Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Differential Diagnosis ofWell-Differentiated Squamous CellCarcinoma from Non-NeoplasticOral Mucosal Lesions: NewCytopathologic EvaluationMethod Dependent onKeratinization-Related Parametersbut Not Nuclear AtypismHitoshi Hara, PHD,1 Tsuneo Misawa, DDS, PHD,2 Eri Ishii, CT,1
Miki Nakagawa, CT,1 Saki Koshiishi, CT,1 Kenji Amemiya, CT,1
Toshio Oyama, MD,1 Kazuya Tominaga, DDS, PHD,3 Jun Cheng, MD, PHD,4
Akio Tanaka, DDS, PHD,3 and Takashi Saku, DDS, PHD3,4*
Background: The cytology of oral squamous cell carcinoma(SCC) is challenging because oral SCC cells tend to be well dif-ferentiated and lack nuclear atypia, often resulting in a falsenegative diagnosis. The purpose of this study was to establishpractical cytological parameters specific to oral SCCs.Methods: We reviewed 123 cases of malignancy and 53 of non-neoplastic lesions of the oral mucosa, which had been
diagnosed using both cytology and histopathology specimens.From those, we selected 12 SCC and 4 CIS cases that had ini-tially been categorized as NILM to ASC-H with the Bethesdasystem, as well as 4 non-neoplastic samples categorized as LSILor ASC-H as controls, and compared their characteristic find-ings. After careful examinations, we highlighted five cytologicalparameters, as described in Results. Those 20 cytology sampleswere then reevaluated by 4 independent examiners using theBethesda system as well as the 5 parameters.Results: Five cytological features, (i) concentric arrangement oforangeophilic cells (indicating keratin pearls), (ii) large numberof orangeophilic cells, (iii) bizarre-shaped orangeophilic cellswithout nuclear atypia, (iv) keratoglobules, and (v) uneven fila-mentous cytoplasm, were found to be significant parameters. Allmalignant cases contained at least one of those parameters, whilenone were observed in the four non-neoplastic cases with nuclearatypia. In reevaluations, the Bethesda system did not help thescreeners distinguish oral SCCs from non-neoplastic lesions, whileuse of the five parameters enabled them to make a diagnosis ofSCC.Conclusion: Recognition of the present five parameters is usefulfor oral SCC cytology. Diagn. Cytopathol. 2017;00:000–000. VC
2017 Wiley Periodicals, Inc.
Key Words: concentric cellular arrangement; filamentous cyto-plasm; keratinization; keratoglobules; oral squamous cellcarcinoma
1Pathology Division, Yamanashi Prefectural Central Hospital, Kofu,Japan
2Oral Surgery Division, Yamanashi Prefectural Central Hospital,Kofu, Japan
3Department of Oral Pathology, Osaka Dental University, Hirakata,Japan
4Division of Oral Pathology, Department of Tissue Regeneration andReconstruction, Niigata University Graduate School of Medical andDental Sciences, Niigata, Japan
*Correspondence to: Takashi Saku, DDS, PhD, Osaka Dental Univer-sity, 8-1 Kuzuha Hanazono-cho, Hirakata 573-1121, Japan.E-mail: [email protected] grant sponsor: JSPS KAKENHI; contract grant numbers:JP25305035; JP26305032, and JP15K15693.
Conflicts of Interest Disclosure: The authors have no conflicts of inter-est to declare.
Received 28 September 2016; Revised 21 January 2017; Accepted 24January 2017
DOI: 10.1002/dc.23685Published online 00 Month 2017 in Wiley Online Library (wileyonli-
nelibrary.com).
VC 2017 WILEY PERIODICALS, INC. Diagnostic Cytopathology, Vol. 00, No 00 1

Oral cancer is one of the most common types of human
cancers, ranking eighth among whole body cancers world-
wide,1 and its frequency of oral cancer is well known to
be higher in southern Asia, especially in developing coun-
tries,2 such as India3 and Pakistan.4 According to our own
studies, it was sixth most common in Myanmar5 and the
most prominent (19.6%) in Yemen.6 At the same time,
increasing oral cancer frequency has been reported in
European countries, including Denmark, France, Germa-
ny, and Scotland, with prevalence mainly in males.7 Since
the most common type of oral cancer is squamous cell
carcinoma (SCC), these statistics are considered to also
reflect those for SCC.3
Death and incidence rates of oral cancer according to
age tend to be opposite in the United States as compared
to Asian countries. In the United States, the age-adjusted
death and incidence rates for males were decreased by
0.6- and 0.8-folds, respectively, in the 37 years up to
2012.8 In contrast, those rates in Taiwan were increased
by 8.5- and 14.4-folds, respectively, in the 33-year period
up to 2012.9 As for Japan, the age-adjusted death rate
from oral and pharyngeal cancer was reported to have
increased by 2.1-folds, while the rough overall rate
increased by 8.5-folds in the past 57–62 years up to
2014.10,11 Such an obvious decreasing tendency of oral
cancer in the United States seems to be the result of an
early medical examination campaign for oral cancer pre-
vention that features early detection and early treatment,
for which cytology has been applied.12
When compared with cervical and esophageal SCCs,
oral SCCs show greater differentiation in histological
findings, a phenomenon that may be due to differences in
their embryonal origin, ectodermal or endodermal.13
Well-differentiated SCCs present one of the most chal-
lenging tasks for interpreting cytology findings of oral
mucosal lesions, since they lack nuclear atypia, as
described in the WHO Blue Book.14 However, cytological
diagnosis is basically performed by referring to nuclear
atypia appearing in any organ. Thus, when this cytologi-
cal concept is applied to oral mucosal lesions, false-
negative results are inevitable in significant numbers of
oral SCC cases, as the sensitivity (true positive/true posi-
tive plus false-negative) of cytological diagnosis for oral
cancer has been reported to vary at 87.4,15 96.5,16 and
85.4%.17 These findings may indicate some limits of
exfoliative cytology,18 although the reason for the higher
rate of false-negative results has not been investigated in
detail. Rather, in clinical practice, there is a general
impression among clinicians that cytological diagnosis is
not always reliable, especially in clinically gray-zone
cases. Thus, it is important to establish oral-SCC-specific
diagnostic criteria based on the concept that most oral
SCC cases can be well differentiated and occasionally
lack nuclear atypia, and that the Bethesda System widely
used for clinical cytological examinations is primarily for
cervical and not oral lesions.
The purpose of this study was to elucidate which cyto-
logical parameters other than nuclear atypia are effective
for differential diagnosis of well-differentiated oral SCCs
and non-neoplastic lesions with nuclear atypia. To this
end, cytological findings were carefully compared with
histological findings in oral carcinoma in situ (CIS) and
SCC cases, which were objectively diagnosed based on
immunohistochemistry findings.
Materials and Methods
Specimens
Cytology specimens were obtained from patients who vis-
ited the Oral Surgery Clinic of Yamanashi Prefectural
Central Hospital, Kofu, Japan, during the 96-month peri-
od from 2004 to 2011. We examined a total of 603 speci-
mens, which accounted for 0.82% of the 73,736 cytology
specimens collected at that hospital during the same peri-
od. They were composed of 424 (70.3%) curette-scraping
samples from oral mucosal surfaces and 179 (29.7%) fine
needle aspiration samples from deeper soft parts, includ-
ing lymph nodes and salivary glands. Initial screening of
those 424 oral mucosal specimens by curette scraping
was randomly and independently performed by 4 screen-
ers, each of whom had >10 years of experience in cyto-
pathology (1 expert cytologist, 3 pathologists), to select
specimens from non-neoplastic cases, which were deter-
mined by whether they contained >200 squamous epithe-
lial cells smeared on a slide glass. Malignant cases were
chosen when 30 or more diagnosable cells were present
in the smear. From those, we then selected 123 cases of
malignancy (119 SCCs, 4 CISs) and 53 cases with non-
neoplastic lesions, both of which also had histology speci-
mens in adequate condition available for re-evaluation
using immunohistochemical hallmarks for oral malignan-
cy, such as loss of keratin (K) 13 or K19, as well as
emergence of K10, K16, and K17,19–22 and podopla-
nin.23,24 The study protocol for analyzing biopsy and
cytology samples was reviewed and approved by the Ethi-
cal Board of Yamanashi Prefectural Central Hospital.
Patients were not asked to give informed consent, because
anonymous specimens and clinical data were used.
