Embed Size (px)
Citation preview

> The easiest way to measure strabismus:
Objective, accurate and documented diagnosis.
Helps diagnose and improve your treatments.
Allows you to follow the evolution of your patients.
Relieves you and assures your correct practices.
> The most powerful research tool in ocular motility
which can measure:
How much the ocular deviation is (between both
eyes).
What the behaviour of the pupils is.
How the eyes are oscillating.
And if the eye is in torsion and how much this
torsion is.
> Detecting the pupil and scanning the iris we can measure:
Ocular deviation at any point in space
(horizontal + vertical + torsional).
Ductions, versions and vergences.
Saccadic and following movements.
Cover test.
Digital Hess test (9 Gaze Points).
Concomitant and paralytic strabismus.
Ocular motility Field.
Bielchowsky Test.
Nystagmus.
Pupillary dynamics (pupillography).
Accommodation, convergence and miosis
reflex.
Motility and centering of ocular prosthesis.
And soon, eyelid dynamics and visual
therapy.
DIAGNOSIS AND MANAGEMENT ARE IMPROVED THANKS TO BETTER AND OBJECTIVE MEASUREMENTS
This means GAZELAB

Both eyes uncovered
Glasses concept 9 gaze positions test
0,6±0,9 0,5±0,9 0,3±0,9 0,2±0,9 0,3±0,9 0,3±0,9
0,4±0,9 0,3±0,9 0,0±0,9 0,1±0,9 0,6±0,9 -0,2±0,9
-0,3±0,9 0,1±0,9 0,3±0,9 0,3±0,9 0,5±0,9 0,3±0,9
Horizontal Vertical
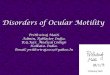
Strabismus can be diagnosed in children and adults using digital videocameras mounted on standard trial frames. The 9 gaze positions test helps to measure with objectivity and accuracy the ocular motility disorders. These better measurements improve the diagnostic support, the surgical planning and the monitoring. Display results in a normal patient (bottom)
The patient is required to look at a laser test projected on the wall in each of the 9 gaze positions. The exam is performed in 3 different ways: both eyes uncovered,
right eye covered (left eye fixing) left eye covered (right eye fixing).
The computer processes simultaneously the horizontal and vertical data of each point, as well as the torsional data measured in degrees. The resultant reports show the images of both eyes for each point analysed.
In addition to the 9 gaze positions, the device allows you to do other tests like Bielchowsky test, papillary dynamics, nystagmography, etc.
> Less than 400g
> Quicker than 2 minutes

ADVANTAGES:
Effectivity - It increases accuracy
and diagnostic measurement
capability. As a consequence it
improves the surgical success rate
and facilitates post-surgery
monitoring.
Flexibility - It allows you to
explore many of the eye positions.
Documentability– It generates
documentary evidence attached to
the clinical history.
Pre-programmability - with scan
patterns defined by the specialist.
Easy to use - provides the
possibility of delegating scanning
tasks to physician assistants.
Versatility - It allows the
implementation of other features
related to ocular motility.
Videoculograph (VOG) with laser projection system, integral with the patient's head, that allows to measure and accurately diagnose complex deviations of gaze in all directions. Why Gazelab? It has the ability to analyze every muscle independently. It improves the surgical success rate. It controls the gaze of the patient with the projection system and explores concrete
positions. It allows measurement independent of the Explorer. It allows Pattern Projection, Gaze Position & the Recording all together in the same
reference system. The head movements don’t affect the Measurements.
This medical device is equipped with two cameras with infrared vision which enables to record eye movements with great precision. It also supplied with a laser projector able to projects at any point in space. Components:
1. Laser projector 2. Cameras with infrared vision The device includes an ad hoc computer with the necessary applications preinstalled.
Glasses concept
1
2

