Embed Size (px)
Citation preview

Dow
nloadedfrom
https://journals.lww.com
/continuumby
BhDMf5ePH
Kav1zEoum1tQ
fN4a+kJLhEZgbsIH
o4XMi0hC
ywCX1AW
nYQp/IlQ
rHD3bhnalqTQ
iPuGRXx5KyPdFZxo9C
56RINY1tvxttd6Q
zCr6PR
M+bdgG
w==
on06/18/2020
Downloadedfromhttps://journals.lww.com/continuumbyBhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3bhnalqTQiPuGRXx5KyPdFZxo9C56RINY1tvxttd6QzCr6PRM+bdgGw==on06/18/2020
Diagnostic Approachto Diplopia
Marc Dinkin, MD
ABSTRACTPurpose of Review: This article offers a pragmatic roadmap to the practicingneurologist on how to approach the patient with double vision. Strategies of historytaking and examination techniques are reviewed, followed by a broad overview of thecauses of diplopia organized by neuroanatomic localization. Diplopia may be the firstsymptom of serious vision or life-threatening neurologic disease, and its correctlocalization and diagnosis are therefore essential. The systems responsible for ocularmovement and alignment in the vertical and horizontal plane include complexsupranuclear circuitry, brainstem nuclei, cranial nerves III, IV, and VI, and their respectiveneuromuscular junctions and target muscles. Disruption at any point within this systemor within the vestibular afferents that govern eye movement in response to headmovements may therefore produce diplopia, leading to a broad differential diagnosisfor the patient with diplopia. With a careful history and examination, the neurologistshould be able to observe the patterns of diplopia that reveal the site of dysfunction,thus generating a shorter localization-specific list of possible etiologies. Examination ofocularmotility including smooth pursuit and saccadic function, followed, if necessary, bytesting designed to uncovermisalignments of the eyes, including cover andMaddox rodtesting, are primary components of the efferent neurologic examination. Further testingdesigned to detect myasthenia (eg, lid testing and fatigable upgaze) and orbital disease(eg, measuring proptosis, testing for resistance to retropulsion) may be necessary.Recent Findings: Recent advances in the diagnosis of diplopia include the observationthat vertical diplopia from skew deviation is more likely to improve with supinepositioning than that caused by trochlear nerve palsies. Advances in the field of ocularmyasthenia include the observation of decreased conversion to the generalized formwith treatment with either steroids or thymectomy, although these conclusions need tobe confirmed by prospective, randomized trials. Rarely, pure ocular myasthenia may beassociated with the muscle-specific tyrosine kinase (MuSK) antibody.Summary: With proper skills, the neurologist can elucidate the localization of diplopia,even in cases of complex ocular misalignment, and generate a management plan thatcan address the underlying disease, and, in many cases, ameliorate or cure the diplopia.
Continuum (Minneap Minn) 2014;20(4):942–965.
INTRODUCTIONDouble vision, or diplopia, is a com-mon visual concern that may be thefirst warning of vision-threatening orlife-threatening neurologic disease.While some cases of diplopia areaccompanied by obvious ocular motil-ity deficits that allow easy diagnosis ofan underlying injury, often the physical
findings are more subtle and can bevexing to neurologists and ophthalmolo-gists alike. The evaluation of diplopia,using a detailed and targeted history, anexamination of ocular alignment andmotility, and, when appropriate, neuro-imaging of the brain and orbits, is anessential skill for all practicing neurolo-gists. This article will take a broad view of
Address correspondence toDr Marc Dinkin, Weill CornellOphthalmology, 1305 YorkAvenue, Floor 11, New York,NY 1002,[email protected].
Relationship Disclosure:Dr Dinkin has receivedpersonal compensation formedical record review andaffidavit preparation fromseveral law firms and hasserved on an advisory boardfor Acorda Therapeutics.
Unlabeled Use ofProducts/InvestigationalUse Disclosure:Dr Dinkin reports no disclosure.
* 2014, American Academyof Neurology.
Supplemental digital content:Videos accompanying this ar-ticle are cited in the text asSupplemental Digital Content.Videos may be accessed byclicking on links provided inthe HTML, PDF, and iPadversions of this article; theURLs are provided in the printversion. Video legends beginon page 963.
942 www.ContinuumJournal.com August 2014
Review Article
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

diplopia, offering the reader a frameworkfor the focused attainment of patienthistory as well as a comprehensive reviewof the efferent neuro-ophthalmic exami-nation and how it may be used todistinguish the various categories of dis-ease that may present with double vision.
ANATOMIC FRAMEWORKThis section provides a brief review of theneuroanatomic pathways that govern eye
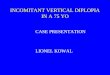
movements and stabilize them within theorbits duringheadmovements.Figure 8-1summarizes the pathways responsiblefor horizontal eye movements, includingyoked versions (conjugate movementsof the eyes) and vergence (convergenceand divergence) movements, as well asthe horizontal vestibular ocular re-sponse. Figure 8-2 addresses the samesystems in the vertical plane.1,2 In bothfigures, the boxed elements indicate
KEY POINT
h Diplopia may be thepresenting symptom ofpotentially blinding orlife-threatening disease.The ability to localize,workup, and appropriatelymanage double vision isessential to the practicingneurologist.
FIGURE 8-1 Control of horizontal eye movements. Voluntary lateral gaze is governed by theparapontine reticular formation (PPRF), under cortical control by the contralateralfrontal eye field. The PPRF excites the adjacent abducens nucleus (VIn) which
contains two major populations of neurons. The first are the cell bodies of the abducens nerve thatstimulates the ipsilateral lateral rectus (LR). The second population of neurons are interneurons whoseaxons decussate and ascend within the medial longitudinal fasciculus (MLF) to synapse with theneurons of the medial rectus subnucleus (MR [white text]) of the oculomotor nucleus (IIIn). Theseneurons then form the branch of the third nerve to the medial rectus, resulting in yoked adductionof the contralateral eye together with abduction of the ipsilateral eye. The convergence nucleus (CN)activates as part of the accommodative reaction, resulting in bilateral MR (white text) activation. Thehorizontal vestibular ocular reaction is governed by the horizontal semicircular canal (HSCC). Withleft head turn, endolymphatic fluid deforms hair cells in the cupula of the HSCC, leading to activationof the vestibular nerve (VIII) and the ipsilateral medial vestibular nucleus (MVN). The contralateral VInis stimulated in turn, leading to contralateral gaze, as described above. Pathologic conditions areshown in boxes: a lesion of the PPRF or VIn would cause an ipsilateral gaze palsy. Note that aninternuclear ophthalmoplegia results from a lesion of the MLF. The VIn fires, resulting in abduction ofthe ipsilateral eye, but the message to adduct never reaches the contralateral medial rectus muscle(MR [black text]). One-and-a-half syndrome results from a lesion encompassing the VIn and the MLFon one side. Thus, there is an ipsilateral gaze palsy and a contralateral internuclear ophthalmoplegia.
Aq = aqueduct; R = red nucleus; CI = convergence insufficiency; NMJ = neuromuscular junction.
943Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

points in the pathway where disruptionmay result in diplopia.
HISTORYTaking a careful history can oftenlocalize the site of anatomic dysfunctioncausing diplopia and, in some cases,even delineate the underlying diseaseprocess, before even examining thepatient or obtaining any neuroimaging.
Question 1: Does the DoubleVision Go Away When ClosingEither Eye?If the diplopia persists with either eyeopen by itself, it is monocular, resultingfrom aberrant refraction, so that identi-cal light rays land on different parts ofthe retina. The patient typically de-scribes a second ‘‘ghost image.’’ Astig-matism,3 corneal pathology, dry eyes,
KEY POINTS
h Yoked horizontal eyemovements arecontrolled by a series ofnuclei and tracts,including theparapontine reticularformation, abducensnucleus, mediallongitudinal fasciculus,and the medial rectussubnucleus of cranialnerve III. The ability todistinguish centralcauses of horizontaldiplopia from cranialneuropathies or orbitaldisease depends on anunderstanding of therelevant neuroanatomy.
h Vertical eye movementsare governed by therostral interstitialnucleus of the mediallongitudinal fasciculusand interstitial nucleusof Cajal, both located inthe mesencephalon.These nuclei control theoculomotor nucleiresponsible for verticalgaze and the trochlearnucleus.
h A careful history of apatient’s double visionmay elucidate theetiology before theexamination is started.Queries regarding thepresence of diplopiawith either eye closed,in the distance andnear, and in variousfields of gaze, may beused to confirm andlocalize a neurologiccause of diplopia.
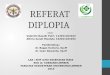
FIGURE 8-2 Control of vertical eye movements. Vertical saccades are governed by the rostralinterstitial nucleus of the medial longitudinal fasciculus (riMLF), while theinterstitial nucleus of Cajal (INC) is involved in smooth pursuit and maintenance
of the eyes in eccentric vertical gaze. The medial riMLF stimulates the ipsilateral inferior rectussubnucleus of IIIn (IR [white text]) resulting in ipsilateral depression and IVth nucleus (IVn),whose fibers decussate and cause contralateral depression. There are also fibers from the INCthat decussate to the opposite riMLF, so that its activation would result in activation of all fourmuscles of depression. Upgaze appears to be governed by the lateral riMLF, which stimulatesthe inferior oblique (IO [white text]) and superior rectus (SR [white text]) subnuclei of IIIn,resulting in ipsilateral and contralateral (the SR fibers decussate) elevation, respectively. Therelative height of the two eyes is governed by afferents from the utricle that sense body or headtilt. Ipsilateral head tilt results in utricular activation, carried by the vestibular branch of theeighth nerve (VIII) to the medial vestibular nucleus (MVN), which in turn activates compensatorycontralateral depression (red dotted lines) and ipsilateral elevation (not shown). Injury to thispathway mimics activation of the contralateral pathway, resulting in a pathologic verticalstrabismus known as a skew deviation. Damage within the medulla prior to decussation wouldtherefore result in ipsilateral depression, while injury to the midbrain portion above itsdecussation would result in hypertropia on the side of the lesion.
Aq = aqueduct; R = red nucleus; SR (black text) = superior rectus muscle; NMJ = neuromuscularjunction; SO = superior oblique muscle; IR (black text) = inferior rectus muscle; IO (black text) =inferior oblique muscle.
944 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

