Embed Size (px)
Citation preview

HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
NHSNHS Improvement
A guide for review andimprovement of hospital basedheart failure services
Heart
NHS Improvement

Section 1
Introduction
The impact of heart failure
Recommended components of a heart failure service
Section 2
Service review
Section 3
Heart failure management issues in secondary care
Appendix 1
Appendix 2
Contents
3
3
3
4
5
5
7
7
13
13
Authors
Dr David Walker, Consultant Cardiologist, Hastings and Rother NHS Trust and NHS Improvement National Clinical Lead
Elaine Kemp, National Improvement Lead, NHS Improvement
Acknowledgements
Dr James Beattie, NHS Improvement National Clinical Lead
Dr Mark Dancy, NHS Improvement National Clinical Chair
Ms Janine O’Rourke, NHS Improvement National Clinical Advisor
Mr Michael Connelly, NHS Improvement National Clinical Lead
Dr Nigel Rowell, NHS Improvement National Clinical Lead

Introduction
The information in this documenthas been brought together by NHSImprovement, to help hospitalteams to review their heart failure(HF) service.
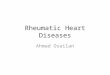
Nationally, there is marked variationin the length of stay andreadmission rate for heart failure in-patients (fig 1). It might be arguedthat a longer than average length ofspell reflects close attention todetail, to ensure that care isoptimised prior to discharge.However, if this is the case it shouldbe reflected in a low readmissionrate, which often it is not.Alternatively a short length of staymight indicate a very efficientservice – or conversely one wherepressure on beds leads toinappropriate early discharge beforemanagement is complete. The“Holy Grail” of short length of spelland low readmission rate does existbut is currently rare in the UK.
For providers where both of theseindicators are above the nationalaverage, a systematic review ofservices may help to identifyproblem areas and directsubsequent improvement work. Thetwo main aims of completing areview are to optimise the time apatient spends in hospital, withearly diagnosis and treatment, andto maximise the effective use ofresources within the trust and widerNHS community.
Section 1
A guide for review and improvement of hospital based heart failure services 3
www.improvement.nhs.uk/heart
The impact of heartfailure
Heart failure affects one in ahundred people in the UK, around620,000 people, increasing toaround 7 percent over the age of75. In 2009/10 Hospital EpisodeStatistics (HES) data showed therewere 73,752 hospital spells for heartfailure (coded in the first position)with a mean length of stay of 11.76days and a median of 8 days. Tenpercent of patients (8,385) werereadmitted with heart failure inunder 29 days. The governmentproposal not to pay hospitals for thistype of readmission in the futuremeans providers will be underpressure to reduce unnecessaryreadmissions. As an example ahospital where 20 patients arereadmitted with an average 5 daysstay could cost £30,000.
The national heart failure audit1
also highlights that:
• Within a year of admission for heart failure, 32% of patients died
• Mortality is significantly better for those who have access to specialist care i.e. those seen by cardiologists or specialist heart failure services (23 per cent).
In 2009/10, Basildon andThurrock University Hospitalreduced their heart failureadmissions median length ofstay from 12 days to fourdays, releasing 1,249 bed daysper year, a cost saving of£312,250.
This was achieved byspeeding up the diagnosis,optimising care quickly andlinking in to communityservices for early discharge.
1National Heart Failure Audit, 2010
Figure 1: LOS/readmission rates

4 A guide for review and improvement of hospital based heart failure services
Recommendedcomponents of a heartfailure service
NHS Improvement has reviewedmany successful heart failureservices (HF) services over the lastfew years, and this has revealedconsiderable consistency in theirorganisation. Certain key‘components’ are usually presentand these are outlined in the tableson the right. These components areby no means confined to secondarycare settings, and indeed in manycases are successfully delivered inprimary care. Even though thisresource is designed mainly forsecondary care, it is essential to lookat the totality of the serviceincluding the interaction betweencommunity and hospital.Optimisation of the primary-secondary care interface aroundreferral and discharge is critical forthe efficient use of resources.
www.improvement.nhs.uk/heart
1. System for early accurate diagnosis of outpatients
a.Serum NP testing to streamline referrals from primary careb.Rapid Access HF Clinic (in primary or secondary care)c. Echo on the day of clinical assessment d.Management plan produced on the daye.Ensure confirmed HF patients go on heart failure registers
2. Optimisation of treatment
a.System for uptitrating medication – hospital or community basedb.Agreed care planc.Patient education to facilitate self managementd.Access to cardiac rehabilitatione.Access to implantable cardiac devices
3. Identification of heart failure in patients
a.Serum NP and early inpatient echob.Management in dedicated area with expertise – Junior docs/nursesc.Close liaison/collaborative working with community over discharge planning
d.Discharge with a care management plan
4. Multidisciplinary team working
a.Case management discussions across primary-secondary care interface - early discharge, admission avoidance - seamless service
b.Consultant lead/+GP/hospital HF nurse(s)/community HF nurse(s) etcc.Designated care co-ordination
5. Supportive and palliative care
a.Unnecessary admission avoidance at end of life - preferred priorities of care
b.Palliative care involvementc.End of life models for example - Liverpool Care Pathway or the Gold Standards Framework - community
d.24/7 generic end of life care provision in the community into which heart failure specialists contribute

