Embed Size (px)
Citation preview

40 JCN 2018, Vol 32, No 1
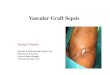
Cellulitis is an acute bacterial infection of the dermis and subcutaneous tissues,
characterised by localised swelling, erythema, pain, tenderness and warmth (Goettsch et al, 2006; Figure 1). It is associated with significant morbidity (Cox et al, 1998; Tay et al, 2015), and complications include necrotising fasciitis, septicaemia, post-streptococcal nephritis and death (Clinical Resource Efficiency Support Team [CREST], 2005; Sepsis Alliance — www.sepsis.org/sepsis-and/cellulitis/).
Erysipelas is a bacterial infection of the dermis and the upper subcutaneous tissue, often hallmarked by a defined raised edge, reflecting dermal involvement (Cranendonk et al, 2014). In the past, it was viewed as a separate entity to cellulitis, however, more recently, it has been classified as a
Diagnosis and management of lower limb cellulitis
form of cellulitis owing to difficulty in clinical distinction and the similarity of causative factors and treatment (Chira and Miller, 2010).
The bacteria that most commonly cause cellulitis are streptococci (Morris, 2003), with some cases also due to staphylococcal or mixed infection, especially if the cellulitis is localised or follows a penetrating injury (Cox et al, 1998).
CLINICAL FEATURES AND INVESTIGATIONS
Cellulitis develops rapidly. The first signs may be a flu-like illness with the person developing a high temperature and feeling cold and shivery before the local signs appear on the leg. The skin becomes red, hot, swollen and painful with a clear line of demarcation between normal and affected skin (Wingfield, 2009; Beasley, 2011; Wingfield, 2012). It is useful to mark this line at first
examination, as this allows for observation of the condition, and provides a baseline against which to measure any improvement or deterioration. Blistering or ulceration of the skin may occur and usually only one leg is affected (CREST, 2005). Local lymph nodes may also feel tender (Cox, 2002).
Blood cultures are rarely positive (2–4%) and should be reserved for patients with severe infection and/or sepsis (Aly et al, 1996; CREST, 2005). However, a complete blood count may assist in assessing the severity of illness with marked leucocytosis, new onset anaemia caused by haemolysis, or thrombocytopenia suggesting a lead up to sepsis (Eron et al, 2003). Raised C-reactive protein (CRP) level, while not disease-specific, confirms the inflammatory response and provides an empirical measure for improvement. Elevated levels of blood urea and creatinine suggest intravascular volume depletion
Jane Todhunter, vascular nurse practitioner, North Cumbria University Hospitals
Lower limb cellulitis is a common acute medical condition that results in a large number of hospital admissions (Clinical Resource Efficiency Support Team [CREST], 2005). It is a growing and costly problem. The NHS spends between £172–£254 million a year on inpatient treatment of people with lower leg cellulitis (Curtis, 2011). The clinical presentation of cellulitis is similar to other conditions and diagnostic errors are common and may prolong hospital stay (Nazarko, 2012). Community nurses are involved in caring for people at risk of cellulitis and are often responsible for referring on suspected cases and then continuing treatment upon discharge. It is essential that community nurses are aware of the evidence base for diagnosis, differential diagnosis, treatment and management, as well as the long-term prevention of cellulitis. This paper discusses the evidence base for treatment and prevention of cellulitis and presents a case study.
KEYWORDS: Accurate diagnosis Prevention Leg oedema Antibiotic therapy Compression
Jane Todhunter
WOUND CARE
Figure 1.Cellulitis of the lower limb.
© 2018
Wou
nd C
are P
eople
Ltd

JCN 2018, Vol 32, No 1 41
WOUND CARE
or renal failure, while raised creatine kinase levels may indicate myonecrosis (necrotic damage, particularly to muscle tissue) caused by necrotising fasciitis or gas gangrene (Eron et al, 2003).
