Embed Size (px)
Citation preview
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 1 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
DIFFUSED TOXIC GOITER: A FIVE YEAR EXPERIENCE
AUTHORS: S. ALIYU, A. G. IBRAHIM
ADDRESS: DEPARTMENT OF SURGERYs UNIVERSITY OF MAIDUGURI TEACHING
HOSPITAL MAIDUGURI BORNO STATE NORTH EASTERN NIGERIA.
CORRESPONDANCE: DR SULEIMAN ALIYU DEPARTMENT OF SURGERY
UNIVERSITY OF MAIDUGURI TEACHING HOSPITAL P.M.B1414 MAIDUGURI
BORNO STATE NIGERIA
TEL. +2348035015309
EMAIL: [email protected]
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 2 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
ABSTRACT: Background: Grave’s disease is the commonest endocrine auto
immune disorder in women it is characterized by diffuse enlargement of the
thyroid gland associated with elevated serum thyroid hormones manifesting with
clinical features of thyrotoxicosis. Other features are opthalmopathy, and
acropachy. It is an IgG antibody mediated. Grave’s disease is one of the
indications for thyroidectomy; the study reviewed our 3 year experience in the
management of patients with the disease. Patients and Methods: We reviewed
all patients with Diffused toxic goiter (Grave’s disease) managed in the University
of Maiduguri Teaching Hospital (UMTH) between January 2010 and December
2014. Patients with emergency presentation (thyrocardia) were resuscitated and
optimized. All patients were rendered euthyroid with carbimazole and
propranolol on outpatient basis. Subtotal thyroidectomy under general
anesthesia was done in all patients. Results: A total of 85 patients were analyzed,
78 were females and 7 males with a female to male ratio of 11.14: 1. Age ranged
from 14 – 70 years with a mean of 31.84 years and SD of 10.89, mean age for
females, and males were 31.74, and 32.86 respectively. The peak age group was
20 – 29 accounting for 41.18%, and 78.82% of the patients were under the age of
40 years. The presenting clinical features were anterior neck swelling, heat
intolerance, and hair loss/darkening of skin in all patients. Associated
autoimmune diseases were type 1 diabetic mellitus in 5.88%, Rheumatoid
arthritis in 3.53%, and systemic lupus erythromatosis (SLE) in 1.18%.
Postoperative complications were respiratory obstruction in 11.76%, and
transient hypocalcaemia in 10.59%. Conclusion: Grave’s disease is common, with
spectrum of manifestations characterized by goiter, thyrotoxicosis, and
psychosocial problems. Subtotal thyroidectomy is still a viable option in
developing countries.
KEYWARDS: Diffused Toxic Goiter, Psychosocial problems, Subtotal
Thyroidectomy, Outcome of Management.
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 3 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
Introduction: Graves’ disease owes its name to the Irish physician; Robert James
Grave’s who described the condition in 1835. It is a syndrome comprising
hyperthyroidism with a diffuse goiter, eye disease characterized by inflammation
and involvement of intra orbital structures, dermopathy refer to as pretibial
myxedema, and rare involvement of the nails, fingers and long bones known as
acropachy. Prior to Graves’ description the Greek philosopher Aristotle and the
English physician Caleb Parry had described the condition1. The disease is the
most common autoimmune disease representing 50-80% of cases of
hyperthyroidism in the U.S.A2 it occurs more commonly among women, smokers,
and patients with other autoimmune diseases or a family history of thyroid
autoimmunity3. The emergence of this autoimmune process is probably due to an
underlying genetic susceptibility with superimposed environmental factors
particularly HLA alleles on chromosome 6 namely HLA- DRB1-08, DRB3-0202, and
HLA-DQA1-0501 are known to confer an increased risk of Graves’ disease4-5. There
is always a trigger before the onset of clinical features. Such triggers include
stressful life events, infection, job loss, or bereavement, exposure to high doses of
iodine, and recent child birth. The clinical features include weight loss despite
increase appetite, heat intolerance, irritability, insomnia, sweatiness, diarrhea,
palpitations, muscular weakness, and menstrual irregularity. Others are diffused
goiter, fine resting tremor, tachycardia, hypereflexia, eyelid lag, worm smooth
skin, and proximal myopathy. Rarely atrial fibrillation and thyroid bruit reflecting
increased thyroid vascularity. Older patients are more likely to present with
depression, weight loss, and cardiovascular features like congestive cardiac failure
than younger patients6. This hyper dynamic congestive cardiac failure is also
called thyrocardia. Women may presents for cosmetic reasons, with concerns
about goiter, eye changes, or hair loss7-8. These cosmetic problems were under
reported, especially in developing countries where gender inequality, cultural
factors, poor socioeconomic status and low level of education put women at
disadvantage. Most women are dependent on men therefore loss of self esteem
and body image lead many women that are not gainfully employed in to
depression and suicidal tendency, marital separation, divorce and instability are
common among women with Graves’ disease. Total thyroidectomy with thyroxine
replacement is currently the gold standard in goiter surgery for both benign and
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 4 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
malignant conditions9-10. Many developing countries have a peculiar problem of
non availability of thyroxine and where available is too expensive and
unaffordable to be taken for life. This is a strong indication for subtotal
thyroidectomy in our environment. The study reviewed our experience in Graves’
disease management.
