Embed Size (px)
Citation preview

Diagnosis and Management of Diabetic Neuropathies
Part 4
Aaron I. Vinik, MD, PhD, FCP, MACP Professor of Medicine/Pathology/NeurobiologyDirector of Research and Neuroendocrine Unit
Eastern Virginia Medical SchoolStrelitz Diabetes Center for
Endocrine and Metabolic DisordersNorfolk, Virginia

• Noninvasive, no exposure to radiation
• Allows repetitions, follow-ups, longitudinal studies
• Task and rest in the same session
• Good spatial and temporal resolution
• Can be used to study brain, brain stem, and spinal cord
What Are the Advantages of fMRI?
2.3
8.0
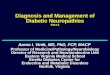
Brain response to noxious heat

Increased Cerebral Activation as a Result of Central Sensitization in Healthy Subjects
Zambreanu L, et al. Pain. 2005;114:397-407.
Normal nociceptive transmission (no hyperalgesia)
Central sensitization (secondary hyperalgesia)60 g monofilament after 45° C + capsaicin
Functional MRI

Skin Biopsies
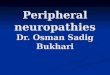
• Skin biopsy – determines damage to
small nerve fibers– allows quantification of
somatic IENFs– has a diagnostic
efficiency of 88.4%– is an invasive technique
requiring local anaesthesia
Devigili G et al. Brain. 2008;131:1912.Sorensen L et al. Diabetes Care. 2006;29:883.
Kennedy WR. Muscle Nerve. 2004;756:756.Pittenger GL et al. Diabetes Care. 2004;27:1974.
Neuropathy Controls
0
5
10
15
20
IEN
F/m
m
IENF, intra-epidermal nerve fibers
Reduced IENF density in painful diabetic neuropathy

Generic Scales Commonly Used in Clinical Trials
Pain Quality of Life/Outcomes• 11-point numeric rating scale
• 4-point verbal rating scale (VRS)
• Visual analog scale (VAS)
• McGill Pain Questionnaire (MPQ)
• Brief Pain Inventory (BPI)
• Medical Outcomes Survey Short Form-36 (MOS SF-36)
• Sleep interference scales
• Quality of life (QoL)

Neuropathic Pain Scales Commonly Used in Clinical Trials
• 11-point Neuropathy Pain Scale (NPS)
• Neuropathic Pain SymptomInventory (NPSI)
• Brief Pain Inventory (BPI)• Leeds Assessment of Neuropathic
Symptoms and Signs (S-LANSS)• Neuropathic Pain Questionnaire
(NPQ)• Neuropathy Total Symptom Score
(NTSS)• Total Symptom Score (TSS)• Neuropathy Symptom Score (NSS)• Neuropathy Impairment Score (NIS)• Michigan Neuropathy Screening
Instrument (MNSI)
Neuropathic Pain Symptom Inventory
Date: First name: Last name: Sex: Age: You are suffering from pain due to injury or disease of the nervous system. This pain may be of several types. You may have spontaneous pain, i.e. pain in the absence of any stimulation, which may be long-lasting or occur as brief attacks. You may also have pain provoked or increased by brushing, pressure, or contact with cold in the painful area. You may feel one or several types of pain. This questionnaire has been developed to help your doctor to better evaluate and treat various types of pain you feel. We wish to know if you feel spontaneous pain, that is pain without any stimulation. For each of the following questions, please select the number that best describes your average spontaneous pain severity during the past 24 h. Select the number 0 if you have not felt such pain (circle one number only). Q1. Does your pain feel like burning? No burning 0 1 2 3 4 5 6 7 8 9 10 Worst burning imaginable Q2. Does your pain feel like squeezing? No squeezing 0 1 2 3 4 5 6 7 8 9 10 Worst squeezing imaginable Q3. Does your pain feel like pressure? No pressure 0 1 2 3 4 5 6 7 8 9 10 Worst pressure imaginable Q4. During the past 24 h, your spontaneous pain has been present: Permanently / _ / Between 8 and 12 h / _ / Between 4 and 7 h / _ / Between 1 and 3 h / _ / Less than 1 h / _ / We wish to know if you have brief attacks of pain. For each of the following questions, please select the number that best describes the average severity of your painful attacks during the past 24 h. Select the number 0 if you have not felt such pain (circle one number only). Q5. Does your pain feel like electric shocks? No shocks 0 1 2 3 4 5 6 7 8 9 10 Worst shocks imaginable Q6. Does your pain feel like stabbing? No stabbing 0 1 2 3 4 5 6 7 8 9 10 Worst stabbing imaginable Q7. Is your pain provoked or increased by brushing on the painful area? No pain 0 1 2 3 4 5 6 7 8 9 10 Worst pain imaginable Q9. Is your pain provoked or increased by pressure on the painful area? No pain 0 1 2 3 4 5 6 7 8 9 10 Worst pain imaginable
NEUROPATHY PAIN SCALE
Instructions: There are several different aspects of pain which we are interested in measuring: pain sharpness, heathold, dullness, intensity, overall unpleasantness, and surface vs. deep pain. Many people are able to tell the difference between many aspects of their pain: for example, how much it hurts and how unpleasant or annoying it is. Although often the intensity of pain has a strong influence on how unpleasant the experience of pain is, some people are able to experience more pain than others before they feel very bad about it. There are scales for measuring different aspects of pain. For one patient, a pain might feel extremely hot, but not at all dull, while another patient may not experience any heat, but feel like their pain is very dull. We expect you to rate very high on some of the scales below and very low on others. We want you to use the measures that follow to tell us exactly what you experience.

