Embed Size (px)
Citation preview

Injury, Int. J. Care Injured 43 (2012) 96–102
Difficulties in establishing long-term trauma outcomes data collections.Could trauma outcomes be routinely monitored in New South Wales,Australia: Piloting a 3 month follow-up?
Rebecca Mitchell a,b,*, Wendy L. Watson a, Kate Curtis a,c, Ian Harris d, Patricia McDougall e
a NSW Injury Risk Management Research Centre, University of New South Wales, Sydney NSW 2052, Australiab School of Aviation, University of New South Wales, Australiac St George Public Hospital, Sydney Australia and Sydney Nursing School, University of Sydney, Australiad South Western Sydney Clinical School, University of New South Wales, Australiae New South Wales Institute of Trauma and Injury Management, Australia
A R T I C L E I N F O
Article history:
Accepted 5 January 2011
Keywords:
Trauma outcomes
Methodology
Implementation
A B S T R A C T
Injuries represent a significant health burden in Australia. In New South Wales (NSW), no routine follow-
up of post-injury health outcomes is conducted. This article describes the development of a protocol and
the conduct of a pilot study to collect information on trauma outcomes at 3 months post-injury at two
trauma centres. A modified Victorian model of trauma outcomes monitoring was adopted, with potential
participants required to ‘opt in’ to the collection. Fifty-three percent of individuals contacted consented
to opt in, with 75% of these completing an interview. The data items collected were able to provide an
indicator of the impact of trauma on individuals. This study has highlighted that there are important
methodological issues to be addressed in terms of recruitment in establishing long-term trauma
outcomes data collections that are representative of the trauma population. Ultimately, information
from a long-term trauma outcomes collection could be linked to data collections to conduct research
across the injury continuum.
� 2011 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
Introduction
Injuries, whilst largely preventable, represent a significanthealth burden around the world24 and in Australia.5 New SouthWales (NSW) is the largest populated State in Australia, witharound 7.2 million residents,3 and approximately 2300 individualsare seriously injured (Injury Severity Score (ISS) > 15) and receivespecialist care at trauma centres in NSW each year.29 Traumaticinjuries leave many individuals with severe disabilities andchronic conditions that affect their health-related quality of life(HRQoL) and often require long-term health care.
Recovery from serious injury can be lengthy as individualsattempt to regain pre-injury functional ability.18 The impact ofserious injury on individuals generally, in terms of ability to performactivities of daily living (ADL), care needs, and measures of HRQoL,including physical and emotional long-term effects, are not wellquantified in NSW. Specific studies have been conducted to identifyboth short- and long-term trauma outcomes in a number ofcountries, including the United States,18,22,25,30 Taiwan,20 NSW,17
Queensland1 and New Zealand10 using questionnaires and/or
* Corresponding author. Tel.: +61 2 9385 7379, fax: +61 2 9385 6040.
E-mail address: [email protected] (R. Mitchell).
0020–1383/$ – see front matter � 2011 Elsevier Ltd. All rights reserved.
doi:10.1016/j.injury.2011.01.006
interviews with individuals post-injury, but none of these studiescollect data on a routine, ongoing basis. Victoria is the only state inAustralia where trauma outcomes are routinely monitored throughthe Victorian State Trauma Outcomes Registry (VSTOR)16 and theVictorian Orthopaedic Trauma Outcomes Registry (VOTOR).33
The routine monitoring of HRQoL outcomes post-injury could beused for quality assurance purposes to examine the effectiveness ofdifferent types of trauma treatment, to identify factors that mayspeed or restrict the recovery process, and to monitor resourcedemand for rehabilitation and health-related auxiliary services.Whether or not a system for monitoring long-term trauma outcomescould be implemented in NSW needs to be investigated. The aim ofthis research is to pilot the development and collection of long-termtrauma outcomes data in NSW at 3 months post-injury.
Method
The VSTOR model was used as a basis for the trial of the NSWtrauma outcomes data collection, in terms of the information to becollected and the data collection protocol. VSTOR was establishedin response to a Ministerial Review of Trauma and EmergencyServices and uses an ‘opt out’ policy for initial entry into theregistry to minimise potential recruitment bias.9 In Victoria, underthe opt out policy, trauma patients are sent a participant

R. Mitchell et al. / Injury, Int. J. Care Injured 43 (2012) 96–102 97
information sheet regarding their inclusion in the registry andinformation regarding procedures to follow if they wish to beremoved from the registry. Consent is obtained from traumapatients at the time of follow-up when they are contacted bytelephone for interview.
