Embed Size (px)
Citation preview

Diagnostic Yield of the Comprehensive Assessmentof Developmental Delay/Mental Retardation in anInstitute of Child Neuropsychiatry
Agatino Battaglia,1* Elena Bianchini,1 and John C. Carey2
1Stella Maris Scientific Research Institute, Institute of Child Neurology and Psychiatry, University of Pisa,Calambrone (Pisa), Italy
2Division of Medical Genetics, Department of Pediatrics, University of Utah, Salt Lake City, Utah
The Consensus Conference of the AmericanCollege of Medical Genetics has establishedguidelines regarding the evaluation of pa-tients with mental retardation (MR) [Curryet al., Am. J. Med. Genet. 72:468–477, 1997].They emphasized the high diagnostic utilityof cytogenetic studies and of neuroimagingin certain clinical settings. However, dataon the diagnostic yield of these studies inwell-characterized populations of individu-als with MR are scant. Majnemer and She-vell [J. Pediatr. 127:193–199, 1995] attained adiagnostic yield of 63%. However, this studyincluded only 60 patients and the classifica-tion included pathogenetic and causalgroups. The Stella Maris Institute has evalu-ated systematically patients with develop-mental delay (DD)/MR and performed vari-ous laboratory studies and neuroimaging inalmost all patients. We report a retrospec-tive analysis of the diagnostic yield of 120consecutive patients observed at our Insti-tute during the first 6 months of 1996. Therewere 77 males and 43 females; 47 weremildly delayed (IQ 70–50), 31 were moder-ately delayed (IQ 50-–35), and 42 were se-verely delayed (IQ 35–20). Diagnostic stud-ies (history, physical examination, standardcytogenetics, fragile X testing, molecularstudies, electroencephalography, electro-myography, nerve conduction studies, neu-roimaging, and metabolic screening tests)yielded a causal diagnosis in 50 (41.6%) anda pathogenetic diagnosis in 47 (39.2%) of the120 patients. Causal categories includedchromosomal abnormalities (14), Fra(X)syndromes (4), known MCA/MR syndromes
(19), fetal environmental syndromes (1),neurometabolic (3) disorders, neurocutane-ous (3) disorders, hypoxic-ischemic enceph-alopathy (3), other encephalopathies (1),and congenital bilateral perisylvian syn-drome (2). Pathogenetic categories includedidiopathic MCA/MR syndromes (35), epilep-tic syndromes (10), and isolated lissenceph-aly sequence (2). Diagnostic yield did notdiffer across categories and degree of DD.Our results, while confirming the diagnosticutility of cytogenetic/molecular genetic, andneuroimaging studies, suggest the useful-ness of accurate electroencephalogram re-cordings, and stress the importance of athorough physical examination. Referral toa university child neurology and psychiatryservice, where a comprehensive assessmentwith a selected battery of investigations ispossible, yields etiologic findings in a highpercentage of DD/MR patients, with impor-tant implications for management, progno-sis and recurrence risk estimate. Am. J.Med. Genet. 82:60–66, 1999.© 1999 Wiley-Liss, Inc.
KEY WORDS: developmental delay; mentalretardation; comprehensiveassessment; diagnostic yield;rational evaluation
INTRODUCTION
Mental retardation (MR) is a variable, heteroge-neous manifestation of central nervous system dys-function, a test result, an educational dilemma, a causeof personal and social anxiety, and a public signal ofconcern. The American Association on Mental Retar-dation recently (in 1992) defined it as follows: ‘‘Mentalretardation refers to substantial limitations in presentfunctioning. It is characterized by significantly sub-average intellectual functioning, existing concurrentlywith related limitations in two or more of the following
*Correspondence to: Dr. Agatino Battaglia, Stella Maris Scien-tific Research Institute, Institute of Child Neurology and Psy-chiatry, University of Pisa, via dei Giacinti 2, 56018, Calam-brone (Pisa), Italy.