complex cataracts, poorly centeredintraocular lenses, and severe structuralretinal pathology4 should be consid-ered. If the issue is refractive, thediplopia will usually resolve with appli-cation of a pinhole or proper correc-tion of astigmatism. Diplopia caused byocular misalignment (binocular) re-solves with closure of either eye.
Question 2: Are the Two ImagesSeparatedVertically, Horizontally,Obliquely, or Torsionally?Once the diplopia is confirmed asbinocular, the orientation of the twoimages should be elucidated. Purehorizontal diplopia suggests medial rec-tus or lateral rectus dysfunction (whichcan result from cranial neuropathies,orbital pathology, or myasthenia), or aninternuclear ophthalmoplegia (INO).Pure vertical diplopia suggests either atrochlear nerve palsy or skew deviation,the latter of which reflects an imbalancein the vestibular-ocular signal governingocular torsion and vertical alignment inresponse to body or head tilt. Obliquediplopia may result from oculomotorpalsies (since muscles governing bothhorizontal and vertical motility can beaffected), diffuse orbital disease, orocular myasthenia. Trochlear nervepalsies may also result in torsionaldiplopia, caused by extorsion of theaffected eye.
Question 3: Is the DiplopiaWorse at Distance or at Near?Worsening of horizontal diplopia atdistance, such as when driving, isconsistent with lateral rectus orabducens nerve dysfunction, sinceabduction is necessary for divergence.Worsening of horizontal diplopia atnear, typically manifesting as troublereading or seeing a smartphone, isconsistent with medial rectus dysfunc-tion, as may be found in an oculomo-tor palsy, since adduction is required
for convergence, but may also reflecta convergence insufficiency, whichmanifests as a limitation of conver-gence in the presence of full medialrectus function.
Question 4: In Which DirectionIs the Double Vision Worse?Worsening of vertical diplopia indowngaze implicates either a trochlearpalsy or inferior rectus weakness, whilea worsening in upgaze will occur incomplete third nerve palsies since thereis weakness of both the superior rectusand inferior oblique. A worsening inupgaze also occurs in inferior obliqueoveraction, since the affected eye willelevate more than normal in upgaze. Aworsening of horizontal diplopia inlateral gaze in one direction implicateseither the ipsilateral lateral rectus orcontralateral medial rectus. The answerto question 3 can distinguish the two.
Question 5: Is There a Historyof Congenital Strabismus orAbnormal Head Position?The term strabismus refers to anyocular misalignment of the eyes, butmay specifically be used to refer to acongenital misalignment which typi-cally reflects a deficiency in higher-order neuromuscular control of eyeposition, and may also reflect cranialneuropathies or muscle defects.Chronic head turns or tilts are acommon compensatory response.Surprisingly, many patients will notinclude a remote history of strabismusin their past medical history untilspecifically asked, and most will notconsider an abnormal head positionimportant. Since adult-onset diplopiamay result from a decompensation ofa childhood strabismus, the examinershould always inquire about priorstrabismus, a ‘‘lazy eye,’’ eye patchingas a child, childhood eye surgery, andany abnormal head positions.
945Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Question 6: Are AssociatedPain, Headache, or NeurologicSymptoms Present?Headache may accompany aneurysmalthird nerve palsies but also occurs in62% of ‘‘microvascular’’ cranial neu-ropathies,5 which refer to infarctionsof the cranial nerves presumably dueto insufficiency of the vasa nervorum,typically in patients with vascular riskfactors such as hypertension or diabe-tes mellitus. In patients aged 55 orover, the presence of a concurrentheadache, scalp tenderness, or jawclaudication should raise the questionof temporal arteritis. Finally, pain witheye movement suggests orbital dis-ease, such as idiopathic orbital inflam-mation, or an orbital apex lesion.
EXAMINATIONMotility: Ductions, Versions,and VergencesA careful assessment of ocular motilityis essential to localization and diagno-sis of diplopia. Examining each eyeindividually (ductions) may reveal sub-tle limitations of movement in one eyethat could be missed if visualizedalongside a fellow eye with greaterlimitations. This is followed by anexamination of both eyes together,versions. See Supplemental DigitalContent 8-1, links.lww.com/CONT/A124 for a demonstration of testingof versions. To test versions, thepatient is asked to fixate on a targetwhich is then slowly moved laterally,testing the lateral rectus of theabducting eye and medial rectus ofthe adducting eye. Once in lateralposition, the target is moved superi-orly and then inferiorly. This will testthe superior rectus and inferior rectus,respectively, in the abducted eye andthe inferior oblique and superioroblique, respectively, in the adductedeye. The same is then repeated incontralateral gaze. Torsional motility
may be noted to occur in oppositionto head or body tilting when aided bythe presence of prominent conjuncti-val vessels. Convergence and diver-gence may be tested by the slowmovement of the fixation target intoward the nose and outward again.
Forced DuctionsIn cases of orbital disease, diplopiafrequently results from restriction ofan extraocular muscle due to infiltra-tion, fibrosis, or bony entrapmentfollowing trauma. In such cases, aworsening in a certain direction sug-gests restriction of the antagonistmuscle. For example, a vertical diplo-pia that worsens in upgaze in a patientwith thyroid eye disease is likely toreflect inferior rectus restriction ratherthan superior rectus weakness. Oph-thalmologists, after anesthetizing thecornea, may attempt to move the eyepassively by gently grabbing hold ofthe conjunctiva with a forceps or eventwo Q-tips. If the eye still will notmove in the direction of weakness, arestrictive etiology is likely.
Misalignment: Tropias andPhoriasIn some cases, diplopia occurs inpatients with full or near-full motilityof both eyes but whose eyes arenevertheless misaligned. This suggestscongenital strabismus but also is typ-ical for skew deviations,6 and even incases of some ocular motor palsies,the limitations in motility may besubtle. When the misalignment ispresent with both eyes open, it is calleda heterotropia or tropia, but if it mani-fests only when stereo fusion is disrupted(eg, with unilateral eye closure), it istermed a heterophoria or phoria. Pre-fixes may be used to qualify the direc-tion of the misalignment: exotropiarefers to outward deviation, esotropiato inward deviation, hypertropia to
KEY POINTS
h The diplopia examinationbegins with testing ofductions (themovement of each eyeindividually), versions(both eyes moving in thesame direction), andvergences (the eyesmoving in oppositehorizontal direction).Forced duction testingcan be performed by anophthalmologist andmay reveal a restrictionsuggestive of orbitaldisease.
h A tropia is amisalignment of theeyes that manifests evenwith both eyes open. Aphoria is a misalignmentthat is only presentwhen binocular vision isdisrupted, as whencovering one eye.
946 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