A guide for review and improvement of hospital based heart failure services 5
Service review
A service review provides keystakeholders (such as healthprofessionals, service managers andpatients) with a baseline assessmentto determine how well a service iscurrently provided and howeffectively it interfaces with patients.This information can then be usedto prioritise and plan changes forimprovement and measure theimpact after implementation.
1. Engage key stakeholdersKey stakeholders include anyonewho is responsible for, delivers partof, is a user of, or is affected by theheart failure service. As a minimumthis team should initially includerepresentation from the admittingand receiving medical teams, thelead clinician, nurse specialists, theservice manager and patients. Thiscomposition of the team may needto be adjusted during the review toconsider specific aspects of theservice.
It is important that as well asaccurate audit data, the opinions ofeach of these groups are capturedand form part of the baseline.Patient centred care should form thebackbone of any change and thereare many ways to ensure thatpatients and carers views driveimprovement. For further advice andguidance click here»
www.improvement.nhs.uk/heart
Section 2
2. Characterise the currentservice provisionDocument and characterise thecurrent service by each hospital site.This should include the currentlength of stay and readmission ratein comparison with the nationalbenchmark. This local HES data canbe provided by the trust informationdepartment (Appendix 2).
Hospital Episode Statistics (HES)data are generated by the hospitalcoding team, using informationfrom patients’ notes. Commissionersuse HES data to calculate thepayments a service receives.Apparently inaccurate hospital datarequires further investigationsupported by the originating clinicalteam, rather than outright rejection.If HES data is incorrect, payment forservices will be incorrect.
The National Heart Failure Auditprovides information on heartfailure treatment across the UK,including patient profiles, length ofhospital admission, interventions,medication and outcome. Dataentry into the national heart failureaudit is a Care Quality Commissionquality indicator. However, currentlynot all trusts are entering everyheart failure patient. Patients onwhom data has not been collectedare more likely to be those admittedunder specialities other thancardiology. It is also likely, andsupported by the audit itself, thatthese are the patients with longerlengths of stay and pooreroutcomes.
Using the heart failure audit asan accurate measure of asuccessful heart failure service isonly appropriate if it isrepresentative of all heart failurepatients.
An audit of patient notes confirmswhere in the patient pathwayconstraints repeatedly impinge uponpatient care or effective use ofresources and can be used to checkthe accuracy of HES coding.
3. Share the baseline with keystakeholdersSharing baseline details with keystakeholders will help validate thedata and inform the team. Note -avoid making comparisons betweenproviders or clinical teams as theremay be errors in the data orclinically appropriate reasons fordiffering indicators.
4. Map out the processThe basic improvement cycle can bedescribed as ‘PDSA’ – plan, do,study, act. For more details and for awide range of improvement toolsand techniques click here»
Involve all stakeholders in creatingand authenticating the process map.
Map out and record the steps whichoccur in a standard patient pathway,making sure to measure how longeach takes and where there arehandoffs (management of care orpaperwork changes hands). This willhighlight time where there is noadded benefit to patient care.

