Embed Size (px)
Citation preview

Diagnosis and Pathogenesis of Retinal Pigment EpithelialTears
Nisha R. Krishan, M.D., Suresh R. Chandra, M.D., and Thomas S. Stevens, M.D.
Ten cases of retinal pigment epithelial tearswere observed in eight patients with serouspigment epithelial detachments associatedwith age-related macular degeneration. Eightof the ten tears were spontaneous and alloccurred at the detachment margin. The resulting area of exposed choroid was sometimesinitially mistaken for pigment epithelial atrophy. In two cases it was misdiagnosed aschoroidal neovascularization and treated withlaser photocoagulation. All but two patientssuffered severe visual loss.
SEROUS DETACHMENT of retinal pigment epithelium, a well-recognized feature of agerelated macular degeneration,' produces suchcomplications as geographic atrophy of theoverlying retinal pigment epithelium and choroidal neovascularization.P" Another newly described complication is tearing of the retinalpigment epithelium along the detachment margin. This was first reported by Hoskin, Bird,and Sehmi' and other accounts have appearedsince then.P'" Such tears may originate spontaneously or after laser photocoagulation.t-"-"Swanson, Kalina, and Guzak" reported twocases of pigment epithelial tears after retinaldetachments and one with a chorioretinal scar.
Hoskin, Bird, and Sehmi' estimated that retinal pigment epithelial tears occur in approximately 10% of pigment epithelial detachments,and are more common than previously recognized. The infrequent recognition of such tearsmay result from their misdiagnosis as atrophyof the pigment epithelium or choroidal neovascularization.
Accepted for publication July 8, 1985.From the Department of Ophthalmology, University
of Wisconsin Medical School, Madison, Wisconsin. Thisstudy was supported in part by a grant from Research toPrevent Blindness, Inc., New York, New York.
Reprint requests to Suresh R. Chandra, M.D., ClinicalScience Center, Department of Ophthalmology, 600Highland Ave., Madison, WI 53792.
During the past two years, we have observedten cases of retinal pigment epithelial tears ineight patients with serous pigment epithelialdetachments associated with age-related macular degeneration. The area of exposed choroidwas sometimes initially mistaken for pigmentepithelial atrophy. In two cases it was misdiagnosed as choroidal neovascularization andtreated with laser photocoagulation.
