Embed Size (px)
Citation preview

Aimee Kelliher, SPT
1
Differential Diagnosis of Unilateral Upper Extremity Weakness: A Case Report
Background and Purpose. Many shoulder problems present with similar signs and symptoms of limited
motion, pain, and weakness. The differential diagnosis process can thereby present a challenge to
rehabilitation professionals. This report describes a student physical therapist’s evaluation per order
from a patient’s burn clinic for orthopedic consult for rotator cuff tear. It aims to illustrate the potential
value of differential diagnostic skills in the inpatient rehabilitation setting.
Case Description. A 52-year-old male was hospitalized due to burn injuries incurred as the result of a
home accident. Two days following initial inpatient therapy evaluations, the burn clinic ordered a
consult for rotator cuff tear. Subjective and objective data inconsistent with signs and symptoms of a
cuff tear led the student physical therapist to notify the patient’s physician regarding her findings.
Outcomes. The patient’s physician chose to run an electromyographic study of the left upper arm the
following day. Study results argued for brachial plexopathy. Inpatient rehabilitation was continued for
two weeks before the patient was discharged home with a recommendation for continued outpatient
physical therapy.
Discussion. Diagnoses in the inpatient environment affect multiple aspects of patients’ plans of care.
The course of physical therapy treatment for a patient with brachial plexopathy differs notably from that
which is appropriate following rotator cuff tear. Physical therapists have consistently been
demonstrated to be highly knowledgeable of musculoskeletal conditions and capable of recognizing
need for referral. Via the use of clinical examination skills, the student physical therapist in this case was
able to rule out a patient’s current diagnosis and come to an alternate conclusion, ultimately insuring a
more cost-effective inpatient stay and optimal patient outcome.
Manuscript Word Count: 3,497

Aimee Kelliher, SPT
2
Background and Purpose:
Shoulder injury is an ailment frequently presented to health care practitioners, having been reported in
the general population to be the third most common musculoskeletal disorder.1 Of the numerous
sources of shoulder dysfunction, the most common is rotator cuff tear.1 According to the American
Academy of Orthopedic Surgeons, 7.5 million physician visits occurred in 2006 due to shoulder issues
with about half of those attributable to cuff injuries.2 The frequency of full and partial-thickness tears
increases significantly with advancing age, evidenced by research which revealed that 4% of individuals
aged nineteen to thirty-nine and 54% of those aged greater than sixty exhibited cuff tears via MRI.3
Patients with shoulder injury are quite familiar to the rehabilitation environment. According to the
American Physical Therapy Association’s (APTA) Guide to Physical Therapist (PT) Practice, PTs have the
responsibility of forming a therapy diagnosis for each patient which encompasses not only impairments
and functional limitations, but also diseases and disorders when applicable.4 Therefore, it is important
for rehabilitation professionals to be able to perform accurate differential diagnosis and evaluation of
individuals with shoulder dysfunction.
The challenge comes with the reality that a multitude of shoulder problems tend to present with similar
signs and symptoms of limited motion, pain, and weakness. Sources of symptoms include, but are not
limited to, subacromial impingement, joint dislocation, ligament sprain, musculo-tendinous tear,
neurological insult, altered capsule extensibility, fracture, and other joint pathology.1,5
The purpose of this case report is to describe a student physical therapist’s evaluation of a patient
recently admitted to acute rehabilitation per order from the patient’s burn clinic for orthopedic consult
for rotator cuff tear. The student physical therapist (SPT) was currently in her fourth clinical rotation
and anticipating graduation in four months. Subjective and objective data inconsistent with signs and
symptoms of a cuff tear led the student to notify the patient’s physician regarding her findings. This
report aims to illustrate the potential value of clinical testing and differential diagnostic skills in the
inpatient rehabilitation setting.
Case Description: Patient History and Systems Review:
A 52-year-old man of slender build was hospitalized due to burn injuries incurred as the result of a home
accident. Burns totaled 15% of his total body surface area and were located over parts of his face, scalp,
ears, neck, forearms, and hands. He had also experienced inhalation injury and was intubated for
seventeen days following admission to the hospital. The patient was referred to inpatient rehabilitation
by his burn clinic, which remained responsible for all of his wound care, thirty-one days after admission.
Orders were sent for physical and occupational therapy evaluation and treatment. At this time, per
physician report, the patient “denie[d] chest pain, shortness of breath, nausea, vomiting, or diarrhea.”
Past medical history included chronic alcohol and poly-substance abuse and no past surgeries.

