Embed Size (px)
Citation preview
DIABETIC FOOT CARE: INVESTING IN PREVENTION
IS COST-EFFECTIVE
Dr Karel Bakker
Chair IDF Consultative Section
IWGDF
Foot facts worldwide
• Over 1,000,000 amputations per year
• Every 30 seconds a leg is lost to diabetes
Foot facts
• People with diabetes are 25 times more likely to lose a leg than people without the condition
• Throughout the world, up to 70% of all leg amputations happen to people with diabetes
Foot facts
• In developed countries one in every six people with diabetes will have an ulcer during their lifetime
• In developing countries, foot problems related to diabetes are thought to be even more common
• 85% of diabetes-related lower extremity amputations are preceded by a foot ulcer
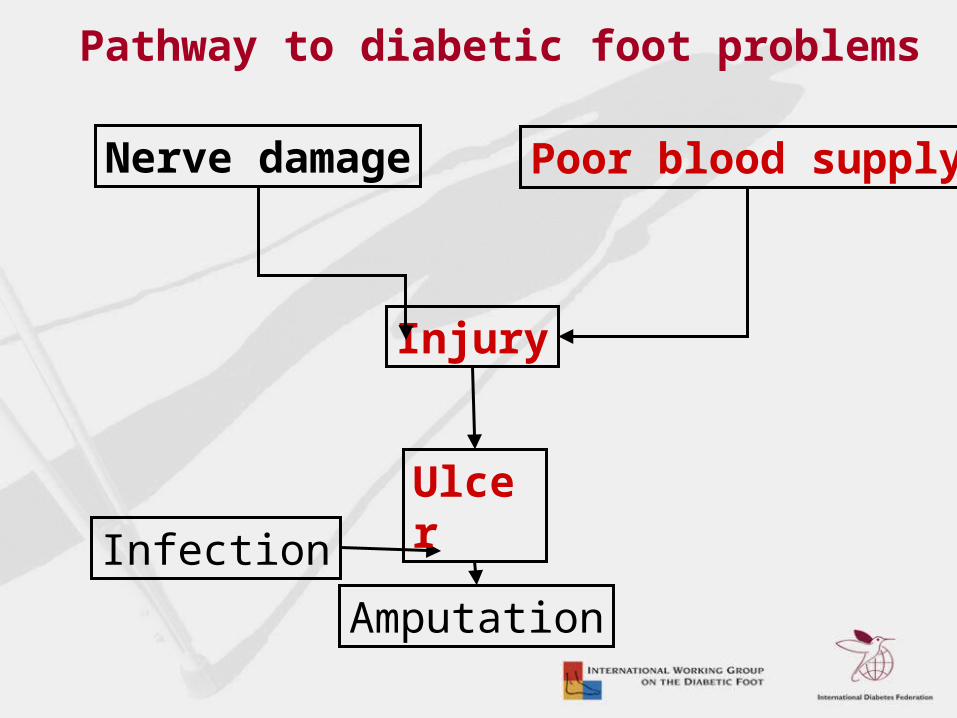
Nerve damage Poor blood supply
Injury
Infection
Amputation
Ulcer
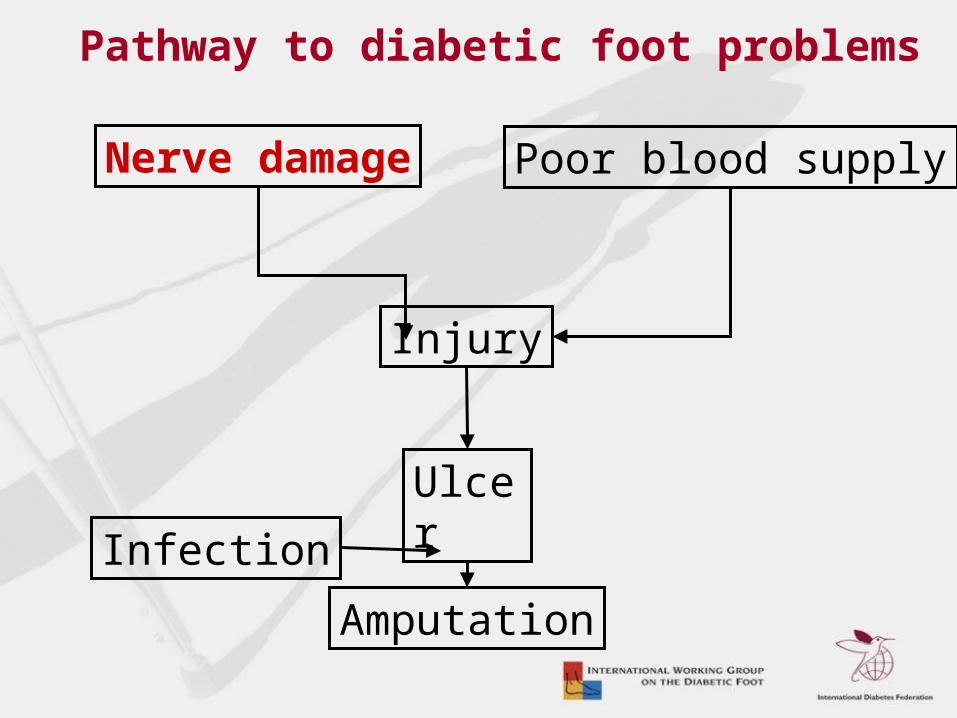
Pathway to diabetic foot problems

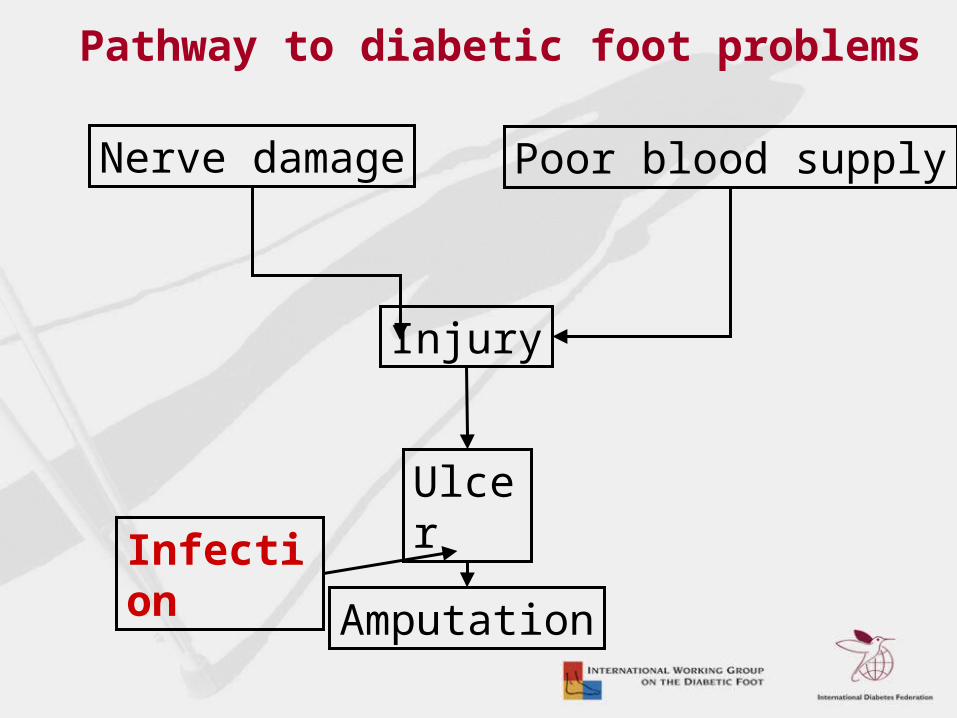
Nerve damage Poor blood supply
Injury
Infection
Amputation
Ulcer
Pathway to diabetic foot problems

