Embed Size (px)
DESCRIPTION
refarat diabetic foot
Citation preview

DIABETIC FOOT
I. INTRODUCTION
Diabetes mellitus (DM) refers to a group of common metabolic disorders
that share the phenotype of hyperglycemia. Several distinct types of DM are
caused by a complex interaction of genetics and environmental factors. Depending
on the etiology of the DM, factors contributing to hyperglycemia include reduced
insulin secretion, decreased glucose utilization, and increased glucose production.
The metabolic deregulations associated with DM causes secondary
pathophysiologic changes in multiple organ systems that impose a tremendous
burden on the individual with diabetes and on the health care system.1
In the United States, DM is the leading cause of end-stage renal disease
(ESRD), non traumatic lower extremity amputations, and adult blindness. It also
predisposes to cardiovascular diseases. With an increasing incidence worldwide,
DM will be a leading cause of morbidity and mortality for the foreseeable future.1
Two features of the current classification of DM diverge from previous
classifications. First, the terms insulin-dependent diabetes mellitus (IDDM) and
non-insulin-dependent diabetes mellitus (NIDDM) are obsolete. 1
The complications of longstanding diabetes mellitus often appear in the
foot, causing chronic disability. Factors affecting the foot are: (1) a predisposition
to peripheral vascular disease; (2) damage to periph- eral nerves; (3) reduced
resistance to infection.2
II. EPIDEMIOLOGY
1

The prevalence of foot ulceration in the general diabetic population is 4–
10%, being lower (1.5–3.5%) in young and highest (5–10%) in older patients. The
lifetime risk for foot ulcers in diabetic patients is about 15%. The major adverse
outcome of foot ulceration is amputation. Data from several studies have
documented that foot ulcers precede approximately 85% of all amputations
performed in patients with diabetes. Risk of ulceration and amputation increases
2- to 4-fold with both age and duration of diabetes.3
More than 30 per cent of patients attending diabetic clinics have evidence
of peripheral neuropathy or vascular disease and about 40 per cent of non-
traumarelated amputations in British hospitals are for complications of diabetes. 2
‘Charcot joints’ occur in less than 1 per cent of diabetic patients, yet
diabetes is the commonest cause of a neuropathic joint in Europe and America
(leprosy and tertiary syphilis being the other common causes worldwide). The
mid-tarsal joints are the most commonly affected, followed by the MTP and ankle
joints. There is usually a provocative incident, such as a twisting injury or a
fracture, following which the joint collapses relatively painlessly.2
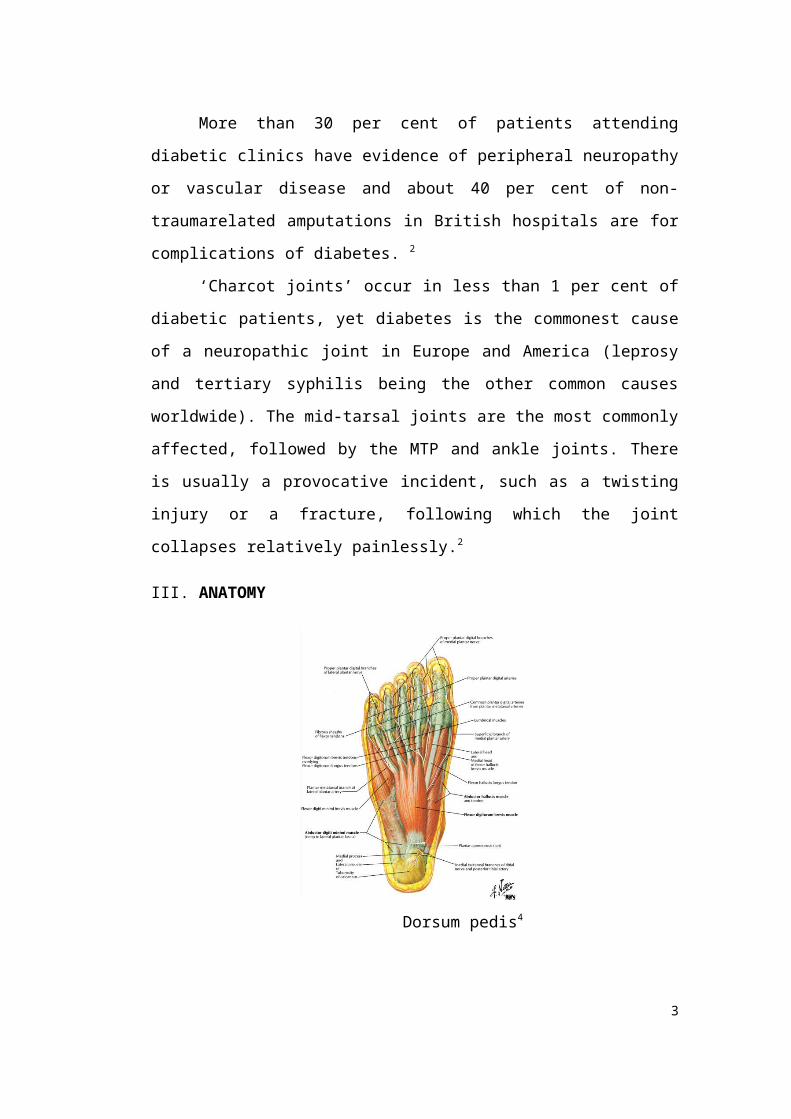
III. ANATOMY
Dorsum pedis4
2
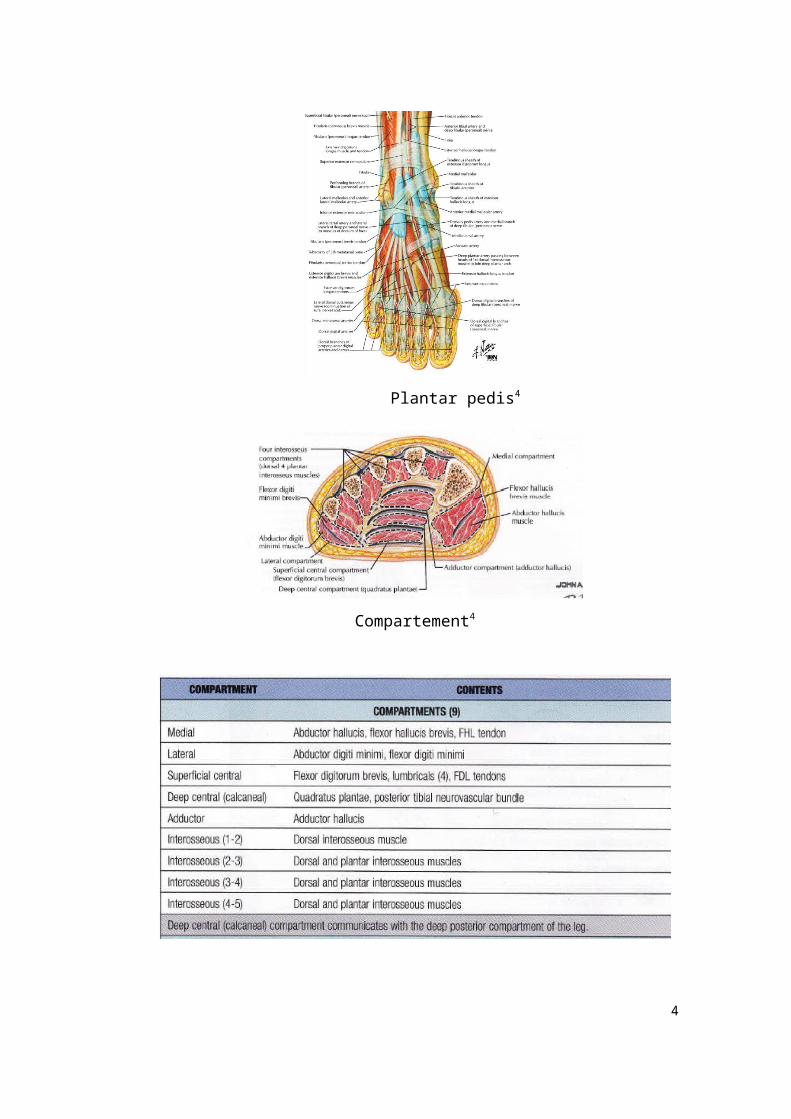
Plantar pedis4
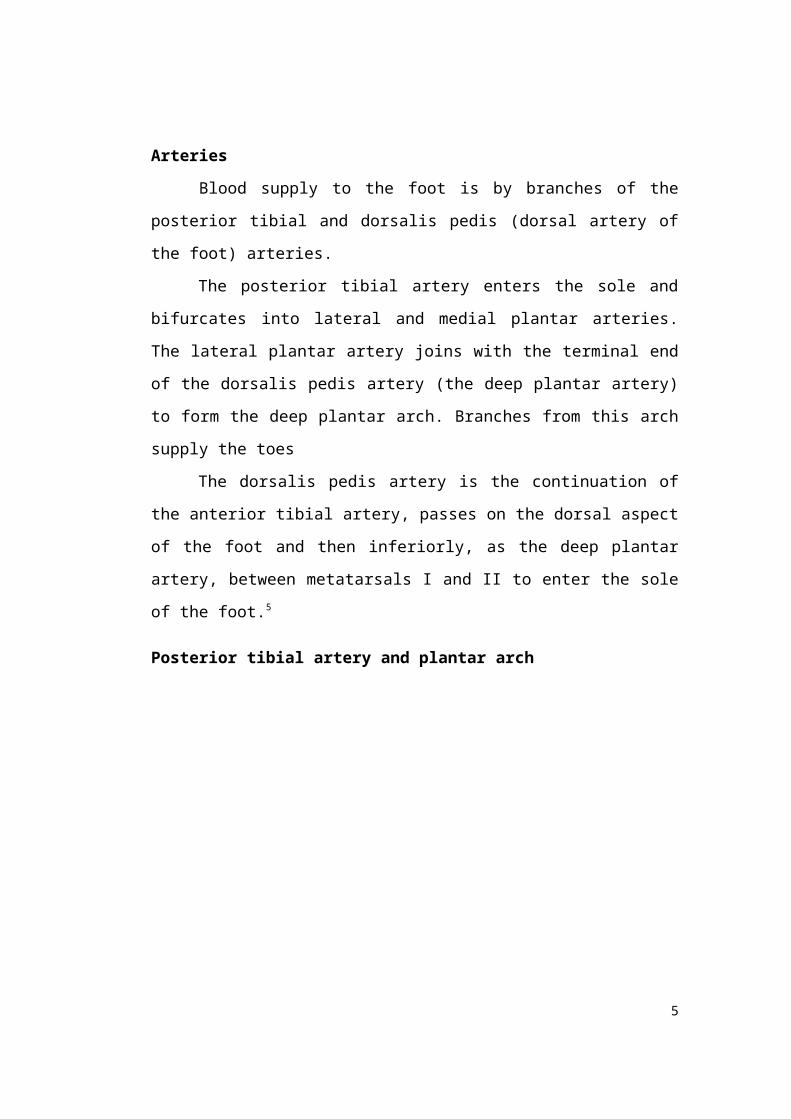
Compartement4
3
Arteries
Blood supply to the foot is by branches of the posterior tibial and dorsalis
pedis (dorsal artery of the foot) arteries.
