-
Diagnostic Role ofHead-Bending and Lying-DownTestsin Lateral
Canal Benign Paroxysmal Positional Vertigo
Sertac Yetiser and Dilay Ince
Department of Otorhinolaryngology, Anadolu Medical Center,
Kocaeli, Turkey
Objectives: To compare the diagnostic value of the
head-bendingtest (HBT), lying-down positioning test (LDPT) and
patients re-port to identify the affected canal in
video-nystagmographically(VNG) confirmed patients with lateral
canal benign paroxysmalpositional vertigo (LC-BPPV).Study Design:
Case series with chart review.Setting: Head-bending, lying-down
positioning and the head-rollmaneuver (HRM) under VNG guidance. The
data were collectedin a referral community hospital.Patients:
Seventy-eight patients (32 apogeotropic and 46 geotropicnystagmus)
with LC-BPPVwho had been recruited between 2009and 2013 were
enrolled in the study.Main Outcome Measures: Patients were tested
with the HRMand then were asked about subjectively worse side.
Later, they weresubjected to HBT when sitting and the LDPT. The
results werecompared and studied with the 1-way ANOVA and
chi-squaretests. Statistical significance was set at p G
0.05.Results: Affected side was identified by HRM in 75% of
pa-tients with apogeotropic nystagmus and 95.6% of patients
with
geotropic nystagmus. Approximately 65.6% of patients with
apo-geotropic and 52% of patients with geotropic nystagmus had
nys-tagmus during LDPT. However, its comparability with HRM waslow.
However, treatment plan based on LDPT results alone pro-vided
relief of symptoms in additional 12.5% of patients withapogeotropic
and in 2.2% of patients with geotropic nystagmus.Approximately 63%
of patients with apogeotropic and 56% ofpatients with geotropic
nystagmus were able to tell the worse side.Nystagmus comparable
with HRM during HBT was low and notdiagnostic.Conclusion: HRM has
the greatest diagnostic value of position-ing tests in LC-BPPV in
this study. LDPT provides some contri-bution in the diagnosis of
LC-BPPV but much less than HRM.Patients subjective feeling of
vertigo was also a useful test. How-ever, HBTwas not as sensitive
as other measures in uncertain cases.Key Words: Positional
vertigoVVertigoVParoxysmal.
Otol Neurotol 00:00Y00, 2015.
Patients with benign paroxysmal positional vertigo ofthe lateral
canal (LC-BPPV) are diagnosed as having geo-tropic or apogeotropic
bidirectional nystagmus during thehead-roll maneuver (HRM) in the
supine position (1Y3).The type of nystagmus and the severity of
vertigo sensa-tion during this test will help diagnose the involved
sidewhen the head is turned (1). An analysis of slow phasevelocity
of the recorded nystagmus will also guide to de-termine the site
with more intense nystagmus. A severe andbrief sense of evoked
vertigo is generally worse on the
affected side for geotropic type nystagmus and worse onthe
healthy side for apogeotropic type nystagmus. Identi-fication of
the affected side is very important in selection ofthe proper
direction to apply the barbeque or liberatorymaneuvers (4Y7).
However, this task is not always easy toaccomplish because the
evoked nystagmus may be equallysevere on both sides or may be too
weak to diagnose.HRM in the supine position is very helpful in
diagnosing
the affected side in LC-BPPV.However, it has been reportedthat
almost 10% of patients with unilateral LC-BPPV mayhave symmetrical
nystagmus which makes it difficult todetermine the side of the
lesion (8). The examiner then needsto use additional methods for
selection of the affected side,such as the head-bending test (HBT)
when sitting, the lying-down positioning test (LDPT), or the
patients subjectivefeeling of vertigo (9). Patients with LC-BPPV
frequentlyexperience a sudden sense of spinningwhen they bend
theirhead forward or backward intentionally or unintentionallysuch
as when falling asleep while reading a newspaperwhen sitting, lying
down from a sitting position, or gettingout of bed. Those patients
may have a brief nystagmus
Address correspondence and reprint requests to Sertac Yetiser,
M.D.,Department of Otorhinolaryngology and Head Neck Surgery,
AnadoluMedical Center, Cumhuriyet mah, 2255 sok, No:3, Gebze 41400,
Kocaeli,Turkey; E-mail: [email protected],
[email protected] study, similar or the same
form, has not been submitted to any
other journal for publication or presented in any medical
meeting before.The data were collected and drafted by D. Ince. Data
analysis, drafting,
and final approval were completed by S. Yetiser.None of the
authors have any financial, consultant, and institutional
interest for the work or any grant or financial support provided
by com-panies toward the completion of the work. Authors have no
conflict ofinterest and no disclosures.