Painful Diabetic Polyneuropathy
EFNS Canadian IASP1st Line TCA
GabapentinPregabalin
TCA GabapentinPregabalin
TCA, GabapentinPregabalinSNRIs
2nd Line SNRI
LamotrigineOpioidsTramadol
SNRITop. lidocaine
OpioidsTramadol
3rd Line TramadolCR opioid
Antiepileptics MexiletineNMDA antagonistTop. capsaicin
4th Line Cannabinoid, methadone, lamotrigine, topiramate, valproic acid

Painful Diabetic NeuropathyOdds Ratios and NNTs for 50% Pain Relief
• Tricyclic antidepressants: 22.24 (NNT=3.4)(desipramine, imipramine, amitriptyline)
• Traditional ACDs: 5.33 (6.0)(carbamazepine, valpraote, oxcarbazepine)
• Opioids and tramadol: 4.25 (3.1)
• Newer-generation ACDs: 3.25(gabapentin, pregabalin 300−600 mg*) (3.3−4.1)
• SNRI (duloxetine 60/120 mg*): 2.55/2.1 (7.2/4.2)
Wong M et al. BMJ. 2008;335:87.Chong MS, Hester J. Drugs. 2007;67:569.*FDA-approved indication.

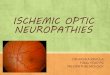
• Post-hoc analysis of data from patients who reached their target dose• Mean reduction in pain intensity: Greatest for lamotrigine 400 mg (P<0.05 vs placebo)
−2.7 for lamotrigine 400 mg −2.5 for lamotrigine 300 mg−2.0 for placebo
1 2 3 4 5 6 7 8 9 11 13 15 17 19
Painful Diabetic NeuropathyLamotrigine
Vinik AI et al. Pain. 2007;128:169.
−1.5
−2.0
−2.5
0
−0.5
−1.0
−3.0
−3.51 2 3 4 5 6 7 8 9 11 13 15 17 19
Study 1
Pai
n I
nte
ns
ity
Ch
an
ge
Fro
m B
ase
lin
e
**
** * * *
Dose Escalation Maintenance
Last Observation Carried Forward0
−0.5
−1.0
−3.0
−3.5
Study 2
Dose Escalation Maintenance
−1.5
−2.0
−2.5
PlaceboLamotrigine 200 mgLamotrigine 300 mgLamotrigine 400 mg
*P<0.05 vs placebo
Used with permission from IASP

Painful Diabetic Neuropathy Topiramate
• 3 RCTs that were negative1
• 50% vs 34% with >30% relief of pain, decreased pain, and improved sleep2
Mean Pain Score Worst Pain75
70
65
60
55
50
45
400 4 8 12
Week
Pai
n V
isu
al A
nal
og
Sca
leS
core
(0−
100
mm
)
P=0.028P=0.038
3.2
3.0
2.8
2.6
2.4
2.2
2.0
1.80 4 8 12
Week
Sco
re O
ver
Pas
t W
eek
(0−
4)
P=0.026P=0.003
1. Thienel U et al. Acta Neurol Scand. 2004;110:221.2. Raskin P et al. Topiramate vs placebo in painful diabetic neuropathy:
analgesic and metabolic effect. Neurology. 2004;63:865-873.
Topiramate Placebo