Received 23 June 1998; Accepted 3 August 1998
American Journal of Medical Genetics 82:60–66 (1999)
© 1999 Wiley-Liss, Inc.

applicable adaptive skill areas: communication, self-care, home living, social skills, community use, self-direction, health and safety, functional academics,leisure and work.’’ Mental retardation may become evi-dent during infancy or early childhood as developmen-tal delay (DD).
It is a common clinical problem in pediatrics, occur-ring in approximately 2 to 10% of the population[Stevenson, 1996; McLaren and Bryson, 1987; Drillienet al., 1988; Simeonsson and Sharp, 1992]. Althoughrecent data from the United States Department of Edu-cation [Massey and McDermott, 1995] indicate that theprevalence of MR among school age children (6–17years) is around 1.14%, it is probably still the mostfrequent reason for referral to an institute of child neu-rology and psychiatry.
Despite its frequency and its huge impact on society,controversy still exists, within the medical profession,regarding the appropriate clinical and laboratory in-vestigations directed at the understanding of itscauses. As a consequence, a diagnostic evaluation ofunnecessary complexity, invasiveness, expensiveness,and hurt to the patient is carried out in many in-stances.
The Consensus Conference of the American Collegeof Medical Genetics on the evaluation of patients withmental retardation (MR)/developmental delay (DD) es-tablished guidelines [Curry et al., 1997] and empha-sized the high diagnostic utility of cytogenetic studiesand of neuroimaging in certain clinical settings.
However, data on the diagnostic yield of these evalu-ations in well-characterized populations of individualswith mental retardation is scant. A few studies docu-menting systematic investigation of individuals in in-stitutions for persons with mental retardation werepublished in the 1970s [Moser and Wolf, 1971; Gus-tavson et al., 1977a, 1977b; Laxova et al., 1977; Opitzet al., 1978]. These studies are well summarized byMoser et al. [1990]. These works mostly dealt with pa-tients who had severe to profound MR; moreover, op-tions for laboratory testings have improved substan-tially since that time.
In a recent study by Majnemer and Shevell [1995],the diagnostic yield was stated as 63%. However thisstudy only included 60 patients and the etiologic clas-sification comprised descriptive grouping as well ascausal ones.
At the Stella Maris Clinical Research Institute, auniversity-based institute of child neurology and psy-chiatry, we have evaluated systematically patients re-ferred because of DD/MR and performed a comprehen-sive assessment in almost all of them (Table I). Thepurpose of the present study was to determine thecausal or diagnostic yield of the comprehensive assess-ment of DD/MR carried out in our institution, in anattempt to address the unanswered questions still ex-isting on the issue.
MATERIALS AND METHODS
We report a retrospective analysis of the diagnosticyield of 120 consecutive patients observed at our Insti-tute during the first 6 months of 1996. These patients
represent the Institute patients evaluated and followedby a child neurologist. Seven of the patients had beenseen previously and diagnosed at our Institute, andwere being followed. Patients with an established di-agnosis, such as Down syndrome, were excluded. Therewere 77 males and 43 females, age 21⁄2 to 19 years.Forty-seven were mildly delayed (IQ 70–50), 31 weremoderately delayed (IQ 50–35), and 42 were severelydelayed (IQ 35–20). Essential elements of the evalua-tion included: a three-generation pedigree; pre-, peri-,and post-natal history; complete physical examinationfocused on the presence of anomalies, including minoranomalies; neurologic examination; and assessment ofthe behavior phenotype (Table I).
If, after a complete pre-, peri, and post-natal historyand clinical examination, a causal diagnosis was notevident, standard cytogenetic and molecular fragile Xstudies (FRAXA-FRAXE), metabolic and endocrino-logic screening, skeletal X-rays, heart and abdomen ul-trasonography, ophthalmologic and audiologic evalua-tions, neuroimaging, and neurophysiology studies werecarried out.