www.improvement.nhs.uk/heart
6 A guide for review and improvement of hospital based heart failure services
It is suggested to start the map fromthe time of presentation to thetrust, noting where the referralcomes from, through to the time offirst follow-up post discharge. Thestages can be divided, for example,into presentation and diagnosis,treatment and optimisation,discharge and follow-up.
Review the impact of services whichfeed into and receive patients toand from the in-patient service, suchas the system for referral fromprimary care and how patients aredischarged to community services.
List and quantify the impact of anyconstraints identified in the process.For example, if waiting for an in-patient echo causes delay, recordthe waiting time and the number ofpatients waiting. Calculate howmany bed days are wasted eachyear and what this costs, thencompare this with the cost ofproviding additional echo resources,to help inform subsequentdecisions.
5. Prioritise and planimprovementsCreate a list of where improvementsare required and the order in whichthese should be implemented.Section 3 describes some of thecommon challenges and suggestshow these might be tackled.
Once you have confidentlyidentified and measured theconstraints on the service, agreewith the key stakeholders whatactions should be taken to optimisecare and which should beimplemented first.
Ensure that these proposals areagreed with all the clinical team andby patient representatives. Supportfrom the management team is alsoessential to make sure the changesare in line with trust policy.
It is important to set goals for yourimprovements. There is very littlepoint in making changes if youcannot accurately assess whetherthe impact made is positive. Set abaseline for each of yourimprovements, then regularlymeasure this goal after theimprovement is implemented toensure it is effective, finally embedthis measurement into the regularrunning of the service so as theensure that the improvement ismaintained. An example might beto reduce the wait for an inpatientecho from the baseline median ofsix days, down to two days.
6. Action and reassessImplementation is a key step. Forfurther advice and guidance look onthe NHS improvement heart failurewebsite here»
Examples of how other heart failureservice providers have implementedchange within their service can beaccessed here»

www.improvement.nhs.uk/heart
A guide for review and improvement of hospital based heart failure services 7
Heart failure management issues in secondary care
Outpatients: Early accurate diagnosis and treatment
InpatientsReorganisation of heart failure carefor inpatients raises a number ofissues. In an ideal situation, all HFpatients should be managed whenin hospital, by a team led by aconsultant cardiologist or HFspecialist, on a specialist ward(cardiology or HF).
However, at present, in manyhospitals in the UK, HF patients arespread throughout the medical andcare of the elderly wards. Thereasons for this are many, butinclude elderly age, the presence ofco-morbidities and the variability ofpresentation (and subsequentdifficulty in rapid identification).Occasionally the influence of co-morbidities is so significant thatmanagement based on a care of theelderly ward is more appropriate.
Section 3
1. System for early accurate diagnosis of outpatients
a.Serum NP testing to streamline referrals from primary careb.Rapid Access HF Clinic (in primary or secondary care)c. Echo on the day of clinical assessment d.Management plan produced on the daye.Ensure confirmed HF patients go on heart failure registers
2. Optimisation of treatment
a.System for uptitrating medication – hospital or community basedb.Agreed care planc.Patient education to facilitate self managementd.Access to cardiac rehabilitatione.Access to implantable cardiac devices
Close integration of HF servicesacross primary and secondary care isessential at all stages of the patientpathway. New patients presentingto hospital with advanced HF orknown patients presenting withpoorly controlled symptoms may bean indication that some patients arenot being identified early enoughand treated effectively. The protocolfor initial investigation andsubsequent referral of suspectednew HF patients to specialistservices must be easily accessible toall in primary care. Once thediagnosis has been confirmed, theremust be an agreed care plan whichcovers support, up-titration ofmedication, subsequent follow upetc. to make sure that patients donot fall through the net. Rapid,comprehensive intervention in thisway can often avoid the need foradmission in this high risk group.

www.improvement.nhs.uk/heart
8 A guide for review and improvement of hospital based heart failure services
The crucial first step in thereorganisation of inpatient servicesis to identify patients presentingwith heart failure. There are twomain options here:
(i) Identification at the frontdoorThis is the ideal situation. Patientswith breathlessness or oedemasuggestive of HF should have animmediate serum NP measurement.Patients with a positive or borderlineresult should then receiveechocardiography in <24 hours toconfirm the diagnosis and suggestan underlying cause. Once patientshave been identified they can bedirected to the appropriate cardiacor HF ward, where this is notcurrently available aiming to clusterHF patients onto the same wardshould be a priority. Where there aremultiple problems or major co-morbidities the patient can receiveshared care on a medical or care ofthe elderly ward.
Rapid identification and assessmentat the front end of the hospital mayalso make it possible to avoidadmission for some patients, withthe Acute Heart Failure Nurse(AHFN) adjusting treatment andarranging early follow up with thecommunity HF nurse (CHFN).
(ii) Identification of patients on the wardsThe reality of the current situation isthat in many hospitals HF patientsare scattered throughout the wards.Access to serum NP for in-patientsremains infrequent, and so whereHF is suspected from the clinical
Identifying patients admitted with heart failure
3. Identification of heart failure in patients
a.Serum NP and early inpatient echob.Management in dedicated area with expertise – Junior docs/nursesc.Close liaison/collaborative working with community over discharge planning
d.Discharge with a care management plan
In April 2009, West Herts Hospital introduced an integrated HFpathway in which patients received urgent serum NP testing onadmission, followed by rapid access to echo. Daily cardiologyward rounds were then organised to advise on these patientsand optimise treatment and this lead to a significant reduction inreadmissions.
Serum NP testing also helped identify patients admitted underanother specialty, reducing the time nurse specialists spentlocating patients and reducing unnecessary echo’s.
Readmissions
picture, in-patient echocardiographyis usually requested. Referral forechocardiography without serum NPscreening can often overwhelm in-patient capacity and delays indiagnosis ensue. This inevitablydelays definitive treatment plansand prolongs hospital stay.
Cost of bed days saved = £69,000. Cost of providing serum NP = £38,800.Overall saving of £30,200 in one year.

