Embed Size (px)
Citation preview

DIABETIC NEPHROPATHY & CHRONIC RENAL FAILURE /CHONIC KIDNEY DISEASE

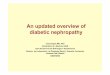
0 2 5 11-23 13-25 15-27
Incipient Nephropathy Predictors?HyperfiltrationMicroalbuminuriaRising BPPoor glycemic contol
Onset Of DM
Onset of Rising ESRDProteinuria S.Cr
HTN
Functional changes GFR increase (renal hypertrophy) reversible albuminuria increase kidney size
Structural changes increase GBM thickening Mesangial expansion nodular (Kimmelstiel-Wilson) & diffuse forms of intercapillary glomerulosclerosis capsular drop lesion fibrin cap lesion
IDDM, 30-40% DNNIDDM, 10-20% DN


Morphologic changes• Glomeruli:
– increase GBM thickening– Mesangial expansion – nodular (Kimmelstiel-Wilson) & diffuse forms of intercapillary
glomerulosclerosis– capsular drop lesion– fibrin cap lesion
• Tubulointerstitium,& tubular functional defects– Interstitial scarring– Impaired tubular reabsorption of low MW proteins and albumin– Increased Na reabsorption leading to volume expansion– Hypercalciuria– Impaired excretion of H & K ions
• Vascular, hyaline thickening of the arteriolar wall• Glomerular haemodynamic changes
– Decreasing Pglom: ACE-I, ARB, low protein diet

Transient microalbuminuria
• Hyperglycemia• Hypertension• Congestive heart failure• Urinary tract infection• Excessive physical exercise • Albumin Excretion Rate / AER
– Normal < 30 mg/day– Microalbuminuria 30-300 mg/d– Overt proteinuria AER> 300 mg/d


Overt Diabetic Nephropathy
• In early DN the albuminuria is secondary to a loss of the anionic charge barrier of the GCW
• In established DN, the proteinuria is due to the presence of an increased number of nonselective and large pores
• The presence of persistent proteinuria heralds the overt phase of DN
• >95% of patients with DN have D Retinopathy• Rate of decline in GFR has been reported as linear in a
given patient, but wide differing between patients• ~ 1 ml/min per month, with 50% of patients reaching
ESRD ~ 7 years after the onset of proteinuria. • Recent reports suggest that is has slowed down ~10
years

Complication of DM
• Microvascular– Retinopathy– Nephropathy
• Macrovascular– Peripheral vascular disease– Coronary artery disease– Cerebrovascular disease
• Diabetic neuropathy, incl. gastroparesis• Hyperkalemic RTA

Syndrome ‘X’
• Obesity
• Decreased glucose tolerance, Insulin resistance & hyperinsulinemia
• Hypertension
• Hyperlipidemia, esp triglycerides
• Increased risk for atheroscerosis

NIDDM
• Patients on HD in a dialysis unit ~ 30-50% because of NIDDM & diabetic nephropathy
• Many patients with NIDDM will die of other causes (cardiovascular) before reaching ESRD
• Natural history less well characterized• Heterogeneous group, with many comorbid
conditions, hypertension, obesity• 10-20% incidence of DN, mostly after 10-20 y• Familial predisposition

Management • Control of Diabetes, HbA1c <7• Control of hypertension, BP<130/80,
if proteinuria BP<125/75• Low salt diet• Control of hyperlipidemia• Weight control• Smoking cessation• Management of other comorbid conditions;
cardiovascular, anemia, cerebrovascular, physical inactivity...
• ACE-I, ARB, combination

CHRONIC KIDNEY DISEASECKD

usg


CKD
• Diabetic Nephropathy• Hypertension• Glomerulonephritis
– Acute– Rapidly Progressive GN – Chronic GN– Secondary GN ( Infections, Malignancies,
Autoimmune Ds,…) • Drugs & Toxins• Hereditary : Alport’s, PCKD, ….• Congenital : VU Reflux• Obstructive Nephropathy


Signs & Symptoms
• Edema
• High Blood Pressure
• Nocturia
• Frequency & Dysuria
• Loin pain unrelated to movements
• Hematuria
• Proteinuria

CRF & ESRD
• Poor appetite. Nausea & vomiting • Insomnia & Restlessness • Labile mood swings• Asthenia • Shortness of breath.
– Pulmonary edema. Metabolic acidosis• Cardiac arrhythmias. Hyperkalemia• Hypertensive urgencies / emergencies• LVH• Anemia• Malnutrition • Hyperphosphatemia• Hyperparathyroidism

KIDNEY DIDEASE
• Prevalent in identifiable groups– Aging , > 50
– DM
– Hypertension
– Cardiovascular disease, CVD
– Family members
– Herbal medicine (jamu), Analgetics




RISK FACTORS(+)--- CHECK URINE & CR -----MCU
NORMAL HEMATURIA/PROTEINURIA
HIGH CR
RENAL US--------CRF/Hydronephrosis
ESTIMATE GFR / 24H U CCT
SPOT U Prot/Cr RATIO / 24H U Prot
IMMUNOLOGY SEROLOGY :C3,C4,ANA,ANCA
ETIOLOGY??? RENAL BIOPSY
DIAGNOSIS & PROGNOSIS
SPECIFIC THERAPY : STEROID, IMMURAN
CYCLOPHOSPHAMIDE, CYCLOSPORIN, MMF/CELLCEPT
START NONSPEC IFIC THERAPY
REGULAR CHECKS
PREVENTIVE ACTION
, a-dsDNA, GBM-Ab







