Embed Size (px)
Citation preview


The Dental Chart
• Is a record of current status of teeth
• Aids treatment planning
• Facilitates third party communication
• Is a medicolegal requirement
• May be used for forensic purposes
How to start my diagnoses :
*It’s very important to know how to diagnose a case to do your treatment plane .
*You should clean and dry the teeth before diagnosing it for caries .
*sometimes you need to send your patient to home and give him OHI to
diagnose him in another visit ,if he has a bad oral hygiene.
*if the patient is having a pain , treat the pain, then send your patient to home (
treating a pain is more important than doing you diagnoses ).
*good lightning is essential .
*use the probe to remove debris .
* some use the probe for staining fissure , if the probe stick in the fissure then it’s
caries , but this is not 100% true ,as sometimes the probe stick because it’s very
short .( so using the probe to detect caries is something objective ) .

Diagnosis of dental caries :
*it’s very hard to detect early lesion .
*you have to follow the sequence of detecting caries every time, to establish
routine , so you will make sure you don’t miss any thing ..
*The sequence of caries detecting is :
From the upper right 8 to the upper left 8 then lower left 8 to the lower right 8 .
* it’s hard to diagnose incipient caries ( early lesion ) especially staining fissure (
you can’t know if it’s staining or arrested caries or active caries) also it’s hard to
diagnose occlusal caries, proximal caries ( needs bitwing most of the time ) and
root caries .
*Use your clinical judgment to assess the need for ordering radiographs , and you
need to answer some question for that ?
> why I need this radiograph ?
> what it the thing I want to diagnose ?
> or why I don’t want to take a radiograph ?
* don’t use a radiograph if it’s not going to be useful in your diagnosis , for ex :
with irreversible pulpitis .
*we use our clinical finding ,history ,and vitality testing to judge if it’s reversible or
irreversible pulpitis ,but not radiograph .

So as we said , use the mirror and the probe to examine the teeth ,following the
sequence , use the probe only to remove debris , and to feel if the dentins is soft
or not , but don’t push the probe in a stained fissure as it might be an arrested
caries and you break the mineralized enamel around it .
*it’s also difficult to differentiate between calculus and caries , as the calculus
may be green ,brown or reddish .
What to look for :
1.cavitaion
2.chalkiness (enamel chalkiness is a sign of early caries )
3. Brown/ blue/grey Discoloration
* those 3 points are the most important points to differentiate between caries and other lesion .
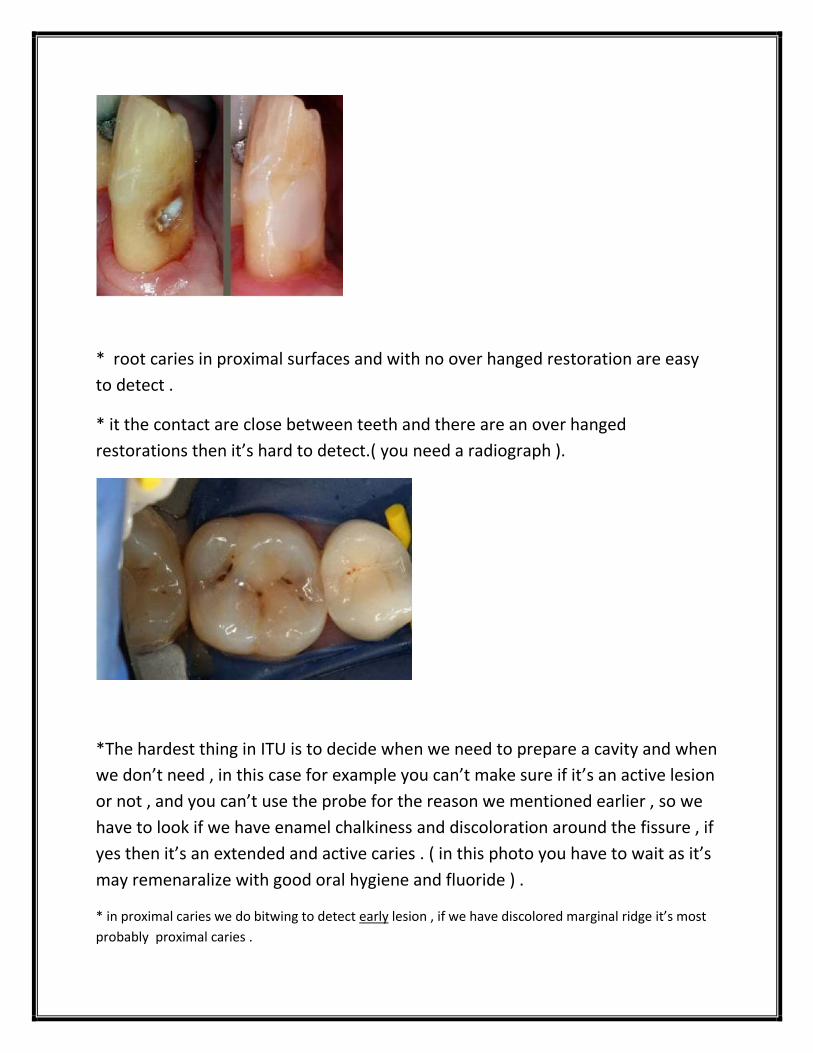
* root caries in proximal surfaces and with no over hanged restoration are easy
to detect .
* it the contact are close between teeth and there are an over hanged
restorations then it’s hard to detect.( you need a radiograph ).
*The hardest thing in ITU is to decide when we need to prepare a cavity and when
we don’t need , in this case for example you can’t make sure if it’s an active lesion
or not , and you can’t use the probe for the reason we mentioned earlier , so we
have to look if we have enamel chalkiness and discoloration around the fissure , if
yes then it’s an extended and active caries . ( in this photo you have to wait as it’s
may remenaralize with good oral hygiene and fluoride ) .
* in proximal caries we do bitwing to detect early lesion , if we have discolored marginal ridge it’s most
probably proximal caries .

