Embed Size (px)
Citation preview

J6
Tmcosnttpm
D
J
O
m
©
0
d
Oral Maxillofac Surg8:74-82, 2010
Diagnostic Accuracy of PanoramicRadiography in Determining Relationship
Between Inferior Alveolar Nerve andMandibular Third Molar
Momen A. Atieh, BDS, MSc*
Purpose: The aim of this review was to determine the diagnostic accuracy of panoramic radiographicmarkers in the detection of the relationship between the mandibular canal and third molar roots.
Materials and Methods: A literature search of electronic databases, Cochrane Oral Health Group’sTrials Register, National Research Register, conference proceedings, and abstracts was performed toidentify studies that had investigated the diagnostic accuracy of the 3 panoramic radiographic markers(ie, darkening of the root, interruption of the radiopaque borders, and diversion of the mandibular canal).RevMan, version 5.0, and Meta-DiSc software programs were used for the pooled analyses and theconstruction of a summary receiver operating characteristic curve.
Results: A total of 5 studies were included, involving 894 observations. The overall pooled sensitivityand specificity for darkening of the root was calculated as 51.2% (95% confidence interval [CI] 42% to60%) and 89% (95% CI 87% to 90%), respectively. The interruption of radiopaque borders showed apooled sensitivity of 53.5% (95% CI 78.1% to 81.8%) and a pooled specificity of 80% (95% CI 78.1% to81.8%). The diversion of the canal criterion had a pooled sensitivity of 29.4% (95% CI 21.8% to 38.1%)and a pooled specificity of 94.7% (95% CI 93.6% to 95.7%). The area under the receiver operatingcharacteristic curve was 70% to 77%.
Conclusions: The results of this meta-analysis suggest a reasonable diagnostic accuracy for panoramicradiography in the preoperative evaluation of the relationship between third molars and the canal.Additional studies are needed to examine a more accurate, accessible, and cost-effective initial radio-graphic technique before third molar surgery.© 2010 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 68:74-82, 2010uAtoom
o2(ptIsrmSlt
he surgical extraction of third molars is one of theost common oral and maxillofacial surgical pro-
edures, and several complications can occur post-peratively.1,2 The impairment of lower lip and chinensation up to the midline owing to inferior alveolarerve (IAN) injury is one of the complications relatedo mandibular third molar surgery. The IAN travels inhe mandibular canal within the mandible in closeroximity to the apices of the lower molar teeth. Itainly carries sensory fibers and supplies the mandib-
*Sir John Walsh Research Institute, University of Otago School of
entistry, Dunedin, New Zealand.
Address correspondence and reprint requests to Dr Atieh: Sir
ohn Walsh Research Institute, School of Dentistry, University of
tago, PO Box 647, Dunedin 9054 New Zealand; e-mail:
2010 American Association of Oral and Maxillofacial Surgeons
278-2391/10/6801-0013$36.00/0
boi:10.1016/j.joms.2009.04.074
74
lar lower teeth, as well as the chin and lower lip.lthough permanent numbness is not common, the
emporary altered sensation can last for variable peri-ds, depending on the surgical method,3,4 experiencef the surgeon,5,6 and the relationship between theandibular third molar and the IAN.7,8
The incidence of transient IAN injury after removalf a lower third molar has ranged from 0.4%5 to0.3%,9 and the reported risk of permanent IAN injurychronic paresthesia) has been less than 1%.8,10-12 Areoperative evaluation of the true relationship be-ween the roots of the mandibular third molar and theAN would help in predicting, and possibly avoiding,ensory impairment. Therefore, radiography has beenoutinely used as a part of the preoperative assess-ent before the extraction of the lower third molar.
everal investigators have described the anatomic re-ationship of the IAN and mandibular third molareeth and have identified several radiologic signs (Ta-
le 1).13-19 These signs have been regarded as the
sijdvsaer
cterIlmbpntmm
M
wtc
M1Rsguner
rvhnnIrnAMJnOTet
bi1asItcaiwdtbmegttv
DD
NDI
DN
M y. J Or
MOMEN A. ATIEH 75
tandard markers for identifying the likelihood of IANnjury. However, the accurate prediction of IAN in-ury remains a problematic issue owing to the lack ofetailed information obtained through the use of con-entional 2-dimensional methods. Other methodsuch as computed tomography could provide a moreccurate assessment of the position of the IAN. How-ver, it is costly and subjects the patients to greateradiation dosage.20
Today, pantomography is the imaging method ofhoice to assess impacted lower third molars andheir relationship with the IAN.7 Several studies havevaluated the diagnostic accuracy of the panoramicadiographic findings in identifying patients at risk ofAN injury after extraction of the lower third mo-ars.7,21,22 However, the use of such a radiographic
odality as a preoperative diagnostic tool has nevereen assessed systematically. Thus, the purpose of theresent systematic study was to evaluate the diag-ostic accuracy of the radiologic signs in predictinghe degree of intimacy between the IAN and theandibular third molars using conventional panto-ography.