elevation of an eye, and hypotropia to alower eye. Exophoria, esophoria,hyperphoria, and hypophoria are usedto describe the misalignment for phorias.Several methods are used to determinethe relative position of the two eyes invarious fields of gaze and ultimatelylocalize the cause of the diplopia.
Cover TestingWhen the patient’s visual acuity, abilityto move the eyes, and ability tocooperate are all intact, cover testingmay help indicate a tropia or phoria.
Cover-uncover test. The cover-uncover test differentiates a tropiafrom a phoria. First, one eye is occludedwhile the patient is fixating on a target.If the fellow eye shifts to pick upfixation, it must have been deviatedprior to occlusion of the other eye, andone can conclude that a tropia ispresent. If, however, the fellow eyedoes not shift, but instead the occludedeye moves in the direction of weaknesswhile covered (noted as the eye returnsto fixation after the occluder is re-moved), a phoria is present. In eithercase, the type of tropia or phoria can bedetermined by noting the direction ofrefixation of the deviated eye. An inwardmovement of an eye when it is uncov-ered informs the examiner that the eyehad been outwardly deviated whencovered, which is called an exo (tropiaor phoria). An outward movement withuncovering reflects a prior inward devi-ation or eso. If the uncovered eyemovesdownward, it is consistent with anipsilateral hyper or contralateral hypo.
Alternate cover test. By alternatingwhich eye is covered, the physicianwill bring out phorias and tropias, andcan quickly determine the direction ofdeviation. Even when misalignment isthe result of unilateral eye weakness,both eyes will move when uncoveredduring the alternate cover test. Thisresults from the Hering law of equal
innervation, which states that an equalforce must be supplied to both eyes.In a mild left abducens palsy, forexample, a covered left eye will devi-ate medially and refixate to the targetwhen uncovered. When the right eyeis covered, however, a good deal ofleftward force must be applied to pullthe weak left eye to fixation and thatsame force applied to the healthyright eye deviates it medially (second-ary deviation). When it is uncovered, ittoo will have to refixate from anadducted position. Finally, a prismrod with multiple strengths may beplaced over one eye and steadilyincreased until the refixation move-ments cease, thus estimating theprism required to ameliorate the dip-lopia. Typically, patients benefit from astrength of 50% to 75% of the mea-sured prism, ensuring some contin-ued effort on their part. The examinermay perform the alternate cover testin the nine cardinal fields of gaze tolook for changes in the degree ofrefixation. In the case of vertical de-viations, checking in right and lefthead tilt is also helpful. When thepatient is gazing in the direction of aneye’s weakness, the movements will begreater (Supplemental Digital Content8-2, links.lww.com/CONT/A125).
Maddox Rod TestingA Maddox rod is a red lens with multiplealigned prisms that will convert a whitelight into a red line. During testing, thelens is held over the right eye (byconvention), while a light is shined atthe patient. The left eye will see the whitelight, but the right eye will see a red line,which can be horizontal (to test verticalalignment) or vertical (to test horizontalalignment). Thus, akin to covering oneeye, stereo fusion is disrupted, andphorias will emerge. A review of horizon-tal and vertical Maddox rod techniques ispresented in Figure 8-3 and Figure 8-4,
KEY POINT
h Ocular misalignments(phorias and tropias)may be observed usingthe alternate cover testor Maddox rod test.Testing in the ninecardinal fields of gaze aswell as in head tilt canelucidate the pattern ofweakness and helplocalize the responsiblelesion.
947Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

respectively. Although its limitations, in-cluding the induction of excessiveesophoria and inability to see the redline in some patients, have been notedsince the beginning of the 20th century,7
Maddox rod testing remains a practicaland fast means of assessing phorias inmost patients.
Parks-BielschowskyThree-Step TestAs described by Marshall Parks,8 asuperior oblique palsy can be identi-fied in three steps:
1. Determine which eye is hypertropic.2. Confirm that the hypertropia
worsens in contralateral gaze.3. Confirm that the hypertropia
worsens in ipsilateral head tilt.
An ophthalmologist might answerthese questions bymeasuring the prism
needed to correct the hypertropia ineach position, but the author finds thateliciting a subjective response from thepatient regarding the distance betweenthe red line and white light on theMaddox rod test (in each direction ofgaze and in head tilt) provides a fasterand, in most cases, equally reliablesolution. The test is not perfect, as thispattern may be mimicked by orbitaldisease or ocular myasthenia gravis.
Double Maddox rod. Bilateraltrochlear palsy may be seen after headtrauma or congenitally occur. It maybe elusive, as one palsy dominates inprimary gaze, but will produce acharacteristic pattern of a hypertropiain lateral gaze of whichever eye isadducted and a V-pattern esotropia(meaning that the esotropia is worsein downgaze) due to weakness of the
FIGURE 8-3 Horizontal Maddox rod. A, Patient with a left esotropia. B, The right eye (OD) sees a vertical red line in themiddle, but the left eye (OS) sees the white light (yellow in the figure for illustrative clarity) deviated to the left.The result is a white light to the left of the red line with both eyes (OU) open. C, Repeat testing in right andleft gazes indicates a worsening in left gaze, consistent with lateral rectus weakness of the left eye.
948 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

superior oblique’s tertiary function, ie,abduction. Because the superioroblique intorts the eye (rolls it alongthe coronal plane so that the top ofthe eye rotates toward the nose), aunilateral fourth nerve palsy will resultin extorsion of an eye (the top of theeye is rotated toward the ear), but byonly 10 degrees or less. In bilateraltrochlear palsies however, intorsion ofboth eyes is affected so that thecombined extorsion is higher, at amedian of 14.5 degrees.9 The doubleMaddox rod test allows the neuro-ophthalmologist to quantify the relativeextorsion of the two eyes and detect thepresence of bilateral trochlear palsies.One Maddox lens is placed at 0 degrees
while the other is offset by about10 degrees and a light is shined at thepatient. Using a knob, the patient isasked to rotate the second lens until thered lines ‘‘line up.’’ The resulting devia-tion reflects the total relative extorsionbetween the two eyes.
Hirschberg TestOne may more easily detect a tropiaby comparing the location of thereflection of a penlight on the corneaof both eyes, termed the Hirschbergtest. This is particularly useful whenpoor vision or cooperation precludescover testing or Maddox rod examina-tion. In the case of an exotropia, forexample, the reflection will fall medial
KEY POINT
h Using a Maddox rodover each eye (doubleMaddox rod test), thepractitioner canestimate the degree ofocular torsion betweenthe two eyes, as is seenin cases of fourth nervepalsy.
Fig
44/
C
FIGURE 8-4 Vertical Maddox rod. A, Patient with a left hypertropia. B, The right eye (OD) sees a horizontal red line in themiddle, but the left eye (OS) sees the white light (yellow in the figure for illustrative clarity) below it. The patientsees a white light under a red line with both eyes (OU) open, consistent with a left hypertropia. C, The hypertropiais worse in right gaze, downgaze, and left head tilt, all consistent with a fourth nerve palsy.
949Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

to the pupillary axis in at least one eye. Inthe Krimsky test, various prisms may beheld in front of an eye until onenormalizes the location of the reflection,thus estimating the degree of misalign-ment and required prism needed to treatthe diplopia. This test has recently beenshown to correlate well with measure-ments using cover testing.10
FunduscopyFunduscopy may provide additionalclues to the etiology of diplopia.Papilledema in the setting of esotropiasuggests intracranial hypertension-related abducens palsies. Retinal pig-mentary deposition in association withdiffuse ophthalmoplegia and ptosis sug-gests the mitochondrial disease Kearns-Sayre syndrome. Finally, retinal arteryocclusion or anterior ischemic opticneuropathy, in association with anacute ocular motor palsy, reflects tem-poral arteritis until proven otherwise.
Viewing the fundus under highmagnification can help the neuro-ophthalmologist confirm torsional de-viations of either eye. Dilation is neces-sary, as the optic disc and fovea wouldneed to be seen simultaneously. Ahorizontal light beam projected acrossthe fovea will typically cross the opticdisc with approximately one-third of thedisc below it.11 Cyclotorsion (turning inthe coronal plane) of the eye in eitherdirection will cause the beam to inter-cept the disc either higher or lowerthan normally predicted.12
Afferent Neuro-ophthalmicExaminationIn any patient with diplopia, assessmentof afferent visual function is essential. Aretrobulbar optic neuropathy accompany-ing cranial nerve III, IV, or VI dysfunctionsuggests an orbital apex syndrome, whilea bitemporal hemianopia suggests asuprasellar lesion with chiasmal compres-sion and spread to the cavernous sinus,
such as a large pituitary adenoma orpituitary apoplexy. The recognition ofamblyopia in an eye, which manifests asdecreased acuity in the absence ofspecific optic nerve field defects, ishelpful in identifying a decompensationof a congenital phoria that was associat-ed with the amblyopia.
General Neurologic ExaminationA complete neurologic examination isessential to the localization and diag-nosis of most disorders responsible fordiplopia. For example, the recognitionof a hemiparesis contralateral to a thirdnerve palsy suggests injury at thelevel of the third nerve fascicle as itpasses through the cerebral peduncle.Areflexia would suggest Guillain-Barresyndrome or the Miller-Fisher variant,while an associated delirium or amne-sia raises the specter of Wernickeencephalopathy.
PATTERNS OF DISEASEDetecting Infantile StrabismusPatients with a strabismus of infantileonset may manage to fuse for years, untilage, disease, or drug exposures lead toan eventual decompensation and associ-ated diplopia. Determining when this isthe case is crucial in preventing needlessworkups and anxiety. Examples of infan-tile strabismus syndromes include con-genital trochlear nerve palsies, Duanesyndrome (abducens palsy with globeretraction in adduction), Brown syn-drome (congenital fibrosis of the superi-or oblique tendon with depression inadduction), and inferior oblique overac-tion with an associated V-patternesotropia. Methods used to detect suchcases are summarized in Table 8-1.
Ruling Out Orbital DiseaseDouble vision may be the first or onlysign of diseases affecting the orbit, in-cluding thyroid eye disease, inflammatorydisease, trauma, infection, neoplasm, and
KEY POINTS
h The general neurologicexamination, testing ofafferent visual function,and the funduscopicfindings all may helplocalize the lesionresponsible for diplopia.
h Extraneous workups canbe avoided by therecognition ofcongenital strabismuspatterns. A tolerance bythe patient of strongprisms (fusionalamplitude), thepresence of chroniccontralateral head tilt inpast photographs incases of trochlear nervepalsy, and globein cases of abducenspalsy (Duane syndrome)are all suggestive ofcongenital disease.
950 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

