Embed Size (px)
Citation preview

Diagnosis and management of acute deep vein
thrombosis a joint consensus document from
the European society of cardiology working
groups of aorta and peripheral vascular diseases
and pulmonary circulation and right ventricular
function
Lucia Mazzolai1 Victor Aboyans2 Walter Ageno3 Giancarlo Agnelli4
Adriano Alatri1 Rupert Bauersachs56 Marjolein PA Brekelmans7 Harry R Buller7
Antoine Elias8 Dominique Farge9 Stavros Konstantinides610 Gualtiero Palareti11
Paolo Prandoni12 Marc Righini13 Adam Torbicki14 Charalambos Vlachopoulos15
and Marianne Brodmann16
1Division of Angiology Heart and Vessel Department Lausanne University Hospital Ch du Mont-Paisible 18 1011 Lausanne Switzerland 2Department of CardiologyDupuytren University Hospital and Inserm 1098 Tropical Neuroepidemiology School of Medicine 2 avenue martin Luther-King 87042 Limoges cedex France 3Departmentof Clinical and Experimental Medicine University of Insubria Via Ravasi 2 21100 Varese Italy 4Internal and Cardiovascular Medicine - Stroke Unit University of Perugia SAndrea delle Fratte 06156 Perugia Italy 5Department of Vascular Medicine Klinikum Darmstadt GmbH Grafenstraszlige 9 64283 Darmstadt Germany 6Center for Thrombosisand Hemostasis University Medical Center Mainz Langenbeckstr 1 55131 Mainz Germany 7Department of Vascular Medicine Academic Medical Center Meibergdreef 91105 AZ Amsterdam The Netherlands 8Cardiology and Vascular Medicine Toulon Hospital Centre 54 Rue Henri Sainte-Claire Deville 83100 Toulon France 9AssistancePublique-Hopitaux de Paris Saint-Louis Hospital Internal Medicine and Vascular Disease Unit and Groupe Francophone on Thrombosis and Cancer Paris 7 DiderotUniversity Sorbonne Paris Cite 1 Avenue Claude Vellefaux 75010 Paris France 10Department of Cardiology Democritus University of Thrace Greece 11CardiovascularDiseases University of Bologna Via Albertoni 15 40138 Bologna Italy 12Department of Cardiovascular Sciences Vascular Medicine Unit University of Padua Via NicoloGiustiniani 2 35121 Padua Italy 13Division of Angiology and Hemostasis Department of Medical Specialties Geneva University Hospital Rue Gabrielle Perret-Gentil 41205 Geneva Switzerland 14Department of Pulmonary Circulation and Thromboembolic Diseases Medical Center for Postgraduate Education ul Plocka 26 01-138Warszawa Otwock Poland 15Department of Cardiology Athens Medical School Profiti elia 24 14575 Athens Greece and 16Division of Angiology Medical UniversityGraz Graz Austria
Received 18 July 2016 revised 4 November 2016 editorial decision 30 December 2016 accepted 9 January 2017
Introduction
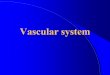
Venous thromboembolism (VTE) incidence increases sharply withage (Figure 1) and appears steady over the last 25 years despite pre-ventive strategies1 Women are more often affected at younger agesthis ratio reverses in the elderly2 Incidence is similar in Blacks butlower in Asians3 Almost two-thirds of VTE cases are isolated deepvein thromboses (DVTs) and 80 are proximal4
Recent European population studies reported DVT incidence of70ndash140 cases100000 person-year5
Deep vein thrombosis are mostly secondary to predisposing fac-tors common with pulmonary embolism (PE) (webtable 1)6 Distal(below knee) DVTs are more frequently related to transient situ-ations while proximal ones to chronic conditions7 In 25ndash50 of firstDVT episodes no predisposing factor is identified
In patients with DVT without PE short-term mortality ratesof 2ndash5 were reported more frequent in proximal than distalDVT7 Recurrence risk is high especially within first 6months8
Early- and mid-term complications include thrombosis extensionand PE and DVT recurrence (see Supplementary material onlineonly section)
The opinions expressed in this article are not necessarily those of the Editors of the European Heart Journal or of the European Society of Cardiology
Corresponding author Tel thorn41 21 3140750 Fax thorn 41 21 3140761 Email luciamazzolaichuvch
Published on behalf of the European Society of Cardiology All rights reserved VC The Author 2017 For permissions please email journalspermissionsoupcom
Corresponding author Tel thorn41 21 3140750 Fax thorn 41 21 3140761
Email luciamazzolaichuvch
European Heart Journal (2017) 00 1ndash14 CURRENT OPINIONdoi101093eurheartjehx003
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Long-term complications include post-thrombotic syn-drome (PTS) defined as chronic venous symptoms andorsigns secondary to DVT It represents the most frequentchronic DVT complication occurring in 30ndash50 of patientswithin 2 years after proximal DVT9 In 5ndash10 of cases PTS issevere9 Previous ipsilateral DVT proximal location (ilio-fem-oral gt popliteal) and residual veins obstruction are most sig-nificant PTS risk factors Obesity and poor INR control during
the first 3-months treatment are additional independent riskfactors10
Villalta score is used for PTS diagnosis and treatment evaluation(Table 1)11
Diagnosis
Deep vein thrombosis withoutpulmonary embolism symptomsClinical signs and symptoms are highly variable and unspecific but re-main the cornerstone of diagnostic strategy Symptoms include painswelling increased skin veins visibility erythema and cyanosis accom-panied by unexplained fever
Probability assessment and D-dimertestingPre-test probability assessment is the first step in the diagnostic algo-rithm of DVT suspicion (Figure 2) Sensitivity and specificity of clinicalsymptoms are low when considered individually however theircombination using prediction rules allows pre-test clinical probabil-ity classification into two- (DVT unlikely or likely) or three-categories(low- intermediate- or high-clinical probability) corresponding toincreasing disease prevalence1213 Wells score has been widely vali-dated and can be applied both to out- and inpatients (Table 2) Theexpertsrsquo panel favours the modified two-level pre-test probability asit is more straightforward14
Normal D-dimers render DVT unlikely15 however D-dimers havelow specificity Quantitative ELISA or ELISA-derived assays (gt95sensitivity) allow ruling out DVT in patients with DVT lsquounlikelyrsquoNegative ELISA D-dimer can exclude DVT without further testing in30 of patients16 with 3-month thromboembolic risk lt1 withouttreatment13 Quantitative latex-derived and whole-blood agglutin-ation assay have lower sensitivity (85ndash90)17 In patients with lsquolikelyrsquo
Figure 1 Venous thromboembolism incidence according to age group
Table 1 Villalta score11
Symptoms and
Clinical signs
None Mild Moderate Severe
Symptoms
Pain 0 points 1 points 2 points 3 points
Cramps 0 points 1 points 2 points 3 points
Haeviness 0 points 1 points 2 points 3 points
Paresthesia 0 points 1 points 2 points 3 points
Pruritus 0 points 1 points 2 points 3 points
Clinical signs
Pretibial edema 0 points 1 points 2 points 3 points
Skin induration 0 points 1 points 2 points 3 points
Hyperpigmentation 0 points 1 points 2 points 3 points
Redness 0 points 1 points 2 points 3 points
Venous ectasia 0 points 1 points 2 points 3 points
Pain on calf
compression
0 points 1 points 2 points 3 points
Venous ulcer Absent Present
Points are summed into a total score (range 0ndash33) Post Thrombotic syndrome(PTS) is defined by a total score of gt_5 or the presence of a venous ulcer PTS isclassified as mild if Villalta score is 5ndash9 moderate if 10ndash14 and severe if gt_15 orvenous ulcer is present
2 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
DVT D-Dimer testing is not necessary imaging is requiredTherapeutic anticoagulation should be initiated if not contraindi-cated in patients with DVT lsquolikelyrsquo until imaging
Imaging
Venous ultrasound (VUS) is the first line DVT imaging modality(other imaging see Supplementary material online only section) It isbased on B-mode combined or not with color-Doppler US andpower imaging techniques DVT diagnostic criteria are cross-sectional vein incompressibility direct thrombus imaging with veinenlargement and abnormal spectral and color-Doppler flow VUScan be performed by examining popliteal and common femoral veinsonly [2-point2-region compression venous ultrasonography (CUS)or limited CUS] or by extended imaging of inferior vena cava iliacand femoral veins and calf veins (whole-leg VUS or complete VUS)There are controversies as to whether explore symptomatic legonly or both1819
In clinically suspected DVT VUS provides overall sensitivity of942 for proximal and 635 for isolated distal DVT with an overallspecificity of 93820 Combination with color-Doppler US increasessensitivity but lowers specificity20 When DVT is suspected (withoutPE symptoms) anticoagulation may be safely withheld in patientswith a single normal complete VUS Same is true for limited CUS pro-vided it can be repeated and integrated within a diagnostic strategy
including clinical probability and D-dimer assessment21 Overall 3-month VTE incidence rate after negative complete VUS is 05722
but both methods are reported to be equivalent in randomized tri-als2324 Complete VUS may be helpful to explain patientrsquos complaintby providing up to 42 alternative diagnosis25 Point-of care US per-formed by emergency physicians using limited CUS has shown goodperformance (961 sensitivity 968 specificity)26 and may be usefulif vascular laboratories are not available 247 provided its integrationin a validated diagnostic strategy27
In patients with clinically suspected recurrent DVT comparison oftest results with baseline imaging at discontinuation of anticoagulationcan safely rule out diagnosis of recurrence28 A 2- or 4-mm29ndash31 in-crease in vein diameter between two measurements at the commonfemoral and popliteal veins after full compression is the most vali-dated US criterion
Deep vein thrombosis with pulmonaryembolism symptomsDiagnostic approach is described in corresponding 2014 EuropeanSociety of Cardiology (ESC) Guidelines6 Proximal DVT confirmationin a normotensive patient with suspected PE essentially confirms VTEand justifies anticoagulation as after formal PE diagnosis In unstable pa-tients with right ventricular overload but no possibility to confirm PECUS showing proximal DVT facilitates initiation of reperfusion
Lower limb DVT suspicion
Clinical probability assessement (2-level modified Wells score)
DVT unlikely DVT likely
D-Dimers
Negative Positive Complete venous US
No DVT Proximal DVT
Treatment At least 3-months AC DOACs in non cancer patients if no contraindications
3-months evaluation Venous US riskbenefit complianceand patientrsquos preference
Stop anticoagulation Extended AC Yearly evaluation
Isolated distal DVT
High risk recurrence Low risk recurrence
No treatment Treatment 3-months AC
Treatment or surveillance 4-6 wk AC (full or lower dose) or venous US surveillance
Figure 2 Proposed deep vein thrombosis diagnostic and management algorithm AC anticoagulation DOAC direct oral anticoagulant
Diagnosis and management of acute DVT 3
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
therapy CUS diagnostic yield is high in the presence of clinical DVTsigns32 Among unselected PE patients proximal DVT at CUS is foundin 17 patients33 Proximal DVT has high specificity and may justifytreatment even if pulmonary CT is negative6 While negative CUS can-not exclude PE it can justify withholding anticoagulation in patientswith non-diagnostic ventilationperfusion scan and PE-unlikely163435
In symptomatic patients with isolated sub-segmental PE or inciden-tal asymptomatic PE concomitant DVT justifies anticoagulation3637
Deep vein thrombosis imaging may also be useful if secondarily a pa-tient is suspected of VTE recurrence with DVT signs Moreoverpresence of concomitant DVT has been suggested as an independent30-days death risk factor following PE38
Consensus statement diagnosisbull Clinical prediction rule (two-level modified Wells score) is recom-
mended to stratify patients with suspected lower limb DVTbull ELISA D-dimer measurement is recommended in lsquounlikelyrsquo clinical
probability patients to exclude DVTbull Venous US is recommended as first line imaging method for DVT
diagnosisbull Venous CT scan should be reserved to selected patients onlybull Venous US should be proposed also in case of confirmed PE for
initial reference venous imaging useful in case of DVT recurrencesuspicion or further stratification in selected patients
bull Venous US may be considered for further stratification in selectedpatients with concomitant suspected PE
Initial (first 5ndash21 days) and long-term (first 3ndash6 months) phasemanagement
Deep vein thrombosis withoutpulmonary embolismAnticoagulation in non-cancer patients
Deep vein thrombosis treatment consists of three phases (Figure 3)39
Initial treatment (5ndash21 days following diagnosis) during this period pa-tients receive either parenteral therapy and are transited to vitamin K an-tagonists (VKA) or use high-dose direct oral anticoagulants (DOACs)Long-term treatment (following 3ndash6 months) patients are treated withVKA or DOACs39 Initial and long-term treatments are mandatory forall DVT patients Decision of extended treatment (beyond first 3ndash6months) is based on benefitrisk balance of continued anticoagulation
Initial treatment(first 5-21 days)
Long term treatment
(first 3-6 months)
Extended treatment
(following initial 3-6 months)
Apixaban 10 mg bid for 7 days Apixaban 5mg bid Apixaban 25mg bid beyond 6 months
Dabigatran 150 mg bid preceded by LMWH for 5-10 days
Edoxaban 60 mg od (30mg od if ClCreat 50-30ltmlmin or concomitant potent P-P inhibitors) preceded by LMWH for 5-10 days
Rivaroxaban 15 mg bid for 21 days Rivaroxaban 20mg od Rivaroxaban 10 mg or 20 mg od beyond 6 months
VKA to achieve INR 2-3 preceded by LMWH for 5-10 days
Figure 3 Deep vein thrombosis treatment phases ClCreat creatinine clearance LMWH low molecular weight heparin P-P inhibitors protonpump inhibitors VKA vitamin K antantagonist
Table 2 The Wells score1213
Clinical variable Points
Active cancer (treatment ongoing or within previous 6
months or palliative)
thorn1
Paralysis paresis or recent plaster immobilization of
the lower extremities
thorn1
Recently bedridden for 3 days or more or major sur-
gery within the previous 12 weeks requiring general
or regional anesthesia
thorn1
Localized tenderness along the distribution of the deep
venous system
thorn1
Entire leg swelling thorn1
Calf swelling at least 3 cm larger than that on the
asymptomatic leg (measured 10 cm below the tibial
tuberosity)
thorn1
Pitting edema confined to the symptomatic leg thorn1
Collateral superficial veins (non varicose) thorn1
Previously documented DVT thorn1
Alternative diagnosis at least as likely as DVT -2
Three-level Wells score
Low lt1
Intermediate 1ndash2
High gt2
Two-level Wells score
Unlikely lt_1
Likely gt_2
4 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
In patients with severe renal failure (creatinine clearance lt30
mLmin) unstable renal function or high bleeding risk iv unfrac-tionated heparin (UFH) may be preferable (short half-life and pro-tamine sulfate reversibility) Less solid is the evidence in favor ofUFH in obese (BMI gt40 kgm2) and underweight patients (lt50 kg)Main disadvantage of UFH is its inter-individual dose variabilityrequiring laboratory monitoring and dose adjustment AdditionallyUFH is associated with high risk of heparin-induced thrombocyto-penia For these reasons low-molecular weight heparin (LMWH)is the parenteral treatment of choice LMWHs are at least as effect-ive as UFH and probably safer40 Fondaparinux can also be used asparenteral agent41 Both LMWH and fondaparinux do not havespecific antidote
Recently DOACs have emerged as valid options for DVT treat-ment39 Dabigatran and edoxaban were studied following initial 7ndash9days treatment with a parenteral agent Apixaban and rivaroxabanwere evaluated by the lsquosingle drug approachrsquo (Figure 3)
DOACs have longer elimination half-lives than UFH or LMWHand may accumulate in patients with suboptimal renal (creatinineclearance lt30 mLmin) or hepatic function (Child-Pugh class B or C)Patients with poor renal andor hepatic function pregnancylactationthrombocytopenia were excluded from Phase III studies Patientswith active cancer were scarcely represented (3ndash8 of entire studypopulation)
DOACs are at least as effective as and probably safer than paren-teral drugVKA treatment42 A meta-analysis (27023 patients)showed similar VTE recurrence rates in patients receiving DOACsor conventional therapy (20 vs 22 RR 090) Major bleeding (RR061) fatal bleeding (RR 036) intracranial bleeding (RR 037) andclinically relevant non-major bleeding (RR 073) were significantlylower in DOACs-treated patients42 DOACs reversal agents arebeing investigated Idarucizumab (Dabigatran reversal agent) is cur-rently available for clinical use4344
Thrombolysisthrombectomy
Early clot removal may prevent at least partly PTS developement45
Catheter-directed thrombolysis (CDT) is more efficient than sys-temic lysis mainly due to less bleeding as thrombolytic agent is directlyadministered within the clot Three major randomized controlled trialscompared different CDT modalities on top of anticoagulation andcompression with a control group (anticoagulation and compressiononly) The CAVENT trial included 209 patients with first-time acuteDVT (iliac common femoral andor upper femoral vein)46 AdjuvantCDT was associated with a 26 RR PTS reduction over 2 years (411vs 556 P = 004) compared with anticoagulation alone46 Amount ofresidual post-CDT thrombus correlated with venous patency rates at24-months (P = 004) Persistence of venous patency at 6 and 24months correlated with PTS freedom (P lt 0001) A 32 of patientshad major bleed but there were no intracranial bleeds or deathsOverall trial found no differences in long-term (2 years) quality of lifebetween patients with- or without CDT Results have been confirmedafter 5 years follow-up47
Mechanical thrombus removal alone is not successful and needsadjuvant thrombolytic therapy In PEARL I and II studies only 5 ofpatients were treated without thrombolytics48
Up to 83 of patients treated by any catheter-based therapy needadjunctive angioplasty and stenting49 Primary acute DVT stenting isnot recommended due to lack of data
Vena cava filter
Vena cava filter may be used when anticoagulation is absolutely contra-indicated in patients with newly diagnosed proximal DVT One majorcomplication is filter thrombosis Therefore anticoagulation should bestarted as soon as contraindications resolve50 and retrievable filter rap-idly removed Filter placement in addition to anticoagulation does notimprove survival5152 except in patients with hemodynamically unstablePE or after thrombolytic therapy53 Increased DVT recurrence hasbeen shown with permanent51 but not with retrievable filters52
Compression
Goal of compression is to relieve venous symptoms and eventuallyprevent PTS54
Elastic compression stockings efficacy has been challenged by theSOX trial55 A total of 806 patients with proximal DVT have beenrandomized to either 30ndash40 mmHg or placebo (lt5 mmHg) stock-ings Cumulative 2 years PTS incidence was similar (526 vs 523HR= 10) No difference in PTS severity or quality-of-life was observ-ed55 However compliance definition (stockings wearing for gt_3 daysweek) was significantly lower than in previous studies (56vs90)56 Although role of stockings in PTS prevention may be un-certain their use remains a reasonable option for controlling symp-toms of acute proximal DVT57
Compression associated with early mobilization and walking exer-cise has shown significant efficacy in venous symptom relieve in pa-tients with acute DVT58 Caution should be used in patients withsevere peripheral artery disease
Home vs in-hospital management
Most patients with DVT may be treated on a home basis (seeSupplementary material online only section)
Deep vein thrombosis with pulmonaryembolismManagement of patients with acute PE is described in the 2014 ESCguideline6 (summary in the see Supplementary material online onlysection)
Isolated distal deep vein thrombosisWhether isolated distal DVT should be treated with anticoagulationis still debated A recent trial randomized patients with a first isolateddistal DVT to LMWH or placebo for 42 days59 Rate of symptomaticproximal DVT or PE at 42 days was not different between LMWHand placebo (33 vs 54) major or clinically relevant non-majorbleeding occurred more frequently in the LMWH group (5 vs 0P = 003) These data seem to support that not all isolated distal DVTshould receive full-dose anticoagulation
Approach is to anticoagulate full-dose for at least 3 months as forproximal DVTs patients at high-risk VTE (Table 3)60 Shorter LMWHtreatment (4ndash6 weeks) even at lower doses or ultrasound surveil-lance could be effective and safe in low-risk patients (Table 3)61 Nodata are available on DOACs All patients with acute isolated distal
Diagnosis and management of acute DVT 5
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
DVT should be recommended to wear elastic stockings6263 Follow-up VUS is recommended to monitor thrombosis progressionevolu-tion both in the presence or absence of anticoagulation
Incidence of recurrent VTE appears to be similar to that of patientswith proximal DVT6465
Consensus statement initial and long-term
managementbull Patients with proximal DVT should be anticoagulated for at least
3-monthsbull Patients with isolated distal DVT at high-risk of recurrence should
be anticoagulated as for proximal DVT for those at low risk ofrecurrence shorter treatment (4ndash6 weeks) even at lower anti-coagulant doses or ultrasound surveillance may be considered
bull In the absence of contraindications DOACs should be preferredas first-line anticoagulant therapy in non-cancer patients with pro-ximal DVT
bull Adjuvant CDT may be considered in selected patients with ilio-common femoral DVT symptoms lt14 days and life expectancygt1 year if performed in experienced centres
bull Primary acute DVT stenting or mechanical thrombus removalalone are not recommended
bull Vena cava filters may be considered if anticoagulation is contraindi-cated their use in addition to anticoagulation is notrecommended