Otology & Neurotology00:00Y00 2015, Otology &
Neurotology, Inc.
1
Copyright 2015 Otology & Neurotology, Inc. Unauthorized
reproduction of this article is prohibited.
-
associated with these conditions. From this observation,Nuti and
Asprella proposed a test to confirm the diagnosisof the affected
canal in LC-BPPV (10,11). They proposed ahorizontal nystagmus
beating to the healthy side in case ofgeotropic nystagmus
(posterior arm canalolithiasis; otolithslocated away from cupula)
and to the affected side in caseof apogeotropic nystagmus (anterior
arm canalolithiasis;otoliths located close to the cupula or
cupulolithiasis; oto-liths attached to the cupula) when patients
are lying downwith their head in a straight head hanging
position.When the head is erect in a sitting patient, an angle
of
30 degrees exists between the horizontal plane and the lat-eral
canal inwhich therewill be nogravitational force and nomovement of
otoliths inside the canal (10,11). Bending thehead 60 degrees
forward brings the lateral canal to 30 de-grees with reference to
the horizontal plane, and this headmotion causes ampullopetal
floating of the otoliths resultingin a nystagmus toward the
affected ear in geotropic nys-tagmus, or cupular deflection in the
opposite direction, to-ward the unaffected ear in apogeotropic
nystagmus (10,11).Changing the head position to 30 degrees backward
willalso change the angle of the lateral canal to an approxi-mately
vertical position, and the otoliths will move chang-ing their
direction and velocity (10,11). On the other hand,bringing the
patient quickly from the seated position to thesupine position will
push the otoliths downward because ofboth gravity and deceleration
forcing them toward theutricle if they are free in the canal or
toward the ampulla ifthey are attached to the cupula. Therefore,
this move willevoke a nystagmus beating toward the healthy side in
the
case of geotropic nystagmus or toward the affected side inthe
case of apogeotropic nystagmus.The aim of this study is to compare
the diagnostic value
of HBT when sitting, LDPT, and the patients report ofseverity of
sense of vertigo during HRM in the supine po-sition in patients
with LC-BPPV.
MATERIALS AND METHODS
Seventy-eight patients with LC-BPPV who had been
recruitedbetween 2009 and 2013 were enrolled in the study. A verbal
and asigned informed consent were obtained from each patient.
Theprocedures were in accordance with the ethical standards of
thedeclaration of Helsinki and of the institutional review board.
Therewere 36 men and 42 women with age ranging from 14 to 84
years(42.28 T 11.29). Duration of symptoms was ranging between2
days and 12 weeks. Main inclusion criteria were normal oto-scopic
examination, normal hearing threshold, and no problemsother than
BPPV. Those with hearing loss, tinnitus, abnormal eardrum, or other
vestibular or neurologic problems and those whoused medication
recently which could affect the vestibular systemwere excluded.
Data were collected in a referral community hos-pital. All patients
were first tested with VNG (Micromedical Tech-nologies, Inc,USA)
for spontaneous nystagmus in the seated primarygaze position before
starting the test battery and those with spon-taneous nystagmus
were excluded from the study. Tests were per-formed in the order of
spontaneous nystagmus, HRM, HBT, andLDPT. The type, duration, and
direction of nystagmus were re-corded with an infrared wireless
video camera. VNG is done bygoggles with closed camera system (open
eyes, closed vision) andno fixation effect was allowed during the
test. Between each test,the patient rested for 15 to 20 minutes to
prevent fatigue.
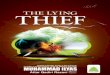
FIG. 1. View of head-roll maneuver while the patient is lying
down. Geotropic or apogeotropic nystagmus (bidirectional,
horizontal) is seenin patients with LC-BPPV (APO, apogeotropic;
GEO, geotropic). Dark arrow indicates the direction of the
nystagmus.