The posterior tibial artery enters the sole and bifurcates into lateral and
medial plantar arteries. The lateral plantar artery joins with the terminal end of the
dorsalis pedis artery (the deep plantar artery) to form the deep plantar arch.
Branches from this arch supply the toes
The dorsalis pedis artery is the continuation of the anterior tibial artery,
passes on the dorsal aspect of the foot and then inferiorly, as the deep plantar
artery, between metatarsals I and II to enter the sole of the foot.5
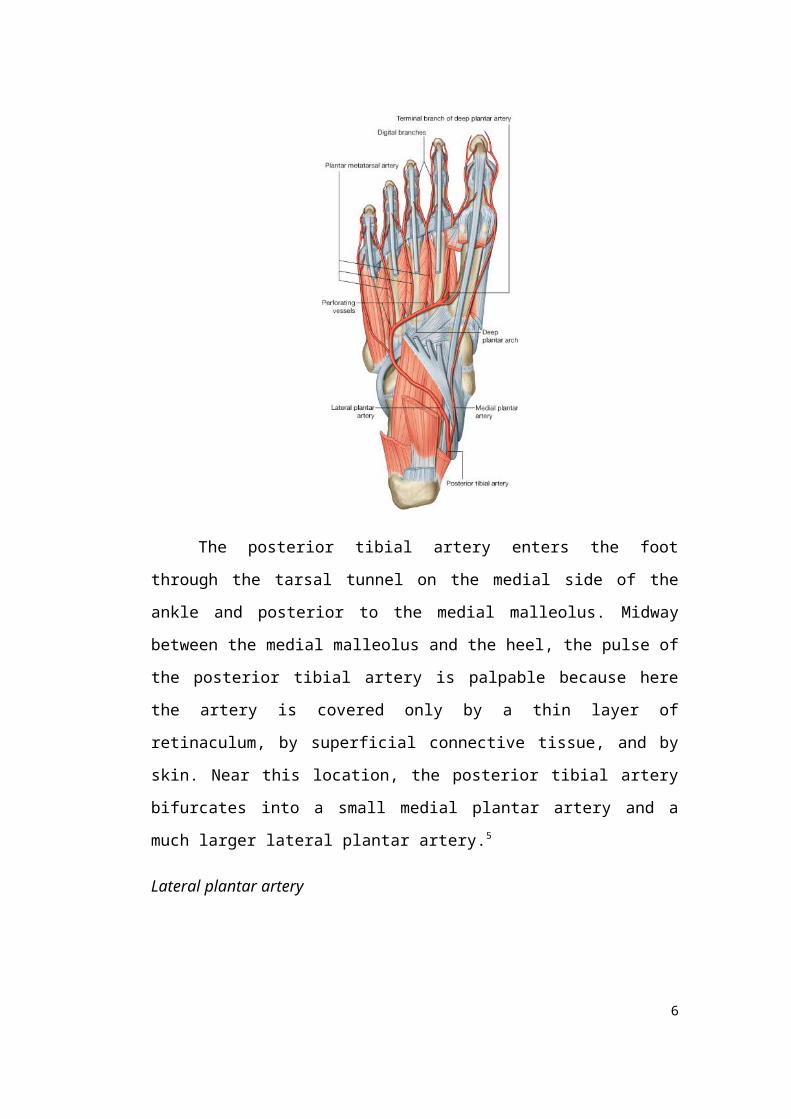
Posterior tibial artery and plantar arch
The posterior tibial artery enters the foot through the tarsal tunnel on the
medial side of the ankle and posterior to the medial malleolus. Midway between
the medial malleolus and the heel, the pulse of the posterior tibial artery is
palpable because here the artery is covered only by a thin layer of retinaculum, by
4
superficial connective tissue, and by skin. Near this location, the posterior tibial
artery bifurcates into a small medial plantar artery and a much larger lateral
plantar artery.5
Lateral plantar artery
The lateral plantar artery passes anterolaterally into the sole of the foot,
first deep to the proximal end of the abductor hallucis muscle and then between
the quadratus plantae and flexor digitorum brevis muscles. It reaches the base of
metatarsal V where it lies in the groove between flexor digitorum brevis and
abductor digiti minimi muscles. From here, the lateral plantar artery curves
medially to form the deep plantar arch, which crosses the deep plane of the sole
on the metatarsal bases and the interossei muscles.
Between the bases of the metatarsals I and II, the deep plantar arch joins
with the terminal branch (deep plantar artery) of the dorsalis pedis artery, which
enters the sole from the dorsal side of the foot.5
Major branches of the deep plantar arch include:
a digital branch to the lateral side of the little toe;
four plantar metatarsal arteries, which supply digital branches to adjacent
sides of toes I to V and the medial side of the great toe;
three perforating arteries, which pass between the bases of metatarsals II to
V to anastomose with vessels on the dorsal aspect of the foot.5
Medial plantar artery
The medial plantar artery passes into the sole of the foot by passing deep
to the proximal end of the abductor hallucis muscle. It supplies a deep branch to
adjacent muscles and then passes forward in the groove between the abductor
hallucis and the flexor digitorum brevis muscles. It ends by joining the digital
branch of the deep plantar arch, which supplies the medial side of the great toe.
Near the base of metatarsal I, the medial plantar artery gives rise to a
superficial branch, which divides into three vessels that pass superficial to the
5
flexor digitorum brevis muscle to join the plantar metatarsal arteries from the deep
plantar arch.
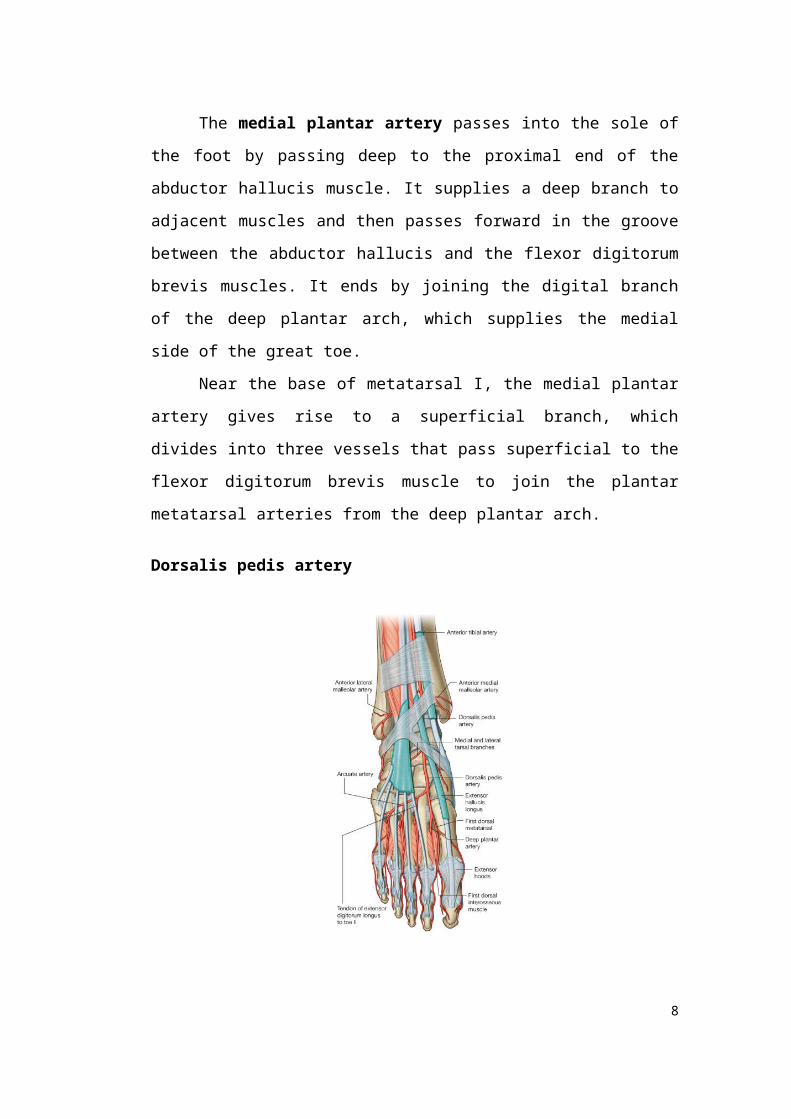
Dorsalis pedis artery
The dorsalis pedis artery is the continuation of the anterior tibial artery
and begins as the anterior tibial artery crosses the ankle joint. It passes anteriorly
over the dorsal aspect of the talus, navicular, and intermediate cuneiform bones,
and then passes inferiorly, as the deep plantar artery, between the two heads of the
first dorsal interosseous muscle to join the deep plantar arch in the sole of the foot.
