Embed Size (px)
Citation preview

J. Behav. Thu. & Exp. Psvchior Vol. 25, No. 4, pp. 31 I-316, 1994. 0 1994 Elsaxr Science Ltd
Printed in Great Britam. All nghts reserved 000%7916/94 $7.00 + 0.00
Pergamon
00057916(94)00054-9
DIFFERENCES BETWEEN CLINICAL AND NURSING INPATIENT STAFF: IMPLICATIONS FOR TRAINING IN BEHAVIORAL REHABILITATION
PATRICK W. CORRIGAN
University of Chicago Center for Psychiatric Rehabilitation
Summary - Line-level staff have been trained in behavioral rehabilitation strategies by program developers who believe that this training may lead to better quality of inpatient care. The effects of staff training, however, may be mitigated by characteristics of the various disciplines that constitute the staff. Differences in nursing versus clinical staff may be particularly relevant to inpatient staff training in behavioral rehabilitation. To identify these differences, 80 clinical and 210 nursing staff members at a state hospital completed measures of work-related stress, knowledge of behavior therapy, and impressions of behavioral interventions. Results showed that clinical staff had significantly more formal education and knowledge of behavioral treatment. Nursing staff reported greater work-related stress. Despite these differences, the two samples did not differ in terms of commitment to social learning ideology or perceptions of barriers to behavior therapy. Moreover, the pattern of staff variables that predict social learning ideology or perceptions of barriers to behavior therapy was similar across samples. The impact of differences in clinical and nursing staff on staff training is discussed.
Behavioral rehabilitation, when combined with medication therapies, has been shown to have a significant impact on the course of severe mental illness (Liberman, Corrigan, & Schade, 1989). Particularly useful rehabilitation strategies include the token economy (Ayllon & Azrin, 1968; Paul & Lentz, 1977), psychosocial skills training (Bellack, Turner, Hersen, & Luber, 1984; Wallace & Liberman, 1985), and behavior family management (Anderson, Reiss, & Hogarty, 1986; Falloon, Boyd, & McGill, 1984). Inpatients who participate in these interventions tend to show significant reductions in psychiatric symptoms and marked improvement in social functioning. Unfortunately, few inpatients units regularly incorporate behavioral rehabilitation interventions into their day-to-day treatment armamentarium despite these successes (Boudewyns, Fry, & Nightingale, 1986; Corrigan, MacKain, & Liberman, 1984; Hall & Baker, 1986).
Recently, investigators have identified organizational barriers that impede the implementation of behavioral rehabilitation in inpatient settings (Backer, Liberman, & Kuehnel, 1986; Emerson & Emerson, 1987). Foremost among these barriers are staff-related obstacles;
e.g., many line-level clinicians are not knowledgeable about general principles that govern behavioral rehabilitation (Bernstein, 1982; Repucci & Saunders, 1974). Furthermore, inpatient staff may experience excessive work- related stress that undermines the faithful implementation of rehabilitation strategies (Corrigan, Kwartarini, & Pramana, 1992).
Staff-related barriers might be at least partially diminished by training line-level staff on the specific steps required to carry out rehabilitation programs (Anthony, Cohen, & Farkas, 1987; Liberman et al., 1982; Rogers et al., 1986). Staff training strategies include discussion of basic
Requests for reprints should be addressed to Patrick Corrigan, University of Chicago Center for Psychiatric Rehabilitation, 7230 Arbor Drive, Tinley Park, IL 60477, U.S.A.
311

312 PATRICK W. CORRIGAN
information regarding major mental illness and social learning, behavioral rehearsal of specific training skills (e.g., staff members modeling the subtleties of basic conversation skills), and ongoing consultation to address the problems that line-level staff may encounter when actually implementing these rehabilitation strategies. In addition to educating staff members about rehabilitation principles, training helps staff develop cogent programs that reduce the level of on-unit chaos and subsequently, staff stress.