Aimee Kelliher, SPT
3
Examination of the patient’s lower extremities, trunk, and physical mobility status was completed by a
PT, while examination of the upper extremities and ability to perform activities of daily living (ADL) was
performed by an occupational therapist the next morning. A speech language pathologist deemed the
patient’s orientation, expressive and receptive language, memory, and executive functioning within
normal limits.
An order was sent from the burn clinic two days following initial evaluations requesting an orthopedic
consult for rotator cuff tear. The patient had been receiving a total of three hours of physical and
occupational therapy daily in order to improve his static and dynamic seated and standing balance while
transferring, toileting, dressing, ambulating, and climbing stairs. He had also been working on donning/
doffing his compression gloves and exhibited increased time and effort with all ADL. Before the
incident, the patient was independently able to perform all physical mobility and ADL. His therapy goal
was to return to independent function. When asked to verbalize his main complaint, the patient
reported left arm weakness which he had first noticed on the day of admission to acute rehabilitation.
Clinical Impression #1:
The patient seemed a good candidate for consultation as he was approaching his mid-50’s, had
experienced a traumatic incident, and was complaining of significant arm weakness. “Weakness is the
primary sign of loss of integrity of the rotator cuff” and one common method of incurring cuff tears is as
the result of trauma.1 The patient’s mechanism of injury needed to be elaborated upon to gain more
differential information. Other classic signs associated with rotator cuff tear include: positive Neer
and/or Hawkins impingement test/s; drop arm sign (more severe cases); pain with resistance of the
supraspinatus or infraspinatus muscles; painful arc of abduction; loss of active motion (particularly into
abduction); loss of external rotation (massive tears); supraspinatus atrophy; and night pain.1,6 Although
pain is classically coupled with a rotator cuff tear, if the tear spans the full-thickness of a tendon, the
patient may have no pain.1 The chances of incurring a painless, full-thickness tear are not substantial,
however, resulting in the SPT’s desire to attempt to produce painful symptoms with additional tests and
measures. Clinical reasoning was that the patient may have reduced activity of his weak, non-dominant,
extremity significantly enough during the course of his hospitalization due to its impaired ability, that he
had not allowed it to reach any painful point/s in his shoulder active range of motion (AROM). The
patient’s weakness needed to be localized and tied specifically to certain cuff muscles in order to better
pinpoint the location of insult and tailor his plan of care.