DIFFERENTIAL DIAGNOSES
The clinical presentation of cellulitis is similar to other conditions (see below; Table 1) and diagnostic errors are common (Nazarko, 2012). David et al (2011) found a diagnosis error rate of 28% in patients admitted to hospital with cellulitis. This is corroborated by Levell et al (2011), who reviewed referrals to a single-centre cellulitis clinic and found a misdiagnosis rate of 33%. It is most commonly confused with varicose eczema, lipodermatosclerosis and deep vein thrombosis (DVT), but may also be confused with contact dermatitis, lymphoedema or thrombophlebitis (Cox, 2002; Levell et al, 2011). This is due to the similar presentation of redness and swelling to the lower limbs.
Varicose eczema Varicose eczema is an inflammatory skin condition associated with chronic venous disease (Figure 2). It often affects both legs and causes crusting, scaling and itch (CREST, 2005). The person is not unwell and does not have a high temperature as a result. The skin will respond to steroid ointment, emollient treatment and compression bandaging.
LipodermatosclerosisLipodermatosclerosis is associated with chronic venous disease (Bianchi, 2013). It is a thickening or fibrosis of the tissues under the skin causing them to feel hard and woody and forms a fibrin cuff around the lower gaiter (National Institute for Health and Care Excellence [NICE], 2017). This results in the classic inverted champagne-shaped leg (Figure 3). It can develop acutely; causing pain, redness and swelling of the leg, but the person is not unwell.
Deep vein thrombosis (DVT)This causes pain and swelling in one leg without any redness. The
person usually does not feel unwell or have a fever (CREST, 2005).
Contact dermatitis This is caused by the presence of an allergen or irritant to the skin (Figure 4). It usually settles with removal of the irritant and washing the leg, but steroid ointment may also help. In the author’s clinical experience, the leg may itch and feel uncomfortable, but the person is not unwell or have a fever, unless the dermatitis becomes infected (NHS Choices, 2016).
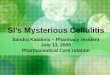
Lymphoedema Lymphoedema causes chronic swelling of the limb. In Figure 5 it presents as bilateral red legs from chronic, untreated oedema. There is no tenderness, and the person is not unwell or have a fever, but, being a lifelong condition, can have a significant negative impact on patient quality of life (Green, 2008). Compression bandaging should be started with a view to maintenance treatment with long-term compression garments or wraps once limb volume reduction has been achieved (Hunter, 2017).
Superficial thrombophlebitis Figure 6 shows unilateral superficial thrombophlebitis to the patient’s left leg around the medial gaiter. It is tender to touch, with visible varicose veins. The person is not unwell and does not have a fever. Treatment should involve anti-inflammatory gel and compression. Once resolved, a duplex scan of the venous system may be taken, with a view to intervention. Treatment of the veins usually involves endothermal ablation (NICE, 2013).
CLASSIFICATION AND TREATMENT OF CELLULITIS
Most cases of cellulitis are caused by beta-haemolytic streptococci or Staphylococcus aureus, so empirical treatment should be active against these organisms (CREST, 2005). In many clinical settings, there appears to be variation in the treatment of the condition — it is not always evidence-based and may frequently be undertreated
Figure 2.Varicose eczema.
Figure 3.Lipodermatosclerosis.
Figure 4.Contact dermatitis.
Figure 5.Lymphoedema.
Figure 6.Superficial thrombophlebitis.
© 2018
Wou
nd C
are P
eople
Ltd

How to enterYou will be asked to submit a written statement of 500–600 words, considering the questions below, to support why you feel this nurse/team has made an outstanding contribution to wound care practice.
What exceptional impact has their practice/care had on their colleagues and/or patients? What specific initiative have they instigated that has made a real difference to patient lives? Is there any one patient episode that stands out as exceptional practice in challenging circumstances? How has this contribution affected patient care? How has this contributed to tissue viability nursing overall? Is there any evidence to support the entry (national guidelines, literature, etc).
This award is in partnership with
Nominate yourself, colleagues or team to celebrate achievements in wound prevention and management inthe communityDo you know anyone who is making a real difference to patients’ wound care in your area? Maybe you are proud of something you have achieved and feel others could benefit from sharing this experience?