The pulse of the dorsalis pedis artery on the dorsal surface of the foot can be felt
by gently palpating the vessel against the underlying tarsal bones between the
tendons of extensor hallucis longus and the tendon of extensor digitorum longus
to the second toe.
Branches of the dorsalis pedis artery include lateral and medial tarsal
branches, an arcuate artery, and a first dorsal metatarsal artery:
the tarsal arteries pass medially and laterally over the tarsal bones,
supplying adjacent structures and anastomosing with a network of vessels
formed around the ankle;
6

the arcuate artery passes laterally over the dorsal aspect of the
metatarsals near their bases and gives rise to three dorsal metatarsal
arteries, which supply dorsal digital arteries to adjacent sides of digits II
to V, and to a dorsal digital artery that supplies the lateral side of the digit
V;
the first dorsal metatarsal artery (the last branch of the dorsalis pedis
artery before the dorsalis pedis artery continues as the deep plantar artery
into the sole of the foot) supplies digital branches to adjacent sides of the
great and second toes.
The dorsal metatarsal arteries connect with perforating branches from the deep
plantar arch and similar branches from the plantar metatarsal arteries.5
Veins
There are interconnected networks of deep and superficial veins in the
foot. The deep veins follow the arteries. Superficial veins drain into a dorsal
venous arch on the dorsal surface of the foot over the metatarsals
the great saphenous vein originates from the medial side of the arch and
passes anterior to the medial malleolus and onto the medial side of the leg;
the small saphenous vein originates from the lateral side of the arch and
passes posterior to the lateral malleolus and onto the back of the leg. 5
Nerves
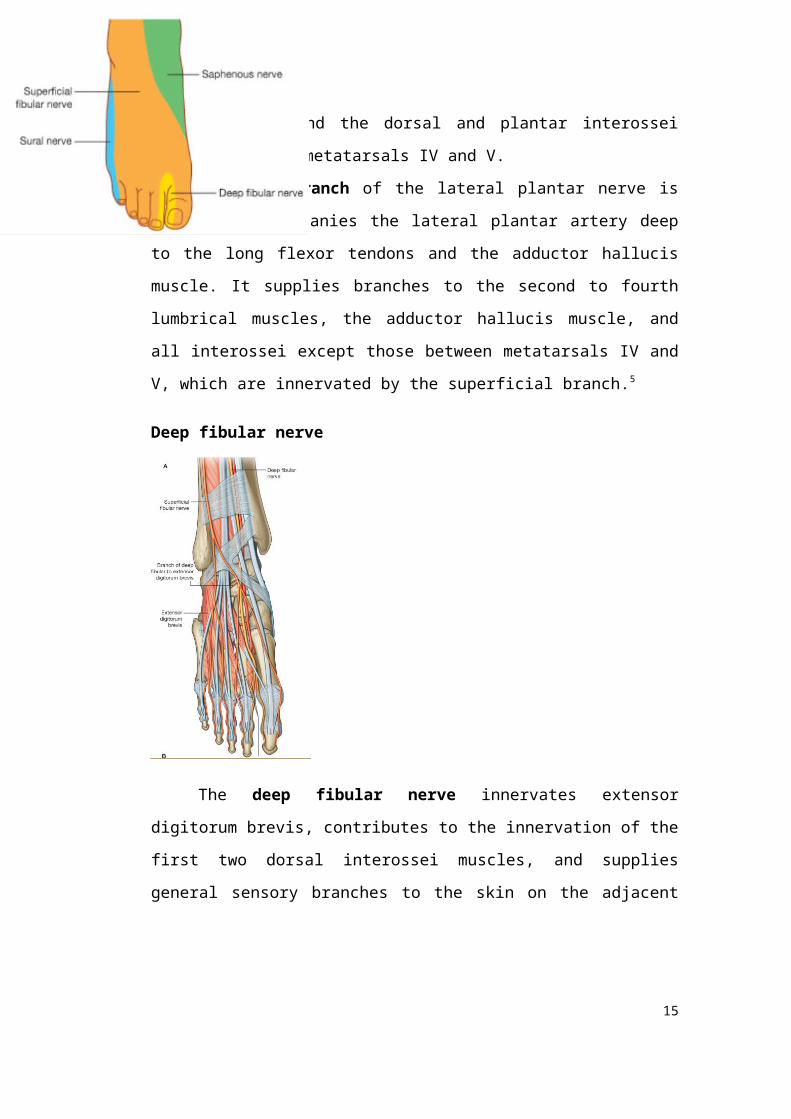
The foot is supplied by the tibial, deep fibular, superficial fibular, sural, and
saphenous nerves.
all five nerves contribute to cutaneous or general sensory innervation;
the tibial nerve innervates all intrinsic muscles of the foot except for
extensor digitorum brevis, which is innervated by the deep fibular nerve;
7
the deep fibular nerve often also contributes to the innervation of the first
and second dorsal interossei.5
Tibial nerve5
The tibial nerve enters the foot through the tarsal tunnel posterior to the
medial malleolus. In the tunnel, the nerve is lateral to the posterior tibial artery,
and gives origin to medial calcaneal branches, which penetrate the flexor
retinaculum to supply the heel. Midway between the medial malleolus and the
heel, the tibial nerve bifurcates with the posterior tibial artery into:
a large medial plantar nerve;
a smaller lateral plantar nerve
The medial and lateral plantar nerves lie together between their corresponding
arteries.
Medial plantar nerve
The medial plantar nerve is the major sensory nerve in the sole of the
foot. It innervates skin on most of the anterior two-thirds of the sole and adjacent
surfaces of the medial three and one-half toes, which includes the great toe. In
addition to this large area of plantar skin, the nerve also innervates four intrinsic
muscles-abductor hallucis, flexor digitorum brevis, flexor hallucis brevis, and the
first lumbrical.
The medial plantar nerve passes into the sole of the foot deep to the
abductor hallucis muscle and forward in the groove between abductor hallucis and
flexor digitorum brevis, supplying branches to both these muscles
8

The medial plantar nerve supplies a digital branch (proper plantar digital
nerve) to the medial side of the great toe and then divides into three nerves
(common plantar digital nerves) on the plantar surface of flexor digitorum
brevis, which continue forward to supply proper plantar digital branches to
adjacent surfaces of toes I to IV. The nerve to the first lumbrical originates from
the first common plantar digital nerve.5
Lateral plantar nerve
The lateral plantar nerve is an important motor nerve in the foot because
it innervates all intrinsic muscles in the sole, except for the muscles (abductor
hallucis, flexor digitorum brevis, flexor hallucis brevis, and first lumbrical)
supplied by the medial plantar nerve. It also innervates a strip of skin on the
lateral side of the anterior two-thirds of the sole and the adjacent plantar surfaces
of the lateral one and one-half digits.5
9
The lateral plantar nerve enters the sole of the foot by passing deep to the
proximal attachment of the abductor hallucis muscle. It continues laterally and
anteriorly across the sole between the flexor digitorum brevis and quadratus
plantae muscles, supplying branches to both these muscles, and then divides near
the head of metatarsal V into a deep and superficial branch.
The superficial branch of the lateral plantar nerve gives rise to a proper
plantar digital nerve, which supplies skin on the lateral side of the little toe and
to a common plantar digital nerve, which divides to supply proper plantar
digital nerves to skin on the adjacent sides of toes IV and V.
The proper plantar digital nerve to the lateral side of the little toe also
innervates flexor digiti minimi brevis and the dorsal and plantar interossei
muscles between metatarsals IV and V.