Aimee Kelliher, SPT
4
Examination:
The consultation began the morning after receiving the order with the SPT observing AROM of the
upper extremities as described by Norkin, White, and Magee.7,8 She began with the bilateral shoulders
and progressed to the elbows, forearms, wrists, hands, and cervical spine. Glenohumeral (GH) joint
adduction, horizontal adduction, and horizontal abduction were excluded from testing. Significant
findings included: impaired abilities to flex, abduct, extend, and rotate the left shoulder; difficulty
extending the left elbow; and trouble supinating the left forearm. Ranges of motion were visually
estimated to be no more than 15 to 20 degrees. Visual estimation of shoulder AROM has been
suggested to be acceptable to identify differences between affected and contralateral extremities within
subjects with an ICC >.70 .9 The patient was able to flex his left elbow, pronate his left forearm, and
move his left wrist and hand fully, however did so with increased time and caution. Next, PROM was
tested for all motions of the left GH joint, elbow, forearm, and wrist and estimated visually to be within
normal limits. Lastly, a slightly inferiorly subluxed left GH joint was observed compared to the right,
which can be done by noting increased vertical space between the acromioclavicular joint and head of
the humerus.8
The SPT subsequently tested resisted isometric motions (RIM) of the patient’s left upper extremity as
described by O’Sullivan and Magee with the patient in sitting.8,10 The hand was tested via grip strength.
Results were all weak and painless. Examination of left rotator cuff muscle function was attempted via
special testing, including the full can test for the supraspinatus, infraspinatus muscle strength test,
hornblower’s test for the teres minor, and abdominal compression test for the subscapularis as outlined
by Magee.8 The patient was unable to assume initial testing positions for the supraspinatus and teres
minor tests and exhibited extreme weakness with infraspinatus and subscapularis testing. The
infraspinatus muscle test holds an overall 90.1% specificity and 41.6% sensitivity for the identification of
tendinitis, partial and full thickness tears, and bursitis, while the abdominal compression test has
specificity of 98% and sensitivity of 40% for detecting subscapularis pathology.11, 12 A neurological
screen was then completed, consisting of deep tendon reflexes (DTR) for the bilateral biceps brachii,
brachioradialis, and triceps brachii muscles, light touch sensation of the left upper extremity dermatome
key points, and light touch over larger areas of the left upper extremity in order to identify possible
peripheral nerve involvement. Published data regarding the validity and reliability of these commonly-
utilized neurological clinical tests is limited. The left C4 myotome was also tested via shoulder shrug
ability, as the musculature it innervates was not activated by AROM or RIM, and was found to be
normal. Reflexes were measured as illustrated by Magee and found to be decreased bilaterally, 1+/4+
on the deep tendon reflex grading scale.8 Light touch was tested with the patient in sitting using the
fingertips for contact. Gentle side-to-side rubbing was applied to the surface of the skin over each
dermatome key point as defined by the American Spinal Injury Association beginning with C1 and ending
with T2. Each main peripheral-nerve-innervated area as illustrated by Netter was also tested.13
Sensation of the patient’s cheek, which he reported to feel normally, was used as a reference. Without
looking, the patient was asked to localize the touch and report if it felt differently from the cheek
sensation. If so, he was asked to describe how it was different. Dermatome key points were unaffected
except for mild to moderate decreased sensation over the medial epicondyle. Peripheral nerve testing

Aimee Kelliher, SPT
5
revealed that the lateral upper arm was affected with the same decreased sensation as the epicondyle.
The SPT then asked the patient his mechanism of injury. He was unable to identify an incident in
particular, but did report that he had run into a door leading with his left shoulder while escaping from
the fire. The SPT lastly palpated the supraclavicular fossa on the anterior neck, resulting in localized pain
on the involved side. Palpation of the supraclavicular fossa for pain has been identified to be
appropriate for diagnosis of thoracic outlet syndrome, which involves compression of the neurovascular
structures near the antero-lateral neck.14 The entire examination process had lasted ten to fifteen
minutes. Tables 1 and 2 provide examination findings.
Clinical Impression #2:
The primary initial thought during the examination process was that the patient’s level of weakness was
uncharacteristically extensive for a rotator cuff tear. Not only were the cuff muscles affected, but elbow
prime movers were as well. It was firstly evident that the deltoid muscle was involved. It is a prime
mover for higher degrees of shoulder flexion, abduction, and extension. The patient could initiate all of
these movements, but could not complete them. The patient was also extremely limited into active
external rotation, of which the teres minor and infraspinatus are the main agonists. Internal rotation
was impaired as well, which is governed by the subscapularis, pectoralis major, and latissimus dorsi
muscles.15 Considering the lack of elbow extension and forearm supination, it could also be concluded
that the triceps brachii, anconeus, supinator, and/or biceps brachii muscle/s were affected in some
capacity.16 Other muscles of the arm could not be discounted either due to the quality of movement
noted with elbow flexion, forearm pronation, wrist, and hand AROM.
RIM testing was performed as a follow-up test and measure to AROM due to the fact that pain
reproduction with this test is a good indicator of local contractile tissue damage.10 Although AROM was
not painful, the SPT postulated that by adding resistance to movement, which requires increased force
production and recruitment of motor units, pain may have occurred. The RIM result of “weak and
painless” is indicative of a disorder of the nervous system, injury to the neuromuscular junction,
complete rupture, or disuse atrophy.10 The SPT deemed it unlikely that the patient completely ruptured
as many muscles as it would take to produce such weakness. Disuse atrophy was ruled out along the
same line of reasoning that weakness was too severe. Therefore, following RIM testing, it was
determined that the root cause of the patient’s symptoms was likely neurological in nature. Inferior
subluxation of the GH joint observed during AROM provided additional support for this thought, as
subluxation is often noted when loss of muscle control occurs secondary to a stroke or other nerve
injury.8 Possibilities included dysfunction of the central nervous system (CNS), spinal nerve root
compression, or peripheral nerve insult. Although reflexes were not normal, since they were decreased
bilaterally the results were deemed insignificant.8 Dominant weakness, a unilateral presentation
without hyperreflexia, and no other upper neuron lesion signs or symptoms, such as ataxia or cognitive
changes, allowed the CNS to be ruled out as source of symptoms.17 Sensory testing provided the