congenital myopathies. Such conditionsmay be missed by the neurologist who isnot as accustomed to thinking aboutorbital disease. Red flags include propto-sis, periorbital edema, resistance toretropulsion, and lid retraction. An oph-thalmologist may quantify the degree ofproptosis using a Hertel ophthal-mometer, which uses angled mirrors tosimultaneously project lateral views ofboth eyes with superimposed rulers.However, the general neurologist maybe able to estimate the severity ofproptosis simply by viewing the patientfrom the side and noting the anteriorextent of one eye versus the other.Resistance to retropulsion refers to alimitation in the degree of backwardmovement of the globe when gentlypushed on with two fingers during eyeclosure. Its presence suggests aretrobulbar tumor or thyroid eye dis-ease, although in one study the physi-cians’ estimation of the resistance didnot reliably predict the actual forceneeded to push the eye back.13
As previously mentioned, the mo-tility limitation in orbital disease oftenreflects antagonist muscle restrictionrather than weakness of the agonistmuscle. MRI of the brain only shows afew slices through the orbits andwill often miss orbital disease. Thincuts through the orbits, with T1fat-saturated images (removing thebright T1 signal of intraorbital fat)increase sensitivity for orbital disease,while orbital CT is especially useful incases of trauma and suspected bonyabnormalities. As orbital disease is notcovered elsewhere in this issue of
, special attention willbe given here.
Orbital inflammation. Idiopathicorbital inflammation (formerly knownas orbital pseudotumor) can affect themuscles, soft tissue, and even opticnerve, potentially resulting in blind-ness. In some cases, only one muscleis affected, producing an orbital myo-sitis. In addition to diplopia, patientstypically report pain, especially with
KEY POINTS
h Orbital disease is afrequent mimicker ofneurogenic diplopia andis most frequently theresult of orbitalinflammation, thyroideye disease, or orbitaltumors.
h Signs of orbital diseaseinclude proptosis,conjunctival injection orswelling, resistance toretropulsion, and apositive forced ductiontest.
TABLE 8-1 Testing for Infantile Strabismus
Examination Description
Fusional amplitude In the case of vertical phorias, chroniccompensation results in a tolerance fora wide range of vertical deviations suchthat the patient will fuse the images andnot experience diplopia even when moreprism is given than required. This range isknown as the fusional amplitude. Scoresof 93 diopters suggest chronicity.
Worsening of trochlearpalsy in upgaze
This finding suggests secondary inferior obliqueoveraction that occurs over many years.
Family album tomography(‘‘FAT scan’’)
A review of older pictures of the patientmay reveal a head tilt contralateral to thehypertropia, offering further reassuranceof a congenital trochlear palsy.
Forced duction In cases of Brown syndrome, the adductedeye will not elevate with passive attempts becauseof superior oblique tendon restriction. Thisdistinguishes it from an inferior oblique paresis.
951Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

eye movement, proptosis, and, insevere cases, vision loss. Sarcoidosis,rheumatoid arthritis, and some vascu-litides (including granulomatosis withpolyangiitis14 and, rarely, giant cellarteritis15) may lead to orbital inflam-mation (Figure 8-5). Recently, somecases of idiopathic orbital inflamma-tion, particularly with inflammation ofthe ocular adnexa (ie, eyelids, lashes,extraocular muscles, and lacrimal sys-tem), have been linked to IgG4, asubclass of IgG that appears linkedwith multiple forms of systemic in-flammatory disease.16 Table 8-2 pro-
vides a review of inflammatory orbitaldisease and appropriate testing.
Treatment of idiopathic orbital in-flammation includes corticosteroids,nonsteroidal anti-inflammatory drugs(NSAIDS), and, in rare cases, radiationtherapy, but in one 10-year retrospec-tive study evaluating all treatmentmodalities, only 63% showed a long-term complete remission.17
Thyroid eye disease. A lymphocyticinflammatory infiltration of the orbitaltissues occurs in approximately 50% ofpatients with Grave disease and somewith Hashimoto thyroiditis.18 Smoking,
FIGURE 8-5 Examples of orbital inflammation in three patients. A, Orbital myositis of medialrectus (yellow arrow) seen on orbital MRI. The diagnosis was missed on multiplebrain MRIs. B, Bilateral orbital inflammation (yellow arrows) was the first sign of
disease in this patient with temporal arteritis. Note temporal artery enhancement (blue arrow). C,Massive infiltration of eye muscles on the right, especially lateral rectus (yellow arrow) was seenin this patient with proptosis. Elevated angiotensin-converting enzyme (ACE) level and extensionoutside of the orbit to the pterygopalatine fossa in the same patient (D, green arrows) suggestedsarcoidosis.
952 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

family history, and female sex are riskfactors. Clinical findings include prop-tosis, conjunctival injection (redness)over points of eye muscle insertion,
chemosis (swelling of the conjunctiva),and lid edema and erythema (Figure 8-6).The difficult task of distinguishing thyroideye disease from other inflammatory
TABLE 8-2 Types of Inflammatory Orbital Disease and Workup
Type Workup
Sarcoidosis Chest CT, angiotensin-converting enzyme(ACE) level
Thyroid eye disease Thyroid function tests, thyroid antibodies
Systemic lupuserythematosus
Antinuclear antibody (ANA)
Rheumatoid arthritis Rheumatoid factor (RF)
Granulomatosiswith polyangiitis
Central antineutrophilic cytoplasmic antibody(c-ANCA)
Giant cell arteritis Erythrocyte sedimentation rate (ESR),C-reactive protein (CRP), temporal artery biopsy
FIGURE 8-6 Thyroid eye disease. A, A 65-year-old woman presented with lid erythema andedema, lid retraction, conjunctival injection, chemosis, and proptosis of botheyes. Note the widening of the palpebral fissure of the left eye. B, Coronal
noncontrast CT reconstruction of the orbits revealed thickening of multiple extraocularmuscles. C, Axial noncontrast CT of the orbits. Note the relative sparing of the medial rectustendons in both eyes (red arrows). D, Axial postcontrast MRI of a different patient whopresented with diplopia and a left optic neuropathy. Note the crowding at the left orbital apex(yellow arrow) consistent with thyroid eye disease.
953Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