aterials and Methods
The present study was conducted in accordanceith the principles of the Cochrane Collaboration and
he guidelines in reporting reviews of diagnostic ac-uracy (the STARD Intuitive).23
SEARCH METHOD
The following electronic databases were searched:EDLINE (1969 to October 1, 2008); EMBASE (1980/
981 to October 2008); the Cochrane Methodologyegister (to October 1, 2008); and the ISI Web ofcience. The search was performed without any lan-uage restriction and the following keywords weresed: “inferior alveolar nerve” or “inferior dentalerve” and “injury” or “damage” and “third molarxtraction” or “third molar surgery” and “panoramic
Table 1. RADIOGRAPHIC MARKERS
Sign
arkening of root13,15 Increased radioluceneflected roots17,18 Abrupt deviation of
canal or around itarrowing of root19 Deep grooving or park and bifid of root apex19 Double shadow of p
nterruption of radiopaque bordersof mandibular canal15,19
Deep grooving or p
iversion of mandibular canal19 Upward displacemearrowing of mandibular canal19 Reduction of diamet
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiograph
adiography” or “orthopantomogram” or “pantomog- a
aphy” and “sensitivity” or “specificity” or “predictivealue” or “likelihood ratio.” Additionally, a compre-ensive manual search of the following dental jour-als from 2000 to 2008 was conducted: British Jour-al of Oral and Maxillofacial Surgery, Clinical Oralnvestigations, Dento-Maxillo-Facial Radiology, Eu-opean Journal of Oral Sciences, International Jour-al of Oral and Maxillofacial Surgery, Journal of themerican Dental Association, Journal of Cranio-axillofacial Surgery, Journal of Dental Research,
ournal of Oral and Maxillofacial Surgery, and Jour-al of Orofacial Pain, Oral Surgery Oral Medicineral Pathology Oral Radiology and Endodontology.he bibliographies of all the retrieved articles, confer-nce proceedings, and abstracts were further searchedo identify other relevant studies.
STUDY SELECTION
All the studies that investigated the relationshipetween IAN injury and third molar surgery were
ncluded if they met the following inclusion criteria:) the use of panoramic radiography in the preoper-tive evaluation; 2) the use of at least 3 radiologicigns13,15,19 to describe the relationship between theAN and lower third molars; and 3) the inclusion ofhe outcomes of interest or sufficient raw data toalculate the sensitivity, specificity, and diagnosticccuracy of each radiographic marker in relation tonjury or exposure of IAN. The reference standard
as composed of the clinical findings and follow-upuring and after surgical extraction of the mandibularhird molar. An intraoperative sighting of the IANundle indicated its close relationship to the thirdolars.24 Thus, the exposure of the IAN at surgical
xtraction or the presence of paresthesia was re-arded as positive reference standard results. Pares-hesia was defined as any postoperative sensation ofingling, pricking, or numbness of the tissues inner-ated by the IAN. The reviewer was not masked to
Description
e to impingement of canal on molar rootsroots to buccal or lingual or both sides of mandibular
ion of molar root where canal crosses itntal membrane where canal crosses apexion of molar roots
andibular canal as it crosses lower third molarcanal as molar roots pass partially or completely around it
al Maxillofac Surg 2010.
cy dumolar
erforateriodo
erforat
nt of mer of
uthors’ identity, affiliations, or journal identification.

u1ppfissd(
o(stegct
wttDMptsra
iorftc
oLmpip(tTa(dad0ptwtoaishees
R
sriecssniso(t
mMp
76 DIAGNOSTIC ACCURACY OF PANORAMIC RADIOGRAPHY
DATA ABSTRACTION
The following data were extracted from each studysing an extraction form developed by the reviewer:) authors’ names; 2) country of origin; 3) year ofublication; 4) demographic characteristics of thearticipants; 5) type of impaction; 6) radiographicndings; 7) true-positive results; 8) false-positive re-ults; 9) false-negative results; 10) true-negative re-ults; 11) sensitivity; 12) specificity; 13) positive pre-ictive value (PPV); and 14) negative predictive valueNPV).