To enter, simply visit www.jcn.co.uk/awards
Outstanding Practice in Wound Care Award 2018
© 2018
Wou
nd C
are P
eople
Ltd

JCN 2018, Vol 32, No 1 43
WOUND CARE
(Marwick et al, 2011). There is little in the literature to guide clinical decision-making regarding the type, route and duration of antibiotic therapy. Classification of the patient with cellulitis may assist with the decisions that need to be made about how and where to treat, but there is limited evidence that using a classification system can modify clinical outcome.
There are two prominent classification systems within the literature, namely; Eron (2000) and the Novia Scotia Adult Cellulitis Guidelines (Campbell et al, 2009), with similar categories of grading used in both. Eron’s classification system divides people with cellulitis into four classes (Table 2). Classes one and two have the potential to be treated at home, while classes three and four are usually admitted to hospital due to the severity of their condition.
Class one patients are normally treated with oral antibiotics, usually flucloxacillin, but classes two and above with intravenous (IV) therapy to benefit from a rapid increase of antibiotic in the blood. It is common practice for both IV benzylpenicillin and flucloxacillin to be prescribed in the management of hospitalised
patients (CREST, 2005), however, there is no evidence of additional benefit from this combination and it is sufficient to use flucloxacillin alone (Tan et al, 2007). For those with an allergy to penicillin, the alternative is clarithromycin (CREST, 2005).
There is a lack of meta-analyses to advise which empirical treatment for cellulitis is most effective, therefore antibiotic therapy should be guided by the clinical picture, microbiology rationale and local guidelines. Expert advice from microbiology should be sought when a patient is not responding to standard treatment.
The timing of the switch from IV to oral antibiotics appears to be
based more on clinical experience than research. The consensus is that most patients may be safely switched to oral agents after three to four days (Eron et al, 2003; CREST, 2005), but the timing should be guided by the clinical picture when the signs and symptoms of the infection are improving. Most people will require one to two weeks of antibiotic therapy, or until there is a marked improvement in the clinical signs (Eron et al, 2003).
CAUSES AND RISK FACTORS
There is scant research on the risk factors for cellulitis. Three case controlled studies provide some level four evidence to suggest a disruption of the cutaneous barrier caused by leg ulcers, injury, tinea pedis, or leg
Table 1: Common differential diagnoses of cellulitis (Nazarko, 2012)
Varicose eczema Lipodermatosclerosis DVT Cellulitis
Symptoms
No feverItchingHistory of varicose veins or DVT
No feverPain and discomfortHistory of varicose veins or DVT
No feverCalf pain and discomfort
May have feverPainfulNo relevant history
Signs Normal temperatureDoes not feel unwellBilateralInflamedErythematousNo tendernessCrustingUlcersChronic venous skin changes may be presentVaricose veins may be visible
Normal temperatureDoes not feel unwellBilateralInflamed ErythematousNo tendernessHardening and thickening of the tissuesAtrophie blancheHaemosiderin stainingInverted champagne- shaped legsVaricose veins may be visible
Normal temperatureDoes not feel unwell UnilateralMay be erythematousTender
High temperatureFeels unwellUnilateralInflamedErythematousTenderBlistersOedematous limb
Investigations White cell count normalCRP normalBlood culture negative
White cell count normalCRP normal in chronic state, but raised in acuteBlood culture negative
Positive D-dimerWhite cell count normalCRP raisedBlood culture negative
White cell count raisedCRP raisedBlood culture usually negative
Table 2: Cellulitis classifications (Eron, 2000)
Class Descriptions
One Patients have no signs of systemic toxicity, have no uncontrolled comorbidities and can usually be managed with oral antimicrobials on an outpatient basis
Two Patients are either systemically ill or systemically well but with a comorbidity such as peripheral vascular disease, chronic venous insufficiency or morbid obesity, which may complicate or delay resolution of their infection
Three Patients may have a significant systemic upset such as acute confusion, tachycardia, tachypnoea, hypotension or may have unstable comorbidities that may interfere with a response to therapy or have a limb-threatening infection due to vascular compromise
Four Patients have sepsis syndrome or severe life-threatening infection, such as necrotising fasciitis
© 2018
Wou
nd C
are P
eople
Ltd

44 JCN 2018, Vol 32, No 1
tinea pedis, who suddenly felt unwell one evening after work. He felt shivery and had a temperature. He thought he was getting a cold and took two paracetamol tablets and went to bed. He had a disturbed night and realised later that he had suffered hallucinations. In the morning, he was aware that his left leg was extremely painful and was horrified to see that it was red, hot and swollen. He phoned his GP who referred him to A&E. While in the ambulance he became nauseous and vomited, and his temperature was 40.1 degrees.