If the eye moves, how is it that none of the
medical devices that can be currently found in
an ophthalmologist clinic can measure the
dynamic of the eyes? This was the question
posed by Dr. Joan Prat Bartomeu when the
idea of developing a measurement technique
that could accurately capture and measure
ocular biomechanics came up.
Most of the already existing ophthalmological
devices explore parts of the eye (anatomical
structures) from a static point of view. For
example, through the slit lamp you can
observe the anterior segment of the eye;
Some historic considerations in digitalization of ocular movements.
The first eye-trackers made around 20 years ago were used specially for research and
marketing applications. They were able to know where the eyes were looking. Neither their
constructive concept nor software applications were designed for clinical use.
Ophthalmologists remember the eye-tracker implemented in Excimer Laser; the laser was
blocked when the eye lost the green spot because of its movement.
The videonistagmographer (VNG) measured the eye movements in patients with
nystagmus. Some otolaryngologists used this device to study vertigo during the last
decade. Only a few ophthalmologist used it for diagnosis of any sort of nystagmus. The
problem were that VNG took measurements in millimeters and not in degrees or prism
diopters.
The videoculography (VOG) is, on the other hand, a system that measures the ocular
deviations in cases of strabismus or extraocular muscle palsies. It analyzes eye movements
using a monitored image by computer. Two previous European devices weren’t useful for
clinical purposes although they were used for research.
Videopupillography (VPG) is nowadays in the research centers, used by a few
neurophthalmologist or neurologist. It records the pupillary light reactions with accuracy in
cases in which the optic nerve is affected or in cases of cerebral diseases.
the ophthalmoscope does the same with the ocular fundus; or the OCT (Optical Coherence
Tomography) that shows cuts of the retina and choroid. For all of them the patient must be
still.
In any case, it is impossible to measure the movements with present ophthalmic devices:
- Is it possible to have an ocular motility field? We have a campimeter that gives us a visual
field! Is it possible to study the behaviour of a concrete extraocular muscle?
- With what accuracy can a nystagmus be measured?
- Which are the changes that occur during the light pupillary reflex? Is the velocity of
contraction and dilatation important?
- Perhaps it could be useful to know the blinking parameters in a facial palsy or other
disorders.
A little bit of history about Videoculography

Dots Coordinates Horizontal Dif. Vertical Dif.
1 0,30 -15.9 -1.9
2 0,20 -16.2 -0.2
3 0,10 -16.4 -0.4
4 0,0 -15.8 2.2
REPORT: Right Exotropy
In the pictures above, it can be observed that the left eye followed correctly the vertical pattern, while the right eye maintains a steady drift towards the right.
It can be observed at each coordinate what the deviation of the right eye is compared to the red cross (0,0).
Right Left
Basic Concepts of reliable VOG The gaze is the result of 2 main movements made by eye and head. So, the VOG must be attached to the head to avoid the register of head movements. The device should be only mounted as a helmet, on the head. Any other system could avoid the head movements during the digital recording.
If you want to know where the eyes are looking you have to fix a project system in the same head mounted device. Then you could move a test projected on a wall in your desired way. Cameras record the eyes when they move while doing the test. A computer vision software takes measurements during all the procedure. What can you digitalize with a VOG?
You can digitalize the primary position and the 9 main positions of the gaze at an exactly known point in coordinate axis. And perhaps more importantly, you can also register the behavior of the eyes in the specific ocular action muscles, all 6 plus 6 muscles. This is the best way to understand the role of every muscle in ocular motility disorder. Exam method
1: Primary position with or without and cover test 2: Horizontal movements (0, -40º and +40º) 3: Superior movements (up to -23º, 0 and +23º)* 4: Inferior movements (down to-23º, 0 and +23º) 5: Bielchowsky test (torsions 15º,30º,and 45º)
Strabismus: exotropy