Categorization Using Bethesda System
The 2001 Bethesda System (TBS) for reporting cervical
or vaginal cytology was the initial method used for cyto-
logical evaluations in a hospital setting.25 Among the 123
malignant cases, 107 (87.0%) were initially diagnosed as
having malignant [9 with high-grade squamous intraepi-
thelial lesion (HSIL) (7.3%), and 98 with SCC (79.7%)].
Of the remaining 16 cases not correctly diagnosed as
malignant, 5 (4.1%) were initially diagnosed as negative
Diagnostic Cytopathology DOI 10.1002/dc
HARA ET AL.
2 Diagnostic Cytopathology, Vol. 00, No 00
for intraepithelial lesions or malignancy (NILM), 1
(0.8%) with atypical squamous cells of undetermined sig-
nificance (ASC-US), 3 (2.4%) with low-grade squamous
intraepithelial lesion (LSIL), and 7 (5.7%) with ASC,
though those do not exclude HSIL (ASC-H). These 16
malignant tumors occurred in the tongue, gingiva, buccal
mucosa, or lip, as shown in Table I. Thus, the 1 expert
cytologist and 3 pathologists who served as screeners
reexamined those 16 cases by referring to the 53 non-
neoplastic lesion cases, including 1 case of LSIL and 3 of
ASC-H, all of which occurred in the gingiva as well as
the 107 malignant cases above mentioned, to determine
the cytological characteristics of oral SCC and CIS cells
other than nuclear factors.
Selection of Five Parameters for Cytologic Features
While reviewing the 20 (16 malignant, 4 non-neoplastic)
cases, each of which had samples available on 2–10
slides (Table I), the screeners listed the varieties of cyto-
plasmic appearance as possible cytological parameters by
comparing histological features with special attention giv-
en to modes of keratinization. Furthermore, they again
reviewed the remaining 107 malignant and 49 non-
neoplastic cases in addition to these 20 cases for their
cytological findings. As described in the Results section,
we finally selected the following five parameters: (i) con-
centric arrangement of orangeophilic cells indicating kera-
tin pearls; (ii) large number of orangeophilic cells; (iii)
bizarre-shaped orangeophilic cells with a spindle- or
caudate-shape with deep orange-yellow color and distinct
cell borders, but without nuclear atypia; (iv) keratoglo-
bules, a term used to designate small round cells with
deep orangeophilic cytoplasm; and (v) uneven filamentous
cytoplasm. We termed this cytologic evaluation method
based on the presence or absence of these five parameters
as the five parameter system (FPS).
Reevaluation by TBS and FPS
Among the 16 malignant cases (12 SCC, 4 CIS), which
were selected for the reevaluation test, 2 with SCC and 3
with CIS were initially diagnosed as NILM, 1 with SCC
as ASC-US, 3 with SCC as LSIL, and 6 with SCC and 1
with CIS as ASC-H, while the 4 non-neoplastic cases
were diagnosed as LSIL or ASC-H (Table I). Each case
had 2–10 slide specimens available (Table I), thus only 1
from each was selected by choosing a slide that either
contained a reasonable amount of cells or the one with
the larger numbers of cells when only 2 or 3 slides were
available, for a total of 20 slides from the 20 cases exam-
ined. This selection of slides for the reevaluation test was
performed by the first author and corresponding authors.
To avoid bias in the selection, it was not reconfirmed
whether all five of the parameters were present. Reevalua-
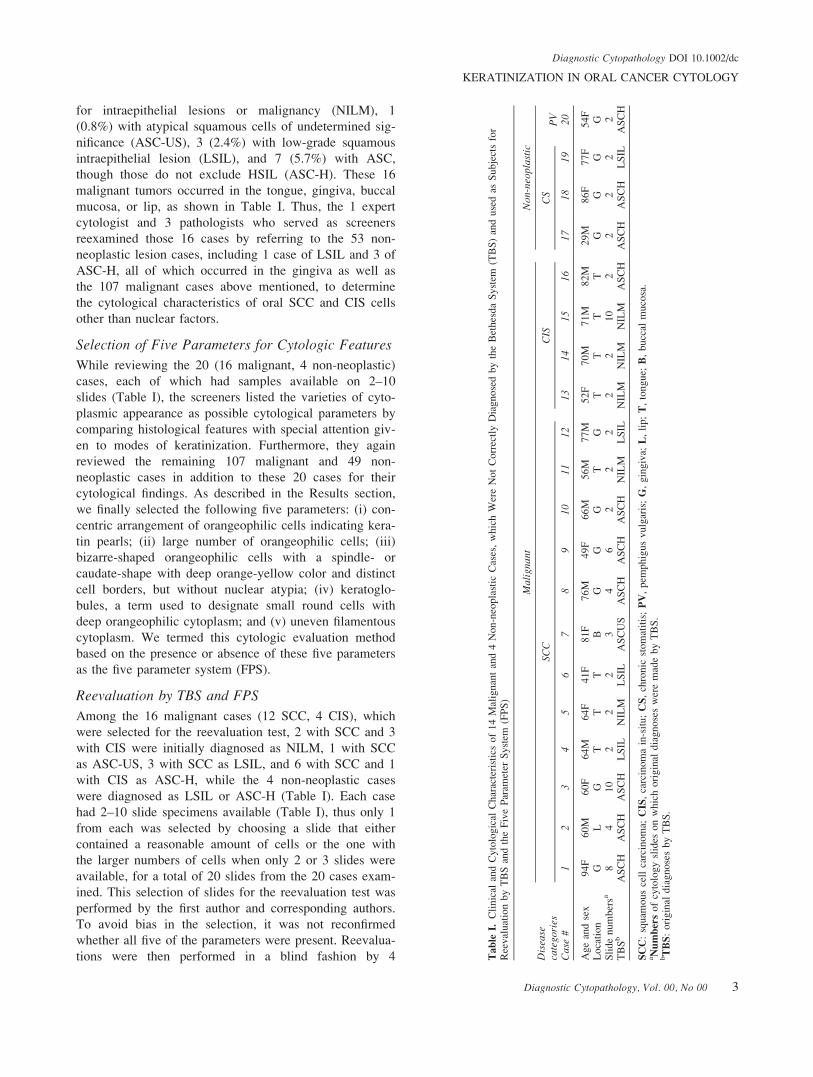
tions were then performed in a blind fashion by 4 Tab
leI.
Cli
nic
alan
dC
yto
logic
alC
har
acte
rist
ics
of
14
Mal
ignan
tan
d4
Non-n
eopla
stic
Cas
es,
whic
hW
ere
Not
Corr
ectl
yD
iagnose
dby
the
Bet
hes
da
Syst
em(T
BS
)an
duse
das
Subje
cts
for
Ree
val
uat
ion
by
TB
San
dth
eF
ive
Par
amet
erS
yst
em(F
PS
)
Dis
ease
cate
gori
es
Mal
igna
ntN
on-n
eopl
asti
c
SCC
CIS
CS
PV
Cas
e#
12
34
56
78
910
11
12
1314
1516
1718
1920
Age
and
sex
94F
60M
60F
64M
64F
41F
81F
76M
49F
66M
56M
77M
52F
70M
71M
82M
29M
86F
77F
54F
Loca
tion
GL
GT
TT
BG
GG
TG
TT
TT
GG
GG
Sli
de
num
ber
sa8
410
22
23
46
22
22
210
22
22
2T
BS
bA
SC
HA
SC
HA
SC
HL
SIL
NIL
ML
SIL
AS
CU
SA
SC
HA
SC
HA
SC
HN
ILM
LS
ILN
ILM
NIL
MN
ILM
AS
CH
AS
CH
AS
CH
LS
ILA
SC
H
SC
C:
squam
ous
cell
carc
inom
a;C
IS,
carc
inom
ain
-sit
u;
CS
,ch
ronic
stom
atit
is;
PV
,pem
phig
us
vulg
aris
;G
,gin
giv
a;L
,li
p;
T,
tongue;
B,
bucc
alm
uco
sa.
aN
um
ber
sof
cyto
logy
slid
eson
whic
hori
gin
aldia
gnose
sw
ere
mad
eby
TB
S.
bT
BS
:ori
gin
aldia
gnose
sby
TB
S.