QUALITY ASSESSMENT
The QUADAS tool25,26 was used to assess the meth-dologic quality of the diagnostic accuracy studiesTable 2). The scale consists of 14 items, whichhould be answered as “yes,” “no,” or “unclear.” Theool does not calculate a summary quality score forach study. Incorporating an overall quality score isenerally subjective, and it does not take into ac-ount the importance of each item and any poten-ial biases.27,28
STATISTICAL ANALYSIS
The analysis was conducted using RevMan soft-are, version 5.0 (RevMan, Copenhagen, Sweden;
he Nordic Cochrane Centre, the Cochrane Collabora-ion, 2008), and Meta-DiSc software, version 1.4 (Meta-iSc, Clinical Biostatistics Unit, Ramón y Cajal Hospital,adrid, Spain). For each radiographic marker, the true-ositive, false-positive, false-negative, and true-nega-ive results were calculated. The overall pooledensitivity, specificity, PPV, NPV, positive likelihoodatio (LR�), negative likelihood ratio (LR�), and di-gnostic odds ratio (DOR) for each radiographic find-
Table 2. QUADAS LIST25,26
Item No. Description
1 Representative patient spectrum2 Clear description of selection criteria3 Acceptable reference standard4 Acceptable delay between tests5 Avoiding partial verification bias6 Avoiding differential verification bias7 Avoiding incorporation bias8 Sufficient description of index test9 Sufficient description of reference test
10 Blinded interpretation of index test results11 Blinded interpretation of reference test results12 Availability of clinical data to the researchers13 Reporting of uninterpretable/intermediate/
indeterminate results14 Explanation of withdrawals from study
Data from Whiting et al.25,26
vomen A. Atieh. Diagnostic Accuracy of Panoramic Radiogra-
hy. J Oral Maxillofac Surg 2010.
ng were either extracted or calculated using the dataf the 2-by-2 contingency tables. The variation in theesults across the studies was assessed visually usingorest plots and statistically using Cochran’s Q test. Inhe case of heterogeneity, P less than .1 was usuallyonsidered significant.A random-effects model was used to calculate the
verall pooled estimates of sensitivity, specificity, andRs with 95% confidence intervals (CIs). The LRseasure the discriminating ability of a diagnostic orredictive test, with a high LR� and lower LR�
ndicating good discriminating ability. The forestlot and summary receiver operating characteristicSROC) curve were generated to graphically presenthe interaction between sensitivity and specificity.he overall test performance was quantified using therea under the SROC curve. The area under the curveAUC) measures the overall capacity of the test toiscriminate between participants with the diseasend those without it. An AUC of 0.5 indicates pooriscriminative ability; 0.75 to 0.92 is good, 0.93 to.97 is very good, and an area of 1.0 indicates aerfect test.29 The DOR is a single summary statistichat describes the odds of positive test results in thoseith the disease compared with the odds of positive
est results in those without the disease. The DOR isften constant, regardless of the diagnostic threshold,nd ranges from 0 to infinity, with greater valuesndicating greater accuracy.30 Meta-regression analy-is can be used to investigate the potential sources ofeterogeneity, such as study design, sampling method,xposure time, and other imaging characteristics. How-ver, such an analysis was not attempted because of themall number of included studies.
esults
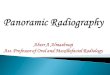
The initial electronic search identified a total of 940tudies (Fig 1). Of these 940 studies, 13 potentiallyelevant studies were selected for additional exam-nation. After a full article review, 8 studies werexcluded for the following reasons: 3 had usedomputed tomography findings as the referencetandard,31-33 3 had not used the radiologic markers totudy the relationship between the mandibular ca-al and the roots of the third molar,34-36 and 2 had
nsufficient data to calculate the sensitivity andpecificity.37,38 Thus, 5 studies,21,22,39-41 with a totalf 1,179 patients were included in the meta-analysisTable 3). No additional studies were identifiedhrough the manual search or reference checks.
DESCRIPTIVE RESULTS
All the participants required extraction of 1 orore mandibular third molars. A total of 894 obser-
ations of the 3 standard radiographic markers13,15,19

wcetcmsrmirpotta
aipawsem
ttisemmn
iggTwfsm
atmtpa
M y. J Or
MOMEN A. ATIEH 77
ere made in 1,793 operation sites. One study41 in-luded both prospective and retrospective data. How-ver, the retrospective data were excluded, becausehe use of panoramic radiography was not clear in allases. Another study was prospective,39 and the re-aining 3 studies were retrospective.21,22,40 Of the 5
tudies, 2 studies22,39 described the diagnostic accu-acy according to the results of IAN exposure afterandibular third molar extraction, and 3 stud-
es21,40,41 reported the presence of IAN injury as theeference standard. Because the objective of theresent review was to assess the diagnostic accuracyf panoramic radiography in detecting the close rela-ionship between the mandibular canal and lowerhird molars, both reference methods were accepted,nd all the studies were included in the meta-analysis.