The impact of staff training will probably vary with the educational background and duties of staff disciplines for whom training is provided; e.g., psychologists familiar with learning theory may learn and implement behavioral rehabilitation strategies more quickly than psychiatrists whose perceptions of severe mental illness are dominated by a medical model. Differences in two groups of line-level staff - nursing and clinical staff - may be particularly relevant to the effects of staff training and program development on the psychiatric inpatient unit (Donat & McKeegan, 1990; Wilkinson, 1973). These two groups tend to form distinct components of the treatment team on many settings. Nursing staff includes the registered nurses, licensed practical nurses, and psychiatric technicians who are responsible for the moment-to-moment management of living conditions on the unit. Clinical staff is a more heterogeneous group including activity therapists, social workers, psychologists, and psychiatrists who tend to be responsible for the more therapeutic endeavors of the unit.
Differences between these groups that affect staff training on rehabilitation strategies may arise from several sources including educational backgrounds. Clinical staff tend to have completed more formal education than nursing staff, including specific introduction to behavioral principles. Therefore, clinical staff are likely to have greater knowledge about behavioral interventions. Differences may also arise because of the pattern of interactions each group has with patients. Nursing interactions with patients tend to be incessant throughout the day because their work space is located on the unit with the patients.
Moreover, nursing staff are more likely to work evening/night shifts where they may be exposed to the problems that occur when staff-patient ratios are lower. Clinical staff tend to have more controlled interactions with patients because they have off-unit offices to where they can withdraw (Emerson & Emerson, 1987; Sullivan, 1989). As a result, nursing staff are more likely to report greater stress associated with work.
In this study, we examined the manner in which differences in educational background and work- related stress relate to staff attitudes about behavioral rehabilitation on their units. Little information has been found in the literature regarding differences in staff subgroups even though several studies have examined these hypotheses on inpatient staff as a whole (Edelson & Paul, 1976; Ellsworth, 1965; Moos, 1972). Our group conducted one of these more genera1 studies where staff variables were collected on 332 inpatient staff members (Corrigan, Kwartarini, & Pramana, 1992; Corrigan, in press). These data are reexamined in the study described in this paper to look for clinical versus nursing staff differences.
Methods
Staff members of Camarillo State Hospital and Developmental Center (CSHDC) completed an extensive written survey assessing their perceptions of issues related to clinical practice and behavioral rehabilitation. Survey participants reported age, gender, education, job title (e.g., psychiatrist, nurse, psychiatric technician, recreational therapist, social worker), and number of years employed at the facility. They also reported previous training experiences with behavior therapy by providing total number of classes or conferences they had attended on behavior therapy or modification. In addition, participants completed four standardized instruments:
(I) Behavior Vignettes Test (BVT). Participants read 20 clinical problems and chose the correct
Clinical and Nursing Staff
intervention from four multiple choice options the 18 items has good (Heifetz, Baker, & Pease, 1981). This test has test-retest reliability. been used extensively to assess a subject’s knowledge of behavioral treatment strategies. (4) Social Learning
313
internal consistency and
Ideology Subscale of the
Opinions of Mental Illness (OMI) Test. Subjects (2) Inpatient Job Stress Questionnaire (ZJSQ). rated their agreement with nine items that
Subjects completed nine items that measured represented staff members’ acceptance of social inpatient staff stressors. Scores from these items learning principles (Paul & Lentz, 1977). were combined to yield two internally consistent factors: stress that results from administrative issues and from clinical practice (Browner et al., Results 1987; Corrigan, 1993).