In case of congenital anomalies, standard cytoge-netic, high-resolution banding (HRB), fluorescent insitu hybridization (FISH), and other molecular studieswere performed (apparent Angelman syndrome, Prader-Willi syndrome, Wolf-Hirschhorn syndrome, velo-cardio-facial syndrome, and all idiopathic MCA/MRsyndromes). Physical findings on neurologic examina-tion, such as micro- or macrocrania, abnormal muscletone or reflexes, coordination abnormalities, or a his-tory suggestive of hypoxic-ischemic encephalopathy ledto neuroimaging. Magnetic resonance imaging (MRI)was the study of first choice; computerized tomography(CT) was carried out only in a few patients who hadtuberous sclerosis complex, or a suspected craniosyn-ostosis. In case of motor involvement we studied so-matosensory-evoked potentials, while electromyogra-phy and nerve conduction studies were carried outwhenever a neuromuscular disorder was suspected. In
TABLE I. Comprehensive Assessment of Patients with DD/MR
Three-generation pedigreePre-, peri-, and post-natal historyPhysical examination focused on the presence of anomalies
(including minor anomalies)Neurologic examinationLaboratory investigations (chromosomes, Fra(X) metabolic/
endocrinologic, heart/abdominal echo, EEG/EPs/EMG, CT/MRI, X-ray survey, audiologic)
Ophthalmologic evaluationNeuropsychological evaluation with IQ testingPsychiatric interview to include personality styleEvaluation of language production and comprehensionEducation evaluation including achievement tests
TABLE II. Waking/Sleep Video-EEG-Polygraphy
Seizures/epilepsySignificant language impairmentAngelman syndromeInv dup(15) syndromeWolf-Hirschhorn syndrome
Diagnostic Yield of the Comprehensive Assessment of DD/MR 61

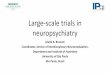
case of language impairment audiometry and brain-stem auditory-evoked potentials were performed. Elec-troencephalograms (EEGs) were performed on virtu-ally all patients, and more accurate studies, such aswaking and sleep video-EEG-polygraphy, were done inspecific situations (Table II, Fig. 1).
Most of our patients had repeated evaluations,whether as part of the functional work-up or in an at-tempt to better define over time their physical and/orbehavior phenotype.
RESULTS
After completion of history, physical examinationand other investigations, the etiologic diagnosis re-mained unknown in 23 (19.1%) of the 120 patients. Inthe remaining 97 (80.8%) a diagnosis was determinedand fell into causal and pathogenetic categories (TableIII). The causal categories included the following: chro-mosomal abnormalities in 14 (11.6%) (Table IV); Fra(X)syndromes in four (3.3%); known MCA/MR syndromesin 19 (15.8%) (Table V); neurocutaneous disorders inthree (2.5%) (tuberous sclerosis in two patients andneurofibromatosis type 1 in one patient); neurometa-bolic disorders in three (2.5%) (neuroaxonal dystrophyin two patients and Menkes kinky hair disease in one
TABLE III. Diagnostic Yield of DD/MR (n 4 120)
N %
Causal categoriesChromosomal 14 11.6Fragile (X) syndrome 4 3.3Known MCA/MR syndromes 19 15.8Neurocutaneous disorders 3 2.5Neurometabolic disorders 3 2.5Congenital bilateral perisylvian syndrome 2 1.6Toxin (FAS) 1 .8Presumed hypoxic/ischemic eucephalopathy 3 2.5Infection 1 .8
Pathogenetic categoriesEpileptic syndromes 10 8.3Isolated lissencephaly sequence 2 1.6Idiopathic MCA/MR syndrome 35 29.1
Unknown cause (by elimination) 23 19.1
TABLE IV. Chromosomal Abnormalities Diagnosedin 14 Patients
Chromosomal abnormality n
del (9p) 3del (4p) 3del (5p) 27q+ 147,XXY 1inv dup(15) 147,XX,+13 1del 15q (Prader-Willi) 1del 22q11 (velo-cardio-facial) 1
Fig. 1. Surface polygraphic EEG recording in a patient with Lennox-Gastaut syndrome. Left: during wakefulness, diffuse burst of ill-definedspike/wave complexes at 1.5–2.5 Hz of 7-sec duration with a very marked reduction of muscular contraction (over both temporal areas), accompanied byeye staring. Center: diffuse, fast recruiting rhythms are accompanied by tachypnea, during slow sleep. Right: during REM sleep disappearance ofparoxysmal features.