Diagnostic Cytopathology DOI 10.1002/dc
KERATINIZATION IN ORAL CANCER CYTOLOGY
Diagnostic Cytopathology, Vol. 00, No 00 3

examiners, 2 experts with >20 years of experience each
as a cytologist and 2 nonexperts with <2 years of experi-
ence each. One of the expert cytologists, the first author,
was involved in the screening of the 20 cases and fixed
the 5 parameters for oral SCC as described above. Since
the other 3 examiners were not familiar with the 5 cyto-
logical parameters noted above, they underwent compre-
hensive training, during which slides containing the 5
parameter features from the other 107 cases, that had cor-
rectly been diagnosed as malignant by TBS, of the 123
malignancies were presented to them, until they were
able to recognize the parameters. The 20 slides used for
reevaluation were not used for training the 3 examiners,
hence they examined those for the first time during the
reevaluation. A repeatability test was performed by asking
the examiners for their evaluations of 20 specimens by
use of TBS or by FPS, in which the presence (1) or
absence (2) of parameters (i) (ii), (iii), (iv), and (v) were
determined. Their final diagnoses were then compared
between the two systems.
Statistical Analysis
Cytological parameter data were statistically analyzed
using Fisher’s exact test with Graph-Pad Instat (version
3.06 for Windows; GraphPad Software, San Diego, CA).
P-values <0.05 were considered to be statistically
significant.
Results
TBS Evaluation
Of the 123 malignant cases, 107 (87.0%) had been cor-
rectly diagnosed as malignant by TBS, including 1
(0.8%) HSIL (severe dysplasia), 4 (3.3%) HSIL (severe
dysplasia/CIS), 1 (0.8%) HSIL (CIS), 3 (2.4%) HSIL
(CIS/SCC), and 98 (79.7%) SCC cases. However, the
remaining 16 (13.0%) had not been diagnosed as malig-
nant by TBS and were selected as the main materials for
the present study, as described in Materials and Methods.
Cytology specimens from the 16 target cases common-
ly contained keratinizing superficial layer type (ST) and
keratinizing intermediate layer type (IMT) cells, and rare-
ly non-keratinizing ST/IMT/parabasal layer type cells.
Interestingly, malignancy in these 16 cases was clinically
doubtful, though histopathological findings later con-
firmed them to be malignant. Among the 53 non-
neoplastic cases, 1 (1.9%) was categorized as LSIL, 3 as
ASC-H (5.7%) (Table I), and the remaining 49 (92.5%)
as NILM. Histopathologically, they were confirmed to be
mucositis, granulation tissue (fibroepithelial polyp or pyo-
genic granuloma), or fistulas. Thus, the 4 non-neoplastic
cases with nuclear atypia and the 16 malignant cases
were selected for a reevaluation study.
Extraction of Parameters Specific to Oral SCC
In our review of cytology specimens from the 123 malig-
nant cases including the 16 malignant cases selected for
reevaluation and 53 non-neoplastic cases, including 4 nor-
mal control samples, we gave attention to not only nucle-
ar but also cytoplasmic findings. As a result, 5 findings
were considered to be most conspicuous in the 16 malig-
nant but not in the non-neoplastic cases. In addition, these
5 findings were confirmed to be present in some of the
remaining 107 cases. For this portion of the study, three
of the four examiners who took the reevaluation testing
were not involved. Those five parameters are described in
detail in the following sections.
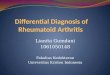
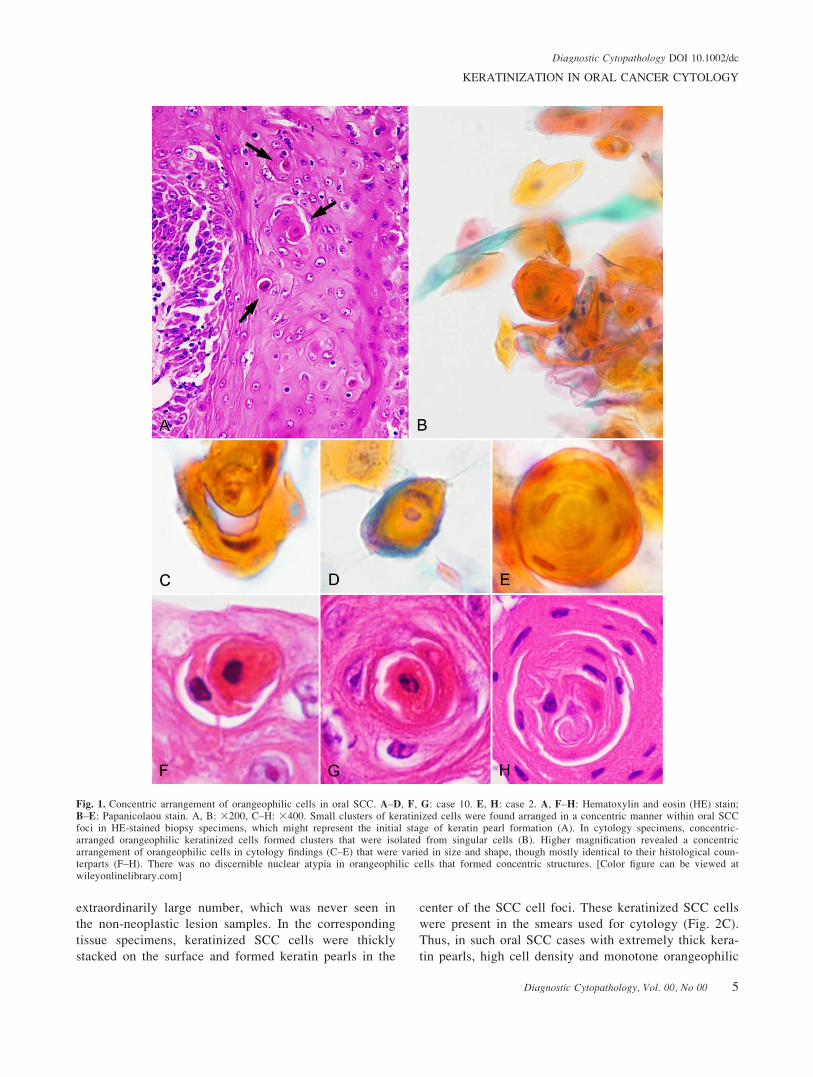
Concentric arrangement of orangeophilic cells indicat-ing keratin pearls. Small clusters of keratinized cells
were often found arranged in a concentric manner, which
might represent a minimal formation of keratin pearls
within oral SCC foci in HE-stained biopsy specimens
(Fig. 1A, arrows). In cytology specimens, clusters of
orangeophilic keratinized cells arranged in a concentric
manner were often isolated from aggregates of smeared
cells (Fig. 1B). In higher magnification observations, con-
centric arrangements of orangeophilic cells in cytology
findings varied in size and shape (Figs. 1C–E), although
they were mostly identical to each histological counter-
part (Figs. 1F–H). SCC cells surrounding the concentric
core of keratinized cells loosing nuclei had polygonal
(Fig. 1F) or flat (Fig. 1G) shapes. Among those with a
flat shape, surrounding flat cells were occasionally
arranged in a concentric manner as squamous eddies or
classic keratin pearls (Fig. 1H). Thus, these concentric
arrangements of orangeophilic cells were considered to
indicate an initial stage of keratin pearl development.
When keratinized cells began to form concentric struc-
tures, they tended to detach from each other (Figs. 1C, F,
and G), though they were densely packed in larger con-
centric structures (Figs. 1E and H). It was difficult to dis-
tinguish any nuclear atypia in those orangeophilic cells
that formed concentric structures. Such concentric
arrangement of keratinized cells was observed in 9 (75%)
of the 12 SCC cases, whereas that was not seen (0%) in
the 4 CIS and 53 non-neoplastic cases.
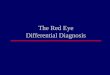
Large numbers of orangeophilic cells. Most of the
cytology specimen smears from malignant cases con-
tained cells with a monotone appearance and orangeo-
philic cytoplasm containing nuclei (Fig. 2A). Those
orangeophilic cell clusters contained <10% nonorangeo-
philic cells, among which there were no green-stained
basal or parabasal cells. With higher magnification, those
keratinized cells consistently showed a low nuclear/cyto-
plasm (N/C) ratio (Fig. 2B). Thus, it was difficult to
determine the malignant or neoplastic characteristics of
these orangeophilic cells, though there was an
Diagnostic Cytopathology DOI 10.1002/dc
HARA ET AL.
4 Diagnostic Cytopathology, Vol. 00, No 00
extraordinarily large number, which was never seen in
the non-neoplastic lesion samples. In the corresponding
tissue specimens, keratinized SCC cells were thickly
stacked on the surface and formed keratin pearls in the
center of the SCC cell foci. These keratinized SCC cells
were present in the smears used for cytology (Fig. 2C).