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 5 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
Patients and Methods: The study reviewed all patients with Diffused toxic goiter
(Grave’s disease) managed in the University of Maiduguri Teaching Hospital
(UMTH) between January 2010 and December 2014. Permission for the study was
granted by the Hospital Ethical and Research Committee. Written informed
consent was obtained from the patients. Information was extracted from clinical
and laboratory records and data analyzed using SPSS version 16. The diagnosis
was made from clinical and laboratory evaluation. Investigations done were
Thyroid function test (T3, T4, and TSH), urinalysis, full blood count, blood
chemistry, indirect laryngoscopy, electrocardiography, and echo cardiography
where necessary. Patients with emergency presentation (thyrocardia) were
resuscitated and optimized, and patients were rendered euthyroid with
carbimazole and propranolol on outpatient basis before surgery. All patients had
subtotal thyroidectomy under general anesthesia with endotracheal intubation.
Prophylactic antibiotic (ceftriaxone) was given at induction. Patients were
monitored postoperatively and followed up after discharge.
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 6 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
Results: A total of 85 patients were analyzed, 78 were females and 7 males with a
female to male ratio of 11.14: 1. Age ranged from 14 – 70 years with a mean of
31.84 years and SD of 10.89, mean age for females, and males were 31.74, and
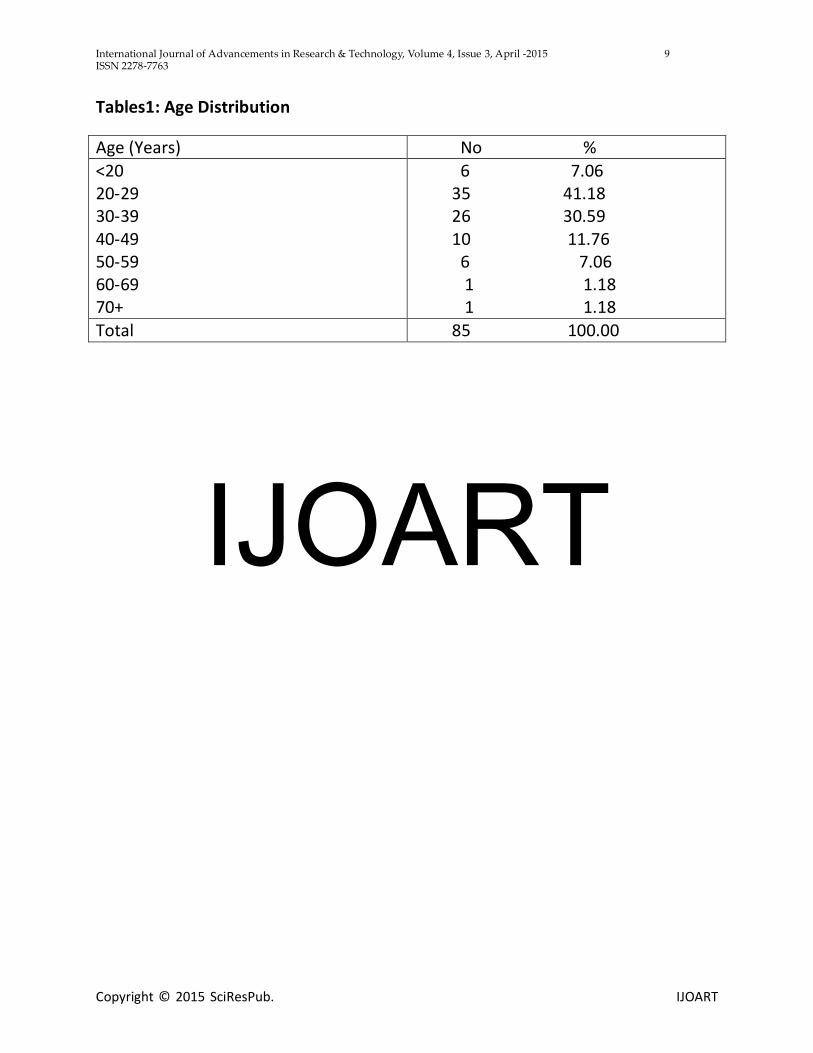
32.86 respectively. The peak age group was 20 – 29 accounting for 35 (41.18%),
and 67 (78.82%) of the patients were under the age of 40 years table 1. The
presenting clinical features were anterior neck swelling, heat intolerance, and hair
loss/darkening of skin in all patients table 2. Co-morbid medical conditions were
hypertension in 11 (12.94%), type one diabetic mellitus in 5 (5.88%), Rheumatoid
arthritis in 3 (3.53%), asthma in 2 (2.35%), and systemic lupus erythromatosis
(SLE) in 1 (1.18%). Histology confirmed Graves’ disease in all patients with
associated nodules in 11 (12.94%) no malignancy was found. Postoperative
complications were respiratory obstruction in 10 (11.76%), comprising of
laryngeal edema in 6 (7.06%), recurrent laryngeal nerve palsy in 1 (1.18%), and
hematoma in 3 (3.53%). Others were transient hypocalcaemia in 9 (10.59%),
recurrence in 2 (2.35%) (Who subsequently had total thyroidectomy with
thyroxine replacement for life), and keloid/hypertrophic scar in7 (8.24%). There
was no mortality. The mean hospital stay, and duration of follow up were 5 days,
and 27 months.
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 7 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
Discussion: The study revealed the mean age for Graves’ disease to be 31.84
years, and the patient’s age ranged from 14 – 70 years. This indicates by far