Ethical approval
Ethical approval for the pilot study to collect the traumaoutcomes data was sought from the NSW Population and HealthServices Research Ethics Committee (PHSREC). The PHSREC wouldnot approve the use of an opt out procedure for initial recruitmentinto the trauma outcomes study as is conducted in Victoria16 andNew Zealand.10 Instead, consent to contact was required to beobtained in hospital (see Enrolment in pilot study section) andparticipants were required to be given two opportunities to opt outof the outcomes study after they had consented to be contacted.The first when they received a second participant informationsheet in the mail (see Enrolment in pilot study section), and thesecond, when they were contacted by interviewers (see Long-termtrauma outcomes minimum dataset section). Ethics approval fromPHSREC (No.: 09/CIPHS/25) for the trauma outcomes study wasgranted on the proviso that this recruitment protocol was used.This approval was ratified by the UNSW Human Research EthicsCommittee (Ref.: 09283).
Case identification and inclusion criteria
Following presentation to the Emergency Department (oradmission following transfer), medical staff with the hospital’strauma team determined if an individual met the case inclusioncriteria. The inclusion criteria were any injured individual, aged 18years and over, who had the presence of at least one of the following:
(i) admission to an intensive care unit > 24 h requiring mechani-cal ventilation;
(ii) injury severity score > 15 (ISS > 15); or(iii) urgent surgery (intracranial, intrathoracic or intra-abdominal
injury, or for fixation of pelvic or spinal fractures).
Individuals who did not speak English were excluded from thepilot study as funding was not available for interpreter services.Also excluded were individuals who had a serious to critical headinjury (identified using the Abbreviated Injury Scale (AIS)2 scoregreater than or equal to 3) as valid, comparable caregiver proxymeasures of health outcomes were not available for all instru-ments used in this study. The proportion of individuals who wereexcluded because they were non-English speakers or had a seriousto critical head injury was recorded.
Data collection at the trauma service
Both of the trauma centres participating in the pilot study weremajor referral hospitals in NSW who each treated just over 10% ofall severe trauma (i.e., ISS > 15) in NSW. Each trauma centreroutinely collected information on patients who present to eachcentre and for patients with an ISS > 15 their data is provided forinclusion in the NSW Trauma Registry.29 Information recorded inthe NSW Trauma Registry includes information collected inhospital regarding the trauma patient, circumstances of theincident and the treatment the patient received. However, theamount of information collected by each individual trauma servicevaries but includes: gender, age, date of injury, time of injury,mechanism of injury, place of injury, date of arrival, time of arrival,mode of arrival, Intensive Care Unit (ICU) admission, ICU length ofstay, separation status, AIS, ISS, and length of stay. In addition, for
the trauma outcomes study each patient’s contact details(telephone and postal address) were recorded by the traumacentre. For each patient that met the case inclusion criteria, anidentification number was assigned.
Enrolment in pilot study
Potential participants were contacted, prior to discharge, by thehospital Trauma Co-ordinator (or their assistant) and providedwith a participant information sheet containing details about thepurpose of the trauma outcomes pilot study, the information beingcollected, and how the information was to be collected. Theinformation sheet also informed the participant that they would becontacted via telephone at 3 months post-injury to participate in afollow-up survey about their post-injury health outcomes and thatinformation from their interview would be combined withinformation about their hospital stay, their injuries, and thetreatment they received whilst in hospital. If the participant washappy to be contacted, they were asked to sign a form authorisingthe hospital to provide their contact details and some basicinformation about their injury to the research team. Participantswere asked to provide their full name, address and telephonenumbers (mobile and alternate number) and mechanism of injury(e.g. motor vehicle crash and fall). Once a signed permission tocontact form was obtained by the hospital, the Trauma Co-ordinator forwarded the contact details to the research team.
Two weeks prior to being telephoned, participants weremailed a second participant information sheet by the researchteam that contained details of their inclusion in the traumaoutcomes data collection, the purpose of the collection, theinformation being collected, and what to do if they wish to beremoved from the collection. The information sheet alsoinformed the individual that they would be contacted viatelephone at 3 months post-injury to inquire about their health.If they wished to be removed from the trauma outcomes datacollection, an individual simply left a telephone message (i.e.,their name and admitting hospital) to this effect. Deathsoccurring in hospital for participants in the study cohort wereidentified within each participating hospital’s trauma centre’sdata registry. If a participant had died post-discharge, con-dolences were offered and the call terminated.
Telephone interviews
Trained interviewers, employed by the NSW Health Depart-ment’s NSW Health Survey Program (except ‘program’ incomputers), telephoned each participant at 3 months post-injuryto inquire about their health outcomes. During the telephone call,the interviewer confirmed that the participant received theparticipant information sheet regarding the trauma outcomesdata collection in the mail and gave them the opportunity towithdraw from the study. Up to five call-backs were undertaken, atvarious times of day, in an attempt to contact the participant,before the participant was considered lost to follow-up.
