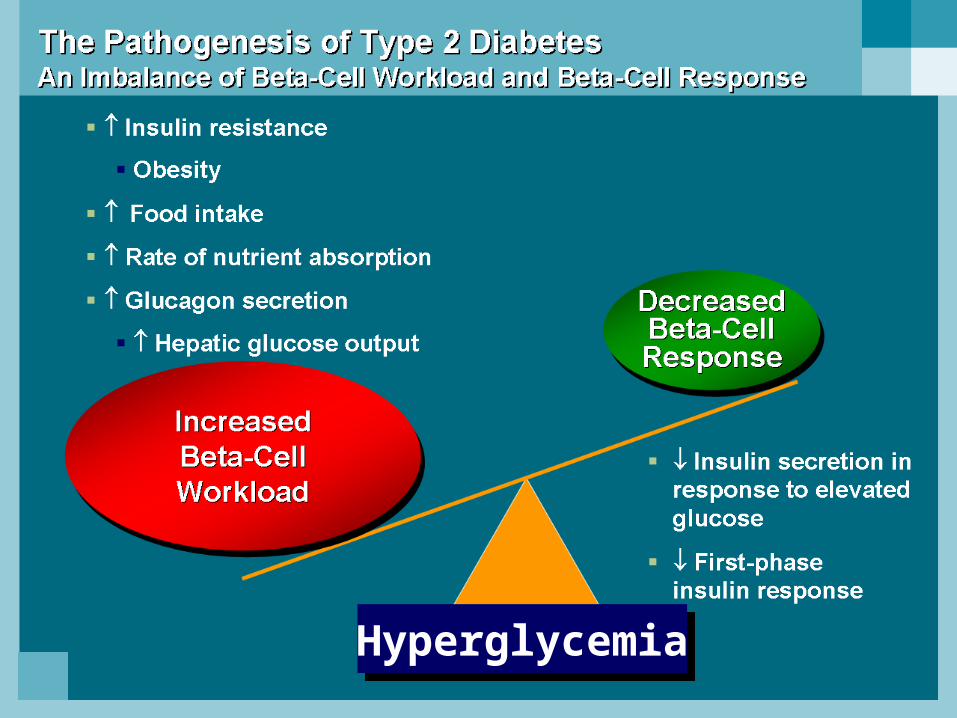
HyperglycemiaHyperglycemia
9
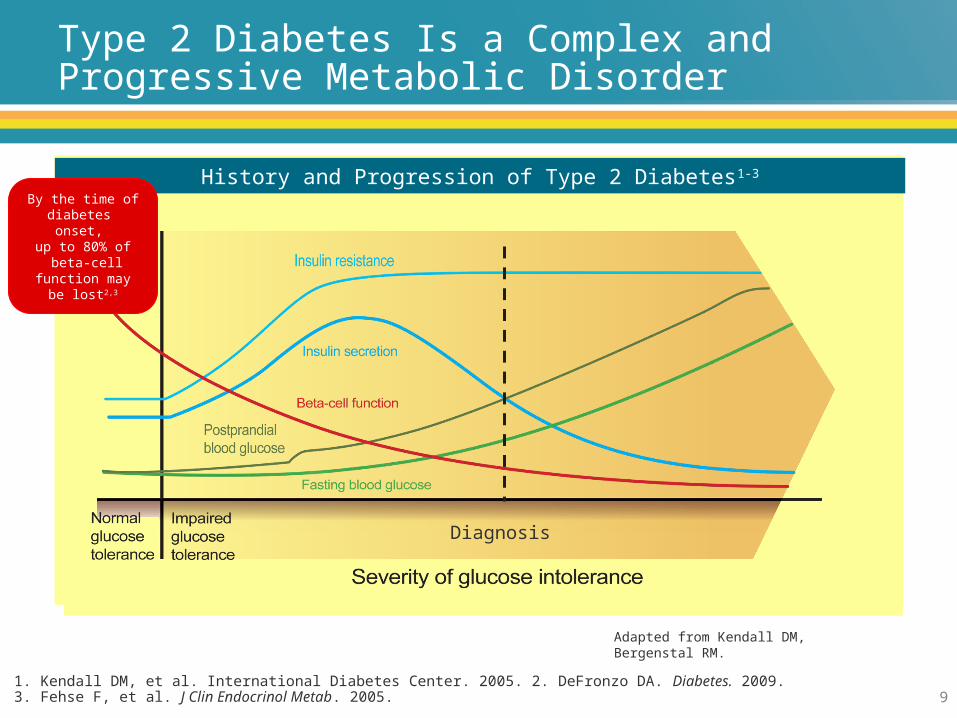
Type 2 Diabetes Is a Complex and Progressive Metabolic Disorder
1. Kendall DM, et al. International Diabetes Center. 2005. 2. DeFronzo DA. Diabetes. 2009. 3. Fehse F, et al. J Clin Endocrinol Metab. 2005.
Adapted from Kendall DM, Bergenstal RM.
History and Progression of Type 2 Diabetes1-3
By the time of diabetes onset,
up to 80% of beta-cell function
may be lost2,3
Diagnosis

10
Unmet Needs for Type 2 DM Treatment
Durable HbA1c control (i.e. help improve Beta-cell function).
Addressing islet dysfunction (i.e., addressing both insulin and glucagon secretion.
Addressing both fasting and postprandial sugars
Minimum risk of treatment-limiting adverse events:
-Minimum risk of hypoglycemia
-Minimum risk of weight gain
-No increased risk of edema
-No increased risk of heart failure