Thus, in such oral SCC cases with extremely thick kera-
tin pearls, high cell density and monotone orangeophilic
Fig. 1. Concentric arrangement of orangeophilic cells in oral SCC. A–D, F, G: case 10. E, H: case 2. A, F–H: Hematoxylin and eosin (HE) stain;B–E: Papanicolaou stain. A, B: 3200, C–H: 3400. Small clusters of keratinized cells were found arranged in a concentric manner within oral SCCfoci in HE-stained biopsy specimens, which might represent the initial stage of keratin pearl formation (A). In cytology specimens, concentric-arranged orangeophilic keratinized cells formed clusters that were isolated from singular cells (B). Higher magnification revealed a concentricarrangement of orangeophilic cells in cytology findings (C–E) that were varied in size and shape, though mostly identical to their histological coun-terparts (F–H). There was no discernible nuclear atypia in orangeophilic cells that formed concentric structures. [Color figure can be viewed atwileyonlinelibrary.com]
Diagnostic Cytopathology DOI 10.1002/dc
KERATINIZATION IN ORAL CANCER CYTOLOGY
Diagnostic Cytopathology, Vol. 00, No 00 5
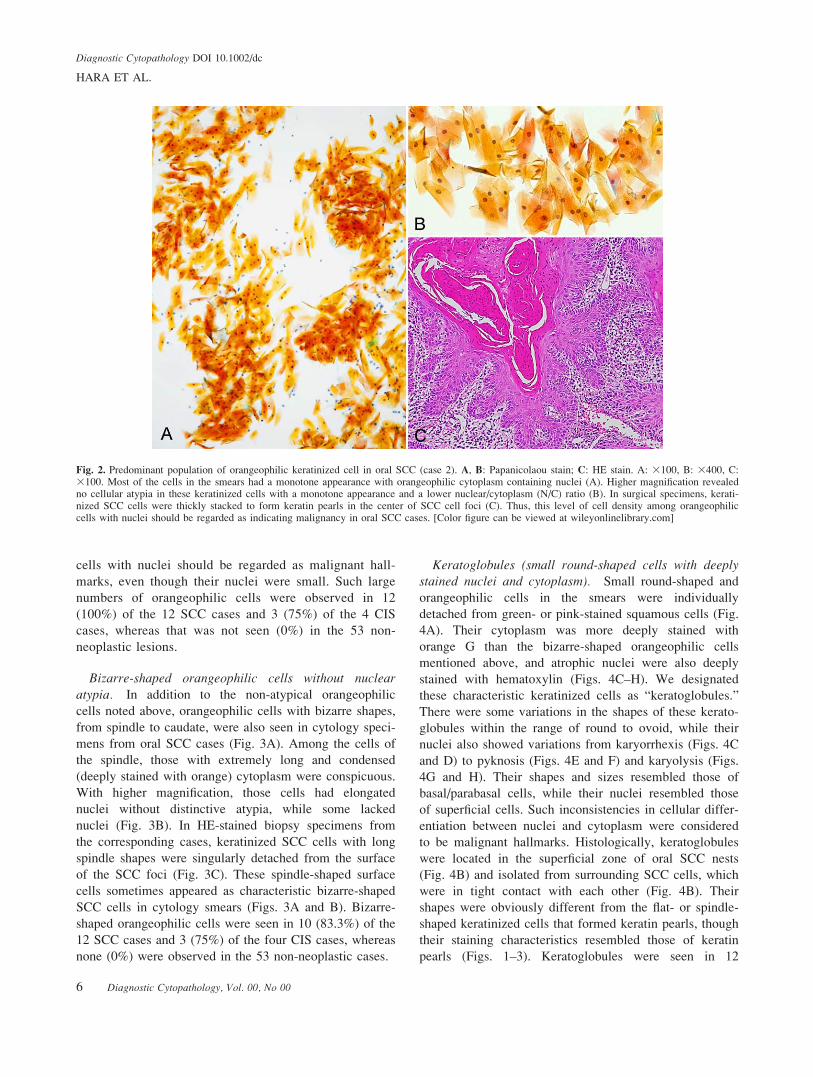
cells with nuclei should be regarded as malignant hall-
marks, even though their nuclei were small. Such large
numbers of orangeophilic cells were observed in 12
(100%) of the 12 SCC cases and 3 (75%) of the 4 CIS
cases, whereas that was not seen (0%) in the 53 non-
neoplastic lesions.
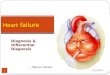
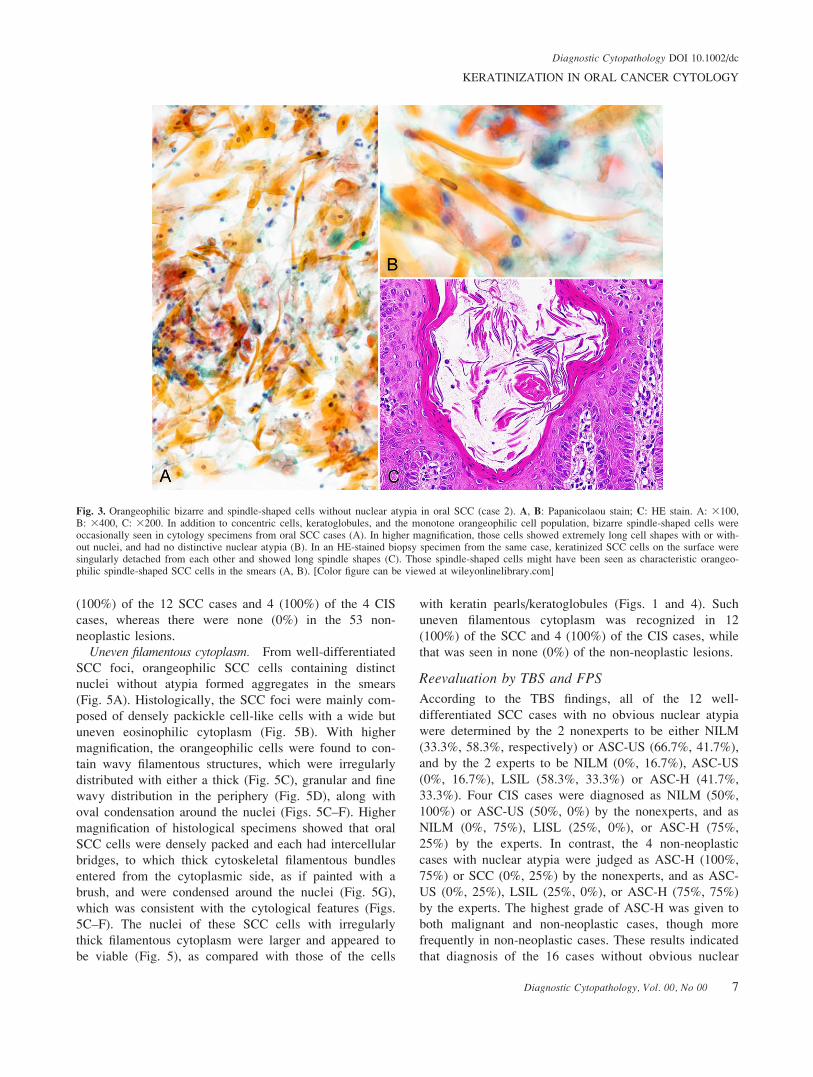
Bizarre-shaped orangeophilic cells without nuclearatypia. In addition to the non-atypical orangeophilic
cells noted above, orangeophilic cells with bizarre shapes,
from spindle to caudate, were also seen in cytology speci-
mens from oral SCC cases (Fig. 3A). Among the cells of
the spindle, those with extremely long and condensed
(deeply stained with orange) cytoplasm were conspicuous.
With higher magnification, those cells had elongated
nuclei without distinctive atypia, while some lacked
nuclei (Fig. 3B). In HE-stained biopsy specimens from
the corresponding cases, keratinized SCC cells with long
spindle shapes were singularly detached from the surface
of the SCC foci (Fig. 3C). These spindle-shaped surface
cells sometimes appeared as characteristic bizarre-shaped
SCC cells in cytology smears (Figs. 3A and B). Bizarre-
shaped orangeophilic cells were seen in 10 (83.3%) of the
12 SCC cases and 3 (75%) of the four CIS cases, whereas
none (0%) were observed in the 53 non-neoplastic cases.
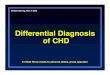
Keratoglobules (small round-shaped cells with deeplystained nuclei and cytoplasm). Small round-shaped and
orangeophilic cells in the smears were individually
detached from green- or pink-stained squamous cells (Fig.
4A). Their cytoplasm was more deeply stained with
orange G than the bizarre-shaped orangeophilic cells
mentioned above, and atrophic nuclei were also deeply
stained with hematoxylin (Figs. 4C–H). We designated
these characteristic keratinized cells as “keratoglobules.”