All interviewers signed a Code of Conduct and a ConfidentialityAgreement. Interviewers only had access to the participant’s name,contact phone number and mechanism of the injury. Theinformation on the cause of the injury was provided to theinterviewers in order to establish the context surrounding theinjury event and to ensure interviewers are aware of sensitivitiesthat might exist around the event.
Long-term trauma outcomes minimum dataset
Interviewers used a standardised telephone protocol to collectinformation on the participant’s functional capacity, health status

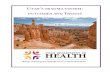
Number o f potential partici pants that w ere eligib le to be rec rui ted was: n=176
Number o f eligib le particip ants who died was: n=1 6
Number o f eligib le particip ants that w ere excluded du e to se rious to critic al h ead in jury was: n=92
Number o f eligib le partici pants who r efus ed to partici pate was: n=1 4
Number o f partici pants: n=36
Number o f eligib le partici pants that w ere no t aske d to pa rticipa te: n= 18
Fig. 1. Summary of eligible participants and participant response.
R. Mitchell et al. / Injury, Int. J. Care Injured 43 (2012) 96–10298
and quality of life using validated instruments. The interview tookbetween 10 and 15 min to complete and included:
� Current residential status, including: at home without additionalcare; at home with additional care; other response;� Short-form 12 Health Survey (SF-12);� Glasgow Outcome Scale – Extended (GOSE);� Occupation and education;� Working or studying before injury? – yes/no;� Return to work or study? – yes/no; and� Capacity of return to work or study? – full-time or reduced
capacity (modified duties and/or reduced hours).
Data linkage – NSW trauma data and the trauma outcomes data
collection
Each trauma centre provided the research team with the datacollected in their trauma centre’s registry for individuals whohad consented to contact. No identifying information (i.e., name,address) was contained in the data provided and data was thenlinked by the research team to the information collected in thetelephone interviews using the study participant identificationnumbers. De-identified demographic information on all exclud-ed cases and refusals was also provided for comparativepurposes.
Analysis was performed using SAS version 9.1.31 A t-test wasused to compare continuous variables between participants andnon-participants. To examine the association between participantsand non-participants and categorical variables, a chi-square test ofindependence or Fisher’s exact test was used. For the chi-squareanalysis, place of incident was grouped into ‘street/highway’,‘home’ and ‘other specified place’ and injury mechanism wasgrouped into ‘road traffic-related’ and ‘fall and other’.
Results
During the recruitment period, 176 patients were assessed forinclusion in the study. Of these, 92 (52.3%) patients were excludeddue to serious to critical head injures and 16 (9.1%) patients died.Of the remaining 68 patients who were eligible to participate, 18
Table 1Comparison of participants and non-participant characteristics.
Characteristics Participants (n = 36)
Age, mean (range) 42.9 (18–82)
Sex (%)
Male 28 (77.8)
Female 8 (22.2)
Injury mechanism (%)
Road traffic-related 23 (63.9)
Motor vehicle crash 11 (30.6)
Motor cycle crash 4 (11.1)
Pedestrian 7 (19.4)
Pedal cycle 1 (2.8)
Fall and other 13 (36.2)
Fall 11 (30.6)
Violence 0 (0)
Recreation 1 (2.8)
Other and not known 1 (2.8)
Place of incident (%)
Street/highway 23 (63.9)
Home 7 (19.4)
Other specified place 6 (16.8)
Trade and service area 2 (5.6)
Residential institution 1 (2.8)
Industrial workplace 2 (5.6)
Sports and athletic areas 0 (0)
Other and not known specified places 1 (2.8)
Injury severity score, mean (range) 25.2 (10–50)
(26.5%) were not asked to participate due to the holiday leave ofone of the study site coordinators and 14 (20.6%) patients refusedto participate. Thirty-six (52.9%) patients consented to becontacted by the study investigators to participate in the research(Fig. 1).
There were no significant differences between patients whoconsented to participate and those who did not participate by age(t(66) = �0.32, p = 0.75), ISS (t(66) = �0.22, p = 0.8), gender
Non-participants (n = 32) Test statistic and p-value
44.6 (18–96) T(66) = �0.32; p = 0.75
x2 = 0.12, df = 1, p = 0.7
26 (81.3)
6 (18.8)
x2 = 0.81, df = 1, p = 0.4
17 (53.1)
9 (28.1)
5 (15.6)
2 (6.3)
1 (3.1)
15 (47.0)
10 (31.3)
2 (6.3)
1 (3.1)
2 (6.3)
x2 = 1.38, df = 2, p = 0.5
16 (50.0)
8 (25.0)
8 (25.1)
2 (6.3)
2 (6.3)
1 (3.1)
0 (0)
3 (9.4)
25.7 (16–57) T(66) = �0.22; p = 0.8

Table 2Interviewed participant characteristics (n = 27).