We are not using this classification.
*some conditions resemble caries , you have to be able to distinguish between them ,like : abfraction .
*abfraction is a newly used term (1990) it used to be diagnosed as abrasion from a tooth brush.

* now , caries come with chalkiness ,discoloration , broken enamel and a soft
dentin , while abfraction no chalkiness , the enamel still contact with a shiny
surface and a hard dentin .
* abfraction happens to patient with bruxism which will break enamel down at
the cervical region .
Abfraction
* it’s advisable to ask the patient if he has pain when he eats sweet or cold water ,
then you can conclude that the dentin is exposed .
Examination of restoration :
You examine restoration to decide if it’s good or needs repair or replacement .
We look for :
• overhanging restorations ( usually we look at the margins )
• Marginal fit ( margin between restoration and the tooth )
• Fracture
• Contact relationship

• Marginal ridge height
• Recurrent caries ( we know it when the dentin is soft and exposed )
• Esthetics
* you need bitwing for class 2 to detect recurrent carries and overhang.
note 1 : if the caries reach < ½ enamel then it’s insipient and will remenaralise
with good oral hygiene and fluoride, if it reaches more than ½ you have to do
restoration .
note 2 : radiograph is not helpful except when the caries reach the dentinoenaml
junction .
note 3 : buccal surface in amalgam class 2 restoration normally discolored with
time ( enamel not chalky , no undermined enamel so it’s normal )
note 4 : when we have a composite restoration in the posterior teeth ( class 2 )
look for the margins , we might have marginal gap , as the saliva make the etching
hard at the proximal surface .
note 5 : we use ( I? ) for early lesion in charting ,when not exactly knowing what is
the case , so dentist in conz will judge if it needs to be prepared or not .

over hanged , needs to be replaced .
broken restoration and recurrent caries .
composite here is inadequate ,should be at
the same level of the adjacent tooth , and maybe it’s discoloration .
marginal gap .

Tooth wear :
Attrition ( resulted from contact between teeth ( bruxism ))
Abrasion ( contact between teeth and another material )
Erosion ( contact between teeth and acidic material(mostly) or chemical )
Abfraction ( buccal surface usually ,resulted from occlusal forces )
Abfraction
and as we said there is a debate if it’s abfraction or abrasion
from tooth brush .
erosion
Caused by:
1. Regurgitation ( also called GERD (Gastroesophageal reflux disease ) , ARD(acid
reflux disease) ,vomiting ).
2. bolymia : patients who keep slim and induce vomiting ( so erosion on
the palatal surface ,usually upper teeth as the lower is protected by
the tongue ).
3. Soda drinking .
4. Acidic fruits ( lemon )

At attrition the lower teeth don’t reach the free gingival margin ,so make
the patient bite and check .
Attrition :
Happens on the opposing tooth also ,as it’s due to contact between two teeth.