There were some variations in the shapes of these kerato-
globules within the range of round to ovoid, while their
nuclei also showed variations from karyorrhexis (Figs. 4C
and D) to pyknosis (Figs. 4E and F) and karyolysis (Figs.
4G and H). Their shapes and sizes resembled those of
basal/parabasal cells, while their nuclei resembled those
of superficial cells. Such inconsistencies in cellular differ-
entiation between nuclei and cytoplasm were considered
to be malignant hallmarks. Histologically, keratoglobules
were located in the superficial zone of oral SCC nests
(Fig. 4B) and isolated from surrounding SCC cells, which
were in tight contact with each other (Fig. 4B). Their
shapes were obviously different from the flat- or spindle-
shaped keratinized cells that formed keratin pearls, though
their staining characteristics resembled those of keratin
pearls (Figs. 1–3). Keratoglobules were seen in 12
Fig. 2. Predominant population of orangeophilic keratinized cell in oral SCC (case 2). A, B: Papanicolaou stain; C: HE stain. A: 3100, B: 3400, C:3100. Most of the cells in the smears had a monotone appearance with orangeophilic cytoplasm containing nuclei (A). Higher magnification revealedno cellular atypia in these keratinized cells with a monotone appearance and a lower nuclear/cytoplasm (N/C) ratio (B). In surgical specimens, kerati-nized SCC cells were thickly stacked to form keratin pearls in the center of SCC cell foci (C). Thus, this level of cell density among orangeophiliccells with nuclei should be regarded as indicating malignancy in oral SCC cases. [Color figure can be viewed at wileyonlinelibrary.com]
Diagnostic Cytopathology DOI 10.1002/dc
HARA ET AL.
6 Diagnostic Cytopathology, Vol. 00, No 00
(100%) of the 12 SCC cases and 4 (100%) of the 4 CIS
cases, whereas there were none (0%) in the 53 non-
neoplastic lesions.
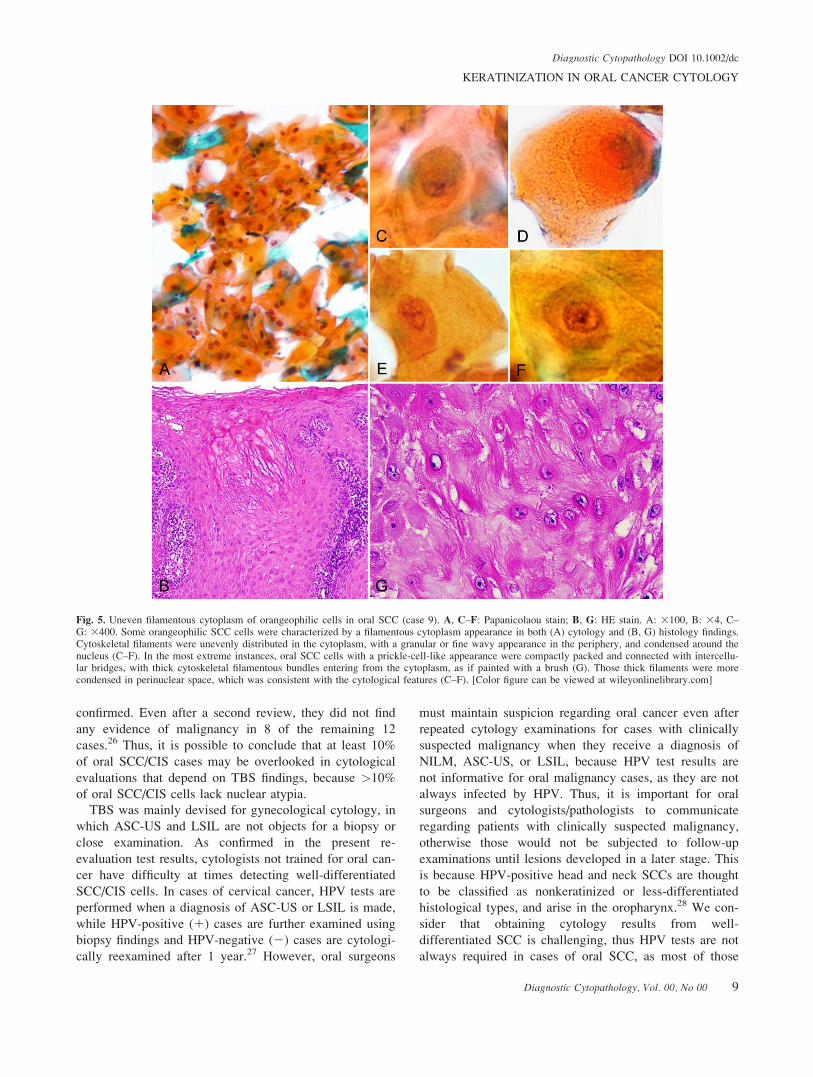
Uneven filamentous cytoplasm. From well-differentiated
SCC foci, orangeophilic SCC cells containing distinct
nuclei without atypia formed aggregates in the smears
(Fig. 5A). Histologically, the SCC foci were mainly com-
posed of densely packickle cell-like cells with a wide but
uneven eosinophilic cytoplasm (Fig. 5B). With higher
magnification, the orangeophilic cells were found to con-
tain wavy filamentous structures, which were irregularly
distributed with either a thick (Fig. 5C), granular and fine
wavy distribution in the periphery (Fig. 5D), along with
oval condensation around the nuclei (Figs. 5C–F). Higher
magnification of histological specimens showed that oral
SCC cells were densely packed and each had intercellular
bridges, to which thick cytoskeletal filamentous bundles
entered from the cytoplasmic side, as if painted with a
brush, and were condensed around the nuclei (Fig. 5G),
which was consistent with the cytological features (Figs.
5C–F). The nuclei of these SCC cells with irregularly
thick filamentous cytoplasm were larger and appeared to
be viable (Fig. 5), as compared with those of the cells
with keratin pearls/keratoglobules (Figs. 1 and 4). Such
uneven filamentous cytoplasm was recognized in 12
(100%) of the SCC and 4 (100%) of the CIS cases, while
that was seen in none (0%) of the non-neoplastic lesions.
Reevaluation by TBS and FPS
According to the TBS findings, all of the 12 well-
differentiated SCC cases with no obvious nuclear atypia
were determined by the 2 nonexperts to be either NILM
(33.3%, 58.3%, respectively) or ASC-US (66.7%, 41.7%),
and by the 2 experts to be NILM (0%, 16.7%), ASC-US
(0%, 16.7%), LSIL (58.3%, 33.3%) or ASC-H (41.7%,
33.3%). Four CIS cases were diagnosed as NILM (50%,
100%) or ASC-US (50%, 0%) by the nonexperts, and as
NILM (0%, 75%), LISL (25%, 0%), or ASC-H (75%,
25%) by the experts. In contrast, the 4 non-neoplastic
cases with nuclear atypia were judged as ASC-H (100%,
75%) or SCC (0%, 25%) by the nonexperts, and as ASC-
US (0%, 25%), LSIL (25%, 0%), or ASC-H (75%, 75%)
by the experts. The highest grade of ASC-H was given to
both malignant and non-neoplastic cases, though more
frequently in non-neoplastic cases. These results indicated
that diagnosis of the 16 cases without obvious nuclear
Fig. 3. Orangeophilic bizarre and spindle-shaped cells without nuclear atypia in oral SCC (case 2). A, B: Papanicolaou stain; C: HE stain. A: 3100,B: 3400, C: 3200. In addition to concentric cells, keratoglobules, and the monotone orangeophilic cell population, bizarre spindle-shaped cells wereoccasionally seen in cytology specimens from oral SCC cases (A). In higher magnification, those cells showed extremely long cell shapes with or with-out nuclei, and had no distinctive nuclear atypia (B). In an HE-stained biopsy specimen from the same case, keratinized SCC cells on the surface weresingularly detached from each other and showed long spindle shapes (C). Those spindle-shaped cells might have been seen as characteristic orangeo-philic spindle-shaped SCC cells in the smears (A, B). [Color figure can be viewed at wileyonlinelibrary.com]
Diagnostic Cytopathology DOI 10.1002/dc
KERATINIZATION IN ORAL CANCER CYTOLOGY
Diagnostic Cytopathology, Vol. 00, No 00 7

atypia was extremely challenging when using TBS
(Table II).