2 S. YETISER AND D. INCE
Otology & Neurotology, Vol. 00, No. 00, 2015
Copyright 2015 Otology & Neurotology, Inc. Unauthorized
reproduction of this article is prohibited.
-
Presence of brief latency, short duration, and adaptation
oftransient nystagmus were always noted to confirm peripheraltype
positional nystagmus. Geotropic or apogeotropic nystag-mus
(bi-directional, horizontal) during HRM while the patientwas lying
down was initially documented (Fig. 1). The patientshead was first
turned to the right side for 3 minutes and then tothe center
position. Later, the head was turned to the left side tosee evoked
nystagmus. The affected side was determined accordingto the
severity of nystagmus as seen on the VNG recording.Nystagmus of
greater velocity was on the affected side in patientswith geotropic
nystagmus and on the healthy side in patients withapogeotropic
nystagmus. Patients were defined as undeterminedlaterality for
geotropic or apogeotropic form if the analysis of therecorded
images shows similar slow phase eye velocity on bothsides. Patients
were also asked about how they felt and which sidewas worse for the
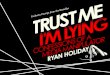
sense of vertigo during HRM.Later, the patients were subjected
toHBT at sitting in 3 different
positions (Fig. 2). First, the head was quickly bent forward
by60 degrees (Position A) while the patient was in the sitting
po-sition. Then, the patients head was put in the straight
position(position B). This was actually a movement action from
positionA to position B (different from primary gaze position to
seek forspontaneous nystagmus). Finally, the head was bent backward
by30 degrees (position C). This was again a movement action
fromposition B to position C. The test was performed with VNG,
andeach position was held for 5 minutes to obtain sufficient time
torecord the evoked nystagmus. The head was grasped and fixed bythe
technician at each position. Finally, the patient was askedto lie
down from the sitting position (LDPT) and again evokednystagmus was
recorded by VNG (Fig. 3). Horizontal positionalnystagmus seen
during LDPT was toward the healthy side inpatients with geotropic
nystagmus and toward the affected side in
patients with apogeotropic nystagmus. Positional nystagmus
duringHBT in patients with geotropic nystagmus was toward the
affectedside in position A and toward the healthy side in positions
B and C.However, in patients with apogeotropic nystagmus, it was
towardthe healthy side in position A and toward the affected side
inpositions B and C.Patients having nystagmus with asymmetric
intensity on both
sides during HRM in the supine position under VNG (the
affectedside was clear for geotropic or apogeotropic type
nystagmus) andthose having nystagmus with almost equal intensity
were deter-mined. Patients having no nystagmus during LDPT and/or
HBTand those having nystagmus during the tests confirming the
af-fected side as detected by HRMwere determined. Finally,
patientswho were unable to tell the affected side from the severity
of senseof vertigo during the HRM (equal intensity or very mild
senseof spinning), and those who reported asymmetric severity of
senseof vertigo during the HRM were determined. Mean values
werecompared for each group. Patients with apogeotropic
nystagmuswere treated with Barbeque, Semonts, or Gufoni maneuvers,
andpatients with geotropic nystagmus were treated with Barbeque
orGufoni maneuvers. All patients were controlled within 5 to 7
daysafter therapeutic maneuvers. The 1-way ANOVA and
chi-squaregoodness of fit tests were used for comparative analysis
of thegroups. Statistical significance was set at p G 0.05.
RESULTS
Thirty-two patients had apogeotropic, and 46 patientshad
geotropic type nystagmus, which were noted in HRM.Identification of
the affected side was possible in 24 of the32 patients with
apogeotropic type nystagmus (75%) by
FIG. 2. View of head bending test at sitting in 3 positions in a
patient assuming with healthy left side. A, bending forward; B,
straight; C,bending backward. APO indicates apogeotropic; GEO,
geotropic. Dark arrow indicates the direction of the nystagmus.
3HEAD-BENDING AND LYING-DOWN TESTS
Otology & Neurotology, Vol. 00, No. 00, 2015
Copyright 2015 Otology & Neurotology, Inc. Unauthorized
reproduction of this article is prohibited.