Eighty members of the clinical staff and 210 (3) Barriers to Implementation of Behavior members of the nursing staff completed the survey
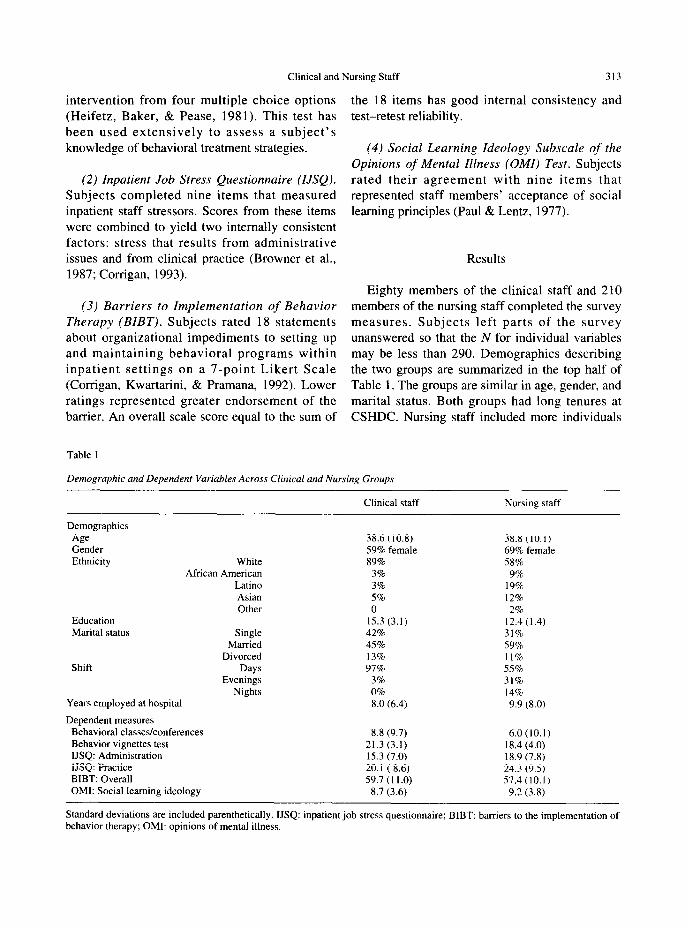
Therapy (BZBT). Subjects rated 18 statements measures. Subjects left parts of the survey about organizational impediments to setting up unanswered so that the N for individual variables and maintaining behavioral programs within may be less than 290. Demographics describing inpatient settings on a 7-point Likert Scale the two groups are summarized in the top half of (Corrigan, Kwartarini, & Pramana, 1992). Lower Table 1. The groups are similar in age, gender, and ratings represented greater endorsement of the marital status. Both groups had long tenures at barrier. An overall scale score equal to the sum of CSHDC. Nursing staff included more individuals
Table I
Demqgraphic and Dependent Variables Across Clinical and Nursing Groups
Clinical staff Nursing staff
Demographics
Age 38.6 (10.8) 38.8 (10.1) Gender 59% female 69% female Ethnicity White 89% 58%
African American 3% 9% Latin0 3% 19% Asian 5% 12% Other 0 2%
Education 15.3 (3.1) 12.4(1.4) Marital status Single 42% 31%
Married 45% 59% Divorced 13% 11%
Shift Days 97% 55% Evenings 3% 31%
Nights 0% 14% Years employed at hospital 8.0 (6.4) 9.9 (8.0)
Dependent measures Behavioral classes/conferences 8.8 (9.7) 6.0 (10.1) Behavior vignettes test 21.3 (3.1) 18.4 (4.0) IJSQ: Administration 15.3 (7.0) 18.9 (7.8) IJSQ: Practice 20.1 ( 8.6) 24.3 (9.5) BIBT: Overall 59.7 (1 I .O) 57.4 (10.1) OMI: Social learning ideology 8.7 (3.6) 9.2 (3.8)
Standard deviations are included parenthetically. IJSQ: inpatient job stress questionnaire; BIBT: barriers to the implementation of behavior therapy; OMI: opinions of mental illness.
313 PATRICK W. CORRIGAN
from nonwhite ethnic groups (x2 = 19.96, p < .OO I ) and worked shifts other than days more often than clinical staff (x? = 44.68, p < .OOOl). As expected, the clinical group had completed significantly more years of formal education [F( 1.275) = I 10.2, p < .OOOl ].
Means and standard deviations of the dependent measures in the survey are also included in Table 1. A oneway MANOVA testing for differences in these variables between groups was significant [F(7.137) = 3.52, p < .005]; however, only 137 subjects completed all dependent measures so the MANOVA represented data provided by less than half of the sample. Subsequent ANCOVA’s were conducted to determine between group differences across specific variables; education was included as a covariate in the analyses to assure that between group differences were not a function of difference in educational level. A Bonferroni adjustment to reduce the error associated with multiple tests yielded a more conservative alpha of ,005.