QUALITY ASSESSMENT
The methodologic quality of the included studies wasssessed using the QUADAS 14-item list.25,26 For the firsttem, 2 studies39,41 failed to report the age groups of theatients; thus, their representative spectrum was scoreds “unclear.” All the selected studies recruited patientsho required extraction of the mandibular third molars,
tated the place of recruitment, used an acceptable ref-rence standard, reported IAN exposure or injury after
Sa
Final number of eligible studies includethe meta-analysis (n=5)
S---
Potentially appropriate studies identifieddetailed full-text evaluation (n=13)
Total number of studies identified fromelectronic search (n=940)
FIGURE 1. Flowcha
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiograph
andibular third molar surgery without delay in all par- 9
icipants, and described the use of pantomography ashe index test. Thus, all the studies scored “yes” fortems 2 to 8 and items 12 to 14. However, item 9 wascored as “unclear” for all the studies, because the ref-rence standard was determined by an objective assess-ent and lacked the description of more subjectiveeasures such as the use of light touch, pin prick,oxious heat, or 2-point discrimination.With regard to blinding, only 2 studies21,22 scored
tem 10 as “yes,” because the use of blinded investi-ators for the assessment of the preoperative radio-raphic findings of the pantomography was reported.he blinded assessment of the reference test resultsas not clearly stated, and item 11 was scored as “no”
or 2 studies39,40 and “unclear” for the remaining 3tudies.21,22,41 The quality assessment results are sum-arized in Table 4.
META-ANALYSIS
All the selected studies were included in the meta-nalysis of the 3 predefined radiographic markers. Forhe diagnostic ability of the “darkening of the root”arker in identifying an intimate relationship be-
ween the third molar and the mandibular canal, theooled sensitivity was 51.2% (95% CI 42% to 60%),nd the pooled specificity was 89% (95% CI 87% to
excluded after screening the titles bstracts (n=927)
excluded (n=8): se of computed tomography (n=3) logical criteria was not used (n=3) icient data (n=2)
ing review process.
al Maxillofac Surg 2010.
tudiesnd/or a
d in
tudies The u Radio Insuff
for
the
rt show
0%; Fig 2). Thus, the pooled PPV was 23.9%, and the

psut
.s1d
S
C
PM
E
PS
S
P
N
ve; PP
M y. J Or
11111
M
78 DIAGNOSTIC ACCURACY OF PANORAMIC RADIOGRAPHY
ooled NPV was 96.3%. Significant heterogeneity forensitivity and specificity was observed, allowing these of SROC. The pooled LR� was 4.26 (95% CI 2.47o 7.34) and the pooled LR� was 0.60 (95% CI .47 to
Table 3. STUDY CHARACTERISTICS
Characteristic Bell39
tudy design Prospective
ountry UnitedKingdom
atients (n) 219ean age (yr) NR
xtracted lower thirdmolars/radiographic observations (n)
300/135
revalence of IAN injury/exposure (%) 12ensitivity (%)
Darkening of root 34Interruption of radiopaque bordersof mandibular canal
34
Diversion of mandibular canal 2.9pecificity (%)
Darkening of root 96Interruption of radiopaque bordersof mandibular canal
63
Diversion of mandibular canal 99.6PV (%)Darkening of root 52Interruption of radiopaque bordersof mandibular canal
11
Diversion of mandibular canal 50PV (%)Darkening of root 92Interruption of radiopaque bordersof mandibular canal
88
Diversion of mandibular canal 89
Abbreviations: NR, not reported; IAN, inferior alveolar ner
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiograph
Table 4. METHODOLOGIC QUALITY ASSESSMENT
Item Be
1. Representative patient spectrum Un2. Clear description of selection criteria Ye3. Acceptable reference standard Ye4. Acceptable delay between tests Ye5. Avoiding partial verification bias Ye6. Avoiding differential verification bias Ye7. Avoiding incorporation bias Ye8. Sufficient description of index test Ye9. Sufficient description of reference test Un0. Blinded interpretation of index test results No1. Blinded interpretation of reference test results No2. Availability of clinical data Ye3. Reporting of uninterpretable results Ye4. Explanation of withdrawals from study Ye
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiography. J Or
78), indicating acceptable predictive ability. Theummary DOR was calculated at 8.0 (95% CI 4.32 to4.81) and the AUC at 0.77, demonstrating reasonableiagnostic performance.