Graves’ disease is the disease of the young in this environment compared to
similar study by Jolanta et al11 that found older patients with the mean age of
47.12years, and age range of 18 – 84 years. Similarly the mean ages for males and
females of 32.86years and 31.74years respectively were lower than their findings.
Globally however there is a rising incidence of Graves’ disease among children
especially in the Far East12. The traditionally recognized clinical features13 of
Graves’ disease were similar to our findings. However this study revealed the
depth of psychosocial disturbance associated with Graves’ disease as evidence by
the findings of hostile/quarrelsome disposition, and domestic problems of
separation or divorce in 85.88%, and 27.06% respectively. Graves’ disease
patients are found to have low self esteem and body image due to associated
poor cosmetic outlook (hair loss, goiter, extholpthalmus, and dermopathy) in
(91.76%). The fore going psychosocial problems constitute a major part of the
unreported features of Graves’ disease that the current study found. Graves’
disease is known to be associated with other autoimmune disorders like
myasthenia gravis, type 1 diabetes mellitus14-15. The current study found type 1
diabetes mellitus, and rheumatoid arthritis. The histology revealed Graves’
disease in all patients with nodules in 12.94% however there was no incidental
carcinoma in variance with study by Mishra et al16that found incidental carcinoma
in their series. The postoperative complications in our series were respiratory
obstruction in 11.76% (from hematoma 3.53%, laryngeal edema 7.06%, and
recurrent laryngeal nerve palsy 1.18%), and transient hypocalcaemia in 10.59%.
These complications were similar to complications of subtotal thyroidectomy but
lower than found in total thyroidectomy as reported in comparative study of total
versus subtotal thyroidectomy by Colak et al17. Globally there is a reduction in the
complications associated with thyroidectomy, therefore the reluctance to
recommend thyroidectomy for definitive treatment of Graves’ disease has been
challenged in recent years. A study by Pearce et al18 showed that thyroidectomy is
more cost effective than either radio iodine ablation or antithyroid medication
and offers patient a better quality of life. The argument today is which surgery is
the best? Total thyroidectomy on the one hand, and near total or subtotal
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 8 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
thyroidectomy on the other hand based on variation in complications19-21. The
current study had 2.35% recurrent goiter that were offered completion
thyroidectomy. Alessandro et al22 in a 20 year follow up period found a
recurrence of 2-70% of cases, and advocated for total thyroidectomy at the initial
surgery because surgical treatment of such recurrence is associated with higher
complications.
