Embed Size (px)
Citation preview
Johns Hopkins Advanced Studies in Medicine n S549
ABSTRACT
According to the American DiabetesAssociation, approximately 82 000 nontraumaticlower-limb amputations were performed amongpeople with diabetes in the United States in 2002.Guidelines on managing the patient with diabeteswith suspected or evident foot infection, preparedby members of the Infectious Diseases Society ofAmerica, were published recently. This articlereviews the information from those guidelinesfocusing on the workup and treatment of a patientwith diabetic foot infection. Optimal managementof diabetic foot infections requires appropriate cul-ture (ie, after the wound has been cleaned, and fromthe deepest site possible) and appropriate antibiotic(ie, empirically covering for Staphylococcus andStreptococcus for mild infections and coveringaerobic and anaerobic organisms in patients withmoderate to severe infections). If hospitalizationis required, timely surgical consultation and inter-vention is critical. Surgical consultation shouldinvolve surgeons experienced with diabetic footcomplications.(Adv Stud Med. 2006;6(6C):S549-S554)
Foot infections in persons with diabetes arecommon and costly.1 They account for thelargest number of diabetes-related hospitalbed days.2 They are also the most commoncause of nontraumatic leg amputations.3,4
According to the American Diabetes Association,approximately 82 000 nontraumatic lower-limbamputations were performed among people with dia-betes in the United States in 2002. The risk of a legamputation—the most severe and permanent localmorbidity of diabetic foot infection—is 15 to 40 timesgreater for a person with diabetes than the generalpopulation.5
THE GUIDELINES
Lipsky et al published guidelines on managing thepatient with diabetes with suspected or evident footinfection, prepared by members of the InfectiousDiseases Society of America.2-4 The information focus-ing on the management of a patient with diabetic footinfection is summarized in Figure 1.6
For patients with clinically infected wounds, themost important initial task is to recognize thosepatients who require immediate hospitalization, par-enteral and broad-spectrum empirical antibiotic thera-py, and urgent consideration of diagnostic testing andsurgical consultation.6 Hospitalization should be con-sidered in patients who present with any of the fol-lowing: systemic toxicity (eg, fever and leukocytosis),metabolic instability (eg, severe hypoglycemia or aci-dosis), rapidly progressive deep-tissue infection, sub-stantial necrosis or gangrene, the presence of criticalischemia, requirement of urgent diagnostic or thera-peutic intervention, and inability to care for self orinadequate home support.6
The guidelines classify diabetic foot infectionsusing 4 categories: uninfected, mild, moderate, andsevere (Table 1).6 For patients with an infected footwound, it is important to assess the severity of infec-
PROCEEDINGS
DIAGNOSIS AND MANAGEMENT OF DIABETIC FOOT INFECTION*
—
James S. Tan, MD, MACP, FCCP†
*This article is based on a satellite symposium held inconjunction with the Interscience Conference onAntimicrobial Agents and Chemotherapy Annual Meeting inWashington, DC, on December 17, 2005.
†Professor and Vice Chairman of Internal Medicine,Head, Infectious Disease Section, Northeastern OhioUniversities College of Medicine, Chairman, Department ofMedicine, Summa Health System, Akron, Ohio.
Address correspondence to: James S. Tan, MD, MACP,FCCP, Chairman, Department of Medicine, Summa HealthSystem, 55 Arch Street, Suite 1A, Akron, OH 44304. E-mail: [email protected].

S550 Vol. 6 (6C) n June 2006
PROCEEDINGS
tion: the depth and the tissue involved, evidence ofsystemic infection, presence of metabolic instability,and critical limb ischemia. Although it is not usuallynecessary to perform an magnetic resonance imaging(MRI), a plain X ray should be obtained. The patient’scomorbid conditions and psychosocial status shouldalso be reviewed.
If hospitalization is not required, the woundshould be debrided and probed. If bone is felt with ametal probe, there is a high probability ofosteomyelitis. Obtaining the appropriate wound cul-ture is also important. We recommend cleaning thewound first, and taking a deep-tissue specimen for cul-turing. Swabs taken directly from the ulcer can be mis-leading. After a wound care regimen is prescribed,empiric therapy can be initiated. Mild infections canbe treated on an outpatient basis with oral therapywith antistaphylococcal and antistreptococcal activi-ties. However, if the patient has gastroparesis, oralagents may not be well absorbed. In any case, thepatient should be re-evaluated in 3 to 5 days (prefer-
CASE STUDY
A 56-YEAR-OLD MAN WITH DIABETIC FOOT INFECTION
DS is a 56-year-old man who presents with a 5-dayhistory of a rapidly swelling and foul-smelling left fore-foot (Figure 1). DS has insulin-dependent diabetes,with a known history of a chronic foot ulcer. As shownin Figure 1, the surrounding tissue had color indicatinggenerally good vascularity.