eseral21
Gomeset al40
Rood andShehab41
Sedaghatfaret al22
pective Retrospectivecohort
Prospective Retrospectivecohort
States Brazil UnitedKingdom
United States
5 153 552 23034ls 27
19.96 NR 24
250 260/75 760/157 423/277
2 3.5 3.08 5.7
5 33 38 710 22 24 75
0 11 29 42
3 80 95 864 94 96 66
2 98 98 89
1 5.6 17 245 11 14 12
4 20 33 19
3 97 98 983 94 98 98
9 96 98 96
V, positive predictive value; NPV, negative predictive value.
al Maxillofac Surg 2010.
Blaeseret al21
Gomeset al40
Rood andShehab41
Sedaghatfaret al22
Yes Yes Unclear YesYes Yes Yes YesYes Yes Yes YesYes Yes Yes YesYes Yes Yes YesYes Yes Yes YesYes Yes Yes YesYes Yes Yes YesUnclear Unclear Unclear UnclearYes No Unclear YesUnclear No Unclear UnclearYes Yes Yes YesYes Yes Yes YesYes Yes Yes Yes
Blaet
Retros
United
2CasesContro
50/
3
68
5
75
8
32
3
99
8
ll39
clearsssssssclear
sss
al Maxillofac Surg 2010.

tipFswaLtsa
a(9hmwg1Ao(tr
Belsd
hmtdrc4ctc
D
farcboim
ttdsmrmit
Frt
M
Fs
M y. J Or
MOMEN A. ATIEH 79
For the “interruption of the radiopaque borders ofhe mandibular canal,” the calculated pooled sensitiv-ty was 53.5% (95% CI 44.5% to 62.3%), and theooled specificity was 80% (95% CI 78.1% to 81.8%;ig 3). The sensitivity and specificity both showedignificant heterogeneity. The pooled PPV and NPVas 15.6% and 96.1%, respectively. The predictive
bility was considered average, because the pooledR� was estimated at 2.05 (95% CI 1.33 to 3.15), andhe pooled LR� was 0.69 (95% CI 0.48 to 0.99). Theummary DOR for this radiographic marker was lowert 3.66 (95% CI 1.50 to 8.95), with an AUC of 0.70.
For the “diversion of the mandibular canal,” thenalysis showed an overall pooled sensitivity of 29.4%95% CI 21.8% to 38.1%) and pooled specificity of4.7% (95% CI 93.6% to 95.7%; Fig 4), with significanteterogeneity among the included studies. Further-ore, the pooled PPV was 27.9%, and the pooled NPVas 95.1%. The predictive ability was considered
ood, with a pooled LR� of 5.49 (95% CI 2.58 to1.71) and pooled LR� of 0.77 (95% CI 0.52 to 1.14).similar reasonable discriminative ability was dem-
nstrated, with an estimated summary DOR of 7.7395% CI 3.83 to 15.61) and AUC of 0.70. The AUCs ofhe SROCs for the 3 radiographic markers are summa-ized in Figure 5.
The post-test probability was calculated usingayes’ theorem,42 and the pretest probability wasstimated at a mean of 11.3%, considering the preva-ence of IAN injury/exposure reported in the selectedtudies. Thus, 35% of patients with a panoramic ra-iographic marker of “darkening of the roots” would
IGURE 3. Forest plot of sensitivity and specificity for marker, inepresent point estimates of sensitivity and specificity, and black linerue negative.
IGURE 2. Forest plot of sensitivity and specificity for marker, daensitivity and specificity, and black lines, its 95% CIs. TP, true-po
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiograph
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiography. J Or
ave a true close relationship between the lower thirdolars and the mandibular canal, and only 21% of
hose with an “interruption of the radiographic bor-ers of the mandibular molars” would have a trueelationship. The greatest post-test probability wasalculated for the third radiographic marker, because1.2% of patients with “diversion of the mandibularanal” would have a true intimate relationship be-ween the lower third molars and the mandibularanal.