bull Compression therapy associated with early mobilization and walk-ing exercise should be considered to relieve acute venoussymptoms
Extended phase management(beyond first 3ndash6 months)
Duration of anticoagulationOnce anticoagulation is stopped risk of VTE recurrence over yearsafter a first episode is consistently around 3066 Risk is more thandoubled in patients with unprovoked (annual rate gt70) vs those with(transient) provoked VTE67 and among the latter in medical rather
Table 3 Conditions or risk factors for complicationsafter a first isolated distal DVT
High-risk conditions Low-risk conditions
Previous VTE events Isolated distal DVT second-
ary to surgery or other
transient risk factors (plas-
ters immobilization
trauma long trip etc)
provided complete
mobilization is achieved
Males Isolated distal DVT occurring
during contraceptive or
replacement hormonal
therapy (provided therapy
has been interrupted)
Age gt50 years
Cancer
Unprovoked isolated distal DVT
Secondary isolated distal DVT with
persistently hampered mobilization
Isolated distal DVT involving the
popliteal trifurcation
Isolated distal DVT involving gt1 calf vein
Isolated distal DVT present in both legs
Presence of predisposing diseases
(eg inflammatory bowel diseases)
Known thrombophilic alterations
Axial vs Muscular isolated distal DVT
Table 4 Risk of recurrence after a first episode of unprovoked VTE
Risk factors for DVTrecurrence
Proximal DVT location Male sex Persistence of residual vein thrombosis at ultrasound
Obesity Non-zero blood group High D-dimer values
Old age Early PTS development Role of inherited thrombophilia is controversial
Clinical prediction rules assessing risk of recurrent VTE after first episode of unprovoked VTE71
Score Vienna prediction model DASH score HERDOO-2
Parameters bull D-dimer level at 3 weeks
and 3 9 15 24 months after
stopping anticoagulationbull Male sexbull VTE location (Distal DVT
Proximal DVT PE)
bull Abnormal D-dimer 3ndash5 weeks after
stopping anticoagulationbull Male sexbull Agelt50 yearsbull VTE not associated with
oestrogen-progestatif therapy
in women
bull Abnormal D-dimer before
stopping anticoagulationbull Post thrombotic symptoms
(hyperpigmentation edema
and redness)bull Age gt_65 yearsbull BMI gt_30
Validation study Yes Yes Yes
Commentaries Different nomograms are available
to calculate risk of VTE recurrence
at different time
Patients with low score (lt_1) have
an annual
recurrence rate of 31
It is applicable in women only
Women with low score (lt_1)
have an annual recurrence rate of 13
6 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
than surgical patients68 Patients with a first symptomatic unprovokedDVT are at higher risk of recurrence than those with a first unpro-voked PE69 Factors related to DVT recurrence are listed in Table 4
For proximal DVT andor PE 3-months anticoagulation is the bestoption if transient and reversible risk factors were present70 In allother patients prolonging anticoagulation protects from recurrence(70ndash90) but exposes to risk of unpredictable bleeding complica-tions Decision to discontinue or not anticoagulation should there-fore be individually tailored and balanced against bleeding risk takingalso into account patientsrsquo preferences Three clinical prediction ruleshave been derived and prospectively validated to detect low-recurrence risk patients (Table 4)71 A number of bleeding scoreswere evaluated none showed sufficient predictive accuracy or hadsufficient validation to be recommended in routine clinicalpractice7273
Continuing indefinite anticoagulation with the same drug adminis-tered during the first months is the best option for patients with mul-tiple VTE episodes or strong VTE familial history those with majorthrombophilia or longstanding medical diseases at high thromboticrisk70 Indefinite anticoagulation can also be considered in patientswith first episode of unprovoked VTE especially in those with severepresentation provided they are at low bleeding risk70 Finally discon-tinuing anticoagulation in non-cancer patients with repeatedly nega-tive D-dimer (before drug interruption 15 30 60 and 90 daysfollowing interruption) has proved to be safe in patients with unpro-voked proximal DVT provided veins are recanalized or remained sta-ble for 1 year74 However using moderately sensitive D-dimer assayduring and 30 days after stopping anticoagulation these results werenot confirmed in men and in women with VTE not associated withoestrogen treatment75 Similarly when measurements were re-peated using a quantitative assay D-dimer testing failed to identifysubgroups with very low recurrence rate76
AntithromboticsVitamin K antagonists
Four randomized studies evaluated VKA [target international normal-ized ratio (INR) 20ndash30] for VTE extended treatment in patientscompleting 3-months anticoagulation77ndash80 Recurrent VTE occurredless in the VKA groups (combined OR 007)81 Bleeding was signifi-cantly higher81
The ELATE study82 randomized patients to conventional intensity(INR 20ndash30) or low-intensity (INR 15ndash1ndash9) Recurrence rate was07 vs 19100 patient-years respectively (HR 28) with no differencein major bleeding Yet the low-intensity VKA therapy should bediscouraged
Direct oral anticoagulants
Dabigatran (150 mg bid) was as effective as warfarin and more ef-fective than placebo in preventing recurrent VTE (Table 5) Risk ofmajor bleeding was reduced compared with warfarin83
With Rivaroxaban (20 mg od) risk of VTE recurrence was lowercompared with placebo (HR 019) while bleeding risk was notincreased (Table 5)84 Standard and lower dose (10 mg od) also signif-icantly reduced risk of recurrence compared to aspirine without sig-nificant increase in bleeding85
VTE recurrence occurred significantly less in standard and lowerdose Apixaban (5 and 25 mg bid) vs placebo (Table 5) Bleeding didnot differ between groups86
Recurrence rates with Edoxaban 60 mg were similar to thewarfarin-treated group (post hoc analysis) (Table 5)87 Major bleedingwas lower in the edoxaban group
Data from Phase IV studies are scarce but results from XALIA areconsistent with observations of rivaroxaban and warfarin88
Aspirin
Two studies investigated aspirin 100 mg vs placebo in patients withidiopathic VTE who completed initial anticoagulation treatment8990
Pooled HR for VTE recurrence was 068 and 147 for bleeding91
Other
Recent evaluation of Sulodexide vs placebo in patients with unpro-voked VTE who completed standard course of anticoagulationshowed a HR for VTE recurrence of 049 (P = 002)92 No majorbleeding episodes were observed
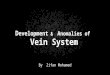
Venous occlusion recanalizationEndovascular techniques are available for selected patients withPTS57 Case series and prospective cohort trials suggest that at leastsome subgroups of PTS patients (CEAP classes 4ndash6 Figure 4) maybenefit from addition of endovascular therapy into overall manage-ment strategy
In patients with moderate-to-severe PTS and iliac vein obstructionendovascular stent placement may be used to restore vein patencyIn preliminary studies stent placement in chronically occluded iliacveins contributed to ulcers healing PTS symptoms relief and reducedobstructive venous sequel93
No randomized controlled trials are available the largest seriesfound patients with moderate-to-severe PTS to have reduced pain(P lt 00001) severe pain (from 41 to 11) and severe swelling(from 36 to 18) increased ulcer healing (68) and reduced ven-ous pressure following recanalization with stent placement93
Claudication improvement better outflow fraction and calf pumpfunction was also observed94
In selected infrequent cases surgical vein bypass may be an optionto relieve venous hypertension
Follow-upPatients with DVT should be followed to avoid risk of recurrence aswell as DVT and anticoagulation-related complicationsDevelopment of renal failure changes in body weight or pregnancythat may require anticoagulation adjustment should be monitoredCompliance as well as benefitrisk balance should be assessed regu-larly VUS at anticoagulation discontinuation is useful in determiningbaseline residual vein thrombosis
Consensus statement extended managementbull Decision to discontinue or not anticoagulation should be individu-
ally tailored balancing risk of recurrence against bleeding risk tak-ing into account patientsrsquo preferences and compliance
bull In the absence of contraindications DOACs should be preferredas first line anticoagulant therapy in non-cancer patients Currently
Diagnosis and management of acute DVT 7
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

Long-term complications include post-thrombotic syn-drome (PTS) defined as chronic venous symptoms andorsigns secondary to DVT It represents the most frequentchronic DVT complication occurring in 30ndash50 of patientswithin 2 years after proximal DVT9 In 5ndash10 of cases PTS issevere9 Previous ipsilateral DVT proximal location (ilio-fem-oral gt popliteal) and residual veins obstruction are most sig-nificant PTS risk factors Obesity and poor INR control during
the first 3-months treatment are additional independent riskfactors10
Villalta score is used for PTS diagnosis and treatment evaluation(Table 1)11
Diagnosis
Deep vein thrombosis withoutpulmonary embolism symptomsClinical signs and symptoms are highly variable and unspecific but re-main the cornerstone of diagnostic strategy Symptoms include painswelling increased skin veins visibility erythema and cyanosis accom-panied by unexplained fever
Probability assessment and D-dimertestingPre-test probability assessment is the first step in the diagnostic algo-rithm of DVT suspicion (Figure 2) Sensitivity and specificity of clinicalsymptoms are low when considered individually however theircombination using prediction rules allows pre-test clinical probabil-ity classification into two- (DVT unlikely or likely) or three-categories(low- intermediate- or high-clinical probability) corresponding toincreasing disease prevalence1213 Wells score has been widely vali-dated and can be applied both to out- and inpatients (Table 2) Theexpertsrsquo panel favours the modified two-level pre-test probability asit is more straightforward14
Normal D-dimers render DVT unlikely15 however D-dimers havelow specificity Quantitative ELISA or ELISA-derived assays (gt95sensitivity) allow ruling out DVT in patients with DVT lsquounlikelyrsquoNegative ELISA D-dimer can exclude DVT without further testing in30 of patients16 with 3-month thromboembolic risk lt1 withouttreatment13 Quantitative latex-derived and whole-blood agglutin-ation assay have lower sensitivity (85ndash90)17 In patients with lsquolikelyrsquo
Figure 1 Venous thromboembolism incidence according to age group
Table 1 Villalta score11
Symptoms and
Clinical signs
None Mild Moderate Severe
Symptoms
Pain 0 points 1 points 2 points 3 points
Cramps 0 points 1 points 2 points 3 points
Haeviness 0 points 1 points 2 points 3 points
Paresthesia 0 points 1 points 2 points 3 points
Pruritus 0 points 1 points 2 points 3 points
Clinical signs
Pretibial edema 0 points 1 points 2 points 3 points
Skin induration 0 points 1 points 2 points 3 points
Hyperpigmentation 0 points 1 points 2 points 3 points
Redness 0 points 1 points 2 points 3 points
Venous ectasia 0 points 1 points 2 points 3 points
Pain on calf
compression
0 points 1 points 2 points 3 points
Venous ulcer Absent Present
Points are summed into a total score (range 0ndash33) Post Thrombotic syndrome(PTS) is defined by a total score of gt_5 or the presence of a venous ulcer PTS isclassified as mild if Villalta score is 5ndash9 moderate if 10ndash14 and severe if gt_15 orvenous ulcer is present
2 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
DVT D-Dimer testing is not necessary imaging is requiredTherapeutic anticoagulation should be initiated if not contraindi-cated in patients with DVT lsquolikelyrsquo until imaging
Imaging
Venous ultrasound (VUS) is the first line DVT imaging modality(other imaging see Supplementary material online only section) It isbased on B-mode combined or not with color-Doppler US andpower imaging techniques DVT diagnostic criteria are cross-sectional vein incompressibility direct thrombus imaging with veinenlargement and abnormal spectral and color-Doppler flow VUScan be performed by examining popliteal and common femoral veinsonly [2-point2-region compression venous ultrasonography (CUS)or limited CUS] or by extended imaging of inferior vena cava iliacand femoral veins and calf veins (whole-leg VUS or complete VUS)There are controversies as to whether explore symptomatic legonly or both1819
In clinically suspected DVT VUS provides overall sensitivity of942 for proximal and 635 for isolated distal DVT with an overallspecificity of 93820 Combination with color-Doppler US increasessensitivity but lowers specificity20 When DVT is suspected (withoutPE symptoms) anticoagulation may be safely withheld in patientswith a single normal complete VUS Same is true for limited CUS pro-vided it can be repeated and integrated within a diagnostic strategy
including clinical probability and D-dimer assessment21 Overall 3-month VTE incidence rate after negative complete VUS is 05722
but both methods are reported to be equivalent in randomized tri-als2324 Complete VUS may be helpful to explain patientrsquos complaintby providing up to 42 alternative diagnosis25 Point-of care US per-formed by emergency physicians using limited CUS has shown goodperformance (961 sensitivity 968 specificity)26 and may be usefulif vascular laboratories are not available 247 provided its integrationin a validated diagnostic strategy27
In patients with clinically suspected recurrent DVT comparison oftest results with baseline imaging at discontinuation of anticoagulationcan safely rule out diagnosis of recurrence28 A 2- or 4-mm29ndash31 in-crease in vein diameter between two measurements at the commonfemoral and popliteal veins after full compression is the most vali-dated US criterion
Deep vein thrombosis with pulmonaryembolism symptomsDiagnostic approach is described in corresponding 2014 EuropeanSociety of Cardiology (ESC) Guidelines6 Proximal DVT confirmationin a normotensive patient with suspected PE essentially confirms VTEand justifies anticoagulation as after formal PE diagnosis In unstable pa-tients with right ventricular overload but no possibility to confirm PECUS showing proximal DVT facilitates initiation of reperfusion
Lower limb DVT suspicion
Clinical probability assessement (2-level modified Wells score)
DVT unlikely DVT likely
D-Dimers
Negative Positive Complete venous US
No DVT Proximal DVT
Treatment At least 3-months AC DOACs in non cancer patients if no contraindications
3-months evaluation Venous US riskbenefit complianceand patientrsquos preference
Stop anticoagulation Extended AC Yearly evaluation
Isolated distal DVT
High risk recurrence Low risk recurrence
No treatment Treatment 3-months AC
Treatment or surveillance 4-6 wk AC (full or lower dose) or venous US surveillance
Figure 2 Proposed deep vein thrombosis diagnostic and management algorithm AC anticoagulation DOAC direct oral anticoagulant
Diagnosis and management of acute DVT 3
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
therapy CUS diagnostic yield is high in the presence of clinical DVTsigns32 Among unselected PE patients proximal DVT at CUS is foundin 17 patients33 Proximal DVT has high specificity and may justifytreatment even if pulmonary CT is negative6 While negative CUS can-not exclude PE it can justify withholding anticoagulation in patientswith non-diagnostic ventilationperfusion scan and PE-unlikely163435
In symptomatic patients with isolated sub-segmental PE or inciden-tal asymptomatic PE concomitant DVT justifies anticoagulation3637
Deep vein thrombosis imaging may also be useful if secondarily a pa-tient is suspected of VTE recurrence with DVT signs Moreoverpresence of concomitant DVT has been suggested as an independent30-days death risk factor following PE38
Consensus statement diagnosisbull Clinical prediction rule (two-level modified Wells score) is recom-
mended to stratify patients with suspected lower limb DVTbull ELISA D-dimer measurement is recommended in lsquounlikelyrsquo clinical
probability patients to exclude DVTbull Venous US is recommended as first line imaging method for DVT
diagnosisbull Venous CT scan should be reserved to selected patients onlybull Venous US should be proposed also in case of confirmed PE for
initial reference venous imaging useful in case of DVT recurrencesuspicion or further stratification in selected patients
bull Venous US may be considered for further stratification in selectedpatients with concomitant suspected PE
Initial (first 5ndash21 days) and long-term (first 3ndash6 months) phasemanagement
Deep vein thrombosis withoutpulmonary embolismAnticoagulation in non-cancer patients
Deep vein thrombosis treatment consists of three phases (Figure 3)39
Initial treatment (5ndash21 days following diagnosis) during this period pa-tients receive either parenteral therapy and are transited to vitamin K an-tagonists (VKA) or use high-dose direct oral anticoagulants (DOACs)Long-term treatment (following 3ndash6 months) patients are treated withVKA or DOACs39 Initial and long-term treatments are mandatory forall DVT patients Decision of extended treatment (beyond first 3ndash6months) is based on benefitrisk balance of continued anticoagulation
Initial treatment(first 5-21 days)
Long term treatment
(first 3-6 months)
Extended treatment
(following initial 3-6 months)
Apixaban 10 mg bid for 7 days Apixaban 5mg bid Apixaban 25mg bid beyond 6 months
Dabigatran 150 mg bid preceded by LMWH for 5-10 days
Edoxaban 60 mg od (30mg od if ClCreat 50-30ltmlmin or concomitant potent P-P inhibitors) preceded by LMWH for 5-10 days
Rivaroxaban 15 mg bid for 21 days Rivaroxaban 20mg od Rivaroxaban 10 mg or 20 mg od beyond 6 months
VKA to achieve INR 2-3 preceded by LMWH for 5-10 days
Figure 3 Deep vein thrombosis treatment phases ClCreat creatinine clearance LMWH low molecular weight heparin P-P inhibitors protonpump inhibitors VKA vitamin K antantagonist
Table 2 The Wells score1213
Clinical variable Points
Active cancer (treatment ongoing or within previous 6
months or palliative)
thorn1
Paralysis paresis or recent plaster immobilization of
the lower extremities
thorn1
Recently bedridden for 3 days or more or major sur-
gery within the previous 12 weeks requiring general
or regional anesthesia
thorn1
Localized tenderness along the distribution of the deep
venous system
thorn1
Entire leg swelling thorn1
Calf swelling at least 3 cm larger than that on the
asymptomatic leg (measured 10 cm below the tibial
tuberosity)
thorn1
Pitting edema confined to the symptomatic leg thorn1
Collateral superficial veins (non varicose) thorn1
Previously documented DVT thorn1
Alternative diagnosis at least as likely as DVT -2
Three-level Wells score
Low lt1
Intermediate 1ndash2
High gt2
Two-level Wells score
Unlikely lt_1
Likely gt_2
4 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
In patients with severe renal failure (creatinine clearance lt30
mLmin) unstable renal function or high bleeding risk iv unfrac-tionated heparin (UFH) may be preferable (short half-life and pro-tamine sulfate reversibility) Less solid is the evidence in favor ofUFH in obese (BMI gt40 kgm2) and underweight patients (lt50 kg)Main disadvantage of UFH is its inter-individual dose variabilityrequiring laboratory monitoring and dose adjustment AdditionallyUFH is associated with high risk of heparin-induced thrombocyto-penia For these reasons low-molecular weight heparin (LMWH)is the parenteral treatment of choice LMWHs are at least as effect-ive as UFH and probably safer40 Fondaparinux can also be used asparenteral agent41 Both LMWH and fondaparinux do not havespecific antidote
Recently DOACs have emerged as valid options for DVT treat-ment39 Dabigatran and edoxaban were studied following initial 7ndash9days treatment with a parenteral agent Apixaban and rivaroxabanwere evaluated by the lsquosingle drug approachrsquo (Figure 3)
DOACs have longer elimination half-lives than UFH or LMWHand may accumulate in patients with suboptimal renal (creatinineclearance lt30 mLmin) or hepatic function (Child-Pugh class B or C)Patients with poor renal andor hepatic function pregnancylactationthrombocytopenia were excluded from Phase III studies Patientswith active cancer were scarcely represented (3ndash8 of entire studypopulation)
DOACs are at least as effective as and probably safer than paren-teral drugVKA treatment42 A meta-analysis (27023 patients)showed similar VTE recurrence rates in patients receiving DOACsor conventional therapy (20 vs 22 RR 090) Major bleeding (RR061) fatal bleeding (RR 036) intracranial bleeding (RR 037) andclinically relevant non-major bleeding (RR 073) were significantlylower in DOACs-treated patients42 DOACs reversal agents arebeing investigated Idarucizumab (Dabigatran reversal agent) is cur-rently available for clinical use4344
Thrombolysisthrombectomy
Early clot removal may prevent at least partly PTS developement45
Catheter-directed thrombolysis (CDT) is more efficient than sys-temic lysis mainly due to less bleeding as thrombolytic agent is directlyadministered within the clot Three major randomized controlled trialscompared different CDT modalities on top of anticoagulation andcompression with a control group (anticoagulation and compressiononly) The CAVENT trial included 209 patients with first-time acuteDVT (iliac common femoral andor upper femoral vein)46 AdjuvantCDT was associated with a 26 RR PTS reduction over 2 years (411vs 556 P = 004) compared with anticoagulation alone46 Amount ofresidual post-CDT thrombus correlated with venous patency rates at24-months (P = 004) Persistence of venous patency at 6 and 24months correlated with PTS freedom (P lt 0001) A 32 of patientshad major bleed but there were no intracranial bleeds or deathsOverall trial found no differences in long-term (2 years) quality of lifebetween patients with- or without CDT Results have been confirmedafter 5 years follow-up47
