Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Diagnostic performance of CTesophagography in patientswith suspected esophageal rupture
Tatiana Suarez-Poveda & Carlos H. Morales-Uribe & Alvaro Sanabria &
Adriana Llano-Sánchez & Andrés Mauricio Valencia-Delgado &
Luis Fernando Rivera-Velázquez & John Fernando Bedoya-Ospina
Received: 31 January 2014 /Accepted: 1 April 2014# Am Soc Emergency Radiol 2014
Abstract Esophageal rupture is a surgical catastrophe. Thegold standard for diagnosing is iodine, water-soluble contrastmedium esophagography. CT esophagography has shownpromising results. This study aimed to assess the diagnosticperformance of CT esophagography in patients with a suspi-cion of esophageal rupture. This prospective study assessedthe performance of a diagnostic test and was approved bylocal IRB committee. Patients who presented with a clinicalsuspicion of esophageal rupture were included. CTesophagography findings were described by the emergencyradiologist. Clinical outcomes (presence or absence of esoph-ageal rupture) were reported by surgeons. The operative char-acteristics were calculated. A final predictive scale for rupturewas built. A total of 64 patients were recruited (age 26.5 years,90 % male, 82 % trauma). Sensitivity, specificity, and positiveand negative likelihood ratios (LRs) were 77.7 % (95 %confidence interval (CI) 45–100), 94.3 % (87.2–100), 14(9.81–19.9), and 0.24 (0.05–1.22), respectively. The finalmodel for predicting rupture included five variables: age (oddsratio (OR) 1.03; 95 % CI, 0.95–1.11; p=0.04), leakage ofcontrast media into the mediastinum or pleural space (OR10.0; 95 % CI, 0.64–156.9; p=0.10), extraluminal air or fluidcollections (OR 43.1; 95 % CI, 1.52–1217.3; p=0.027),
esophageal wall thickening (OR 10.1; 95 % CI, 0.50–202.8;p=0.12), and left pneumothorax or pleural effusion (OR 6.5;95%CI, 0.31–132.7; p=0.2). The overall agreement was 0.40(95 % CI, 0.09–0.72) for the predictive model. The modelsensitivity was 50.0 %, and the specificity was 98.4 %. CTesophagography shows a good diagnostic performance inpatients with a suspected esophageal rupture.
Keywords Esophageal perforation .Multidetector computedtomography . Diagnosis . Radiography . Esophagogram
Introduction
Esophageal rupture is a surgical catastrophe, especially whendiagnosed late. After 24 h, the mortality rate for an undiag-nosed rupture is 10–40% [1–3] due to mediastinitis and septicshock. Patients usually present with vomiting, dull chest pain,and subcutaneous emphysema, but these signs occur late inthe disease, and when present, they are not easily recognizeddue to the low prevalence of the condition [4].
The gold standard for diagnosing in patients with a suspi-cion of esophageal rupture is iodine, water-soluble contrastmedium esophagography, which has a specificity close to100 % but only a moderate sensitivity of approximately75 % [5]. In addition to diagnosis, this method helps todetermine the location of the perforation but has some disad-vantages, such as being operator-dependent and unusable incritically ill patients [6, 7].
Recently, the introduction of a new technique, called CTesophagography, has shown promising results because themodality provides the best image resolution and significantanatomic detail. However, there are only a few studies with asmall number of patients, which do not offer enough evidenceto support its wide use in clinical settings [4, 7, 8]. Because CTesophagography can be performed in critically ill patients or
T. Suarez-Poveda (*) :A. Llano-Sánchez :A. M. Valencia-Delgado : L. F. Rivera-Velázquez :J. F. Bedoya-OspinaDepartment of Radiology, Universidad de Antioquia—Hospital SanVicente Fundacion, Calle 64 No. 51 D-154, Medellin, Colombiae-mail: [email protected]
C. H. Morales-UribeDepartment of Surgery, Universidad de Antioquia—Hospital SanVicente Fundacion, Medellin, Colombia
A. SanabriaDepartment of Surgery, Universidad de Antioquia—Hospital PabloTobon Uribe, Medellin, Colombia
Emerg RadiolDOI 10.1007/s10140-014-1222-4

simultaneously with other studies in trauma patients, CT canbe a good tool for the diagnosis of esophageal rupture. Thisstudy aimed to assess the diagnostic performance of CTesophagography compared to surgical findings or clinicalfollow-up in patients with a suspicion of esophageal ruptureand to develop a set of imaging findings to determine the riskof rupture. We also assessed the agreement in the interpreta-tion of imaging findings to determine the possibility for clin-ical use in nonspecialized centers.