Aimee Kelliher, SPT
6
knowledge that either the T1 nerve root, medial brachial cutaneous peripheral nerve, C5 nerve root,
and/or axillary nerve were affected. The SPT supposed it much more likely for the patient in question to
have incurred peripheral nerve injuries during the time span from the burn incident to his arrival to
therapy than to have obtained two affected nerve roots four levels apart. If a root is impaired, both its
dermatome and myotome will show signs of involvement, which was not the case with this patient, who
had no discernible nerve root pattern of neurological impairment.18 Multiple peripheral nerves were
clearly affected based upon the extent of the deficits. According to light touch sensation testing
findings, the patient’s left axillary and medial brachial cutaneous nerves were involved. Based upon the
muscular weakness identified during AROM and RIM findings, the axillary, radial, and several other
upper extremity nerves were potentially involved based upon the muscles they innervate. For example,
the axillary nerve innervates the deltoid and teres minor muscles, while the radial nerve innervates the
triceps brachii and supinator muscles.
At this point in the examination process, the SPT surmised the patient’s left brachial plexus as the likely
source of symptoms. Multiple nerve fibers join together to form a close network in the plexus as they
exit C5 through T1 vertebral foramina. Damage to this area can easily affect several peripheral nerves.
The SPT questioned the patient regarding his mechanism of injury in order to gain support for this
hypothesis by determining if it was likely to have caused damage to the plexus. Brachial plexus injury
most commonly occurs via closed nerve traction or compression.19,20 After surmising that the patient’s
mechanism could have indeed pulled his head and neck away from his shoulder, resulting in traction,
pain with palpation of the left supraclavicular plexus finalized the student’s hypothesis of brachial
plexopathy.
Outcome:
The SPT notified the patient’s physician the next day regarding her findings, explaining that signs and
symptoms did not seem consistent with a rotator cuff tear. All notable AROM, RIM, and sensation
testing findings, as well as the patient’s possible mechanism of injury, were mentioned.
The physician chose to run an electromyographic (EMG) study of the left upper arm “for suspected
neuropathy involving LUE” (left upper extremity) the following day. Study results were found to be
abnormal for the deltoid and biceps brachii muscles. The deltoid exhibited decreased recruitment while
the biceps brachii had recruitment within normal limits but exhibited positive sharp waves (PSW). The
triceps brachii, supraspinatus, and infraspinatus muscles, on the other hand, were without abnormal
spontaneous activity. The physician did note, however, that “EMG findings may not be abnormal even
in presence of neuropathy for up to six weeks post-injury, so lack of abnormal findings in other muscles
does not necessarily exclude a more extensive nerve injury.” The patient was only about five weeks
from initial injury at the time the study was run. Overall, the physician concluded, in investigating “left
cervical radiculopathy versus upper trunk plexopathy…. Presence of sensory abnormal argue[d] for
plexopathy.”