Day oneMr W was admitted for bed rest, pain relief and IV flucloxacillin (pain assessment was undertaken using the ward’s usual pain scoring chart and analgesic ladder). Blood cultures were sent for analysis. At this stage, cellulitis had spread from the lower gaiter region to just above his knee. Blood test results showed: White cell count (WCC): 22.3
(normal range 4–11) CRP: 175 (normal <5) D-dimer: negative Blood cultures: negative.
Day fourThere was little or no improvement after five days of IV flucloxacillin. After discussion with microbiology, it was decided to continue the antibiotic therapy. Mr W’s left leg was tender, grossly swollen and he could not weight bear. He had a duplex scan to rule out DVT and his deep venous system was patent.
Day sevenBy day seven there was still no clinical improvement, although systemic markers were starting to improve. Blisters had developed on the posterior medial aspect of his gaiter region, with necrotic tissue apparent underneath them. Necrotising fasciitis was a concern
WOUND CARE
allylamine compounds (Cox, 2002; CREST, 2005; Chlebicki and Oh, 2014). It seems that these aspects of treatment are often ignored (Cox, 1998).
Prophylactic antibiotic therapy may be beneficial in preventing recurrence of cellulitis (Jorup-Ronstrom and Britton, 1987). The PATCH trials found that following the first episode or recurrence of cellulitis of the leg, prophylactic, low-dose penicillin is an effective and cost-effective intervention at preventing subsequent attacks (Thomas et al, 2013). Patients with a high body mass index (BMI, >33), pre-existing oedema, or at least three episodes are less likely to have a response to prophylaxis than other patients (Thomas et al, 2013). It is possible that obese patients require higher therapeutic doses of penicillin than those used within the trials, and reducing chronic leg oedema is an area of prophylaxis that needs to be adequately addressed (Thomas et al, 2013).
ROLE OF THE COMMUNITY NURSE
Community nurses are ideally placed to assist people to reduce their risk of cellulitis through the following measures: Advice regarding weight loss
for people with obesity (Nazarko, 2012)
Treatment of venous ulcers through compression therapy (Wounds UK, 2016)
Referring patients with venous ulcers to the vascular teams for assessment and intervention of varicose veins (NICE, 2013)
Reducing and preventing leg oedema with compression garments if blood flow to the legs is adequate (Stalbow, 2004)
Advising patients on healthy skin care by washing and applying emollients to their legs to maintain the cutaneous barrier (Baxter and McGregor, 2001; Bianchi, 2013).
CASE STUDY
Mr W is a 57-year-old man with type 2 diabetes and a history of
oedema are risk factors (Dupuy et al, 1999; Roujeau et al, 2004; Mokni et al, 2006). Dupuy et al (1999) also found that lymphoedema, venous insufficiency and being overweight were additional risk factors. A few case series have suggested that saphenectomy might predispose a patient to cellulitis (Baddour and Bisno, 1985). It is evident that increasing numbers of adults are vulnerable to developing lower leg cellulitis in line with rising levels of obesity and the growing prevalence of lower limb oedema.