Material and methods
This cross-sectional prospective study assessed the perfor-mance of a diagnostic test. The study was approved by theEthics in Research Committee of the Hospital San VicenteFundacion and Universidad de Antioquia. All adult patientswho presented to the emergency department at the HospitalSan Vicente Fundacion between August 1, 2009 and October1, 2011 with a clinical suspicion of esophageal rupture fromany cause (trauma, after an endoscopic procedure, cancer,foreign bodies, and injuries from caustic soda) were consid-ered for inclusion in this study. Patients who declined wereexcluded from the study.
Data collection from the medical records of the selectedpatients was performed using a specially designed form. The-se data included demographic information, probable cause ofrupture, the CT esophagography findings described by theemergency radiologist, and clinical outcomes.
CT esophagography
For the CT esophagography, we used a GE LightSpeed, 64-slice multidetector CT. The scan included the neck and thoraxfrom the mandibular angle to the diaphragm. A single-baseline phase was performed prior to contrast injection witha 5-mm section thickness, a pitch of 0.984:1, a gantry rotationtime of 0.5 s, and a reconstruction interval of 1.25 mm.Subsequently, all of the patients received 50 ml of water-soluble iodine contrast (iobitridol; Omnipaque 300,Laboratorios Temis Lostaló) in water at a 10 % concentrationthrough a nasogastric tube located at the cricopharyngealsphincter and infused manually. Then, a new CT was per-formed using the same parameters. For the patients with aclinical indication for angiography or chest CT, 50 ml ofintravenous contrast was infused at 3 ml/s with a delay of40 s, and this phase was considered the baseline beforeinjecting the oral contrast.
Parameters to assess CT esophagography
The emergency room radiologist was instructed to complete apreviously designed formwith the imaging findings described
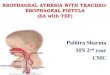
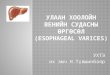
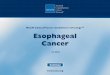
in the literature. The findings were as follows: esophageal walldiscontinuity, esophageal wall thickening defined as an asym-metric thickening of the esophageal wall (a difference higherthan 5 mm between injured and noninjured wall), leakage ofcontrast media into the mediastinum or pleural space (Fig. 1),extra luminal air or fluid collections (Fig. 2), left pneumotho-rax or pleural effusion (Fig. 3), and pneumomediastimum or amarked esophageal fistula. Finally, the radiologist had tomakean overall assessment as positive for rupture, negative forrupture, or undetermined.
Outcomes
The outcomes were the presence or absence of esophagealrupture. In patients who underwent surgery, the result reportedby the surgeon was considered to be the gold standard. Forpatients who did not undergo surgery, a long-term clinicalassessment longer than 8 days was considered to be the goldstandard. Perforation identified by surgical inspection or in theclinical follow-up based on sepsis or mediastinitis from apleural empyema was considered to be a positive sign. Theother cases were considered to be negative.
Data analysis
The information from the forms was entered into a database(Epidat 3.0, WHO, USA). For the statistical analysis, com-mercially available software (Stata 9.0, Stata Corporation,TX) was used. Descriptive statistics was used to show thedistribution of the variables in the population. The overalloperative characteristics of CT esophagography (sensitivity,specificity, positive and negative predictive values, and posi-tive and negative likelihood ratios) and each imaging findingwere calculated. A sensitivity analysis was used for undeter-mined cases, to assess the change in performance characteris-tics when they were considered to be positive or negative.
Fig. 1 A neck CT scan of a patient with gunshot injury. There is anirregular right esophageal wall with contrast media leakage (white arrow)and air in the adjacent soft tissue
Emerg Radiol

Logistic regression was used to identify independent riskfactors for esophageal rupture (either present or absent). Weincluded age and all imaging findings in the full model.
Before performing the logistic regression, a colinearityanalysis of included variables was performed, selecting those
to be used. A logistic regression was then performed to provethe independent contribution of each variable to the finalmodel. For all of the variables, the odds ratio (OR) with95 % confidence interval (CI) was reported. A final predictivescale for rupture was built using each imaging variable.
The operative characteristics and receiver operating char-acteristic (ROC) area curve for the model and the scales werealso reported. The validity of this scale was assessed using arandom sample approach by testing the scale developed withthe complete sample population in ten different random pa-tients and 50 % of the observations in the main database. Forall of the statistical tests, p<0.05 was considered to be statis-tically significant.