Aimee Kelliher, SPT
7
Inpatient physical and occupational therapy was continued for the next two weeks, focusing on active
use of the involved extremity without undue stress on the shoulder. Neuromuscular control of the
extremity improved, though strength on a manual muscle test scale did not. The patient advanced all of
his ADL Functional Independence Measure scores from 3- 5 up to 6 and was discharged home with a
recommendation for continued physical therapy in the outpatient setting to continue to increase
function of the LUE and decrease time and effort with daily tasks.
Discussion:
Brachial plexopathy accounts for 14% of all upper extremity neurological disorders and 10% of all
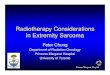
peripheral nerve problems.21 Supraclavicular injuries are more common than infraclavicular, with
incidence in one report as 72% supraclavicular versus 28% infraclavicular in a total of 509 traction
injuries.22 The supraclavicular plexus is divided into three trunks, the upper, middle, and lower plexus
(Figure 1). Upper plexus injuries are the most common of the three, usually occurring as a result of
closed traction, while avulsion is more often the cause of lower plexus pathology. Likely possibilities in
this patient case were self-injury in the home before hospital arrival, as surmised by the SPT at the time
of examination, or sustained postoperative paralysis, which stems from multiple surgical factors,
including prolonged patient positioning and loss of muscle tone due to anaesthesia.19 According to its
typical presentation of painless weakness and paresthesias, while the former exhibits paresthesias and
pain, the latter actually seems a more fitting etiology for this patient.
Classic signs of brachial plexus insult include tenderness over the plexus and weakness in muscles
innervated by involved portions of the plexus.6 These signs were evidenced in this patient, while certain
signs of rotator cuff tear were not, such as pain with abduction AROM, with resisted motions, and at
night. Impingement and drop arm testing were not performed with the patient since he was unable to
assume proper initial testing positions. Certain other classic signs of rotator cuff tear were illustrated by
the patient, such as loss of active motion and weakness. This could likely be the reason the patient’s
burn clinic ordered a consult for rotator cuff tear. Loss of motion for cuff tears is particularly into
shoulder abduction and external rotation, however, and this patient had nearly equal losses in all
motions of the shoulder as well as more distally. Much research regarding cases of plexopathy occurring
due to various mechanisms exists in the literature. Explanations of clinical decision-making processes
behind diagnoses are limited, however, with the most applicable research report describing the
differential diagnostic process behind suprascapular neuropathy in patients with shoulder dysfunction
and diagnoses of subacromial impingement.24
It is essential for patients to be fitted with correct diagnoses in the inpatient environment as it affects
multiple aspects of their plans of care, including medical services, rehabilitation treatment, and
reimbursement. With health care reform on the rise, it is becoming increasingly important for health
care facilities to emphasize controlling their expenditures.25,26 This is of particular concern to units
which accept a high percentage of patients with Medicaid insurance, such as the facility which