Case Reports
Case 1A 77-year-old woman said she had had
blurred vision in both eyes for the past year.Her visual acuity was R.E.: 6/200 and L.E.:13/200. There were large bilateral detachmentsof the retinal pigment epithelium with tearsalong the temporal margins.
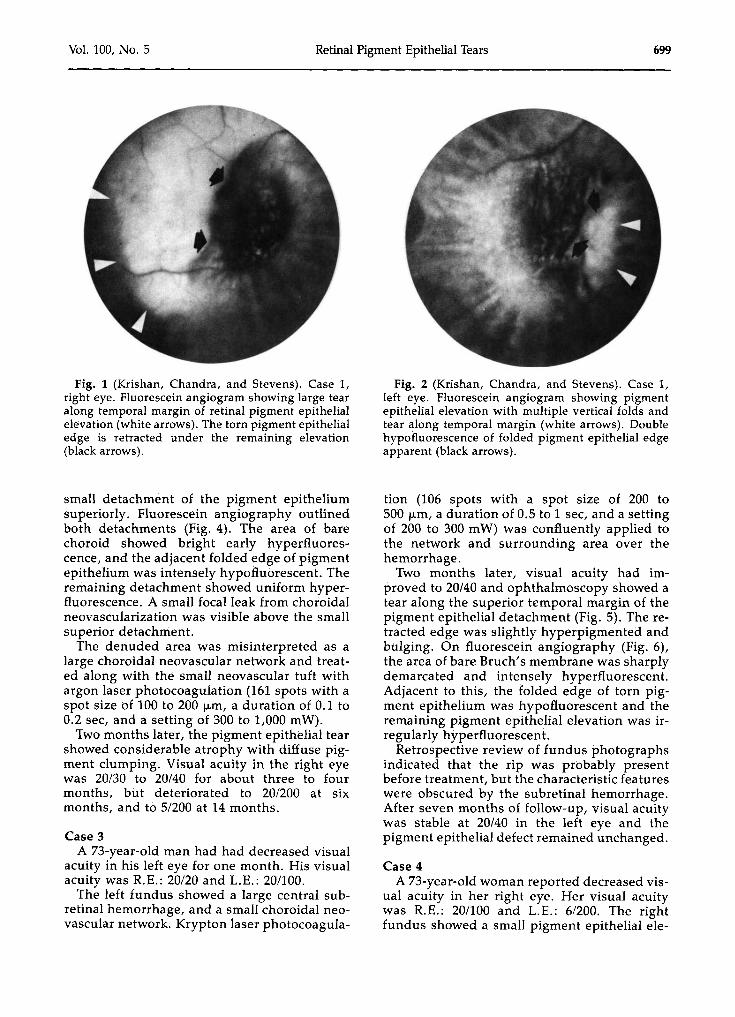
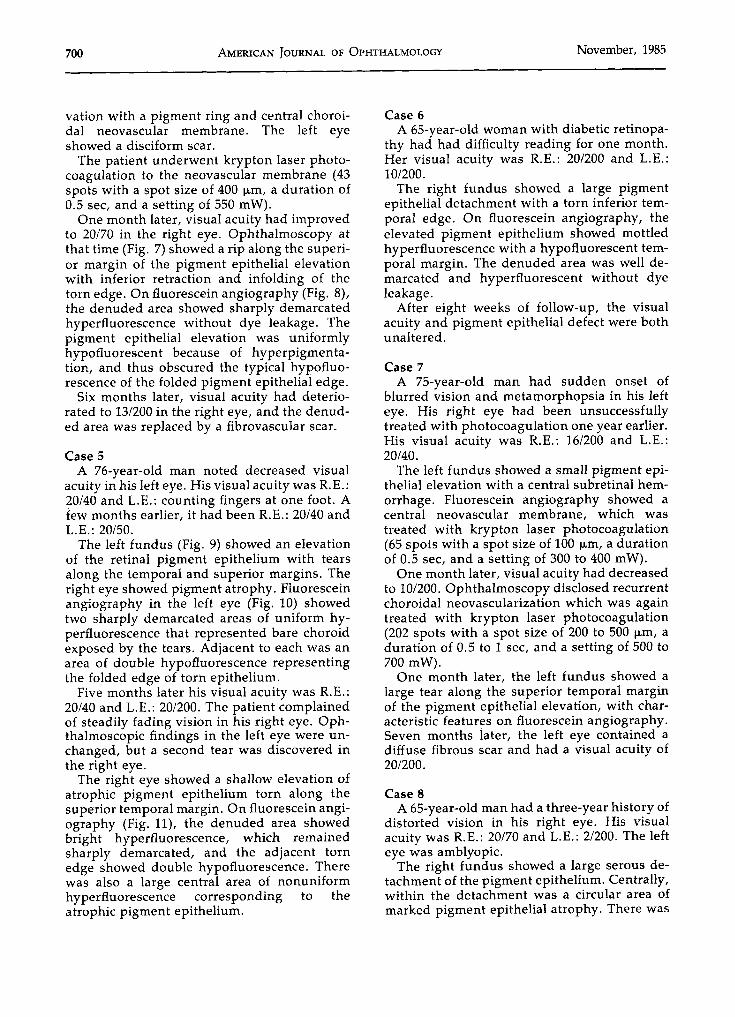
On fluorescein angiography, the pigment epithelial elevation in the right eye (Fig. 1) washypofluorescent with some central mottled hyperfluorescence secondary to pigment changes.The denuded area was sharply demarcatedand showed intense hyperfluorescence withminimal subretinal dye leakage. The temporalmargin of the pigment epithelial elevationshowed double hypofluorescence corresponding to the retracted torn edge. Tension lineswere visible as radiating bands of hypofluorescence extending from the pigment epithelialelevation. The left eye (Fig. 2) showed similarfindings except that the elevated pigment epithelium had formed a number of vertical folds.
Case 2A 62-year-old woman reported decreased vis
ual acuity, metamorphopsia, and a central scotoma in her right eye. Her visual acuity wasR.E.: 20/30 and L.E.: 20/20.
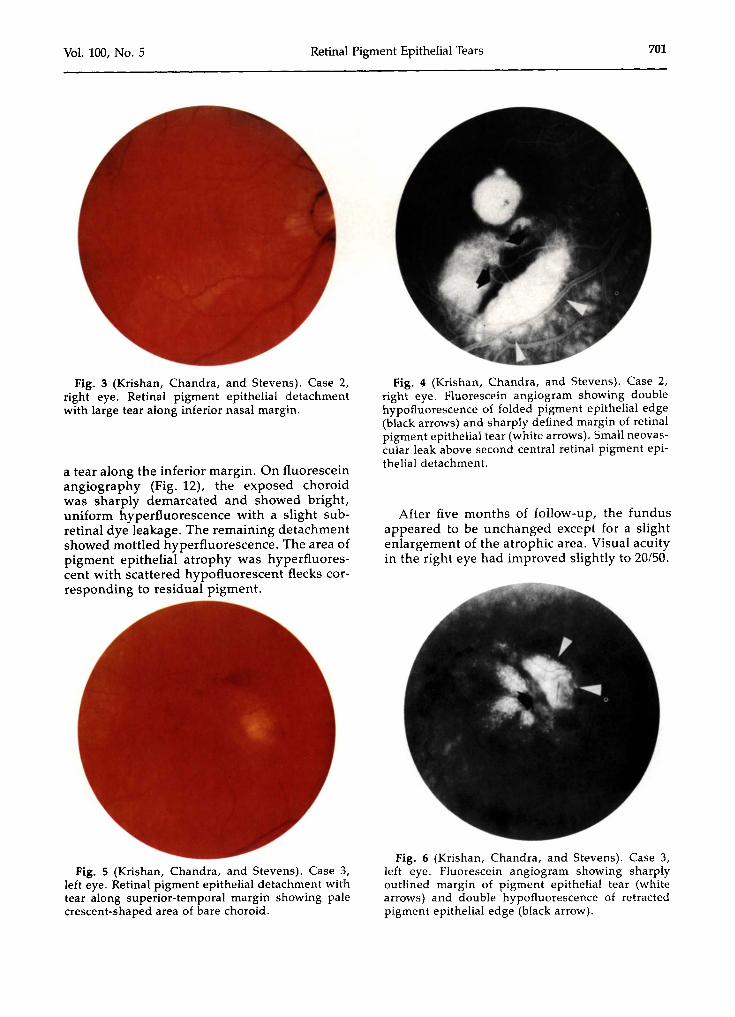
The right fundus (Fig. 3) disclosed a largepigment epithelial detachment with a tearalong the inferior margin. There was a second
698 ©AMERICAN JOURNAL OF OPHTHALMOLOGY 100:698-707, NOVEMBER, 1985
Vol. 100, No.5 Retinal Pigment Epithelial Tears 699
Fig. 1 (Krishan, Chandra, and Stevens). Case 1,right eye. Fluorescein angiogram showing large tearalong temporal margin of retinal pigment epithelialelevation (white arrows). The torn pigment epithelialedge is retracted under the remaining elevation(black arrows).
small detachment of the pigment epitheliumsuperiorly. Fluorescein angiography outlinedboth detachments (Fig. 4). The area of barechoroid showed bright early hyperfluorescence, and the adjacent folded edge of pigmentepithelium was intensely hypofluorescent. Theremaining detachment showed uniform hyperfluorescence. A small focal leak from choroidalneovascularization was visible above the smallsuperior detachment.