www.improvement.nhs.uk/heart
A guide for review and improvement of hospital based heart failure services 9
In this situation, the role of theAHFN specialist is critical. They needto make sure that all patients areknown to the HF team and receiveinput from the HF consultant. Oftenthis requires "trawling" of thewards which is time consuming,although providing a "hotline" forwards to inform the AHFN ofsuspected patients can reduce theworkload. Additionally some formof alert system via the hospital ITsystem which is activated whenknown HF patients are admitted isalso useful.
Although inevitably this system ismore fragmented and timeconsuming than option (i), onceidentified by the AHFN, patients canreceive appropriate input to theirmanagement and discharge can befacilitated via discussions with theCHFN.
Questions you might consider: • Are there a high percentage of patients presenting with NYHA class 4? (NYHA explained - www.abouthf.org/questions_stages.htm).
• Are the patients presenting to A&E new presentations, or knownHF patients decompensating?
• Should the patient be presenting earlier/elsewhere?
• Once admitted, is the process geared towards rapid diagnosis?
• Is serum NP used as a predictor to enable patients to enter the correct pathway at the door?
• Is echocardiography available within 24hours of admission/ positive serum NP?
Specialist assessmentOnce identified, all patients shouldbe assessed by the HF specialistteam (consultant/nurse) as early aspossible in their admission, to makeappropriate management plans.Subsequent input from the HF teamcan then be stratified according toclinical status i.e. severity ofpresentation (new patients) ordeterioration (previously diagnosedpatients).
Acute managementThe more severely unwell patientsusually require complex treatmentregimes which include intra venous(IV) diuretics - either by intermittentinjection or by continuous infusion.Daily assessments of these patients,is essential to ensure appropriatefluid loss without excessiveimpairment of renal function, orelectrolyte imbalance. In the currentsystem in the NHS where juniormedical staff, frequently changefirms, experienced nursing staffhave a major role to play inmonitoring the patients during thisstage. The HF specialist should beavailable for advice on a daily basis.When the patient is not on a cardiacward, the AHFN is ideally placed toliaise between the HF specialist andthe ward staff.
Note: Redesign of the inpatientechocardiography service toprioritise these patients canhave a significant benefit onlength of stay. Definitivetreatment is often not institutedbefore echocardiographicconfirmation of diagnosis andthis is expensive for the NHSand potentially serious for thepatients. For further informationon how to calculate demandand capacity click here»
Note: Acute management isbest delivered on a cardiac orheart failure ward where thenursing and junior medical staff,are familiar with the protocolsand can respond tocomplications. This is likely tounderpin the improvement inmortality seen in the HF Auditfor patients managed on cardiacwards.