-
HRM (11 in right ear and 13 in left ear). Eighteen patientswith
apogeotropic nystagmus were able to tell the worse sidein terms of
sense of severity during HRM (18/32; 56%).Eight patients had
nystagmus during HBT position A (8/32;25%) and 7 patients had
nystagmus during HBT position C(7/32; 21.7%). None of the patients
had any nystagmusduring HBT position B. Twenty-one patients had
nystag-mus during LDPT (21/32; 65.6%), but it was comparablewith
the side of the affected canal detected by HRM in 15patients
(15/32; 46.7%), and it was vertical or not compa-rable with HRM in
6 patients (Fig. 4).Identification of the affected side was
possible in 44 of
the 46 patients with geotropic type nystagmus (95.6%) byHRM (21
in right ear and 22 in left ear). Twenty-ninepatients were able to
tell the worse side in terms of senseof severity during HRM (29/46;
63%). Thirteen patientshad nystagmus during HBT position A (13/46;
28.3%), and15 patients had nystagmus during HBT position C
(15/46;32.6%). None of the patients had nystagmus during
HBTposition- B. Twenty four patients had nystagmus duringLDPT
(24/46; 52%), but it was comparable with the side ofthe affected
canal detected by HRM in 10 patients (10/46;21.7%). It was slightly
beating up (4 patients) or down(2 patients) or horizontal but not
comparable with HRM(8 patients) (Fig. 5).Twenty-three patients with
apogeotropic nystagmus
and laterality sign on HRM responded the treatment. The
treatment plan was based on LDPT findings in 6 of 7patients with
equal nystagmus on both sides during HRMand was effective in 4
after several attempts. Therefore,the number of patients with cure
increased from 71.8%(23/32) to 84.3% (27/32), when HRM and LDPT
arecombined as diagnostic tools, if improvement of symp-toms after
therapeutic maneuvers are assumed to enhancethe determination of
the laterality. Forty-three patients withgeotropic nystagmus and
laterality sign on HRM were res-ponded the treatment. Treatment
plan was based on theLDPT findings in 2 patients and was effective
in one ofthem. Therefore, the number of patients with cure
increasedfrom 93.4% (43/46) to 95.6% (44/46), when combinationof
the HRM and LDPT are used as the diagnostic tests.Comparative
analysis of the test results for patients with
geotropic and apogeotropic type nystagmus is presented inTable
1. Diagnostic value of both the LDPT and patientsreports was better
in patients with apogeotropic nystagmusand also in those with
geotropic nystagmus, compared withthe value of HBT. No
statistically significant differencewas found when comparing the
diagnostic value of HBT inthe 3 positions, LDPT and patients
reports between pa-tients with geotropic and those with
apogeotropic nystag-mus (p 9 0.05). The number of patients who were
curedafter treatment and inwhomdiagnostic evaluationwas basedon
LDPT alone was statistically significantly better in pa-tients with
apogeotropic nystagmus compared with patients
FIG. 3. View of lying down positioning test in a patient
assuming with healthy left side (APO, apogeotropic; GEO,
geotropic). Dark arrowindicates the direction of the nystagmus.
4 S. YETISER AND D. INCE
Otology & Neurotology, Vol. 00, No. 00, 2015
Copyright 2015 Otology & Neurotology, Inc. Unauthorized
reproduction of this article is prohibited.
-
having geotropic nystagmus (p = 0.018). However, whenall
diagnostic tests were used together, the overall cure ratein
patients with geotropic type nystagmus was
statisticallysignificantly better than patients with apogeotropic
typenystagmus (p = 0.044).
DISCUSSION
Studies related with the diagnostic issues of LC-BPPVare
generally based on HRM only and comparative analysiswith other
methods is lacking. Few studies have been pub-lished analyzing the
diagnostic value of LDPT to determinethe affected canal in patients
with LC-BPPV. Han et al. haveanalyzed the presence of lying-down
nystagmus (toward
the healthy ear in geotropic and toward the affected ear
inapogeotropic type) in 152 patients with LC-BPPV and haveobserved
this nystagmus in 38.2% of patients with docu-mented LC-BPPV (36.4%
of the geotropic and 41.5% ofthe apogeotropic type) (9). We have
found higher incidenceof evoked nystagmus during LDPT in our series
(65.6% forapogeotropic nystagmus and 52% for geotropic
nystagmus),although the number of patients is smaller. However,
itscontribution to the diagnosis was less than HRM.It seems that it
is not always possible to evoke the nys-
tagmus with LDPT. This could be related with the densityand the
amount of the otoliths or their distance to the cupulainside the
membranous labyrinth to evoke nystagmus orwith the examiner who is
unable to do the test adequately
FIG. 4. The overall test results of patients with apogeotropic
type nystagmus.
