Embed Size (px)
Citation preview
Different Forms of Migraine in Childhood and Adolescence: Notes on PersonalityTraits
G. Lanzi, U. Balottin, R. Borgatti, M. Guderzo and E. Scarabello
Division of Child Neuropsychiatry of Neurological Institute 'Fondazione C. Mondino", University of Pavia.
Reprint requests to: Prof. Giovanni Lanzi, Fondazione C. Mondino, Cattedra di Neuropsichiatria Infantile, ViaPalestro 3, 27100 Pavia, Italy.
This work was in part presented at third Congress of the International Headache Society; Florence-September22-25, 1987.
Accepted for Publication: July 19, 1988
SYNOPSISThe present study was proposed to explore the association between specific psychopathological factors and
the different types of migraine.
15 subjects with classic migraine (7 males and 8 females; avg. age 14.9), 15 subjects with common migraine (5males and 10 females; avg. age 10.5) and 15 subjects with chronic daily headache (8 males and 7 females; avg.age 11.3) were examined.
The psychological study of each of them was performed through individual interviews, psychodynamic testingand parental conferences in order to study the individual's personality in a dynamic fashion.
With the same modalities 29 normal subjects were also studied (11 males and 18 females; avg. age 11.3).
In the remote clinical histories of migrainous subjects the authors found: psychosomatic disturbances in ahigh percentage of cases (70% in classic and common migraine; 72% in chronic daily headache; 27% in controlsubjects: F = 7.3 p< 0.01); the presence of a psychologically important event directly associated with the onset ofthe disease (55% for chronic daily headache, 31% for classic migraine, 27% for common migraine}.
As regards the results of statistical analysis of some of the most objective parameters of the Rorschach theauthors found: the number of responses of human movement (M) were significantly lower in headache patients,while popular responses (P%), spaces response (S%) and Dr % responses worn in higher percentage incomparison with control. The headache patients also showed significant deceases of F+% and extended F+%while kinesthetic shock and K-type responses were significantly present.
The authors conclude that in migrainous subjects there is a contact with reality which is uninvolvedemotionally, and detached, with prevalently rationalized and intellectualized modalities that correspond to theneed of blocking the emergence of emotional phantoms.
(Headache 28:618-622, 1988)
One of the most fascinating problems in the study of migraine or essential headaches in general, concerns therelationships among the clinical forms presented. Certain authors still believe that in reality there exist "many forms ofmigraine", and that behind each clinical entity hides a diverse and peculiar pathology; its neurochemical origin justifies not onlythe symptoms, but also its pharmacological sensitivity.'
Other authors, for example, Appenzeller and Raskin,2 and ourselves,3 maintain that, on the other hand, only one clinicalentity is present, which expresses itself in forms differing in type and severity. According to this line of thought, the variedmodalities of clinical expression of migraine are distributed along a continuous spectrum which includes complicatedmigraine, the classic and common forms of migraine, in addition to muscular tension headaches and chronic dallyheadaches.
This topic has found new support from the recent discoveries of Olesen and Lauritzen,4,5 who have demonstrated that inclassic migraine, there are alterations of cerebral blood flow which are not found in common migraine. Also recentlydocumented in Headache, 1985, is the lively discussion of this subject between Wilkinson6 and Olesen.7 We fully agree withWilkinson when she underlines the affinities in origin which give a common etiology to both common and classic migraine. Topoint out a fact, also made by Wilkinson, the same patient may manifest in close temporal sequence different clinical forms ofmigraine, which at times may also be contemporaneous. We have already noted in our past studies how, between a phase ofcommon and classic migraine, there may be delineations present such as family grief, a separation or divorce of parents.
On the other hand, there are traditional authors such as Vahlquist,8 Wolff,9 Friedman,10 and others, who for decadesunderlined the existence and importance of the relationships between migraine, other essential headaches andpsychopathologic factors. Friedman,10 in 1950, wrote that "in migraine, as also in other forms of chronic headache, a varietyof conflicts and unconscious needs may have pathogenetic value." More recently (1980), the same author11 reaffirms that"among the various types of
headache largely attributable to emotions, migraine, muscular-tension headache, psychogenic headacheand its varied combinations, are all included."
Even though these concepts are now, on the whole, accepted by many, the explanation still remainsobscure as to why a child or adolescent develops a chronic daily headache rather than a common or classicform of migraine. Possible explanations could include a diverse neurobiological constitution orneuroendocrine alterations associated with a deficit in the equilibrium of different neurotransmitters, whichcould be observed in one subject rather than another. In addition to these possible etiologic factors for theclinical forms of headache, one should also consider, that in a biologically predisposed individual, a differentpersonality type and a different quality of interpersonal relationships may be other etiologic factors involved.