iscussion
The present systematic review and meta-analysisollowed the guidelines of the STARD committee23
nd Cochrane Collaboration in evaluating the accu-acy of the 3 panoramic radiographic criteria used bylinicians to evaluate the risk of injury to the IANundle. Five studies, with a total of 894 observationsf the 3 chosen radiographic markers, were included
n the meta-analysis to investigate the proximity of theandibular canal to the lower third molars.The radiographic markers were the darkening of
he root or increased radiolucency, interruption ofhe radiopaque borders of the mandibular canal, andiversion of the mandibular canal. Those 3 signs wereelected because they have been described as theost significant markers for the prediction of a close
elationship between the IAN and the lower thirdolars.7,41 A high specificity (the ability to exclude an
ntimate relationship) and low sensitivity (the abilityo identify a true intimate relationship) was demon-
ion of radiographic borders of mandibular canal. Solid squares5% CIs. TP, true-positive; FP, false-positive; FN, false-negative; TN,
g of third molar roots. Solid squares represent point estimates ofP, false-positive; FN, false-negative; TN, true negative.
al Maxillofac Surg 2010.
terrupts, its 9
rkeninsitive; F
al Maxillofac Surg 2010.

st7tt“g
etesT
bcotcrgta
tsu
Fs
M y. J Or
Fo
M
80 DIAGNOSTIC ACCURACY OF PANORAMIC RADIOGRAPHY
trated, with an area under the SROC of 70% for bothhe “interruption” and the “diversion” markers and7% for the “darkening” marker. A moderate diagnos-ic accuracy was also demonstrated by the values ofhe summary DORs (8.00, 3.66, and 7.73 for thedarkening,” “interruption,” and “diversion” radio-raphic markers, respectively).Panoramic radiography is therefore more reliable in
xcluding the close relationship between the root andhe nerve in the absence of these radiographic mark-rs than in confirming the presence of a true relation-hip in the presence of these radiographic findings.he low sensitivity of the radiographic markers can
IGURE 4. Forest plot of sensitivity and specificity for marker, diensitivity and specificity, and black lines, its 95% CIs. TP, true po
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiograph
IGURE 5. SROC curves for 3 radiographic markers. Symbols reprverall diagnostic accuracy.
omen A. Atieh. Diagnostic Accuracy of Panoramic Radiography. J Or
e partly explained by the 2-dimensional nature ofonventional radiography and the anatomic positionf the mandibular canal, which is located buccally tohe roots of the lower third molars in 61% of theases, on the lingual side in 33%, and between theoots in 3%.43 Thus, the presence of 1 of the radio-raphic markers is not necessarily an accurate indica-ion of the intimate relationship between the rootsnd the canal.
The present review had several limitations. First,he analysis was performed on a small number oftudies. Second, the search strategy did not identifynpublished data, which could have contributed to
of mandibular canal. Solid squares represent point estimates ofFP, false positive; FN, false negative; TN, true negative.
al Maxillofac Surg 2010.
ncluded studies in meta-analysis, and solid lines (SROCs) represent
versionsitive;
esent i
al Maxillofac Surg 2010.

trprsraitmuib
atgtMthowtbmddaafanat
aiihrscpottt
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
MOMEN A. ATIEH 81
he publication bias. Nevertheless most systematiceviews of diagnostic tests have failed to include un-ublished data, because studies of diagnostic accu-acy are not common or registered as interventiontudies. Third, heterogeneity was evident among theesults across the included studies, which could bettributed to the experience of the examiners, errorsn exposure and positioning, and the overall quality ofhe radiographs. However, the present study showedoderate levels of diagnostic accuracy and a limited
sefulness of the conventional radiographic markersn the preoperative assessment of the relationshipetween the third molars and the mandibular canal.Despite its limitations, panoramic radiography has
lways been recommended as the radiographic inves-igation of choice in the practice of third molar sur-ery.7,44 Such an imaging technique has been provedo be relatively safe, reliable, and readily accessible.oreover, the incidence of complications or injury to
he inferior alveolar neurovascular bundle might notave been alarming enough to question the reliabilityf such an investigation. However, the dilemma ariseshen the surgeon must decide whether more de-
ailed radiologic investigations are required. It haseen suggested that the radiographic finding of 2 orore markers might improve the sensitivity in pre-
icting a true intimate relationship and hence an in-ication for applying other imaging techniques suchs computed tomography to confirm the diagnosisnd provide the surgeon with additional detailed in-ormation about the anatomy of the mandibular canalnd third molar roots.32 However, such imaging tech-iques might still be less popular among cliniciansnd patients owing to the cost and dose-related fac-ors.