The deep branch of the lateral plantar nerve is motor and accompanies the
lateral plantar artery deep to the long flexor tendons and the adductor hallucis
muscle. It supplies branches to the second to fourth lumbrical muscles, the
adductor hallucis muscle, and all interossei except those between metatarsals IV
and V, which are innervated by the superficial branch.5
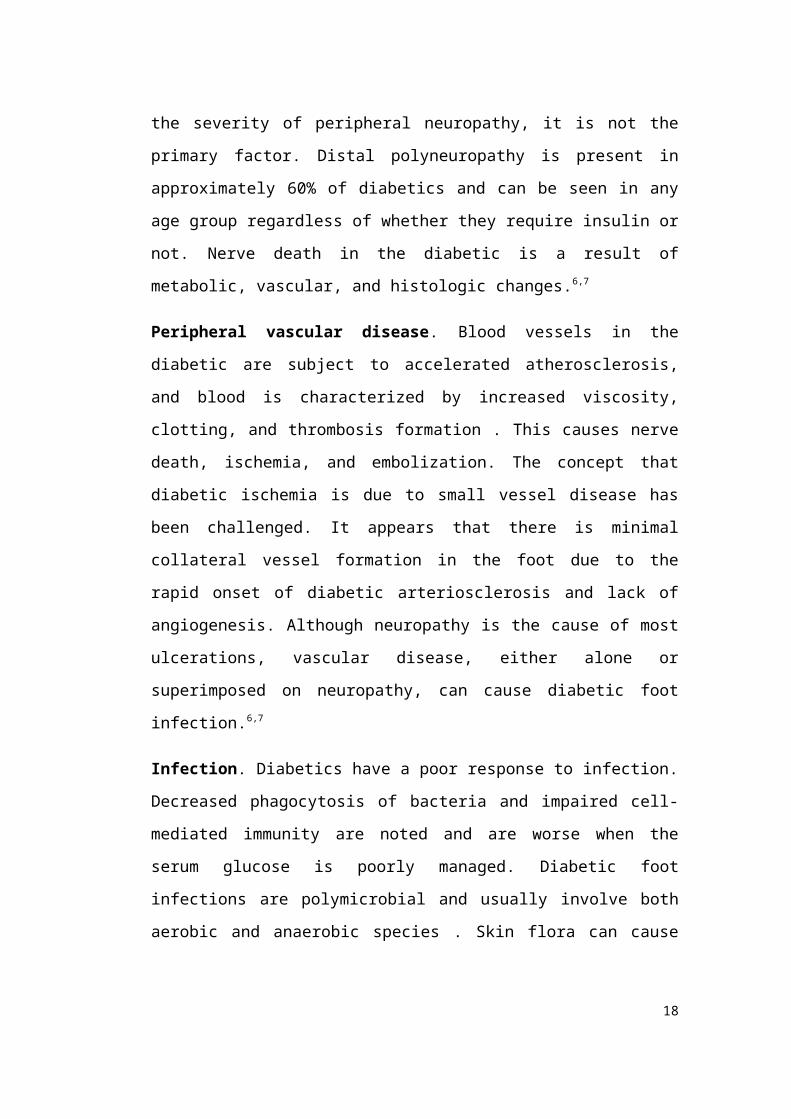
Deep fibular nerve
10

The deep fibular nerve innervates extensor digitorum brevis, contributes
to the innervation of the first two dorsal interossei muscles, and supplies general
sensory branches to the skin on the adjacent dorsal sides of the first and second
toes and to the web space between them.
The deep fibular nerve enters the dorsal aspect of the foot on the lateral
side of the dorsalis pedis artery, and is parallel with and lateral to the tendon of
the extensor hallucis longus muscle. Just distal to the ankle joint, the nerve gives
origin to a lateral branch, which innervates extensor digitorum brevis from its
deep surface.
The deep fibular nerve continues forward on the dorsal surface of the foot,
penetrates deep fascia between metatarsals I and II near the metatarsophalangeal
joints, and then divides into two dorsal digital nerves, which supply skin over
adjacent surfaces of toes I and II.
Small motor branches, which contribute to the supply of the first two dorsal
interossei muscles, originate from the deep fibular nerve before it penetrates deep
fascia.5
Superficial fibular nerve
The superficial fibular nerve is sensory to most skin on the dorsal aspect
of the foot and toes except for skin on adjacent sides of toes I and II (which is
innervated by the deep fibular nerve) and skin on the lateral side of the foot and
little toe (which is innervated by the sural nerve;).
The superficial fibular nerve penetrates deep fascia on the anterolateral
side of the lower leg and enters the dorsal aspect of the foot in superficial fascia. It
gives rise to cutaneous branches and dorsal digital nerves along its course.5
Sural nerve
The sural nerve is a cutaneous branch of the tibial nerve that originates
high in the leg. It enters the foot in superficial fascia posterior to the lateral
malleolus close to the short saphenous vein. Terminal branches innervate skin on
the lateral side of the foot and dorsolateral surface of the little toe.5
11

Saphenous nerve
The saphenous nerve is a cutaneous branch of the femoral nerve that
originates in the thigh. Terminal branches enter the foot in superficial fascia on
the medial side of the ankle and supply skin on the medial side of the proximal
foot.
IV. ETIOLOGY
Peripheral neuropathy. Peripheral neuropathy is usually present in patients with
diabetic foot infections. Although peripheral vascular disease can contribute to the
severity of peripheral neuropathy, it is not the primary factor. Distal
polyneuropathy is present in approximately 60% of diabetics and can be seen in
any age group regardless of whether they require insulin or not. Nerve death in the
diabetic is a result of metabolic, vascular, and histologic changes.6,7
Peripheral vascular disease. Blood vessels in the diabetic are subject to
accelerated atherosclerosis, and blood is characterized by increased viscosity,
clotting, and thrombosis formation . This causes nerve death, ischemia, and
embolization. The concept that diabetic ischemia is due to small vessel disease has
been challenged. It appears that there is minimal collateral vessel formation in the
foot due to the rapid onset of diabetic arteriosclerosis and lack of angiogenesis.
Although neuropathy is the cause of most ulcerations, vascular disease, either
alone or superimposed on neuropathy, can cause diabetic foot infection.6,7
Infection. Diabetics have a poor response to infection. Decreased phagocytosis of
bacteria and impaired cell-mediated immunity are noted and are worse when the
serum glucose is poorly managed. Diabetic foot infections are polymicrobial and
usually involve both aerobic and anaerobic species . Skin flora can cause deep
infections in diabetics, occasionally making it difficult to determine the
correlation between cultures taken from superficial ulcers or sinus tracts and the
true pathogens causing deep infection . Therefore, the most meaningful cultures
are those that are taken in the operating room from deep tissue underneath the
12

ulcers or open wounds. Many of the acute soft tissue infections are caused by
streptococci or Staphylococcus aureus, which may be found as the single
pathogenic species. With an a monomicrobic anaerobic infection.6,7
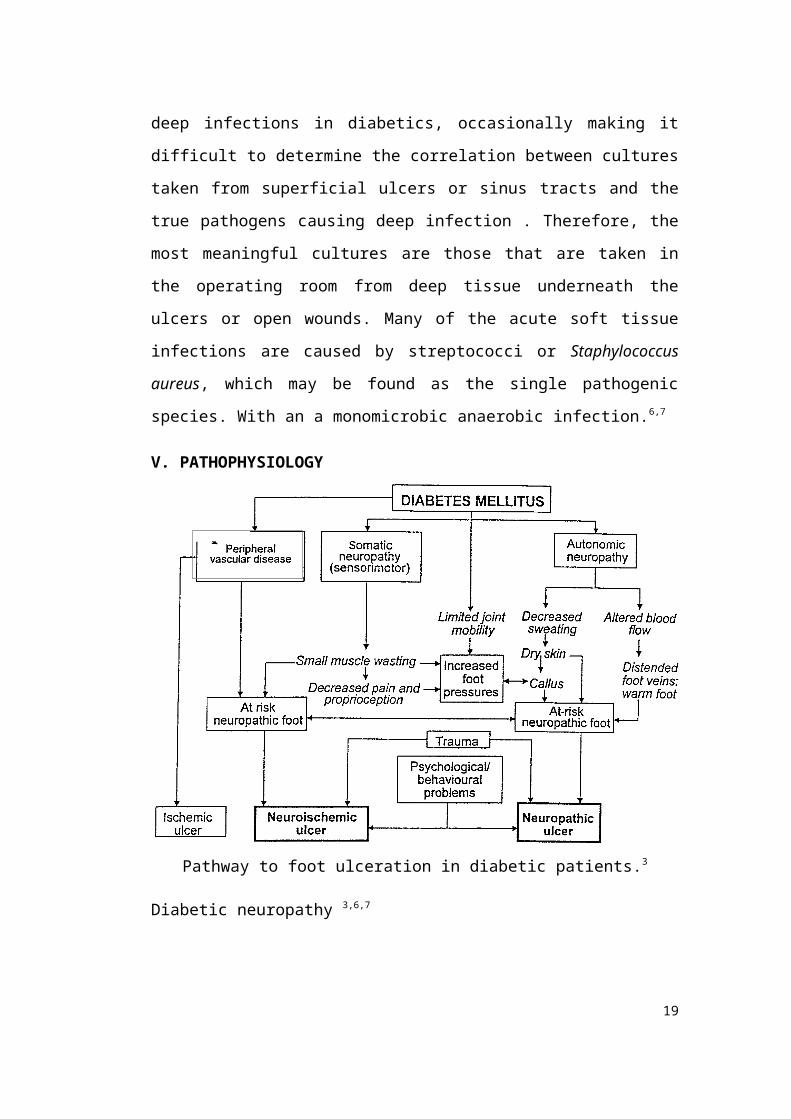
V. PATHOPHYSIOLOGY
Pathway to foot ulceration in diabetic patients.3
Diabetic neuropathy 3,6,7
1. The diagnosis of foot ulcerations results in the greatest rate of hospital
admissions in diabetic patients, as well as lower extremity amputations.
2. The combination of neuropathy and excess pressure on the plantar foot leads to
ulceration.
3. Sensation
Polyneuropathic loss of sensation begins in a stocking distribution of the
feet and progresses proximally.
Diagnosed by the inability to perceive the 5.07 Semmes-Weinstein
monofilament
13
90% of patients who cannot feel the 5.07 monofilament have lost
protective sensation to their feet and are at risk for ulceration.
With the Therapeutic Shoe Bill, money is allocated for neuropathic
patients to purchase extradepth shoes and total contact inserts (three per
year) for ulcer prevention.
4. Autonomic neuropathy
An abnormal sweating mechanism leads to a dry foot.
Vulnerable to fissuring cracks, which then become portals for infection.
5. Motor neuropathy
Most commonly involves the common peroneal nerve
Resultant loss of tibialis anterior motor function and a footdrop
Small intrinsic musculature of the foot also commonly affected, resulting
in claw toes and subsequent toe-tip ulcerations due to excessive pressure
Hypomobility syndrome3,6,7
1. Result of excessive glycosylation of the soft tissues of the extremities.
2. Leads to decreased joint ROM
Peripheral vascular disease3,6,7
1. Occurs in 60% to 70% of patients who have had diabetes for over 10 years,
involving both large and small vessels
2. Noninvasive vascular examination should be performed when pulses are not
palpable.