Mechanical thrombus removal alone is not successful and needsadjuvant thrombolytic therapy In PEARL I and II studies only 5 ofpatients were treated without thrombolytics48
Up to 83 of patients treated by any catheter-based therapy needadjunctive angioplasty and stenting49 Primary acute DVT stenting isnot recommended due to lack of data
Vena cava filter
Vena cava filter may be used when anticoagulation is absolutely contra-indicated in patients with newly diagnosed proximal DVT One majorcomplication is filter thrombosis Therefore anticoagulation should bestarted as soon as contraindications resolve50 and retrievable filter rap-idly removed Filter placement in addition to anticoagulation does notimprove survival5152 except in patients with hemodynamically unstablePE or after thrombolytic therapy53 Increased DVT recurrence hasbeen shown with permanent51 but not with retrievable filters52
Compression
Goal of compression is to relieve venous symptoms and eventuallyprevent PTS54
Elastic compression stockings efficacy has been challenged by theSOX trial55 A total of 806 patients with proximal DVT have beenrandomized to either 30ndash40 mmHg or placebo (lt5 mmHg) stock-ings Cumulative 2 years PTS incidence was similar (526 vs 523HR= 10) No difference in PTS severity or quality-of-life was observ-ed55 However compliance definition (stockings wearing for gt_3 daysweek) was significantly lower than in previous studies (56vs90)56 Although role of stockings in PTS prevention may be un-certain their use remains a reasonable option for controlling symp-toms of acute proximal DVT57
Compression associated with early mobilization and walking exer-cise has shown significant efficacy in venous symptom relieve in pa-tients with acute DVT58 Caution should be used in patients withsevere peripheral artery disease
Home vs in-hospital management
Most patients with DVT may be treated on a home basis (seeSupplementary material online only section)
Deep vein thrombosis with pulmonaryembolismManagement of patients with acute PE is described in the 2014 ESCguideline6 (summary in the see Supplementary material online onlysection)
Isolated distal deep vein thrombosisWhether isolated distal DVT should be treated with anticoagulationis still debated A recent trial randomized patients with a first isolateddistal DVT to LMWH or placebo for 42 days59 Rate of symptomaticproximal DVT or PE at 42 days was not different between LMWHand placebo (33 vs 54) major or clinically relevant non-majorbleeding occurred more frequently in the LMWH group (5 vs 0P = 003) These data seem to support that not all isolated distal DVTshould receive full-dose anticoagulation
Approach is to anticoagulate full-dose for at least 3 months as forproximal DVTs patients at high-risk VTE (Table 3)60 Shorter LMWHtreatment (4ndash6 weeks) even at lower doses or ultrasound surveil-lance could be effective and safe in low-risk patients (Table 3)61 Nodata are available on DOACs All patients with acute isolated distal
Diagnosis and management of acute DVT 5
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
DVT should be recommended to wear elastic stockings6263 Follow-up VUS is recommended to monitor thrombosis progressionevolu-tion both in the presence or absence of anticoagulation
Incidence of recurrent VTE appears to be similar to that of patientswith proximal DVT6465
Consensus statement initial and long-term
managementbull Patients with proximal DVT should be anticoagulated for at least
3-monthsbull Patients with isolated distal DVT at high-risk of recurrence should
be anticoagulated as for proximal DVT for those at low risk ofrecurrence shorter treatment (4ndash6 weeks) even at lower anti-coagulant doses or ultrasound surveillance may be considered
bull In the absence of contraindications DOACs should be preferredas first-line anticoagulant therapy in non-cancer patients with pro-ximal DVT
bull Adjuvant CDT may be considered in selected patients with ilio-common femoral DVT symptoms lt14 days and life expectancygt1 year if performed in experienced centres
bull Primary acute DVT stenting or mechanical thrombus removalalone are not recommended
bull Vena cava filters may be considered if anticoagulation is contraindi-cated their use in addition to anticoagulation is notrecommended
bull Compression therapy associated with early mobilization and walk-ing exercise should be considered to relieve acute venoussymptoms
Extended phase management(beyond first 3ndash6 months)
Duration of anticoagulationOnce anticoagulation is stopped risk of VTE recurrence over yearsafter a first episode is consistently around 3066 Risk is more thandoubled in patients with unprovoked (annual rate gt70) vs those with(transient) provoked VTE67 and among the latter in medical rather
Table 3 Conditions or risk factors for complicationsafter a first isolated distal DVT
High-risk conditions Low-risk conditions
Previous VTE events Isolated distal DVT second-
ary to surgery or other
transient risk factors (plas-
ters immobilization
trauma long trip etc)
provided complete
mobilization is achieved
Males Isolated distal DVT occurring
during contraceptive or
replacement hormonal
therapy (provided therapy
has been interrupted)
Age gt50 years
Cancer
Unprovoked isolated distal DVT
Secondary isolated distal DVT with
persistently hampered mobilization
Isolated distal DVT involving the
popliteal trifurcation
Isolated distal DVT involving gt1 calf vein
Isolated distal DVT present in both legs
Presence of predisposing diseases
(eg inflammatory bowel diseases)
Known thrombophilic alterations
Axial vs Muscular isolated distal DVT
Table 4 Risk of recurrence after a first episode of unprovoked VTE
Risk factors for DVTrecurrence
Proximal DVT location Male sex Persistence of residual vein thrombosis at ultrasound
Obesity Non-zero blood group High D-dimer values
Old age Early PTS development Role of inherited thrombophilia is controversial
Clinical prediction rules assessing risk of recurrent VTE after first episode of unprovoked VTE71
Score Vienna prediction model DASH score HERDOO-2
Parameters bull D-dimer level at 3 weeks
and 3 9 15 24 months after
stopping anticoagulationbull Male sexbull VTE location (Distal DVT
Proximal DVT PE)
bull Abnormal D-dimer 3ndash5 weeks after
stopping anticoagulationbull Male sexbull Agelt50 yearsbull VTE not associated with
oestrogen-progestatif therapy
in women
bull Abnormal D-dimer before
stopping anticoagulationbull Post thrombotic symptoms
(hyperpigmentation edema
and redness)bull Age gt_65 yearsbull BMI gt_30
Validation study Yes Yes Yes
Commentaries Different nomograms are available
to calculate risk of VTE recurrence
at different time
Patients with low score (lt_1) have
an annual
recurrence rate of 31
It is applicable in women only
Women with low score (lt_1)
have an annual recurrence rate of 13
6 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
than surgical patients68 Patients with a first symptomatic unprovokedDVT are at higher risk of recurrence than those with a first unpro-voked PE69 Factors related to DVT recurrence are listed in Table 4
For proximal DVT andor PE 3-months anticoagulation is the bestoption if transient and reversible risk factors were present70 In allother patients prolonging anticoagulation protects from recurrence(70ndash90) but exposes to risk of unpredictable bleeding complica-tions Decision to discontinue or not anticoagulation should there-fore be individually tailored and balanced against bleeding risk takingalso into account patientsrsquo preferences Three clinical prediction ruleshave been derived and prospectively validated to detect low-recurrence risk patients (Table 4)71 A number of bleeding scoreswere evaluated none showed sufficient predictive accuracy or hadsufficient validation to be recommended in routine clinicalpractice7273
Continuing indefinite anticoagulation with the same drug adminis-tered during the first months is the best option for patients with mul-tiple VTE episodes or strong VTE familial history those with majorthrombophilia or longstanding medical diseases at high thromboticrisk70 Indefinite anticoagulation can also be considered in patientswith first episode of unprovoked VTE especially in those with severepresentation provided they are at low bleeding risk70 Finally discon-tinuing anticoagulation in non-cancer patients with repeatedly nega-tive D-dimer (before drug interruption 15 30 60 and 90 daysfollowing interruption) has proved to be safe in patients with unpro-voked proximal DVT provided veins are recanalized or remained sta-ble for 1 year74 However using moderately sensitive D-dimer assayduring and 30 days after stopping anticoagulation these results werenot confirmed in men and in women with VTE not associated withoestrogen treatment75 Similarly when measurements were re-peated using a quantitative assay D-dimer testing failed to identifysubgroups with very low recurrence rate76
AntithromboticsVitamin K antagonists
Four randomized studies evaluated VKA [target international normal-ized ratio (INR) 20ndash30] for VTE extended treatment in patientscompleting 3-months anticoagulation77ndash80 Recurrent VTE occurredless in the VKA groups (combined OR 007)81 Bleeding was signifi-cantly higher81
The ELATE study82 randomized patients to conventional intensity(INR 20ndash30) or low-intensity (INR 15ndash1ndash9) Recurrence rate was07 vs 19100 patient-years respectively (HR 28) with no differencein major bleeding Yet the low-intensity VKA therapy should bediscouraged
Direct oral anticoagulants
Dabigatran (150 mg bid) was as effective as warfarin and more ef-fective than placebo in preventing recurrent VTE (Table 5) Risk ofmajor bleeding was reduced compared with warfarin83
With Rivaroxaban (20 mg od) risk of VTE recurrence was lowercompared with placebo (HR 019) while bleeding risk was notincreased (Table 5)84 Standard and lower dose (10 mg od) also signif-icantly reduced risk of recurrence compared to aspirine without sig-nificant increase in bleeding85
VTE recurrence occurred significantly less in standard and lowerdose Apixaban (5 and 25 mg bid) vs placebo (Table 5) Bleeding didnot differ between groups86
Recurrence rates with Edoxaban 60 mg were similar to thewarfarin-treated group (post hoc analysis) (Table 5)87 Major bleedingwas lower in the edoxaban group
Data from Phase IV studies are scarce but results from XALIA areconsistent with observations of rivaroxaban and warfarin88
Aspirin
Two studies investigated aspirin 100 mg vs placebo in patients withidiopathic VTE who completed initial anticoagulation treatment8990
Pooled HR for VTE recurrence was 068 and 147 for bleeding91
Other
Recent evaluation of Sulodexide vs placebo in patients with unpro-voked VTE who completed standard course of anticoagulationshowed a HR for VTE recurrence of 049 (P = 002)92 No majorbleeding episodes were observed
Venous occlusion recanalizationEndovascular techniques are available for selected patients withPTS57 Case series and prospective cohort trials suggest that at leastsome subgroups of PTS patients (CEAP classes 4ndash6 Figure 4) maybenefit from addition of endovascular therapy into overall manage-ment strategy
In patients with moderate-to-severe PTS and iliac vein obstructionendovascular stent placement may be used to restore vein patencyIn preliminary studies stent placement in chronically occluded iliacveins contributed to ulcers healing PTS symptoms relief and reducedobstructive venous sequel93
No randomized controlled trials are available the largest seriesfound patients with moderate-to-severe PTS to have reduced pain(P lt 00001) severe pain (from 41 to 11) and severe swelling(from 36 to 18) increased ulcer healing (68) and reduced ven-ous pressure following recanalization with stent placement93
Claudication improvement better outflow fraction and calf pumpfunction was also observed94
In selected infrequent cases surgical vein bypass may be an optionto relieve venous hypertension
Follow-upPatients with DVT should be followed to avoid risk of recurrence aswell as DVT and anticoagulation-related complicationsDevelopment of renal failure changes in body weight or pregnancythat may require anticoagulation adjustment should be monitoredCompliance as well as benefitrisk balance should be assessed regu-larly VUS at anticoagulation discontinuation is useful in determiningbaseline residual vein thrombosis
Consensus statement extended managementbull Decision to discontinue or not anticoagulation should be individu-
ally tailored balancing risk of recurrence against bleeding risk tak-ing into account patientsrsquo preferences and compliance
bull In the absence of contraindications DOACs should be preferredas first line anticoagulant therapy in non-cancer patients Currently
Diagnosis and management of acute DVT 7
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

DVT D-Dimer testing is not necessary imaging is requiredTherapeutic anticoagulation should be initiated if not contraindi-cated in patients with DVT lsquolikelyrsquo until imaging
Imaging
Venous ultrasound (VUS) is the first line DVT imaging modality(other imaging see Supplementary material online only section) It isbased on B-mode combined or not with color-Doppler US andpower imaging techniques DVT diagnostic criteria are cross-sectional vein incompressibility direct thrombus imaging with veinenlargement and abnormal spectral and color-Doppler flow VUScan be performed by examining popliteal and common femoral veinsonly [2-point2-region compression venous ultrasonography (CUS)or limited CUS] or by extended imaging of inferior vena cava iliacand femoral veins and calf veins (whole-leg VUS or complete VUS)There are controversies as to whether explore symptomatic legonly or both1819
In clinically suspected DVT VUS provides overall sensitivity of942 for proximal and 635 for isolated distal DVT with an overallspecificity of 93820 Combination with color-Doppler US increasessensitivity but lowers specificity20 When DVT is suspected (withoutPE symptoms) anticoagulation may be safely withheld in patientswith a single normal complete VUS Same is true for limited CUS pro-vided it can be repeated and integrated within a diagnostic strategy
including clinical probability and D-dimer assessment21 Overall 3-month VTE incidence rate after negative complete VUS is 05722
but both methods are reported to be equivalent in randomized tri-als2324 Complete VUS may be helpful to explain patientrsquos complaintby providing up to 42 alternative diagnosis25 Point-of care US per-formed by emergency physicians using limited CUS has shown goodperformance (961 sensitivity 968 specificity)26 and may be usefulif vascular laboratories are not available 247 provided its integrationin a validated diagnostic strategy27
In patients with clinically suspected recurrent DVT comparison oftest results with baseline imaging at discontinuation of anticoagulationcan safely rule out diagnosis of recurrence28 A 2- or 4-mm29ndash31 in-crease in vein diameter between two measurements at the commonfemoral and popliteal veins after full compression is the most vali-dated US criterion
Deep vein thrombosis with pulmonaryembolism symptomsDiagnostic approach is described in corresponding 2014 EuropeanSociety of Cardiology (ESC) Guidelines6 Proximal DVT confirmationin a normotensive patient with suspected PE essentially confirms VTEand justifies anticoagulation as after formal PE diagnosis In unstable pa-tients with right ventricular overload but no possibility to confirm PECUS showing proximal DVT facilitates initiation of reperfusion
Lower limb DVT suspicion
Clinical probability assessement (2-level modified Wells score)
DVT unlikely DVT likely
D-Dimers
Negative Positive Complete venous US
No DVT Proximal DVT
Treatment At least 3-months AC DOACs in non cancer patients if no contraindications
3-months evaluation Venous US riskbenefit complianceand patientrsquos preference
Stop anticoagulation Extended AC Yearly evaluation
Isolated distal DVT
High risk recurrence Low risk recurrence
No treatment Treatment 3-months AC
Treatment or surveillance 4-6 wk AC (full or lower dose) or venous US surveillance
Figure 2 Proposed deep vein thrombosis diagnostic and management algorithm AC anticoagulation DOAC direct oral anticoagulant
Diagnosis and management of acute DVT 3
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
therapy CUS diagnostic yield is high in the presence of clinical DVTsigns32 Among unselected PE patients proximal DVT at CUS is foundin 17 patients33 Proximal DVT has high specificity and may justifytreatment even if pulmonary CT is negative6 While negative CUS can-not exclude PE it can justify withholding anticoagulation in patientswith non-diagnostic ventilationperfusion scan and PE-unlikely163435
In symptomatic patients with isolated sub-segmental PE or inciden-tal asymptomatic PE concomitant DVT justifies anticoagulation3637
Deep vein thrombosis imaging may also be useful if secondarily a pa-tient is suspected of VTE recurrence with DVT signs Moreoverpresence of concomitant DVT has been suggested as an independent30-days death risk factor following PE38
Consensus statement diagnosisbull Clinical prediction rule (two-level modified Wells score) is recom-
mended to stratify patients with suspected lower limb DVTbull ELISA D-dimer measurement is recommended in lsquounlikelyrsquo clinical
probability patients to exclude DVTbull Venous US is recommended as first line imaging method for DVT
diagnosisbull Venous CT scan should be reserved to selected patients onlybull Venous US should be proposed also in case of confirmed PE for
initial reference venous imaging useful in case of DVT recurrencesuspicion or further stratification in selected patients
bull Venous US may be considered for further stratification in selectedpatients with concomitant suspected PE
Initial (first 5ndash21 days) and long-term (first 3ndash6 months) phasemanagement
Deep vein thrombosis withoutpulmonary embolismAnticoagulation in non-cancer patients
Deep vein thrombosis treatment consists of three phases (Figure 3)39
Initial treatment (5ndash21 days following diagnosis) during this period pa-tients receive either parenteral therapy and are transited to vitamin K an-tagonists (VKA) or use high-dose direct oral anticoagulants (DOACs)Long-term treatment (following 3ndash6 months) patients are treated withVKA or DOACs39 Initial and long-term treatments are mandatory forall DVT patients Decision of extended treatment (beyond first 3ndash6months) is based on benefitrisk balance of continued anticoagulation
Initial treatment(first 5-21 days)
Long term treatment
(first 3-6 months)
Extended treatment
(following initial 3-6 months)
Apixaban 10 mg bid for 7 days Apixaban 5mg bid Apixaban 25mg bid beyond 6 months
Dabigatran 150 mg bid preceded by LMWH for 5-10 days
Edoxaban 60 mg od (30mg od if ClCreat 50-30ltmlmin or concomitant potent P-P inhibitors) preceded by LMWH for 5-10 days
Rivaroxaban 15 mg bid for 21 days Rivaroxaban 20mg od Rivaroxaban 10 mg or 20 mg od beyond 6 months
VKA to achieve INR 2-3 preceded by LMWH for 5-10 days
Figure 3 Deep vein thrombosis treatment phases ClCreat creatinine clearance LMWH low molecular weight heparin P-P inhibitors protonpump inhibitors VKA vitamin K antantagonist
Table 2 The Wells score1213
Clinical variable Points
Active cancer (treatment ongoing or within previous 6
months or palliative)
thorn1
Paralysis paresis or recent plaster immobilization of
the lower extremities
thorn1
Recently bedridden for 3 days or more or major sur-
gery within the previous 12 weeks requiring general
or regional anesthesia
thorn1
Localized tenderness along the distribution of the deep
venous system
thorn1
Entire leg swelling thorn1
Calf swelling at least 3 cm larger than that on the
asymptomatic leg (measured 10 cm below the tibial
tuberosity)
thorn1
Pitting edema confined to the symptomatic leg thorn1
Collateral superficial veins (non varicose) thorn1
Previously documented DVT thorn1
Alternative diagnosis at least as likely as DVT -2
Three-level Wells score
Low lt1
Intermediate 1ndash2
High gt2
Two-level Wells score
Unlikely lt_1
Likely gt_2
4 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
In patients with severe renal failure (creatinine clearance lt30
mLmin) unstable renal function or high bleeding risk iv unfrac-tionated heparin (UFH) may be preferable (short half-life and pro-tamine sulfate reversibility) Less solid is the evidence in favor ofUFH in obese (BMI gt40 kgm2) and underweight patients (lt50 kg)Main disadvantage of UFH is its inter-individual dose variabilityrequiring laboratory monitoring and dose adjustment AdditionallyUFH is associated with high risk of heparin-induced thrombocyto-penia For these reasons low-molecular weight heparin (LMWH)is the parenteral treatment of choice LMWHs are at least as effect-ive as UFH and probably safer40 Fondaparinux can also be used asparenteral agent41 Both LMWH and fondaparinux do not havespecific antidote
Recently DOACs have emerged as valid options for DVT treat-ment39 Dabigatran and edoxaban were studied following initial 7ndash9days treatment with a parenteral agent Apixaban and rivaroxabanwere evaluated by the lsquosingle drug approachrsquo (Figure 3)
DOACs have longer elimination half-lives than UFH or LMWHand may accumulate in patients with suboptimal renal (creatinineclearance lt30 mLmin) or hepatic function (Child-Pugh class B or C)Patients with poor renal andor hepatic function pregnancylactationthrombocytopenia were excluded from Phase III studies Patientswith active cancer were scarcely represented (3ndash8 of entire studypopulation)
DOACs are at least as effective as and probably safer than paren-teral drugVKA treatment42 A meta-analysis (27023 patients)showed similar VTE recurrence rates in patients receiving DOACsor conventional therapy (20 vs 22 RR 090) Major bleeding (RR061) fatal bleeding (RR 036) intracranial bleeding (RR 037) andclinically relevant non-major bleeding (RR 073) were significantlylower in DOACs-treated patients42 DOACs reversal agents arebeing investigated Idarucizumab (Dabigatran reversal agent) is cur-rently available for clinical use4344
Thrombolysisthrombectomy
Early clot removal may prevent at least partly PTS developement45