Characteristics n %
Age group (years)
18–24 8 29.6
24–44 8 29.6
45–64 7 25.9
65+ 4 14.8
Sex
Male 20 74.1
Female 7 25.9
Highest level of education
Completed some high school/school certificate 10 37.0
Completed year 12 high school or equivalent 5 18.5
TAFE certificate or diploma 9 33.3
University or tertiary institute degree 3 11.1
Injury mechanism
Road traffic-related 20 74.1
Fall and other 7 25.9
Place of incident
Street/highway 20 74.1
Home and other 7 25.9
Injury severity score
Serious (9–15) 4 14.8
Severe (16–24) 11 40.7
Critical (25+) 12 44.4
Length of stay (days)
5–7 5 18.5
8–14 7 25.9
15–28 8 29.6
29+ 6 22.2
R. Mitchell et al. / Injury, Int. J. Care Injured 43 (2012) 96–102 99
(x2 = 0.12, df = 1, p = 0.7), injury mechanism (x2 = 0.81, df = 1,p = 0.4) or place of incident (x2 = 1.38, df = 2, p = 0.5) (Table 1). Ofthe 36 individuals who consented to participate, 27 (75.0%)completed the interview, 4 (11.1%) were unable to be contacted, 3(8.3%) refused to participate and 2 (5.6%) telephoned and asked tobe removed from the trauma outcomes data collection. There wereno significant differences by age (t(34) = �0.27, p = 0.8), ISS(t(34) = �1.03, p = 0.3), gender (p = 0.7) or injury mechanism(p = 1.0) for participants and individuals who could not becontacted or who later refused to be interviewed.
Around three-quarters of the interviewed participants weremale and over half (59.2%) were aged less than 45 years. Around
Table 3Interviewed participant outcomes at 3 months post-injury.
Characteristics n %
Living status (n = 27)
At home without additional care 16 59.3
At home with additional care 8 29.6
Other 3 11.1
Work or study (n = 27)
Working 20 74.1
Home duties 1 3.7
Student 2 7.4
Retired 4 14.8
Return to work (if working prior to injury, n = 21)
No 13 61.9
Yes 8 38.1
Currently working or studying full- or part-time since your injury (n = 8)
Full-time 6 75.0
Part-time/causal 1 12.5
Both working and studying 1 12.5
In what capacity returned to work or study (n = 8)
Same role as before injury 5 62.5
Same role, but reduced capacity 3 37.5
Health and well-being (SF-12, n = 27)
Physical component, mean (sd) 34.4 (10.2)
Mental component, mean (sd) 47.4 (10.8)
Everyday activities and return to function (GOSE, n = 27)
Lower severe disability 2 7.4
Upper severe disability 25 92.6
one-third of participants each completed some high school or aTAFE certificate or diploma. Just less than three-quarters (74.1%) ofparticipants were injured in a road traffic crash on a public road.The majority of participants (85.1%) were either severely (ISS 16–24), or critically (ISS > 25), injured and just over half (51.8%) spent15 days or more in hospital (Table 2).
Following the injury, 40.7% of participants remained at homewith additional care or had moved in with relatives or partners.The majority of participants (81.5%) were either working orstudying prior to the injury and just under two-thirds (61.9%) hadreturned to work or study, but most in a full-time (75.0%) capacityin their same role (62.5%). The mean physical and mentalcomponent scores of the SF-12 were 34.4 and 47.4, respectively,indicating below average scores compared to Australian norms.6
Almost all participants were rated by the GOSE in the upper sphereof severely disabled (Table 3).
Discussion
Information from trauma registries, such as mortality rates orlength of stay in hospital, have long been used to measure thequality of trauma care and outcomes.14,21,27 Using this sort ofinformation to measure trauma outcomes essentially ignores thehealth outcomes and experience of trauma survivors.14 Thecollection of longer term trauma outcomes from trauma survivorspost-injury can provide information on the management of patientcare, the consequences and health burden of traumatic injury,along with information on prognostic factors that may influencerecovery.9,23
Whilst collecting information from trauma survivors onrecovery from injury is beneficial to monitor trauma outcomes,the value of the information collected is reliant on the informationbeing representative of the whole trauma population. In thecurrent study, 25% of individuals who initially agreed to participatein the pilot study were unable to be contacted or later refused toparticipate. This response rate is similar to a Queensland study1 oftrauma outcomes that used postal questionnaires to obtaininformation on trauma outcomes and to a Taiwanese study20 thatused telephone interviews to obtain outcome information both at 3months post injury, where around one-third of the individuals whoinitially consented to participate did not end up responding. Whilstthere were no significant differences between participants andnon-participants in the current study, either pre or post receivinginitial consent to contact, with a larger sample size there is thepotential that a trauma outcomes data collection may not berepresentative of the trauma population as a whole.