FIG. 5. The overall test results of patients with geotropic type
nystagmus.
5HEAD-BENDING AND LYING-DOWN TESTS
Otology & Neurotology, Vol. 00, No. 00, 2015
Copyright 2015 Otology & Neurotology, Inc. Unauthorized
reproduction of this article is prohibited.
-
because the lying down movement should be so quick. Wehave also
some concern about the order of the tests.We havedone first HBT,
then later LDPT. This may cause dispersalof the debris in some
patients. Doing several tests alwaysin the same order is one of the
limitations of this study.The order of tests would be randomized to
reduce the effectof one test to another one. Several tests may also
raise aquestion of fatigability and adaptation, although we
alwayscared about resting patients for 15 to 20 minutes.
Anotherlimitation could be blinding of investigators. Ideally, a
personinterpreting a test should be blinded to the results of all
theother tests. Testing and interpretation were made by
differentpeople in this study. However, interpretation of all tests
wasmade by the sameperson. Finally, some limitationsmay existto
raise a general conclusion for the utility of a clinical test ina
single center study, which needs to be reviewed by a multicenter
study.Choung et al. have reviewed the effect of the so-called
bow and lean test (affected ear was in the same directionas
bowing nystagmus in geotropic nystagmus and the samedirection as
leaning nystagmus in apogeotropic nystagmus)to determine the side
of the affected canal in 26 patientswith LC-BPPV. This test, which
was actually similar to theHBT, revealed no nystagmus in 3 patients
(11.5%) and wasnot comparable with HRM in the supine position in 7
pa-tients (26.9%) (12). Lee et al. have reviewed the
lateralizingvalue of head bending nystagmus in 54 patients with
LC-BPPV while sitting (13). Fifteen patients had no head-bending
nystagmus (27.8%), and it was not comparablewith head turning
asymmetric nystagmus in the supineposition in 5 patients. The
overall diagnostic value was63% (34/54).Identification of the
affected side with HRM is gener-
ally possible in patients with LC-BPPV in the presenceof
nystagmus with asymmetric intensity and the relief ofsymptoms after
therapeutic maneuver confirms the de-termination of the laterality.
It seems that the cure rate ishigh for both geotropic and
apogeotropic type LC-BPPVif the laterality is clearly evident by
HRM. Forty-threeof 44 patients with geotropic and 23 of 24 patients
withapogeotropic nystagmus responded well at least to one ofthe
therapeutic maneuvers. However, HRM indicated theinvolved side in
75% of patients with apogeotropic nys-tagmus and 95.6% of patients
with geotropic nystagmusin this series. Therefore, it is an
important measure toalways include other diagnostic signs in the
test battery toincrease the rate of identification of the involved
side.
Our findings do not support the diagnostic contributionof HBT in
identification of the affected side. It has beenconcluded in this
study that the diagnostic role of patientssubjective feeling of
vertigo, which has not been paidmuchattention in previous studies,
is reliable and the diagnosticreliability of patients report and
LDPT is statistically moresignificant than HBT. However, despite
all these diagnos-tic tests, there were 3 patients with
bi-directional geotropic(1 patient) and apogeotropic nystagmus (2
patients) withsymmetric severity where the affected side remained
un-diagnosed. Several attempts at therapeutic maneuvers
wererequired on both sides in these patients, and the cure
waseventually delayed. Although it has been scarcely reported,this
raises a possibility of a bilateral disease.
CONCLUSION
In conclusion, HRM has the greatest diagnostic value
ofpositioning tests in LC-BPPV in this study. LDPT providessome
contribution in the diagnosis of LC-BPPV but muchless than HRM.
LDPT was useful when combined with theHRM, especially if the
patients had symmetric nystagmuson turning their head to either
side. Patients subjectivefeeling of vertigo was also a useful test.
Therefore, patientsreport and LDPT should be included in the test
battery ofpatients with LC-BPPV. However, HBT was not as sensi-tive
as other measures in uncertain cases in this series.