The clinical history should include an evaluation for possible sources of immunosuppression or neutropenia, such as diabetes, chronic steroid use, malignancy and the use of immunosuppressive agents, as these may predispose the patient to infection and affect clinical decision-making and duration of treatment (Bailey and Kroshinsky, 2011)
A proportion of patients who have had a first episode of cellulitis may subsequently suffer a recurrence. A selection of single-centre studies and case series suggest a recurrence rate between 8–20% per year, rising to 47% over a three-year follow-up period (Jorup-Ronstrom and Britton, 1987; Cox, 2006; Tay et al, 2015).
PREVENTION OF RECURRING CELLULITIS
Although there are no published clinical guidelines that focus on the prevention of recurrent cellulitis, there is agreement that to reduce the likelihood of recurrent episodes and long-term morbidity, leg oedema should be treated with compression, and tinea pedis, if present, with topical imidazole or
▼ Practice point
Diabetes has not been shown to be a risk factor for cellulitis in several case controlled studies (McNamara et al, 2007).
▼ Practice point
The relationship between chronic oedema and cellulitis is a vicious cycle, with each episode causing further damage to the lymphatic system and leading to increased swelling of the limb (Cox, 2006).
© 2018
Wou
nd C
are P
eople
Ltd

JCN 2018, Vol 32, No 1 45
WOUND CARE
and so after discussion with the microbiology team his antibiotic therapy was switched to IV tazocin and clindamycin. Blood results were: WCC: 9.4 CRP: 153.
Day eightA vascular nurse practitioner was now asked to review. Although Mr W’s leg was very oedematous, the acute nature of the cellulitis meant that it would be too painful to apply compression bandages. He was asked to remain on bed rest, with further review two days later.
Day 10At this point, the vascular nurse practitioner started reduced compression bandaging, as his leg was still painful. Although the cellulitis was still extensive, it was starting to recede.
Day 12Oedema was now responding to the reduced compression. The line of demarcation was also receding, and Mr W’s leg was feeling less tender. His blood results were: WCC: 10 CRP: 35.
Day 14 By day 14, Mr W’s acute cellulitis had resolved. His blood results at this stage were: WCC: 8.8 CRP: 24.
Although he still had wound and
skin care issues, i.e. necrotic tissue requiring debridement and leg oedema, he was discharged home on full compression. He was not prescribed oral antibiotics, but was to be followed up at the vascular nurse clinic in five days’ time.
Once his skin healed about four weeks after discharge, he was measured for class 2 RAL standard below-knee compression hosiery, and was to be followed up at six months.
DISCUSSION
Mr W’s raised white cell count and CRP provided baseline markers of the extent of the infection, as well as showing a useful clinical picture of systemic response to treatment, as the trend can be monitored.
It is difficult to obtain bacterio-logical proof of streptococcal causation, as there is usually no obvious focus of infection from which to obtain samples (Cox, 2002). Needle aspiration from the edge of the cellulitic area has a yield of 10–20%, as does aspiration of blister fluid (Cox, 2002). The blood cultures were negative, which was not unexpected as they often fail to identify the causative organisms in cases of cellulitis (Perl et al, 1999). However, it is useful to take them, as resistance to antimicrobial
therapy can be identified and resolved in some cases (Holzapfel et al, 1999). There is a higher rate of positive blood cultures in necrotising fasciitis (Cox, 2002).
It is reasonable to exclude the differential diagnosis of DVT using D-dimer and Duplex ultra-sonography.
Necrotising fasciitis, which may evolve from cellulitis, is particularly important to identify. Features such as blistering or superficial necrosis are suspicious and may occur in either disorder, but in isolation do not warrant surgical intervention (Cox, 2002). Marked local tenderness and increasing ‘crescendo pain’ are important indicators, along with neutrophilia
▼ Practice point
Tazocin is a combination of two antibiotics, piperacillin and tazobactam, with broad spectrum activity against an extended range of bacterial species. Piperacillin is an extended-spectrum penicillin antibiotic, but it can be destroyed by an enzyme produced by bacteria called beta lactamase. Tazobactam inhibits beta lactamase and prevents the destruction of piperacillin (British National Formulary [BNF] 2017).