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 9 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
Tables1: Age Distribution
Age (Years) No %
<20 20-29 30-39 40-49 50-59 60-69 70+
6 7.06 35 41.18 26 30.59 10 11.76 6 7.06 1 1.18 1 1.18
Total 85 100.00
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 10 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
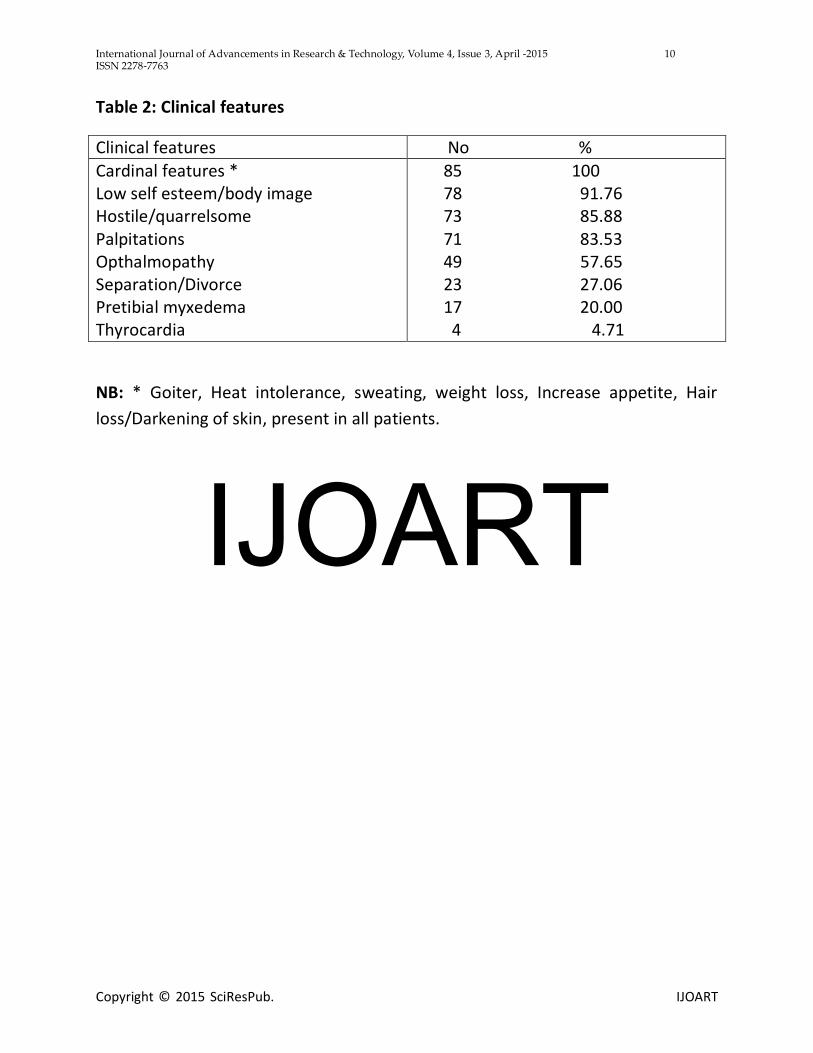
Table 2: Clinical features
Clinical features No %
Cardinal features * Low self esteem/body image Hostile/quarrelsome Palpitations Opthalmopathy Separation/Divorce Pretibial myxedema Thyrocardia
85 100 78 91.76 73 85.88 71 83.53 49 57.65 23 27.06 17 20.00 4 4.71
NB: * Goiter, Heat intolerance, sweating, weight loss, Increase appetite, Hair
loss/Darkening of skin, present in all patients.