diseases of the orbit is made easier bythe recognition of several classic findings,described in Table 8-3.
Orbital neoplasm. Orbital neo-plasm, whether in the form of a bulkytumor or diffuse infiltration of musclesand soft tissues, may present withdiplopia. Proptosis and resistance toretropulsion are common features, butsuperior orbital tumors may result in adownward displacement of the globe inthe orbit, hypoglobus, while metastaticbreast cancer may cause enophthalmos,a recession of the globe within theorbit.21 Table 8-4 demonstrates therelative incidence of orbital tumors inone study.22 While the lack ofdiffusion-weighted signal on MRI wasshown to predict benign disease with a75% concordance rate in one study,23
biopsy is necessary for a definitivediagnosis. Figure 8-7 describes the rareoccurrence of a granulocytic sarcomain the orbit presenting as diplopia.
Diplopia associated with traumaand defects in the bony orbit. Asdemonstrated by Figure 8-8, directmechanical orbital trauma may
cause ophthalmoparesis through re-striction and entrapment of orbitalmuscles or even muscle disinsertionfrom the globe. Hypoglobus andenophthalmos are common. OrbitalCT is the preferred imaging study insuch cases as it clearly shows bonyfractures and defects. Early surgicalrepair of the orbital wall with relaxa-tion of involved muscles can helpprevent scarring.
Rarely, obstruction of the ostium ofthe maxillary sinus can block aeration,producing a negative pressure thatpulls down on the inferior wall of theorbit. This silent sinus syndrome mayresult in enophthalmos and a down-ward displacement (hypoglobus) ofthe eye, the latter of which may leadto a vertical diplopia.24
Iatrogenic DiplopiaTrauma to extraocular muscles mayoccur after cataract, retina, orbital, andsinus surgery. Diplopia occurs in0.17% to 0.85% of patients followingcataract extraction.25 In one largestudy, approximately 25% of cases
KEY POINTS
h Signs of thyroid eyedisease include lidretraction, lid lag,increased intraocularpressure in upgaze, andsparing of the tendonson orbital CT or MRI.
h The orbit may beaffected by a widevariety of neoplasmsthat cause diplopia,including benign lesions(eg, dermoid cysts,cavernous hemangiomas)and malignant lesions (eg,non-Hodgkin lymphoma,adenoid cystic carcinoma,and metastases).
h Double vision may resultfrom orbital trauma,typically due to muscleentrapment within abony fracture. Theselesions may be missedon general brain MRI, soorbital imaging shouldbe pursued in any casesof suspectedtrauma-related diplopia.
TABLE 8-3 Findings in Thyroid Eye Disease
Finding Description
Lid retraction Results from circulating thyroid hormoneand, eventually, infiltration and scarringof the levator palpebrae.
Lid lag (Von Graefe sign) Up to 8% of patients with thyroid eye diseasedemonstrate a delay in the lowering of the lidwith globe depression.19 Both lid retractionand lag may result in secondary keratopathy.
Increased intraocularpressure in upgaze
Greater than 4 mm Hg, presumably a resultof compression by inflamed inferior rectus;nonspecific and has been reported in controls.20
Tendon sparing Orbital imaging demonstrates enlargementand increased enhancement of the musclesand/or soft tissue of the orbits in both thyroid eyedisease and idiopathic orbital inflammation, theprimary difference being that the muscle tendonsare typically spared in thyroid eye disease.
954 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

TABLE 8-4 Orbital Tumors and Pseudotumors: Lesion Types in 268Consecutive Patients Undergoing Biopsies of SuspectedOrbital Tumorsa
Tumor% of All OrbitalTumors
Secondary orbital tumor 26%
Lymphoproliferative lesion (74% of which were lymphoma) 25%
Metastatic tumor 10%
Epithelial lacrimal gland tumors (67% of which wereadenoid cystic carcinoma)
10%
Inflammatory condition 8%
Vascular lesion 7%
Mesenchymal tumor 7%
Optic nerve or nerve sheath tumor 3%
Peripheral nerve tumor 1%
Histiocytic lesion 1%
Cystic lesion 1%
Miscellaneous G1%a Modified with permission from Shinder R, et al, Head Neck.22 B 2010 Wiley Periodicals, Inc.onlinelibrary.wiley.com/doi/10.1002/hed.21498/abstract.
FIGURE 8-7 Orbital tumor. A 20-year-old painter presented with oblique diplopia and a redand proptotic eye on the right (A). Neuro-ophthalmic examination revealedlimitation of adduction, elevation, and depression of the right eye. Thyroid eye
disease was suspected, but MRI orbits revealed a mass lesion in the lateral-superior orbit (B).A complete cell blood count showed a leukocytosis with blasts, and biopsy of the lesion (C)confirmed a granulocytic sarcoma. Chemotherapy was initiated for systemic leukemia and,within days, visual symptoms resolved (not shown) and the patient remained in remission.
955Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

involved muscle restriction or paresis,26
ostensibly due to trauma to the musclecone (where the origins of theextraocular muscles coalesce in the pos-terior orbit) from retro-orbital anesthesia,which occurs more frequently in the lefteye because of a greater difficulty of lefteye injections in right-handed surgeons.In these cases, most patients had either ahypotropia (54%) or hypertropia (44%)of the affected eye. Other mechanismsinclude an unmasking of a congenitalphoria with resumption of binocularvision (34%), a prismatic effect by theimplanted lens (4%), and concurrentonset of systemic disease (5%).
Detecting Myasthenia GravisEssentially any pattern of ophthalmoplegiaor ocular deviation can be mimicked by
myasthenia gravis, in which the neuro-muscular blockade of acetylcholine re-ceptors has a particular predilection forthe highly metabolic and fatigableextraocular muscles. An inherently sim-plified folding of the postsynapticendplate in extraocular muscles makesthem susceptible to the effects offurther simplification associated withacetylcholine receptor destruction, thuspredisposing them to loss of the safetyfactor that ensures proper neuromus-cular transmission.27 A recent historyof trouble breathing, swallowing, orwalking may suggest the disease,but generalized symptoms may beabsent (ocular myasthenia). The con-current finding of fatigable ptosis is ared flag, but, in unclear cases, severalexamination techniques, summarizedin Table 8-5, may prove pivotal inmaking the diagnosis.
These examination findings arecomplemented by further testing, whichmay include acetylcholine receptor anti-bodies (present in only 50% of ocularmyasthenia cases), muscle-specific tyro-sine kinase (MuSK) antibodies, repetitivestimulation nerve conduction testing,and single fiber EMG. Figure 8-9 de-scribes an examination of a patient withocular myasthenia gravis. SupplementalDigital Content 8-3, links.lww.com/CONT/A128, demonstrates enhancedptosis in a patient with the disease.Furthermore, improvement of eitherptosis or ophthalmoplegia after injectionof the acetylcholinesterase inhibitoredrophonium (edrophonium test),35 orafter 30 minutes of rest and lid closure(the sleep test),36 or 2 minutes ofapplication of ice (ice test)37 suggeststhe diagnosis.
TrendsThe existence of pure ocular myastheniaassociated with the MuSK antibody isquestionable. A large study of 110 pa-tients with MuSK myasthenia described
KEY POINTS
h Ocular myastheniapresents with isolatedfatigable ptosis and/orophthalmoplegia and isoften accompanied byfatigable upgaze,enhanced ptosis, and alid twitch.
h Screening for ocularmyasthenia includes theedrophonium test, sleeptest, and ice test. Thedisease may beconfirmed by thefinding of acetylcholinereceptor antibodies(although these are only50% sensitive), or adecrement on repetitivenerve stimulation. Thediagnosis is furthersupported by a findingof jitter on single fiberEMG.
FIGURE 8-8 Muscle entrapment. Apreviously healthy 53-year-old
woman reported vertical diplopia afterfalling down the stairs. Examination showedlimitation of elevation, depression, andadduction of the left eye, suggestive of aposttraumatic, partial third nerve palsy. Withan unremarkable MRI of the brain andmagnetic resonance angiography (MRA) ofthe head, the patient was prepared fordischarge. As no ptosis or mydriasis waspresent, a CT of the orbits was obtained andrevealed a blowout fracture of the inferiororbit and protrusion of the inferior rectusthrough the defect with associatedentrapment (red arrow).
956 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

36% with purely ocular symptoms atonset, but all subsequently generalized.38
However, some case reports have de-scribed chronic MuSK-related ocularmyasthenia without generalization, inone case over a 10-year period withoutimmunosuppression.39 The manage-ment of ocular myasthenia remainscontroversial. Since 50% to 80% ofpatients progress to generalized myas-thenia, prevention of this transforma-tion is a central goal of treatment, inaddition to ocular symptom control.Several studies have suggested thattreatment of ocular myasthenia withsteroids may decrease the conversionrate to generalized myasthenia,40,41 al-though the conclusion is tempered bythe retrospective, nonrandomized na-ture of these studies. Whether patients
with ocular myasthenia withoutthymoma should undergo thymectomyhas yet to be conclusively determined.In a recent retrospective study of 115Chinese patients with ocular myasthe-nia who underwent transsternal thy-mectomy, none developed generalizeddisease over a mean follow-up of 44.5months, suggesting a role for thesurgery even in purely ocular patients,but prospective, controlled trials areneeded to more conclusively confirmthe benefits of thymectomy.42
Cranial NeuropathiesDisease of the cranial nerves is cov-ered in detail in the article ‘‘DiplopiaDue to Ocular Motor Cranial Neurop-athies’’ by Wayne T. Cornblath, MD,FAAN, in this issue of .
TABLE 8-5 Examination Findings in Ocular Myasthenia
Finding Description
Fatigable upgaze Maintain upgaze for at least 1 minute beforeassessing for fatigability.
‘‘Cogan lid twitch28’’ A rapid recovery in the neuromuscular junction whilerested in downgaze results in enhanced release on returnto primary gaze. Also described in cases of brainstemtumors,29 parasellar tumors, and aneurysms.30 Sensitivityis 50% and positive predictive value is 25%.31
Curtaining Lifting of the weak lid leads to a slow drooping ofthe fellow lid, presumably related to the Hering lawof equal innervation.
‘‘Quiver movements32’’(lightning saccades)
Attributed to a relative preservation of the twitchfiber system responsible for the initiation of saccades,even as the tonic fiber system subserving later stagesof the saccade is injured. Pale global singly innervatedfibers, which fire at the onset of saccades and appearto govern the initial acceleration phase, possess amore complex postsynaptic folding than otherextraocular muscle fibers,33 which helps protect themfrom the effects of myasthenia. This may explainthe presence of these lightning saccades.
Orbicularis weakness Suggests ocular myasthenia gravis rather than cranialneuropathies.
Orbicularis ‘‘peek’’ sign Small palpebral fissure widening with scleral showfollowing a brief period of lid apposition against apatient’s gentle closure. Seen in 3 of 25 patients withocularmyasthenia gravis and 0 of 200 control subjects.34
957Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