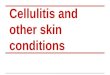
Figure 7.Cellulitis of the lower limb, as outlined in the case study.
© 2018
Wou
nd C
are P
eople
Ltd

?? JCN 2015, Vol 29, No 5
WOUND CARE
46 JCN 2018, Vol 32, No 1
(Baxter and McGregor, 2001). Emollients should be used as part of skin and wound management to help rehydrate the skin. Moist wound healing principles are usually applied to heal the remaining wounds on the leg, such as de-roofed blisters and epidermal skin loss. Clinical experience has shown that the use of zinc paste bandages applied under compression bandaging can help to soothe and rehydrate the skin and remove any remaining dry scales of skin. Monofilament debridement pads have also been found to have positive effects in removing skin scales (NICE, 2014). As persistent leg oedema can be a long-term complication, patients should be advised to wear compression garments to reduce swelling and the risk of recurring episodes of cellulitis (Cox et al, 1998).
CONCLUSION
Cellulitis is a painful and distressing condition, resulting in inpatient hospital stays. The mainstay of treatment is IV antibiotics and bed rest, followed by compression therapy in conjunction with wound and skin care. There are a growing number of adults vulnerable to developing lower leg cellulitis due to rising levels of obesity and chronic lower limb oedema. Community nurses are ideally placed to use an evidence-based approach to address risk factors such as obesity, oedema and venous disease, as well as playing a vital role in timely referrals for accurate diagnosis and treatment.
REFERENCES
Aly AA, Roberts NM, Seipol KS, MacLellan,
DG (1996) Case survey of management
of cellulitis in a tertiary teaching hospital.
Med J Aust 165: 553–6
Baddour LM, Bisno AL (1985) Non-group A
beta-haemolytic streptococcal cellulitis:
association with venous and lymphatic
compromise. Am J Med 79(2): 155–9
Bailey E, Kroshinsky D (2011) Cellulitis:
diagnosis and management. Dermatol
Ther 24(2): 229–39
Baxter H, McGregor F (2001) Understanding
and managing cellulitis. Nurs Standard
15(44): 50–6
Beasley A (2011) Management of patients
with cellulitis of the lower limb. Nurs
Standard 26(11): 50–5
Bianchi J (2013) The CHROSS Checker:
a tool kit to detect early skin
changes associated with venous and
lymphovenous disease. J Community Nurs
27(34): 43–9
Campbell SG, Burton-Macleod R, Howlett
T (2009) A cellulitis guideline at a
community hospital — we can reduce
costs by standardizing care. J Emerg
Primary Health Care 7(1): 1–12
Chlebicki MP, Oh CC (2014) Recurrent
cellulitis: risk factors, aetiology,
pathogenesis and treatment. Curr Infect
Dis Rep 16(422): 1–8
Chira S, Miller LG (2010) Staphylococcus
aureus is the most common identified
cause of cellulitis: a systematic review.
Epidemiol Infect 138: 313–7
Clinical Resource Efficiency Support Team
(2005) Guidelines on the Management
of Cellulitis in Adults. CREST, Belfast.
Available online: www.acutemed.co.uk/
docs/Cellulitis%20guidelines,%20
CREST,%2005.pdf
Cox NH, Colver GB, Paterson WD (1998)
Management and morbidity of cellulitis of
the leg. J R Soc Med 91(12): 634–7
Cox NH (2002) Management of lower leg
cellulitis. Clin Med 2(1): 23–7
Cox NH (2006) Oedema as a risk factor for
multiple episodes of cellulitis/erysipelas
of the lower leg: a series with community
follow-up. Br J Dermatol 155: 947–50
Cranendonk DR, Opmeer BC, Prins JM,
Joost Wiersinga W (2014) Comparing
short to standard duration of antibiotic
therapy for patients hospitalised with
cellulitis (DANCE): study protocol for a
randomised controlled trial. BMC Infect
Dis 14: 235–42
Curtis L (2011) Unit Costs of Health and
Social Care 2011. Personal Social Services
Research Unit, University of Kent,
Canterbury. Available online: http://tinyurl.
com/c3mxfqq (accessed 14 January, 2017)
David CV, Chira S, Eells SJ, et al (2011)
Diagnostic accuracy in patients admitted
to hospitals with cellulitis. Dermatol
Online J 17(3). Available online: www.
ncbi.nlm.nih.gov/pubmed/21426867
and hypotension, due to associated streptococcal toxic shock syndrome (Cox, 2002). Magnetic resonance imaging (MRI) scan is the most useful investigation to distinguish necrotising fasciitis, and treatment with surgical intervention is of utmost importance (Cox, 2002).