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 11 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
References:
1. Weetman A.P. Graves’ disease. Horm Res 2003; 59(1): 114 – 118
2. Brent G. A. Graves’ disease N Engl J Med 2008; 358: 2544 – 2554
3. Manji N., Carr-Smith J. D., Boelaert K., Allahabadia A. Armitage M.,
Chatterjee V. K et al. Influence of age, gender, smooking and family history
on autoimmune thyroid disease phenotype. J Clin Endocrinol Metab 2006;
91: 4873 – 4880
4. Stenszky V., Kozma I., Balazs C., Rochlitz s., Bear J. C., Farid N. R. The
genetics of Graves’ disease: HLA and Disease susceptibility. J Clin Endocrinol
Metab 1985; 61: 735 – 740
5. Yanagawa T., Mangklabruks A., De Groot L. J. Strong association between
HLA – DQA 0501 and Graves’ disease in a Caucasian population. J Clin
Endocrinol Metab 1994: 79 (1): 227 – 9
6. Kein I., Ojamaa K. Thyroid hormone and the cardiovascular system N Engl J
Med 2008; 344: 501 – 509
7. Abraham-Nordlin M. Graves’ disease: Along term quality of life follow up of
patients randomized to treatment with antithyroid drugs, radioiodine, or
surgery. Thyroid 2005; 15: 1279 – 1286
8. Reasner C. A. Autoimmune thyroid disease and type 1 diabetes. Diabetes
1993; 1: 343 – 351
9. Reeve T. S., Delbridge L., Cohen A., Crummer P. Total thyroidectomy the
preferred option for multi nodular goiter. Ann Surg 1983; 6: 782 – 786
10. Igbal M., Mehmood Z., Rsul S., Inamullah H., Shah S.S., Bokhari I.
Carcinoma of thyroid in multi and uni nodular goiter. J Coll Physician Surg
2010; 5: 310 – 312
11. Jolanta K., Jerzy S. T., Maria K., Helena J., Beata C., Anna d. Age and size of
goiter in hyperthyroidism. Endocrine Abstracts 2010; 22: 814
12. Wong G. W., Cheng P. S. Increasing incidence of childhood Graves’ disease
in Hong Kong: a follow up study Clin Endocrinol (oxf) 2001: 54 (4) 547 50
13. Christian M. A, Bernard L.C., Jack R.W. Current concepts in Graves Disease
Ther Adu Endocrinol Metab 2011; 2(3): 135 – 144
IJOART
International Journal of Advancements in Research & Technology, Volume 4, Issue 3, April -2015 12 ISSN 2278-7763
Copyright © 2015 SciResPub. IJOART
14. Imran M., Mir Y., Aiffa A., Kudyar R.P. Auto immune thyroid disease with
myasthenia gravis in a 28 – year old male: a case report. Cases Journal
2009; 2: 8766 doi: 10.4076/1757 – 1626 – 28766
15. Zhebrun D., Kudryashova Y., Baberoko A., Maslyansky Kunitskaya N.,
Popcova D., Wushina A., Grineva E., Kostareva A., Shlyakhto E. Association
of PTPN22 1858T/T genotype with type 1 diabetes, Graves’ disease but not
with rheumatoid arthritis in Russian population. Aging(Albany N Y) 2011;
3(4): 368 – 73
16. Mishra A., Mishra S. Thyroid nodules in Graves’ disease: Implications in an
endemically iodine deficient area J Postgrad Med 2001; 47: 244
17. Colak T., Akca T., Kanik A., Ypici D., Aydin S. Total versus subtotal
thyroidectomy for the management of benign multi nodular goiter in an
endemic region. ANZ Journal of Surgery 2004; 74: 974 – 978 doi10
1111/j.1445 – 1433.2004.03139.x
18. Pearce H.E.N., Wong A.K et al. Treatment options for Graves’ disease a cost
– effectiveness analysi J Am Coll Surg 2009; 209: 170 – 9 el 2
19. Koyuncu A., Aydin C. Topcu O et al. could total thyroidectomy become the
standard treatment for Graves’ disease. Surg Today 2010; 40: 22 – 5
20. Schussler – Fiorenza C. M., Bruns C. M., Chen H. The surgical management
of Graves disease J Surg Res 2006; 153: 207 – 14
21. Digonnet A., Willemse E., Dekeyser C. Near total Thyroidectomy is an
optional treatment for Graves disease Euro Arch Otorhinolaryngol 2009;
267: 955 – 60
22. Alessandro C., Maria D.V., Antonio Z., Emanuele L. M., Andrea C. The
recurrent goiter: Prevention and management. Annl: Haliani di chirurgia
2008; 79(4): 247 - 53
IJOART