Nonsignificant trends were f.ound which suggested that the clinical group had attended more classes and conferences on behavioral principles [F(l,l89) = 3.26, p = .07]. Moreover, the clinical staff earned a far greater score on the BVT than the nursing staff [F(1,271) = 30.9, p < .OOOl]. Nursing staff reported more stressors on the job than their clinical counterparts. They earned higher scores on the Administration IF(l.245) = 10.8, p < 10.8, p < .OOl] and the Practice LF(1.245) = I 1.0, p < .OOI] Subscales of the IJSQ.
Despite differences in knowledge of behavior therapy and work-related stress, the two samples did not differ in terms of commitment to social learning ideology. No significant difference was found on this subscale of the OMI [F( 1,247) = 0.8, ns]. Similarly, the two groups did not differ on BIBT overall scores [F( 1,207) = 2.4, ns].
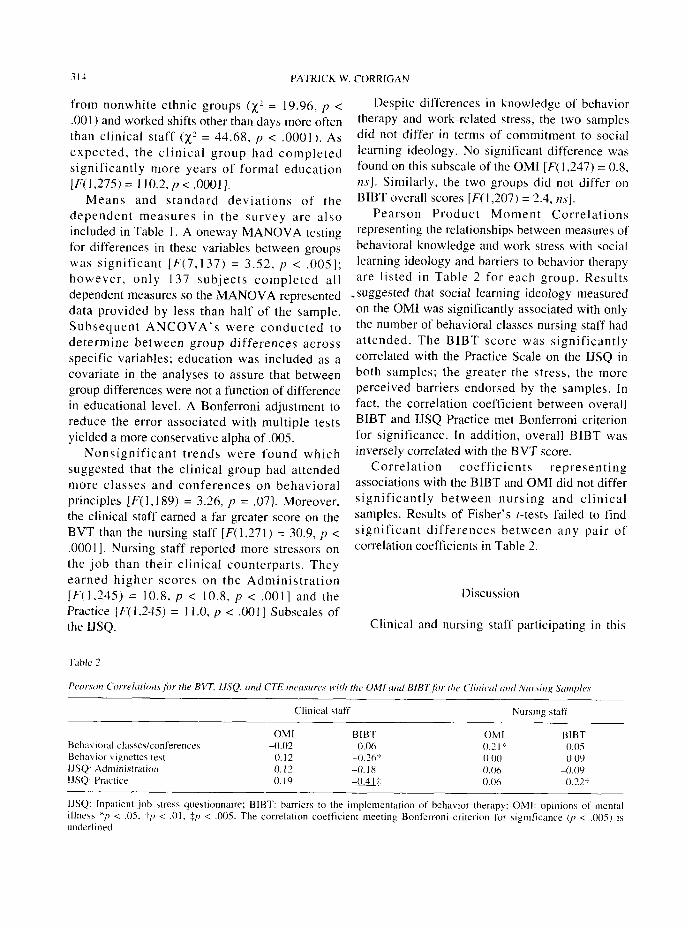
Pearson Product Moment Correlations representing the relationships between measures of behavioral knowledge and work stress with social learning ideology and barriers to behavior therapy are listed in Table 2 for each group. Results
-suggested that social learning ideology measured on the OMI was significantly associated with only the number of behavioral classes nursing staff had attended. The BIBT score was significantly correlated with the Practice Scale on the IJSQ in both samples; the greater the stress, the more perceived barriers endorsed by the samples. In fact, the correlation coefficient between overall BIBT and IJSQ Practice met Bonferroni criterion for significance. In addition, overall BIBT was inversely correlated with the BVT score.
Correlation coefficients representing associations with the BIBT and OMI did not differ significantly between nursing and clinical samples. Results of Fisher’s t-tests failed to find significant differences between any pair of correlation coefficients in Table 2.
Discussion
Clinical and nursing staff participating in this
Clinical staff NurGng staff
OMI BIBT OMl BIBT Bchacioral classes/conference\ -0.02 4.06 0.7 I ‘i 0.05 Bcha ior \ ignctte\ test 0.12 -0.36’~ 0.00 0.09 JJSQ: Administration 0. I2 -0.18 0.06 4.09 IJSQ: Practice 4.19 -0.41;: 0.06 -02t
IJSQ: Inpatient job \tress questionnaire; BIBT: barriers to the implementation of behavior therapy: OMI: opinion\ of mental illneu */J < .05. tP < .Ol, $I> < ,005. The correlation coefficient meeting Bonferroni criterion for Ggnificance (I, < ,005) i\ underlined.