In cases of non-responsive cellulitis, it is important to involve microbiology. As there was concern with Mr W regarding necrotising fasciitis, his antibiotic regimen was changed from flucloxacillin to clindamycin and tazocin. The rationale for clindamycin in this situation is that a high bacterial density may be associated with decreased expression of penicillin-binding proteins and poor therapeutic response to penicillin, but clindamycin inhibits protein synthesis and is not affected by inoculum size (Cox, 2002).
Tinea pedis is a recognised risk factor for cellulitis, serving as a portal of entry for pathogenic bacteria (McNamara et al, 2007). Mr W had a history of tinea pedis and had been treating his feet with an antifungal preparation before this episode of cellulitis. He was thus given education about seeking prompt treatment for any further episodes of cellulitis and advised about maintaining a good skin care and hygiene regimen.
Bed rest and leg elevation are an essential aspect of treatment. Elevating the affected limb helps to reduce swelling, decrease pain and aids wound healing. The ideal position, if tolerated, is on bed with the foot positioned higher than the heart (Hofman, 1998). Active foot exercises should also be encouraged to activate the calf muscle pump, which can aid fluid movement (Hofman, 1998).
Compression therapy should be started once the infection has resolved and the patient can tolerate bandaging. The aim of care is to reduce swelling and exudate volume. As oedema reduces, the skin will change from being shiny and taut to dry and cracked, giving the appearance of ‘crazy paving’
JCN
© 2018
Wou
nd C
are P
eople
Ltd

JCN 2018, Vol 32, No 1 47
WOUND CARE
Having read this article,
Your knowledge of the signs and symptons of cellulitis
Risk factors for developing cellulitis
How to distinguish cellulitis from other conditions.
Then, upload the article to the free JCN revalidation e-portfolio as evidence of your continued learning: www.jcn.co.uk/revalidation
RevalidationAlert
Dupuy A, Benchikhi H, Roujeau JC, et al
(1999) Risk factors for erysipelas of the
leg (cellulitis): Case-control study. Br Med
J 318(7198): 1591–4
Eron LJ (2000) Infections of skin and soft
tissues: outcome of a classification
scheme.Clin Infect Dis 29: 1483–8
Eron LJ, Benjamin AL, Low DE, et al (2003)
Managing skin and soft tissue infections:
expert panel recommendations on key
decision points. J Antimicrob Chemother 52
Supplement: i3-i17
Goettsch WG, Bouwes Bavinck JN, Herings
RMC (2006) Burden of illness of bacterial
cellulitis and erysipelas of the leg in the
Netherlands. J Eur Acad Dermatol Venereol
20: 834–9
Green T (2008) Understanding body image
in patients with chronic oedema. Br J
Community Nurs 13(10): S15–S18
Hofman D (1998) Oedema and the
management of venous leg ulcers. J
Wound Care 7(7): 345–8
Holzapfel L, Jacquet-Fracillon T, Rahmani J,
et al (1999) Microbiological evaluation of
infected wounds of the extremities in 214
adults. J Accid Emerg Med 16: 32–4
Hunter M (2017) Adjustable Velcro
compression devices and management of
lower limb lymphoedema. J Community
Nurs 31(5): 20–8
Jorup-Ronstrom CJ, Britton S (1987)
Recurrent erysipelas: predisposing factors
and costs of prophylaxis. Infection
15: 105–6
Levell N, Wingfield C, Garioch J (2011)
Severe lower limb cellulitis is best
diagnosed by dermatologists and
managed with shared care between
primary and secondary care. Br J Dermatol
164: 1326–8
Marwick C, Broomhall J, McCowan C,
et al (2011) Severity assessment of
skin and soft tissue infections: cohort
study of management and outcomes
for hospitalized patients. J Antimicrob
Chemother 66: 387–97
McNamara DR, Tleyjeh IM, Berbari EF, et
al (2007) A predictive model of recurrent
lower extremity cellulitis in a population-
based cohort. Arch Internal Med 167(7): 709–15
Mokni M, Dupuy A, Denguezli M, et al
(2006) Risk factors for erysipelas of the
leg in Tunisia: A multicentre case-control
study. Dermatology 212(2): 108–12
Morris A (2003) Cellulitis and erysipelas.
