8/13/2019 Diagnosis of Type 2 Diabetes at an Older Age.pdf
2/3
privation category (12) (an area-basedmeasure of material
deprivation).
RESULTS There were 3,594 peoplewith type 2 diabetes (48% male)
and7,188 matched comparators identied inthe study. Subject survival
is presentedseparately for men and women in Fig. 1.Over a mean
follow-up period of 4.6 2.9 years, 909 (25.3%) patients in the
di-abetic cohort and 1,651 (23.0%) in thenondiabetic cohortdied.
Formen, therel-ative risk for mortality in the diabetic co-hort
compared with the nondiabeticcohort, adjusted for deprivation,
was1.06(95% CI 0.941.19). There were no dif-
ferences when patients were stratied byageat diagnosis.
Forwomen, theadjustedrelative risk for mortality in the
diabetic
cohort compared with the nondiabeticcohort was 1.29 (1.151.45).
The risksfor those diagnosed with diabetes at6574 years, 7584
years, and 85 yearswere 1.47 (1.211.78), 1.15 (0.971.38), and 1.36
(1.061.73), respec-tively. Cardiovascular deaths accountedfor 49.4%
of the deaths in people withdiabetes and 45.2% in those without
(ad- justed relative risk 1.01 [0.931.10]).
CONCLUSIONS In th is s tudy,men diagnosed with type 2 diabetes
after
65 years of age had no increased risk of mortality compared with
nondiabeticmen of the same age. This result contrastssharply with
the signicant effect of dia-betes on mortality in a population of
olderdiabetic people that included newly diag-nosed individuals and
those with a longerduration of disease (5). Studies that havefound
small differences in mortality, evenin men diagnosed at a later
age, have notadjusted for the confounding effect of de-privation
(possibly independently associ-ated with diabetes prevalence [13]
andmortality).
Our data came from a validated dia-betes system and are known to
be reliable(9). The mean follow-up of almost 5 yearswas similar to
that of an Italian study (7).It may be that mortality of diabetic
andnondiabetic men diverges in later years
after diagnosis, although this did not oc-cur for at least 7
years following diagnosisin our study. A weakness of the study
wasthat we were unable to adjust for cardio-vascular risk factors
at baseline. However,we might expect a poorer prole in thediabetic
cohort (14,15), with adjustmentresulting in even less of a
difference be-tween the two cohorts. The proportion of
cardiovascular deaths was relatively low;however, we used
underlying cause of death to determine whether a death hada
cardiovascular cause, and this may un-derestimate cardiovascular
mortality. Wealso acknowledge that there may be a de-greeof
under-ascertainmentof diabetes inthe nondiabetic cohort.
Our result may be due to a survivoreffect, with men with more
severe diabe-tes having presented and died before theage of 65
years. However, this does notdetract from the important clinical
point:that the effects of diabetes (in this case,mortality) in
those diagnosed at an olderage clearly differs markedly from
thosediagnosed when younger.
In contrast to men, women diagnosed
with type2 diabetesat an older age had anincreased risk of
mortality compared witholder nondiabetic women. This was evi-dent 3
years after diagnosis, particularlyfor women aged 6574 years.
Diabetesmay be a stronger risk factor for womencompared with men
(as our results sug-gest), although whether this can be ac-counted
for by a higher prevalence of classic cardiovascular risk factors
in dia-betic women compared with diabeticmen is still controversial
(16). We wereunable to adjust for cardiovascular risk
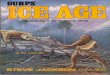
Figure 1 Kaplan-Meier survival curves of older female ( top )
and male ( bottom ) individualswith type 2 diabetes and their
nondiabetic comparators during 19932002.
Diabetes diagnosis in older individuals
2798 DIABETES CARE, VOLUME 27, NUMBER 12, DECEMBER 2004
8/13/2019 Diagnosis of Type 2 Diabetes at an Older Age.pdf
3/3
factors, but our study suggests that theeffects of diabetes may
vary according tosex, even in older individuals.