Acknowledgments: The authors thank all personnel of
thedepartment for their valuable help to the patients. The authors
alsothank to Mr. Murat Gul, associate professor, Giresun
University,Department of Statistics ([email protected]) for his
reviewof the data.
REFERENCES
1. McClure JA. Horizontal canal BPV. J Otolaryngol
1985;14:30Y5.2. Baloh RW, Yue Q, Jacobson KM, Honrubia V.
Persistent direction-
changing positional nystagmus another variant of benign
positionalnystagmus. Neurology 1995;45:1297Y301.
3. Nuti D, Vannucchi P, Pagnini P. Benign paroxysmal
positionalvertigo of the horizontal canal: a form of
canalolithiasis with vari-able clinical features. J Vestib Res
1996;6:173Y84.
4. Lempert T, Tiel-Wilck K. A positional maneuver for treatment
ofhorizontal-canal benign positional vertigo. Laryngoscope
1996;106:476Y8.
5. Appiani GC, Catania G, Gagliardi M, Cuiuli G.
Repositioningmaneuver for the treatment of apogeotropic variant of
horizontalcanal paroxysmal positional vertigo. Otol Neurotol
2005;26:257Y60.
TABLE 1. Comparative analysis of the test results for patients
with geotropic and apogeotropic nystagmus
Tests Geotropic nystagmus (46 patients) Apogeotropic nystagmus
(32 patients) p
Rate of nystagmus seen with HBT-A 28.3% 25% 0.275Rate of
nystagmus seen with HBT-C 32.6% 21.7% 0.088Rate of nystagmus seen
with LDPT 52% 65.6% 0.655Patients subjective feeling of more severe
side 63% 56% 0.109Patients benefit based on LDPT 2.2% 12.5% a
0.018Overall cure rate 95.6% (44/46) 84.3% (27/32) a 0.044
HRM indicates head-roll maneuver; LDPT, Lying down positioning
test; HBT- a, head bending test at position A; HBT- C, head bending
test atposition- C.
a Significant p values.
6 S. YETISER AND D. INCE
Otology & Neurotology, Vol. 00, No. 00, 2015
Copyright 2015 Otology & Neurotology, Inc. Unauthorized
reproduction of this article is prohibited.
-
6. Appiani GC, Catania G, Gagliardi M. A liberatory maneuver for
thetreatment of horizontal canal paroxysmal positional vertigo.
OtolNeurotol 2001;22:66Y9.
7. Casani AP, Vannucci G, Fattori B, Berrettini S. The treatment
ofhorizontal canal positional vertigo. Our experience in 66 case.
La-ryngoscope 2002;112:172Y8.
8. Balatsouras DG, Koukoutsis G, Ganelis P, Korres GS, Kaberos
A.Diagnosis of single- or multiple-canal benign paroxysmal
posi-tional according to the type of nystagmus. Int J Otolaryngol
2011;2011:483965.
9. HanBI, OhHJ, Kim JS. Nystagmuswhile recumbent in horizontal
canalbenign paroxysmal positional vertigo. Neurology
2006;66:706Y10.
10. Nuti D, Vannucchi P, Pagnini P. Lateral canal BPPV: Which is
theaffected side? Audiol Med 2005;3:16Y20.
11. Asprella-Libonati G. Diagnosis and treatment strategy of the
lateralsemicircular canal canalolithiasis. Acta Otorhinolaryngol
Ital 2005;25:277Y83.
12. Choung YH, Shin YR, Kahng H, Park K, Choi SJ. Bow and
leantest to determine the affected ear of horizontal canal benign
par-oxysmal positional vertigo. Laryngoscope 2006;116:1776Y81.
13. Lee SH, Choi KD, Jeong SH, Oh YM, Koo JW, Kim JS.
Nystagmusduring neck flexion in the pitch plane in benign
paroxysmal posi-tional vertigo involving the horizontal canal. J
Neurol Sci 2007;256:75Y80.
7HEAD-BENDING AND LYING-DOWN TESTS
Otology & Neurotology, Vol. 00, No. 00, 2015
Copyright 2015 Otology & Neurotology, Inc. Unauthorized
reproduction of this article is prohibited.