EVALUATION
His temperature was 38.2ºC, with mild hyperten-sion (130/85 mm Hg) and normal heart rate (90 beatsper minute). His blood glucose was 350 mg/dL with anelevated white blood cell count (15 200 cells/mm3).Plain radiograph of the foot showed no osteomyelitis.The ulcer dimensions are 2.5 cm 2 0.8 cm with adepth of 1 cm. A probe to the bone is negative.
DS was hospitalized and antibiotic therapy coveringboth aerobes and anaerobes was initiated. The woundwas debrided on admission, on day 3 of his hospital-ization, and again during surgery. The culture grewmixed aerobic/anaerobic bacteria, including methi-cillin-resistant Staphylococcus aureus (MRSA), thus ananti-MRSA agent was added. DS was clinically stable,and on day 7 of the hospitalization, DS showed con-tinued improvement. Parenteral therapy was continuedfor 2 weeks, and DS was sent home on 2 weeks of oraltherapy.
DISCUSSION
Hospitalization was the appropriate choice for DS.He had 2 criteria for hospital admission: presence of
(Continued on page S551)
Figure 1. Presentation
Figure 1. Approach to Treating a Patient withDiabetes with Foot Infection
Guidelines for Diabetic Foot Infections • CID 2004:39 (1 October) • 893
Figure 2. Algorithm 1, part 2: approach to treating a diabetic patient with a foot infection. 1Consider hospitalization if any of the following criteriaare present: systemic toxicity (e.g., fever and leukocytosis); metabolic instability (e.g., severe hypoglycemia or acidosis); rapidly progressive or deep-tissue infection, substantial necrosis or gangrene, or presence of critical ischemia; requirement of urgent diagnostic or therapeutic interventions; andinability to care for self or inadequate home support.
with the patient to whom it is attached. This distinction is
complicated by the fact that �50% of patients with a limb-
threatening infection do not manifest systemic signs or symp-
toms. After debating several classification schemes, we propose
the one presented in table 6 as a basis for subsequent discussions
in and beyond this guideline (B-II).
TREATMENT OF INFECTION
Avoid prescribing antibiotics for uninfected ulcerations.
Some argue that many apparently uninfected diabetic foot ul-
cers are actually subclinically infected—that is, they contain a
high “bioburden” of bacteria (usually defined as 1105 organisms
per gram of tissue) that results in “critical colonization” levels
and impairs wound healing [54, 109–114]. Available published
evidence does not support the use of antibiotics for the man-
agement of clinically uninfected ulcerations, either to enhance
wound healing or as prophylaxis against infection [115, 116].
Because antibiotic use encourages antimicrobial resistance, in-
curs financial cost, and may cause drug-related adverse effects,
we discourage therapy of uninfected ulcers. In some circum-
stances, it is difficult to decide whether a chronic wound is
infected, such as when the foot is ischemic, has abnormal col-
CT = computed tomography; MRI = magnetic resonance imaging.Reprinted with permission from Lipsky et al. Clin Infect Dis. 2004;39:885-910..3
Johns Hopkins Advanced Studies in Medicine n S551
PROCEEDINGS
ably 3 days) and the necessary consultations should beset up, especially surgical consultation.