The presence of an oculomotor, trochlear,or abducens palsy may reflect compres-sion, infiltration, inflammatory disease, or,especially in older patients, ischemia tothe nerve. Multiple cranial neuropathiessuggest disease of the brainstem, sub-arachnoid space, cavernous sinus, or, inthe presence of an optic neuropathy, theorbital apex. Infectious, inflammatory, orneoplastic meningitic processes maypresent with diplopia due to infiltrationof one of the ocular motor cranialnerves, as evidenced by a case of primaryCNS lymphoma presenting with a thirdnerve palsy (Case 8-1).
Checking for trochlear nerve palsyin the presence of a third nerve palsy.When a complete third nerve palsy
results in paralysis of the medial rectus,it is difficult to test for ipsilateralsuperior oblique weakness since it actsin the vertical plane during adduction.To test its function, the practitionermay instead bring the eye into theabducted position and ask the patientto look down, which should result inintorsion of the globe if the superioroblique is functional. Identifying con-comitant trochlear nerve palsy along-side an oculomotor nerve palsy iscrucial, in that it is unlikely to be theresult of the common and relativelybenign microvascular etiology43 andsuggests a localization either at theorbital apex or within the cavernoussinus.
KEY POINT
h In the presence of acomplete third nervepalsy, fourth nervefunction may beexamined by looking forintorsion of the globeduring combinedabduction-depression.
FIGURE 8-9 Ocular myasthenia. Eye appearance at rest (A) with prominent, nearly completeleft ptosis. Demonstration of enhanced ptosis or curtaining (B) shows developmentof right ptosis with manual elevation of the left lid. Eye appearance after a few
seconds of upgaze (C) shows left ptosis, but inferior third of the pupil and iris are visible. Eyeappearance after 120 seconds of upgaze (D) shows increased left ptosis with nearly completecoverage of the pupil and iris. E, Positive edrophonium test. Resolution of left ptosis 15 secondsafter administration of 1 mg of edrophonium.
Courtesy of Janet C. Rucker, MD.
958 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Case 8-1A 78-year-old woman with hypercholesterolemia presented with diplopia and ptosis. The ptosis began1 year ago and worsened later in the day. Two weeks ago, she awoke in the morning and noticed anoblique diplopia (the second image was higher and over to the right) that resolved with closure ofeither eye. She had tenderness over the head, intense fatigue, and a history of mild pain with chewingthat had since resolved. A noncontrast brain MRI was reported as normal.
On examination, there was an esotropia on left gaze consistent with a left abducens palsy. Anexotropia on right gaze was consistent with a left medial rectus palsy, and a left hypotropia worse inupgaze (and present in both adduction and abduction) indicated left superior rectus and inferioroblique weakness. Together with mild left ptosis, these findings suggested a left oculomotor palsy.Serum tests for temporal arteritis were normal. An MRI of the brain and orbits, with and withoutcontrast, revealed bilateral enlargement and enhancement of the oculomotor, trigeminal, and facialnerves (Figure 8-10). Spine MRI demonstrated diffuse nerve root enhancement. Gangliosides to asialomonosialotetrahexosylganglioside (GM)1 and GM2 were mildly elevated. Lumbar puncture revealed74 white blood cells/2L (93% lymphocytes), an elevated protein level of 101 mg/dL, a normal glucoselevel of 56 mg/dL, and elevated "2-microglobulin level, but cytology and flow cytometry werenegative. Over the next month, two more lumbar punctures were performed, both with similarprofiles and negative cytology, but a gene rearrangement analysis of the third sample was consistentwith a primary T-cell CNS lymphoma.
Comment. This case demonstrates that diplopia may be one of the first and only symptoms oflife-threatening disease, such as primary CNS lymphoma. Multiple diagnostic challenges were faced,including nonspecific symptoms suggestive of temporal arteritis and a reported fatigable ptosis,which, as shown here, may be present in third nerve palsies in addition to ocular myasthenia.The oblique nature of the patient’s double vision helped predict the examination finding of apupil-sparing oculomotor palsy, which in this age group is often microvascular. However, theexamination revealed the unexpected finding of a concomitant abducens palsy. Once multiple cranialneuropathies were discovered, a leptomeningeal process was suspected. Finally, the limitation ofnoncontrast brain MRI in the diagnosis of diplopia is evidenced by the fact that a contrast MRIrevealed obvious pathology of the cranial nerves soon after a noncontrast MRI was negative.
FIGURE 8-10 Imaging studies of the patient in Case 8-1. Enhancement and enlargement ofbilateral oculomotor nerves is seen in an axial contrast-enhanced T1-weightedMRI (A, red arrows). B, Coronal contrast-enhanced T1-weighted MRI demonstratesenlargement and enhancement of the bilateral oculomotor nerves (red arrows)and facial nerves (yellow arrows).
959Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Aberrant regeneration. Longstandingoculomotor nerve palsies may eventu-ally result in regrowth of nerve fibers tothe wrong target. Thus, the fibersmeant for the medial rectus mightinnervate the levator palpebrae or con-
strictor pupillae muscles, resulting in lidelevation or pupillary constriction, re-spectively, during adduction. The pres-ence of such aberrant regenerationconfirms the chronicity of the injuryand rules out a benign microvascular
FIGURE 8-11 A 23-year-old man presented with a left abduction defect (A) accompanied by aright gaze palsy (B). C, Fluid-attenuated inversion recovery (FLAIR) MRI (left)revealed a hyperintense mass lesion, which showed contrast enhancement on
postcontrast T1-weighted MRI (right) within the pons. D, Funduscopic examination revealedevidence of a prior posterior uveitis. Further history revealed a history of chronic mouth ulcers.A diagnosis of neuro-Behçet disease was made. In addition to oral and genital ulcers, Behçetdisease can cause a retinal vasculitis and brainstem inflammatory lesions. The clinical andradiologic examinations improved with steroid treatment (not shown).
960 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