62 Battaglia et al.

patient); exposure to toxins in one (0.8%) (fetal alcoholsyndrome); hypoxic ischemic encephalopathy in three(2.5%); encephalopathy due to encephalitis in one(0.8%); congenital bilateral perisylvian syndrome intwo (1.6%).
The pathogenetic categories included the following:‘‘epileptic syndromes’’ in 10 (8.3%), according to the1989 ILAE classification (Table VI); isolated lissen-cephaly sequence in two (1.6%); idiopathic MCA/MRsyndromes in 35 (29.1%). This latter group consisted ofpatients who had enough minor anomalies to allow theclinician to draw the inference that there was a syn-dromal pattern. The diagnosis had been suspected bythe referring physician in only four (3.3%) of 120 pa-tients.
The evidence needed to determine a causal andpathogenetic diagnosis (Table VII) was provided by his-tory and physical examination alone in 19.1%; whilehistory, physical examination, and laboratory tests to-gether were useful in 50%. Among the latter, the nec-essary tests were represented by cytogenetic/moleculargenetic studies in 35%, EEG in 8.3%, and neuroimag-ing in 5.9%. Laboratory tests alone made the diagnosisin 10.7%. Among these the necessary investigationswere represented by cytogenetic/molecular geneticstudies in 7.5%, neuroimaging in 1.6%, and metabolicstudies in 1.6%.
DISCUSSION
In this cohort of children referred for evaluation ofDD/MR, a causal/pathogenetic diagnosis was reachedin 80.8%. Previous studies have been restricted to in-
stitutionalized cohorts of individuals with severe men-tal retardation [Moser and Wolf, 1971; Laxova et al.,1977; Opitz et al., 1978; McLaren and Bryson, 1987;Hunter et al., 1980; Hagberg and Kyllerman, 1983] andonly scant data exist on determination of etiologic di-agnosis in persons with mild to moderate mental retar-dation [McLaren and Bryson, 1987; Schaefer andBodensteiner, 1992]. This most likely reflects the diffi-culty of ascertainment, as well as the general assump-tion that the causes are cultural and familial ratherthan pathological.
The Stella Maris Clinical Research Institute is a re-ferral university hospital for patients under 18 years ofage with neuropsychiatric and developmental disor-ders. Patients admitted to our Institute come from allover Italy and show not only severe mental retardationand/or severe epilepsy, but, in many instances, mild ormoderate mental retardation or just learning disabili-ties or speech difficulties or behavioral disturbances.Therefore it is likely that our sample represents a rea-sonable cross-section of the spectrum of developmentaldisabilities in our referral network, with the exceptionof metabolic disorders. In fact patients with these dis-orders usually are referred to a nearby center for meta-bolic diseases.
A diagnostic yield of 80.8% exceeds previously pub-lished and inferred estimates. We think that the im-proved yield most likely represents the results of thefollowing factors: 1) the awareness that nowadays de-velopmental/genetic factors underlie most cases of de-
TABLE V. Known MCA/MR Syndromes Diagnosedin 19 Patients
Syndrome n
Brachmann-de Lange syndrome 3KBG syndrome 2Sotos syndrome 2Angelman syndrome 2Provisionally unique syndromea 2Oculo-dento-digital syndrome 1‘‘Michelin-tire’’ 1Waardenburg syndromeb 1Saethre-Chotzen syndrome 1Apert syndrome 1Rubinstein-Taybi syndrome 1NF/Noonan syndrome 1Frontonasal malformation 1
aThis group represents patients with MCA/MR syndromes reported in thepeer-reviewed literature by the authors.bIt is worth noting that the patient had periventricular nodular grey mat-ter heterotopias.