It is known that in the child, referring to the concepts of Anna Freud,12 there is a facilitated access betweenthe psyche and the body, and vice versa. This can explain why early in life, somatic and psychologicalprocesses are not separate; for example, a bodily excitation can be released through mental processes orvice versa. Further development of the Ego by time, brings on the formation of new and purely psychologicalmodes of release through thought and language. As noted by Anna Freud, when this harmoniousdevelopment of the Ego does not occur, there is a direct justification for "the gamut of psychosomaticsymptoms: asthma, eczema, ulcerative colitis, headaches, migraine".
In this present study, we are concerned with ages which do not include the first months or years of life, butthose ages of the latent period, of puberty or adolescence. These are ages in which it is possible to observeregressions to modalities of thought operations which are characterized by a partial or prevalent tendencytowards somatization. This makes possible the consideration that the further development of the Ego and thecorrelated "opening of new psychological modes of release through thought and language", occurs in anincomplete and nonharmonious fashion. In other words, a deficit is created in an area of the Ego necessaryfor symbol formation, and therefore, a tendency is created that utilizes regressive modes of archaic andpremental reactions which leads to somatization of emotional drives. This is what is believed to occur inchildren suffering from migraine or essential headaches in general. It is of note that in these. subjects thequality or type of certain emotions, in particular anger related to narcissistic frustration, can no longer bethought of or perceived by him (due to Ego, which at times presents with defects in thought processes).
Our previous studies,23,14 have underlined how children with migraine present with a high level of Egoinhibition, in reference to the fantasy and emotional aspects and the capacity for empathetic identification.This is confirmed both by certain characteristics which emerge from the interviews and observations, and alsoby peculiar elements perceived by Rorschach protocol. The main characteristic of this type of functioning, aswe have described previously and which is in accordance with the data proposed for several years by Marty,De M'Uzan, David,15 and the French school, is a mode of contact with the inner world, characterized by anon-emotional involvement, by a particular impoverishment of fantasy, and by detachment with prevalentmechanisms of rationalization and intellectualization. This mode of contact with mental objects has beendescribed as "relation blanche", ie., characterized by extreme impoverishment of fantasy aspects andprevalence of a pathological sense of concreteness and reality.
Our synthesis considers the peculiar psycho-pathologic aspects of the child or adolescent with migraine,the existence of which has been confirmed in these past years, but as our study of this topic grew, a newcuriosity was brought to our attention. We asked ourselves if within this relational structure that may bedefined as "blanche", there could also be other particularities and specific differences which would directlyjustify the various types of symptoms presented by the subject.
In effect, the literature does not lend support with previous studies for the presence of psychopathologicdifferences in classic migraine with respect to common migraine or chronic daily headache. It is also true that,in the past, ideas concerning the existence of psychogenic elements in subjects with chronic daily headachewere more accepted, whereas less so in subjects with migraine. A study done by Boag16 which revised theliterature, but which is now outdated, was published in the Handbook of Clinical Neurology and entitled"Psycho-genic Headache". He notes how patients with non-migrainous headaches are more self-aware ofconflictual situations and anxiety. Also, a very clear and specific correlation exists between headaches andstressful environmental situations; and thus the presence of headache is evidently advantageous secondarily,as a mode of self-perpetuation in the continuation of the disease itself. These patients, therefore, have apartial and limited deficit in their ability to symbolize and to confront themselves with their mental objects.
PERSONAL RESEARCH
Our study researches the peculiar psychopathologic differences among the three forms of essentialheadache: classic migraine, common migraine, and chronic daily headache.
We examined 15 subjects with classic migraine between the ages of 12 and 17 yrs, 8 mos. (avg. age14.9; s.d. 3.2), 7 males and 8 females; 15 subjects with common migraine between the ages of 7 yrs and 17yrs, 7 mos. (avg. age 10.5; s.d. 2.2), 5 males and 10 females; 15 subjects with chronic daily head-
ache between the ages of 6 yrs, 3 mos. and 17 yrs (avg. age 11.3; s.d. 3.8), 8 males and 7 females.