Catheter-directed thrombolysis (CDT) is more efficient than sys-temic lysis mainly due to less bleeding as thrombolytic agent is directlyadministered within the clot Three major randomized controlled trialscompared different CDT modalities on top of anticoagulation andcompression with a control group (anticoagulation and compressiononly) The CAVENT trial included 209 patients with first-time acuteDVT (iliac common femoral andor upper femoral vein)46 AdjuvantCDT was associated with a 26 RR PTS reduction over 2 years (411vs 556 P = 004) compared with anticoagulation alone46 Amount ofresidual post-CDT thrombus correlated with venous patency rates at24-months (P = 004) Persistence of venous patency at 6 and 24months correlated with PTS freedom (P lt 0001) A 32 of patientshad major bleed but there were no intracranial bleeds or deathsOverall trial found no differences in long-term (2 years) quality of lifebetween patients with- or without CDT Results have been confirmedafter 5 years follow-up47
Mechanical thrombus removal alone is not successful and needsadjuvant thrombolytic therapy In PEARL I and II studies only 5 ofpatients were treated without thrombolytics48
Up to 83 of patients treated by any catheter-based therapy needadjunctive angioplasty and stenting49 Primary acute DVT stenting isnot recommended due to lack of data
Vena cava filter
Vena cava filter may be used when anticoagulation is absolutely contra-indicated in patients with newly diagnosed proximal DVT One majorcomplication is filter thrombosis Therefore anticoagulation should bestarted as soon as contraindications resolve50 and retrievable filter rap-idly removed Filter placement in addition to anticoagulation does notimprove survival5152 except in patients with hemodynamically unstablePE or after thrombolytic therapy53 Increased DVT recurrence hasbeen shown with permanent51 but not with retrievable filters52
Compression
Goal of compression is to relieve venous symptoms and eventuallyprevent PTS54
Elastic compression stockings efficacy has been challenged by theSOX trial55 A total of 806 patients with proximal DVT have beenrandomized to either 30ndash40 mmHg or placebo (lt5 mmHg) stock-ings Cumulative 2 years PTS incidence was similar (526 vs 523HR= 10) No difference in PTS severity or quality-of-life was observ-ed55 However compliance definition (stockings wearing for gt_3 daysweek) was significantly lower than in previous studies (56vs90)56 Although role of stockings in PTS prevention may be un-certain their use remains a reasonable option for controlling symp-toms of acute proximal DVT57
Compression associated with early mobilization and walking exer-cise has shown significant efficacy in venous symptom relieve in pa-tients with acute DVT58 Caution should be used in patients withsevere peripheral artery disease
Home vs in-hospital management
Most patients with DVT may be treated on a home basis (seeSupplementary material online only section)
Deep vein thrombosis with pulmonaryembolismManagement of patients with acute PE is described in the 2014 ESCguideline6 (summary in the see Supplementary material online onlysection)
Isolated distal deep vein thrombosisWhether isolated distal DVT should be treated with anticoagulationis still debated A recent trial randomized patients with a first isolateddistal DVT to LMWH or placebo for 42 days59 Rate of symptomaticproximal DVT or PE at 42 days was not different between LMWHand placebo (33 vs 54) major or clinically relevant non-majorbleeding occurred more frequently in the LMWH group (5 vs 0P = 003) These data seem to support that not all isolated distal DVTshould receive full-dose anticoagulation
Approach is to anticoagulate full-dose for at least 3 months as forproximal DVTs patients at high-risk VTE (Table 3)60 Shorter LMWHtreatment (4ndash6 weeks) even at lower doses or ultrasound surveil-lance could be effective and safe in low-risk patients (Table 3)61 Nodata are available on DOACs All patients with acute isolated distal
Diagnosis and management of acute DVT 5
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
DVT should be recommended to wear elastic stockings6263 Follow-up VUS is recommended to monitor thrombosis progressionevolu-tion both in the presence or absence of anticoagulation
Incidence of recurrent VTE appears to be similar to that of patientswith proximal DVT6465
Consensus statement initial and long-term
managementbull Patients with proximal DVT should be anticoagulated for at least
3-monthsbull Patients with isolated distal DVT at high-risk of recurrence should
be anticoagulated as for proximal DVT for those at low risk ofrecurrence shorter treatment (4ndash6 weeks) even at lower anti-coagulant doses or ultrasound surveillance may be considered
bull In the absence of contraindications DOACs should be preferredas first-line anticoagulant therapy in non-cancer patients with pro-ximal DVT
bull Adjuvant CDT may be considered in selected patients with ilio-common femoral DVT symptoms lt14 days and life expectancygt1 year if performed in experienced centres
bull Primary acute DVT stenting or mechanical thrombus removalalone are not recommended
bull Vena cava filters may be considered if anticoagulation is contraindi-cated their use in addition to anticoagulation is notrecommended
bull Compression therapy associated with early mobilization and walk-ing exercise should be considered to relieve acute venoussymptoms
Extended phase management(beyond first 3ndash6 months)
Duration of anticoagulationOnce anticoagulation is stopped risk of VTE recurrence over yearsafter a first episode is consistently around 3066 Risk is more thandoubled in patients with unprovoked (annual rate gt70) vs those with(transient) provoked VTE67 and among the latter in medical rather
Table 3 Conditions or risk factors for complicationsafter a first isolated distal DVT
High-risk conditions Low-risk conditions
Previous VTE events Isolated distal DVT second-
ary to surgery or other
transient risk factors (plas-
ters immobilization
trauma long trip etc)
provided complete
mobilization is achieved
Males Isolated distal DVT occurring
during contraceptive or
replacement hormonal
therapy (provided therapy
has been interrupted)
Age gt50 years
Cancer
Unprovoked isolated distal DVT
Secondary isolated distal DVT with
persistently hampered mobilization
Isolated distal DVT involving the
popliteal trifurcation
Isolated distal DVT involving gt1 calf vein
Isolated distal DVT present in both legs
Presence of predisposing diseases
(eg inflammatory bowel diseases)
Known thrombophilic alterations
Axial vs Muscular isolated distal DVT
Table 4 Risk of recurrence after a first episode of unprovoked VTE
Risk factors for DVTrecurrence
Proximal DVT location Male sex Persistence of residual vein thrombosis at ultrasound
Obesity Non-zero blood group High D-dimer values
Old age Early PTS development Role of inherited thrombophilia is controversial
Clinical prediction rules assessing risk of recurrent VTE after first episode of unprovoked VTE71
Score Vienna prediction model DASH score HERDOO-2
Parameters bull D-dimer level at 3 weeks
and 3 9 15 24 months after
stopping anticoagulationbull Male sexbull VTE location (Distal DVT
Proximal DVT PE)
bull Abnormal D-dimer 3ndash5 weeks after
stopping anticoagulationbull Male sexbull Agelt50 yearsbull VTE not associated with
oestrogen-progestatif therapy
in women
bull Abnormal D-dimer before
stopping anticoagulationbull Post thrombotic symptoms
(hyperpigmentation edema
and redness)bull Age gt_65 yearsbull BMI gt_30
Validation study Yes Yes Yes
Commentaries Different nomograms are available
to calculate risk of VTE recurrence
at different time
Patients with low score (lt_1) have
an annual
recurrence rate of 31
It is applicable in women only
Women with low score (lt_1)
have an annual recurrence rate of 13
6 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
than surgical patients68 Patients with a first symptomatic unprovokedDVT are at higher risk of recurrence than those with a first unpro-voked PE69 Factors related to DVT recurrence are listed in Table 4
For proximal DVT andor PE 3-months anticoagulation is the bestoption if transient and reversible risk factors were present70 In allother patients prolonging anticoagulation protects from recurrence(70ndash90) but exposes to risk of unpredictable bleeding complica-tions Decision to discontinue or not anticoagulation should there-fore be individually tailored and balanced against bleeding risk takingalso into account patientsrsquo preferences Three clinical prediction ruleshave been derived and prospectively validated to detect low-recurrence risk patients (Table 4)71 A number of bleeding scoreswere evaluated none showed sufficient predictive accuracy or hadsufficient validation to be recommended in routine clinicalpractice7273
Continuing indefinite anticoagulation with the same drug adminis-tered during the first months is the best option for patients with mul-tiple VTE episodes or strong VTE familial history those with majorthrombophilia or longstanding medical diseases at high thromboticrisk70 Indefinite anticoagulation can also be considered in patientswith first episode of unprovoked VTE especially in those with severepresentation provided they are at low bleeding risk70 Finally discon-tinuing anticoagulation in non-cancer patients with repeatedly nega-tive D-dimer (before drug interruption 15 30 60 and 90 daysfollowing interruption) has proved to be safe in patients with unpro-voked proximal DVT provided veins are recanalized or remained sta-ble for 1 year74 However using moderately sensitive D-dimer assayduring and 30 days after stopping anticoagulation these results werenot confirmed in men and in women with VTE not associated withoestrogen treatment75 Similarly when measurements were re-peated using a quantitative assay D-dimer testing failed to identifysubgroups with very low recurrence rate76
AntithromboticsVitamin K antagonists
Four randomized studies evaluated VKA [target international normal-ized ratio (INR) 20ndash30] for VTE extended treatment in patientscompleting 3-months anticoagulation77ndash80 Recurrent VTE occurredless in the VKA groups (combined OR 007)81 Bleeding was signifi-cantly higher81
The ELATE study82 randomized patients to conventional intensity(INR 20ndash30) or low-intensity (INR 15ndash1ndash9) Recurrence rate was07 vs 19100 patient-years respectively (HR 28) with no differencein major bleeding Yet the low-intensity VKA therapy should bediscouraged
Direct oral anticoagulants
Dabigatran (150 mg bid) was as effective as warfarin and more ef-fective than placebo in preventing recurrent VTE (Table 5) Risk ofmajor bleeding was reduced compared with warfarin83
With Rivaroxaban (20 mg od) risk of VTE recurrence was lowercompared with placebo (HR 019) while bleeding risk was notincreased (Table 5)84 Standard and lower dose (10 mg od) also signif-icantly reduced risk of recurrence compared to aspirine without sig-nificant increase in bleeding85
VTE recurrence occurred significantly less in standard and lowerdose Apixaban (5 and 25 mg bid) vs placebo (Table 5) Bleeding didnot differ between groups86
Recurrence rates with Edoxaban 60 mg were similar to thewarfarin-treated group (post hoc analysis) (Table 5)87 Major bleedingwas lower in the edoxaban group
Data from Phase IV studies are scarce but results from XALIA areconsistent with observations of rivaroxaban and warfarin88
Aspirin
Two studies investigated aspirin 100 mg vs placebo in patients withidiopathic VTE who completed initial anticoagulation treatment8990
Pooled HR for VTE recurrence was 068 and 147 for bleeding91
Other
Recent evaluation of Sulodexide vs placebo in patients with unpro-voked VTE who completed standard course of anticoagulationshowed a HR for VTE recurrence of 049 (P = 002)92 No majorbleeding episodes were observed
Venous occlusion recanalizationEndovascular techniques are available for selected patients withPTS57 Case series and prospective cohort trials suggest that at leastsome subgroups of PTS patients (CEAP classes 4ndash6 Figure 4) maybenefit from addition of endovascular therapy into overall manage-ment strategy
In patients with moderate-to-severe PTS and iliac vein obstructionendovascular stent placement may be used to restore vein patencyIn preliminary studies stent placement in chronically occluded iliacveins contributed to ulcers healing PTS symptoms relief and reducedobstructive venous sequel93
No randomized controlled trials are available the largest seriesfound patients with moderate-to-severe PTS to have reduced pain(P lt 00001) severe pain (from 41 to 11) and severe swelling(from 36 to 18) increased ulcer healing (68) and reduced ven-ous pressure following recanalization with stent placement93
Claudication improvement better outflow fraction and calf pumpfunction was also observed94
In selected infrequent cases surgical vein bypass may be an optionto relieve venous hypertension
Follow-upPatients with DVT should be followed to avoid risk of recurrence aswell as DVT and anticoagulation-related complicationsDevelopment of renal failure changes in body weight or pregnancythat may require anticoagulation adjustment should be monitoredCompliance as well as benefitrisk balance should be assessed regu-larly VUS at anticoagulation discontinuation is useful in determiningbaseline residual vein thrombosis
Consensus statement extended managementbull Decision to discontinue or not anticoagulation should be individu-
ally tailored balancing risk of recurrence against bleeding risk tak-ing into account patientsrsquo preferences and compliance
bull In the absence of contraindications DOACs should be preferredas first line anticoagulant therapy in non-cancer patients Currently
Diagnosis and management of acute DVT 7
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

therapy CUS diagnostic yield is high in the presence of clinical DVTsigns32 Among unselected PE patients proximal DVT at CUS is foundin 17 patients33 Proximal DVT has high specificity and may justifytreatment even if pulmonary CT is negative6 While negative CUS can-not exclude PE it can justify withholding anticoagulation in patientswith non-diagnostic ventilationperfusion scan and PE-unlikely163435
In symptomatic patients with isolated sub-segmental PE or inciden-tal asymptomatic PE concomitant DVT justifies anticoagulation3637
Deep vein thrombosis imaging may also be useful if secondarily a pa-tient is suspected of VTE recurrence with DVT signs Moreoverpresence of concomitant DVT has been suggested as an independent30-days death risk factor following PE38
Consensus statement diagnosisbull Clinical prediction rule (two-level modified Wells score) is recom-
mended to stratify patients with suspected lower limb DVTbull ELISA D-dimer measurement is recommended in lsquounlikelyrsquo clinical
probability patients to exclude DVTbull Venous US is recommended as first line imaging method for DVT
diagnosisbull Venous CT scan should be reserved to selected patients onlybull Venous US should be proposed also in case of confirmed PE for
initial reference venous imaging useful in case of DVT recurrencesuspicion or further stratification in selected patients
bull Venous US may be considered for further stratification in selectedpatients with concomitant suspected PE
Initial (first 5ndash21 days) and long-term (first 3ndash6 months) phasemanagement
Deep vein thrombosis withoutpulmonary embolismAnticoagulation in non-cancer patients
Deep vein thrombosis treatment consists of three phases (Figure 3)39
Initial treatment (5ndash21 days following diagnosis) during this period pa-tients receive either parenteral therapy and are transited to vitamin K an-tagonists (VKA) or use high-dose direct oral anticoagulants (DOACs)Long-term treatment (following 3ndash6 months) patients are treated withVKA or DOACs39 Initial and long-term treatments are mandatory forall DVT patients Decision of extended treatment (beyond first 3ndash6months) is based on benefitrisk balance of continued anticoagulation
Initial treatment(first 5-21 days)
Long term treatment
(first 3-6 months)
Extended treatment
(following initial 3-6 months)
Apixaban 10 mg bid for 7 days Apixaban 5mg bid Apixaban 25mg bid beyond 6 months
Dabigatran 150 mg bid preceded by LMWH for 5-10 days
Edoxaban 60 mg od (30mg od if ClCreat 50-30ltmlmin or concomitant potent P-P inhibitors) preceded by LMWH for 5-10 days
Rivaroxaban 15 mg bid for 21 days Rivaroxaban 20mg od Rivaroxaban 10 mg or 20 mg od beyond 6 months
VKA to achieve INR 2-3 preceded by LMWH for 5-10 days
Figure 3 Deep vein thrombosis treatment phases ClCreat creatinine clearance LMWH low molecular weight heparin P-P inhibitors protonpump inhibitors VKA vitamin K antantagonist
Table 2 The Wells score1213
Clinical variable Points
Active cancer (treatment ongoing or within previous 6
months or palliative)
thorn1
Paralysis paresis or recent plaster immobilization of
the lower extremities
thorn1
Recently bedridden for 3 days or more or major sur-
gery within the previous 12 weeks requiring general
or regional anesthesia
thorn1
Localized tenderness along the distribution of the deep
venous system
thorn1
Entire leg swelling thorn1
Calf swelling at least 3 cm larger than that on the
asymptomatic leg (measured 10 cm below the tibial
tuberosity)
thorn1
Pitting edema confined to the symptomatic leg thorn1
Collateral superficial veins (non varicose) thorn1
Previously documented DVT thorn1
Alternative diagnosis at least as likely as DVT -2
Three-level Wells score
Low lt1
Intermediate 1ndash2
High gt2
Two-level Wells score
Unlikely lt_1
Likely gt_2
4 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
In patients with severe renal failure (creatinine clearance lt30
mLmin) unstable renal function or high bleeding risk iv unfrac-tionated heparin (UFH) may be preferable (short half-life and pro-tamine sulfate reversibility) Less solid is the evidence in favor ofUFH in obese (BMI gt40 kgm2) and underweight patients (lt50 kg)Main disadvantage of UFH is its inter-individual dose variabilityrequiring laboratory monitoring and dose adjustment AdditionallyUFH is associated with high risk of heparin-induced thrombocyto-penia For these reasons low-molecular weight heparin (LMWH)is the parenteral treatment of choice LMWHs are at least as effect-ive as UFH and probably safer40 Fondaparinux can also be used asparenteral agent41 Both LMWH and fondaparinux do not havespecific antidote
Recently DOACs have emerged as valid options for DVT treat-ment39 Dabigatran and edoxaban were studied following initial 7ndash9days treatment with a parenteral agent Apixaban and rivaroxabanwere evaluated by the lsquosingle drug approachrsquo (Figure 3)
DOACs have longer elimination half-lives than UFH or LMWHand may accumulate in patients with suboptimal renal (creatinineclearance lt30 mLmin) or hepatic function (Child-Pugh class B or C)Patients with poor renal andor hepatic function pregnancylactationthrombocytopenia were excluded from Phase III studies Patientswith active cancer were scarcely represented (3ndash8 of entire studypopulation)
DOACs are at least as effective as and probably safer than paren-teral drugVKA treatment42 A meta-analysis (27023 patients)showed similar VTE recurrence rates in patients receiving DOACsor conventional therapy (20 vs 22 RR 090) Major bleeding (RR061) fatal bleeding (RR 036) intracranial bleeding (RR 037) andclinically relevant non-major bleeding (RR 073) were significantlylower in DOACs-treated patients42 DOACs reversal agents arebeing investigated Idarucizumab (Dabigatran reversal agent) is cur-rently available for clinical use4344
Thrombolysisthrombectomy
Early clot removal may prevent at least partly PTS developement45
Catheter-directed thrombolysis (CDT) is more efficient than sys-temic lysis mainly due to less bleeding as thrombolytic agent is directlyadministered within the clot Three major randomized controlled trialscompared different CDT modalities on top of anticoagulation andcompression with a control group (anticoagulation and compressiononly) The CAVENT trial included 209 patients with first-time acuteDVT (iliac common femoral andor upper femoral vein)46 AdjuvantCDT was associated with a 26 RR PTS reduction over 2 years (411vs 556 P = 004) compared with anticoagulation alone46 Amount ofresidual post-CDT thrombus correlated with venous patency rates at24-months (P = 004) Persistence of venous patency at 6 and 24months correlated with PTS freedom (P lt 0001) A 32 of patientshad major bleed but there were no intracranial bleeds or deathsOverall trial found no differences in long-term (2 years) quality of lifebetween patients with- or without CDT Results have been confirmedafter 5 years follow-up47
Mechanical thrombus removal alone is not successful and needsadjuvant thrombolytic therapy In PEARL I and II studies only 5 ofpatients were treated without thrombolytics48
Up to 83 of patients treated by any catheter-based therapy needadjunctive angioplasty and stenting49 Primary acute DVT stenting isnot recommended due to lack of data
Vena cava filter
Vena cava filter may be used when anticoagulation is absolutely contra-indicated in patients with newly diagnosed proximal DVT One majorcomplication is filter thrombosis Therefore anticoagulation should bestarted as soon as contraindications resolve50 and retrievable filter rap-idly removed Filter placement in addition to anticoagulation does notimprove survival5152 except in patients with hemodynamically unstablePE or after thrombolytic therapy53 Increased DVT recurrence hasbeen shown with permanent51 but not with retrievable filters52
Compression
Goal of compression is to relieve venous symptoms and eventuallyprevent PTS54
Elastic compression stockings efficacy has been challenged by theSOX trial55 A total of 806 patients with proximal DVT have beenrandomized to either 30ndash40 mmHg or placebo (lt5 mmHg) stock-ings Cumulative 2 years PTS incidence was similar (526 vs 523HR= 10) No difference in PTS severity or quality-of-life was observ-ed55 However compliance definition (stockings wearing for gt_3 daysweek) was significantly lower than in previous studies (56vs90)56 Although role of stockings in PTS prevention may be un-certain their use remains a reasonable option for controlling symp-toms of acute proximal DVT57