TABLE VI. ‘‘Epileptic Syndromes’’ Diagnosed in 10 Patients
Syndrome n
Lennox-Gestaut syndrome (see Fig. 1) 2Severe myoclonic epilepsy 1Epilepsy with myoclonic-astatic seizures 1Symptomatic generalized epilepsy 3Partial symptomatic epilepsy 2Epilepsy undetermined whether focal or generalized 1
TABLE VII. Evidence Needed for Ascertainment of Causal andPathogenetic Diagnosis*
Method Examples
1. H/P alone (19.1%) Known MCA/MR syndrome-NF1-ITO-FAS
2. H/P + lab (50%)H/P + cytogenetic/
molecular (35%)WHS-PWS-AS-VCFS-FraX-
idiopathic MCA/MR syndromeH/P + EEG (8.3%) Epileptic syndromesH/P + neuroimaging
(5.9%)HIE-TSS-CBPS
H/P + other lab (0.8%) Menkes3. Lab alone (10.7%)
Cyto/molecular (7.5%) FraX; 7q+; Inv dup(15);47,XXY; del(9p)
Neuroimaging (1.6%) Isolated lissencephaly sequenceMetabolic (1.6%) NAD
*H, history; P, physical; FAS, fetal alcohol syndrome; WHS, Wolf-Hirschhorn syndrome; PWS, Prader-Willi syndrome; AS, Angelman syn-drome; VCFS, velo-cardio-facial syndrome; HIE, hypoxic-ischemic enceph-alopathy; TSS, tuberous sclerosis syndrome; CBPS, congenital bilateralperisylvian syndrome; NAD, Neuroaxonal dystrophy.
TABLE VIII. Clinical Conditions in Which Diagnosis ProvidedCrucial Genetic Information (68.3% of Patients)
14 Patients: chromosomal abnormalities4 Patients: Fra(X) syndrome
19 Patients: known MCA/MR syndromes35 Patients: idiopathic MCA/MR syndromes3 Patients: neurometabolic disorders3 Patients: neurocutaneous disorders2 Patients: congenital bilateral perisylvian syndrome2 Patients: isolated lissencephaly sequence
Diagnostic Yield of the Comprehensive Assessment of DD/MR 63

velopmental delay, 2) the knowledge that more andmore developmentally delayed patients may have asyndrome, 3) improved ability in studying and diagnos-ing patterns of malformation, 4) improved diagnostictesting, specifically cytogenetic and molecular tech-niques, neuroimaging, metabolic screenings and de-tailed EEG studies, and 5) long-term follow-up.
All such points emphasize that the successful deter-mination of cause and pathogenesis depends on howhard one looks, as is strongly suggested by our find-ings. Diagnostic yield did not differ substantiallyacross categories of degree of DD. This indicates thatthe clinician should not rely solely on the severity ofdelay to mandate a thorough investigational approach.
Although the number of causal and pathogenetic cat-egories is large, we conclude that children with MCA/MR syndromes make up an important group (59.1%).In 82 (68.3%) of 120 patients a causal or pathogeneticdiagnosis provided crucial information regarding ge-netic counseling and recurrence risks (Table VIII).Laboratory tests most helpful in determining diagno-sis, together with the history and physical examina-tion, were cytogenetic/molecular genetic analysis(15%), detailed EEG studies (8.3%), and neuroimaging(7.5%).
Our yield of cytogenetic/molecular genetics appearsto be well in line with the data reported previously[Bourgeois and Benezech, 1977; Kodama, 1982; Opitzet al., 1982; Rasmussen et al., 1982; Wuu et al., 1984,1991; Gustavson et al., 1987; Srsen et al., 1989; Phelanet al., 1996] where chromosomal abnormalities arefound in 4 to 28% of patients with MR. Six of our cases,
thought to be nonsyndromal, turned out to be XXY, invdup(15), 7q+, del 9p and Fra(X). The four aneuploidcases represented 10.2% of the apparently nonsyndro-mal patients, while the two Fra(X) patients repre-sented 5.1% of this group. This and other experience[Curry et al., 1996] suggest the utility of cytogenetic/molecular genetic analyses in individuals with DD/MR,even in the apparent absence of minor anomalies.