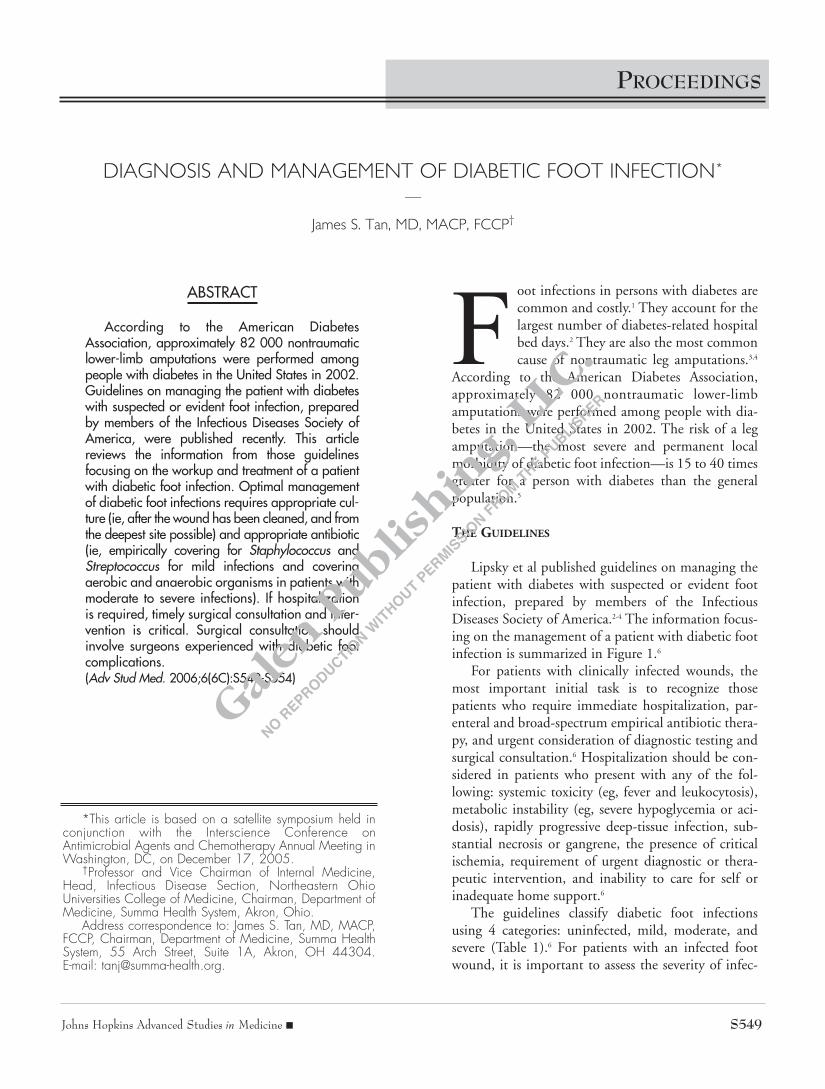
If hospitalization is required, the patient should bemedically stabilized (ie, fluid and electrolyte replace-ment and maintenance, control of blood sugar andacidosis, determination of the extent of local infection,and identification of other infection sites; Figure 1).Surgical consultation should involve surgeons experi-enced with diabetic foot complications (ie, orthopedic,vascular, or podiatric surgeons). Appropriate culturesshould be obtained (ie, wound, blood, and other sitesas necessary) and additional imaging may be consid-ered. Bone scans are nonspecific and generally do notyield more clinically relevant information. Plain radi-ograph of the foot is more cost effective. The most use-ful imaging is MRI of the foot. Empiric antimicrobialtherapy should be initiated (usually parenterally) andthe patient should be re-evaluated at least daily.6
The importance of timely surgical consultation andintervention cannot be overstated. The key to reducingabove-ankle amputation rates and hospital length ofstay is to obtain early surgical debridement andremoval of dead bone. The rate of above-ankle ampu-
(Continued from page S550)
fever and leukocytosis and a rapidly progressive ordeep-tissue infection. Although his blood sugar washigh, it is not a criterion for hospitalization and couldbe managed as an outpatient; however, high bloodsugar can be an indication of the severity of his illness.Figure 2 is an algorithm of DS’s case.1 It follows theguidelines for managing patients with evidence of adiabetic foot infection.
REFERENCE
1. Lipsky BA, Berendt AR, Deery HG, et al. Diagnosis andtreatment of diabetic foot infections. Clin Infect Dis.2004;39:885-910.
Figure 2. Management
900 • CID 2004:39 (1 October) • Lipsky et al.
Figure 4. Algorithm 2: approach to selecting antibiotic therapy for a diabetic patient with a foot infection. MRSA, methicillin-resistant Staphylococcusaureus.
ulceration, a “sausage toe” (i.e., a red, swollen digit) [246], or
an unexplained high WBC count [235] or inflammatory mark-
ers [236] should also arouse suspicion of osteomyelitis (B-II).
Finally, radiologically evident bone destruction beneath an ulcer
should be considered to represent osteomyelitis unless proven
otherwise [247].