www.improvement.nhs.uk/heart
10 A guide for review and improvement of hospital based heart failure services
Discharge planningDischarge planning should begin assoon as the patient is admitted.Early discussion between the AHFNand the CHFN facilitates earlydischarge, without a prolongedperiod of observation afterconversion back to oral medication.Most of this communication cantake place by phone or email, but itis beneficial for the hospital basedand community HFN to meet on aweekly basis to discuss difficultmanagement problems with theconsultant lead, as part of the multi-disciplinary team.
Ideally the rehabilitation teamshould review the patients prior todischarge, in the same way thatpatients are assessed aftermyocardial infarction.
The content of the dischargesummary is also critical. Clear detailsof the treatment provided inhospital and plans after dischargeshould be included, including detailsof monitoring and follow uparrangements. Where the patientsare discharged on sub-optimal dosesof medication (e.g. ACE inhibitors)the reasons for this should be clearlyspecified, as should any requests forassistance from the GP/practicenurses with subsequent up-titration.
Questions you might consider :• Are heart failure patients admittedto different wards/specialties and are there differences in their readmission rate and/or length of stay?
• Are patients who are admitted to non cardiology wards referred for a specialist opinion and how long does this take to happen?
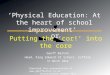
Appointment of an AHFN and concentration of HF patients ontwo wards has reduced in patient mortality in Hastings.
Concentrating HF patients on two wards - General Cardiology and Careof the Elderly Cardiology, with patients being identified by an acute HFN‘trawling’ medical assessment ward (without availability of serum NP),has resulted in a reduction in hospital mortality.
Mortality in hospital 1998-2009
y=4.2955x + 93.886R = -0.744

www.improvement.nhs.uk/heart
A guide for review and improvement of hospital based heart failure services 11
Multidisciplinary team workingA multidisciplinary team approach isuseful at all stages of the patientpathway. We have alreadyhighlighted the role of the HF teamin the management of in-patients.Regular MDT meetings (ideallyweekly) make discharge planningeasier for the more complicatedpatients, and also facilitatemanagement of patients in thecommunity (with the potential foravoidance of admissions).
Questions you might consider:• Do you have a team approach to heart failure management - if so, who makes up this team?
• Are there mechanisms in place and sufficient capacity for all inpatients with HF to be managedby the specialist team?
• Are MDT meetings taking place regularly between primary and secondary care?
Follow up arrangementsRapid follow up after earlydischarge greatly reduces the risk ofreadmission. All patients should beseen within a week of discharge,and this should include assessmentof fluid status (including weight)and renal function. Timelyintervention at this stage can oftenprevent patients becomingdehydrated and developingimpaired renal function oralternatively rapidly regaining theoedema they have lost in hospital.
This role is often best carried out bythe CHFN in the patients home, butwhere this service is not availablealternatives include hospital basedclinics run by the AHFN or practicenurses trained in HF.
Questions you might consider:• Is there sufficiently robust discharge planning including weekends so that patients are discharged at the earliest opportunity?
• Are patients educated in their condition to allow active participation in their care and are they confident about who to contact when things start to deteriorate?
• Are there out of hours patient support services comparable with the support available during working hours?
• Is the follow-up of inpatients designed to ensure that inappropriate readmissions are avoided?
• Is cardiac rehabilitation available for heart failure patients?
• Can patients be discharged early with confidence that they will be reviewed and have renal function checked within a week?
• Do community nurses have accessto hospital information systems tocheck results?
4. Multidisciplinary team working
a.Case management discussions across primary-secondary care interface - early discharge, admission avoidance - seamless service
b.Consultant lead/+GP/hospital HF nurse(s)/community HF nurse(s) etcc.Designated care co-ordination
Equity and inclusiveness
It is fundamental that the AHFN's work is not confined to the cardiacwards, nor to younger age groups. In the current situation where manypatients with HF are admitted to non-cardiac wards, it is these patientswho have the highest mortality. It is sometimes easier for the HF teamsto fall into the trap of delivering a very high quality service to a relativelysmall proportion of the in-patient population with HF, whilst a largergroup remain unsupported and without specialist input.
In addition all types of HF should be included in the service. Patientswith preserved ejection fraction (HFPEF) deserve identical input - and areoften more difficult to manage.