Compression associated with early mobilization and walking exer-cise has shown significant efficacy in venous symptom relieve in pa-tients with acute DVT58 Caution should be used in patients withsevere peripheral artery disease
Home vs in-hospital management
Most patients with DVT may be treated on a home basis (seeSupplementary material online only section)
Deep vein thrombosis with pulmonaryembolismManagement of patients with acute PE is described in the 2014 ESCguideline6 (summary in the see Supplementary material online onlysection)
Isolated distal deep vein thrombosisWhether isolated distal DVT should be treated with anticoagulationis still debated A recent trial randomized patients with a first isolateddistal DVT to LMWH or placebo for 42 days59 Rate of symptomaticproximal DVT or PE at 42 days was not different between LMWHand placebo (33 vs 54) major or clinically relevant non-majorbleeding occurred more frequently in the LMWH group (5 vs 0P = 003) These data seem to support that not all isolated distal DVTshould receive full-dose anticoagulation
Approach is to anticoagulate full-dose for at least 3 months as forproximal DVTs patients at high-risk VTE (Table 3)60 Shorter LMWHtreatment (4ndash6 weeks) even at lower doses or ultrasound surveil-lance could be effective and safe in low-risk patients (Table 3)61 Nodata are available on DOACs All patients with acute isolated distal
Diagnosis and management of acute DVT 5
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
DVT should be recommended to wear elastic stockings6263 Follow-up VUS is recommended to monitor thrombosis progressionevolu-tion both in the presence or absence of anticoagulation
Incidence of recurrent VTE appears to be similar to that of patientswith proximal DVT6465
Consensus statement initial and long-term
managementbull Patients with proximal DVT should be anticoagulated for at least
3-monthsbull Patients with isolated distal DVT at high-risk of recurrence should
be anticoagulated as for proximal DVT for those at low risk ofrecurrence shorter treatment (4ndash6 weeks) even at lower anti-coagulant doses or ultrasound surveillance may be considered
bull In the absence of contraindications DOACs should be preferredas first-line anticoagulant therapy in non-cancer patients with pro-ximal DVT
bull Adjuvant CDT may be considered in selected patients with ilio-common femoral DVT symptoms lt14 days and life expectancygt1 year if performed in experienced centres
bull Primary acute DVT stenting or mechanical thrombus removalalone are not recommended
bull Vena cava filters may be considered if anticoagulation is contraindi-cated their use in addition to anticoagulation is notrecommended
bull Compression therapy associated with early mobilization and walk-ing exercise should be considered to relieve acute venoussymptoms
Extended phase management(beyond first 3ndash6 months)
Duration of anticoagulationOnce anticoagulation is stopped risk of VTE recurrence over yearsafter a first episode is consistently around 3066 Risk is more thandoubled in patients with unprovoked (annual rate gt70) vs those with(transient) provoked VTE67 and among the latter in medical rather
Table 3 Conditions or risk factors for complicationsafter a first isolated distal DVT
High-risk conditions Low-risk conditions
Previous VTE events Isolated distal DVT second-
ary to surgery or other
transient risk factors (plas-
ters immobilization
trauma long trip etc)
provided complete
mobilization is achieved
Males Isolated distal DVT occurring
during contraceptive or
replacement hormonal
therapy (provided therapy
has been interrupted)
Age gt50 years
Cancer
Unprovoked isolated distal DVT
Secondary isolated distal DVT with
persistently hampered mobilization
Isolated distal DVT involving the
popliteal trifurcation
Isolated distal DVT involving gt1 calf vein
Isolated distal DVT present in both legs
Presence of predisposing diseases
(eg inflammatory bowel diseases)
Known thrombophilic alterations
Axial vs Muscular isolated distal DVT
Table 4 Risk of recurrence after a first episode of unprovoked VTE
Risk factors for DVTrecurrence
Proximal DVT location Male sex Persistence of residual vein thrombosis at ultrasound
Obesity Non-zero blood group High D-dimer values
Old age Early PTS development Role of inherited thrombophilia is controversial
Clinical prediction rules assessing risk of recurrent VTE after first episode of unprovoked VTE71
Score Vienna prediction model DASH score HERDOO-2
Parameters bull D-dimer level at 3 weeks
and 3 9 15 24 months after
stopping anticoagulationbull Male sexbull VTE location (Distal DVT
Proximal DVT PE)
bull Abnormal D-dimer 3ndash5 weeks after
stopping anticoagulationbull Male sexbull Agelt50 yearsbull VTE not associated with
oestrogen-progestatif therapy
in women
bull Abnormal D-dimer before
stopping anticoagulationbull Post thrombotic symptoms
(hyperpigmentation edema
and redness)bull Age gt_65 yearsbull BMI gt_30
Validation study Yes Yes Yes
Commentaries Different nomograms are available
to calculate risk of VTE recurrence
at different time
Patients with low score (lt_1) have
an annual
recurrence rate of 31
It is applicable in women only
Women with low score (lt_1)
have an annual recurrence rate of 13
6 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
than surgical patients68 Patients with a first symptomatic unprovokedDVT are at higher risk of recurrence than those with a first unpro-voked PE69 Factors related to DVT recurrence are listed in Table 4
For proximal DVT andor PE 3-months anticoagulation is the bestoption if transient and reversible risk factors were present70 In allother patients prolonging anticoagulation protects from recurrence(70ndash90) but exposes to risk of unpredictable bleeding complica-tions Decision to discontinue or not anticoagulation should there-fore be individually tailored and balanced against bleeding risk takingalso into account patientsrsquo preferences Three clinical prediction ruleshave been derived and prospectively validated to detect low-recurrence risk patients (Table 4)71 A number of bleeding scoreswere evaluated none showed sufficient predictive accuracy or hadsufficient validation to be recommended in routine clinicalpractice7273
Continuing indefinite anticoagulation with the same drug adminis-tered during the first months is the best option for patients with mul-tiple VTE episodes or strong VTE familial history those with majorthrombophilia or longstanding medical diseases at high thromboticrisk70 Indefinite anticoagulation can also be considered in patientswith first episode of unprovoked VTE especially in those with severepresentation provided they are at low bleeding risk70 Finally discon-tinuing anticoagulation in non-cancer patients with repeatedly nega-tive D-dimer (before drug interruption 15 30 60 and 90 daysfollowing interruption) has proved to be safe in patients with unpro-voked proximal DVT provided veins are recanalized or remained sta-ble for 1 year74 However using moderately sensitive D-dimer assayduring and 30 days after stopping anticoagulation these results werenot confirmed in men and in women with VTE not associated withoestrogen treatment75 Similarly when measurements were re-peated using a quantitative assay D-dimer testing failed to identifysubgroups with very low recurrence rate76
AntithromboticsVitamin K antagonists
Four randomized studies evaluated VKA [target international normal-ized ratio (INR) 20ndash30] for VTE extended treatment in patientscompleting 3-months anticoagulation77ndash80 Recurrent VTE occurredless in the VKA groups (combined OR 007)81 Bleeding was signifi-cantly higher81
The ELATE study82 randomized patients to conventional intensity(INR 20ndash30) or low-intensity (INR 15ndash1ndash9) Recurrence rate was07 vs 19100 patient-years respectively (HR 28) with no differencein major bleeding Yet the low-intensity VKA therapy should bediscouraged
Direct oral anticoagulants
Dabigatran (150 mg bid) was as effective as warfarin and more ef-fective than placebo in preventing recurrent VTE (Table 5) Risk ofmajor bleeding was reduced compared with warfarin83
With Rivaroxaban (20 mg od) risk of VTE recurrence was lowercompared with placebo (HR 019) while bleeding risk was notincreased (Table 5)84 Standard and lower dose (10 mg od) also signif-icantly reduced risk of recurrence compared to aspirine without sig-nificant increase in bleeding85
VTE recurrence occurred significantly less in standard and lowerdose Apixaban (5 and 25 mg bid) vs placebo (Table 5) Bleeding didnot differ between groups86
Recurrence rates with Edoxaban 60 mg were similar to thewarfarin-treated group (post hoc analysis) (Table 5)87 Major bleedingwas lower in the edoxaban group
Data from Phase IV studies are scarce but results from XALIA areconsistent with observations of rivaroxaban and warfarin88
Aspirin
Two studies investigated aspirin 100 mg vs placebo in patients withidiopathic VTE who completed initial anticoagulation treatment8990
Pooled HR for VTE recurrence was 068 and 147 for bleeding91
Other
Recent evaluation of Sulodexide vs placebo in patients with unpro-voked VTE who completed standard course of anticoagulationshowed a HR for VTE recurrence of 049 (P = 002)92 No majorbleeding episodes were observed
Venous occlusion recanalizationEndovascular techniques are available for selected patients withPTS57 Case series and prospective cohort trials suggest that at leastsome subgroups of PTS patients (CEAP classes 4ndash6 Figure 4) maybenefit from addition of endovascular therapy into overall manage-ment strategy
In patients with moderate-to-severe PTS and iliac vein obstructionendovascular stent placement may be used to restore vein patencyIn preliminary studies stent placement in chronically occluded iliacveins contributed to ulcers healing PTS symptoms relief and reducedobstructive venous sequel93
No randomized controlled trials are available the largest seriesfound patients with moderate-to-severe PTS to have reduced pain(P lt 00001) severe pain (from 41 to 11) and severe swelling(from 36 to 18) increased ulcer healing (68) and reduced ven-ous pressure following recanalization with stent placement93
Claudication improvement better outflow fraction and calf pumpfunction was also observed94
In selected infrequent cases surgical vein bypass may be an optionto relieve venous hypertension
Follow-upPatients with DVT should be followed to avoid risk of recurrence aswell as DVT and anticoagulation-related complicationsDevelopment of renal failure changes in body weight or pregnancythat may require anticoagulation adjustment should be monitoredCompliance as well as benefitrisk balance should be assessed regu-larly VUS at anticoagulation discontinuation is useful in determiningbaseline residual vein thrombosis
Consensus statement extended managementbull Decision to discontinue or not anticoagulation should be individu-
ally tailored balancing risk of recurrence against bleeding risk tak-ing into account patientsrsquo preferences and compliance
bull In the absence of contraindications DOACs should be preferredas first line anticoagulant therapy in non-cancer patients Currently
Diagnosis and management of acute DVT 7
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

In patients with severe renal failure (creatinine clearance lt30
mLmin) unstable renal function or high bleeding risk iv unfrac-tionated heparin (UFH) may be preferable (short half-life and pro-tamine sulfate reversibility) Less solid is the evidence in favor ofUFH in obese (BMI gt40 kgm2) and underweight patients (lt50 kg)Main disadvantage of UFH is its inter-individual dose variabilityrequiring laboratory monitoring and dose adjustment AdditionallyUFH is associated with high risk of heparin-induced thrombocyto-penia For these reasons low-molecular weight heparin (LMWH)is the parenteral treatment of choice LMWHs are at least as effect-ive as UFH and probably safer40 Fondaparinux can also be used asparenteral agent41 Both LMWH and fondaparinux do not havespecific antidote
Recently DOACs have emerged as valid options for DVT treat-ment39 Dabigatran and edoxaban were studied following initial 7ndash9days treatment with a parenteral agent Apixaban and rivaroxabanwere evaluated by the lsquosingle drug approachrsquo (Figure 3)
DOACs have longer elimination half-lives than UFH or LMWHand may accumulate in patients with suboptimal renal (creatinineclearance lt30 mLmin) or hepatic function (Child-Pugh class B or C)Patients with poor renal andor hepatic function pregnancylactationthrombocytopenia were excluded from Phase III studies Patientswith active cancer were scarcely represented (3ndash8 of entire studypopulation)
DOACs are at least as effective as and probably safer than paren-teral drugVKA treatment42 A meta-analysis (27023 patients)showed similar VTE recurrence rates in patients receiving DOACsor conventional therapy (20 vs 22 RR 090) Major bleeding (RR061) fatal bleeding (RR 036) intracranial bleeding (RR 037) andclinically relevant non-major bleeding (RR 073) were significantlylower in DOACs-treated patients42 DOACs reversal agents arebeing investigated Idarucizumab (Dabigatran reversal agent) is cur-rently available for clinical use4344
Thrombolysisthrombectomy
Early clot removal may prevent at least partly PTS developement45
Catheter-directed thrombolysis (CDT) is more efficient than sys-temic lysis mainly due to less bleeding as thrombolytic agent is directlyadministered within the clot Three major randomized controlled trialscompared different CDT modalities on top of anticoagulation andcompression with a control group (anticoagulation and compressiononly) The CAVENT trial included 209 patients with first-time acuteDVT (iliac common femoral andor upper femoral vein)46 AdjuvantCDT was associated with a 26 RR PTS reduction over 2 years (411vs 556 P = 004) compared with anticoagulation alone46 Amount ofresidual post-CDT thrombus correlated with venous patency rates at24-months (P = 004) Persistence of venous patency at 6 and 24months correlated with PTS freedom (P lt 0001) A 32 of patientshad major bleed but there were no intracranial bleeds or deathsOverall trial found no differences in long-term (2 years) quality of lifebetween patients with- or without CDT Results have been confirmedafter 5 years follow-up47
Mechanical thrombus removal alone is not successful and needsadjuvant thrombolytic therapy In PEARL I and II studies only 5 ofpatients were treated without thrombolytics48
Up to 83 of patients treated by any catheter-based therapy needadjunctive angioplasty and stenting49 Primary acute DVT stenting isnot recommended due to lack of data
Vena cava filter
Vena cava filter may be used when anticoagulation is absolutely contra-indicated in patients with newly diagnosed proximal DVT One majorcomplication is filter thrombosis Therefore anticoagulation should bestarted as soon as contraindications resolve50 and retrievable filter rap-idly removed Filter placement in addition to anticoagulation does notimprove survival5152 except in patients with hemodynamically unstablePE or after thrombolytic therapy53 Increased DVT recurrence hasbeen shown with permanent51 but not with retrievable filters52
Compression
Goal of compression is to relieve venous symptoms and eventuallyprevent PTS54
Elastic compression stockings efficacy has been challenged by theSOX trial55 A total of 806 patients with proximal DVT have beenrandomized to either 30ndash40 mmHg or placebo (lt5 mmHg) stock-ings Cumulative 2 years PTS incidence was similar (526 vs 523HR= 10) No difference in PTS severity or quality-of-life was observ-ed55 However compliance definition (stockings wearing for gt_3 daysweek) was significantly lower than in previous studies (56vs90)56 Although role of stockings in PTS prevention may be un-certain their use remains a reasonable option for controlling symp-toms of acute proximal DVT57
Compression associated with early mobilization and walking exer-cise has shown significant efficacy in venous symptom relieve in pa-tients with acute DVT58 Caution should be used in patients withsevere peripheral artery disease
Home vs in-hospital management
Most patients with DVT may be treated on a home basis (seeSupplementary material online only section)
Deep vein thrombosis with pulmonaryembolismManagement of patients with acute PE is described in the 2014 ESCguideline6 (summary in the see Supplementary material online onlysection)
Isolated distal deep vein thrombosisWhether isolated distal DVT should be treated with anticoagulationis still debated A recent trial randomized patients with a first isolateddistal DVT to LMWH or placebo for 42 days59 Rate of symptomaticproximal DVT or PE at 42 days was not different between LMWHand placebo (33 vs 54) major or clinically relevant non-majorbleeding occurred more frequently in the LMWH group (5 vs 0P = 003) These data seem to support that not all isolated distal DVTshould receive full-dose anticoagulation
Approach is to anticoagulate full-dose for at least 3 months as forproximal DVTs patients at high-risk VTE (Table 3)60 Shorter LMWHtreatment (4ndash6 weeks) even at lower doses or ultrasound surveil-lance could be effective and safe in low-risk patients (Table 3)61 Nodata are available on DOACs All patients with acute isolated distal
Diagnosis and management of acute DVT 5
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
DVT should be recommended to wear elastic stockings6263 Follow-up VUS is recommended to monitor thrombosis progressionevolu-tion both in the presence or absence of anticoagulation
Incidence of recurrent VTE appears to be similar to that of patientswith proximal DVT6465
Consensus statement initial and long-term
managementbull Patients with proximal DVT should be anticoagulated for at least
3-monthsbull Patients with isolated distal DVT at high-risk of recurrence should
be anticoagulated as for proximal DVT for those at low risk ofrecurrence shorter treatment (4ndash6 weeks) even at lower anti-coagulant doses or ultrasound surveillance may be considered
bull In the absence of contraindications DOACs should be preferredas first-line anticoagulant therapy in non-cancer patients with pro-ximal DVT
bull Adjuvant CDT may be considered in selected patients with ilio-common femoral DVT symptoms lt14 days and life expectancygt1 year if performed in experienced centres
bull Primary acute DVT stenting or mechanical thrombus removalalone are not recommended
bull Vena cava filters may be considered if anticoagulation is contraindi-cated their use in addition to anticoagulation is notrecommended
bull Compression therapy associated with early mobilization and walk-ing exercise should be considered to relieve acute venoussymptoms
Extended phase management(beyond first 3ndash6 months)
Duration of anticoagulationOnce anticoagulation is stopped risk of VTE recurrence over yearsafter a first episode is consistently around 3066 Risk is more thandoubled in patients with unprovoked (annual rate gt70) vs those with(transient) provoked VTE67 and among the latter in medical rather
Table 3 Conditions or risk factors for complicationsafter a first isolated distal DVT
High-risk conditions Low-risk conditions
Previous VTE events Isolated distal DVT second-
ary to surgery or other
transient risk factors (plas-
ters immobilization
trauma long trip etc)
provided complete
mobilization is achieved
Males Isolated distal DVT occurring
during contraceptive or
replacement hormonal
therapy (provided therapy
has been interrupted)
Age gt50 years
Cancer
Unprovoked isolated distal DVT
Secondary isolated distal DVT with
persistently hampered mobilization
Isolated distal DVT involving the
popliteal trifurcation
Isolated distal DVT involving gt1 calf vein
Isolated distal DVT present in both legs
Presence of predisposing diseases
(eg inflammatory bowel diseases)
Known thrombophilic alterations
Axial vs Muscular isolated distal DVT
Table 4 Risk of recurrence after a first episode of unprovoked VTE
Risk factors for DVTrecurrence
Proximal DVT location Male sex Persistence of residual vein thrombosis at ultrasound
Obesity Non-zero blood group High D-dimer values
Old age Early PTS development Role of inherited thrombophilia is controversial
Clinical prediction rules assessing risk of recurrent VTE after first episode of unprovoked VTE71
Score Vienna prediction model DASH score HERDOO-2
Parameters bull D-dimer level at 3 weeks
and 3 9 15 24 months after
stopping anticoagulationbull Male sexbull VTE location (Distal DVT
Proximal DVT PE)
bull Abnormal D-dimer 3ndash5 weeks after
stopping anticoagulationbull Male sexbull Agelt50 yearsbull VTE not associated with
oestrogen-progestatif therapy
in women
bull Abnormal D-dimer before
stopping anticoagulationbull Post thrombotic symptoms
(hyperpigmentation edema
and redness)bull Age gt_65 yearsbull BMI gt_30
Validation study Yes Yes Yes
Commentaries Different nomograms are available
to calculate risk of VTE recurrence
at different time
Patients with low score (lt_1) have
an annual
recurrence rate of 31
It is applicable in women only
Women with low score (lt_1)
have an annual recurrence rate of 13
6 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
than surgical patients68 Patients with a first symptomatic unprovokedDVT are at higher risk of recurrence than those with a first unpro-voked PE69 Factors related to DVT recurrence are listed in Table 4
For proximal DVT andor PE 3-months anticoagulation is the bestoption if transient and reversible risk factors were present70 In allother patients prolonging anticoagulation protects from recurrence(70ndash90) but exposes to risk of unpredictable bleeding complica-tions Decision to discontinue or not anticoagulation should there-fore be individually tailored and balanced against bleeding risk takingalso into account patientsrsquo preferences Three clinical prediction ruleshave been derived and prospectively validated to detect low-recurrence risk patients (Table 4)71 A number of bleeding scoreswere evaluated none showed sufficient predictive accuracy or hadsufficient validation to be recommended in routine clinicalpractice7273