Aimee Kelliher, SPT
8
accommodated the patient in this report. As is widely recognized by the healthcare community, the
value for a stay reimbursed by Medicaid is significantly lower than any other insurance. The earlier an
accurate patient diagnosis is confirmed, the sooner a proper plan of care may be formulated and
administered. The sooner the patient will then theoretically make gains, meet his/her goals, and be
discharged from therapy, resulting in a more cost-effective patient stay.
The course of a plan of care for a patient with brachial plexopathy differs notably from that which is
appropriate following rotator cuff tear. Only a brief period of immobilization to minimize inflammation
and tension on the area immediately follows injury or surgery to the plexus before beginning movement
as soon as possible. Movement minimizes adhesions and contractures and assists in regeneration of
affected nerve pathways.20, 26 Conservative treatment for a chronic rotator cuff tear, on the other hand,
involves a four-week period progressing from shoulder PROM to active-assisted ROM while completely
avoiding abduction and flexion with pronation due to risk of greater damage or pain due to
impingement.6 Ice is indicated as a modality for cuff tear during early rehabilitation whereas it is not
particularly indicated with plexopathy as it serves to slow nerve conduction, which is essential to
maintain the viability of target tissue during recovery.26 Conversely, electrical stimulation may be used
with plexopathy to assist in motor retraining, while it is not specified for use with a cuff tear.20
Conclusion:
The case has already been made for the value of differential diagnostic skills in the outpatient PT setting
to reduce healthcare utilization as a result of direct access and APTA Vision Statement for PT 2020,
arguing that PTs are highly knowledgeable of musculoskeletal conditions and highly capable of
recognizing the need for referral due to the presence of a condition that is not neuromusculoskeletal in
nature or needs further evaluation by another healthcare professional.4,27-29 Via the use of clinical
examination skills in the inpatient setting, the SPT in this case was able to rule out a patient’s current
diagnosis and come to an alternate conclusion of brachial plexopathy in less than a quarter of an hour,
ultimately insuring a better outcome for the patient. If she had not been familiar with differential
diagnosis of the shoulder joint and able to distinguish between neurological and musculoskeletal injury,
the patient may have retained an improper diagnosis and been treated with an unsuitable plan of care
throughout his stay. Functional abilities likely would not have progressed as well and his stay would
have resulted in less than desirable resource utilization and overall patient outcome.

Aimee Kelliher, SPT
9
Table 1.
Left Upper Extremity ROM and Strength Test & Measure Findings
Joint Motion Tests and Measures
AROM PROM RIM
Shoulder
Flexion X X
Extension X X
Abduction X X
ER X X
IR X X
Elbow Flexion _ X
Extension X X
Forearm Pronation _ X
Supination X X
Wrist All motions _ X
Hand All motions _ X
Cervical spine All motions Not tested
“X” indicates abnormal result; “--” indicates abnormal result due to quality of motion only

Aimee Kelliher, SPT
10
Table 2.
Left Upper Extremity Neurological Test & Measure Findings
Nerve/Root Tests and Measures
Light Touch DTR
C1
C2
C3
C4
C5 X
C6
C7
C8
T1 X
T2
Supraclavicular
Axillary X
Dorsal antebrachial cutaneous
Medial antebrachial cutaneous
X
Lateral antebrachial cutaneous
Median
Ulnar
Radial
“X” indicates abnormal result


Aimee Kelliher, SPT
12
Figure 1.
Brachial Plexus
Obtained from Wikimedia Commons at http://en.wikipedia.org/wiki/File:Brachial_plexus_2.svg.