In contrast, when using FPS, most of the malignant
cases with at least 1 of the 5 parameters confirmed were
not overlooked by any of the 4 examiner cytologists. As
shown in Table II, detection rates were quite similar
between the second expert and 2 nonexperts. All of the
parameters were noted at higher rates in SCC (60–96%)
and CIS (63–81%), except for parameter (i), which was
not always present in malignant cases but never detected
in reactive lesions by the 4 cytologists (Table II, right-
most column). The total numbers of the 5 parameters
confirmed in each case (Table II, bottom of each lesion
category) indicated that all parameters were not necessari-
ly included in each malignant specimen. However, there
were no differences in malignant judgment between the 2
experts and 1 of the nonexperts (12/12 SCC cases; 4/4
CIS), and nearly no differences with the other nonexpert
(11/12 SCC; 4/4 CIS), although the nonexperts tended to
identify fewer of the 5 parameters. In spite of those
reduced numbers, the nonexperts gave a malignant judg-
ment even when only a single parameter was noted, indi-
cating that any of the 5 parameters is a helpful indicator
of malignancy. In the CIS cases, at most 3 or 4 parame-
ters were included, and the nonexperts tended to overlook
them more frequently (3/4 cases). Nevertheless, as shown
in Table II, none of the 5 parameters were identified in
non-neoplastic cases, even those with nuclear atypism.
Discussion
The goal of this study was to determine cytological crite-
ria specific to well-differentiated oral SCC and CIS,
which lack discernible nuclear atypia, because their char-
acteristic of no or few atypical features tends to lead to
false-negative diagnoses.18 To this end, we newly deter-
mined 5 parameters for cytoplasmic features of well-
differentiated (keratinized) oral SCC cells after compara-
tive examinations of cytological and histological findings.
The present trial was successful for discriminating SCC
cells in cytology specimens based on their cytoplasmic
characteristics. An advantage of FPS is that it can widen
the value of cytological examinations for oral SCC cases,
most of which are well differentiated and difficult to pre-
cisely diagnose based only on nuclear features shown by
TBS.
This study showed that TBS functioned well for oral
cases (119 SCC, 4 CIS) that had nuclear atypia, while it
did not function well for 16 (13%) cases with cytology
specimens showing no obvious nuclear atypia. Similar
results were previously reported by Koch et al.,26 who
were able to cytologically detect 92 (88.5%) of 104
malignant (SCC and CIS) cases that were histologically
Fig. 4. Keratoglobules in oral SCC (case 10). A, C–H: Papanicolaou stain; B: HE stain. A: 3400, B: 3200, C–H: 3400. Singular small round-shapedand orangeophilic cells were found detached from green- or pink-stained squamous cells in the smears (A). The cytoplasm of these cells was deeplystained with orange G, while atrophic nuclei were also deeply stained with hematoxylin (C–H). These characteristic keratinized cells were designatedin this study as “keratoglobules.” They showed some variations in shape from round to ovoid, while their nuclei also showed variations from karyor-rhexis (C, D) to pyknosis (E, F), and karyolysis (G, H). Histologically, keratoglobules were located in the superficial zone of oral SCC nests and isolat-ed from surrounding SCC cells, which were in tight contact with each other (B). These were obviously different from flat or spindle-shapedkeratinized cells that formed keratin pearls (shown in Figs. 1–3). [Color figure can be viewed at wileyonlinelibrary.com]
Diagnostic Cytopathology DOI 10.1002/dc
HARA ET AL.
8 Diagnostic Cytopathology, Vol. 00, No 00
confirmed. Even after a second review, they did not find
any evidence of malignancy in 8 of the remaining 12
cases.26 Thus, it is possible to conclude that at least 10%
of oral SCC/CIS cases may be overlooked in cytological
evaluations that depend on TBS findings, because >10%
of oral SCC/CIS cells lack nuclear atypia.
TBS was mainly devised for gynecological cytology, in
which ASC-US and LSIL are not objects for a biopsy or
close examination. As confirmed in the present re-
evaluation test results, cytologists not trained for oral can-
cer have difficulty at times detecting well-differentiated
SCC/CIS cells. In cases of cervical cancer, HPV tests are
performed when a diagnosis of ASC-US or LSIL is made,
while HPV-positive (1) cases are further examined using
biopsy findings and HPV-negative (2) cases are cytologi-
cally reexamined after 1 year.27 However, oral surgeons
must maintain suspicion regarding oral cancer even after
repeated cytology examinations for cases with clinically
suspected malignancy when they receive a diagnosis of
NILM, ASC-US, or LSIL, because HPV test results are
not informative for oral malignancy cases, as they are not
always infected by HPV. Thus, it is important for oral
surgeons and cytologists/pathologists to communicate
regarding patients with clinically suspected malignancy,
otherwise those would not be subjected to follow-up
examinations until lesions developed in a later stage. This
is because HPV-positive head and neck SCCs are thought
to be classified as nonkeratinized or less-differentiated
histological types, and arise in the oropharynx.28 We con-
sider that obtaining cytology results from well-
differentiated SCC is challenging, thus HPV tests are not
always required in cases of oral SCC, as most of those
Fig. 5. Uneven filamentous cytoplasm of orangeophilic cells in oral SCC (case 9). A, C–F: Papanicolaou stain; B, G: HE stain. A: 3100, B: 34, C–G: 3400. Some orangeophilic SCC cells were characterized by a filamentous cytoplasm appearance in both (A) cytology and (B, G) histology findings.Cytoskeletal filaments were unevenly distributed in the cytoplasm, with a granular or fine wavy appearance in the periphery, and condensed around thenucleus (C–F). In the most extreme instances, oral SCC cells with a prickle-cell-like appearance were compactly packed and connected with intercellu-lar bridges, with thick cytoskeletal filamentous bundles entering from the cytoplasm, as if painted with a brush (G). Those thick filaments were morecondensed in perinuclear space, which was consistent with the cytological features (C–F). [Color figure can be viewed at wileyonlinelibrary.com]
Diagnostic Cytopathology DOI 10.1002/dc
KERATINIZATION IN ORAL CANCER CYTOLOGY
Diagnostic Cytopathology, Vol. 00, No 00 9
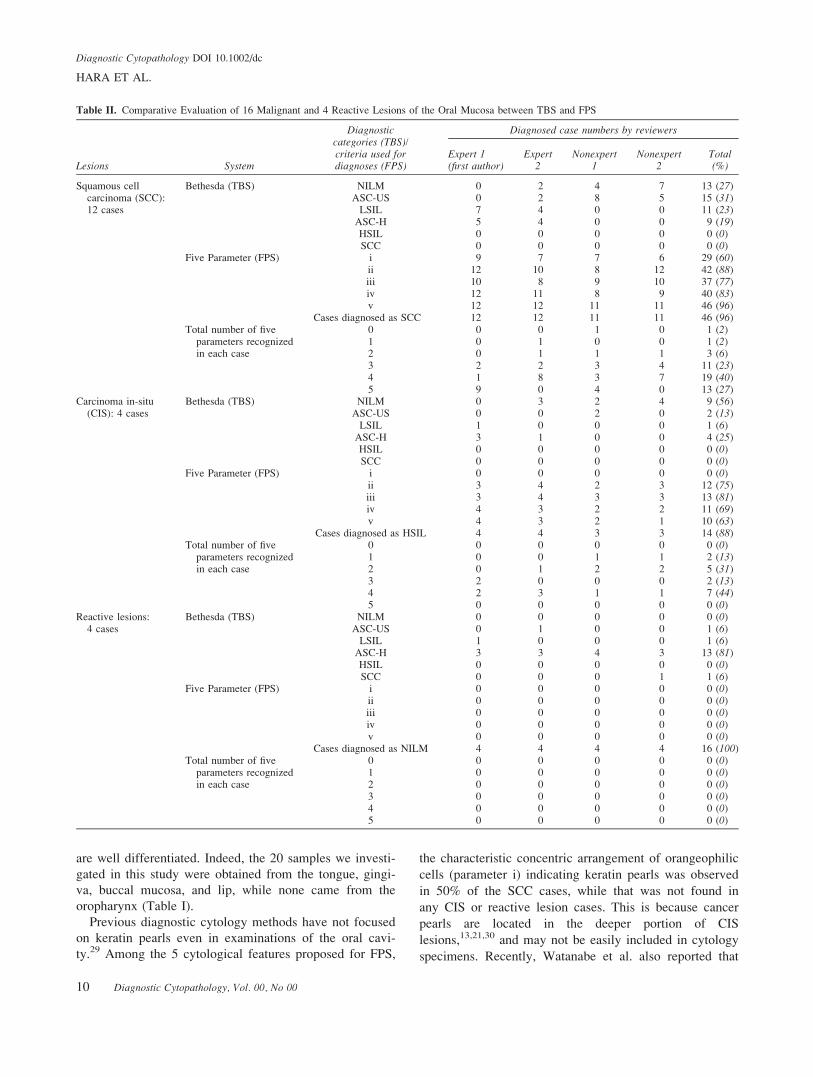
are well differentiated. Indeed, the 20 samples we investi-
gated in this study were obtained from the tongue, gingi-
va, buccal mucosa, and lip, while none came from the
oropharynx (Table I).