The denuded area was misinterpreted as alarge choroidal neovascular network and treated along with the small neovascular tuft withargon laser photocoagulation (161 spots with aspot size of 100 to 200 urn, a duration of 0.1 to0.2 sec, and a setting of 300 to 1,000 mW).
Two months later, the pigment epithelial tearshowed considerable atrophy with diffuse pigment clumping. Visual acuity in the right eyewas 20/30 to 20/40 for about three to fourmonths, but deteriorated to 20/200 at sixmonths, and to 51200 at 14 months.
Case 3A 73-year-old man had had decreased visual
acuity in his left eye for one month. His visualacuity was R.E.: 20/20 and L.E.: 20/100.
The left fundus showed a large central subretinal hemorrhage, and a small choroidal neovascular network. Krypton laser photocoagula-
Fig. 2 (Krishan, Chandra, and Stevens). Case 1,left eye. Fluorescein angiogram showing pigmentepithelial elevation with multiple vertical folds andtear along temporal margin (white arrows). Doublehypofluorescence of folded pigment epithelial edgeapparent (black arrows).
tion (106 spots with a spot size of 200 to500 urn, a duration of 0.5 to 1 sec, and a settingof 200 to 300 mW) was confluently applied tothe network and surrounding area over thehemorrhage.
Two months later, visual acuity had improved to 20/40 and ophthalmoscopy showed atear along the superior temporal margin of thepigment epithelial detachment (Fig. 5). The retracted edge was slightly hyperpigmented andbulging. On fluorescein angiography (Fig. 6),the area of bare Bruch's membrane was sharplydemarcated and intensely hyperfluorescent.Adjacent to this, the folded edge of torn pigment epithelium was hypofluorescent and theremaining pigment epithelial elevation was irregularly hyperfluorescent.
Retrospective review of fundus photographsindicated that the rip was probably presentbefore treatment, but the characteristic featureswere obscured by the subretinal hemorrhage.After seven months of follow-up, visual acuitywas stable at 20/40 in the left eye and thepigment epithelial defect remained unchanged.
Case 4A 73-year-old woman reported decreased vis
ual acuity in her right eye. Her visual acuitywas R.E.: 201100 and L.B.: 6/200. The rightfundus showed a small pigment epithelial ele-
700 AMERICAN JOURNAL OF OPHTHALMOLOGY November, 1985
vation with a pigment ring and central choroidal neovascular membrane. The left eyeshowed a disciform scar.
The patient underwent krypton laser photocoagulation to the neovascular membrane (43spots with a spot size of 400 urn, a duration of0.5 sec, and a setting of 550 mW).
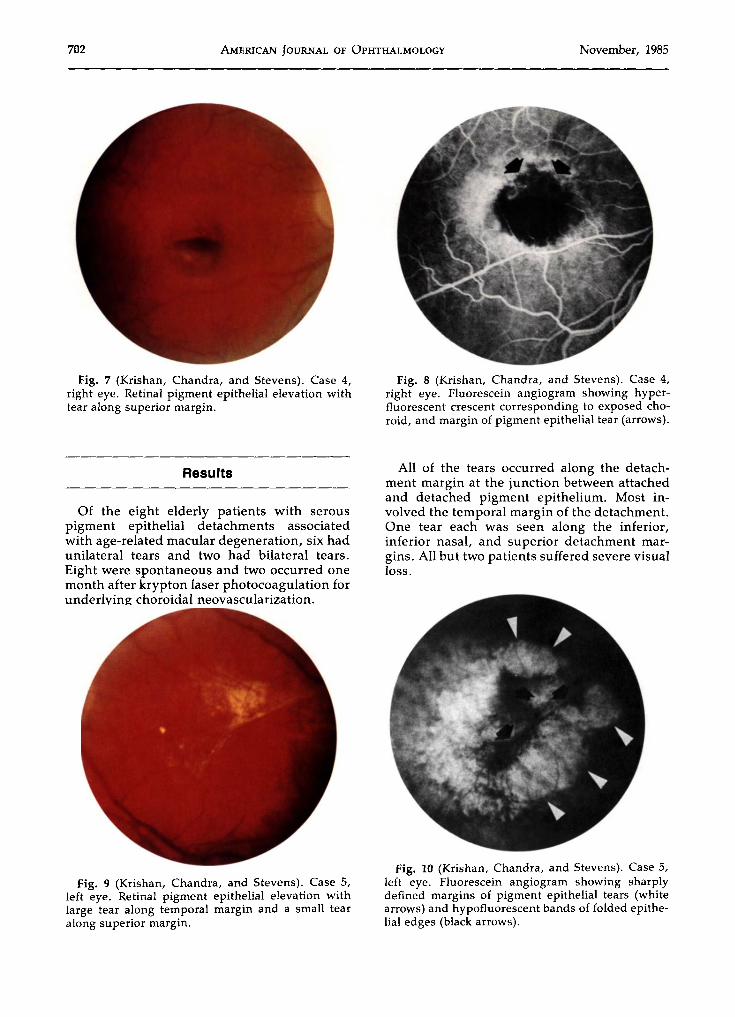
One month later, visual acuity had improvedto 20/70 in the right eye. Ophthalmoscopy atthat time (Fig. 7) showed a rip along the superior margin of the pigment epithelial elevationwith inferior retraction and infolding of thetorn edge. On fluorescein angiography (Fig. 8),the denuded area showed sharply demarcatedhyperfluorescence without dye leakage. Thepigment epithelial elevation was uniformlyhypofluorescent because of hyperpigmentation, and thus obscured the typical hypofluorescence of the folded pigment epithelial edge.