Waveforms (normal is triphasic)
Ankle-brachial indices (minimum for healing, 0.45; normal, 1.0)
Calcifications in the artery can falsely elevate the ankle-brachial index.
Greater than 1.3 is nonphysiologic and consistent with calcification of the
vessels.
Absolute toe pressures (minimum for healing, 40 mm Hg; normal, 100
mm Hg)
14
3. Transcutaneous oxygen pressure of the toes greater than 40 mm Hg have been
found to be predictive of healing.
Immune system impairment3,6,7
1. Poor cellular defenses such as abnormal phagocytosis, altered chemotaxis of the
WBCs, and a poor cytotoxic environment (due to hyperglycemia) to fight off
bacteria lead to difficulty in fighting off infection once it has developed.
E. Metabolic deficiency
1. Reduced total protein less than 6.0 g/dL, WBC count less than 1500, and
albumin levels less than 2.5 g/dL result in poor healing potential.
VI. CLINICAL PRESENTATION
Neuropathic3
Neuropathy is present in about 85–90%
of foot ulcers in patients with diabetes.
Develop at areas of high plantar
pressures
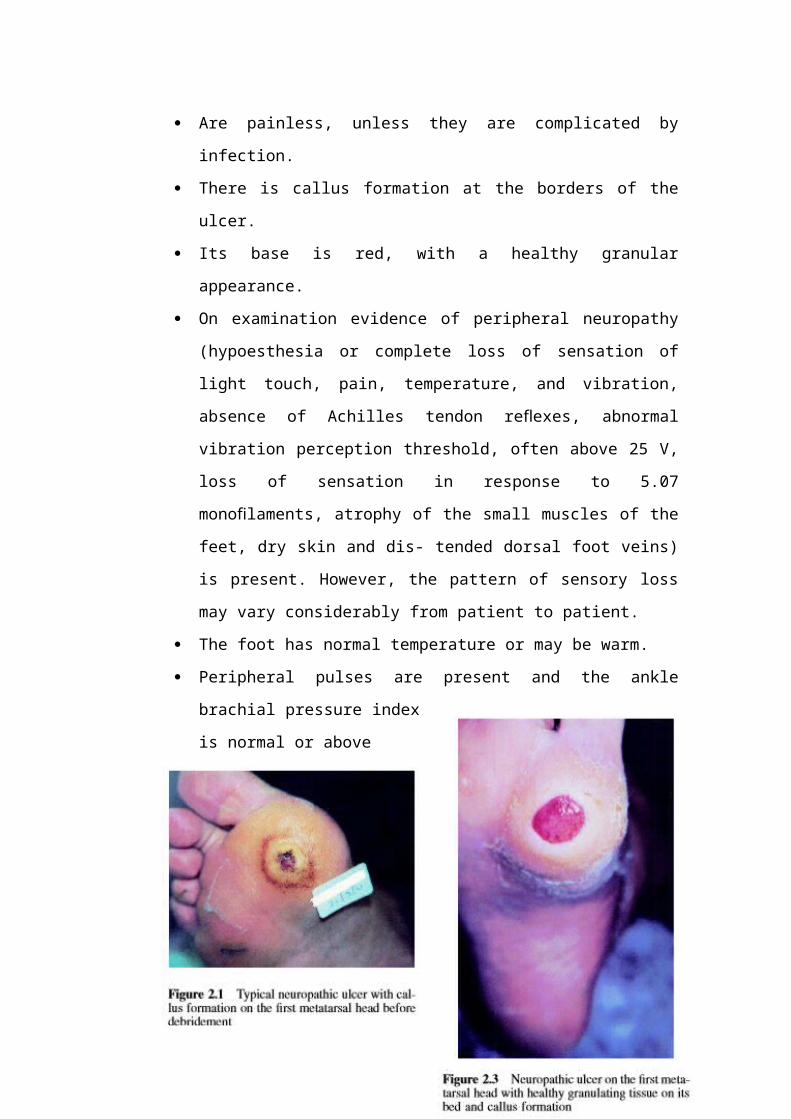
Are painless, unless they are
complicated by infection.
There is callus formation at the borders
of the ulcer.
Its base is red, with a healthy granular
appearance.
On examination evidence of peripheral
neuropathy (hypoesthesia or complete
loss of sensation of light touch, pain,
temperature, and vibration, absence of
Achilles tendon reflexes, abnormal vibration perception threshold, often
above 25 V, loss of sensation in response to 5.07 monofilaments, atrophy
of the small muscles of the feet, dry skin and dis- tended dorsal foot veins)
15

is present. However, the pattern of sensory loss may vary considerably
from patient to patient.
The foot has normal temperature or may be warm.
Peripheral pulses are present and the ankle brachial pressure index is
normal or above
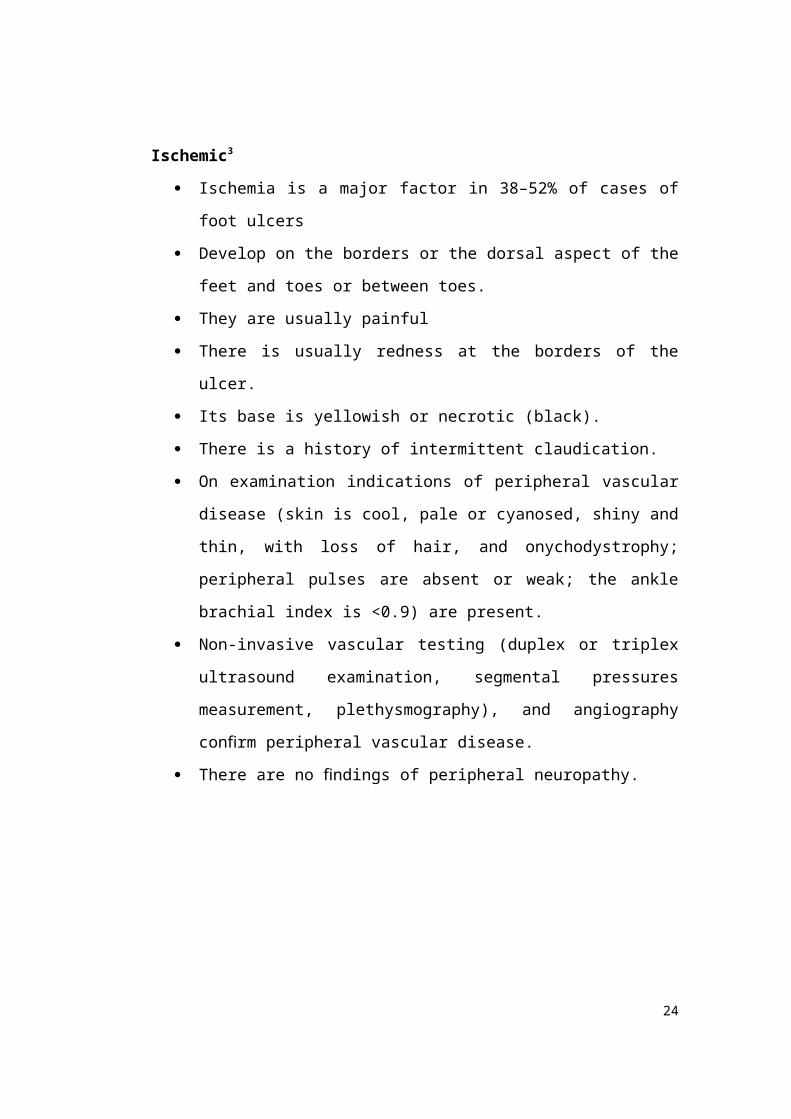
Ischemic3
Ischemia is a major factor in 38–52% of cases of foot ulcers
Develop on the borders or the dorsal aspect of the feet and toes or between
toes.
They are usually painful
There is usually redness at the borders of the ulcer.
Its base is yellowish or necrotic (black).
There is a history of intermittent claudication.
16

On examination indications of peripheral vascular disease (skin is cool,
pale or cyanosed, shiny and thin, with loss of hair, and onychodystrophy;
peripheral pulses are absent or weak; the ankle brachial index is <0.9) are
present.
Non-invasive vascular testing (duplex or triplex ultrasound examination,
segmental pressures measurement, plethysmography), and angiography
confirm peripheral vascular disease.
There are no findings of peripheral neuropathy.