etiology (Supplemental Digital Content8-4, links.lww.com/CONT/A126).
Supranuclear and InternuclearDiplopiaThere are essentially two main causes ofsupranuclear or internuclear diplopia,which are discussed in greater detail inthe article ‘‘Supranuclear Eye MovementAbnormalities’’ by Eric R. Eggenberger,DO, MSEpi, FAAN, in this issue of
.Internuclear ophthalmoplegia. In the
horizontal plane, disruption of the mediallongitudinal fasciculus (Figure 8-1)results in failed adduction of the ipsilat-eral eye in contralateral gaze, with anabducting nystagmus of the contralateraleye, together termed an internuclearophthalmoplegia. Sparing of conver-gence, if present, confirms internuclearophthalmoplegia, as it would not bespared with dysfunction of the oculo-motor nerve or the medial rectusmuscle. Pontine disease may also affectthe abducens nucleus or parapontinereticular formation, resulting in a conju-gate gaze palsy in the direction oppositeto the internuclear ophthalmoplegia, in
which case it is known as one-and-a-halfsyndrome.44 Alternatively, a conjugategaze palsy may occur in one directiondue to parapontine reticular formationinjury, with an abducens palsy in theother direction due to injury of theabducens nerve fascicle (Figure 8-11).
Skew deviation. In the verticalplane, skew deviation is a vertical mis-alignment of the eyes resulting frominappropriate utricular-vestibular-ocularoutput, essentially mimicking the phys-iologic vertical deviations that normallycompensate for head or body tilt. Ascan be seen in Figure 8-2 (red dashedline with arrows), the responsible path-ways emanating from the medial vestib-ular nucleus decussate in the pons,after which they travel along the mediallongitudinal fasciculus, so that a mesen-cephalic skew is frequently accompaniedby an internuclear ophthalmoplegiawhere the internuclear ophthalmoplegiais on the side of the higher eye. Becauseof this pontine decussation, a medullaryskew will result in the ipsilateral eye beinglower, while a mesencephalic skew willresult in the ipsilateral eye being higher.Figure 8-12 shows an example of skew.
KEY POINTS
h Internuclearophthalmoplegiareflects a lesion of themedial longitudinalfasciculus and results infailure of adduction ofthe contralateral eye inattempted gaze to oneside. When found inassociation with acontralateral gaze palsy,it is termed a one-and-a-half syndrome.
h When vestibular outputfrom the utricle regardingtilt of the head or bodyis disrupted on one side,the result is a pathologicvertical misalignment ofthe eyes known as askew deviation. Themisalignment is often, butnot always, comitant (equalin all directions of gaze).
h When skew deviationresults from a medullarylesion, the ipsilateral eye islower; when it results froma mesencephalic lesion,the ipsilateral eye is higher.
FIGURE 8-12 Skew deviation. A 22-year-old woman presented with a vertical diplopia and a left hypertropia. A, Trochlearnerve palsy was initially suspected until examination revealed a comitant hypertropia and improvement inthe supine position, consistent with skew. Additional findings included a torsional nystagmus, right facial
and left body numbness, and ocular-lateropulsion (a conjugate movement of the eyes toward the side of the lesion whenthe eyes are closed) all pointing to a right Wallenberg syndrome. MRI showed a fluid-attenuated inversion recovery (FLAIR)hyperintense (B, arrow) and enhancing (C, arrow) lesion in the right lateral medulla. Note that the lower eye was on the side ofthe lesion, which is the rule for medullary skew. Multiple sclerosis was diagnosed with the development of a subsequent lesion.
961Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Distinguishing a skew deviationfrom a trochlear nerve palsy. Whilethe typical pattern of skew deviation iscomitant (meaning that the ocularmisalignment is the same in all direc-tions of gaze and in both directions ofhead tilt), alternative patternsmay occur,and distinguishing skew from a fourthnerve palsy may be difficult. Someevidence suggests that the hypertropiaof skewmay improve in amplitude in the
supine position, as the utricle is takenout of the plane of gravity.45
Convergence insufficiency. WithParkinson disease, or rarely with advanc-ing age, convergence may become lim-ited, and adduction of the dominant eyemay be substituted, with the fellow eyeleft in primary position. Convergenceinsufficiency is also common in children,resulting in difficulty reading, oftenaccompanied by horizontal diplopia. In
KEY POINT
h The amplitude of thevertical misalignmentappears to improve inthe supine position inskew deviations but notwith trochlear nervepalsies.
FIGURE 8-13 A framework for the assessment of the patientwith diplopia. (1) Differentiatemonocular frombinocular diplopia.(2) If binocular, use history to predict localization. (3) Screen for fatigability and ptosis. If present, considermyasthenia. (4) If extraocular motility is limited, look for signs of orbital disease such as restriction, proptosis, or
positive forced ductions. (5) If no restriction occurs, use the pattern of limitation to diagnose cranial neuropathy or internuclearophthalmoplegia. (6) If extraocular motility is not limited but there is a tropia, use cover testing or Maddox rod to deduce thepattern of misalignment in multiple fields of gaze. (7) If vertical tropia is present, test for improvement in supine, indicative ofskew. Note that exotropia or esotropia that is comitant in all directions suggests an infantile strabismus. Alternatively, aninfantile esotropia or exotropiamay be comitant in the horizontal plane, but worsen in upgaze or downgaze.When an exotropia isworse in upgaze (or an esotropia is worse in downgaze), it is termed a V pattern. When an exotropia is worse in downgaze (or anesotropia is worse in upgaze), it is termed an A pattern. These patterns are suggestive of infantile strabismus.
IV = fourth nerve palsy; III = oculomotor nerve palsy; Hx = history; INO = internuclear ophthalmoplegia; B/L = bilateral;CI = convergence insufficiency; VI = abducens palsy; EOM = extraocular movements; EXO = exotropia; ESO = esotropia;HYPER = hypertropia; A/V = A pattern or V pattern; DI = divergence insufficiency; IOO = Inferior oblique overaction.
962 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

childhood convergence insufficiency,improvement occurred in 73% of pa-tients receiving office-based vergence/accommodative therapy with home re-inforcement versus 35% with placebotherapy.46 Prism glasses may be useful inadults with convergence insufficiency.
TrendsAn esotropia at distance in patients over65 years old in the absence of lateralrectus weakness has been termed dis-tance esotropia of the elderly. A recentstudy suggests that this entity may prog-ress over time, although the etiology forthis condition remains unknown.47
The sensitivity of the third step ofthe Parks-Bielschowsky Three-StepTest for true bilateral superior obliqueparesis was found to be only 40% inone study, although this limitation mayin part result from false-positive errorsusing the study’s criteria for the condi-tion which was the observation ofbilateral fundus extorsion (both fundiwere observed to be rotated along thecoronal plane so that the top of theretina was closer to the nose).48
A recent study reviewed 34 patientspresenting to the emergency depart-ment with painful ophthalmoplegia.The authors found that third and sixthnerve palsies were the most commonetiology, each accounting for 35% of thepatients. Of note, CT and MRI of thehead demonstrated low sensitivities forresponsible etiologies (14% and 50%,respectively), while an erythrocyte sedi-mentation rate of greater than 50 mm/hwas 100% sensitive for temporal arteritis,and pupillary mydriasis was 100% sen-sitive for aneurysmal causes.49
A ROADMAP FOR DIPLOPIAUsing the principles of history takingand examination discussed in thisarticle, the neurologist should able todiagnose even the most challengingcase of diplopia. An algorithm for the
localization of diplopia can be foundin Figure 8-13.
VIDEO LEGENDSSupplemental Digital Content 8-1
Testing of versions in a man with a left orbitalapex syndrome. Video shows a 75-year-old manwho developed gradually progressive proptosisand ptosis in his left eye accompanied by anoblique diplopia. Visual field loss and a relativeafferent pupillary defect ensued in the left eye aswell. Neuro-ophthalmic examination reveals thatthe left eye is depressed and deviates laterally inprimary gaze. Testing of versions show a lack ofadduction and elevation of the left eye, andlimited depression which, along with ptosis, isconsistent with a left oculomotor palsy. Abductionof the left eye is also limited, consistent with a leftabducens palsy.
The presence of a left oculomotor palsy andan ipsilateral abducens palsy is suggestive of eithercavernous sinus syndrome or orbital apex syn-drome. In this case, however, the presence of anoptic neuropathy (not shown), which would notoccur from a cavernous sinus lesion, is the cluethat the site of the lesion is the orbital apex. Theproptosis is also most consistent with an orbitalapex mass, and MRI with contrast (see axial andcoronal images at end of video) revealed a largeleft orbital apex meningioma in this patient.
links.lww.com/CONT/A124
B 2014 American Academy of Neurology.
Supplemental Digital Content 8-2
Alternate cover test. This video of the samepatient as in Supplemental Digital Content 8-1shows an exotropia (reflective of left medialrectus weakness) and a left hypotropia (reflectiveof left superior rectus and inferior obliqueweakness). Notice how the movements of theright eye are greater than the left eye during thetest, even though it is not the paretic eye; the lefteye is unable to move because of paresis. Thedeviation of the right eye (there is both anexotropia and hypertropia) is an example of asecondary deviation and results from the Heringlaw of equal innervation, which states that anequal force is provided to each eye.
links.lww.com/CONT/A125
B 2014 American Academy of Neurology.
Supplemental Digital Content 8-3
Enhanced ptosis (curtaining). When the ex-aminer lifts the right eyelid, the left eyelid fallsfurther, and when the left lid is lifted, theapparently normal right lid begins to droop,
KEY POINT
h Convergenceinsufficiency in childrenoften responds tooffice-based vergence/accommodative therapywith homereinforcement, whileadult patients withlesions of theconvergence centers oftenrequire prismatic therapy.
963Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