Six months later, visual acuity had deteriorated to 13/200 in the right eye, and the denuded area was replaced by a fibrovascular scar.
Case 5A 76-year-old man noted decreased visual
acuity in his left eye. His visual acuity was R.E.:20/40 and L.E.: counting fingers at one foot. Afew months earlier, it had been R.E.: 20/40 andL.E.: 20/50.
The left fundus (Fig. 9) showed an elevationof the retinal pigment epithelium with tearsalong the temporal and superior margins. Theright eye showed pigment atrophy. Fluoresceinangiography in the left eye (Fig. 10) showedtwo sharply demarcated areas of uniform hyperfluorescence that represented bare choroidexposed by the tears. Adjacent to each was anarea of double hypofluorescence representingthe folded edge of torn epithelium.
Five months later his visual acuity was R.E.:20/40 and L.E.: 20/200. The patient complainedof steadily fading vision in his right eye. Ophthalmoscopic findings in the left eye were unchanged, but a second tear was discovered inthe right eye.
The right eye showed a shallow elevation ofatrophic pigment epithelium torn along thesuperior temporal margin. On fluorescein angiography (Fig. 11), the denuded area showedbright hyperfluorescence, which remainedsharply demarcated, and the adjacent tornedge showed double hypofluorescence. Therewas also a large central area of nonuniformhyperfluorescence corresponding to theatrophic pigment epithelium.
Case 6A 65-year-old woman with diabetic retinopa
thy had had difficulty reading for one month.Her visual acuity was R.E.: 20/200 and L.E.:10/200.
The right fundus showed a large pigmentepithelial detachment with a torn inferior temporal edge. On fluorescein angiography, theelevated pigment epithelium showed mottledhyperfluorescence with a hypofluorescent temporal margin. The denuded area was well demarcated and hyperfluorescent without dyeleakage.
After eight weeks of follow-up, the visualacuity and pigment epithelial defect were bothunaltered.
Case 7A 75-year-old man had sudden onset of
blurred vision and metamorphopsia in his lefteye. His right eye had been unsuccessfullytreated with photocoagulation one year earlier.His visual acuity was R.E.: 16/200 and L.B.:20/40.
The left fundus showed a small pigment epithelial elevation with a central subretinal hemorrhage. Fluorescein angiography showed acentral neovascular membrane, which wastreated with krypton laser photocoagulation(65 spots with a spot size of 100 urn, a durationof 0.5 sec, and a setting of 300 to 400 mW).
One month later, visual acuity had decreasedto 10/200. Ophthalmoscopy disclosed recurrentchoroidal neovascularization which was againtreated with krypton laser photocoagulation(202 spots with a spot size of 200 to 500 urn, aduration of 0.5 to 1 sec, and a setting of 500 to700 mW).
One month later, the left fundus showed alarge tear along the superior temporal marginof the pigment epithelial elevation, with characteristic features on fluorescein angiography.Seven months later, the left eye contained adiffuse fibrous scar and had a visual acuity of20/200.
Case 8A 65-year-old man had a three-year history of
distorted vision in his right eye. His visualacuity was R.E.: 20/70 and L.E.: 2/200. The lefteye was amblyopic.
The right fundus showed a large serous detachment of the pigment epithelium. Centrally,within the detachment was a circular area ofmarked pigment epithelial atrophy. There was
Vol. 100, No.5 Retinal Pigment Epithelial Tears 701
Fig. 3 (Krishan, Chandra, and Stevens). Case 2,right eye. Retinal pigment epithelial detachmentwith large tear along inferior nasal margin.
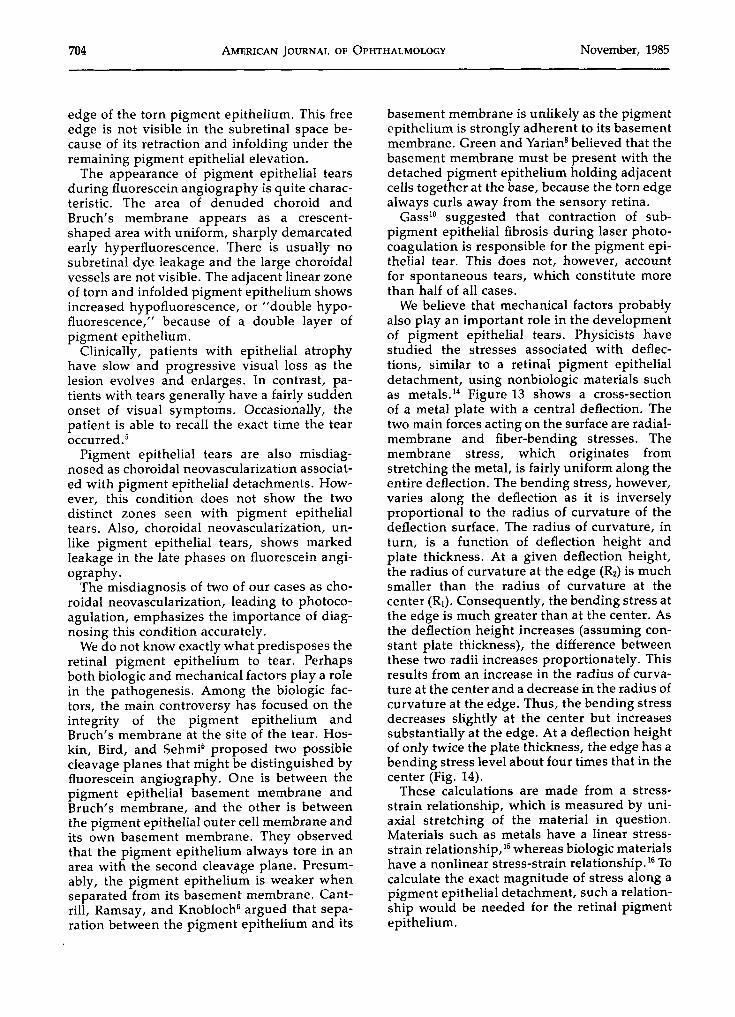
a tear along the inferior margin. On fluoresceinangiography (Fig. 12), the exposed choroidwas sharply demarcated and showed bright,uniform hyperfluorescence with a slight subretinal dye leakage. The remaining detachmentshowed mottled hyperfluorescence. The area ofpigment epithelial atrophy was hyperfluorescent with scattered hypofluorescent flecks corresponding to residual pigment.