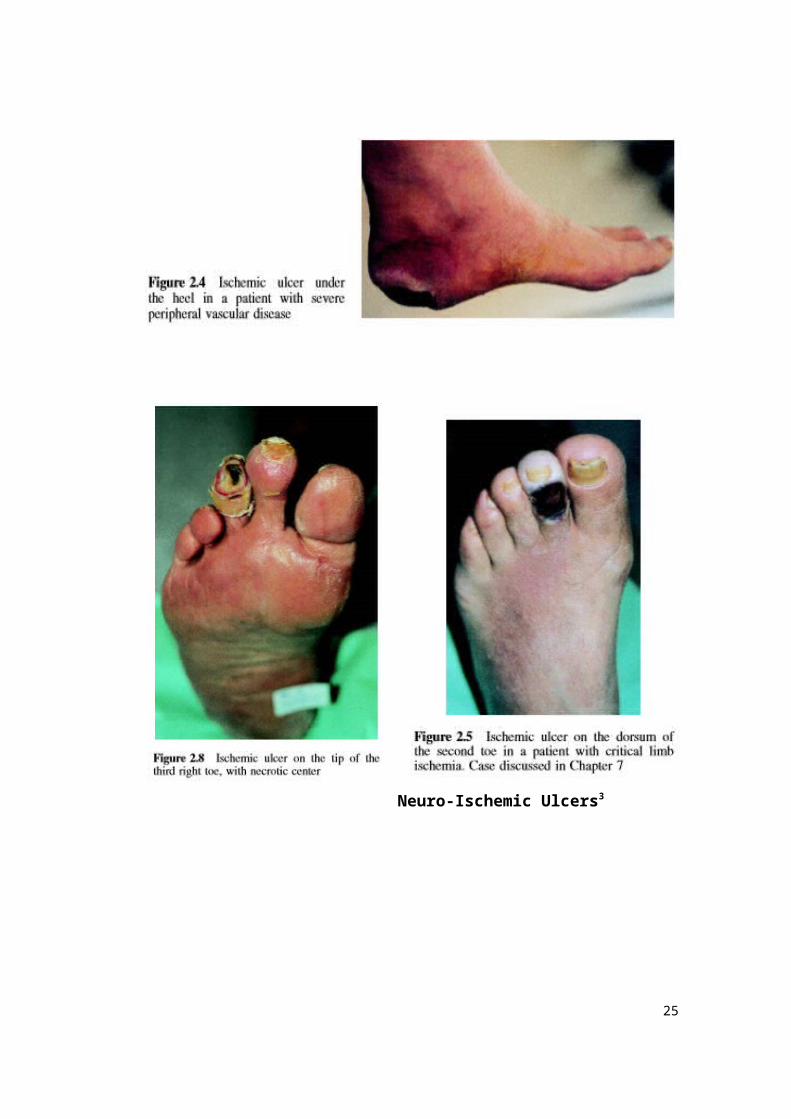
Neuro-Ischemic Ulcers3
17
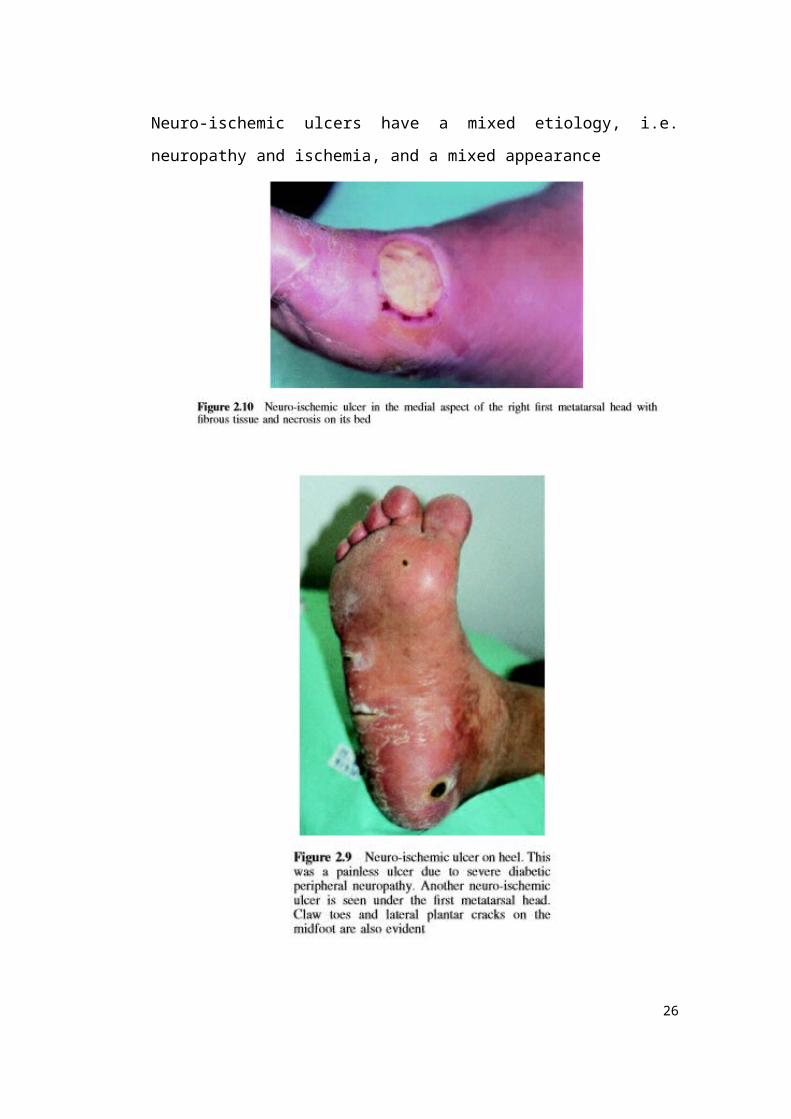
Neuro-ischemic ulcers have a mixed etiology, i.e. neuropathy and ischemia, and a
mixed appearance
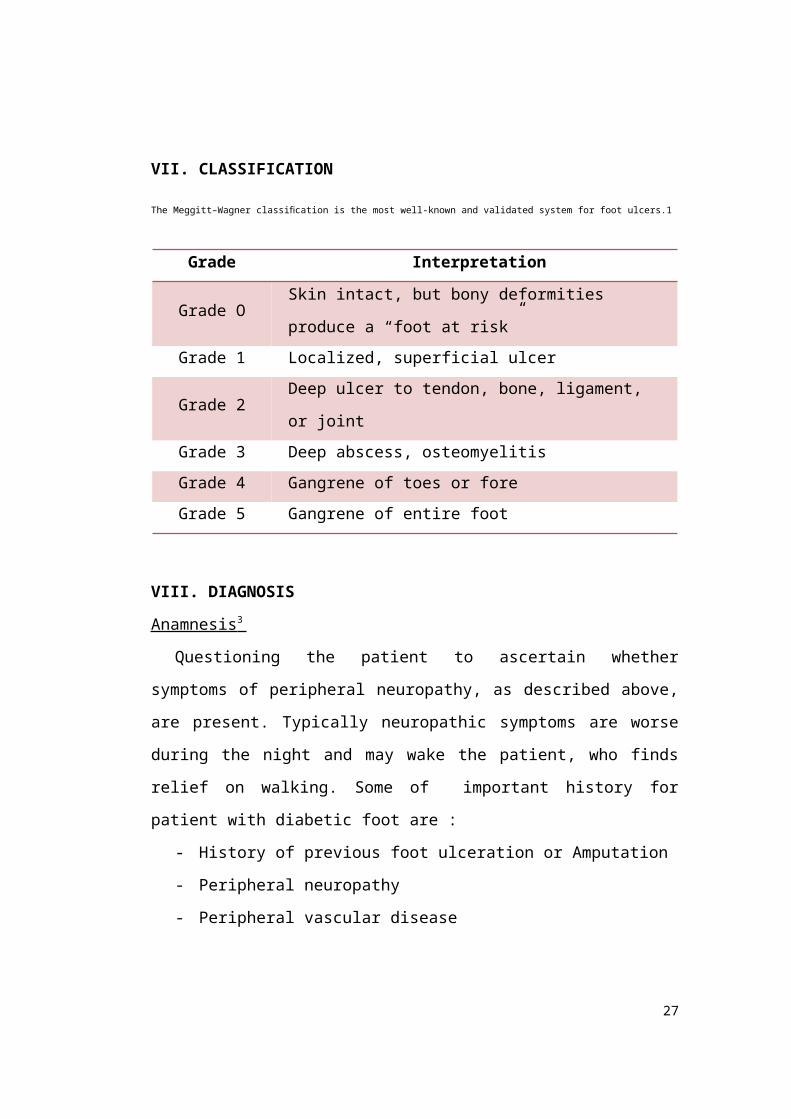
VII. CLASSIFICATION
18
The Meggitt–Wagner classification is the most well-known and validated system for foot ulcers.1
Grade Interpretation
Grade O Skin intact, but bony deformities produce a “foot at risk”
Grade 1 Localized, superficial ulcer
Grade 2 Deep ulcer to tendon, bone, ligament, or joint
Grade 3 Deep abscess, osteomyelitis
Grade 4 Gangrene of toes or fore
Grade 5 Gangrene of entire foot
VIII. DIAGNOSIS
Anamnesis 3
Questioning the patient to ascertain whether symptoms of peripheral
neuropathy, as described above, are present. Typically neuropathic symptoms are
worse during the night and may wake the patient, who finds relief on walking.
Some of important history for patient with diabetic foot are :
- History of previous foot ulceration or Amputation
- Peripheral neuropathy
- Peripheral vascular disease
- Trauma (poor footwear, walking barefoot, objects inside the shoes)
- Foot deformities (prominent metatarsal heads, claw tow, hammer toe, pes
cavus, nail deformities, deformities related to previous trauma and surgery,
bony prominences, etc.)