For the pilot study, the data items collected were able to providean indicator of the impact of trauma on individuals in their attemptto return to their previous level of physical functioning. The profileof the trauma population in the current study had a similarproportion of males and females and mean age of participants toother Australia trauma outcomes studies1,14,17 and the majority oftrauma cases were as a result of road traffic-related trauma, againsimilar to other trauma outcomes research.14,17,30
Both the GOSE scale and the mean physical and mentalcomponent scores of the SF-12 showed that individuals at 3months post-injury had a drastically reduced HRQoL compared towhat might be expected in a normative or community sample.34,36
The SF-12 scores in the current study were very similar to the 3month post-trauma outcome scores obtained in a Queenslandstudy.1 It is of note that, whilst some individuals had returned towork at 3 months post injury, all individuals were rated as‘severely disabled’ by the GOSE. Along with functional abilities, theGOSE also takes into account the ability to resume social andrecreational pursuits, family and friend relationships and activitiesof daily living, such as local travel and shopping.36 It appears that at

R. Mitchell et al. / Injury, Int. J. Care Injured 43 (2012) 96–102100
3 months post-injury individuals are not yet sufficiently recoveredto fulfil all of these categories, which would be likely to improve ataround 6 months post-injury as has been the case for injuredindividuals in Victoria.15
The use of specialist computer assisted telephone interviews(CATI) staff to conduct the trauma outcome interviews workedwell for the pilot study. Using CATI staff from a Health Departmentprovided an impetus for the quality assurance aspect of the traumaoutcomes study in terms of the assessment of clinical outcomesfrom hospital treatment.
This pilot study demonstrates that there is the potential toestablish a routine long-term trauma outcomes data collection inNSW. The establishment of this collection would allow NSW tomonitor, on an on-going basis, longer term injury outcomesbeyond survival post-injury in terms of quality of life includingboth physical and psychological effects. The collection would alsoallow the examination of the effectiveness of trauma managementand be capable of modelling some of the predictors of injuryoutcome, such as return to function, return to work, and quality oflife.
However, prior to the potential of a long-term trauma outcomesdata collection being realised, there are a number of problems thatneed to be resolved to assist in the establishment of the collection.These are similar problems likely to be faced by other researchersand clinicians wishing to establish long-term trauma outcomescollections. The requirement to use an ‘opt in’ process for the datacollection was problematic and this is not the model successfullyused in Victoria and New Zealand, where an ‘opt out’ methodologyis employed.9,10 The use of the opt in model resulted in the researchteam being reliant on the good will of champions in the traumaservices to recruit individuals into the collection. Within the pilotstudy, the recruitment process stalled at one trauma centre whenone local champion went on leave for a short period of time. InVictoria, VSTOR was established following a Ministerial Review ofTrauma and Emergency Services that recommended and legislatedfor the establishment of ongoing monitoring of outcomes fromtrauma care26 and it is possible that such an impetus for theestablishment of a long-term trauma outcomes collection in NSWwill be necessary.
Whilst a recommendation from government would be benefi-cial to establish an ‘opt out’ trauma outcomes data collection, thereis currently no impediment under NSW legislation (i.e., HealthRecords and Information Privacy Act 2002 (NSW) StatutoryGuidelines on Research28) or Australia’s National Health andMedical Research Council’s (NHMRC) National Statement onEthical Conduct in Human Research4 for a waiver of therequirement for written informed consent. In fact, 75% ofAustralian clinical registries have an opt off consent approach.13
There are, however, certain conditions that need to be satisfiedbefore an ethics committee can waive the requirement for consent.These include that the research carries a low risk (i.e., where theonly foreseeable risk is one of discomfort4) to participants. Thelong-term trauma outcomes data collection involved participantscompleting a 10 min telephone interview that could have beenviewed as an inconvenience by some participants (i.e., a low risk).The benefits from the research should justify any risks of harmassociated with not seeking consent. In this case, the developmentof a long-term trauma outcomes data collection would havesignificant implications for a region’s ability to monitor longerterm injury outcomes and provide information on clinicalprocedures and their effectiveness.