Confirming the diagnosis. Because bony destruction is
usually not seen on plain radiography performed during the
early stages of disease and neuro-osteoarthropathy can mimic
infection, diagnosing osteomyelitis at the time the patient first
presents to the hospital can be difficult [248–250]. Character-
istic progressive changes on serial plain radiographs may help
in more-chronic cases [247, 251]. Radioisotope scans are more
sensitive than radiographs for detecting osteomyelitis during
the early stages of this diseases, but they are expensive and can
be time-consuming [252]. The reported performance charac-
teristics of various types of nuclear medicine scans varies, but
the specificity of technetium bone scans is generally low [240,
MRSA = methicillin-resistant Staphylococcus aureus.Reprinted with permission from Lipsky et al. Clin Infect Dis. 2004;39:885-910.1
Table 1. Clinical Classification of Diabetic FootInfections Based on Severity
Uninfected Wound lacking purulence or any manifestationof infection
Mild Presence of ≥2 manifestations of inflammation(purulence, erythema, pain, tenderness, warmth, orinduration), but any cellulitis/erythema extends <2cm around the ulcer, and infection is limited to theskin or superficial subcutaneous tissues; no otherlocal complications or systemic illness
Moderate Infection (as above) in a patient who is well andmetabolically stable but has ≥1 of the followingcharacteristics:
• Cellulitis extending >2 cm• Lymphangitis streaking• Spread beneath the superficial fascia, deep-
tissue abscess, gangrene, and involvement of muscle, tendon, joint, or bone