revealing an underlying ptosis in the right eye aswell. This enhanced ptosis or ‘‘curtaining’’ istypical for ocular myasthenia gravis since thedisease affects the neuromuscular junction ofboth eyes. The centrally mediated compensationfor the left-sided ptosis was distributed to themilder right eye, initially obscuring its milderptosis, as would be expected from the Heringlaw of equal innervation, which states that forceapplied to one eye is also applied to the other.
links.lww.com/CONT/A128
B 2014 American Academy of Neurology.
Supplemental Digital Content 8-4
Aberrant regeneration of the left oculomotornerve. In adduction, the lid lifts, reflectingaberrant regeneration of the adduction fibersof the oculomotor nerve to the levatorpalpebrae muscle fibers. The presence ofaberrant regeneration is consistent with chron-ic oculomotor palsy.
links.lww.com/CONT/A126
B 2014 American Academy of Neurology.
REFERENCES1. Pierrot-Deseilligny CH, Chain F, Gray F, et al.
Parinaud’s syndrome: electro-oculographicand anatomical analyses of six vascularcases with deductions about vertical gazeorganization in the premotor structures.Brain 1982;105(pt 4):667Y696.
2. Bhidayasiri R, Plant GT, LeighRJ. A hypotheticalscheme for the brainstem control of verticalgaze. Neurology 2000;54(10):1985Y1993.
3. Coffeen P, Guyton DL. Monocular diplopiaaccompanying ordinary refractive errors.Am J Ophthalmol 1988;105(5):451Y459.
4. Lepore FE, Yarian DL. Monocular diplopia ofretinal origin. J Clin Neuroophthalmol1986;6(3):181Y183.
5. Wilker SC, Rucker JC, Newman NJ, et al.Pain in ischaemic ocular motor cranial nervepalsies. Br J Ophthalmol 2009;93(12):1657Y1659
6. Brodsky MC, Donahue SP, Vaphiades M,Brandt T. Skew deviation revisited. SurvOphthalmol 2006;51(2):105Y128.
7. Dolman P. The Maddox Rod Screen Test.Trans Am Ophthalmol Soc 1919;17:235Y249.
8. Parks MM. Isolated cyclovertical musclepalsy. AMA Arch Ophthalmol 1958;60(6):1027Y1035.
9. Ohtsuki H, Hasebe S, Hanabusa K, et al.Intraoperative adjustable suture surgeryfor bilateral superior oblique palsy.Ophthalmology 1994;101(1):188Y193.
10. Joo KS, Koo H, Moon NJ. Measurement ofstrabismic angle using the distance Krimskytest. Korean J Ophthalmol 2013;27(4):276Y281.
11. Bixenman WW, von Noorden GK. Apparentfoveal displacement in normal subjects andin cyclotropia. Ophthalmology 1982;89(1):58Y62.
12. Spierer A. Measurement of cyclotorsion.Am J Ophthalmol 1996;122(6):911Y912.
13. Frueh BR, Musch DC, Grill R, et al. Orbitalcompliance in Graves’ eye disease.Ophthalmology 1985;92(5):657Y665.
14. Parelhoff ES, Chavis RM, Friendly DS.Wegener’s granulomatosis presenting asorbital pseudotumor in children. J PediatrOphthalmol Strabismus 1985;22(3):100Y104.
15. Lee AG, Tang RA, Feldon SE, et al. Orbitalpresentations of giant cell arteritis. GraefesArch Clin Exp Ophthalmol 2001;239(7):509Y513.
16. Berry-Brincat A, Rose GE. Idiopathic orbitalinflammation: a new dimension with thediscovery of immunoglobulin G4-relateddisease. Curr Opin Ophthalmol 2012;23(5):415Y419.
17. Yuen SJ, Rubin PA. Idiopathic orbitalinflammation: distribution, clinical features,and treatment outcome. Arch Ophthalmol2003;121(4):491Y499.
18. Wiersinga WM, Bartalena L. Epidemiologyand prevention of Graves’ ophthalmopathy.Thyroid 2002;12(10):855Y860.
19. Gaddipati RV1, Meyer DR. Eyelid retraction,lid lag, lagophthalmos, and von Graefe’ssign: quantifying the eyelid features ofGraves’ ophthalmopathy. Ophthalmology2008;115(6):1083Y1088.
20. Spierer A, Eisenstein Z. The role of increasedintraocular pressure on upgaze in theassessment of Graves ophthalmopathy.Ophthalmology 1991;98(10):1491Y1494.
21. Kuzma BB, Goodman JM. Slowly progressivebilateral enophthalmos from metastatic breastcarcinoma. Surg Neurol 1998;50(6):600Y602.
22. Shinder R, Al-Zubidi N, Esmaeli B. Survey oforbital tumors at a comprehensive cancercenter in the United States. Head Neck2010;33(5):610Y614.
23. Roshdy N, Shahin M, Kishk H, et al. MRI indiagnosis of orbital masses. Curr Eye Res2010;35(11):986Y991.
24. Saffra N, Rakhamimov A, Saint-Louis LA,Wolintz RJ. Acute diplopia as the presentingsign of silent sinus syndrome. Ophthal PlastReconstr Surg 2013;29(5):e130Ye131.
964 www.ContinuumJournal.com August 2014
Diagnostic Approach to Diplopia
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

25. Golnik KC, West CE, Kaye E, et al. Incidenceof ocular misalignment and diplopia afteruneventful cataract surgery. J CataractRefract Surg 2000;26(8):1205Y1209.
26. Nayak H, Kersey JP, Oystreck DT, et al.Diplopia following cataract surgery: a reviewof 150 patients. Eye 2008;22(8):1057Y1064.
27. Spencer RF, Porter JD. Biological organizationof the extraocular muscles. Prog Brain Res2006;151:43Y80.
28. Cogan DG. Myasthenia gravis: a review ofthe disease and a description of lid twitchas a characteristic sign. Arch Ophthalmol1965;74:217Y221.
29. Ragge NK, Hoyt WF. Midbrain myasthenia:fatigable ptosis, ‘lid twitch’ sign, andophthalmoparesis from dorsal midbrainglioma. Neurology 1992;42(4):917Y919.
30. Moorthy G, Behrens MM, Drachman DB,et al. Ocular pseudomyasthenia or ocularmyasthenia ‘plus’: a warning to clinicians.Neurology 1989;39(9):1150Y1154.
31. Van Stavern GP, Bhatt A, Haviland J,Black EH. A prospective study assessing theutility of Cogan’s lid twitch sign in patientswith isolated unilateral or bilateral ptosis.J Neurol Sci 2007;256(1Y2):84Y85.
32. Cogan DG, Yee RD, Gittinger J. Rapid eyemovements in myasthenia gravis. I.Clinical observations. Arch Ophthalmol1976;94(7):1083Y1085.
33. Serra A, Ruff RL, Leigh RJ. Neuromusculartransmission failure in myasthenia gravis:decrement of safety factor and susceptibilityof extraocular muscles. Ann N Y Acad Sci2012;1275:129Y135.
34. Osher RH, Griggs RC. Orbicularis fatigue:the ‘peek’ sign of myasthenia gravis.Arch Ophthalmol 1979;97(4):677Y679.
35. Osserman KE, Kaplan LI. Rapid diagnostictest for myasthenia gravis: increased musclestrength,without fasciculations, after intravenousadministration of edrophonium (tensilon)chloride. J AmMed Assoc 1952;150(4):265Y268.
36. Odel JG, Winterkorn JM, Behrens MM.The sleep test for myasthenia gravis.A safe alternative to Tensilon. J ClinNeuroophthalmol 1991;11(4):288Y292.
37. Sethi KD, Rivner MH, Swift TR. Ice pack testfor myasthenia gravis. Neurology 1987;37(8):1383Y1385.
38. Guptill JT, Sanders DB, Evoli A. Anti-MuSKantibody myasthenia gravis: clinical findingsand response to treatment in two largecohorts. Muscle Nerve 2011;44(1):36Y40.
39. Zouvelou V, Papathanasiou A, Koros C, et al.Pure ocular anti-musk myasthenia underno immunosuppressive treatment.Muscle Nerve 2013;48(3):464.
40. Kupersmith MJ, Moster M, Bhuiyan S, et al.Beneficial effects of corticosteroids onocular myasthenia gravis. Arch Neurol1996;53(8):802Y804.
41. Monsul NT, Patwa HS, Knorr AM, et al.The effect of prednisone on the progressionfrom ocular to generalized myastheniagravis. J Neurol Sci 2004;217(2):131Y133.
42. Liu Z, Feng H, Yeung S-CJ, et al. Extendedtranssternal thymectomy for the treatmentof ocular myasthenia gravis. Ann ThoracSurg 2011;92(6):1993Y1999.
43. Keane JR. Multiple cranial nerve palsies:analysis of 979 cases. Arch Neurol2005;62(11):1714Y1717.
44. Wall MD, Wray SH. The one-and-a-halfsyndromeVa unilateral disorder of thepontine tegmentum: a study of 20 casesand review of the literature. Neurology1983;33(8):971Y980.
45. Wong AM. Understanding skew deviationand a new clinical test to differentiate itfrom trochlear nerve palsy. J AAPOS.2010;14(1):61Y67.
46. Convergence Insufficiency Treatment TrialStudy Group. Randomized clinical trial oftreatments for symptomatic convergenceinsufficiency in children. Arch Ophthalmol2008;126(10):1336Y1349.
47. Godts D, Mathysen DG. Distance esotropia inthe elderly. Br J Ophthalmol 2013;97(11):1415Y1419.
48. Muthusamy B, Irsch K, Peggy Chang HY,Guyton DL. The sensitivity of theBielschowsky head tilt test in diagnosingacquired bilateral superior oblique paresis.Am JOphthalmol 2014. [Epub ahead of print].
49. Anagnostou E, Kouzi I, Kararizou E.Painful ophthalmoplegia: the role ofimaging and steroid response in theacute and subacute setting. J Neurol Sci2013;331(1Y2):145Y149.
965Continuum (Minneap Minn) 2014;20(4):942–965 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.