Results
Sixty-four patients were initially recruited. One patient waslost to follow-up, leaving 63 patients for the final analysis. Themean age was 26.5 years (range 15–76 years). A total of 57 ofthe patients were men (90.5 %).
The primary causes of esophageal rupture suspicion areshown in Fig. 4. Nine patients had a surgical or clinicalconfirmation of rupture (14.3 %), eight due to gunshotwounds, and one due to foreign body ingestion. The radiolo-gist globally classified the CT esophagography as positive inten patients, indeterminate in one patient, and negative in theothers (Table 1). There were no complications with oral orintravenous contrast infusion.
Classifying the indeterminate results as negative, the sen-sitivity, specificity, positive predictive value (PPV), negativepredictive value (NPV), and positive and negative likelihoodratios (LRs) were 77.7 % (95 % CI, 45–100), 94.3 % (87.2–100), 70.0 % (34.8–93.3), 96.2 % (87.0–99.5), 14 (9.81–19.9), and 0.24 (0.05–1.22), respectively. Classifying the in-determinate results as positive, the results were 77.8 % (40.0–
Fig. 2 A chest CT scan after a gunshot wound. There is apneumomediastinum (white arrow) and irregularity of the anterior esoph-ageal wall with contrast media leakage (black arrow) after a gunshotinjury. A small left hemothorax and a fracture of the right clavicle, withbullet fragments is also seen
Fig. 3 A chest CTscan after a gunshot injury. There is periesophageal air(white arrow) with left pneumothorax (black arrow). There is no contrastmedia leakage Fig. 4 Causes of esophageal rupture suspicion
Emerg Radiol

97.2), 92.6 % (82.1–97.9), 63.6 % (30.8–89.1), 96.2 % (86.8–99.5), 10.5 (7.35–15.0), and 0.24 (0.05–1.12), respectively.
The sensitivity, specificity, positive and negative predictivevalues, and positive and negative LRs for each imaging find-ing are shown in Table 2. The agreement measured using thekappa coefficient was 0.30 for wall thickening, 0.56 for air/liquid collections, 0.57 for leakage, and 0.64 forpneumothorax/pleural effusion. The overall agreement was0.40 (95 % CI, 0.09–0.72) for the predictive model. In thelogistic regression model, the presence of an esophageal fis-tula was predicted perfectly. Therefore, this variable wasexcluded from the model, and its presence was considered toconfirm a rupture. Variable discontinuity and leakage into themediastinum or pleural space showed a high colinearity;therefore, we excluded the former. The final model forpredicting rupture included the following five variables: age(OR 1.03; 95 % CI, 0.95–1.11; p=0.04), leakage of contrastmedia into the mediastinum or pleural space (OR 10.0; 95 %CI, 0.64–156.9; p=0.10), extraluminal air or fluid collections(OR 43.1; 95 % CI, 1.52–1217.3; p=0.027), esophageal wallthickening (OR 10.1; 95 % CI, 0.50–202.8; p=0.12), and leftpneumothorax or pleural effusion (OR 6.5; 95 % CI, 0.31–132.7; p=0.2). The Hosmer-Lemeshow goodness-of-fit prob-ability was 0.79. The model sensitivity was 50.0 %, and thespecificity was 98.4 % with a rate of 91.5 % for the correctlyclassified data. The area under ROC curve for this model was0.95. With these variables, two predictive indexes were built:one using the OR coefficients obtained from the logisticregression and a second classifying the finding as present orabsent (Table 3). Accepting the parsimony principle of statis-tics would suggest choosing an instrument with a similar
performance but a lower number of variables and consideringthat instrument to be the first model to have scoring gapsrelated to the weight provided to each variable. Thus, weselected the second index as the best strategy to quantify therisk of rupture. After testing various levels to set a cutoff point,we decided to divide the scale into an ordinal scale by grade ofrisk: low risk, with a value of 0 and probability of rupture of0 %; intermediate risk, with a value of 1 and a probability ofrupture of 13 %; and high risk, with a value greater than 1 anda probability of rupture of 50 % (range 50 to 100 %). Arandom sample approach to validate the index showed theROC area curve from 0.80 (95 % CI, 0.64–0.95) in the worstcase to 0.97 (95 % CI, 0.91–1.0) in the best case.