Consent can be waived if it is impracticable to obtain consent orif there is no known reason for thinking that participants would nothave consented. The logistics of obtaining individual writteninformed consent on a state wide scale would not be feasible andwould likely result in non-respondent bias that would threaten the
population basis of the collection.12,19 Roughly, only 1% ofparticipants choose to opt out of VSTOR14 and it is envisaged thatother regions would have a similar opt out proportion. Non-respondent bias is a known limitation of registry data collec-tions.19,32 Within-hospital recruitment bias could result from thepatient being with visitors, being too ill or not on the ward at thetime of recruitment or due to time constraints or a lack ofcommitment by medical staff to enrol individuals. Tu andcolleagues,32 in an examination of the effectiveness of obtaininginformed consent and participation in the Canadian StrokeRegistry, found that there was a poor participation rate, withonly 39.3% of patients enrolled to participate. The most commonreason for non-participation was that the participant left hospitalbefore they could be approached by medical staff. Othermechanisms of participant recruitment, such as recruitment viamail out with mail back of consent forms, can also result insignificant recruitment bias with only the most motivatedparticipants ‘opting in’. Those who fail to opt in are likely to havepoorer outcomes and are therefore likely to benefit most frominterventions derived from the research.19,32
Lastly, for consent to be waived there must be sufficientprotection of an individual’s privacy and an adequate plan toprotect data confidentiality. Privacy protection and data confi-dentiality in the pilot study were guaranteed as the linked data filedid not contain any identifying information (i.e., surname, firstname) only a participant number, and information was stored on asecure, password protection computer server. Ingelfinger andDrazen19 consider that if adequate safeguards are present forprivacy and confidentiality then the requirement for informedconsent could be waived. They considered that an appropriatesafeguard for privacy was the involvement of a third party betweenidentifiable and unidentifiable data. On a state wide level, datalinkage for the long-term trauma data collection could beconducted by a third agency. Within NSW the Centre for HealthRecord Linkage (CHeReL) could fulfil this role. As this was a 3month pilot project, funding was not available for CHeReL toperform the data linkage.
The current research met the waiver of consent criteria asdescribed above, but was still not approved to use an opt outmethodology for recruitment. Cameron et al.9 acknowledge thedifficulties of ethics committees in reconciling informed consentand confidentiality issues with the need for quality assurance intrauma treatment and outcomes and suggested that legislationmight be the most effective route to establish new registries. Ifrequired to seek written informed consent, long-term traumaoutcomes data collections will not reach their full potential, due toselection biases and only limited inferences about traumatreatment and outcomes will be able to be conducted.
On-going resources for the long-term trauma outcomes datacollection will need to be considered, along with appropriatetimeframes for follow-up interviews. Adequate and sustainableresources would be needed in terms of staff to manage, interpretand collect data.9 In the current study, the interviews alone costAUD$100 per participant which was in addition to clinical stafftime required to recruit participants and collect and enter traumadata, and the time required for the research team to manage theparticipant database, mail out secondary participant informationsheets, coordinate the interview process, clean and analyse thetrauma data and link the trauma and interview data collections. InVictoria, data collection costs are estimated at AUD$100 perparticipant,9 but interviews are conducted by medical studentsrather than Health Department staff, and VSTOR is largelysupported by Transport Accident Commission (TAC) and theVictorian Department of Human Services. An annual estimate forVSTOR is approximately AUD$90,000.16 If a long-term traumaoutcomes data collection is to be set up in NSW, the cost of the

R. Mitchell et al. / Injury, Int. J. Care Injured 43 (2012) 96–102 101
initial establishment and on-going administration will be consid-erable. However, the benefits of obtaining this sort of informationfrom a representative sample of trauma cases in NSW wouldinclude the capacity to model ongoing service provision, informpolicy development, and monitor outcomes across traumaservices.