Severe Infection in a patient with systemic toxicity ormetabolic instability
• Fever, chills, tachycardia, hypotension, confu-sion, and vomiting
• Leukocytosis, acidosis, azotemia, and severe hyperglycemia
Data from Lipsky et al.3
S552 Vol. 6 (6C) n June 2006
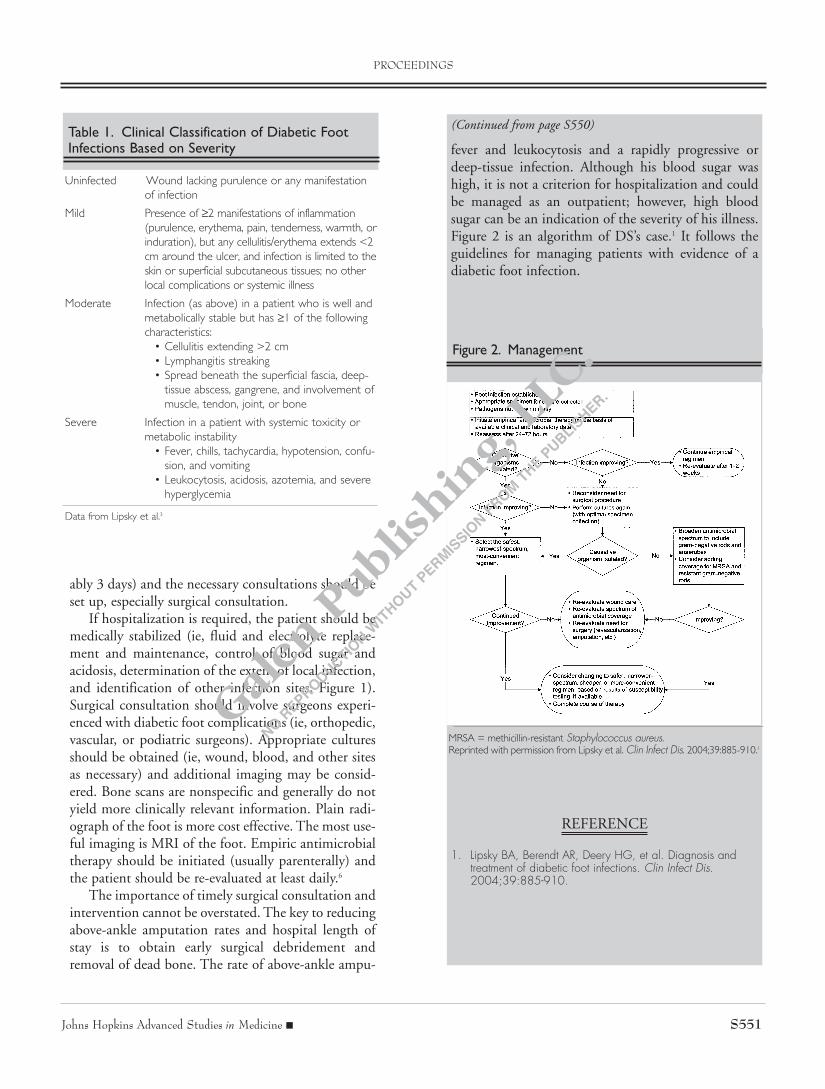
tation was compared in 164 patients with diabeticinfection, who were divided into 2 groups: thosepatients who did not undergo surgical interventionduring the first 3 days of hospitalization but receivedintravenous empiric antimicrobial therapy (87 patients)and those who underwent surgical interventionpromptly and received intravenous antimicrobial thera-py (77 patients). As shown in Figure 2, those patients
who received surgical intervention had significantly fewerabove-ankle amputations during the same hospitalizationor subsequent admission after a 12-month follow-up.The early surgical intervention group was also associatedwith a reduced length of stay by at least 6 days.7
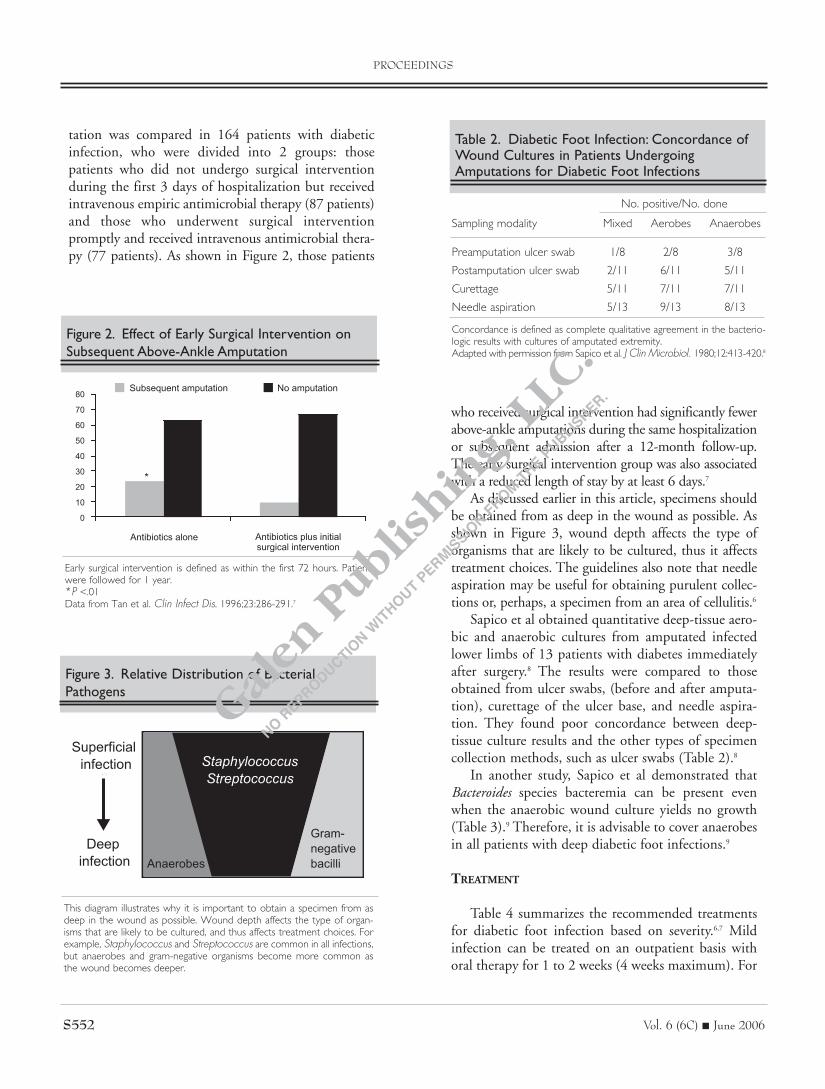
As discussed earlier in this article, specimens shouldbe obtained from as deep in the wound as possible. Asshown in Figure 3, wound depth affects the type oforganisms that are likely to be cultured, thus it affectstreatment choices. The guidelines also note that needleaspiration may be useful for obtaining purulent collec-tions or, perhaps, a specimen from an area of cellulitis.6
Sapico et al obtained quantitative deep-tissue aero-bic and anaerobic cultures from amputated infectedlower limbs of 13 patients with diabetes immediatelyafter surgery.8 The results were compared to thoseobtained from ulcer swabs, (before and after amputa-tion), curettage of the ulcer base, and needle aspira-tion. They found poor concordance between deep-tissue culture results and the other types of specimencollection methods, such as ulcer swabs (Table 2).8