Continuing indefinite anticoagulation with the same drug adminis-tered during the first months is the best option for patients with mul-tiple VTE episodes or strong VTE familial history those with majorthrombophilia or longstanding medical diseases at high thromboticrisk70 Indefinite anticoagulation can also be considered in patientswith first episode of unprovoked VTE especially in those with severepresentation provided they are at low bleeding risk70 Finally discon-tinuing anticoagulation in non-cancer patients with repeatedly nega-tive D-dimer (before drug interruption 15 30 60 and 90 daysfollowing interruption) has proved to be safe in patients with unpro-voked proximal DVT provided veins are recanalized or remained sta-ble for 1 year74 However using moderately sensitive D-dimer assayduring and 30 days after stopping anticoagulation these results werenot confirmed in men and in women with VTE not associated withoestrogen treatment75 Similarly when measurements were re-peated using a quantitative assay D-dimer testing failed to identifysubgroups with very low recurrence rate76
AntithromboticsVitamin K antagonists
Four randomized studies evaluated VKA [target international normal-ized ratio (INR) 20ndash30] for VTE extended treatment in patientscompleting 3-months anticoagulation77ndash80 Recurrent VTE occurredless in the VKA groups (combined OR 007)81 Bleeding was signifi-cantly higher81
The ELATE study82 randomized patients to conventional intensity(INR 20ndash30) or low-intensity (INR 15ndash1ndash9) Recurrence rate was07 vs 19100 patient-years respectively (HR 28) with no differencein major bleeding Yet the low-intensity VKA therapy should bediscouraged
Direct oral anticoagulants
Dabigatran (150 mg bid) was as effective as warfarin and more ef-fective than placebo in preventing recurrent VTE (Table 5) Risk ofmajor bleeding was reduced compared with warfarin83
With Rivaroxaban (20 mg od) risk of VTE recurrence was lowercompared with placebo (HR 019) while bleeding risk was notincreased (Table 5)84 Standard and lower dose (10 mg od) also signif-icantly reduced risk of recurrence compared to aspirine without sig-nificant increase in bleeding85
VTE recurrence occurred significantly less in standard and lowerdose Apixaban (5 and 25 mg bid) vs placebo (Table 5) Bleeding didnot differ between groups86
Recurrence rates with Edoxaban 60 mg were similar to thewarfarin-treated group (post hoc analysis) (Table 5)87 Major bleedingwas lower in the edoxaban group
Data from Phase IV studies are scarce but results from XALIA areconsistent with observations of rivaroxaban and warfarin88
Aspirin
Two studies investigated aspirin 100 mg vs placebo in patients withidiopathic VTE who completed initial anticoagulation treatment8990
Pooled HR for VTE recurrence was 068 and 147 for bleeding91
Other
Recent evaluation of Sulodexide vs placebo in patients with unpro-voked VTE who completed standard course of anticoagulationshowed a HR for VTE recurrence of 049 (P = 002)92 No majorbleeding episodes were observed
Venous occlusion recanalizationEndovascular techniques are available for selected patients withPTS57 Case series and prospective cohort trials suggest that at leastsome subgroups of PTS patients (CEAP classes 4ndash6 Figure 4) maybenefit from addition of endovascular therapy into overall manage-ment strategy
In patients with moderate-to-severe PTS and iliac vein obstructionendovascular stent placement may be used to restore vein patencyIn preliminary studies stent placement in chronically occluded iliacveins contributed to ulcers healing PTS symptoms relief and reducedobstructive venous sequel93
No randomized controlled trials are available the largest seriesfound patients with moderate-to-severe PTS to have reduced pain(P lt 00001) severe pain (from 41 to 11) and severe swelling(from 36 to 18) increased ulcer healing (68) and reduced ven-ous pressure following recanalization with stent placement93
Claudication improvement better outflow fraction and calf pumpfunction was also observed94
In selected infrequent cases surgical vein bypass may be an optionto relieve venous hypertension
Follow-upPatients with DVT should be followed to avoid risk of recurrence aswell as DVT and anticoagulation-related complicationsDevelopment of renal failure changes in body weight or pregnancythat may require anticoagulation adjustment should be monitoredCompliance as well as benefitrisk balance should be assessed regu-larly VUS at anticoagulation discontinuation is useful in determiningbaseline residual vein thrombosis
Consensus statement extended managementbull Decision to discontinue or not anticoagulation should be individu-
ally tailored balancing risk of recurrence against bleeding risk tak-ing into account patientsrsquo preferences and compliance
bull In the absence of contraindications DOACs should be preferredas first line anticoagulant therapy in non-cancer patients Currently
Diagnosis and management of acute DVT 7
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

DVT should be recommended to wear elastic stockings6263 Follow-up VUS is recommended to monitor thrombosis progressionevolu-tion both in the presence or absence of anticoagulation
Incidence of recurrent VTE appears to be similar to that of patientswith proximal DVT6465
Consensus statement initial and long-term
managementbull Patients with proximal DVT should be anticoagulated for at least
3-monthsbull Patients with isolated distal DVT at high-risk of recurrence should
be anticoagulated as for proximal DVT for those at low risk ofrecurrence shorter treatment (4ndash6 weeks) even at lower anti-coagulant doses or ultrasound surveillance may be considered
bull In the absence of contraindications DOACs should be preferredas first-line anticoagulant therapy in non-cancer patients with pro-ximal DVT
bull Adjuvant CDT may be considered in selected patients with ilio-common femoral DVT symptoms lt14 days and life expectancygt1 year if performed in experienced centres
bull Primary acute DVT stenting or mechanical thrombus removalalone are not recommended
bull Vena cava filters may be considered if anticoagulation is contraindi-cated their use in addition to anticoagulation is notrecommended
bull Compression therapy associated with early mobilization and walk-ing exercise should be considered to relieve acute venoussymptoms
Extended phase management(beyond first 3ndash6 months)
Duration of anticoagulationOnce anticoagulation is stopped risk of VTE recurrence over yearsafter a first episode is consistently around 3066 Risk is more thandoubled in patients with unprovoked (annual rate gt70) vs those with(transient) provoked VTE67 and among the latter in medical rather
Table 3 Conditions or risk factors for complicationsafter a first isolated distal DVT
High-risk conditions Low-risk conditions
Previous VTE events Isolated distal DVT second-
ary to surgery or other
transient risk factors (plas-
ters immobilization
trauma long trip etc)
provided complete
mobilization is achieved
Males Isolated distal DVT occurring
during contraceptive or
replacement hormonal
therapy (provided therapy
has been interrupted)
Age gt50 years
Cancer
Unprovoked isolated distal DVT
Secondary isolated distal DVT with
persistently hampered mobilization
Isolated distal DVT involving the
popliteal trifurcation
Isolated distal DVT involving gt1 calf vein
Isolated distal DVT present in both legs
Presence of predisposing diseases
(eg inflammatory bowel diseases)
Known thrombophilic alterations
Axial vs Muscular isolated distal DVT
Table 4 Risk of recurrence after a first episode of unprovoked VTE
Risk factors for DVTrecurrence
Proximal DVT location Male sex Persistence of residual vein thrombosis at ultrasound
Obesity Non-zero blood group High D-dimer values
Old age Early PTS development Role of inherited thrombophilia is controversial
Clinical prediction rules assessing risk of recurrent VTE after first episode of unprovoked VTE71
Score Vienna prediction model DASH score HERDOO-2
Parameters bull D-dimer level at 3 weeks
and 3 9 15 24 months after
stopping anticoagulationbull Male sexbull VTE location (Distal DVT
Proximal DVT PE)
bull Abnormal D-dimer 3ndash5 weeks after
stopping anticoagulationbull Male sexbull Agelt50 yearsbull VTE not associated with
oestrogen-progestatif therapy
in women
bull Abnormal D-dimer before
stopping anticoagulationbull Post thrombotic symptoms
(hyperpigmentation edema
and redness)bull Age gt_65 yearsbull BMI gt_30
Validation study Yes Yes Yes
Commentaries Different nomograms are available
to calculate risk of VTE recurrence
at different time
Patients with low score (lt_1) have
an annual
recurrence rate of 31
It is applicable in women only
Women with low score (lt_1)
have an annual recurrence rate of 13
6 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
than surgical patients68 Patients with a first symptomatic unprovokedDVT are at higher risk of recurrence than those with a first unpro-voked PE69 Factors related to DVT recurrence are listed in Table 4
For proximal DVT andor PE 3-months anticoagulation is the bestoption if transient and reversible risk factors were present70 In allother patients prolonging anticoagulation protects from recurrence(70ndash90) but exposes to risk of unpredictable bleeding complica-tions Decision to discontinue or not anticoagulation should there-fore be individually tailored and balanced against bleeding risk takingalso into account patientsrsquo preferences Three clinical prediction ruleshave been derived and prospectively validated to detect low-recurrence risk patients (Table 4)71 A number of bleeding scoreswere evaluated none showed sufficient predictive accuracy or hadsufficient validation to be recommended in routine clinicalpractice7273
Continuing indefinite anticoagulation with the same drug adminis-tered during the first months is the best option for patients with mul-tiple VTE episodes or strong VTE familial history those with majorthrombophilia or longstanding medical diseases at high thromboticrisk70 Indefinite anticoagulation can also be considered in patientswith first episode of unprovoked VTE especially in those with severepresentation provided they are at low bleeding risk70 Finally discon-tinuing anticoagulation in non-cancer patients with repeatedly nega-tive D-dimer (before drug interruption 15 30 60 and 90 daysfollowing interruption) has proved to be safe in patients with unpro-voked proximal DVT provided veins are recanalized or remained sta-ble for 1 year74 However using moderately sensitive D-dimer assayduring and 30 days after stopping anticoagulation these results werenot confirmed in men and in women with VTE not associated withoestrogen treatment75 Similarly when measurements were re-peated using a quantitative assay D-dimer testing failed to identifysubgroups with very low recurrence rate76
AntithromboticsVitamin K antagonists
Four randomized studies evaluated VKA [target international normal-ized ratio (INR) 20ndash30] for VTE extended treatment in patientscompleting 3-months anticoagulation77ndash80 Recurrent VTE occurredless in the VKA groups (combined OR 007)81 Bleeding was signifi-cantly higher81
The ELATE study82 randomized patients to conventional intensity(INR 20ndash30) or low-intensity (INR 15ndash1ndash9) Recurrence rate was07 vs 19100 patient-years respectively (HR 28) with no differencein major bleeding Yet the low-intensity VKA therapy should bediscouraged
Direct oral anticoagulants
Dabigatran (150 mg bid) was as effective as warfarin and more ef-fective than placebo in preventing recurrent VTE (Table 5) Risk ofmajor bleeding was reduced compared with warfarin83
With Rivaroxaban (20 mg od) risk of VTE recurrence was lowercompared with placebo (HR 019) while bleeding risk was notincreased (Table 5)84 Standard and lower dose (10 mg od) also signif-icantly reduced risk of recurrence compared to aspirine without sig-nificant increase in bleeding85
VTE recurrence occurred significantly less in standard and lowerdose Apixaban (5 and 25 mg bid) vs placebo (Table 5) Bleeding didnot differ between groups86
Recurrence rates with Edoxaban 60 mg were similar to thewarfarin-treated group (post hoc analysis) (Table 5)87 Major bleedingwas lower in the edoxaban group
Data from Phase IV studies are scarce but results from XALIA areconsistent with observations of rivaroxaban and warfarin88
Aspirin
Two studies investigated aspirin 100 mg vs placebo in patients withidiopathic VTE who completed initial anticoagulation treatment8990
Pooled HR for VTE recurrence was 068 and 147 for bleeding91
Other
Recent evaluation of Sulodexide vs placebo in patients with unpro-voked VTE who completed standard course of anticoagulationshowed a HR for VTE recurrence of 049 (P = 002)92 No majorbleeding episodes were observed
Venous occlusion recanalizationEndovascular techniques are available for selected patients withPTS57 Case series and prospective cohort trials suggest that at leastsome subgroups of PTS patients (CEAP classes 4ndash6 Figure 4) maybenefit from addition of endovascular therapy into overall manage-ment strategy
In patients with moderate-to-severe PTS and iliac vein obstructionendovascular stent placement may be used to restore vein patencyIn preliminary studies stent placement in chronically occluded iliacveins contributed to ulcers healing PTS symptoms relief and reducedobstructive venous sequel93
No randomized controlled trials are available the largest seriesfound patients with moderate-to-severe PTS to have reduced pain(P lt 00001) severe pain (from 41 to 11) and severe swelling(from 36 to 18) increased ulcer healing (68) and reduced ven-ous pressure following recanalization with stent placement93
Claudication improvement better outflow fraction and calf pumpfunction was also observed94
In selected infrequent cases surgical vein bypass may be an optionto relieve venous hypertension
Follow-upPatients with DVT should be followed to avoid risk of recurrence aswell as DVT and anticoagulation-related complicationsDevelopment of renal failure changes in body weight or pregnancythat may require anticoagulation adjustment should be monitoredCompliance as well as benefitrisk balance should be assessed regu-larly VUS at anticoagulation discontinuation is useful in determiningbaseline residual vein thrombosis
Consensus statement extended managementbull Decision to discontinue or not anticoagulation should be individu-
ally tailored balancing risk of recurrence against bleeding risk tak-ing into account patientsrsquo preferences and compliance
bull In the absence of contraindications DOACs should be preferredas first line anticoagulant therapy in non-cancer patients Currently
Diagnosis and management of acute DVT 7
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

than surgical patients68 Patients with a first symptomatic unprovokedDVT are at higher risk of recurrence than those with a first unpro-voked PE69 Factors related to DVT recurrence are listed in Table 4
For proximal DVT andor PE 3-months anticoagulation is the bestoption if transient and reversible risk factors were present70 In allother patients prolonging anticoagulation protects from recurrence(70ndash90) but exposes to risk of unpredictable bleeding complica-tions Decision to discontinue or not anticoagulation should there-fore be individually tailored and balanced against bleeding risk takingalso into account patientsrsquo preferences Three clinical prediction ruleshave been derived and prospectively validated to detect low-recurrence risk patients (Table 4)71 A number of bleeding scoreswere evaluated none showed sufficient predictive accuracy or hadsufficient validation to be recommended in routine clinicalpractice7273
Continuing indefinite anticoagulation with the same drug adminis-tered during the first months is the best option for patients with mul-tiple VTE episodes or strong VTE familial history those with majorthrombophilia or longstanding medical diseases at high thromboticrisk70 Indefinite anticoagulation can also be considered in patientswith first episode of unprovoked VTE especially in those with severepresentation provided they are at low bleeding risk70 Finally discon-tinuing anticoagulation in non-cancer patients with repeatedly nega-tive D-dimer (before drug interruption 15 30 60 and 90 daysfollowing interruption) has proved to be safe in patients with unpro-voked proximal DVT provided veins are recanalized or remained sta-ble for 1 year74 However using moderately sensitive D-dimer assayduring and 30 days after stopping anticoagulation these results werenot confirmed in men and in women with VTE not associated withoestrogen treatment75 Similarly when measurements were re-peated using a quantitative assay D-dimer testing failed to identifysubgroups with very low recurrence rate76
AntithromboticsVitamin K antagonists
Four randomized studies evaluated VKA [target international normal-ized ratio (INR) 20ndash30] for VTE extended treatment in patientscompleting 3-months anticoagulation77ndash80 Recurrent VTE occurredless in the VKA groups (combined OR 007)81 Bleeding was signifi-cantly higher81
The ELATE study82 randomized patients to conventional intensity(INR 20ndash30) or low-intensity (INR 15ndash1ndash9) Recurrence rate was07 vs 19100 patient-years respectively (HR 28) with no differencein major bleeding Yet the low-intensity VKA therapy should bediscouraged
Direct oral anticoagulants
Dabigatran (150 mg bid) was as effective as warfarin and more ef-fective than placebo in preventing recurrent VTE (Table 5) Risk ofmajor bleeding was reduced compared with warfarin83
With Rivaroxaban (20 mg od) risk of VTE recurrence was lowercompared with placebo (HR 019) while bleeding risk was notincreased (Table 5)84 Standard and lower dose (10 mg od) also signif-icantly reduced risk of recurrence compared to aspirine without sig-nificant increase in bleeding85
VTE recurrence occurred significantly less in standard and lowerdose Apixaban (5 and 25 mg bid) vs placebo (Table 5) Bleeding didnot differ between groups86
Recurrence rates with Edoxaban 60 mg were similar to thewarfarin-treated group (post hoc analysis) (Table 5)87 Major bleedingwas lower in the edoxaban group
Data from Phase IV studies are scarce but results from XALIA areconsistent with observations of rivaroxaban and warfarin88
Aspirin
Two studies investigated aspirin 100 mg vs placebo in patients withidiopathic VTE who completed initial anticoagulation treatment8990
Pooled HR for VTE recurrence was 068 and 147 for bleeding91
Other
Recent evaluation of Sulodexide vs placebo in patients with unpro-voked VTE who completed standard course of anticoagulationshowed a HR for VTE recurrence of 049 (P = 002)92 No majorbleeding episodes were observed
Venous occlusion recanalizationEndovascular techniques are available for selected patients withPTS57 Case series and prospective cohort trials suggest that at leastsome subgroups of PTS patients (CEAP classes 4ndash6 Figure 4) maybenefit from addition of endovascular therapy into overall manage-ment strategy
In patients with moderate-to-severe PTS and iliac vein obstructionendovascular stent placement may be used to restore vein patencyIn preliminary studies stent placement in chronically occluded iliacveins contributed to ulcers healing PTS symptoms relief and reducedobstructive venous sequel93
No randomized controlled trials are available the largest seriesfound patients with moderate-to-severe PTS to have reduced pain(P lt 00001) severe pain (from 41 to 11) and severe swelling(from 36 to 18) increased ulcer healing (68) and reduced ven-ous pressure following recanalization with stent placement93
Claudication improvement better outflow fraction and calf pumpfunction was also observed94
In selected infrequent cases surgical vein bypass may be an optionto relieve venous hypertension
Follow-upPatients with DVT should be followed to avoid risk of recurrence aswell as DVT and anticoagulation-related complicationsDevelopment of renal failure changes in body weight or pregnancythat may require anticoagulation adjustment should be monitoredCompliance as well as benefitrisk balance should be assessed regu-larly VUS at anticoagulation discontinuation is useful in determiningbaseline residual vein thrombosis
Consensus statement extended managementbull Decision to discontinue or not anticoagulation should be individu-
ally tailored balancing risk of recurrence against bleeding risk tak-ing into account patientsrsquo preferences and compliance
bull In the absence of contraindications DOACs should be preferredas first line anticoagulant therapy in non-cancer patients Currently
Diagnosis and management of acute DVT 7
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

Tab
le5
Exte
nd
ed
seco
nd
ary
pre
ven
tio
no
fV
TE
co
mp
ari
son
ofre
sult
sfr
om
Ph
ase
III
tria
lsw
ith
dir
ect
ora
lan
tico
agu
lan
ts
Dir
ect
ora
lan
tico
agu
-
lan
ttr
ial
Desi
gn
nT
reatm
en
t
regim
en
Recu
rren
tV
TE
or
VT
E-r
ela
ted
death
(o
fp
op
u-
lati
on
H
R)
Majo
rb
leed
ing
(o
fp
op
ula
tio
n
HR
)
Intr
acra
nia
lh
em
-
orr
hage
(o
f
po
pu
lati
on
H
R)
Gast
roin
test
inal
ble
ed
ing
(o
f
po
pu
lati
on
H
R)
Death
fro
man
y
cau
se(
ofp
op
u-
lati
on
H
R)
Dab
igat
ran
RE-
MED
Y7
RE-
SON
AT
E84
Ran
dom
ized
dou
ble-
blin
dR
ando
miz
edd
oubl
e-bl
ind
2866
1343
Dab
igat
ran
150
mg
bid
vs
war
fari
n(IN
R2
0ndash3
0)D
abig
atra
n15
0m
gb
idv
spl
aceb
o
Dab
igat
ran
150
mg
vs
war
fari
n1
8vs
13
HR
144
95
CI
078
ndash26
4P
=0
01no
n-in
feri
ority
Rec
urre
ntor
fata
lV
TE
orun
expl
aine
dde
ath
Dab
igat
ran
150
mg
vs
plac
ebo
04
vs5
6H
R0
089
5C
I0
02ndash0
25
Plt
000
1fo
rsu
perio
rity
Dab
igat
ran
150
mg
vs
war
fari
n0
9vs
18
HR
052
95
CI
027
ndash10
2P
=0
06D
abig
atra
n15
0m
gvs
pl
aceb
o0
3vs
0N
oH
Rre
port
edP
=1
0
Dab
igat
ran
150
mg
vs
war
fari
n0
1vs
03
No
HR
repo
rted
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Dab
igat
ran
150
mg
vs
war
fari
n0
3vs
06
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
plac
ebo
03
vs0
No
HR
repo
rted
Dab
igat
ran
150
mg
vs
war
fari
n1
2vs
13
HR
090
95
CI
047
ndash17
2P
=0
74D
abig
atra
n15
0m
gvs
pl
aceb
o0
vs0
3N
oH
Rre
port
ed
Riv
arox
aban
EIN
STEI