In Victoria, post-injury interviews are conducted at 6, 12 and24 months.16 Other research has used different follow-upinterview timeframes, such as 1, 4 and 12 months,11 3 months,1,20
3, 6 and 12 months8 and 12 months or greater.17,18,23,25,30 Thecurrent pilot study used a 3 month follow-up period, largely dueto the research grant reporting timeframes. Little research hasbeen conducted on the most appropriate timeframes for follow-up of trauma survivors. Any follow-up timeframes would bedependent on the population under study, the severity of thetrauma experienced and the objectives of the research.35 Ideally,3, 12 and 24 month follow-up periods would be preferable as mostinjured individuals appear to recover reasonably quickly (that is,within the first 3 months)35 and usually experience full recoveryby 12 months post-injury. However, for those individuals withsevere trauma a follow-up assessment at 24 months is recom-mended.7
Incorporating a trauma outcomes collection along side atrauma registry would be a practical response to where to host anoutcome collection. Since the commencement of this research, theNSW Institute of Trauma and Injury Management (ITIM) hasimplemented a state wide system, the NSW Collector TraumaRegistry, to collect standardised information on trauma patientsadmitted to 13 trauma centres in NSW. The long-term traumaoutcomes data collection could potentially form an extension ofthis registry, with an additional module added to the Collectorsystem to record information on trauma outcomes. Havingbiostatistical and research support, through alignment to auniversity or academic institution, would also be beneficial forthe outcomes collection.16
The establishment of reporting mechanisms to feedback totrauma centres regarding long-term patient outcomes should beconsidered and, in the longer term, mechanisms to monitor dataquality and protocols for data accessibility for research purposesshould be developed. Ultimately, information from a long-termtrauma outcomes collection could be linked to data collections toconduct research across the injury continuum (i.e., injury riskfactors, injury event circumstances, clinical treatment, and long-term injury outcomes) as there is a strong need for a betterunderstanding of the relationships between different stages of theinjury continuum.
Conclusion
The development of long-term trauma outcomes data collec-tions would be beneficial as the information collection could beused to describe the longer term impact of injury trauma on theindividual and the health system, including identification of themost effective approaches for trauma management and rehabili-tation. However, this study has highlighted that there are still somemethodological issues, particularly in relation to recruitmentprocesses, to be addressed before successful implementation oflong-term trauma outcomes data collections that are representa-tive of the trauma population.
Acknowledgements
This research was funded by a University of NSW Early CareerResearch grant. R. Mitchell was supported by an ARC-linkage post-doctoral fellowship (LP0990057) and W. Watson was supported bythe NSW Health Department.
The authors wish to thank Dr Belinda Gabbe for providinginformation regarding the operation of VSTOR, NSW Health SurveyProgram (except ‘program’ In Computers) staff, in particular JasonVan Ritten and Lindy Fritsche and the NSW Health Survey Program(except ‘program’ In Computers) interviewers, for conducting post-injury interviews, Kerrianne Hancock for assistance with recruit-ment, Erica Caldwell and Sarita Karanth for assistance withextracting trauma data at Liverpool hospital and trauma casemanagers at St. George Hospital: Alana Clements, Belinda Munroe,Sarah Kourouche and Elizabeth Walter.
References
1. AitkenL, DaveyT,Ambrose J,ConnellyL,Swanson C,Bellamy N.Healthoutcomesofadults 3 months after injury. Injury 2007;38:19–26.
2. Association for the Advancement of Automotive Medicine. The abbreviated injury
scale 2005 – update 2008. Barrington, IL: Association for the Advancement ofAutomotive Medicine; 2008.
3. Australian Bureau of Statistics. Australian demographic statistics. Canberra: Aus-tralian Bureau of Statistics; 2009. [Dec 2009, catalogue no.: 3101.0].
4. Australian Government. National statement on ethical conduct in human research.Canberra: National Health and Medical Research Council; 2007.
5. Australian Institute of Health and Welfare. Australia’s health 2008. Canberra:AIHW; 2008.
6. Avery J, Dal Grande E, Taylor A. Quality of life in South Australia as measured by the
SF12 Health Status Questionnaire. South Australia: Population Research and Out-comes Studies Unit, Department of Human Services; 2004.
7. Bouillon B, Kreder H, Eypasch E, Holbrook T, Kreder H, Mayou R, et al. Quality oflife with multiple injuries – basic issues, assessment and recommendations.Restorative Neurology and Neuroscience 2002;20:125–34.
8. Butcher L, MacKenzie E, Cushing B, Jurkovich G, Morris J, Burgess A, et al. Long-term outcomes after lower extremity trauma. The Journal of Trauma 1996;41:4–9.
9. Cameron P, Finch C, Gabbe B, Collins J, Smith K, McNeil J. Developing Australia’sfirst statewide trauma registry: what are the lessons? Australian & New ZealandJournal of Surgery 2004;74:424–8.
10. Derrett S, Davie G, Ameratunga S, Langley J. Capturing outcomes followinginjury: a New Zealand pilot study. The New Zealand Medical Journal 2010;123.[11 June].
11. Derrett S, Langley J, Hokowhitu B, Ameratunga S, Hansen P, Davie G, et al.
Prospective outcomes of injury study. Injury Prevention 2009;15:351.12. Edlund M, Craig T, Richardson M. Informed consent as a form of volunteer bias.