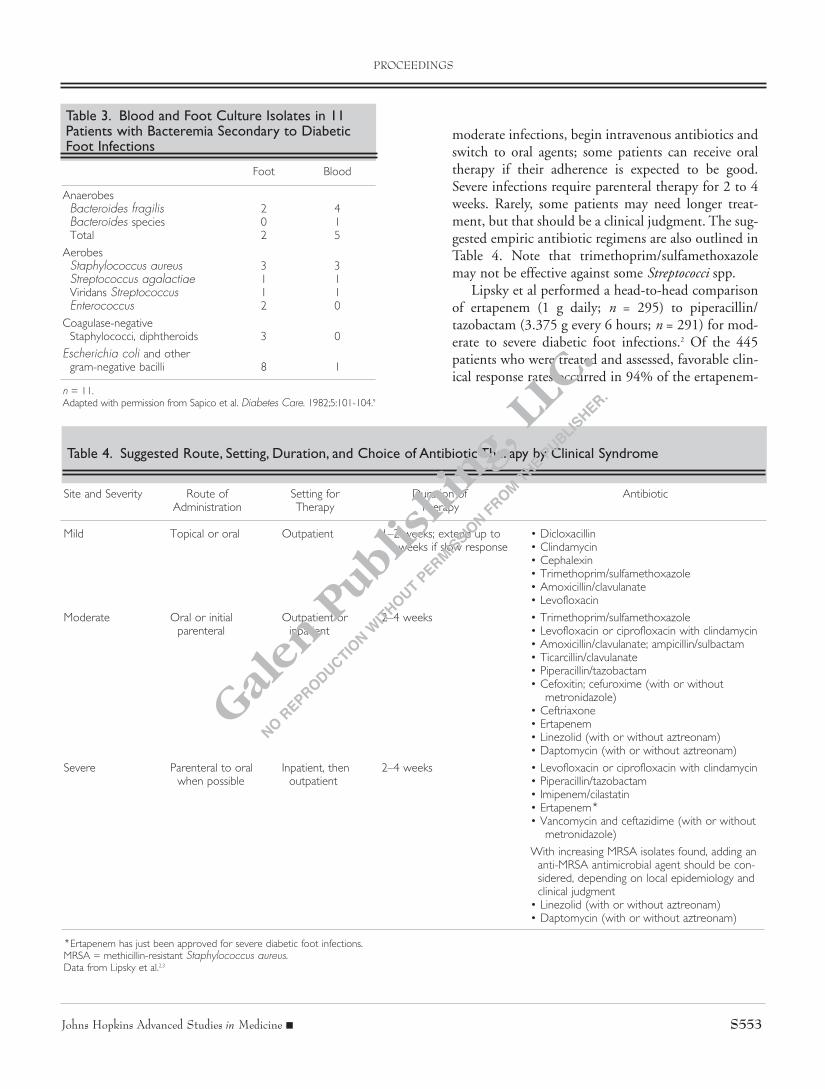
In another study, Sapico et al demonstrated thatBacteroides species bacteremia can be present evenwhen the anaerobic wound culture yields no growth(Table 3).9 Therefore, it is advisable to cover anaerobesin all patients with deep diabetic foot infections.9
TREATMENT
Table 4 summarizes the recommended treatmentsfor diabetic foot infection based on severity.6,7 Mildinfection can be treated on an outpatient basis withoral therapy for 1 to 2 weeks (4 weeks maximum). For
PROCEEDINGS
Figure 2. Effect of Early Surgical Intervention onSubsequent Above-Ankle Amputation
80
70
60
50
40
30
20
10
0
Antibiotics alone Antibiotics plus initialsurgical intervention
Subsequent amputation No amputation
*
Early surgical intervention is defined as within the first 72 hours. Patientswere followed for 1 year.*P <.01Data from Tan et al. Clin Infect Dis. 1996;23:286-291.7
Figure 3. Relative Distribution of BacterialPathogens
StaphylococcusStreptococcus
Anaerobes
Superficial infection
Deep infection
Gram-negativebacilli
This diagram illustrates why it is important to obtain a specimen from asdeep in the wound as possible. Wound depth affects the type of organ-isms that are likely to be cultured, and thus affects treatment choices. Forexample, Staphylococcus and Streptococcus are common in all infections,but anaerobes and gram-negative organisms become more common asthe wound becomes deeper.