Cerebral anomalies on neuroimaging were reportedin 9 to 60% of individuals with MR [Moeschler etal., 1981; Lingam et al., 1982; Sugimoto et al., 1993;Majnemer and Shevell, 1995; Curry et al., 1996; Rootand Carey, 1997]. The diagnostic yield of neuroimagingin our patients was apparently low (7.5%), but it isworth noting that many of our patients had cerebralabnormalities on MRI/CT that were merely descriptivefindings and not adding to our knowledge of cause, andthus were not counted.
To date little, if anything, was reported on the valueof the EEG in MR patients. We stress the relativelyhigh diagnostic yield (8.3%) of EEG investigations inour study group, and recommend EEG studies not onlyin the presence of a clinical history of seizures/epilepsy,but also in other specific clinical settings (Table II). Insuch cases the EEG may be very helpful for treatmentand for diagnostic purposes [Battaglia et al., 1996a,1996b, 1997; Guerrini et al., 1996].
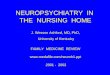
Figure 2 presents an algorithm for the rationalevaluation of a patient with DD/MR. Based on histori-cal and physical examination, the work-up of a patientcan follow various pathways that guide decisions re-garding laboratory testing and imaging studies. For
Fig. 2. Algorithm for rational evaluation of DD/MR patients. CBPS, Congenital bilateral perisylvian syndrome; HIE, hypoxic-ischemic encephalop-athy; ALD, adrenoleucodystrophy; RTS, Rubinstein-Taybi syndrome; KBG, KBG syndrome; PWS, Prader-Willi syndrome; WHS, Wolf-Hirschhorn syn-drome; SLO/RSH, Smith-Lemli-Opitz syndrome.
64 Battaglia et al.

example a patient that has multiple anomalies on ex-amination would have a different series of tests than apatient who presents with neurologic abnormalitieswithout anomalies. The framework is designed to beonly a guideline as the various branches are not nec-essarily mutually exclusive but do provide a way toapproach the patient.
The inference that a patient with an MCA/MR syn-drome has an organized syndromal pattern, even with-out a specific diagnosis, helps with counseling the fam-ily regarding recurrence risk. One is able to utilize em-piric figures for this circumstance [Bartley et al., 1978;Opitz et al., 1978; Herbst et al., 1982]. Moreover, thisgrouping is significant because follow-up of these pa-tients may eventually lead to a definite diagnosis oreven the characterization of a novel syndrome.
The low yield of metabolic tests in our samplematched the clinical expectations. Indeed we agreewith previous statements [Curry et al., 1997] thatmetabolic testing should be highly selective and initi-ated only in the presence of suggestive clinical andphysical findings.
On the whole we think that the most relevant meth-ods available to child neurologists and medical geneti-cists for the evaluation of DD/MR is a thorough physi-cal examination, which, alone, helped us in determin-ing diagnosis in 22 cases (18.3%). The effort made todetermine a causal and pathogenetic diagnosis in ourpatients had obvious implications with respect to man-agement, prognosis, and recurrence risk estimate.
We conclude that the diagnosis of ‘‘global develop-mental delay/mental retardation’’ should not be theend point, but rather a springboard for an effectivesearch for causal factors.
ACKNOWLEDGMENTS
We wish to express our appreciation to the reviewersfor their helpful comments and suggestions.
REFERENCES
Bartley JA, Hall BD. 1978. Mental retardation and multiple congenitalanomalies of unknown etiology: Frequency of occurrence in similarlyaffected sibs of the proband. In: Summitt RL, Bergsma D, editors. Re-cent advances and new syndromes. Birth Defects 14. p 127–137.