- Callus formation
- Neuro-osteoarthropathy
- Limited joint mobility
- Long duration of diabetes
- Poor diabetes control
Physical examination 3
19

All patients with diabetes should be examined annually for peripheral
neuropathy, so that those at risk for ulceration can be identified. The tests for
peripheral neuropathy are many and some of them are quite sophisticated, and are
undertaken only in specialist centers. However, the tests that are used to
characterize the patient with loss of protective sensation are simple, fast and easily
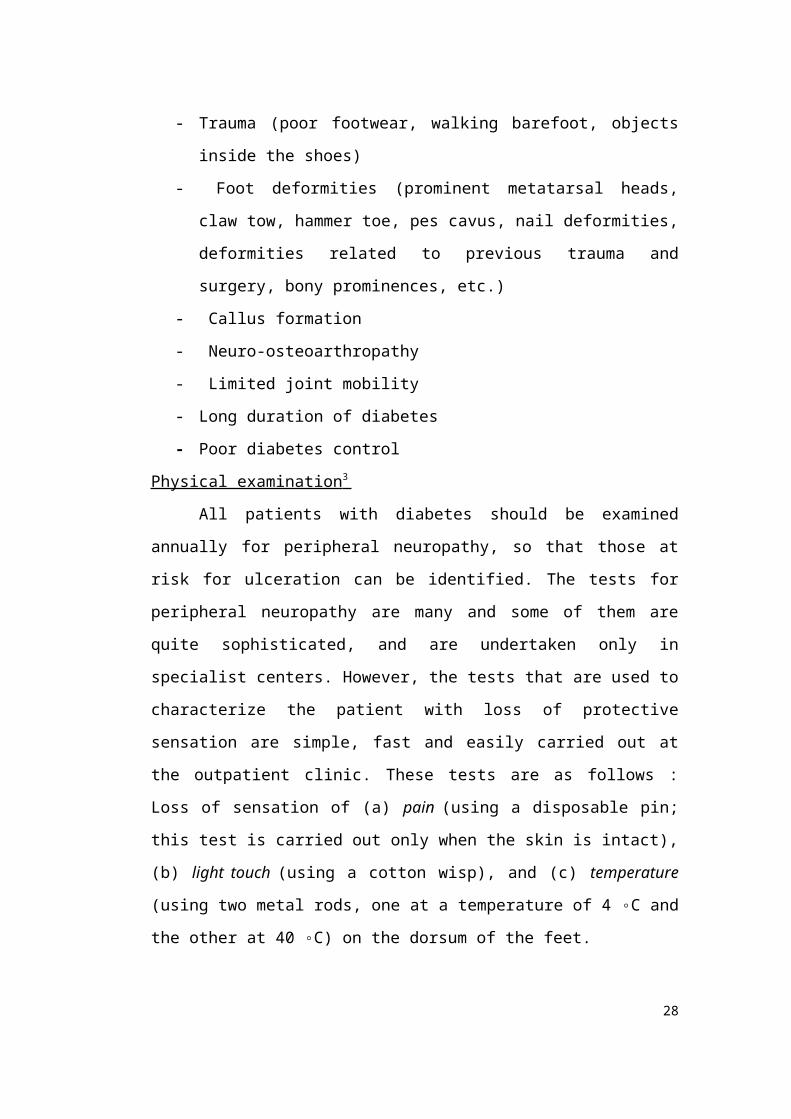
carried out at the outpatient clinic. These tests are as follows : Loss of sensation of
(a) pain (using a disposable pin; this test is carried out only when the skin is
intact), (b) light touch (using a cotton wisp), and (c) temperature (using two metal
rods, one at a temperature of 4 ◦C and the other at 40 ◦C) on the dorsum of the
feet.
Typically, in diabetic peripheral neuropathy the sensory deficit is
pronounced at the periphery of the extremities (in a ‘glove and stocking
distribution’). A zone of hypoesthesia is found between the area of loss of
sensation and a more central area of normal sensation. Achilles tendon reflexes
may be reduced or absent. Wasting of small muscles of the feet results in toe
deformities (claw, hammer, curly toes) and prominent metatarsal heads. Vibration
perception is tested using a 128-Hz tuning fork on the dorsal side of the distal
phalanx of the great toes. A tuning fork should be placed perpendicular to the foot
at a constant pressure. During examination the patient is revented from seeing
where the examiner has placed the tuning fork. Examination is sepeated twice
and there is at least one ‘sham’ application in which the tuning fork is not
vibrating. The patient has normal sensation when his reactions are correct in two
out of three tests, but is at risk for ulceration when they are incorrectin two out of
the three tests.
20

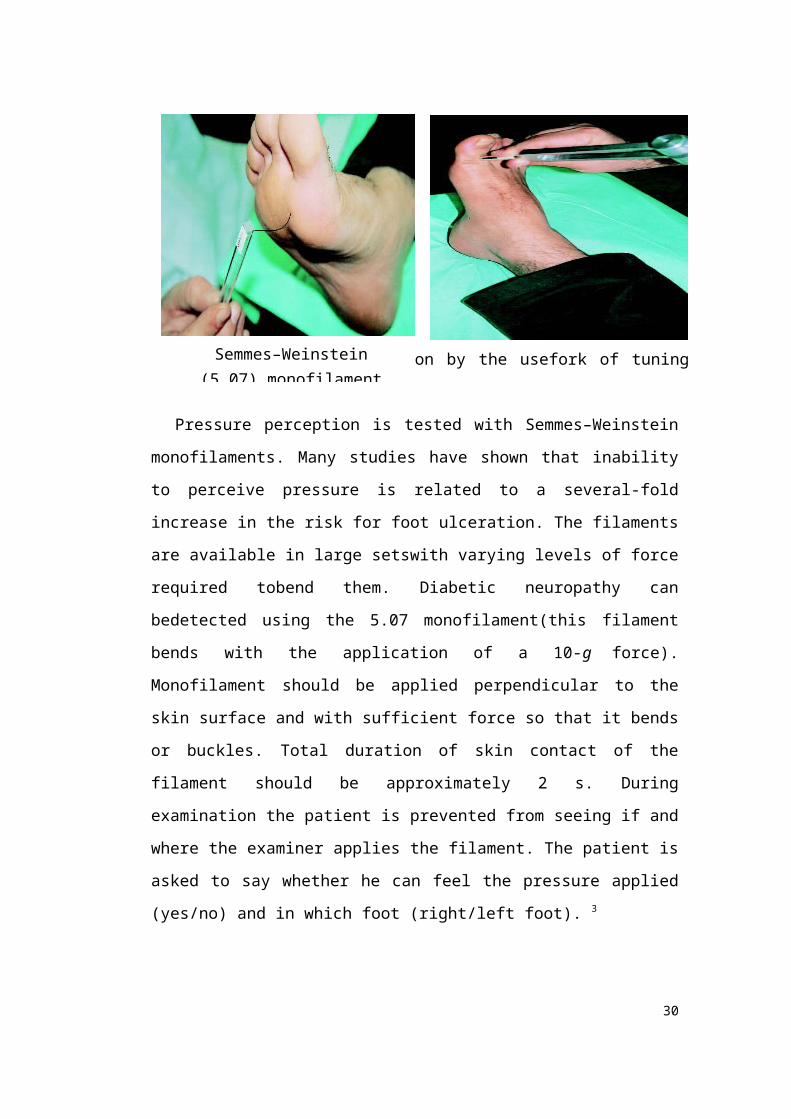
Pressure perception is tested with Semmes–Weinstein monofilaments. Many
studies have shown that inability to perceive pressure is related to a several-fold
increase in the risk for foot ulceration. The filaments are available in large
setswith varying levels of force required tobend them. Diabetic neuropathy can
bedetected using the 5.07 monofilament(this filament bends with the application
of a 10-g force). Monofilament should be applied perpendicular to the skin
surface and with sufficient force so that it bends or buckles. Total duration of skin
contact of the filament should be approximately 2 s. During examination the
patient is prevented from seeing if and where the examiner applies the filament.
The patient is asked to say whether he can feel the pressure applied (yes/no) and
in which foot (right/left foot). 3
Examination is repeated twice at the same site and there is at least one ‘sham’
application, in which no filament is applied (a total of three questions per site).
The patient has normal protective sensation when the correct answer is given for
two out of the three tests and is at risk for ulceration when they are not. The
International Consensuson the Diabetic Foot suggested three sites to be tested on
both feet: the plantaraspect of the great toe, the first and the fifth metatarsal heads.
The filament must be applied at the perimeter and not at an ulcer site, callus, scar
or site of necrotic tissue. 3
21
Semmes–Weinstein (5.07) monofilament
Examination of vibration perception by the usefork of tuning examination

Determination of vibration perception thresholds using a biothesiometer or a
neurothesiometer. Vibration perception threshold is measured at the tip of the
great toes with the vibrating head of the device balanced under its own weight.
(The vibrating stimulus is increased until the patient feels it, the stimulus is then
withdrawn and the test repeated. This test is usually carried out three times at each
site and the mean value is calculated. Several studies have shown that a vibration
perception threshold over 25 V is associated with a 4- to 7-fold increase in risk for
foot ulceration. 3
Additional Examination
X-Ray 3
The clinical presentation and findings on physical examination determine
the need for imaging studies. Imaging studies are often overused. Plain
radiographs suffice in the vast majority of DFI cases. In all patients presenting
with DFI, high-quality radiographs of the feet include anteroposterior (AP),
lateral, and oblique views. Look for loss of soft-tissue planes, lucencies indicating
gas, foreign bodies that may have precipitated the infection, and bony changes
such as erosion and periosteal new bone formation that may indicate
osteomyelitis. The osseous radiographic changes of neuroarthropathy can simulate
osteomyelitis and the differential diagnosis can sometimes be difficult. Lytic
changes in bone without overlying skin ulceration is usually not due to
osteomyelitis but rather due to neuroarthropathy.
X-ray images should be obtained in patients with diabetic foot ulcers to
evaluate for the presence of osteomyelitisand gas in the soft tissues. Osteomyelitis
was noted in this case; however, the soft tissue gas is much more prominent
(Figure 3). The presence of gas on xray of the affected area should prompt the
clinician to obtain images up to the next proximal joint in order to ascertain the
extent of the infection [10]. In cases where gas is not seen, but deep space soft
tissue infection is suspected, computed tomography (CT) or magnetic resonance
imaging (MRI) may be appropriate.
Medial calcification, which is very common in diabetes (Figure 3), renders
the underlying arteries incompressible, resulting in spuriously high ABI values
22
(more than 1.2). In these cases, the severity of arterial occlusive disease can be
assessed by toe pressure measurements. Other causes of inaccurately high ABI
values include too high positioning of the upper body, chronic venous
insufficiency and significant ankle edema. Spurious low ABI values can result
from the rapid deflation of the cuff, excessive probe pressure, and an insufficient
rest period.