Table 2. Diabetic Foot Infection: Concordance ofWound Cultures in Patients UndergoingAmputations for Diabetic Foot Infections
No. positive/No. done
Sampling modality Mixed Aerobes Anaerobes
Preamputation ulcer swab 1/8 2/8 3/8
Postamputation ulcer swab 2/11 6/11 5/11
Curettage 5/11 7/11 7/11
Needle aspiration 5/13 9/13 8/13
Concordance is defined as complete qualitative agreement in the bacterio-logic results with cultures of amputated extremity.Adapted with permission from Sapico et al. J Clin Microbiol. 1980;12:413-420.8
Johns Hopkins Advanced Studies in Medicine n S553
moderate infections, begin intravenous antibiotics andswitch to oral agents; some patients can receive oraltherapy if their adherence is expected to be good.Severe infections require parenteral therapy for 2 to 4weeks. Rarely, some patients may need longer treat-ment, but that should be a clinical judgment. The sug-gested empiric antibiotic regimens are also outlined inTable 4. Note that trimethoprim/sulfamethoxazolemay not be effective against some Streptococci spp.
Lipsky et al performed a head-to-head comparisonof ertapenem (1 g daily; n = 295) to piperacillin/tazobactam (3.375 g every 6 hours; n = 291) for mod-erate to severe diabetic foot infections.2 Of the 445patients who were treated and assessed, favorable clin-ical response rates occurred in 94% of the ertapenem-
PROCEEDINGS
Table 3. Blood and Foot Culture Isolates in 11Patients with Bacteremia Secondary to DiabeticFoot Infections
Foot Blood
AnaerobesBacteroides fragilis 2 4Bacteroides species 0 1Total 2 5
AerobesStaphylococcus aureus 3 3Streptococcus agalactiae 1 1Viridans Streptococcus 1 1Enterococcus 2 0
Coagulase-negativeStaphylococci, diphtheroids 3 0
Escherichia coli and othergram-negative bacilli 8 1
n = 11.Adapted with permission from Sapico et al. Diabetes Care. 1982;5:101-104.9
Table 4. Suggested Route, Setting, Duration, and Choice of Antibiotic Therapy by Clinical Syndrome
Site and Severity Route of Setting for Duration of AntibioticAdministration Therapy Therapy
Mild Topical or oral Outpatient 1–2 weeks; extend up to • Dicloxacillin4 weeks if slow response • Clindamycin
• Cephalexin• Trimethoprim/sulfamethoxazole• Amoxicillin/clavulanate• Levofloxacin
Moderate Oral or initial Outpatient or 2–4 weeks • Trimethoprim/sulfamethoxazoleparenteral inpatient • Levofloxacin or ciprofloxacin with clindamycin
• Amoxicillin/clavulanate; ampicillin/sulbactam• Ticarcillin/clavulanate• Piperacillin/tazobactam• Cefoxitin; cefuroxime (with or without
metronidazole)• Ceftriaxone• Ertapenem• Linezolid (with or without aztreonam)• Daptomycin (with or without aztreonam)
Severe Parenteral to oral Inpatient, then 2–4 weeks • Levofloxacin or ciprofloxacin with clindamycinwhen possible outpatient • Piperacillin/tazobactam
• Imipenem/cilastatin• Ertapenem*• Vancomycin and ceftazidime (with or without
metronidazole)
With increasing MRSA isolates found, adding an anti-MRSA antimicrobial agent should be con-sidered, depending on local epidemiology and clinical judgment
• Linezolid (with or without aztreonam)• Daptomycin (with or without aztreonam)
*Ertapenem has just been approved for severe diabetic foot infections.MRSA = methicillin-resistant Staphylococcus aureus.Data from Lipsky et al.2,3

treated group and 92% of the piperacillin/tazobactam-treated group.2
Also, as noted in the guidelines, aerobic gram-pos-itive cocci (especially Staphylococcus aureus) are the pre-dominant pathogens in diabetic foot infections, andmethicillin-resistant Staphylococcus aureus (MRSA)incidence is an ever-increasing concern, especially withassociated worse outcomes. Therefore, adding an anti-S aureus (and anti-MRSA, depending on local epi-demiology and clinical judgment) antimicrobial agentshould be considered.6
CONTINUING TREATMENT
If the patient improves, the antimicrobial regimenshould reassessed, thus a therapy with narrower spec-trum, lower cost, or greater convenience can be con-sidered (Figure 1).6 The wound care regimen shouldalso be reviewed, and the patient can be prepared for
discharge if hospitalized. Follow-up should occurwithin 1 to 2 weeks, preferably by 1 week.6
If the patient is not improving after empiric thera-py, the physician needs to consider whether the surgi-cal intervention was adequate; the infection wasadequately treated regarding the cultured organism(s),susceptibility, and antimicrobial agent; the patient’svascular status needs augmentation; or if the woundcare regimen needs to be adjusted (Figure 4).6
CONCLUSIONS
Optimal management of diabetic foot infectionsrequires appropriate culture (ie, after the wound hasbeen cleaned, and from the deepest site possible) andappropriate antibiotic (ie, empiric coverage for aerobicand anaerobic organisms). If hospitalization isrequired, timely surgical consultation and interventionis critical. Surgical consultation should involve sur-geons experienced with diabetic foot complications.