Previous diagnostic cytology methods have not focused
on keratin pearls even in examinations of the oral cavi-
ty.29 Among the 5 cytological features proposed for FPS,
the characteristic concentric arrangement of orangeophilic
cells (parameter i) indicating keratin pearls was observed
in 50% of the SCC cases, while that was not found in
any CIS or reactive lesion cases. This is because cancer
pearls are located in the deeper portion of CIS
lesions,13,21,30 and may not be easily included in cytology
specimens. Recently, Watanabe et al. also reported that
Table II. Comparative Evaluation of 16 Malignant and 4 Reactive Lesions of the Oral Mucosa between TBS and FPS
Lesions System
Diagnosticcategories (TBS)/criteria used fordiagnoses (FPS)
Diagnosed case numbers by reviewers
Expert 1(first author)
Expert2
Nonexpert1
Nonexpert2
Total(%)
Squamous cellcarcinoma (SCC):12 cases
Bethesda (TBS) NILM 0 2 4 7 13 (27)ASC-US 0 2 8 5 15 (31)
LSIL 7 4 0 0 11 (23)ASC-H 5 4 0 0 9 (19)HSIL 0 0 0 0 0 (0)SCC 0 0 0 0 0 (0)
Five Parameter (FPS) i 9 7 7 6 29 (60)ii 12 10 8 12 42 (88)iii 10 8 9 10 37 (77)iv 12 11 8 9 40 (83)v 12 12 11 11 46 (96)
Cases diagnosed as SCC 12 12 11 11 46 (96)Total number of five
parameters recognizedin each case
0 0 0 1 0 1 (2)1 0 1 0 0 1 (2)2 0 1 1 1 3 (6)3 2 2 3 4 11 (23)4 1 8 3 7 19 (40)5 9 0 4 0 13 (27)
Carcinoma in-situ(CIS): 4 cases
Bethesda (TBS) NILM 0 3 2 4 9 (56)ASC-US 0 0 2 0 2 (13)
LSIL 1 0 0 0 1 (6)ASC-H 3 1 0 0 4 (25)HSIL 0 0 0 0 0 (0)SCC 0 0 0 0 0 (0)
Five Parameter (FPS) i 0 0 0 0 0 (0)ii 3 4 2 3 12 (75)iii 3 4 3 3 13 (81)iv 4 3 2 2 11 (69)v 4 3 2 1 10 (63)
Cases diagnosed as HSIL 4 4 3 3 14 (88)Total number of five
parameters recognizedin each case
0 0 0 0 0 0 (0)1 0 0 1 1 2 (13)2 0 1 2 2 5 (31)3 2 0 0 0 2 (13)4 2 3 1 1 7 (44)5 0 0 0 0 0 (0)
Reactive lesions:4 cases
Bethesda (TBS) NILM 0 0 0 0 0 (0)ASC-US 0 1 0 0 1 (6)
LSIL 1 0 0 0 1 (6)ASC-H 3 3 4 3 13 (81)HSIL 0 0 0 0 0 (0)SCC 0 0 0 1 1 (6)
Five Parameter (FPS) i 0 0 0 0 0 (0)ii 0 0 0 0 0 (0)iii 0 0 0 0 0 (0)iv 0 0 0 0 0 (0)v 0 0 0 0 0 (0)
Cases diagnosed as NILM 4 4 4 4 16 (100)Total number of five
parameters recognizedin each case
0 0 0 0 0 0 (0)1 0 0 0 0 0 (0)2 0 0 0 0 0 (0)3 0 0 0 0 0 (0)4 0 0 0 0 0 (0)5 0 0 0 0 0 (0)
Diagnostic Cytopathology DOI 10.1002/dc
HARA ET AL.
10 Diagnostic Cytopathology, Vol. 00, No 00

they failed to find keratin pearls in oral CIS specimens.31
In endocervical (EC) smears, epithelial cells without
nuclear atypia contained in keratin pearls have been sim-
ply reported as “parakeratotic cells,” the same as those in
non-neoplastic lesions, without being distinguished from
each other.32 This fact clearly indicates that differential
diagnosis between malignant and benign EC cases is
dependent on nuclear atypia.32 However, such a concen-
tric arrangement of orangeophilic cells does exist in EC
smears, as shown in Fig. 1.39 in the chapter by Abdul-
Karim et al.18 and in Fig. 2.15a (squamous pearl, example
of typical parakeratosis) in the Bethesda 3rd edition,33
though that has been routinely ignored or judged as ASC-
US.18,33 As revealed in this study, detection of keratin
pearls is a reliable method for definitive diagnosis of oral
SCC.
The second feature of FPS is a predominant popula-
tion of keratinized cells (parameter ii). Nuclear atypia
should be minimized in oral SCC cells during the kerati-
nization process, with keratinized cells without nuclear
atypia eventually becoming predominant. Such a tenden-
cy towards keratinization is a very strong characteristic
of oral SCC.13,20 Bizarre-shaped orangeophilic cells
without nuclear atypia (parameter iii) were also found to
be characteristic of oral SCC and CIS, while they were
never found in reactive lesion samples. In EC smears,
these orangeophilic cells may only be recognized as ker-
atotic changes (parakeratosis or atypical parakeratosis).
According to the 3rd edition of TBS 2015, they must be
diagnosed in a range that includes NILM, ASC-US, and
LSIL, but not as HSIL.33 However, when nuclear atypia
is evident, they are regarded as keratinizing SCC.18
Meanwhile, in oral cytology findings, such bizarre-
shaped orangeophilic cells without nuclear atypia have
not been documented. We consider that these cell types
can be a very specific criterion of oral malignancy and
likely originate from stacks of keratinized SCC foci on
the surface.
Keratoglobules (parameter iv), isolated and small
round-shaped keratinized cells containing pyknotic
nuclei, were observed in all of the present SCC and CIS
cases, but never in reactive lesion samples. In addition
to pyknosis, nuclear shapes were interpreted as karyoly-
sis or karyorrhexis. Any type of nuclear morphology
may indicate the process of cell death in association
with keratinization,34 though it remains unknown how
nuclei are cleared in those cells. Nevertheless, these
nuclear shape varieties are definitely different from apo-
ptosis or any other already-known cell death machinery.
Although there are no known reports of keratoglobules
or their analogues in previous studies, the cytoplasm of
keratoglobules may resemble that of keratinized cells
forming keratin pearls. Previously, round-shaped dysker-
atotic foci were shown to be generated in the basal layer
due to hemorrhage resulting from collapsed intraepithe-
lial blood vessels in oral CIS and SCC cases,30 because
hemophagocytosis induces keratinization of epithelial
cells facing connective tissues.21 In gynecological cytol-
ogy, keratinizing basaloid cells are often seen in non-
neoplastic lesions that originate from senile atrophy,18
and miniature squamous cells with small bland and
pyknotic nuclei are considered to represent typical para-
keratosis (Fig. 2.15b in the Bethesda 3rd edition).33
Uneven filamentous cytoplasm (parameter v) was iden-
tified in 100% of the 16 malignant cases, whereas that
was not seen in any of the reactive lesions. This cytologi-
cal feature may represent dyskeratotic changes among
IMT cells in the lower prickle cell layers or singular cel-
lular keratinization among those in the basal half of CIS/
SCC foci,13 in which keratin filaments (tonofilaments) are
not evenly distributed. Such dyskeratotic cells were found
to contain definite and large nuclei with clear nucleo-
plasm and intercellular bridges in the present study,
which is in sharp contrast to keratoglobules with charac-
teristic nuclear collapse shapes of pyknosis, karyolysis, or
karyorrhexis.34 Both keratoglobules and uneven filamen-
tous cytoplasm were simultaneously identified in 100% of
the 16 SCC and CIS cases, while keratin pearls were
found in 60 and 0%, respectively. Uneven filamentous
cytoplasm is considered to be an initial sign of abnormal
keratinization among activated keratinocytes, which
may secondarily accelerate keratinization with nuclear
collapse.