Fig. 5 (Krishan, Chandra, and Stevens). Case 3,left eye. Retinal pigment epithelial detachment withtear along superior-temporal margin showing palecrescent-shaped area of bare choroid.
Fig. 4 (Krishan, Chandra, and Stevens). Case 2,right eye. Fluorescein angiogram showing doublehypofluorescence of folded pigment epithelial edge(black arrows) and sharply defined margin of retinalpigment epithelial tear (white arrows). Small neovascular leak above second central retinal pigment epithelial detachment.
After five months of follow-up, the fundusappeared to be unchanged except for a slightenlargement of the atrophic area. Visual acuityin the right eye had improved slightly to 20/50.
Fig. 6 (Krishan, Chandra, and Stevens). Case 3,left eye. Fluorescein angiogram showing sharplyoutlined margin of pigment epithelial tear (whitearrows) and double hypofluorescence of retractedpigment epithelial edge (black arrow).
702 AMERICAN JOURNAL OF OPHTHALMOLOGY November, 1985
Fig. 7 (Krishan, Chandra, and Stevens). Case 4,right eye. Retinal pigment epithelial elevation withtear along superior margin.
Results
Of the eight elderly patients with serouspigment epithelial detachments associatedwith age-related macular degeneration, six hadunilateral tears and two had bilateral tears.Eight were spontaneous and two occurred onemonth after krypton laser photocoagulation forunderlying choroidal neovascularization.
Fig. 9 (Krishan, Chandra, and Stevens). Case 5,left eye. Retinal pigment epithelial elevation withlarge tear along temporal margin and a small tearalong superior margin.
Fig. 8 (Krishan, Chandra, and Stevens). Case 4,right eye. Fluorescein angiogram showing hyperfluorescent crescent corresponding to exposed choroid, and margin of pigment epithelial tear (arrows).
All of the tears occurred along the detachment margin at the junction between attachedand detached pigment epithelium. Most involved the temporal margin of the detachment.One tear each was seen along the inferior,inferior nasal, and superior detachment margins. All but two patients suffered severe visualloss.
Fig. 10 (Krishan, Chandra, and Stevens). Case 5,left eye. Fluorescein angiogram showing sharplydefined margins of pigment epithelial tears (whitearrows) and hypofluorescent bands of folded epithelial edges (black arrows).
Vol. 100, No.5 Retinal Pigment Epithelial Tears 703
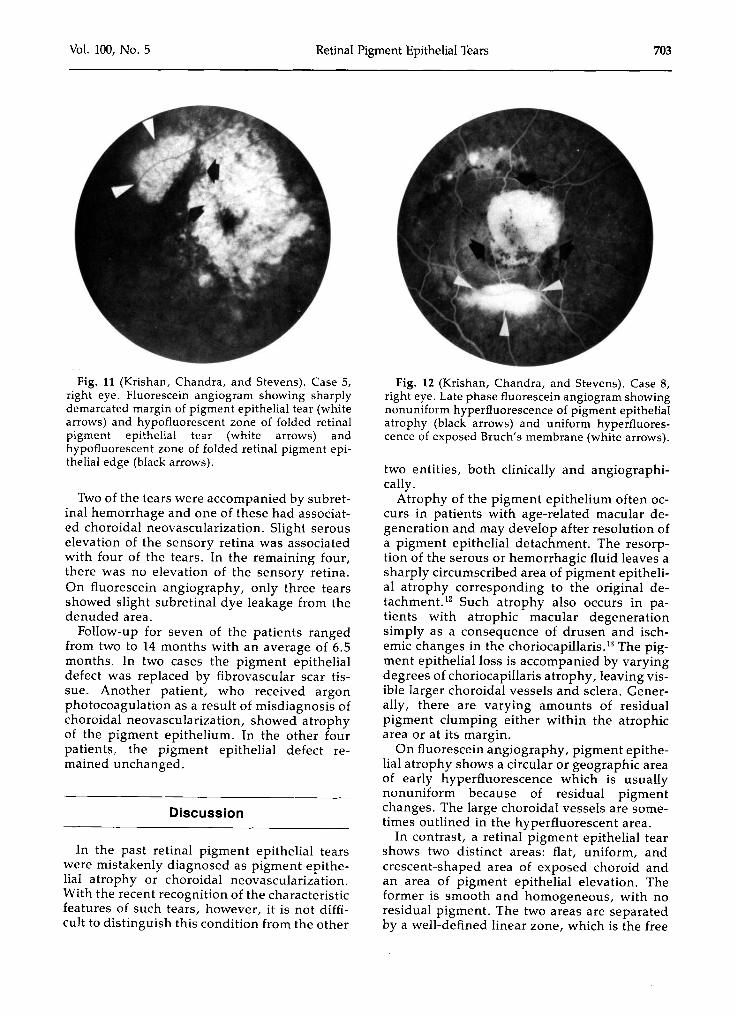
Fig. 11 (Krishan, Chandra, and Stevens). Case 5,right eye. Fluorescein angiogram showing sharplydemarcated margin of pigment epithelial tear (whitearrows) and hypofluorescent zone of folded retinalpigment epithelial tear (white arrows) andhypofluorescent zone of folded retinal pigment epithelial edge (black arrows).