This study therefore highlights theimportance of recognizing the
heteroge-neity of the older diabetic population.
Acknowledgments The authors thankmembers of the DARTS/MEMO
Collaborationand members of the DARTS Steering Groupfor their
support.
References1. Waugh NR, Dallas JH, Jung RT, Newton
RW: Mortality in a cohort of diabetic pa-tients: causesand
relative risks. Diabetolo- gia 32:103104, 1989
2. Stengard JH, Tuomilehto J, Pekkanen J,Kivinen P, Kaarsalo E,
Nissinen A, Kar-
vonen MJ: Diabetes mellitus, impairedglucose tolerance
andmortalityamong el-derly men: the Finnish cohorts of theSeven
Countries Study. Diabetologia 35:760765, 1992
3. Katakura M, Naka M, Kondo T, Nishii N,Komatsu M, Sato Y,
Yamauchi K, Hira-matsu K, Ikeda M, Aizawa T, HashizumeK:
Prospective analysis of mortality, mor-bidity, and risk factors in
elderly diabeticsubjects: Nagano Study. Diabetes Care26:
638644, 20034. Panzram G: Mortality and survival in type
2 (non-insulin-dependent) diabetes mel-litus. Diabetologia
30:123131, 1987
5. Croxson SCM, Price DE, Burden M, Jag-gerC, BurdenAC:
Themortality of elderlypeople withdiabetes. Diabet Med11:250
252, 19946. Roper NA, Bilous RW, Kelly WF, UnwinNC, Connolly VM:
Excess mortality in apopulation with diabetes and the impactof
material deprivation: longitudinal,population based study. BMJ
322:13891393, 2001
7. Muggeo M, Verlato G, Bonora E, BressanF, Girotto S,
Corbellini M, Gemma ML,Moghetti P, Zenere M, Cacciatori V, et
al:The Verona diabetes study: a population-based survey on known
diabetes mellitusprevalence and 5-year all-cause
mortality.Diabetologia 38:318325, 1995
8. Panzram G, Zabel-Langhennig: Prognosis
of diabetes mellitus in a geographicallydened population.
Diabetologia 20:587591, 1981
9. Morris AD, Boyle DI, MacAlpine R,Emslie-Smith A, Jung RT,
Newton RW,MacDonald TM: The diabetes audit andresearch in Tayside
Scotland (DARTS)study: electronic record-linkage to createa
diabetes register. BMJ 315:524528,1997
10. World Health Organization: Manual of the
International Statistical Classicationof Dis-ease, Injuries and
Causes of Death: NinthRevision. Geneva, World Health Org.,1978
11. World Health Organization: InternationalStatistical
Classication of Diseases and Re-lated Health Problems: Tenth
Revision. Ge-
neva, World Health Org.,199412. Carstairs V: Deprivation and
health inScotland. Health Bull (Edinb)48:162175,1990
13. Evans JMM, Newton RW, Ruta DA, Mac-Donald TM, Morris AD:
Socio-economicstatus, obesity and prevalence of type 1and type 2
diabetes mellitus. Diabet Med17:478 480, 2000
14. Laakso M, Ronnemaa T, Pyora la K, Kallio V, Puukka P,
Penttila I: Atheroscleroticvascular disease and its risk factors
innon-insulin-dependent diabetic and non-diabetic subjects in
Finland. Diabetes Care11:449 463, 1988
15. Serrano Rios M, Martinez Larrad MT: Hy-pertension in type 2
diabetes mellitus. InCardiovascular Risk in Type 2 Diabetes.Hancu
N, Ed. Berlin, Springer-Verlag,2003, p. 63 84
16. Kanaya AM, Grady D, Barrett-Connor E:Explaining the sex
difference in coronaryheart disease mortality among patientswith
type 2 diabetes mellitus. Arch InternMed 162:17371745, 2002
Tan and Associates
DIABETES CARE, VOLUME 27, NUMBER 12, DECEMBER 2004 2799