A true close relationship between the third molarsnd the mandibular canal increases the risk of IANnjury, and an accurate evaluation of the relationships essential to avoid the risk of surgery. Surgeons,owever, should be aware of the limitations of theadiographic markers of panoramic radiography andhould consider more detailed imaging in specificases in which more than 1 radiographic marker isresent. Additional studies are needed to examinether predictive markers and investigate a cost-effec-ive, safe, and accessible radiographic technique forhe preoperative assessment of the relationship be-ween the third molar roots and mandibular canal.
eferences1. Mercier P, Precious D: Risks and benefits of removal of im-
pacted third molars: A critical review of the literature. Int J OralMaxillofac Surg 21:17, 1992
2. Daley TD: Third molar prophylactic extraction: A review andanalysis of the literature. Gen Dent 44:310, 1996
3. Rood JP: Permanent damage to inferior alveolar and lingualnerves during the removal of impacted mandibular third mo-
lars: Comparison of two methods of bone removal. Br Dent J172:108, 1992
4. Rud J: Reevaluation of the lingual split-bone technique forremoval of impacted mandibular third molars. J Oral MaxillofacSurg 42:114, 1984
5. Sisk AI, Hammer WB, Shelton DW, et al: Complications follow-ing removal of impacted third molars: The role of the experi-ence of the surgeon. J Oral Maxillofac Surg 44:855, 1986
6. Bataineh AB: Sensory nerve impairment following mandibularthird molar surgery. J Oral Maxillofac Surg 59:1012, 2001
7. Bouloux GF, Steed MB, Perciaccante VJ: Complications of thirdmolar surgery. Oral Maxillofac Surg Clin North Am 19:117,2007
8. Wofford DT, Miller RI: Prospective study of dysesthesia follow-ing odontectomy of impacted mandibular third molars. J OralMaxillofac Surg 45:15, 1987
9. Brann CR, Brickley MR, Shepherd JP: Factors influencing nervedamage during lower third molar surgery. Br Dent J 186:514,1999
0. van Gool AV, Ten Bosch JJ, Boering G: Clinical consequencesof complaints and complications after removal of the mandib-ular third molar. Int J Oral Surg 6:29, 1977
1. Alling CC III: Dysesthesia of the lingual and inferior alveolarnerves following third molar surgery. J Oral Maxillofac Surg44:454, 1986
2. Carmichael FA, McGowan DA: Incidence of nerve damagefollowing third molar removal: A West Scotland oral surgeryresearch group study. Br J Oral Surg 30:78, 1992
3. Main J: Further roentgenographic study of mandibular thirdmolars. J Am Dent Assoc 25:1993, 1938
4. Austin LT: Perforation of roots of impacted lower third molarsby contents of mandibular canal: Report of a case. Am J OrthodOral Surg 33:623, 1947
5. Howe GL, Poyton HG: Prevention of damage to the inferiordental nerve during the extraction of mandibular third molars.Br Dent J 109:355, 1960
6. Merrill RG: Prevention, treatment and prognosis for nerveinjury related to the difficult impaction. Dent Clin North Am23:471, 1979
7. Stockdale CR: The relationship of the roots of mandibular thirdmolars to the inferior dental canal. Oral Surg Oral Med OralPathol 12:1061, 1959
8. Waggener DT: Relationships of third molar roots to the man-dibular canal. Oral Surg Oral Med Oral Pathol 12:853, 1959
9. Seward GR: Radiology in general dental practice. VIII. Assess-ment of lower third molars. Br Dent J 115:45, 1963
0. Ngan DC, Kharbanda OP, Geenty JP, et al: Comparison ofradiation levels from computed tomography and conventionaldental radiographs. Aust Orthod J 19:67, 2003
1. Blaeser B, August MA, Kaban LB, et al: Radiographic risk factorsfor inferior alveolar nerve injury during third molar extraction.J Oral Maxillofac Surg 61:417, 2003
2. Sedaghatfar M, August MA, Dodson TB: Panoramic radio-graphic findings as predictors of inferior alveolar nerve expo-sure following third molar extraction. J Oral Maxillofac Surg63:3, 2005
3. Bossuyt PM, Reitsma JB, Bruns DE, et al: Towards complete andaccurate reporting of studies of diagnostic accuracy: TheSTARD intuitive. Radiology 226:24, 2003
4. Tay AB, Go WS: Effect of exposed inferior alveolar neurovas-cular bundle during surgical removal of impacted lower thirdmolars. J Oral Maxillofac Surg 62:592, 2004