Two of the tears were accompanied by subretinal hemorrhage and one of these had associated choroidal neovascularization. Slight serouselevation of the sensory retina was associatedwith four of the tears. In the remaining four,there was no elevation of the sensory retina.On fluorescein angiography, only three tearsshowed slight subretinal dye leakage from thedenuded area.
Follow-up for seven of the patients rangedfrom two to 14 months with an average of 6.5months. In two cases the pigment epithelialdefect was replaced by fibrovascular scar tissue. Another patient, who received argonphotocoagulation as a result of misdiagnosis ofchoroidal neovascularization, showed atrophyof the pigment epithelium. In the other fourpatients, the pigment epithelial defect remained unchanged.
Discussion
In the past retinal pigment epithelial tearswere mistakenly diagnosed as pigment epithelial atrophy or choroidal neovascularization.With the recent recognition of the characteristicfeatures of such tears, however, it is not difficult to distinguish this condition from the other
Fig. 12 (Krishan, Chandra, and Stevens). Case 8,right eye. Late phase fluorescein angiogram showingnonuniform hyperfluorescence of pigment epithelialatrophy (black arrows) and uniform hyperfluorescence of exposed Bruch's membrane (white arrows).
two entities, both clinically and angiographically.
Atrophy of the pigment epithelium often occurs in patients with age-related macular degeneration and may develop after resolution ofa pigment epithelial detachment. The resorption of the serous or hemorrhagic fluid leaves asharply circumscribed area of pigment epithelial atrophy corresponding to the original detachment. 12 Such atrophy also occurs in patients with atrophic macular degenerationsimply as a consequence of drusen and ischemic changes in the choriocapillaris." The pigment epithelial loss is accompanied by varyingdegrees of choriocapillaris atrophy, leaving visible larger choroidal vessels and sclera. Generally, there are varying amounts of residualpigment clumping either within the atrophicarea or at its margin.
On fluorescein angiography, pigment epithelial atrophy shows a circular or geographic areaof early hyperfluorescence which is usuallynonuniform because of residual pigmentchanges. The large choroidal vessels are sometimes outlined in the hyperfluorescent area.
In contrast, a retinal pigment epithelial tearshows two distinct areas: flat, uniform, andcrescent-shaped area of exposed choroid andan area of pigment epithelial elevation. Theformer is smooth and homogeneous, with noresidual pigment. The two areas are separatedby a well-defined linear zone, which is the free
704 AMERICAN JOURNAL OF OPHTHALMOLOGY November, 1985
edge of the torn pigment epithelium. This freeedge is not visible in the subretinal space because of its retraction and infolding under theremaining pigment epithelial elevation.
The appearance of pigment epithelial tearsduring fluorescein angiography is quite characteristic. The area of denuded choroid andBruch's membrane appears as a crescentshaped area with uniform, sharply demarcatedearly hyperfluorescence. There is usually nosubretinal dye leakage and the large choroidalvessels are not visible. The adjacent linear zoneof torn and infolded pigment epithelium showsincreased hypofluorescence, or "double hypofluorescence," because of a double layer ofpigment epithelium.
Clinically, patients with epithelial atrophyhave slow and progressive visual loss as thelesion evolves and enlarges. In contrast, patients with tears generally have a fairly suddenonset of visual symptoms. Occasionally, thepatient is able to recall the exact time the tearoccurred.'
Pigment epithelial tears are also misdiagnosed as choroidal neovascularization associated with pigment epithelial detachments. However, this condition does not show the twodistinct zones seen with pigment epithelialtears. Also, choroidal neovascularization, unlike pigment epithelial tears, shows markedleakage in the late phases on fluorescein angiography.
The misdiagnosis of two of our cases as choroidal neovascularization, leading to photocoagulation, emphasizes the importance of diagnosing this condition accurately.
We do not know exactly what predisposes theretinal pigment epithelium to tear. Perhapsboth biologic and mechanical factors playa rolein the pathogenesis. Among the biologic factors, the main controversy has focused on theintegrity of the pigment epithelium andBruch's membrane at the site of the tear. Hoskin, Bird, and Sehmi" proposed two possiblecleavage planes that might be distinguished byfluorescein angiography. One is between thepigment epithelial basement membrane andBruch's membrane, and the other is betweenthe pigment epithelial outer cell membrane andits own basement membrane. They observedthat the pigment epithelium always tore in anarea with the second cleavage plane. Presumably, the pigment epithelium is weaker whenseparated from its basement membrane. Cantrill, Ramsay, and Knobloch" argued that separation between the pigment epithelium and its
basement membrane is unlikely as the pigmentepithelium is strongly adherent to its basementmembrane. Green and Yarian" believed that thebasement membrane must be present with thedetached pigment epithelium holding adjacentcells together at the base, because the torn edgealways curls away from the sensory retina.
Gass" suggested that contraction of subpigment epithelial fibrosis during laser photocoagulation is responsible for the pigment epithelial tear. This does not, however, accountfor spontaneous tears, which constitute morethan half of all cases.