Culture 3
Swab cultures from the surface of an ulcer or from sinus drainage have
been shown to be poor indicators of the bacterial species below. Therefore,
clinicians should curet and culture an ulcer from the base for aerobic and
anaerobic organisms. Start with empirical antibiotics if infection is suspected, and
modify them, if necessary, when the culture results and antibiotic sensitivities are
available. The bacterial species seen in DFIs are often multiple and range from
streptococcus or staphylococcus species (the two most common) to gram-negative
organisms and anaerobic organisms. Treatment with intravenous antibiotics based
on a swab culture, or preferably, a deep culture, is helpful if significant cellulitis is
present.
Arteriography 3
23
Extensive calcification of the posterior tibial artery
X-ray reveals soft-tissue gas consistent with gangrene
Arteriography remains the definitive diagnostic procedure before any form
of surgical intervention. It should not be used as a diagnostic procedure to
establish the presence of arterial disease. Contrast material may exaggerate any
preexisting renal disease and for this reason the contrast material used should be
limited as much as possible. In addition, the International Meeting on the
Assessment of Peripheral Vascular Disease in Diabetes strongly recommended
that in diabetic patients arteriography should be carried out before any decision
regarding an amputation is made, in order to assess the exact status of the vascular
tree, particularly when the ankle brachial index and toe systolic pressure indicate
that arterial disease is present.
IX. TREATMENT
Basic principles of wound healing apply equally to diabetic foot ulcers as
to wounds in any other site or condition. Basically, a diabetic foot ulcer will heal
if the following three conditions are satisfied:
Arterial inflow is adequate.
Infection is treated appropriately.
Pressure is removed from the wound and the immediate surrounding area.
Ulcer location (forefoot, midfoot, and heel) and the presence or absence of
arterial disease influence healing rates.7,8
Classification and treatment8,9
Depth-ischemia classification (modification of Wagner- Meggitt classification)
1. Ulcer
Grade Description Treatment
Grade 0 Skin intact with bony
deformity - at risk
Extradepth shoe and pressure-relief
insoles
Grade 1 Localized superficial ulcer
without tendon or bone
involvement
- In-office ulcer debridement
- Total-contact cast
Grade 2 Deep ulcer with exposed - Formal operative debridement of all
24
tendon or joint capsule exposed tendon and nonviable tissue
- Followed by dressing changes and
total-contact casting once wound bed
is healthy
Grade 3 Extensive ulcer with exposed
bone/osteomyelitis or abscess
- Surgical debridement of exposed
bone/ osteomyelitis and nonviable
tissue
- Followed by dressing changes and
total contact casting once wound bed
is healthy
2. Ischemia8
Grade Description Treatment
Grade A Normal vascularity
Grade B Ischemia without gangrene Noninvasive vascular studies and
surgical revascularization if indicated
Grade C Partial (forefoot) gangrene - Noninvasive vascular studies and
surgical revascularization if indicated
- Metabolic assessment
- Delay surgery if albumin is less than
2.5 g/dL or total protein is less than 6
g/dL, and improve nutritional status of
the patient.
- Operative intervention—partial foot
amputation
Grade D complete foot gangrene - Same as with grade C
- Operative intervention : below-the-
knee or above- the-knee amputation
Additional treatment8
25
i. Midfoot collapse may require ostectomy of bony prominence or midfoot
fusion if instability of the midfoot is present.
ii. Equinus contracture is very common, and tendo- Achilles lengthening will
offload the midfoot/forefoot.
Achilles lengthening required
a. Recurrent forefoot/midfoot ulceration
b. Ulceration with equinus deformity
iii. Toe deformities often require joint resection or amputation.
The ultimate goal is an ulcer-free, functional, plantigrade foot that can fit within a
brace or shoe.
Diabetic foot infections8
i. Treat with initial broad-spectrum antibiotic coverage once surgical
cultures are obtained, and adjust once sensitivity results return.
ii. Abscesses require surgical drainage and antibiotics.
iii. Osteomyelitis is treated with antibiotics and usually surgical débridement.
iv. Culture-specific antibiotics from a bone biopsy have proven to be an
effective tool in treating osteomyelitis without the need for bone resection.
Resection of all nonviable or infected soft tissue should also be performed.
v. If culture-specific antibiotic therapy fails, then surgical resection of
infected bone and débridement of surrounding tissue is required in
addition to antibiotic therapy.
vi. Often results in more extensive debridement, including ray resection,
partial calcanectomy (calcaneal involvement), and partial or complete foot
amputation
Amputation level8
26
i. Transmetatarsal
Lowest energy expenditure
No tendon transfer needed
ii. Lisfranc
Must transfer peroneal tendons to the cuboid to prevent varus
Achilles lengthening to prevent equinus
iii. Chopart
Transfer anterior tibialis to talus to prevent equinus.
Achilles lengthening to prevent equinus
iv. Syme
Amputation level with the next lowest energy expenditure after a
transmetatarsal amputation. Superior to both a Lisfranc and Chopart
amputation with regard to the amount of energy required to ambulate
v. Transtibial
Superior results with postoperative casting for 3 to 5 days with conversion to
rigid removal dressing
Pressure Off- loading
The mainstay in the management of an active plantar foot ulcer is the
effective offloading of the ulcer area. Once an ulcer is present, it will not heal
unless the mechanical load on it is removed. In patients with peripheral
neuropathy, it is important to offload at-risk areas of the foot in order to
redistribute pressures evenly. Inadequate offloading leads to tissue damage and
ulceration. The gold standard is the total contact cast (TCC). This is a
wellmoulded, minimally padded foot and lower leg cast that distributes pressures
evenly over the entire plantar surface of the foot. It ensures compliance because it
is not easy for the patient to remove. Using a TCC in patients with a unilateral
uncomplicated plantar ulcer can reduce healing time by
around six weeks.7,8,10
TCCs are contraindicated in patients with ischaemia because of the risk of
inducing further DFUs. They are also not appropriate for patients with infected
27
DFUs or osteomyelitis because, unlike removable devices, they do not allow
wound inspection. Removable devices (such as removable cast walkers,
Scotchcast boots ( healing sandals and crutches, walkers and wheelchairs) should
be selected in these patients. 9,10
Gambar. a) Total Contact Cast (TCC), b) removable Scotch Cast Boots3,9
X. PREVENTION Early detection of potential risk factors for ulceration can decrease the
frequency of wound development. It is recommended that all patients with diabetes undergo foot examinations at least annually to determine predisposing conditions to ulceration.
Patients should be educated regarding the importance of maintaining good glycemic control, wearing appropriate footwear, avoiding trauma, and performingfrequent self-examinations.10
XI. COMPLICATIONS
Charcot joint 2
Neuropathic joint disease ‘Charcot joints’ occur in less than 1 per cent of
diabetic patients, yet diabetes is the commonest cause of a neuropathic joint in
Europe and America (leprosy and tertiary syphilis being the other common causes
worldwide). The mid-tarsal joints are the most commonly affected, followed by
28
a
b

the MTP and ankle joints. There is usually a provoca- tive incident, such as a
twisting injury or a fracture, following which the joint collapses relatively pain-
lessly. X-rays show marked and fairly rapid destruction of the articular surfaces.
These changes are easily mis- taken for infection but the simultaneous
involvement of several small joints and the lack of systemic signs point to a
neuropathic disorder. Joint aspiration and microbiological investigation will also
help to exclude infection.
/
Picture A and B, Note collapse at Lisfranc joints, valgus posturing of forefoot,
and shortening of first ray. Prominence medially is medial cuneiform. C, Same
foot with subluxations at tarsometatarsal joints, fragmentation of bone, shortening
and angulation of first ray, and new bone formation.
Osteomyelitis.3,11
Diagnosis can be a difficult problem in diabetic patients with foot infections;
some physicians will make the dianosis of osteomyelitis if they can palpate bone
thru the skin lesion; this method is quick, inexpensive, and generally accurate;if
there is not a lesion over the area of question, then it is more likely that the lesion
has resulted from Charcot changes;neuropathic osteoarthropathy often appears
29
indistinguishable from osteomyelitis, with multiple and widespread abnormalities
that can appear hot on all three phases of a bone scan; peripheral vascular disease
will also affect the uptake; In-WBC may be most accurate for detection of OM in
the diabetic foot; cellulitis is frequently present and can be confused with OM,
especially if osteoarthritis or neuropathic disease is also present.
Patient usually complain of numbness and a sensation of pins and needles in
her feet at night.
On examination, the patient will have findings of severe neuropathy (no
feeling of light touch, pain, temperature, vibration or a 5.08 monofilament;
Achilles tendon reflexes were absent; the vibration perception threshold was >50
V in both feet). Peripheral pulses were weak and the ankle brachial index was 0.7.
Dry skin and nail dystrophies were present. A superficial ulcer with a slough base
was seen on the dorsum which was red, swollen and painful, having a sausage-
like appearance.
The sausage-like appearance of a toe usually denotes osteomyelitis. Bone
infection was confirmed on X-ray, showing osteolysis of the first and second
phalanges.
/
30
Picture shows a large irregular , soaked and infected neuropathic ulcer with
slough bed and surrounding cellulitis of 3 cm in diameter is shown here. A minor
trauma reported to have occurred 2 years earlier was the cause of this ulcer.
/
Picture shows osteolysis of the first metatarsal head and the base of proximal
phalanx of the hallux with periosteal reaction due to osteomyelitis are shown on
this plain radiograph of the foot illustrated in picture before.
31
a