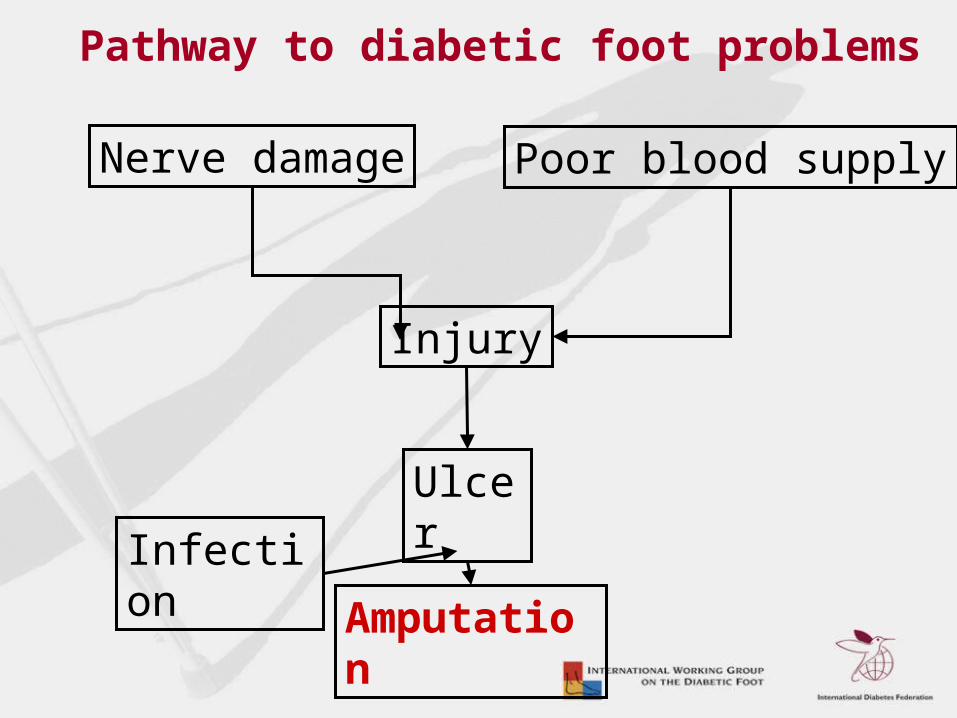
Nerve damage Poor blood supply
Injury
Infection
Amputation
Ulcer
Pathway to diabetic foot problems

Nerve damage Poor blood supply
Injury
Infection
Amputation
Ulcer
Pathway to diabetic foot problems
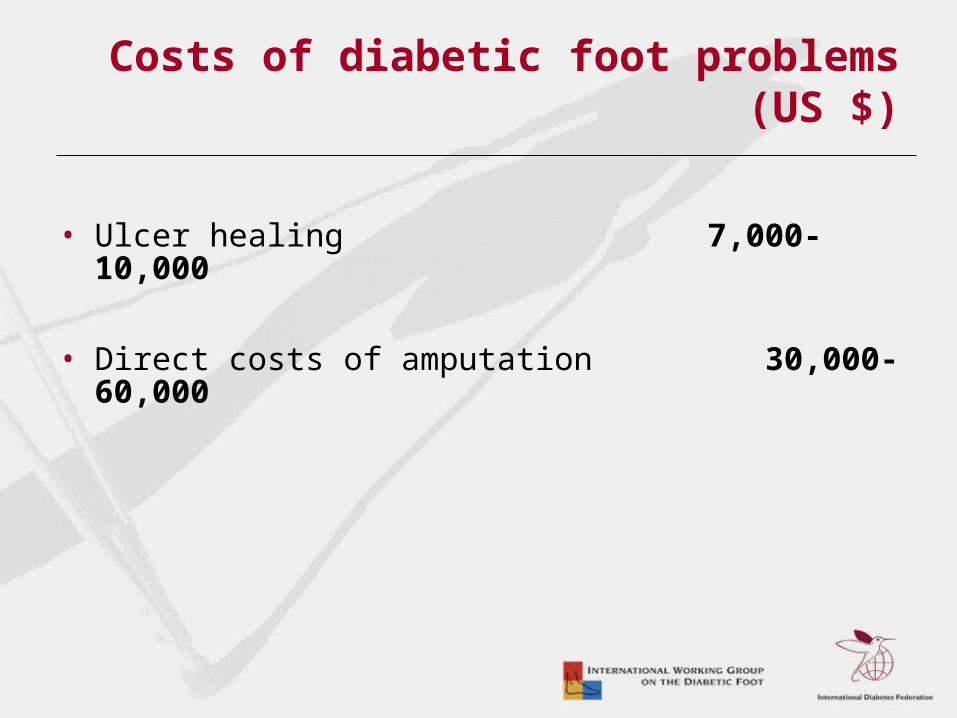
Costs of diabetic foot problems (US $)
• Ulcer healing 7,000-10,000
• Direct costs of amputation 30,000-60,000
Costs of diabetic foot problems
• In developed countries diabetic foot care accounts for 15-25% of total healthcare resources available for diabetes.