Discussion
Esophageal rupture is fatal if not discovered early [1–3].Suspicion of esophageal rupture has been based on theMackler triad [9], which includes vomiting followed by chestor retrosternal pain and subcutaneous emphysema. However,this triad has a low frequency, and despite its high specificity,its sensitivity is low. In fact, many patients have nonspecificsymptoms, such as dyspnea, hypotension, sepsis, shock, co-ma, upper gastrointestinal bleeding, and undetermined chestor upper abdominal symptoms [4]. Therefore, the diagnosis ofrupture is based on a high suspicion and radiologic confirma-tion. Currently, esophagography with water-soluble contrastmedium has been shown to have the best diagnostic perfor-mance [5]. However, the diagnostic performance depends onwhether the patient is awake and able to swallow and thefeasibility of transporting the patient to specific radiologysettings, and only provides information about the digestivesystem.
The wide use of computed tomography has changed theevaluation of patients because CT allows a quick assessmentof many body areas in a few seconds and allows providers torule out of other causes of chest pain, such as aortic dissection.In addition to a common CT, the addition of oral contrast
Table 1 Results for esophageal rupture by CT esophagography in com-parison with true rupture determined by surgical findings/follow-up
Rupture positive Rupture negative
CT esophagography positive 7 3
CT esophagography negative 2 50
CT esophagography undetermined 0 1
Table 2 Performance of individ-ual imaging findings assessed forpatients with suspicion ofesophageal rupture
The operative characteristics ofeach finding are shown incomparison with presence/absence of rupture
PPV positive predictive value,NPV negative predictive value,LR likelihood ratio, NCnot calculable
Finding Sensitivity(%)
Specificity(%)
PPV (%) NPV (%) LR (+) LR (−)
Esophageal wall discontinuity 55.6 96.3 71.4 92.9 15.0 0.46
Esophageal wall thickening 33.3 94.4 50.0 89.5 5.9 0.71
Leakage of contrast media into themediastinum or pleural space
55.6 96.3 71.4 92.9 15.0 0.46
Extraluminal air or fluid collections 66.7 94.4 66.7 94.4 11.9 0.35
Left pneumothorax or pleuraleffusion
55.6 66.7 21.7 90.0 1.7 0.67
Pneumomediastinum 44.4 75.9 23.5 89.1 1.8 0.73
Marked esophageal fistula 11.1 100.0 100.0 87.1 NC 0.89
Emerg Radiol

media to the CT by classical esophagography or a nasogastrictube, CT esophagography, could offer information about thepatency and physical integrity of the upper digestive system[4, 7, 8, 10]. Moreover, the addition of sodium bicarbonate ortartaric acid to the infused fluid and the creation of doublecontrast using air in the nasogastric tube could increase thediagnostic performance of the technique [11]. Unfortunately,there is little evidence about its performance for this uncom-mon condition. Backer et al. [4] reported three patients inwhom esophageal rupture was initially suggested by indirectimaging findings, such as air bubbles in the mediastinum; anabscess adjacent to the esophagus, in the mediastinum or inthe pleural cavity; a left pleural effusion; or a dilated esopha-gus with an adjacent air-water level. Fadoo et al. [7] assessed11 patients with suspected rupture and confirmed the diagno-sis in 5 patients who presented with an air-water level adjacentto the esophagus, free fluid in the mediastinum, esophagealwall thickening, pleural effusion, or extraluminal air on theCT. However, the low number of patients makes extrapolatingthe results difficult. White et al. [8] assessed 12 patients withesophageal rupture and found wall thickening in 9 patientsand mediastinum leakage and extraluminal air in 11 patientswith a good correlation between rupture location and the air-fluid findings. Moreover, for four patients (33 %), the diag-nosis of perforation was suspected based on CT findings andbefore any clinical suspicion. de Lutio di Castelguidone et al.[3] assessed 16 patients with a suspected esophageal ruptureand found imaging findings, including air or liquid adjacent tothe esophagus in 5 patients, wall thickening in 4 patients, thelack of wall continuity in 2 patients, and contrast leakage in 1patient. All of these studies have suggested using indirectimaging, such as extraluminal air or fluid, wall thickening,
or pleural and mediastinal fluid, as signs of esophagealrupture.
Our study reports a high number of patients with as u s p e c t e d e s oph ag e a l r u p t u r e , i n whom CTesophagography was used. The results show good sensi-tivity and specificity when the overall classification wasused, which is comparable to those reported for classicalesophagography. Currently, esophagography shows aspecificity of approximately 100 % but a sensitivity of75 %, supporting the suspicion only during the leakage ofcontrast media but without assessing for other indirectsigns that have been shown to have a good diagnosticperformance. As a dynamic study, esophagography re-quires the active participation of the patient and specificoperator training, which imposes difficulties for somepatients and settings [5]. However, the judgment for eachimaging signal remained obscure, which induced us toassess them individually. As expected, most of the imag-ing findings showed a poor performance when consideredindependently, with the most sensitive finding beingextraluminal air or a fluid collection at 66 % and the mostspecific being wall discontinuity and the leakage of con-trast into the mediastinum.