Clin Evidence 9: 1804–9
National Institute for Health and Care
Excellence (2013) Varicose veins: diagnosis
and management. NICE, London. Available
online: www.nice.org.uk/guidance/cg168
(accessed 14 January, 2018)
National Institute for Health and
Care Excellence (2014) The Debrisoft
monofilament debridement pad for use in
acute or chronic wounds. NICE, London.
Available online://www.nice.org.uk/
guidance/mtg17 (accessed 22 January,
2018)
National Institute for Health and Care
Excellence (2017) Venous eczema and
lipodermatosclerosis. NICE, London.
Available online: https://cks.nice.org.uk/
venous-eczema-and-lipodermatosclerosis
#!topicsummary
Nazarko L (2012) An evidence-based
approach to diagnosis and management
of cellulitis. Br J Community Nurs 17(1):6–12
NHS Choices (2016) Contact Dermatitis. Available online: www.nhs.uk/conditions/contact-dermatitis/ (accessed 22 January, 2018)
Perl B, Gottehrer NP, Raveh D, Schlesinger
Y, Rudensky B, Yinnon AM (1999) Cost-
effectiveness of blood cultures for adult
patients with cellulitis. Clin Infect Dis
29(6): 1483–8
KEY POINTSCellulitis is an acute bacterial infection of the dermis and subcutaneous tissues.
The clinical presentation of cellulitis is similar to other conditions and diagnostic errors are common.
There are number of risk factors, which are linked to the development of cellulitis.
Community nurses are well placed to help people reduce the risk of developing cellulitis.
A proportion of patients who have had a first episode of cellulitis may subsequently suffer a recurrence. Prophylactic antibiotics may be prescribed in the long term in patients at high risk of recurrence.
Roujeau JC, Sigurgeirsson B, Korting
HC, Kerl H, Paul C (2004) Chronic
dermatomycoses of the foot as risk factors
for acute bacterial cellulitis of the leg: A
case-control study.Dermatology 209(4): 301–7
Stalbow J (2004) Preventing cellulitis in
older people with persistent lower limb
oedema. Br J Nurs 13(12): 725–32
Tan R, Newberry DJ, Arts GJ, Onwuamaegbu
ME (2007) The design, characteristics and
predictors of mortality in the North of
England Cellulitis Treatment Assessment
(NECTA). Int J Clin Practice 61(11):1889–93
Tay EY, Fook-Chong S, Oh CC,
Thirumoorthy T, Pang SM, Lee HY
(2015) Cellulitis recurrence score: A tool
for predicting recurrence of lower limb
cellulitis. J Am Acad Dermatol 72(1): 140–5
Thomas KS, Crook AM, Nunn AJ, et al
(2013) Penicillin to prevent recurrent leg
cellulitis. N Engl J Med 368(18): 1695–1703
Wingfield C (2009) Lower limb cellulitis: a
dermatological perspective. Wounds UK
5(2): 26–36
Wingfield C (2012) Diagnosing and
managing lower limb cellulitis. Nurs Times
108(27): 18–21
Wounds UK (2016) Best Practice Statement:
Holistic management of venous leg
ulceration. Wounds UK, London
© 2018
Wou
nd C
are P
eople
Ltd