Battaglia A, Carey JC, Cederholm P, Viskochil D, Brothman A. 1996a.Natural history: Experience with 11 cases of Wolf-Hirschhorn syn-drome. Am J Hum Genet 59(4):36A.
Battaglia A, Carey JC, Thompson JA, Filloux FM. 1996b. EEG studies inthe Wolf-Hirschhorn (4p-) syndrome. EEG Clin Neurophysiol 99:324.
Battaglia A, Gurrieri F, Bertini E, Bellacosa A, Pomponi MG, Paravatou-Petsotas M, Mazza S, Neri G. 1997. The inv dup(15) syndrome: A clini-cally recognizable syndrome with altered behavior, mental retardation,and epilepsy. Neurology 48:1081–1086.
Bodensteiner JB, Schaefer GB. 1995. Evaluation of the patient with idio-pathic mental retardation. J Neuropsychiatry Clin Neurosci 7:361–370.
Bourgeois M, Benezech M. 1977. Cytogenetic survey of 600 mentally re-tarded hospitalized patients. Encephale 3:361–370.
Commission on Classification and Terminology of the International LeagueAgainst Epilepsy. 1989. Proposal for revised classification of epilepsiesand epileptic syndromes. Epilepsia 30:389–399.
Curry CJ, Sandhu A, Frutos L, Wells R. 1996. Diagnostic yield of genetic
evaluations in developmental delay/mental retardation. Clin Res 44:130A.
Curry CJ, Stevenson RE, Aughton D, Byrne J, Carey JC, Cassidy S, Cun-niff C, Graham JM Jr, Jones MC, Kaback MM, Moeschler J, SchaeferBG, Schwartz S, Tarleton J, Opitz J of the American Journal of MedicalGenetics. 1997. Evaluation of mental retardation: Recommendations ofa consensus conference. Am J Med Genet 72:468–477.
Drillien CM, Pickering RM, Drummond MB. 1988. Predictive value ofscreening for difficult areas of development. Dev Med Child Neurol30:294–305.
Evans ED, Carey JC. 1988. Etiologic evaluation of children referred fordevelopmental delay. Clin Res 36:207A.
Guerrini R, De Lorey TM, Bonanni P, Moncla A, Dravet C, Suisse G, LivetMO, Bureau M, Malzac P, Genton P, Thomas P, Sartucci F, Simi P,Serratosa JM. 1996. Cortical myoclonus in Angelman syndrome. AnnNeurol 40:39–48.
Gustavson KH, Hagberg B, Hagberg G, Sars K. 1977a. Severe mentalretardation in a Swedish county 1. Epidemiology, gestational age, birthweight and associated CNS handicap in children born 1959–70. ActaPaediatr Scand 66:373–379.
Gustavson KH, Hagberg B, Hagberg G, Sars K. 1977b. Severe mentalretardation in a Swedish county II. Etiologic and pathogenetic aspectsof children born 1959–1970. Neuropediatrie 8:293–304.
Gustavson KH, Holmgren G, Blomquist HK. 1987. Chromosomal aberra-tions in mildly mentally retarded children in a northern Swedishcounty. Ups J Med Sci 44:154–168.
Hagberg B, Kyllerman M. 1983. Epidemiology of mental retardation: ASwedish survey. Brain Dev 5:441–449.
Herbst DS, Baird PA. 1982. Sib risks for non-specific mental retardation inBritish Columbia. Am J Med Genet 13:197–208.
Hunter AGW, Evans JA, Thompson DR, Ramsay S. 1980. A study of insti-tutionalized mentally retarded patients in Manitoba. I. Classificationand preventability. Dev Med Child Neurol 22:145–162.
Kodama Y. 1982. Cytogenetic and dermatoglyphic studies on severelyhandicapped patients in an institution. Acta Med Okayama 36:383–397.
Laxova R, Ridler MAC, Bowen-Bravery M. 1977. An etiological survey ofthe severely retarded Hertfordshire children who were born betweenJanuary 1, 1965 and December 31, 1967. Am J Med Genet 1:75–86.