• In some developing countries, it has been estimated that foot problems may account for as much as 40% of the resources available
Prevention
• Up to 85% of all diabetes-related amputations can be prevented
• It is possible to save up to 30% of healthcare budget
• Education and podiatry are the most cost effective strategies
Prevention
• In countries where National Diabetes Programmes exist, foot clinics are emerging
• EVA project: opening of 10 foot clinics in 5 countries of the Andes (Bolivia, Peru, Ecuador, Colombia, Venezuela)
• However: Podiatric education is still scarce in many countries of the SACA Region Prevention programmes are still the exception
What can be done?
Cornerstones of Prevention
1. Regular inspection and examination of feet and footwear
2. Identification of the high-risk foot
• People with diabetes
– Make sure you have your feet checked periodically by a healthcare professional
What can be done?
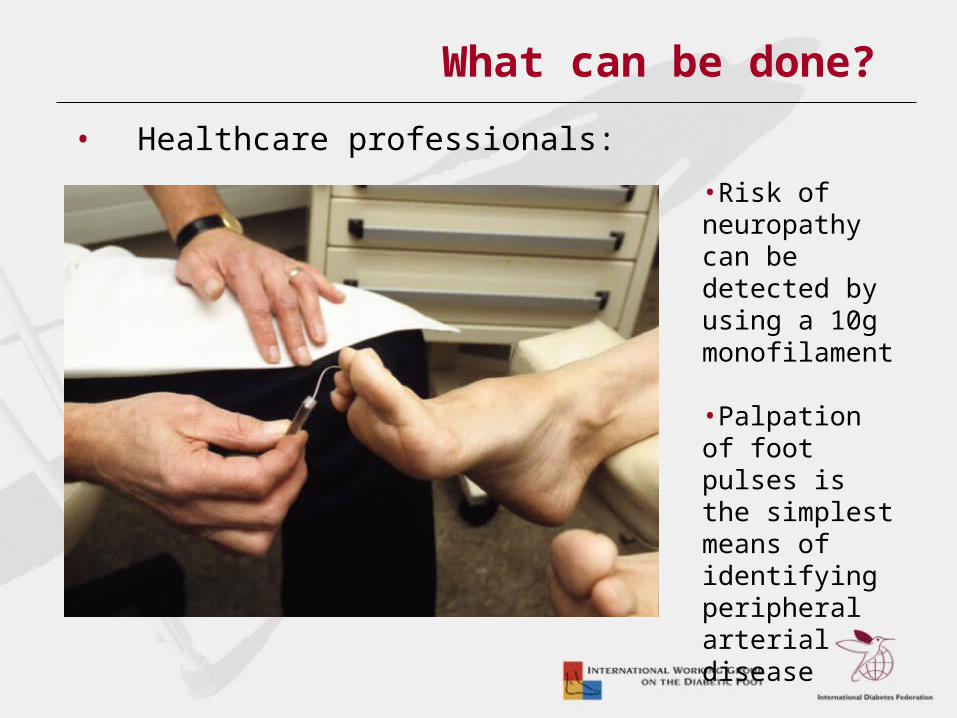
• Healthcare professionals:
•Risk of neuropathy can be detected by using a 10g monofilament
•Palpation of foot pulses is the simplest means of identifying peripheral arterial disease
What can be done?
Cornerstones of Prevention
3. Education of people with diabetes, family members and healthcare workers
4. Appropriate footwear
5. Rapid treatment of all foot problems

Sponsors WDD Campaign 2005
Conclusions
• The human and financial consequences of the diabetic foot are devastating
• Action is possible and affordable• Amputations are preventable • Even in low-resource settings, foot care can
substantially reduce ulceration and amputation• Feet should last a lifetime
Conclusions
Every 30 seconds a limb is lost to diabetes somewhere in the world. . .
. . . This needs to be changed!