REPORT: Left Esotropy + Left Hypertropy
On the pictures of the eye we can observe how the right eye is looking straight at the dot, while the left eye deviates to the left. An increasing hypertrophy appears in the left eye.
At dot number 5 (eyes looking at coordinate 10,0) the left eye deviation towards the right is horizontal=19.5° and vertical=-9.4°. For dot number 8 (eyes looking at coordinate 40,0) the left eye deviation towards the right is horizontal=9° and vertical=-20.5°.
Right Left
Dots Coordi-nates
Horizontal Dif.
Vertical Dif.
1 -40,0 5.2 -4.1
2 -30,0 6.1 -3.9
3 -20,0 10.3 -4.6
4 -10,0 16.6 -7.5
5 10,0 19.5 -9.4
6 20,0 19.4 -12.1
7 30,0 14.9 -17.0
8 40,0 9.0 -20.5
Results presentation The computer processes the horizontal, vertical and torsional data of every point registered during and after the exam. At the end, the reports show all the registered data in several formats that can be saved in any digital support: 1: Serial key photogram. 2: Graphic representation. 3: Data collection on a chart. “Now ophthalmologists can work on strabismus on a scientific data basis, developing and improving their knowledge.”
- Schneider E, Villgrattner T, Vockeroth J, Bartl K, Kohlbecher S, Bardins S,Ulbrich H, Brandt T. EyeSeeCam: an eye movement-driven head camera for the examination of natural visual exploration. Ann N Y Acad Sci. 2009;1164:461-7. - Laria C, Gamio S, Alió JL, Miranda M. Difficult vertical diplopia studied by video-oculography in aphakia after contactlens use. A case report. Binocul Vis Strabismus Q. 2006;21(4):223-30. - Becker R, Krzizok TH, Wassill H. Use of preoperative assessment of positionally induced cyclotorsion: a videoculographic study. Br J Ophthalmol. 2004;88(3):417-21. - Schworm HD, Ygge J, Pansell T, Lennerstrand G. Assessment of ocular counterroll during head tilt using binocular video oculography. Invest Ophthalmol Vis Sci. 2002;43(3):662-7.
Strabismus: esotropy with hypertropy

REPORT
Left Esotropy + Left Hypertrophy
Alternate Fixation
The eye fixation to vertical pattern
changes depending on the point
examined.
For pattern dot number 2 (coordinate
0,20) the fixating eye is the left, while
the right eye looks inward. The visual
difference between right and left eye is
horizontal=23.1° and vertical=-2.9°.
For pattern dot number 5, the fixating
eye is the right one, while the left eye
looks inward. The visual deviation of the
right eye towards the left is
horizontal=17.7° and vertical=-10.6°.
Dots Coordinates Horizontal Dif. Vertical Dif.
1 0,40 21.7 -7.9
2 0,20 23.1 -2.9
3 0,10 23.8 -12.2
4 0,0 23.7 -15.3
5 0,-10 17.7 -10.6
6 0,-30 14.0 6.5
7 0,-40 17.4 -11.9
Right Left
Gazelab can detect the ocular fixation too. So, the cover-uncover test as well as the
alternate cover test can be performed without any problem here. Heterophories were
detected as easily as heterotropies.
However, head tilt and compensatory ocular torsions are not related to ocular fixation. The
device uses a sophisticated algorithm (complete iris images detection) that allows
measurement of the torsions of the eyeball during head movements with total accuracy.
Strabismus: alternant esotropy