Lingam S, Read S, Holland IM, Wilson J, Brett EM, Hoare RD. 1982. Valueof computerised tomography in children with non-specific mental sub-normality. Arch Dis Child 57:381–383.
Majnemer A, Shevell MI. 1995. Diagnostic yield of the neurologic assess-ment of the developmentally delayed child. J Pediatr 127:193–199.
Massey PS, McDermott S. 1995. State-specific rates of mental retarda-tion—United States, 1993. MMWR 45:61–65.
McLaren J, Bryson SE. 1987. Review of recent epidemiological studies ofmental retardation: Prevalence, associated disorders, and etiology. AmJ Ment Retard 92:243–254.
Moeschler JB, Bennet FC, Cromwell LD. 1981. Use of the CT scan in themedical evaluation of the mentally retarded child. J Pediatr 98:63–65.
Moser HW, Wolf PA. 1971. The nosology of mental retardation: Includingthe report of a survey of 1378 mentally retarded individuals at theWalter E. Fernald State School. Birth Defects 7(1):117–134.
Moser HW, Ramey CT, Leonard CO. 1990. Mental retardation. In EmeryAEH, Rimoin DL, editors. Principles and practice of medical genetics.2nd ed. New York: Churchill Livingstone, pp 495–511.
Opitz JM, Kaveggia EG, Durkin-Stamm MV, Pendleton E. 1978. Diagnos-tic/genetic studies in severe mental retardation. Birth Defects 14(6B):1–38.
Opitz JM, Kaveggia EG, Laxova R, Pallister PD. 1982. The diagnosis andprevention of severe mental retardation, Vol. II. Proceedings, interna-tional conference on preventable aspects of genetic morbidity, Cairo. p117–138.
Phelan MC, Crawford EC, Bealer DM. 1996. Mental retardation in SouthCarolina III: Chromosome aberrations. Proc Greenwood Genet Ctr 15:45–60.
Rasmussen K, Nielsen J, Dahl G. 1982. The prevalence of chromosomeabnormalities among mentally retarded persons in a geographicallydelimited area of Denmark. Clin Genet 22:244–255.
Root S, Carey JC. 1997. Brain dysmorphology and developmental disabili-ties. Proc Greenwood Genet Ctr 16:224.
Diagnostic Yield of the Comprehensive Assessment of DD/MR 65

Schaefer GB, Bodensteiner JB. 1992a. Evaluation of the child with idio-pathic mental retardation. Pediatr Clin North Am 39:929–943.
Schaefer GB, Bodensteiner JB. 1992b. Evaluation of the child with idio-pathic mental retardation. Pediatr Neurol 39:929–943.
Simeonsson RJ, Sharp MC. 1992. Developmental delays. In: HockelmanRA, Friedman SB, Nelson NM, Seidel HM, editors. Primary pediatriccare. 2nd ed. St. Louis: Mosby Year Book, p 867–870.
Srsen S, Misovicova N, Srsnova K, Volna J. 1989. Chromosomal aberra-tions in a group of mentally retarded persons. Cesk Psychiatr 85:9–18.
Stevenson R. 1996. Mental retardation. Overview and historical perspec-tive. Proc Greenwood Genet Ctr 15:19–25.
Sugimoto T, Yasuhara A, Nishida N, Murakami K, Woo M, Kobayasashi.1993. MRI of head in the evaluation of microcephaly. Neuropediatrics24:4–7.
Wuu KD, Wuu SW, Liu IW. 1984. A cytogenetic survey of mentally re-tarded children in Taiwan: Final report on the incidence of chromosomeabnormalities. Proceedings of the National Science Council, Republic ofChina—Part B. Life Sci 8:83–88.
Wuu KD, Chiu PC, Li SY, Chen JY, Chao MC, Ko KJ, Wang TR, Hsiao KJ.1991. Chromosomal and biochemical screening on mentally retardedschool children in Taiwan. Jpn J Hum Genet 36:267–274.
66 Battaglia et al.