The American Journal of Psychiatry 1985;142:624–7.13. Evans S, Bohensky M, Cameron P, McNeil J. A survey of Australian clincial
registries: can quality of care be measured?. Internal Medicine Journal, 2009 Oct7, doi:10.1111/j.1445-5994.2009.02068.x.
14. Gabbe B, Cameron P, Hannaford A, Sutherland A, McNeil J. Routine follow up ofmajor trauma patients from trauma registries: what are the outcomes? TheJournal of Trauma 2006:61.
15. Gabbe B, Simpson P, Sutherland A, Williamson O, Judson R, Kossmann T, et al.
Functional measures at discharge: are they useful predictors of longer termoutcomes for trauma registries? Annals of Surgery 2008;247:854–9.
[16]. Gabbe B, Sutherland A, Hart M, Cameron P. Population-based capture of longterm functional and quality of life outcomes following major trauma – theexperiences of the Victorian State Trauma Registry. Journal of Trauma InjuryInfection and Critical Care 2010;69(3):532–6.
17. Harris I, Young J, Rae H, Jalaludin B, Solomon M. Predictors of general healthafter major trauma. Journal of Trauma Injury Infection and Critical Care2008;64:969–74.
18. Holbrook T, Anderson J, Sieber W, Browner D, Hoyt D. Outcome after majortrauma: 12-month and 18-month follow-up results from the trauma recov-ery project. Journal of Trauma Injury Infection and Critical Care 1999;46:765–73.
19. Ingelfinger J, Drazen J. Registry research and medical privacy. New EnglandJournal of Medicine 2004;350:1452–3.
20. Lee B, Chaboyer W, Wallis M. Predictors of health-related quality of life 3months after traumatic injury. Journal of Nursing Scholarship 2008;40:83–90.
21. Lloyd LE, Graitcer PL. The potential for using a trauma registry for injurysurveillance and prevention. American Journal of Preventive Medicine1989;5:34–7.
22. MacKenzie E, Shapiro S, Smith R, Siegel J, Moody M, Pitt A. Factors influencingreturn to work following hosptialisation for traumatic injury. American Journalof Public Health 1987;77:329–34.
23. MacKenzie E, Siegel J, Shapiro S, Moody M, Smith R. Functional recovery andmedical costs of trauma: an analysis by type and severity of injury. The Journalof Trauma 1988;28:281–97.
24. Mathers C, Boerma T, Ma Fat D. Global and regional causes of death. BritishMedical Bulletin 2009:1–26. [September 22].
25. Michaels A, Michaels C, Smith J, Moon C, Peterson C, Long W. Outcome frominjury: general health, work status, and satisfaction 12 months after injury.Journal of Trauma Injury Infection and Critical Care 2000;48:841–50.

R. Mitchell et al. / Injury, Int. J. Care Injured 43 (2012) 96–102102
26. Ministerial Taskforce on Trauma and Emergency Services. The Department ofHuman Services Working Party on Emergency and Trauma Services. Review of
Trauma Emergency Services Victoria 1999. Melbourne: Department of HumanServices; 1999.
27. Moore L, Clark D. The value of trauma registries. Injury 2008;39:686–95.28. NSW Government. Health records and information privacy act 2002. NSW Govern-
ment; 2002.29. NSW Institute of Trauma and Injury Management. The NSW trauma registry profile
of serious to critical injuries 2007. Sydney: NSW Institute of Trauma and InjuryManagement; 2010.
30. Rhodes M, Aronson J, Moerkirk G, Petrash E. Quality of life after the traumacenter. Journal of Trauma 1988;28:931–8.
31. SAS Institute. SAS: statistical software, version 9.1. Cary, North Carolina: SASInstitute; 2003.
32. Tu J, Willison D, Silver F, Fang J, Richards J, Laupacis A, et al. Impracticability ofinformed consent in the registry of the Canadian Stoke Network. The NewEngland Journal of Medicine 2004;350:1414–22.
33. Urquhart D, Williamson O, Gabbe B, Cicuttini F, Cameron P, Richardson M, et al.
Outcomes of patients with orthopaedic trauma admitted to level 1 traumacentres. ANZ Journal of Surgery 2006;76:600–6.
34. Ware J, Kosinski M, Keller S. A 12-item short-form health survey. Medical Care1996;34:220–33.
35. Watson WL. Of life and limb: measuring the burden of non-fatal injurymonash accident
research centre. Melbourne: Monash University; 2005.36. Wilson J, Pettigrew L, Teasdale G. Structured interviews for the glasgow
outcome scale and the extended glasgow outcome scale: guidelines for theiruse. Journal of Neurotrauma 1998;15:573–85.