The age of onset of the headaches for the population with classic migraine was between 6 and 16 yrs (avg. age12.8; s.d. 2.5); with common migraine between 4 and 10 yrs (avg. age 7.3; s.d. 2.6); with chronic daily headachebetween 4 and 14 yrs, 6 mos. (avg. age 8.7; s.d. 3.5). The F value was equal to 8.10 (p<0.01), which indicates thatthe onset of classic migraine was later than common migraine or chronic daily headache. This does not reflect, inour point of view, a sampling error, since they represent peculiar clinical cases of the classic forms of headache.The literature, in fact, concordantly shows that the classic forms predominantly originate during adolescence, andthus, much later than the other forms.2
The diagnosis of headache was made in accordance with the diagnostic criteria of the Research Group onMigraine and Headache of the World Federation of Neurology. For the chronic daily headache we followed thedescription by Nappi and Savoldi from the book: Headache Diagnostic System and Taxonomic Criteria.1
The psychological study of each of our subjects was performed through individual interviews, psychodynamictesting (Rorschach, Blacky Pictures test, Thematic Apperception test, projective drawings, and the Wechslerscale), and parental conferences, in order to study the individual's personality in a dynamic fashion.
With these same modalities, 29 normal subjects were also studied: 11 males and 18 females between the agesof 6 yrs., 8 mos. and 16 yrs., 7 mos. (avg. age 11.3; s.d. 3.3).
The age differences between these subjects and headache patients were not statistically significant regardingthe age at observation (F = 3.83 n.s.).
Among the data collected by interviews and tests, we have taken into consideration certain psychologicalelements already seen as important by various authors, or which at least have had a significant role in the genesisof migraine.
On the remote clinical histories of our subjects, we found that a high percentage of cases (70% in classic andin common migraine; 72% in chronic daily headache; 27.2% in control subjects: F = 7.3 (p<0.01) presentedpsychosomatic disturbances indicative of an early problem in mother-child relationships, such as post-prandialvomiting and sleep disturbances in the first year of life, and recurrent abdominal pains, enuresis, and asthmaticbronchitis in later years.
We also carefully looked for, and found, in a high percentage of cases, the presence of a psychologicallyimportant event directly associated with the onset of the disease (55% for chronic daily headache, 31% for classicmigraine, 27% for common migraine). These values are not significantly different among themselves.
A substantial number of cases, before the onset of headache, reported the death of one or both parents, or of arelative psychologically important for the patient.
For example in one case when a child, suffering with common migraine, began to have complicated migraineafter the death of a maternal uncle with cancer, the mother was extremely worried about her child's health in whichshe identified her dead brother. The boy presented evident identification towards his uncle, while feeling irritatedfor the over-worrisome and suffocating behavior of his mother.
In other occasions, grievous events are less clearly recalled by family members during their consultation, andtherefore, more difficult to evoke. For example, a 13 yr. old girl came to our ambulatory clinic for an attack ofcommon migraine. Only after the third visit, did the father suddenly recall, that exactly 7 yrs. ago immediatelybefore the onset of her disease, the death of the maternal grandmother where the young child usually lived. Duringthe father's conversation, the child had an immediate emotional reaction, bursting into tears. This was thenmasked and negated by a forced laugh, which convinced us of the still vivid presence of the grandmother in thechild's mind. Problems may now arise concerning a correct use of empathetic listening in order to elicit from thesepatients their innermost experiences, and how, after many years, this incomplete grief reaction can occur.
In other cases, the psychologically precipitating factor is represented by the separation of parents, and here wecan also cite several examples. In general, we can say that a distinct variability of individual reactions andmechanisms more or less adaptive to a traumatic event exist. Each unwelcomed external event may assume apsychopathological value only in relation to the level of maturity achieved in the process of separation -individuation and the methods with which this is confronted by the subject.
Less frequently, both patients and their parents are conscious that a psychological factor underlies the origin ofa singular attack (23% in classic migraine; 54% in common migraine; 38% in chronic daily headache n.s.).
On these cases, conditions of repressed anger are almost always found. In general, they are closely tied to theEgo's inability to tolerate frustrations, as though there existed a sort of narcissistically fragile base. An 8 yr-old girlwith common migraine states: "1 get very angry with mother if, for example, she does not allow me to go shoppingor does not let me go to the playground or not let me cook or touch the stove because she is afraid somethingmight happen. I would like to learn how to cook by myself, because if mother lets me, at least I will learn and whenI grow up and get married... Many times I get very upset and do not say anything and then get a headache. I amafraid that mother will leave me
and never come back if I am a bad girl". The whole discussion may be interpreted as the difficulty the child feelswhen faced with separation and individuation while tolerating the absence of the object.
At other times the precipitating factor is seen as a state of apparently common emotional tension. For example,school-work may be the factor in those subjects already high achievers in school.