Clinical and Nursing Staff 31s
study varied in knowledge about behavioral rehabilitation and work-related stress. In particular, findings from this study showed that clinical staff had completed more formal class work; nonsignificant trends also suggested that they had more formal behavioral training. Clinical staff also showed greater knowledge about behavior therapy as measured on the BVT. Nursing staff reported more on-the-job stress related to administrative issues and to clinical practice. They were also more likely to work shifts other than days. These differences did not seem to be attributable to disparities in educational levels
across groups. Despite these disparities, the clinical and
nursing groups did not differ significantly in ideological perception of social learning principles. The two groups showed similar beliefs about the efficacy and relevance of behavioral rehabilitation for this patient population as measured on the OMI subscale. Moreover, the groups did not deviate in terms of perception of barriers to behavior therapy. These findings suggest that nurses will be about as receptive to training in behavioral rehabilitation as clinical staff even though the latter group received more formal training in behavioral interventions.
Further analyses sought to identify individual staff characteristics that predicted social learning ideology and barriers to behavior therapy in each job group. Results suggested that social learning ideology was relatively independent of most of these staff characteristics. Only familiarity with behavior therapy in the nursing sample, represented by number of completed classes and conferences, was found to be associated with social learning ideology. This finding suggests that nurses and psychiatric technicians who do not endorse a social learning ideology are likely to change their beliefs as they participate in staff training on behavioral rehabilitation.
Results also showed that both groups were likely to perceive potent barriers to behavior rehabilitation when they were more stressed 6n the job. Hence, program developers must address work-related stressors if they hope to diminish obstacles that may impede starting up new
rehabilitation programs on a psychiatric unit. Changing staff stressors and receptivity to behavioral rehabilitation is likely to be a reciprocal process. Staff members are frequently stressed because they view the unit as chaotic and out of control. Therefore, development of more potent rehabilitation programs may help staff members to regain this control and diminish their sense of
work-related stress. The two groups did not seem significantly to
differ in terms of staff characteristics that predicted social learning ideology or perceived barriers to behavior therapy. Therefore, the overall findings from this study suggested that staff from either clinical or nursing disciplines should be equally willing to participate in training on behavioral rehabilitation. The clinical staff’s superior knowledge about behavior therapy suggests that they may more easily grasp key concepts. However, staff from both groups are equally likely to champion these concepts towards development of an effective intervention program.
Although groups were similar in their overall view of behavioral rehabilitation, they are likely to differ in identifying relevant content areas to be included in staff training. For example, nursing staff in this study were more likely to be stressed by overly active treatment environments. Therefore, nursing staff are more likely to be interested in intervention programs like the token economy that promote control over the milieu. Perhaps clinical staff who are relatively aloof from the press of the unit milieu will express interest in more habilitative interventions like skills training. Professionals conducting staff training need to be attentive to the possible deviations in program agenda across staff groups when developing a training plan for line-level professionals.
Ac~no~,led~~eme,,fs - The author wishes tu acknowledge the assistance of Brett Buican. who helped to prepare thi\ manuscript, and Roberto Karate who provided a cogent review.
References
Anderson, C. M.. Reisr, D. J.. & Hogarty, G. E. (1986). Schi~ophrmia and thr,fami/y. New York: Guilford Press.

316 PATRICK W. CORRIGAN
Anthony, W. A., Cohen, M., & Farkas, M. (1987). Training and technical assistance in psychiatric rehabilitation. In A. Meyerson (Ed.), Psychiatric disahilitv: clinical, administrative and legal aspects. Washington, DC: American Psychiatric Association.
Ayllon, T.. & Azrin, N. (1968). The token economy: a moti~~ationul system for therapy and rehabilitation. New York: Appleton-Century-Crofts.
Ellsworth, R. B. (1965). A behavioral study of staff attitudes toward mental illness. Journal qf Abnormal Psychology, 70, 194-200.