N-E
xten
tion8
5R
ando
miz
edd
oubl
e-bl
ind
1197
Riv
arox
aban
20m
god
vsp
lace
boR
ecur
rent
VT
ER
ivar
oxab
an20
mg
vs
plac
ebo
13
vs7
1H
R0
189
5C
I0
09ndash0
39
Plt
000
1
Riv
arox
aban
20m
gvs
pl
aceb
o0
7vs
0N
oH
Rre
port
edP
=0
11
No
intr
acra
nial
hem
-or
rhag
esob
serv
edR
ivar
oxab
an20
mg
vs
plac
ebo
05
vs0
No
HR
repo
rted
Riv
arox
aban
20m
gvs
pl
aceb
o0
2vs
03
No
HR
repo
rted
Api
xaba
nA
MPL
IFY
-Ext
ensi
on86
Ran
dom
ized
dou
ble-
blin
d24
86A
pixa
ban
5m
gb
id
orap
ixab
an2
5m
gb
idv
spl
aceb
o
Api
xaba
n5
mg
vsp
la-
cebo
17
vs8
8R
R0
209
5C
I01
1ndash0
34A
pixa
ban
25
mg
vs
plac
ebo
17
vs8
8R
R0
199
5C
I01
1ndash0
33
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
5R
R0
259
5C
I00
3ndash2
24A
pixa
ban
25
mg
vs
plac
ebo
02
vs0
5R
R0
499
5C
I00
9ndash2
64
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
No
intr
acra
nial
hem
-or
rhag
esob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
01
vs0
3N
oR
Rre
port
ed
No
gast
roin
test
inal
blee
dsob
serv
ed
Api
xaba
n5
mg
vsp
la-
cebo
05
vs1
7N
oR
Rre
port
ed
Api
xaba
n2
5m
gvs
pl
aceb
o0
5vs
17
No
RR
repo
rted
Edox
aban
Hok
usai
-VT
Epo
stho
c87
Ran
dom
ized
dou
ble
blin
d72
27Ed
oxab
an60
mg
qd(o
rdo
sere
duce
d30
mg)
vsw
arfa
rin
Edox
aban
vsw
arfa
rin
18
vs1
9H
R0
979
5C
I0
69ndash1
37)
Edox
aban
vsw
arfa
rin
03
vs0
7H
R0
459
5C
I0
22ndash0
92)
Edox
aban
vsw
arfa
rin
lt0
1vs
02
HR
016
95
CI
002
ndash13
6)
Not
asse
ssed
Not
asse
ssed
Dat
afr
omco
mpa
rativ
ePh
ase
IVst
udie
sR
ivar
oxab
anX
ALI
A88
Pros
pect
ive
non-
inte
rven
tiona
l51
42R
ivar
oxab
an15
mg
bid
for
3w
eeks
follo
wed
by20
mg
qdvs
hep
arin
vita
-m
inK
anta
goni
st
Riv
arox
aban
vshe
p-ar
inV
KA
14
vs2
3H
R0
919
5C
I0
54ndash1
54
P=
072
Riv
arox
aban
vshe
p-ar
inV
KA
08
vs2
1H
R0
779
5C
I0
40ndash1
50
P=
044
Not
asse
ssed
Not
asse
ssed
Riv
arox
aban
vshe
p-ar
inV
KA
04
vs3
4H
R0
5195
C
I02
4ndash1
07P
=0
07
8 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

low-dose apixaban and rivaroxaban have shown their benefit inthis setting
bull When VKAs are proposed they should be administered at con-ventional intensity regimen (INR 2ndash3)
bull Aspirin may be considered for extended treatment if anticoagula-tion is contraindicated
bull Endovascular recanalization may be considered in patients withchronic venous occlusion class CEAP 4ndash6
bull Regular (at least yearly) assessment of compliance and benefitriskbalance should be performed in patients on extended treatment
bull At anticoagulation discontinuation venous US should be per-formed to establish a baseline comparative exam in case ofrecurrence
Special situations
Upper extremities deep vein thrombosisUpper extremities DVT (UEDVT) accounts for 10 of all DVTs withan annual incidence of 04ndash1010000 persons9596 Incidence risesbecause of increasing use of central venous catheters cardiac pace-makers and defibrillators9596 Complications are similar althoughless frequent to those of lower limb DVT9596 About 20ndash30 of
UEDVT are primary comprising those caused by anatomic abnormal-ities or following sustained physical efforts97 Secondary DVT includevenous catheter- and devices-related complications cancer preg-nancy and recent armshoulder surgery or trauma Most commonclinical presentation includes pain swelling and skin discoloration Aclinical decision score has been proposed (Table 6)98
D-Dimershowed good negative predictive value in symptomatic DVT99100
VUS is the first choice exam for diagnosis101
A diagnostic algorithm using Constans score D-dimer and VUSwas proposed (Table 6)100 Contrast- CT- and MR-venography arenot recommended for diagnosis but limited to unresolved selectedcases96 Anticoagulation is similar to that of lower limb DVTThrombolysis is not routinely recommended but limited to selectedsevere cases A prognostic score identifying low-risk DVT patientswho could be safely treated at home has been proposed but not yetexternally validated102
Deep vein thrombosis at unusual sitesCerebral vein thrombosis
Most common cerebral vein thrombosis (CVT) presentation includessevere headaches seizures focal neurological deficits and alteredconsciousness103104 For the diagnosis and treatment refer to theSupplementary material online only section
Splanchnic vein thrombosis
Splanchnic vein thrombosis may present as sudden onset of abdom-inal pain with or without other non-specific abdominal
Table 6 Constans clinical score for UEAD
Constans score item Risk score
Central venous catheter or pacemaker thread 1
Localized pain 1
Unilateral edema 1
Other diagnosis at least as plausible -1
Score lt_1 = Upper extremity DVT unlikelyScore gt_2 = Upper extremity DVT likely
Figure 4 Chronic venous disorders clinical classification (CEAP)
Table 7 Khorana decision score in cancer patients
Khorana score patient characteristic Risk
score
Site of cancer
Very high risk (stomach pancreas) 2
High risk (lung lymphoma gynecologic bladder testicular) 1
Pre-chemotherapy platelet count 350 109L or more 1
Hemoglobin level lt10 gdL or use of red cell growth factors 1
Pre-chemotherapy leukocyte count gt11 109L 1
BMI gt_35 kgm2 1
Score gt_3 = high risk Score 1-2= intermediate risk Score 0 = low risk
Diagnosis and management of acute DVT 9
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

symptoms105106 Upper gastrointestinal bleeding or abrupt ascitesworsening may occur in cirrhotic patients lower gastrointestinalbleeding or acute abdomen may occur in patients with mesentericvein thrombosis105 For the diagnosis and treatment refer to theSupplementary material online only section
Deep vein thrombosis and cancerCancer patients show four- to seven-fold increased VTE risk (se-cond cause of death) Incidental VTE is increasingly diagnosed andassociated with worse overall survival VTE risk varies from cancerdiagnosis through treatment with annual incidence rate of 05ndash20 according to cancer site and type metastasis status treat-ment (surgery chemotherapy) use of central venous cathetershospitalization and patient-related factor Risk-assessment mod-els may help stratify individual VTE risk and tailor adequate ther-apy (Table 7)107ndash109
Cancer-related VTE is at high risk of recurrence and bleeding dur-ing treatment risk of death increases up to eight-fold following acuteVTE compared with non-cancer patients LMWH is recommendedfor initial treatment (similar efficacy and higher safety than UFH)Fondaparinux in patients with history of heparin-induced thrombo-cytopenia and UFH in case of renal failure are valid alternatives Venacava filter and thrombolysis should only be considered on a case-by-case basis For long-term treatment superiority of LMWH overshort-term heparin followed by VKA is well documented LMWHused during at least 3 and up to 6 months when compared with VKAsignificantly reduced VTE recurrence with similar safety profile After6 months termination or continuation of anticoagulation should beindividually evaluated benefitndashrisk ratio tolerability patientsrsquo prefer-ence and cancer activity110
In symptomatic catheter-related thrombosis anticoagulation is rec-ommended for at least 3-months LMWHs are suggested althoughVKAs can also be used (no direct comparison available) Central-vein-catheter can be maintained in place if it is functional non-infected and there is good thrombosis resolution Optimal antico-agulation duration has not been determined however 3-monthsduration seems acceptable in analogy with upper extremity DVT(UEDVT)110
For VTE recurrence under proper anticoagulation (INR antiXawithin therapeutical range) 3 options are recommended (i) switchfrom VKA to LMWH in patients treated with VKA (ii) increase
weight-adjusted dose of LMWH by 20ndash25 (iii) vena cava filteruse although no specific results are available for cancer patients
No direct comparison of DOACs with LMWH is currently avail-able Nevertheless data from recent large VTE trials showed non-inferiority in terms of efficacy and safety of DOACs compared withAVK in cancer patients included in the studies111
Deep vein thrombosis in pregnancyVTE remains the leading cause of maternal mortality in industrializedworld112 VTE risk factors are listed in Table 8 Validity of DVT clinicalprediction rules in pregnancy has not yet been tested prospectively113
The LEFt clinical score was proposed113 Although D-dimers increaseduring pregnancy normal values exclude VTE with likelihood similar tonon-pregnant women6 VUS is the primary imaging test114115 Unlesscontraindicated anticoagulation should be initiated until objective test-ing115116 If VUS is negative but clinical suspicion high testing should berepeated117118 Rarely CT or MRI venography may be considered
Treatment is based on heparin anticoagulation (no placenta cross-ing and not significantly found in breast milk)6 LMWHs are safe inpregnancy119ndash121 anti-Xa monitoring and dose adaptation cannot berecommended routinely but may be considered in women at ex-tremes of body-weight or renal disease6 Whether initial full doseanticoagulation can be reduced to intermediate dose for secondaryprevention during ongoing pregnancy remains unclear120 Dose re-duction should be considered for women at high risk of bleedingosteoporosis or low VTE recurrence risk116 Evidence is insufficientto recommend od or bid LMWH but bid may be more suitableperinatally to avoid high anti-Xa levels at time of deliveryAnticoagulation should be continued for at least 6 weeks postnatallyand until at least a total of 3 months treatment117
Consensus statement DVT management in special
situationsbull In case of UEDVT suspicion venous US is the first choice imaging
testbull Treatment of UEDVT is similar to that of lower limb DVT with
regard to anticoagulationbull LMWH are recommended for acute treatment of CVTbull LMWH are recommended for acute treatment of splanchnic vein
thrombosisbull LMWH are recommended for initial and long-term treatment in
cancer patientsbull In cancer patients after 6 months decision of continuation and if
so the mode of anticoagulation should be based on individualevaluation of the benefit-risk ratio tolerability patientsrsquo preferenceand cancer activity
bull During pregnancy venous US is recommended as first line DVTimaging test
bull During pregnancy LMWH is recommended for initial and long-term treatment
bull Anticoagulant treatment should be continued for at least 6 weeksafter delivery with a total of 3-months treatment
Supplementary material
Supplementary material is available at European Heart Journal online
Table 8 VTE risk factors during pregnancy
Prior VTE Preterm delivery
Smoking Pre-eclampsia
Varicosis Caesarean section (specifically in the
emergency situation)
Hyperemesis Postpartum infection or hemorrhage
severe thrombophilia Transfusion
assisted reproductive
technology
Immobilization
BMI gt30 kgm2 Systemic lupus erythematosus
10 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

Conflict of interest Dr Mazzolai reports personal fees fromBayer Health Care personal fees from Pfizer - Bristol-Myers Squibbpersonal fees from Daiichi-Sankyo outside the submitted work DrAboyans reports personal fees from Bayer Healthcare personal feesfrom Boehringer Ingelheim personal fees from Daichii-Sankyo per-sonal fees from Astra-Zeneca personal fees from Sanofi personalfees from MSD personal fees from BMSPfizer alliance personal feesfrom Novartis outside the submitted work Dr Ageno reports grantsand personal fees from Bayer grants and personal fees fromBoehringer Ingelheim personal fees from Daiichi Sankyo personalfees from BMS-Pfizer personal fees from Aspen outside the submit-ted work Dr Agnelli reports personal fees from Bristol-Myers-Squibb personal fees from Pfizer personal fees from BayerHealthcare personal fees from Boehringer Ingelheim personal feesfrom Daiichi Sankyo outside the submitted work Dr Alatri reportspersonal fees from Bayer Health Care personal fees from Pfizer-Bristol-Myers-Squibb outside the submitted work Dr Bauersachsreports personal fees from Bayer Healthcare Boehringer IngelheimPfizer - Bristol-Myers Squibb Daichii-Sankyo outside the submittedwork Dr Buller reports grants from Sanofi-Aventis personal feesfrom Sanofi-Aventis grants from Bayer HealthCare personal feesfrom Bayer HealthCare grants from Bristol-Myers-Squibb personalfees from Bristol-Meyers-Squibb grants from Daiichi Sankyo per-sonal fees from Daiichi Sankyo grants from Glaxo SmithKline per-sonal fees from Glaxo SmithKline grants from Pfizer personal feesfrom Pfizer grants from Roche personal fees from Roche grantsfrom Isis personal fees from Isis grants from Thrombogenics per-sonal fees from Thrombogenics during the conduct of the study DrELIAS reports grants from Bayer Pharma personal fees from BayerPharma grants from Daiichi Sansectrma personal fees from DaiichiSansecto Pharma outside the submitted work Dr Farge reports otherfrom Portola non-financial support from Leo Pharma non-financialsupport from Aspen non-financial support from Pfizer outside thesubmitted work Dr Konstantinides reports grants and personal feesfrom Bayer Health Care grants and personal fees from BoehringerIngelheim grants and personal fees from Daiichi Sankyo personalfees from Pfizer - Bristol-Myers Squibb outside the submitted workDr Palareti reports personal fees from Alfa-Wassermann personalfees from Daiichi-Sankyo personal fees from Siemens personal feesfrom Werfen outside the submitted work Dr Torbicki reportsgrants and personal fees from Bayer Healthcare grants from Pfizeroutside the submitted work Dr Vlachopoulos reports personal feesfrom Bayer reports personal fees from Merck Sharp ampDomereports personal fees from Angelini reports personal fees fromPfizer reports personal fees from Astra Zeneca reports personalfees from Menarini reports personal fees from Elpen reports per-sonal fees from Merck reports personal fees from Serono reportspersonal fees from Novartis reports personal fees from Boehringer-Ingelheim reports personal fees from OMRON reports personalfees from Sanofi Aventis reports personal fees from PharmaSuissreports personal fees from Amgen outside of the submitted work
References1 Silverstein MD Heit JA Mohr DN Petterson TM Orsquofallon WM Melton LJ III
Trends in the incidence of deep vein thrombosis and pulmonary embolism a25-year population-based study Arch Intern Med 1998158585ndash593
2 Heit JA The epidemiology of venous thromboembolism in the communityArterioscler Thromb Vasc Biol 200828370ndash372
3 White RH Zhou H Romano PS Incidence of idiopathic deep venous throm-bosis and secondary thromboembolism among ethnic groups in California AnnIntern Med 1998128737ndash740
4 White RH The epidemiology of venous thromboembolism Circulation2003107(23 Suppl 1)I4ndashI8
5 Raskob GE Angchaisuksiri P Blanco AN Buller H Gallus A Hunt BJ HylekEM Kakkar A Konstantinides SV McCumber M Ozaki Y Wendelboe A WeitzJI Day ISCfWT Thrombosis a major contributor to global disease burdenArterioscler Thromb Vasc Biol 2014342363ndash2371
6 Konstantinides SV Torbicki A Agnelli G Danchin N Fitzmaurice D Galie NGibbs JS Huisman MV Humbert M Kucher N Lang I Lankeit M Lekakis JMaack C Mayer E Meneveau N Perrier A Pruszczyk P Rasmussen LHSchindler TH Svitil P Vonk Noordegraaf A Zamorano JL Zompatori M TaskForce for the D Management of Acute Pulmonary Embolism of the EuropeanSociety of Cardiology 2014 ESC guidelines on the diagnosis and managementof acute pulmonary embolism Eur Heart J 2014353033ndash3069
7 Galanaud JP Kahn SR Khau Van Kien A Laroche JP Quere I [Epidemiology and man-agement of isolated distal deep venous thrombosis] La Revue De Medecine InterneFondee Par La Societe Nationale Francaise De Medecine Interne 201233678ndash685
8 Mearns ES Coleman CI Patel D Saulsberry WJ Corman A Li D HernandezAV Kohn CG Index clinical manifestation of venous thromboembolism pre-dicts early recurrence type and frequency a meta-analysis of randomized con-trolled trials J Thromb Haemost 2015131043ndash1052
9 Prandoni P Kahn SR Post-thrombotic syndrome prevalence prognosticationand need for progress Br J Haematol 2009145286ndash295
10 Baldwin MJ Moore HM Rudarakanchana N Gohel M Davies AH Post-throm-botic syndrome a clinical review J Thromb Haemost 201311795ndash805
11 Soosainathan A Moore HM Gohel MS Davies AH Scoring systems for thepost-thrombotic syndrome J Vasc Surg 201357254ndash261
12 Wells PS Hirsh J Anderson DR Lensing AW Foster G Kearon C Weitz JDrsquoovidio R Cogo A Prandoni P Accuracy of clinical assessment of deep-veinthrombosis Lancet 19953451326ndash1330
13 Wells PS Anderson DR Rodger M Forgie M Kearon C Dreyer J Kovacs GMitchell M Lewandowski B Kovacs MJ Evaluation of D-dimer in the diagnosisof suspected deep-vein thrombosis N Engl J Med 20033491227ndash1235
14 Geersing GJ Zuithoff NP Kearon C Anderson DR Ten Cate-Hoek AJ Elf JLBates SM Hoes AW Kraaijenhagen RA Oudega R Schutgens RE Stevens SMWoller SC Wells PS Moons KG Exclusion of deep vein thrombosis using theWells rule in clinically important subgroups individual patient data meta-ana-lysis BMJ 2014348g1340
15 Righini M Perrier A De Moerloose P Bounameaux H D-Dimer for venousthromboembolism diagnosis 20 years later J Thromb Haemost 200861059ndash1071
16 Perrier A Desmarais S Miron MJ de Moerloose P Lepage R Slosman DDidier D Unger PF Patenaude JV Bounameaux H Non-invasive diagnosis ofvenous thromboembolism in outpatients Lancet 1999353190ndash195
17 Di Nisio M Sohne M Kamphuisen PW Buller HR D-Dimer test in cancer pa-tients with suspected acute pulmonary embolism J Thromb Haemost200531239ndash1242
18 Le Gal G Robert-Ebadi H Carrier M Kearon C Bounameaux H Righini M Is ituseful to also image the asymptomatic leg in patients with suspected deep veinthrombosis J Thromb Haemost 201513563ndash566
19 Galanaud JP Sevestre MA Genty C Pernod G Quere I Bosson JL Is it usefulto also image the asymptomatic leg in patients with suspected deep vein throm-bosis Comment J Thromb Haemost 2015132127ndash2130
20 Goodacre S Sampson F Thomas S van Beek E Sutton A Systematic reviewand meta-analysis of the diagnostic accuracy of ultrasonography for deep veinthrombosis BMC Med Imaging 200556
21 Ageno W Camporese G Riva N Iotti M Bucherini E Righini M KamphuisenPW Verhamme P Douketis JD Tonello C Prandoni P Analysis of an algorithmincorporating limited and whole-leg assessment of the deep venous system insymptomatic outpatients with suspected deep-vein thrombosis (PALLADIO) aprospective multicentre cohort study Lancet Haematol 20152e474ndashe480
22 Johnson SA Stevens SM Woller SC Lake E Donadini M Cheng J Labarere JDouketis JD Risk of deep vein thrombosis following a single negative whole-legcompression ultrasound a systematic review and meta-analysis JAMA2010303438ndash445
23 Bernardi E Camporese G Buller HR Siragusa S Imberti D Berchio AGhirarduzzi A Verlato F Anastasio R Prati C Piccioli A Pesavento R Bova CMaltempi P Zanatta N Cogo A Cappelli R Bucherini E Cuppini S Noventa FPrandoni P Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deepvein thrombosis a randomized controlled trial JAMA 20083001653ndash1659
24 Gibson NS Schellong SM Kheir DY Beyer-Westendorf J Gallus AS McRae SSchutgens RE Piovella F Gerdes VE Buller HR Safety and sensitivity of twoultrasound strategies in patients with clinically suspected deep venous throm-bosis a prospective management study J Thromb Haemost 200972035ndash2041
Diagnosis and management of acute DVT 11
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

25 Elias A Mallard L Elias M Alquier C Guidolin F Gauthier B Viard A Mahouin
P Vinel A Boccalon H A single complete ultrasound investigation of the ven-ous network for the diagnostic management of patients with a clinically sus-pected first episode of deep venous thrombosis of the lower limbs ThrombHaemost 200389221ndash227
26 Pomero F Dentali F Borretta V Bonzini M Melchio R Douketis JD FenoglioLM Accuracy of emergency physician-performed ultrasonography in the diag-nosis of deep-vein thrombosis a systematic review and meta-analysis ThrombHaemost 2013109137ndash145
27 Lewiss RE Kaban NL Saul T Point-of-care ultrasound for a deep venousthrombosis Glob Heart 20138329ndash333
28 Hamadah A Alwasaidi T Leg G Carrier M Wells PS Scarvelis D Gonsalves CForgie M Kovacs MJ Rodger MA Baseline imaging after therapy for unpro-voked venous thromboembolism a randomized controlled comparison of base-line imaging for diagnosis of suspected recurrence J Thromb Haemost201192406ndash2410
29 Prandoni P Cogo A Bernardi E Villalta S Polistena P Simioni P Noventa FBenedetti L Girolami A A simple ultrasound approach for detection of recur-rent proximal-vein thrombosis Circulation 1993881730ndash1735
30 Prandoni P Lensing AW Bernardi E Villalta S Bagatella P Girolami A Thediagnostic value of compression ultrasonography in patients with suspected re-current deep vein thrombosis Thromb Haemost 200288402ndash406
31 Le Gal G Kovacs MJ Carrier M Do K Kahn SR Wells PS Anderson DAChagnon I Solymoss S Crowther M Righini M Perrier A White RH Vickars LRodger M Validation of a diagnostic approach to exclude recurrent venousthromboembolism J Thromb Haemost 20097752ndash759
32 Pollack CV Schreiber D Goldhaber SZ Slattery D Fanikos J Orsquoneil BJThompson JR Hiestand B Briese BA Pendleton RC Miller CD Kline JAClinical characteristics management and outcomes of patients diagnosed withacute pulmonary embolism in the emergency department initial report ofEMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the RealWorld Registry) J Am Coll Cardiol 201157700ndash706
33 Da Costa Rodrigues J Alzuphar S Combescure C Le Gal G Perrier ADiagnostic characteristics of lower limb venous compression ultrasonographyin suspected pulmonary embolism a meta-analysis J Thromb Haemost2016141765ndash1772
34 Wells PS Ginsberg JS Anderson DR Kearon C Gent M Turpie AG BormanisJ Weitz J Chamberlain M Bowie D Barnes D Hirsh J Use of a clinical modelfor safe management of patients with suspected pulmonary embolism AnnIntern Med 1998129997ndash1005
35 Anderson DR Kahn SR Rodger MA Kovacs MJ Morris T Hirsch A Lang EStiell I Kovacs G Dreyer J Dennie C Cartier Y Barnes D Burton E PleasanceS Skedgel C Orsquorouke K Wells PS Computed tomographic pulmonary angiog-raphy vs ventilation-perfusion lung scanning in patients with suspected pulmon-ary embolism a randomized controlled trial JAMA 20072982743ndash2753