Therapy CKD
• Specific Therapy. depends on etiology & histopathology
• Decrease proteinuria / albuminuria
• Tightly control Blood Pressure < 125 / 75
– ACE-I, ARB, non-dihydropyridine-CCB,….
• Tightly control Blood Sugar
• Manage hyperlipidemia
• Stop smoking
• Low protein diet 0.6 – 0.8 g /kg BW/day

• Manage Anemia and other co morbidities,
• Manage Cardiovascular ds,
• Complications of decreased kidney function
• Preparation for kidney failure and RRT
• Initiation of RRT


Progression of CKD• Mechanisms of ongoing renal injury
– Deposition IC, Ag, Ab, matrix, collagen, fibroblasts– Intracapillary coagulation– Vascular necrosis– Hypertension & increased Pglom– Metabolic disturbances, e.g. DM, hyperlipidemia– Continuous inflammation– Nephrocalcinosis ; dystrophic & metastatic– Loss of renal mass / nephrons– Ischemia; imbalance between renal energy demands and supply
• Results in– Glomerulosclerosis– Tubular atrophy– Interstitial fibrosis


Compensatory renal changes in CKD
• Hypertrophy of residual nephrons
• Increased RBF per nephron, but decreased total RBF
• Increased Single Nephron GFR / SNGFR– Increased osmotic / solute load– Hyperfiltration– Increased intraglomerular pressure / Pglom

## NEPHRONS
Pcap +flow
Glomerular Protein Glomerular injury flux hyperfiltration
Glomerulosclerosis
## NEPHRONS

• Pattern of excretory adaptation– Increased filtered load; Cr, BUN– Decreased tubular reabsorption; Na, H2O– Increased tubular secretion; K+, H+, Cr
• Limitation of nephron adaptation– Magnitude– Time, ~response to intake / load, production
• Abrupt changes in intake / production may not be tolerated
– Trade off, expense to other systems• E.g. to preserve P balance PTH increases

VolumeUrine,Uosm,U(Na,K,H)

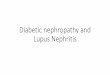
• Multiple mechanisms of chronic hypoxia in the kidney.
• Mechanisms of hypoxia in the kidney of chronic kidney disease include loss of peritubular capillaries (A),
• Decreased oxygen diffusion from peritubular capillaries to tubular and interstitial cells as a result of fibrosis of the kidney (B),
• Stagnation of peritubular capillary blood flow induced by sclerosis of "parent" glomeruli (C),
• Decreased peritubular capillary blood flow as a result of imbalance of vasoactive substances (D),
• Inappropriate energy usage as a result of uncoupling of mitochondrial respiration induced by oxidative stress (E),
• Increased metabolic demands of tubular cells (F), and • Decreased oxygen delivery as a result of anemia (G).

• Treatment modalities that target chronic hypoxia in the kidney
• Improvement of anemia by EPO • Preservation of peritubular capillary blood flow by
blockade of the renin-angiotensin system• Protection of the vascular endothelium
– VEGF – Dextran sulfate
• Antioxidants to improve the efficiency of cellular respiration
• HIF-based therapy (hypoxia inducible factor)– Prolyl hydroxylase inhibitors – Gene transfer of constitutively active HIF

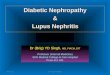
Intact nephron hypothesis• Using experimental animals; urine from each kidney was collected seperately
Before After End K1 K2 K1 K2 K2
GFR 50 50 55 14 24NH3 excr 49 51 66 25 40NH3 excr/100mlGFR 100 100 120 121 167
K2 was partially K1 removedremoved
Conclusion-Normal renal tissue undergoes hypertrophy to compensate for loss of functioning nephrons-Normal tubules adapt, increase in function as other tubules are lost-Diseased nephrons / tubules adapt in the same way ~ increase NH3 excr / 100mlGFR-Even diseased nephrons can increase their GFR



The Uremic Syndrome• Nervous system
– Impaired concentration, perceptual thinking, – Peripheral neuropathy; primarily sensory, paresthesias, restless leg syndrome– Autonomic neuropathy; impaired baroreceptor function, orthostatic hypotension, impaired
sweating– Uremic ancephalopathy
• Hematology system– Anemia is invariably present when renal function fall <30%
• Decreased RBC survival, response to EPO, • Deficiencies of Fe, B12, folate, aluminium overload• Blood loss• Hyper PTH• Inflammation – malnutrition• Bone marrow fibrosis• Inadequate dialysis
– Bleeding diathesis: easy bruising, slow clotting• Prolonged BT & abnormal platelet function• PF3 concentration are generally low, impaired aggregability• Reduced von Willebrand’s factor HMW multimers• Uremic toxins & PTH
– Immune function• Impaired Ab response to viral Ag (not to bacterial)• Decreased T-cells• Cutaneous anergy

• Cardiovascular system– Cardiovascular disease is the leading cause of death in patients
with CKD stage 4-5– Accelerated Atherosclerosis / CAD – Hypertension, ~ 80% of all uremic patients– Pericarditis
• Metabolic abnormalities– Lipids; increase in tot. triglycerides, Lp(a), LDL, decrease HDL– Carbohydrate metabolism; insulin resistance, decreased need
for OAD / insulin in DM– High prolactin; galactorrhea– Men : testosteron is low, FSH / LH normal or high– Women: pg E2 & progesterone are low, FSH /LH normal or
slightly elevated– Abnormalities of thyroid gland function test, normal TSH









CKD stage 5 (ESRD / GGT)
• DIALYSIS / Renal Replacement Therapy– Hemodialysis– Peritoneal Dialysis– Continues Renal Replacement Therapies
• Kidney Transplant– Cadaver – Living related / unrelated