In conclusion, FPS is a powerful tool for cytological
diagnosis of well-differentiated oral SCC. When some of
the five parameters are detected, even though all may not
be simultaneously identified, it is possible to make a diag-
nosis of malignancy. We consider that FPS is much more
effective than TBS for diagnosis of oral SCC and CIS
specimens lacking nuclear atypia. However, the present
series of specimens submitted to reexamination included
only 20 cases, thus it will be necessary for us to perform
further studies to test the diagnostic value of FPS. In
addition, we also anticipate that FPS will be widely
investigated by other groups to confirm its usefulness for
oral SCC cytology examinations.
References
1. de Camargo Cancela M, Voti L, Guerra-Yi M, Chapuis F, MazuirM, Curado MP. Oral cavity cancer in developed and in developingcountries: Population-based incidence. Head Neck 2010;32:357–367.
2. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics,2002. CA Cancer J Clin 2005;55:74–108.
3. Sherin N, Simi T, Shameena PM, Sudha S. Changing trends in oralcancer. Indian J Cancer 2008;45:93–96.
4. Bhurgri Y, Bhurgri A, Hassan SH, et al. Cancer incidence in Kara-chi, Pakistan: First results from Karachi Cancer Registry. Int J Can-cer 2000;85:325–329.
Diagnostic Cytopathology DOI 10.1002/dc
KERATINIZATION IN ORAL CANCER CYTOLOGY
Diagnostic Cytopathology, Vol. 00, No 00 11
5. Oo HN, Myint YY, Maung CN, et al. Oral cancer in Myanmar: apreliminary survey based on hospital-based cancer registries. J OralPathol Med 2011;40:20–26.
6. Sawair FA, Al-Mutwakel A, Al-Eryani K, et al. High relative fre-quency of oral squamous cell carcinoma in Yemen: Qat and tobac-co chewing as its aetiological background. Int J Environ Health Res2007;17:185–195.
7. Petersen PE, Bourgeois D, Bratthall D, Ogawa H. Oral health infor-mation systems – towards measuring progress in oral health promo-tion and disease prevention. Bull World Health Organ 2005;83:686–693.
8. Howlader N, Noone AM, Krapcho M, editors. SEER Cancer Statis-tics Review, 1975-2012, National Cancer Institute, Cancer Statics,CSR Sections, 20. Oral Cavity and Pharynx, Website title: AnnualIncidence Rates, Annual Death Rates. Available at: http://seer.can-cer.gov/csr/1975_2012/results_merged/sect_20_oral_cavity_pharynx.pdf. Accessed on 5/21/2016.
9. Taiwan Cancer Registry. Cancer Incidence Rate in Taiwan, 1998-2002 & 2003-2007. Available at: http://tcr.cph.ntu.edu.tw/main.php?Page5N2. Accessed on 5/21/2016.
10. Portal Site of Official Statistics of Japan, Statistics Bureau, TheMinistry of Internal Affairs and Communications. Trends in age-adjusted death rates (per 100,000 population) from malignant neo-plasms by sex and site: Japan (1950-2014) (Table 5-26). Availableat: http://www.e-stat.go.jp/SG1/estat/eStatTopPortalE.do. Accessedon 5/21/2016.
11. Cancer Registry and Statistics. Cancer Information Service, Nation-al Cancer Center, Japan. Cancer mortality (1958-2014). Availableat: http://ganjoho.jp/reg_stat/statistics/dl/index.html. Accessed on 5/21/2016.
12. Lingen MW, Kalmar JR, Karrison T, Speight PM. Critical evalua-tion of diagnostic aids for the detection of oral cancer. Oral Oncol2008;44:10–22.
13. Kobayashi T, Maruyama S, Cheng J, et al. Histopathological varie-ties of oral carcinoma in situ: Diagnosis aided by immunohisto-chemistry dealing with the second basal cell layer as theproliferating center of oral mucosal epithelia. Pathol Int 2010;60:156–166.
14. Pindborg JJ, Reichart PA, Smith CJ, van der Waal I. Histologicaltyping of cancer and precancer of the oral mucosa. WHO Classifi-cation of Tumours. 2nd ed. Berlin: Springer; 1997. p 24–26.
15. Kaugars GE, Silverman S, Ray AK, et al. The use of exfoliativecytology for the early diagnosis of oral cancers: is there a role forit in education and private practice? J Cancer Educ 1998;13:85–89.
16. Potter TJ, Summerlin DJ, Campbell JH. Oral malignancies associat-ed with negative transepithelial brush biopsy. J Oral MaxillofacSurg 2003;61:674–677.
17. Shklar G, Meyer I, Cataldo E, Taylor R. Correlated study of oralcytology and histopathology. Report on 2,052 oral lesions. OralSurg Oral Med Oral Pathol 1960;13:897–907.
18. Abdul-Karim FW, Brainard J, Michael CW. Cytopathology. In:Chang L, Bostwick DG, editors. Essentials of Anatomic Pathology.3rd ed. New York: Springer; 2011. p 17–23.
19. Mikami T, Cheng J, Maruyama S, et al. Emergence of keratin 17vs. loss of keratin13: their reciprocal immunohistochemical profilesin oral carcinoma in situ. Oral Oncol 2011;47:497–503.
20. Kobayashi T, Maruyama S, Ab�e T, et al. Keratin 10-positive ortho-keratotic dysplasia: A new leukoplakia-type precancerous entity ofthe oral mucosa. Histopathology 2012;61:910–920.
21. Al-Eryani K, Cheng J, Ab�e T, et al. Hemophagocytosis-mediatedkeratinization in oral carcinoma in-situ and squamous cell carcino-ma: A possible histopathogenesis of keratin pearls. J Cell Physiol2013;228:1977–1988.
22. Ida-Yonemochi H, Maruyama S, Kobayashi T, Yamazaki M, ChengJ, Saku T. Loss of keratin 13 in oral carcinoma in-situ: A compara-tive study of protein and gene expression levels using paraffin sec-tions. Mod Pathol 2012;25:784–794.
23. Funayama A, Cheng J, Maruyama S, et al. Enhanced expression ofpodoplanin in oral carcinomas in situ and squamous cell carcino-mas. Pathobiology 2011;78:171–180.
24. Tsuneki M, Yamazaki M, Maruyama S, Cheng J, Saku T. Podopla-nin-mediated cell adhesion through extracellular matrix in oralsquamous cell carcinoma. Lab Invest 2013;93:921–932.
25. Solomon D, Nayar R, editors. The Bethesda System for ReportingCervical Cytology: Definitions, Criteria, and Explanatory Notes.2nd ed. New York: Springer, 2004. p 21–56, 67-122.
26. Koch FP, Kunkel M, Biesterfeld S, Wagner W. Diagnostic efficien-cy of differentiating small cancerous and precancerous lesions usingmucosal brush smears of the oral cavity—a prospective and blindedstudy. Clin Oral Invest 2011;15:763–769.
27. Safaeian M, Solomon D, Wacholder S, et al. Risk of precancer andfollow-up management strategies for women with human papillo-mavirus–negative atypical squamous cells of undetermined signifi-cance. Obstet Gynecol 2007;109:1325–1331.
28. Marur S, D’Souza G, Westra WH, Forastiere AA. HPV-associatedhead and neck cancer: A virus-related cancer epidemic. LancetOncol 2010;11:781–789.
29. Divani S, Exarhou M, Theodorou LN, Georgantzis D, Skoulakis H.Advantages and difficulties of brush cytology in the identificationof early oral cancer. Arch Oncol 2009;17:11–12.
30. Funayama A, Maruyama S, Yamazaki M, et al. Intraepitheliallyentrapped blood vessels in oral carcinoma in-situ. Virchows Arch2012;460:473–480.
31. Watanabe N, Ohkubo T, Shimizu M, Tanaka T. Preneoplasiaand carcinogenesis of the oral cavity. Oncol Discov 2015;3:1.Available at: http://www.hoajonline.com/journals/pdf/2052-6199-3-1.pdf. Accessed on 9/9/2016.
32. Nauth HF. Benign changes of the female genital tract. Gynecologi-cal Cytology. New York: Thieme Press; 2007. p 127–146.
33. Nayar R, Wilbur DC, editors. The Bethesda System for ReportingCervical Cytology. Definitions, Criteria, and Explanatory Notes. 3rded. New York: Springer; 2015. p 29–89, 103-192.
34. Koss LG. Light microscopic estimation of cellular activity, injury,and death. In: Koss LG. editor. Diagnostic Cytology and its histo-pathologic basis. 3rd ed. vol.1 Philadelphia. Toronto: JB LippincottCompany; 1979. p 53–60.
Diagnostic Cytopathology DOI 10.1002/dc
HARA ET AL.
12 Diagnostic Cytopathology, Vol. 00, No 00