Examination of occlousion :
We don’t do this in ITU but we do it in ortho.
• Overbite (upper incisors should overlap the
lower incisors by one third of their crown)
• Overjet (normal 2-3mm)
• Angle's molar relation classification:
Class I [normal]:
Class II [disto-occlusion]
Class III [mesio-occlusion]
• Note if there is crossbite or open bite .
Dental chart : Use symbols to record clinical findings and ,past dental treatments
implants is not here , because it wasn’t as frequently used as now .

Let’s take this example :
We have unurapted 3molar ,remaining root 7 ,crown 6 ,crown 5 ,remaining root and
filling 4,crown 3( etc …)
A it’s for artificial tooth , but not necessary an implant .
Examination of Edentulous or Partially Edentulous Ridge:
• Note degree of resorption
• Note the presence of any retained roots
• Assess prognosis of remaining teeth (extraction ,restoration ,or keep it as abutment )
• Assess treatment needs:
• Pt may require advanced periodontal treatment (prophylaxes for gingivitis , periodontal
treatment for periodontitis) or extractions prior to the construction of :
– Partial denture ( if some teeth is good and could be used as abutment)
OR
– Complete denture ( all the teeth are bad and clearance is needed)
Diagnosis : from clinical & radiological findings
A:provisional diagnosis :
in some cases you can’t make a definitive diagnosis ,for example if your patient is
having a systematic disease and you are waiting the lab test for it , so you make a
provisional diagnosis until the lab test result appear . (based on clinical impression)

b: Differential diagnoses: two or more possible diagnoses
*If unable to make a definitive diagnosis seek consultation or refer the patient
Treatment plan :
*it’s better to treatment plan as phases ( phase 1 ,phase 2 …..etc)
*treatment plan may need adjustment , as it’s influenced by :
1. Patient age
2. Patient health
3. prognosis
4. Expectation : if the patient has a badly carious teeth and you recommend
extraction for it but the patient doesn’t want to extract it ,so you adjust
your treatment plan ,and tell the patient that the teeth will only stay for 2
years and it’s your responsibility.
Chief complain is better to be done at the first phase ( but not always ),it depends on the case you are
dealing with :

Example1 :if a patient come for doing bleaching teeth (whitening ) ,but you find
that the patient has periodontal disease and caries ,so you delay her chief
complain to another phase , as treating pain is a priority .
Example 2 : if the patient wedding is next week ,so doing bleaching is a priority
and should be done at the first phase .
*So the treatment plan phases are not Compulsory , you can adjust them
depending on the case.
Ex3 : if the patient has pulpitis you do only pulp excavation at phase 1 and not
RCT( only remove pain at phase 1 ) .
Ex4 : extraction for 3rd molar if it’s impacted or partially erupted is not a priority
and it’s done at phase 2 ,but if the tooth has pericoronitis and pain , you extract it
at phase 1 , as it’s now linked to relieving symptoms and pain. (periapical
radiograph is used to diagnose 3rd molar ).
*phase 3 is to restore function and esthetics ( crown ,bridge ,denture
,replacement of composite restoration …..etc )
Phase 4 for maintenance and recall ( fluoride supplement depends on the patient
need ) .
* its important not to go from treatment to another irregularly, it’s not logic to
put a crown on a carious teeth , treat the caries first then put the crown .
*some dentist prefer there interest than the patient need , for example they do
implants for a heavy smoker although it’s not allowed .

*periapical radiograph to diagnose an impacted tooth , if the tooth is going to
erupt you leave it , if not you surgically extract it .
Done by : amr sadi



![Ankylosed permanent teeth: incidence, etiology and ... · probably due to tongue thrusting [23]. Alternatively, supra-eruption of opposing teeth might occur. Diagnosis Overall, the](https://img.pdfslide.net/doc/110x75/5e230360f3eb8d36a1454f20/ankylosed-permanent-teeth-incidence-etiology-and-probably-due-to-tongue-thrusting.jpg)






![ChronicPeriodontalDiseaseMayInfluencethePulpSensitivity ...This diagnosis was based on the cri-teria described by Flemmig [13]. Only teeth with no signs of caries, restoration, attrition,](https://img.pdfslide.net/doc/110x75/60b680ab449259717075469f/chronicperiodontaldiseasemayiniuencethepulpsensitivity-this-diagnosis-was.jpg)


