5. Whiting P, Rutjes AW, Reitsma JB, et al: The development ofQUADAS: A tool for the quality assessment of studies of diag-nostic accuracy included in systematic review. BMC Med ResMethodol 3:25, 2003
6. Whiting P, Weswood ME, Rutjes AW, et al: Evaluation ofQUADAS, a tool for the quality assessment of diagnosticaccuracy studies. BMC Med Res Methodol 6:9, 2006
7. Juni P, Witschi A, Bloch RM, et al: The hazards of scoring thequality of clinical trials for meta-analysis. J Am Med Assoc
282:1054, 1999
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
82 DIAGNOSTIC ACCURACY OF PANORAMIC RADIOGRAPHY
8. Whiting P, Harbord R, Kleijinen J: No role for quality scores insystematic reviews of diagnostic accuracy studies. BMC MedRes Methodol 5:19, 2005
9. Deeks JJ: Systematic reviews of evaluation of diagnostic andscreening tests, in Egger M, Smith GD, Altman DG (eds):Systematic Reviews in Health Care: Meta-Analysis in Context(ed 2). London, BMJ Publishing, 2001, pp 248-282
0. Glas AS, Lijmer JG, Prins MH, et al: The diagnostic odds ratio:A single indicator of test performance. J Clin Epidemiol 56:1129, 2003
1. Better H, Abramovitz I, Shlomi B, et al: The presurgical workupbefore third molar surgery: How much is enough? J Oral Max-illofac Surg 62:689, 2004
2. Monaco G, Montevecchi M, Alessandri B, et al: Reliability ofpanoramic radiography in evaluating the topographic relation-ship between the mandibular canal and impacted third molars.J Am Dent Assoc 135:312, 2004
3. Nakamori K, Fujiwara K, Miyazaki A, et al: Clinical assessmentof the relationship between the third molar and the inferioralveolar canal using panoramic images and computed tomog-raphy. J Oral Maxillofac Surg 66:2308, 2008
4. Susarla SM, Dodson TB: Estimating third molar extraction dif-ficulty: A comparison of subjective and objective factors. J OralMaxillofac Surg 63:427, 2005
5. Gülicher D, Gerlach KL: Sensory impairment of the lingual andinferior alveolar nerves following removal of impacted mandib-ular third molars. Int J Oral Maxillofac Surg 30:306, 2001
6. Bell GW, Rodgers JM, Grime RJ, et al: The accuracy of dentalpanoramic tomographs in determining the root morphology ofmandibular third molar teeth before surgery. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 95:119, 20037. Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C: Inferioralveolar nerve damage after lower third molar surgical ex-traction: A prospective study of 1117 surgical extractions.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92:377,2001
8. Jerjes W, El-Maaytah M, Swinson B, et al: Inferior alveolar nerveinjury and surgical difficulty prediction in third molar surgery:The role of dental panoramic tomography. J Clin Dent 17:122,2006
9. Bell GW: Use of dental panoramic tomographs to predict therelation between mandibular third molar teeth and the inferioralveolar nerve: Radiological and surgical findings, and clinicaloutcome. Br J Oral Maxillofac Surg 42:21, 2004
0. Gomes AC, Vasconcelos BC, Silva ED, et al: Sensitivity andspecificity of pantomography to predict inferior alveolar nervedamage during extraction of impacted lower third molars.J Oral Maxillofac Surg 66:256, 2008
1. Rood JP, Shehab BA: The radiological prediction of inferioralveolar nerve injury during third molar surgery. Br J OralMaxillofac Surg 28:20, 1990
2. Deeks JJ, Altman DG: Diagnostic tests 4: Likelihood ratios. BMJ329:168, 2004
3. Tammisalo T, Happonen RP, Tammisalo EH: Stereographicassessment of mandibular canal in relation to the roots ofimpacted lower third molar using multiprojection narrowbeam radiography. Int J Oral Maxillofac Surg 21:8, 1992
4. The Faculty of General Dental Practitioners, the Royal Col-lege of Surgeons of England: Selection Criteria for DentalRadiography. London, Royal College of Surgeons of England,
1998, p 20


![Accuracy of Panoramic Radiography for Detection of Periapical Endodontic … · 2020. 4. 20. · International Endodontic Journal, 40(6), 433-440 [9] Jimenez-Pinzon A, Segura-Egea](https://img.pdfslide.net/doc/110x75/5fe9e4b773d7b255640d3dca/accuracy-of-panoramic-radiography-for-detection-of-periapical-endodontic-2020-4.jpg)