www.improvement.nhs.uk/heart
12 A guide for review and improvement of hospital based heart failure services
5. Supportive and palliative care
a.Unnecessary admission avoidance at end of life - preferred priorities of care
b.Palliative care involvement
Supportive and palliative care
Supportive and palliative, alsosometimes referred to as ‘End oflife' care helps all those withadvanced, progressive and incurableconditions to live as well as possibleuntil they die. It enables the needsof both patients and family to beidentified and met throughout thelast phase of life and intobereavement. It includes physicalcare, management of discomfortand other symptoms and theprovision of psychological, social,spiritual and practical support’
Experience from previous NHSImprovement national projects,shows that service providers oftenaddress process issues and servicedelivery before undertaking end oflife challenges. This may in part beattributed to the difficultiesassociated with the timing of anddelivery of end of life care.
NHS Improvement in conjunctionwith the national end of life careprogramme team published a HeartFailure end of life implementationframework in July 2010. To viewthis document click here»
The key messages highlight:• The disease trajectory for a heart failure patient is not easily predictable, and therefore also timing of EOL care plans
• Advance care planning supports patient wishes about their future care arrangements and whilst it is sometimes a difficult subject to broach is often left too late
• Well structured multidisciplinary team working is essential for individualised, flexible patient centred care
• Excellent communication betweenhealth professionals, patients and carers is fundamental to a good patient experience
• Most people but not all prefer notto die in hospital, however this is where many people do die.
Whilst this resource focuses on theinpatient service a large onlinecollection of work covering thewhole patient pathway,commissioning QIPP and qualitystandards can be found here»
NHS improvement would like toacknowledge and thank all theteams who have willingly sharedtheir experiences for the benefit ofothers. This is an evolvingimprovement resource which doesnot claim to have all the answers.We would welcome feedback andany additional information duringthe draft release of this document.
Please email these [email protected] 30 September 2011.

www.improvement.nhs.uk/heart
A guide for review and improvement of hospital based heart failure services 13
Appendix 1 Checklist for a service review
The checklist below describes thekey elements of a simple servicereview
1. Engage key stakeholders2. Baseline the current service provision
3. Share baseline with key stakeholders
4. Map out the service steps (process map)
5. Prioritise and plan improvementswith key stakeholders
6. Implementation and reassessment
7. Sustained best practice
• Continuous communication is imperative at all times between allkey stakeholders, especially wherethere is patient hand over between heath care professionals or organisational boundaries.
Appendix 2Key sources of information
There are several important sourcesof information and guidance forheart failure service providers whichshould be utilised when undertakinga service review:
• The National Heart Failure audit 2010 - This provides national comparative data to help clinicians and managers improve the quality and outcomes of their services - click here»
• NICE clinical guidance 108 - Chronic heart failure: management of chronic heart failure in adults in primary andsecondary care - This offers evidence-based advice on the careand treatment of people with chronic heart failure, with updated recommendations on diagnosis, pharmacological treatment - click here»
• NICE quality standards – Chronic heart failure – (to be published June 2011)There are a series of evidence based concise statements that show what high-quality care should look like.
• The British Heart FoundationA charitable organisation providing amongst other things resources for both professionals and patients - click here»
• Commissioning – NHS Improvement quick guide to commissioning the heart failure whole pathway of care - click here»
The codes commonly associatedwith heart failure are listed below.To review local information notethat Heart Failure as a diagnosis canbe entered as the primary orsubsequent diagnosis. We wouldsuggest initially reviewing data withheart failure as the primarydiagnosis.
• I50.0 Congestive heart failure • I50.1 Left ventricular failure • I50.9 Heart failure, unspecified • I11.0 Hypertensive heart disease with (congestive) heart failure
• I42.0 Dilated cardiomyopathy • I25.5 Ischaemic cardiomyopathy • I42.9 Cardiomyopathy, unspecified.

14 A guide for review and improvement of hospital based heart failure services
www.improvement.nhs.uk/heart

Dr David WalkerConsultant Cardiologist, Hastings and Rother NHS Trust and NHS Improvement National Clinical Leademail: [email protected]
Elaine KempNational Improvement Lead, NHS Improvement email: [email protected]
Sheelagh MachinDirector, NHS Improvement - Heart email: [email protected]
Contacts

NHSNHS Improvement
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
©NHS Improvement 2011 |All Rights Reserved
Publication Ref: IMP/comms019 - June 2011NHS Improvement3rd Floor | St John’s House | East Street | Leicester | LE1 6NB
Telephone: 0116 222 5184 | Fax: 0116 222 5101
www.improvement.nhs.uk
NHS Improvement
NHS Improvement’s strength and expertise lies in practical service improvement. It has over adecade of experience in clinical patient pathway redesign in cancer, diagnostics, heart, lung andstroke and demonstrates some of the most leading edge improvement work in England whichsupports improved patient experience and outcomes.
Working closely with the Department of Health, trusts, clinical networks, other health sector
partners, professional bodies and charities, over the past year it has tested, implemented, sustained
and spread quantifiable improvements with over 250 sites across the country as well as providing
an improvement tool to over 800 GP practices.
Delivering tomorrow’simprovement agenda for the NHS