The blue graph presents the rapid response of the right pupil diameter over time as a result of two flashes of light. The red graph shows identical response in the left eye.
- Wilhelm H, Peters T, Lüdtke H, Wilhelm B. The prevalence of relative afferent pupillary defects in normal subjects. J Neuroophthalmol. 2007 Dec;27(4):263-7. - Kardon R, Anderson SC, Damarjian TG, Grace EM, Stone E, Kawasaki A. Chromatic pupil responses: preferential activation of the melanopsin-mediated versus outer photoreceptor-mediated pupil light reflex. Ophthalmology. 2009 Aug;116(8):1564-73. - Kankipati L, Girkin CA, Gamlin PD. Post-illumination pupil response in subjects without ocular disease. Invest Ophthalmol Vis Sci. 2010 May;51(5):2764-9. - Kardon R, Anderson SC, Damarjian TG, Grace EM, Stone E, Kawasaki A. Chromatic pupillometry in patients with retinitis pigmentosa. Ophthalmology. 2011 Feb;118(2):376-81. - Kankipati L, Girkin CA, Gamlin PD. The post-illumination pupil response is reduced in glaucoma patients. Invest Ophthalmol Vis Sci. 2011 Apr 8;52(5):2287-92. - Feigl B, Zele AJ, Fader SM, Howes AN, Hughes CE, Jones KA, Jones R. The post-illumination pupil response of melanopsin-expressing intrinsically photosensitive retinal ganglion cells in diabetes. Acta Ophthalmol. 2012 May;90(3):e230-4. - Ishikawa H, Onodera A, Asakawa K, Nakadomari S, Shimizu K. Effects of selective-wavelength block filters on
Light pupillary reflex (LPR) is usually observed directly by the eye of the ophthalmologist. He doesn’t have accurate data about the diameter and even less about speed movements. Gazelab studies the LPR, recording 2 diameters and the surface of the pupillary space
over time of both eyes. Ocular movements don’t affect the results. The device analyzes static and dynamic parameters such as: Initial and final pupil diameter under a concrete light stimulus Speed of contraction and dilatation. In the graphics above we can see the normal LPR after a 2 seconds stimulus with a direct ophthalmoscope at maximum power. First, a fast contraction of about 0,5 seconds up to the maximum miosis. After the light is removed the pupil dilates slowly back to its original diameter in approximately 30 seconds. You can modify the light stimulus in several parameters according to your convenience: intensity, exposition time, repeated time and even colour. Ganglion cells specialized in LPR respond strongly to blue (similar to cobalt blue).
Some authors have investigated the pupil behavior in patients with glaucoma, diabetes, Parkinson disease, retinal dystrophies and other ocular or brain diseases. They use the video-pupillography performed with specific research devices.
Pupil Dynamics

- Kingma H. Clinical testing of the statolith-ocular reflex. ORL J Otorhinolaryngol Relat Spec. 1997;59(4):198-208. - Négrevergne M, Ribeiro S, Moraes CL, Maunsell R, Morata GC, Darrouzet V. [Video-nystagmography and vibration test in the diagnosis of vestibular schwannoma. Review of 100 cases]. Rev Laryngol Otol Rhinol (Bord). 2003;124(2):91-7. - Pérez P, Llorente JL, Gómez JR, Del Campo A, López A, Suárez C. Functional significance of peripheral head-shaking nystagmus. Laryngoscope. 2004;114(6):1078-84. - Hong SK, Koo JW, Kim JS, Park MH. Implication of vibration induced nystagmus in Meniere's disease. Acta Otolaryngol Suppl. 2007;(558):128-31. - Juhola M, Aalto H, Jutila T, Hirvonen TP. Signal analysis of three-dimensional nystagmus for otoneurological investigations. Ann Biomed Eng. 2011;39(3):973-82.
When registering nystagmus, the Gazelab needn’t be calibrated because of its measurement in millimeters and not in degrees in horizontal and vertical movements. However, in torsional movements the device calculates directly using degrees. First we have to define the basic parameters of the nystagmus in the graphics:
Torticolis (head tilt is registered continuously by Gazelab)
Perspectives of oscillation: vertical, horizontal, oblique and torsional
Width (in millimeters or degrees in the torsions)
Frequency: oscillations per minute or per second (Hertz)
Direction (phase velocity: pendular, jerk or irregular)
The test must be performed under different conditions: unilateral occlusion, bilateral occlusion or darkness and in different gaze positions (on the right, on the left, upwards and downwards). Otolaryngologists have been using the VNG for the diagnosis of equilibrium disorders during the last decade by carrying out several tests (caloric, head position…).
Saccadic movement and Nystagmus
REPORT: Irregular nystagmus RED=RE Horizontal; BLUE=RE Vertical Registration of a complex irregular nystagmus in primary gaze position occurring in the three perspectives of oscillation: - Vertical and horizontal oscillation in millimeters: Oscillation of 4 mm in horizontal movement and no oscillation in vertical movement.