As for the other psychodynamic elements considered, a partially conscious form of identification with a parentmigraine sufferer has been noted in a high number of cases and is sometimes verbalized as: "Dad and I are alike... ".
While 45% of the subjects in all the populations studied could identify the precipitating factor of the crisis asrepressed anger, the description which most of the subjects use for their own character indicates a behavior ofrepressed aggression: the patients, in fact, describe themselves as "tranquil types" who try never to get angry, andif they do, are not able to manifest it.
Personality characteristics and psychopathologic dynamics of which we spoke emerged in the variouspsychodiagnostic interviews of the patients and their parents, as well as from results obtained from testingmaterials.
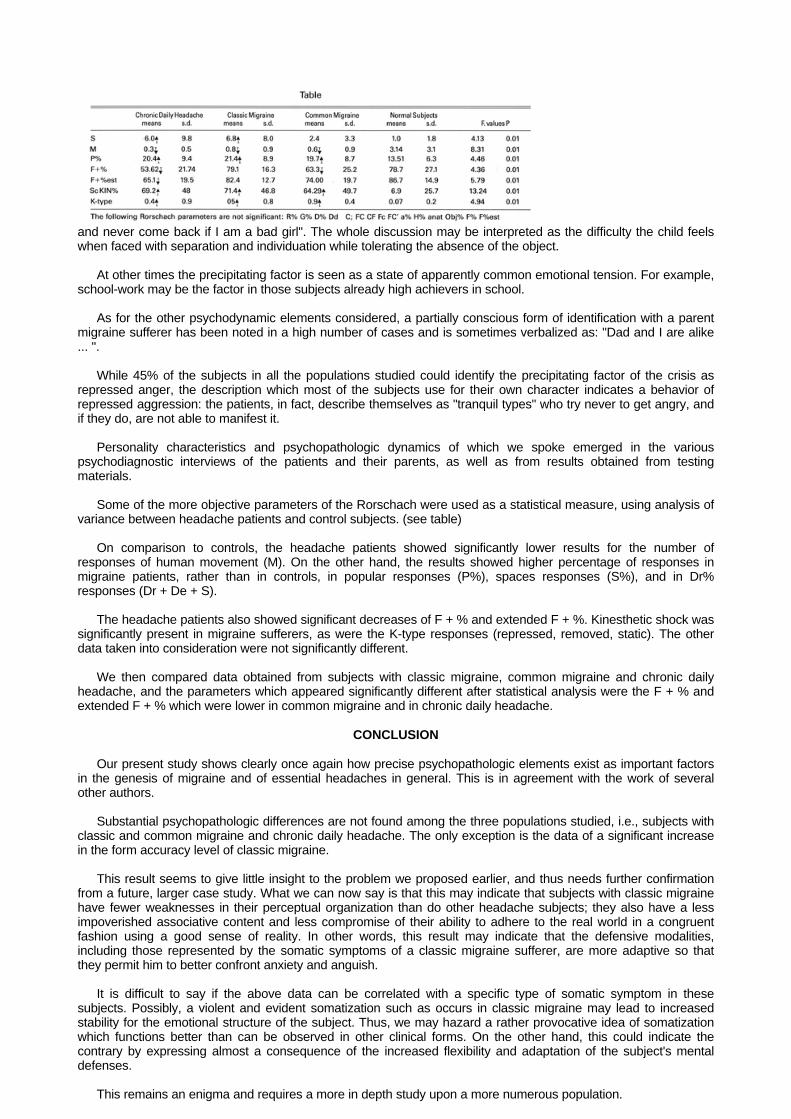
Some of the more objective parameters of the Rorschach were used as a statistical measure, using analysis ofvariance between headache patients and control subjects. (see table)
On comparison to controls, the headache patients showed significantly lower results for the number ofresponses of human movement (M). On the other hand, the results showed higher percentage of responses inmigraine patients, rather than in controls, in popular responses (P%), spaces responses (S%), and in Dr%responses (Dr + De + S).
The headache patients also showed significant decreases of F + % and extended F + %. Kinesthetic shock wassignificantly present in migraine sufferers, as were the K-type responses (repressed, removed, static). The otherdata taken into consideration were not significantly different.
We then compared data obtained from subjects with classic migraine, common migraine and chronic dailyheadache, and the parameters which appeared significantly different after statistical analysis were the F + % andextended F + % which were lower in common migraine and in chronic daily headache.
CONCLUSION
Our present study shows clearly once again how precise psychopathologic elements exist as important factorsin the genesis of migraine and of essential headaches in general. This is in agreement with the work of severalother authors.