REFERENCES
1. American Diabetes Association Web site press release.World Diabetes Day focuses on preventing lower limbamputations. November 14, 2005. Available at:http://www.diabetes.org/uedocuments/WorldDiabetesDay2005FINAL.pdf. Accessed February 15, 2006.
2. Lipsky BA, Armstrong DG, Citron DM, et al. Ertapenem ver-sus piperacillin/tazobactam for diabetic foot infections(SIDESTEP): prospective, randomised, controlled, double-blinded, multicentre trial. Lancet. 2005;366:1695-1703.
3. Lipsky BA, Berendt AR, Deery HG, et al. Diagnosis andtreatment of diabetic foot infections. Clin Infect Dis.2004;39:885-910.
4. Lipsky BA. A report from the international consensus ondiagnosing and treating the infected diabetic foot. DiabetesMetab Res Rev. 2004;20(suppl 1):S68-S77.
5. Pecoraro RE, Reiber GE, Burgess EM. Pathways to diabeticlimb amputation: basis for prevention. Diabetes Care.1990;13:513-521.
6. Reiber GE, Vileikyte L, Boyko EJ, et al. Causal pathways forincident lower-extremity ulcers in patients with diabetes fromtwo settings. Diabetes Care. 1999;22:157-162.
7. Tan JS, Friedman NM, Hazelton-Miller C, et al. Canaggressive treatment of diabetic foot infections reduce theneed for above-ankle amputation? Clin Infect Dis.1996;23:286-291.
8. Sapico FL, Canawati HN, Witte JL, et al. Quantitative aero-bic and anaerobic bacteriology of infected diabetic feet. J Clin Microbiol. 1980;12:413-420.
9. Sapico FL, Bessman AN, Canawati HN. Bacteremia in dia-betic patients with infected lower extremities. DiabetesCare. 1982;5:101-104.
S554 Vol. 6 (6C) n June 2006
Figure 4. Approach to Assessing a Patient withDiabetes with a Foot Infection Who Is NotResponding Well to Treatment
Guidelines for Diabetic Foot Infections • CID 2004:39 (1 October) • 899
Figure 3. Algorithm 1, part 3: approach to assessing a diabetic patient with a foot infection who is not responding well to treatment. TcPO2,transcutaneous partial pressure of O2.
OSTEOMYELITIS
Dealing with osteomyelitis is perhaps the most difficult and
controversial aspect in the management of diabetic foot infec-
tions [239–244]. First among several problems is that the lack
of a consensus definition of the disease hinders the comparison
of available studies and experiences. Next, there are many avail-
able diagnostic tests, but they often yield equivocal results. Fur-
thermore, the presence of osteomyelitis increases the likelihood
of surgical intervention, including amputation, and the re-
quired duration of antibiotic therapy [240]. Finally, osteomy-
elitis impairs healing of the overlying wound and acts as a focus
for recurrent infection.
When to consider the diagnosis. Consider osteomyelitis as
a potential complication of any deep or extensive ulcer, espe-
cially one that is chronic or overlies a bony prominence (figure
5) [245]. Suspect underlying osteomyelitis when an ulcer does
not heal after at least 6 weeks of appropriate care and off-
loading. Any ulcer in which bone is either visible or can be
easily palpated with a sterile blunt metal probe is likely to be
complicated by osteomyelitis [83]. In patients with a limb-
threatening infection, positive results of a probe-to-bone test
may be taken as nearly sufficient for diagnosis, but the per-
formance characteristics of this test have not yet been fully
defined. A swollen foot in a patient with a history of foot
TcPO2 = transcutaneous partial pressure of oxygen.Reprinted with permission from Lipsky et al. Clin Infect Dis. 2004;39:885-910.3
PROCEEDINGS
revascularization