Aimee Kelliher, SPT
13
References:
1. New Zealand Guidelines Group. The Diagnosis and Management of Soft Tissue Shoulder Injuries and Related Disorders: Best Evidence-Based Practice Guideline. 2004. http://www.acc.co.nz/PRD_EXT_CSMP/groups/external_communications/documents/guide/wcm001684.pdf. Accessed April 10, 2012.
2. New therapy device decreases costs for shoulder injuries. PRNewswire. http://www.prnewswire.com/news-releases/new-therapy-device-decreases-costs-for-shoulder-injuries-142609446.html. 2012. Accessed April 10, 2012.
3. Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal Findings on Magnetic Resonance Images of Asymptomatic Shoulders. The Journal of Bone and Joint Surgery. 1995; 77:10-15.
4. Deyle GD. Direct Access Physical Therapy and Diagnostic Responsibility: The Risk-to-Benefit Ratio. Journal of Orthopaedic and Sports Physical Therapy. 2006;36(9):632-634.
5. Walsworth MK, Mills JT III, Michener LA. Diagnosing suprascapular neuropathy in patients with shoulder dysfunction: a report of 5 cases. Physical Therapy. 2004;84(4):359–72.
6. Brotzman SB, Wilk KE. Clinical Orthopaedic Rehabilitation. 2nd ed. Philadelphia, PA: Mosby; 2003.
7. Norkin C C, White DJ. Measurement of Joint Motion: A Guide to Goniometry. 4th ed. Philadelphia, PA: F. A. Davis; 2009.
8. Magee DJ. Orthopedic Physical Assessment. 5th ed. St. Louis, MO: Saunders-Elsevier; 2008.
9. Dinnes J, Loveman E, McIntyre L, Waugh N. The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review. Health Technology Assessment. 2003;7:1–166.
10. O’Sullivan SB, Schmitz T.J. Physical Rehabilitation. 5th ed. St. Louis: F. A. Davis; 2007.
11. Park HB. Yokoia A, Gill H, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial Impingement syndrome. The Journal of Bone and Joint Surgery. 2005;87(7):1446-1455.
12. Barth JR, Burkhart SS, De Beer JF. The bear-hug test: a new and sensitive test for diagnosing a subscapularis tear. Arthroscopy. 2006;22:1076-1084.
13. Netter F. H. Atlas of Human Anatomy. 4th ed. Philadelphia, PA: Saunders Elsevier; 2006.
14. Muscles. American Society for Surgery of the Hand. http://www.assh.org/Public/HandAnatomy/Muscles/Pages/default.aspx. 2011. Accessed April 10, 2012.
15. Hooper TL, Denton J, McGalliard MK, Brisme J, Sizer PS. Thoracic outlet syndrome: a controversial clinical condition: part 1: anatomy, and clinical examination/diagnosis. Journal of Manual and Manipulative Therapy 2010; 18(2):74-83.
16. American Spinal Injury Association. International Standards for Neurological Classification of Spinal Cord Injury. Atlanta, GA; 2011.
17. Goodman CC, Fuller KS. Pathology: Implications for the Physical Therapist. St. Louis, MO: Saunders Elsevier; 2009.

Aimee Kelliher, SPT
14
18. Beers, M. H., Porter R.S., Jones T. V., Kaplan J. L., Berkwits M. The Merck Manual of Diagnosis and Therapy. Whitehouse Station: Merck Research Laboratories; 2006.
19. Ferrante MA. Brachial plexopathies: Classification, causes, and consequences. Muscle and Nerve. 2004;30(1):547-568.
20. Kisner C, Colby L. Therapeutic Exercise: Foundations and Techniques. 5 ed. Philadelphia, PA: F.A. Davis; 2002.
21. McKinley W. Brachial Plexopathies. www.pmr.vcu.edu/presentations/pps/Brachial_Plexopathies2001.pps. Accessed April 11, 2012.
22. Kim DH, Murovic JA, Tiel RL, Kline DG. Infraclavicular brachial plexus stretch injury. Neurosurgical Focus. 2004;16(5):E4.
23. Fredericks CM, Saladin LK. Pathophysiology of the Motor Systems: Principles and Clinical Presentations. Philadelphia: F.A. Davis; 1996.
24. Walsworth MK,Mills JT 3rd, Michener LA. Diagnosing suprascapular neuropathy in patients with shoulder dysfunction: a report of 5 cases. Physical Therapy. 2004;84(4):359-72.
25. Clune S, Kane J. Why Does Health Care Cost So Much in the United States? PBS. http://www.pbs.org/newshour/rundown/2011/11/why-does-healthcare-cost-so-much.html. 2011. Accessed April 11, 2012.
26. Colwell J. Reducing unessessary testing: Physician’s urged to consider “what’s needed” instead of “what’s possible.” http://www.acphospitalist.org/archives/2011/07/coverstory.htm. November 2011. Accessed April 11, 2012.
27. Mitchell JM, de Lissovoy GA. A comparison of resource use and cost in direct access versus physician referral episodes of physical therapy. Physical Therapy. 1997;77(1):10-18.
28. Goodman CC, Kelly-Snyder TE, eds. Differential Diagnosis for Physical Therapists: Screening for Referral. 4th ed. St. Louis, MO: Elsevier; 2008.
29. Childs JD. Whitman JM. Sizer PS, Pugia ML, Flynn TW, Delitto A. A description of physical therapists' knowledge in managing musculoskeletal conditions. BMC Musculoskeletal Disorders. 2005;6(32):1-7. doi:10.1186/1471-2474-6-32.