The prediction of rupture based on CT showed thatthe most statistically significant independent variable wasextraluminal air or a fluid collection with an OR ofapproximately 43, followed by esophageal wall thicken-ing and leakage of contrast into the mediastinum. How-ever, the predictive ability of the complete model onlyreached a 50 % sensitivity. When the findings wereassembled into a simple score, it was possible to notonly maintain the diagnostic performance but also toclassify patients by risk level to help the clinician plana surgical procedure or further diagnostic evaluation. Webelieve that this approach is more useful than makingclinical decisions based on individual findings.
Our agreement for the evaluation of individual signals wasmoderate, and this level of agreement can make interpretingthe studies difficult. However, we believe that a better knowl-edge of the signal and more practice with the technique couldhelp to overcome this weakness.
Some disadvantages should be considered, including theneed for training to detect subtle imaging signals, the necessityto transport patients to the CTscanner, and the lack of utility inpostoperative cases and penetrating trauma, where the air andfluid may not represent esophageal rupture or in the presenceof metallic artifacts that make identifying the described imag-ing signals more difficult. We did not have complicationsrelated with the oral infusion, and this can be related withthe exact location of the tip of the nasogastric tube at thecricopharyngeal sphincter.
In conclusion, we believe that CTesophagography shows agood diagnostic performance in patients with a suspected
Table 3 Comparison of indexes developed to predict esophageal rupture
Index 1(leakage*10) + (air/liquid*43) +(wall thickness*10) + (pleuraleffusion*6)
Index 2(leakage*1) + (air/liquid*1) +(wall thickness*1) + (pleuraleffusion*1)
Index score Rupture (%) Index score Rupture (%)
0 0 0 Low risk 0
6 5.9 1 Intermediate risk 13
10 33.3 2 High risk 50
16 33.3 3 100
43 33.3 4 100
53 66.759 100
69 100
Area under ROC 0.94 (0.87–1.0) Area under ROC 0.91 (0.82–0.99)
In the left column, the crude index with coefficients is directly derivedfrom logistic regression. In the right column, the index is adjusted foreasier clinical use
ROC receiver operating characteristic
Emerg Radiol

esophageal rupture and can be used specifically for criticallyill patients with traumatic injuries in many areas, those whoneed a simultaneous evaluation of the thoracic cavity, andthose in whom classical esophagography is difficult toperform.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Vogel SB, Rout WR, Martin TD et al (2005) Esophageal perforationin adults: aggressive, conservative treatment lowers morbidity andmortality. Ann Surg 241:1016–1021
2. Kiernan PD, Sheridan MJ, Elster E et al (2003) Thoracic esophagealperforations. South Med J 96:158–163
3. de Lutio di Castelguidone E, Merola S, Pinto A et al (2006)Esophageal injuries: spectrum of multidetector row CT findings.Eur J Radiol 59:344–348
4. Backer CL, LoCicero J III, Hartz RS et al (1990) Computed tomog-raphy in patients with esophageal perforation. Chest 98:1078–1080
5. Flynn AE, Verrier ED, Way LWet al (1989) Esophageal perforation.Arch Surg 124:1211–1214
6. Rubesin SE, Levine MS (2003) Radiologic diagnosis of gastrointes-tinal perforation. Radiol Clin N Am 41:1095–1115, v
7. Fadoo F, Ruiz DE, Dawn SK et al (2004) Helical CTesophagographyfor the evaluation of suspected esophageal perforation or rupture.AJR Am J Roentgenol 182:1177–1179
8. White CS, Templeton PA, Attar S (1993) Esophageal perforation: CTfindings. AJR Am J Roentgenol 160:767–770
9. MACKLER SA (1952) Spontaneous rupture of the esophagus; anexperimental and clinical study. Surg Gynecol Obstet 95:345–356
10. Kim SH, Kim YJ, Lee JM et al (2007) Esophageal varices in patientswith cirrhosis: multidetector CT esophagography—comparison withendoscopy. Radiology 242:759–768
11. Brick SH, Caroline DF, Lev-Toaff AS et al (1988) Esophagealdisruption: evaluation with iohexol esophagography. Radiology169:141–1-43
Emerg Radiol