Substantial psychopathologic differences are not found among the three populations studied, i.e., subjects withclassic and common migraine and chronic daily headache. The only exception is the data of a significant increasein the form accuracy level of classic migraine.
This result seems to give little insight to the problem we proposed earlier, and thus needs further confirmationfrom a future, larger case study. What we can now say is that this may indicate that subjects with classic migrainehave fewer weaknesses in their perceptual organization than do other headache subjects; they also have a lessimpoverished associative content and less compromise of their ability to adhere to the real world in a congruentfashion using a good sense of reality. In other words, this result may indicate that the defensive modalities,including those represented by the somatic symptoms of a classic migraine sufferer, are more adaptive so thatthey permit him to better confront anxiety and anguish.
It is difficult to say if the above data can be correlated with a specific type of somatic symptom in thesesubjects. Possibly, a violent and evident somatization such as occurs in classic migraine may lead to increasedstability for the emotional structure of the subject. Thus, we may hazard a rather provocative idea of somatizationwhich functions better than can be observed in other clinical forms. On the other hand, this could indicate thecontrary by expressing almost a consequence of the increased flexibility and adaptation of the subject's mentaldefenses.
This remains an enigma and requires a more in depth study upon a more numerous population.
Although we have not found substantial differences between the populations studied, our research hasallowed us once more to confirm the idea that migraine subjects, considered on the whole, have an elevatedlevel of Ego inhibition, and a reduced ability for empathetic identification, which clearly emerged from theinterviews, and the different projective tests used. With particular attention to the Rorschach protocol, theabove is supported by the low number of responses of human movements, level of form accuracy and by theaccentuation of popular responses. On these subjects there is a contact with reality which is uninvolvedemotionally, detached, with prevalently rationalized and intellectualized modalities, that corresponds to theneed for blocking the emergence of emotional phantoms.
The reason for which certain individuals and not others tend to express conflictual aspects of self bynullifying these at the conscious level through a somatization such as migraine, rather than with otherdefensive mechanisms, may be explained not only by a defect in the antinociceptive system (whose truenature by predisposition or by maturational defect remains to be seen), but also by a particular type ofdefensive organization or by object relationships relative to an archaic mental organization for an uncertainattainment of a separate and individual identity.
This study was made possible by a grant for 60% of funds by the "Ministero della pubblica Istruzione".
REFERENCES
1. Nappi G, Savoldi: Headache. Diagnostic system and taxonomic criteria. John Libbey. Eurotext London.Paris, 1985.
2. Raskin NH, Appenzeller O: Headache. Saunders. Philadelphia, 1980.
3. Lanzi G: La cefalea essenziale nell-età evolutiva. II Pensiero Scientifico Ed. Roma, 1980.
4. Olesen J, Larsen B, Lauritzen M: Focal hyperemia followed by spreading oligemia and impairedactivation of rCBF in Classic Migraine. Ann Neurol 9:344-352, 1981.
5. Lauritzen M, Olsen TS, Lassen NA, Paulsen OB: Changes in regional cerebral blood flow during thecourse of classic migraine attacks. Ann Neurol 13:633-641, 1983.
6. Wilkinson M, Blau JN: Are classical and common migraine different entities? Headache 25:211-212,1985.
7. Olesen J: Are classical and common migraine different entities? Headache 25:213, 1985.
8. Vahlquist B: Migraine in children. Int Arch Allergy 7:348-355, 1955.
9. Wolff HG: Personality features and reactions of subjects with migraine. Arch Neurol Psychiat37:895-921, 1937.
10. Friedman AP, Brenner C: Psychological mechanism in chronic headache. Ass Res Nerv Dis Proc29:605-608, 1950.
11. Friedman AP: Headache as psychophysiological disorder International Congress "Headache 80"Florence Abstract book: 5, 1980.
12. Freud A: Sintomatologia dell'infanzia: tentativo preliminare di una classificazione. In opere vol. IIIBoringhieri Torino, 1979.
13. Lanzi G, Balottin U, Fazzi E, Gamba N. Psychological aspects of migraine in childhood. Cephalalgia3:18-20, 1983.
14. Lanzi G, Balottin U, Fazzi E: Psychopathology of migraine in childhood. International Congress"Headache 85" Copenhagen Abstract book: 158-159, 1985.
15. Marty P, M'Uzan M, David C: L'investigation psychosomatique PUF edit Paris, 1983.
16. Boag T J: Psychogenic headache In Handbook of Clinical Neurology North-Holland Company Ed.Amsterdam. Vol 5, Chapter 24:247-257, 1968.