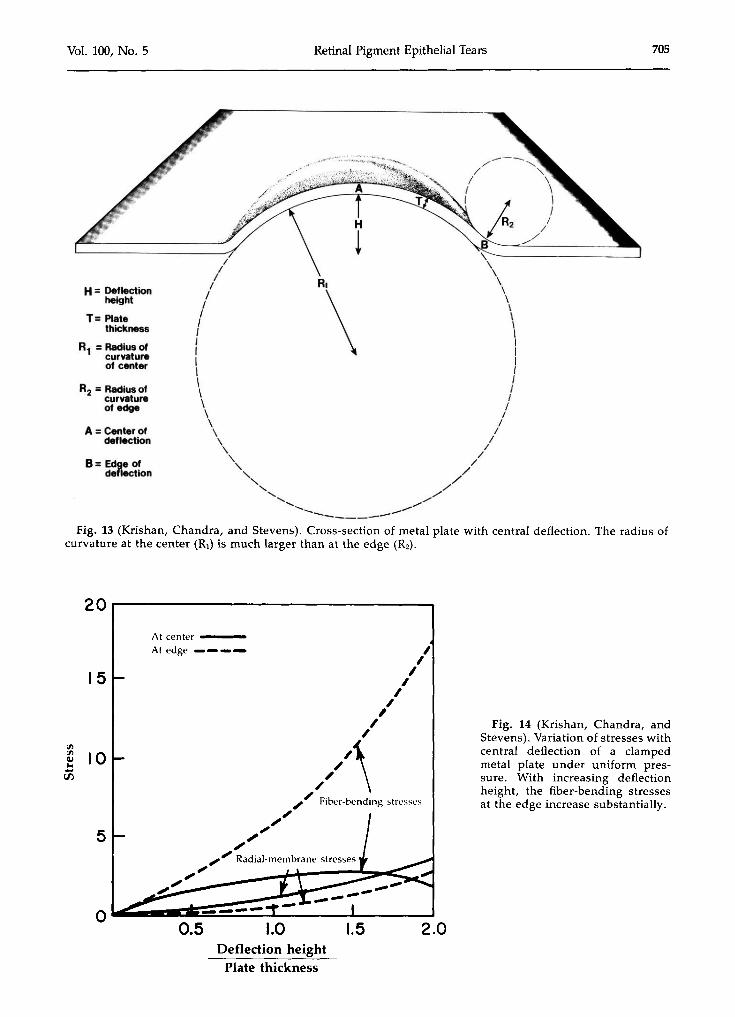
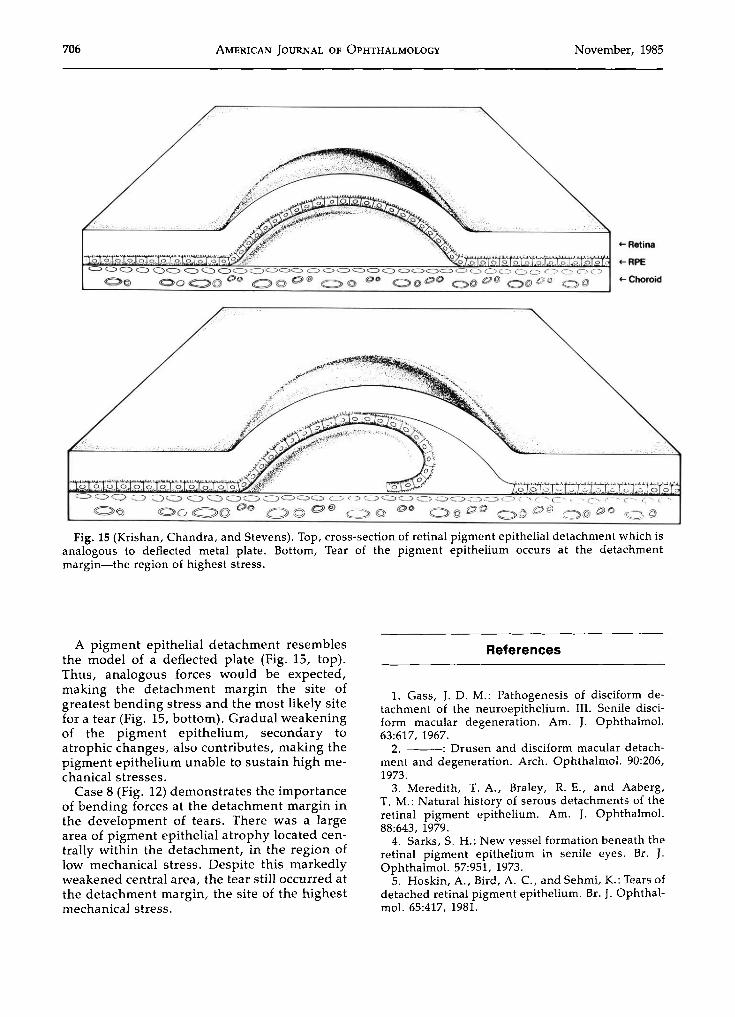
We believe that mechanical factors probablyalso play an important role in the developmentof pigment epithelial tears. Physicists havestudied the stresses associated with deflections, similar to a retinal pigment epithelialdetachment, using nonbiologic materials suchas metals." Figure 13 shows a cross-sectionof a metal plate with a central deflection. Thetwo main forces acting on the surface are radialmembrane and fiber-bending stresses. Themembrane stress, which originates fromstretching the metal, is fairly uniform along theentire deflection. The bending stress, however,varies along the deflection as it is inverselyproportional to the radius of curvature of thedeflection surface. The radius of curvature, inturn, is a function of deflection height andplate thickness. At a given deflection height,the radius of curvature at the edge (R2) is muchsmaller than the radius of curvature at thecenter (R I ) . Consequently, the bending stress atthe edge is much greater than at the center. Asthe deflection height increases (assuming constant plate thickness), the difference betweenthese two radii increases proportionately. Thisresults from an increase in the radius of curvature at the center and a decrease in the radius ofcurvature at the edge. Thus, the bending stressdecreases slightly at the center but increasessubstantially at the edge. At a deflection heightof only twice the plate thickness, the edge has abending stress level about four times that in thecenter (Fig. 14).
These calculations are made from a stressstrain relationship, which is measured by uniaxial stretching of the material in question.Materials such as metals have a linear stressstrain relationship, 15 whereas biologic materialshave a nonlinear stress-strain relationship. 16 Tocalculate the exact magnitude of stress along apigment epithelial detachment, such a relationship would be needed for the retinal pigmentepithelium.