Measurement of Ocular Torsions
- “Counter-roll” (classical knowledge) Kushner BJ, Kraft SE, Vrabec M. Ocular torsional movements in humans with normal and abnormal ocular motility--Part I: Objective measurements. J Pediatr Ophthalmol Strabismus. 1984;21(5):172-7. Kushner BJ. Ocular torsional movements in humans with normal and abnormal ocular motility: Part II--Subjective observations. J Pediatr Ophthalmol Strabismus. 1986;23(1):4-11. - Not movement at all Jampel RS, Shi DX. The absence of so-called compensatory ocular countertorsion: the response of the eyes to head tilt. Arch Ophthalmol. 2002 Oct;120(10):1331-40. - Some movement (13-22%) Schworm HD, Ygge J, Pansell T, Lennerstrand G. Assessment of ocular counterroll during head tilt using binocular video oculography. Invest Ophthalmol Vis Sci. 2002 Mar;43(3):662-7.
GazeLab is able to measure torsions in the paracentral region. The system scans the IRIS detecting the “characteristic points” and tracking them on the video to determine the exact rotation in every moment occurred during the test. Rotation modules can be used for:
Nystagmus: torsional movements are calculated in degrees directly with no need of
calibration. Bielchowsky test (torsions 15º,30º,and 45º): head tilt is registered by GazeLab. Iris scanning in a head mounted device allows measurement of the torsions of the eyeball during head movements with total accuracy. 9 gaze positions test: the computer processes the torsional data of every point registered. Torsional measurements are possible if the point projected on the wall is under 10 degrees.

Ocular Prosthesis
GazeLab provides several advantages for improving the prosthesis quality:
It analyzes motility field in all space points,
It has centering precision,
It shows what the motility limits are,
It can detect synchronization between both eyes.
So the adaptation of the prosthesis can be evaluated before having the right one. GazeLab performs 3 different tests in order to analyze the movement and the right location of the prosthesis:
1
1
2 3
4
GazeLab allows you to measure the difference between the horizontal and vertical movement of the healthy eye and the prosthesis:
Movement limit,
and speed.
Currently, the quality of the prosthesis adjustement is not good enough and it is easy to see that the patient is wearing it, due to lack of centering precision: 5 degrees.
Therefore, it is below the esthetics expectations. Gazelab allows you to better line up the prosthesis with the healthy eye. It increases accuracy thanks to the one degree precision it gives. In this way, esthetic requirements are covered.
GazeLab allows measurement of the deviation between the prosthesis and the healthy eye at each point analyzed, in the same way as it is done in the strabismus module.
3
2
1
4
> Saccade movements:
> Centering
> Following

bcninnova is a technology start-up company founded in 2008 in Barcelona. Our mission: Assist Ophthalmologists in developing, manufacturing and commercializing new “diagnosis support devices” that measure the Ocular Motility using computer vision technologies and other
engineering disciplines. Our vision: Make our devices to become the standard systems to measure ocular motility. Our guiding principles:
Working for the health of the mankind. Passion for quality. Acting fairly, honestly and clearly. Working efficiently. Researcher company’s soul.
Parc de Recerca UAB Edificio EUREKA — Campus Universitat Autònoma de Barcelona (UAB) 08193 Bellaterra (Cerdanyola del Vallès) Barcelona — Spain
www.bcninnova.com [email protected] T: +34 93 586 8964
CECOT Recognition received from the president of the Catalan Government
AAPOS/SNEC 2013—Singapore
ESA 2013 - Marseille