Backer, T., Liberman, R., & Kuehnel, T. (1986). Dissemination and adoption of innovation psychosocial interventions. Journal o,f Consulting and Clinical Psychology, 54, 111-118.
Bellack, A. S., Turner, S. M., Hersen, M., & Luber, R. F. (1984). An examination of the efficacy of social skills training for chronic schizophrenic patients. Hospital and
Community Psychiatry, 35, 1023-1028. Bernstein, G. (1982). Training behavioral change agents: a
conceptual overview. Behavior Therapy, 13, l-23. Boudewyns, P., Fry. T., & Nightingale, E. (1986). Token
economy programs in VA medical centers: where are they today? Behavior Therapist, 6, I26 127.
Browner, C. H., Ellis, K. A.. Ford, T.. Silsby, J.. Tampoya, J.. & Yee, C. (1987). Stress, social support, and health of psychiatric technicians in a state facility. Mental Retardation, 25, 31-31.
Emerson, E., & Emerson, C. (1987). Barriers to the effective implementation of habilitative behavioral programs in an institutional setting. Mental Retardation, 25, 101-106.
Falloon, 1. R. H., Boyd, J. L., & McGill, C. W. (1984). Family care of schizophrenia. New York: Guilford Press.
Hall, J. & Baker, R. (1986). Token economies and schizophrenia: a review. In A. Kerr and P. Smith (Eds.), Contemporary issues in schizophrenia. London: Royal College of Psychiatrists-Gaskell.
Heifetz, L. J., Baker, B. L., & Pease, L. A. (1981). Behavioral vignettes test. Cambridge, MA: Educational Projects.
Liberman, R. P., Corrigan, P. W., & Schade, M. L. (1989). Drug and psychosocial treatment interactions in schizophrenia. International Review, of Psychiatry, I, 283-294.
Liberman, R. P., Eckman, T. et al. (1982). Dissemination of new behavior therapy programs to community mental health programs. American Journal of Psychiatv, 139, 224-226.
Moos, R. H. (1972). Size, staffing, and psychiatric ward treatment environments. Archives qf General P.yychiatv, 26, 414-418.
Corrigan, P. W. (1993). Staff stressors at a developmental center and state hospital. Mental Retardation, 31, 234-238.
Corrigan. P. W., Kwartarini, W. Y.. & Pramana, W. (1992). Staff perception of barriers to behavior therapy at a psychiatric hospital. Behavior Modification, 16, 132-144.
Corrigan, P. W., MacKain, S. J., & Liberman, R. P. (1994). Skills training modules: a strategy for dissemination and utilization of a rehabilitation innovation. In J. Rothman & E. Thomas (Eds.), Intervention research (pp. 3 17-352). Chicago: Hayworth Press.
Paul, G. L., & Lentz, R. J. (1977). Psychosocial treatment of chronic mental patients: milieu versus social learning programs. Cambridge, MA: Harvard University Press.
Repucci, N.. & Saunders, J. (1974). Social psychology of behavior modification: problems of implementation in natural settings. American Psychologist, 2Y, 649-660.
Rogers, E. et al. (1986). Training mental health workers in psychiatric rehabilitation. Schi;ophrenia Bulletin. 12. 709-719.
Donat, D. C., & McKeegan, G. F. (1990). Behavioral knowledge among direct care staff in an inpatient psychiatric setting. Behavioral Residential Treatment, 5, 95-103.
Edelson, R. I., & Paul, G. L. (I 976). Some problems in the use of “attitude” and “atmosphere” scores as indicators of staff effectiveness in institutional treatment. Journal qf Nervous und Mental Diseuse, 162. 248-257.
Sullivan, I. G. (I 989). Burnout: a study of a psychiatric center. Loss. Grief and Care, 3, 83-93.
Wallace, C. J., & Liberman, R. P. (1985). Social skills training for patients with schizophrenia: a controlled clinical trial. Psychiatry Research. 15. 239-247.
Wilkinson. G. (1973). Interaction patterns and staff response to psychiatric innovations. Journal of Health and Sociul
Behavior, 14, 323-329.





