Vol. 100, No.5 Retinal Pigment Epithelial Tears 705
B= Edge ofdeflection
A =Center ofdeflection
R2 = Radius ofcurvatureof edge
H= Deflectionheight
T= Platethickness
R1 = Radius ofcurvatureof center
'---------------17 \-------------'/ \
/ \
( "\ \\I II I\ I\ I\ I\ I\ I\ /\ /
\ /\, //
" /-. //, //"~ ~/
........-- ---~-----Fig. 13 (Krishan, Chandra, and Stevens). Cross-section of metal plate with central deflection. The radius of
curvature at the center (R1) is much larger than at the edge (R2) .
20,..----------------,
Fig. 14 (Krishan, Chandra, andStevens). Variation of stresses withcentral deflection of a clampedmetal plate under uniform pressure. With increasing deflectionheight, the fiber-bending stressesat the edge increase substantially.
2.01.50.5 1.0Deflection height
Plate thickness
,I
II,,,
I,
./'\,,/ Fiber-bending stresses
.,tI'"tI'.,". '" Radial-membrane stresses
"'''.~ -:t;--=:::~~X::",,"
At center ----At edge _
5
15
706 AMERICAN JOURNAL OF OPHTHALMOLOGY November, 1985
+- Retina
+-RPE
+-Choroid
Fig. 15 (Krishan, Chandra, and Stevens). Top, cross-section of retinal pigment epithelial detachment which isanalogous to deflected metal plate. Bottom, Tear of the pigment epithelium occurs at the detachmentmargin-the region of highest stress.
A pigment epithelial detachment resemblesthe model of a deflected plate (Fig. 15, top).Thus, analogous forces would be expected,making the detachment margin the site ofgreatest bending stress and the most likely sitefor a tear (Fig. IS, bottom). Gradual weakeningof the pigment epithelium, secondary toatrophic changes, also contributes, making thepigment epithelium unable to sustain high mechanical stresses.
Case 8 (Fig. 12) demonstrates the importanceof bending forces at the detachment margin inthe development of tears. There was a largearea of pigment epithelial atrophy located centrally within the detachment, in the region oflow mechanical stress. Despite this markedlyweakened central area, the tear still occurred atthe detachment margin, the site of the highestmechanical stress.
References
1. Gass, J. D. M.: Pathogenesis of disciform detachment of the neuroepithelium. III. Senile disciform macular degeneration. Am. J. Ophthalmol.63:617, 1967.
2. ---: Drusen and disciform macular detachment and degeneration. Arch. Ophthalmol. 90:206,1973.
3. Meredith, T. A., Braley, R. E., and Aaberg,T. M.: Natural history of serous detachments of theretinal pigment epithelium. Am. J. Ophthalmol.88:643, 1979.
4. Sarks, S. H.: New vessel formation beneath theretinal pigment epithelium in senile eyes. Br. J.Ophthalmol. 57:951, 1973.
5. Hoskin, A., Bird, A. C.; and Sehrni, K.: Tears ofdetached retinal pigment epithelium. Br. J. Ophthalmol. 65:417, 1981.
Vol. 100, No.5 Retinal Pigment Epithelial Tears 707
6. Cantrill, H. L., Ramsay, R. C.; and Knobloch,W. H.: Rips in the pigment epithelium. Arch. Ophthalmol. 101:1074, 1983.
7. Decker, W. L., Sanborn, G. E., Ridley, M.,Annesley, W. H., and Sorr, E. M.: Retinal pigmentepithelial tears. Ophthalmology 90:507, 1983.
8. Green, S. N., and Yarian, D.: Acute tear ofretinal pigment epithelium. Retina 3:16, 1983.
9. Bird, A. C.; and Sehmi, K. S.: Tears of detachedretinal pigment epithelium. Trans. New OrleansAcad. Ophthalmol., 1983, p. 317.
10. Gass, J. D. M.: Retinal pigment epithelial ripduring krypton red laser photocoagulation. Am. J.Ophthalmol. 98:700, 1984.
11. The Moorfields Macular Study Group: Retinalpigment epithelial detachments in the elderly. A
controlled trial of argon laser photocoagulation. Br.J. Ophthalmol. 66:1, 1982.
12. Swanson, D. E., Kalina, R. E., and Guzak,S. V.: Tears of retinal pigment epithelium. Occurrence in retinal detachments and a chorioretinal scar.Retina 4:115, 1984.
13. Blair, C. J.: Geographic atrophy of retinal pigment epithelium. A manifestation of senile maculardegeneration. Arch. Ophthalmol. 93:19, 1975.
14. Chia, C. Y.: Nonlinear Analyses of Plates.New York, McGraw-Hill, 1980, pp. 112-117.
15. Timoshenko, S.: Strength of Materials, Part 1.Elementary Theory and Problems, 2nd ed. NewYork, D. Van Nostrand, 1940, pp. 1-7.
16. Fung, Y. c.: On pseudo-elasticity of livingtissues. Mechanics Today 5:49, 1980.








![$PQZSJHIU …ousar.lib.okayama-u.ac.jp/files/public/5/56175/...rhages, retinal pigment epithelial tears, and/or chorio-capillaris atrophy [9-11]. The risk of serious complica-tions](https://img.pdfslide.net/doc/110x75/5e274ba9c8f801547e287b2d/pqzsjhiu-ousarlibokayama-uacjpfilespublic556175-rhages-retinal-pigment.jpg)




















![Hydrogen Sulfide Protects Retinal Pigment Epithelial Cells from … · 2020. 8. 20. · human retinal pigment epithelial cell inflammation by inhi-biting ROS formation [12], but](https://img.pdfslide.net/doc/110x75/60dbb5335e46af67e64b77cb/hydrogen-sulfide-protects-retinal-pigment-epithelial-cells-from-2020-8-20-human.jpg)