36 Carrier M Righini M Wells PS Perrier A Anderson DR Rodger MA Pleasance SLe Gal G Subsegmental pulmonary embolism diagnosed by computed tomog-raphy incidence and clinical implications A systematic review and meta-analysisof the management outcome studies J Thromb Haemost 201081716ndash1722
37 Dentali F Ageno W Becattini C Galli L Gianni M Riva N Imberti D SquizzatoA Venco A Agnelli G Prevalence and clinical history of incidental asymptom-atic pulmonary embolism a meta-analysis Thromb Res 2010125518ndash522
38 Becattini C Cohen AT Agnelli G Howard L Castejon B Trujillo-Santos JMonreal M Perrier A Yusen RD Jimenez D Risk stratification of patients withacute symptomatic pulmonary embolism based on presence or absence of lowerextremity DVT systematic review and meta-analysis Chest 2016149192ndash200
39 Becattini C Agnelli G Treatment of venous thromboembolism with new anti-coagulant agents J Am Coll Cardiol 2016671941ndash1955
40 Erkens PM Prins MH Fixed dose subcutaneous low molecular weight heparinsversus adjusted dose unfractionated heparin for venous thromboembolismCochrane Database Syst Rev 20109Cd001100
41 Buller HR Davidson BL Decousus H Gallus A Gent M Piovella F Prins MHRaskob G van den Berg-Segers AE Cariou R Leeuwenkamp O Lensing AWSubcutaneous fondaparinux versus intravenous unfractionated heparin in theinitial treatment of pulmonary embolism N Engl J Med 20033491695ndash1702
42 van Es N Coppens M Schulman S Middeldorp S Buller HR Direct oral anti-coagulants compared with vitamin K antagonists for acute venous thrombo-embolism evidence from phase 3 trials Blood 20141241968ndash1975
43 Pollack CV Jr Reilly PA Eikelboom J Glund S Verhamme P Bernstein RADubiel R Huisman MV Hylek EM Kamphuisen PW Kreuzer J Levy JH SellkeFW Stangier J Steiner T Wang B Kam CW Weitz JI Idarucizumab forDabigatran reversal N Engl J Med 2015373511ndash520
44 Siegal DM Curnutte JT Connolly SJ Lu G Conley PB Wiens BL Mathur VSCastillo J Bronson MD Leeds JM Mar FA Gold A Crowther MA AndexanetAlfa for the reversal of factor Xa inhibitor activity N Engl J Med20153732413ndash2424
45 Alesh I Kayali F Stein PD Catheter-directed thrombolysis (intrathrombus in-jection) in treatment of deep venous thrombosis a systematic review CatheterCardiovasc Interv 200770143ndash148
46 Enden T Haig Y Klow NE Slagsvold CE Sandvik L Ghanima W Hafsahl GHolme PA Holmen LO Njaastad AM Sandbaek G Sandset PM CaVenTSG Long-term outcome after additional catheter-directed thromboly-sis versus standard treatment for acute iliofemoral deep vein throm-bosis (the CaVenT study) a randomised controlled trial Lancet201237931ndash38
47 Haig Y Enden T Grotta O Klow NE Slagsvold CE Ghanima W Sandvik LHafsahl G Holme PA Holmen LO Njaaastad AM Sandbaek G Sandset PMPost-thrombotic syndrome after catheter-directed thrombolysis for deep veinthrombosis (CaVenT) 5-year follow-up results of an open-label randomisedcontrolled trial Lancet Haematol 20163e64ndashe71
48 Garcia MJ Lookstein R Malhotra R Amin A Blitz LR Leung DA Simoni EJSoukas PA Endovascular management of deep vein thrombosis with rheolyticthrombectomy final report of the prospective multicenter PEARL (peripheraluse of angiojet rheolytic thrombectomy with a variety of catheter lengths)registry J Vasc Interv Radiol 201526777ndash785 Quiz 786
49 Engelberger RP Spirk D Willenberg T Alatri A Do DD Baumgartner IKucher N Ultrasound-assisted versus conventional catheter-directedthrombolysis for acute iliofemoral deep vein thrombosis Circ Cardiovasc Interv20158
50 Ray CE Jr Prochazka A The need for anticoagulation following inferior venacava filter placement systematic review Cardiovasc Interv Radiol200831316ndash324
51 PREPIC Study Group Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism the PREPIC (Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave) randomized studyCirculation 2005112416ndash422
52 Mismetti P Laporte S Pellerin O Ennezat PV Couturaud F Elias A Falvo NMeneveau N Quere I Roy PM Sanchez O Schmidt J Seinturier C SevestreMA Beregi JP Tardy B Lacroix P Presles E Leizorovicz A Decousus H BarralFG Meyer G Effect of a retrievable inferior vena cava filter plus anticoagulationvs anticoagulation alone on risk of recurrent pulmonary embolism a random-ized clinical trial JAMA 20153131627ndash1635
53 Stein PD Matta F Keyes DC Willyerd GL Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism Am J Med2012125478ndash484
54 Kearon C Akl EA Comerota AJ Prandoni P Bounameaux H Goldhaber SZNelson ME Wells PS Gould MK Dentali F Crowther M Kahn SR AmericanCollege of Chest Physicians Antithrombotic therapy for VTE disease antith-rombotic therapy and prevention of thrombosis 9th ed American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines Chest2012141(2 Suppl)e419Sndashe494S
55 Kahn SR Shapiro S Wells PS Rodger MA Kovacs MJ Anderson DRTagalakis V Houweling AH Ducruet T Holcroft C Johri M Solymoss SMiron MJ Yeo E Smith R Schulman S Kassis J Kearon C Chagnon I WongT Demers C Hanmiah R Kaatz S Selby R Rathbun S Desmarais S OpatrnyL Ortel TL Ginsberg JS Compression stockings to prevent post-thrombotic syndrome a randomised placebo-controlled trial Lancet2014383880ndash888
56 Brandjes DP Buller HR Heijboer H Huisman MV de Rijk M Jagt H ten CateJW Randomised trial of effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis Lancet 1997349759ndash762
57 Kahn SR Comerota AJ Cushman M Evans NS Ginsberg JS Goldenberg NAGupta DK Prandoni P Vedantham S Walsh ME Weitz JI American HeartAssociation Council on Peripheral Vascular Disease CoCC Council on CStroke N The postthrombotic syndrome evidence-based prevention diagnosisand treatment strategies a scientific statement from the American HeartAssociation Circulation 20141301636ndash1661
58 Partsch H Blattler W Compression and walking versus bed rest in the treat-ment of proximal deep venous thrombosis with low molecular weight heparinJ Vasc Surg 200032861ndash869
59 Righini M Galanaud JP Guenneguez H Brisot D Diard A Faisse P BarrelierMT Desnos CH Jurus C Pichot O Martin M Mazzolai L Choquenet CAccassat S Carrier M Gal GL Mermillod B Laroche JP Bounameaux HPerrier A Kahn S Quere I Anticoagulant therapy for symptomatic distal deepvein thrombosis The cactus randomized placebocontrolled trial J ThrombHaemost 20151350
60 Palareti G How I treat isolated distal deep vein thrombosis (IDDVT) Blood20141231802ndash1809
61 Parisi R Visona A Camporese G Verlato F Lessiani G Antignani PL PalaretiG Isolated distal deep vein thrombosis efficacy and safety of a protocol oftreatment Treatment of Isolated Calf Thrombosis (TICT) Study Int Angiol20092868ndash72
12 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

62 Schwarz T Buschmann L Beyer J Halbritter K Rastan A Schellong S Therapy
of isolated calf muscle vein thrombosis a randomized controlled study J VascSurg 2010521246ndash1250
63 Palareti G Cosmi B Lessiani G Rodorigo G Guazzaloca G Brusi C Valdre LConti E Sartori M Legnani C Evolution of untreated calf deep-vein thrombosisin high risk symptomatic outpatients the blind prospective CALTHRO studyThromb Haemost 20101041063ndash1070
64 Galanaud JP Sevestre MA Genty C Kahn SR Pernod G Rolland C Diard ADupas S Jurus C Diamand JM Quere I Bosson JL Incidence and predictors ofvenous thromboembolism recurrence after a first isolated distal deep veinthrombosis J Thromb Haemost 201412436ndash443
65 Sartori M Migliaccio L Favaretto E Palareti G Cosmi B Two years outcome ofisolated distal deep vein thrombosis Thromb Res 201413436ndash40
66 Boutitie F Pinede L Schulman S Agnelli G Raskob G Julian J Hirsh J KearonC Influence of preceding length of anticoagulant treatment and initial presenta-tion of venous thromboembolism on risk of recurrence after stopping treat-ment analysis of individual participantsrsquo data from seven trials BMJ2011342d3036
67 Prandoni P Noventa F Ghirarduzzi A Pengo V Bernardi E Pesavento R IottiM Tormene D Simioni P Pagnan A The risk of recurrent venous thrombo-embolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism A prospective cohort study in1626 patients Haematologica 200792199ndash205
68 Baglin T Luddington R Brown K Baglin C Incidence of recurrent venousthromboembolism in relation to clinical and thrombophilic risk factors pro-spective cohort study Lancet 2003362523ndash526
69 Kovacs MJ Kahn SR Wells PS Anderson DA Chagnon IGLEG Solymoss SCrowther M Perrier A Ramsay T Betancourt MT White RH Vickars LRodger MA Patients with a first symptomatic unprovoked deep vein thrombosisare at higher risk of recurrent venous thromboembolism than patients with a firstunprovoked pulmonary embolism J Thromb Haemost 201081926ndash1932
70 Kearon C Akl EA Ornelas J Blaivas A Jimenez D Bounameaux H Huisman MKing CS Morris TA Sood N Stevens SM Vintch JR Wells P Woller SCMoores L Antithrombotic therapy for VTE disease CHEST guideline and ex-pert panel report Chest 2016149315ndash352
71 Kyrle PA Eichinger S Clinical scores to predict recurrence risk of venousthromboembolism Thromb Haemost 20121081061ndash1064
72 Loewen P Dahri K Risk of bleeding with oral anticoagulants an updated sys-tematic review and performance analysis of clinical prediction rules AnnHematol 2011901191ndash1200
73 Burgess S Crown N Louzada ML Dresser G Kim RB Lazo-Langner A Clinicalperformance of bleeding risk scores for predicting major and clinically relevantnon-major bleeding events in patients receiving warfarin J Thromb Haemost2013111647ndash1654
74 Palareti G Cosmi B Legnani C Antonucci ED Micheli V Ghirarduzzi A PoliD Testa S Tosetto A Pengo V Prandoni P DULCIS (D-dimer andULtrasonography in Combination Italian Study) Investigators D-dimer to guidethe duration of anticoagulation in patients with venous thromboembolism amanagement study Blood 2014124196ndash203
75 Kearon C Spencer FA Orsquokeeffe D Parpia S Schulman S Baglin T Stevens SMKaatz S Bauer KA Douketis JD Lentz SR Kessler CM Moll S Connors JMGinsberg JS Spadafora L Julian JA D-dimer testing to select patients with a firstunprovoked venous thromboembolism who can stop anticoagulant therapy acohort study Ann Intern Med 201516227ndash34
76 Kearon C Parpia S Spencer FA Baglin T Stevens SM Bauer KA Lentz SRKessler CM Douketis JD Moll S Kaatz S Schulman S Connors JM Ginsberg JSSpadafora L Liaw P Weitz JI Julian JA D-dimer levels and recurrence in pa-tients with unprovoked VTE and a negative qualitative D-dimer test after treat-ment Thromb Res 2016146119ndash125
77 Schulman S Granqvist S Holmstrom M Carlsson A Lindmarker P Nicol PEklund SG Nordlander S Larfars G Leijd B Linder O Loogna E The durationof oral anticoagulant therapy after a second episode of venous thromboembol-ism The Duration of Anticoagulation Trial Study Group N Engl J Med1997336393ndash398
78 Kearon C Gent M Hirsh J Weitz J Kovacs MJ Anderson DR Turpie AGGreen D Ginsberg JS Wells P MacKinnon B Julian JA A comparison of threemonths of anticoagulation with extended anticoagulation for a first episode ofidiopathic venous thromboembolism N Engl J Med 1999340901ndash907
79 Agnelli G Prandoni P Santamaria MG Bagatella P Iorio A Bazzan M Moia MGuazzaloca G Bertoldi A Tomasi C Scannapieco G Ageno W WarfarinOptimal Duration Italian Trial Investigators Three months versus one year oforal anticoagulant therapy for idiopathic deep venous thrombosis N Engl J Med2001345165ndash169
80 Agnelli G Prandoni P Becattini C Silingardi M Taliani MR Miccio M Imberti DPoggio R Ageno W Pogliani E Porro F Zonzin P Warfarin Optimal Duration
Italian Trial Investigators Extended oral anticoagulant therapy after a first epi-sode of pulmonary embolism Ann Intern Med 200313919ndash25
81 Castellucci LA Cameron C Le Gal G Rodger MA Coyle D Wells PS Clifford TGandara E Wells G Carrier M Efficacy and safety outcomes of oral anticoagu-lants and antiplatelet drugs in the secondary prevention of venous thrombo-embolism systematic review and network meta-analysis BMJ 2013347f5133
82 Kearon C Ginsberg JS Kovacs MJ Anderson DR Wells P Julian JA MacKinnonB Weitz JI Crowther MA Dolan S Turpie AG Geerts W Solymoss S vanNguyen P Demers C Kahn SR Kassis J Rodger M Hambleton J Gent MExtended Low-Intensity Anticoagulation For Thrombo-Embolism I Comparisonof low-intensity warfarin therapy with conventional-intensity warfarin therapyfor long-term prevention of recurrent venous thromboembolism N Engl J Med2003349631ndash639
83 Schulman S Kearon C Kakkar AK Schellong S Eriksson H Baanstra D KvammeAM Friedman J Mismetti P Goldhaber SZ RE-MEDY Trials Investigators RE-SONATE Trials Investigators Extended use of dabigatran warfarin or placebo invenous thromboembolism N Engl J Med 2013368709ndash718
84 Bauersachs R Berkowitz SD Brenner B Buller HR Decousus H Gallus ASLensing AW Misselwitz F Prins MH Raskob GE Segers A Verhamme P WellsP Agnelli G Bounameaux H Cohen A Davidson BL Piovella F Schellong SThe EINSTEIN Investigators Oral rivaroxaban for symptomatic venousthromboembolism N Engl J Med 20103632499ndash2510
85 Weitz JJ Lensing AW Prins MH Bauersachs R Beyer-Westendorf JBounameaux H Brighton TA Cohen AT Davidson BL Decousus H FreitasMC Holberg G Kakkar AK Haskell L van Bellen B Pap AF Berkowitz SDVerhamme P Wells PS Prandoni P EINSTEIN CHOICE InvestigatorsRivaroxaban or Aspirin for Extended Treatment of VenousThromboembolism N Engl J Med 2017 in press
86 Agnelli G Buller HR Cohen A Curto M Gallus AS Johnson M Porcari ARaskob GE Weitz JI AMPLIFY-EXT Investigators Apixaban for extended treat-ment of venous thromboembolism N Engl J Med 2013368699ndash708
87 Raskob G Ageno W Cohen AT Brekelmans MP Grosso MA Segers A MeyerG Verhamme P Wells PS Lin M Winters SM Weitz JI Buller HR Extendedduration of anticoagulation with edoxaban in patients with venous thrombo-embolism a post-hoc analysis of the Hokusai-VTE study Lancet Haematol20163e228ndashe236
88 Ageno W Mantovani LG Haas S Kreutz R Monje D Schneider J van EickelsM Gebel M Zell E Turpie AG Safety and effectiveness of oral rivaroxaban ver-sus standard anticoagulation for the treatment of symptomatic deep-veinthrombosis (XALIA) an international prospective non-interventional studyLancet Haematol 20163e12ndashe21
89 Becattini C Agnelli G Schenone A Eichinger S Bucherini E Silingardi MBianchi M Moia M Ageno W Vandelli MR Grandone E Prandoni PWARFASA Investigators Aspirin for preventing the recurrence of venousthromboembolism N Engl J Med 20123661959ndash1967
90 Brighton TA Eikelboom JW Mann K Mister R Gallus A Ockelford P Gibbs HHague W Xavier D Diaz R Kirby A Simes J Investigators A Low-dose aspirinfor preventing recurrent venous thromboembolism N Engl J Med20123671979ndash1987
91 Simes J Becattini C Agnelli G Eikelboom JW Kirby AC Mister R Prandoni PBrighton TA Investigators IS Aspirin for the prevention of recurrent venousthromboembolism the INSPIRE collaboration Circulation 20141301062ndash1071
92 Andreozzi GM Bignamini AA Davi G Palareti G Matuska J Holy MPawlaczyk-Gabriel K Dzupina A Sokurenko GY Didenko YP Andrei LDLessiani G Visona A Sulodexide for the prevention of recurrent venousthromboembolism the sulodexide in secondary prevention of recurrent deepvein thrombosis (SURVET) study a multicenter randomized double-blind pla-cebo-controlled trial Circulation 20151321891ndash1897
93 Neglen P Hollis KC Olivier J Raju S Stenting of the venous outflow in chronicvenous disease long-term stent-related outcome clinical and hemodynamic re-sult J Vasc Surg 200746979ndash990
94 Delis KT Bjarnason H Wennberg PW Rooke TW Gloviczki P Successful iliacvein and inferior vena cava stenting ameliorates venous claudication and im-proves venous outflow calf muscle pump function and clinical status in post-thrombotic syndrome Ann Surg 2007245130ndash139
95 Kucher N Clinical practice Deep-vein thrombosis of the upper extremities NEngl J Med 2011364861ndash869
96 Grant JD Stevens SM Woller SC Lee EW Kee ST Liu DM Lohan DG ElliottCG Diagnosis and management of upper extremity deep-vein thrombosis inadults Thromb Haemost 20121081097ndash1108
97 Thompson JF Winterborn RJ Bays S White H Kinsella DC Watkinson AF Venousthoracic outlet compression and the Paget-Schroetter syndrome a review and rec-ommendations for management Cardiovasc Interv Radiol 201134903ndash910
98 Constans J Salmi LR Sevestre-Pietri MA Perusat S Nguon M Degeilh MLabarere J Gattolliat O Boulon C Laroche JP Le Roux P Pichot O Quere I
Diagnosis and management of acute DVT 13
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018
Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018

Conri C Bosson JL A clinical prediction score for upper extremity deep ven-ous thrombosis Thromb Haemost 200899202ndash207
99 Sartori M Migliaccio L Favaretto E Cini M Legnani C Palareti G Cosmi B D-dimer for the diagnosis of upper extremity deep and superficial venous throm-bosis Thromb Res 2015135673ndash678
100 Kleinjan A Di Nisio M Beyer-Westendorf J Camporese G Cosmi BGhirarduzzi A Kamphuisen PW Otten HM Porreca E Aggarwal A BrodmannM Guglielmi MD Iotti M Kaasjager K Kamvissi V Lerede T Marschang PMeijer K Palareti G Rickles FR Righini M Rutjes AW Tonello C Verhamme PWerth S van Wissen S Buller HR Safety and feasibility of a diagnostic algo-rithm combining clinical probability d-dimer testing and ultrasonography forsuspected upper extremity deep venous thrombosis a prospective manage-ment study Ann Int Med 2014160451ndash457
101 Di Nisio M Van Sluis GL Bossuyt PM Buller HR Porreca E Rutjes AWAccuracy of diagnostic tests for clinically suspected upper extremity deep veinthrombosis a systematic review J Thromb Haemost 20108684ndash692
102 Rosa-Salazar V Trujillo-Santos J Diaz Peromingo JA Apollonio A Sanz O MalyR Munoz-Rodriguez FJ Serrano JC Soler S Monreal M Investigators R A prog-nostic score to identify low-risk outpatients with acute deep vein thrombosis inthe upper extremity J Thromb Haemost 2015131274ndash1278
103 Ferro JM Canhao P Stam J Bousser MG Barinagarrementeria F Investigators IPrognosis of cerebral vein and dural sinus thrombosis results of theInternational Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)Stroke 200435664ndash670
104 Wasay M Bakshi R Bobustuc G Kojan S Sheikh Z Dai A Cheema Z Cerebralvenous thrombosis analysis of a multicenter cohort from the United StatesJ Stroke Cerebrovasc Dis 20081749ndash54
105 Thatipelli MR McBane RD Hodge DO Wysokinski WE Survival and recur-rence in patients with splanchnic vein thromboses Clin Gastroenterol Hepatol20108200ndash205
106 Ageno W Riva N Schulman S Bang SM Sartori MT Grandone E Beyer-Westendorf J Barillari GD Minno MN Dentali F IRSVT study groupAntithrombotic treatment of splanchnic vein thrombosis results of an interna-tional registry Semin Thromb Hemost 20144099ndash105
107 Khorana AA Kuderer NM Culakova E Lyman GH Francis CW Developmentand validation of a predictive model for chemotherapy-associated thrombosisBlood 20081114902ndash4907
108 Pabinger I Thaler J Ay C Biomarkers for prediction of venous thromboembol-ism in cancer Blood 20131222011ndash2018
109 Khorana AA Dalal M Lin J Connolly GC Incidence and predictors of venousthromboembolism (VTE) among ambulatory high-risk cancer patients undergo-ing chemotherapy in the United States Cancer 2013119648ndash655
110 Farge D Bounameaux H Brenner B Cajfinger F Debourdeau P Khorana AAPabinger I Solymoss S Douketis J Kakkar A International clinical practice
guidelines including guidance for direct oral anticoagulants in the treatment andprophylaxis of venous thromboembolism in patients with cancer Lancet Oncol201617e452ndashe466
111 Vedovati MC Germini F Agnelli G Becattini C Direct oral anticoagulants inpatients with VTE and cancer a systematic review and meta-analysis Chest2015147475ndash483
112 Nelson-Piercy C MacCallum P Mackillop L Reducing the risk of thrombosisand embolism during pregnancy and the puerperium (Green-top guideline no37a) R Coll Obstetr Gynaecol 20151ndash40
113 Le Moigne E Genty C Meunier J Arnoult AC Righini M Bressollette L BossonJL Le Gal G Validation of the LEFt score a newly proposed diagnostic tool fordeep vein thrombosis in pregnant women Thromb Res 2014134664ndash667
114 Le Gal G Prins AM Righini M Bohec C Lacut K Germain P Vergos JCKaczmarek R Guias B Collet M Bressollette L Oger E Mottier D Diagnosticvalue of a negative single complete compression ultrasound of the lower limbsto exclude the diagnosis of deep venous thrombosis in pregnant or postpartumwomen a retrospective hospital-based study Thromb Res 2006118691ndash697
115 Le Gal G Kercret G Ben Yahmed K Bressollette L Robert-Ebadi H Riberdy LLouis P Delluc A Labalette ML Baba-Ahmed M Bounameaux H Mottier DRighini M Diagnostic value of single complete compression ultrasonography inpregnant and postpartum women with suspected deep vein thrombosis pro-spective study BMJ 2012344e2635
116 Bates SM Greer IA Middeldorp S Veenstra DL Prabulos AM Vandvik POVTE thrombophilia antithrombotic therapy and pregnancy antithrombotictherapy and prevention of thrombosis 9th ed American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2Suppl)e691Sndashe736S
117 Thomsen A Greer I Thromboembolic disease in pregnancy and the puerper-ium acute management (Green-top guideline no 37b) R Coll Obstetr Gynaecol20151ndash32
118 Chan WS Spencer FA Lee AY Chunilal S Douketis JD Rodger M Ginsberg JSSafety of withholding anticoagulation in pregnant women with suspected deepvein thrombosis following negative serial compression ultrasound and iliac veinimaging CMAJ 2013185E194ndashE200
119 Romualdi E Dentali F Rancan E Squizzato A Steidl L Middeldorp S Ageno WAnticoagulant therapy for venous thromboembolism during pregnancy a sys-tematic review and a meta-analysis of the literature J Thromb Haemost201311270ndash281
120 Bauersachs RM Treatment of venous thromboembolism during pregnancyThromb Res 2009123(Suppl 2)S45ndashS50
121 Bauersachs RM Dudenhausen J Faridi A Fischer T Fung S Geisen UHarenberg J Herchenhan E Keller F Kemkes-Matthes B Schinzel H SpannaglM Thaler CJ Risk stratification and heparin prophylaxis to prevent venousthromboembolism in pregnant women Thromb Haemost 2007981237ndash1245
14 L Mazzolai et al
Downloaded from httpsacademicoupcomeurheartjadvance-article-abstractdoi101093eurheartjehx0033002647by gueston 19 February 2018