Embed Size (px)
Citation preview

Bruno Barbato
Urgences Mains Val de Seine78410 Aubergenville, France.
Anne Virginie Salsac
Laboratoire Biomécanique et Bioingénierie (UMR 7338), CNRS-Université de Technologie de Compiègne
Alliance Sorbonne Université, 60200 Compiègne, France.
DIGIT REPLANTATIONS
FROM BIOMECHANICS TO EFFICIENCY

Mapuche Indians led by chief Galvarino and enslaved by
the Spanish conquerors in the 16th century
LOSS OF A HAND OR DIGIT IS AN EXTREME HANDICAP

ORTHOPAEDIC
The 1970’s saw the rise of handtrauma centers
One-time procedure
PLASTIC
MICRO-SURGERY GEM
THE RISE OF HAND TRAUMA CENTERS

Teaching
Learning
Microsurgery Laboratory
SOS MAINS BOUCICAUT 1972

Le livre Blanc 2018 PMSI
EPIDEMIO CURRENT PRACTICE
In the USA, 12% of finger amputation injuries are treated
with replantation. Most microsurgeons perform less than
5 per year.
Payatakes and al. J Hand Surg Am 2007 Nishizuka and al. J Hand Sur Am 2015.
In France, 15% of finger amputation injuries are treated
with replantation.
In Japan, 29% of finger amputation injuries are treated
with replantation

Fluid biomechanics considerations
General principles of digital replantation
Consensual indications
The Thumb
Distal amputations
Multiple digit amputations
Transmetacarpal amputation
Ring fingers avulsion
SURGICAL EFFICIENCY FOR OPTIMIZED OUTCOMES IN DIGIT REPLANTATION

FLUID
BIOMECHANICS CONSIDERATIONS

∆𝑝 = 𝑄8𝜂𝐿
𝜋𝑅4
=RHProvides information on:
Blood flow behaviour in veins and in smallarteries (quasi-steady flows)
Hydraulic resistance RH induced in a vesselof radius R and length L because of bloodviscosity η.
POISEUILLE LAW

𝑅𝑒 =𝜌𝑈𝐷
𝜂> 2200When
Hardly occurs under physiologicalconditions in blood vessels
May occur in largely stenosed vessels
Risk of thrombosis
with density 𝜌, velocity U
i.e. at large blood flows
HIGHER RISK IF THERE IS ASYMMETRICAL SIZE MISMATCH IN ANASTOMOSIS
TURBULENT FLOW

Zarins, Gidens, Glagov. In: Cerebrovascular insufficiency, New York, 1983
Flow recirculation as in:
Hathcock, Arteriosclerosis, Thrombosis, and Vascular Biology 2006
-> Risk of Thrombosis
HEMODYNAMIC CONSEQUENCES IN ANASTOMOSIS

Unsteady Flow
Time evolution of the blood flow Q over one period T
Velocity profile at different time instances in the cardiac period
Systolic Peak
Diastolic Peak
Salsac et al. Journal of Fluid Mechanics 2006
BLOOD FLOW IN LARGE ARTERIES
Risk of thrombosis

Womersley Number
α = 𝑅𝜌𝜔
𝜂
Velocity Profiles at Systolic Peak
Quasi-steady flow when ⍺ < 3Strong effect of pulsatility
when ⍺ > 5
with density 𝜌, viscosity η
BLOOD FLOW IN LARGE ARTERIES

GENERAL PRINCIPLES OF REPLANTATION

Prior to patient arrival in Emergency Department
Special boxes with ID and details
No colored solutions
No tourniquet required
GENERAL PRINCIPLES

Operative room staff and anesthesia teams should be notified
Eliminate any potential life-threatening lesions or conditions: replantation should not risk the life of the patient
Examination of the hand and x-ray of patient and amputated part(s)
Check the parts are not stored in a freezer compartment
PATIENT ARRIVAL TO THE EMERGENCY DEPARTMENT

Type of injury crush or guillotine: importance of the debridement
Number of amputated parts with or without the Thumb: Priorities in replantation
Macroscopic conditions of amputated parts and hand: associated lesion requiring additional repair surgery
X-ray status: type of bone repair and osteosynthesis anticipation
Patient details and conditions: major influence on final decision
WHAT COULD BE DONE?
ANTICIPATION & EFFICIENCY IN WORKFLOWS AND PROCEDURES

Clinical aspect: blue ribbon sign with pulpecchymosis indicating severe shearing forcealong the neurovascular bundle
Arteries and nerves debridement accordingto the type of injury tagged using 9-0 nylon/veins location
Bone resection is made to avoid damage tothe vessels /skeletal shortening for tensionfree vessels and nerves
Bone synthesis preparation
Extensor and flexor tendons preparation
WHAT CAN BE DONE?
ANTICIPATION & EFFICIENCY IN WORKFLOWS AND PROCEDURES
Amputated part examination and status: backtable and magnifying loupe or microscope

Possible options:
Lengthy process with important functionality consequences
Patient approval
Confident emotional and moral relationship
Non surgical factors and patient details
Upper extremity block anethesia
WHAT WILL BE DONE!
EXPLAINING TO THE PATIENT

Crush injury
Psychiatric disorders
Peripheral vascular disease (Raynaud)
Electrolytes imbalances
In the elderly risk is not only by age but bynumber of comorbidities
Left hand
Tobacco
• Ma and al. J Hand Surg Eur 2015.• Van Adrichem and al. J hand Surg Am 1992.• Waikakul and al. Injury 2000.• Hustedt and al J Hand Surg Am 2016
EFFECTS OF NON-SURGICAL FACTORS

No significant differences between immediate versus overnight delayed Replantations < 15 H Cold ischemia.
• Cavadas and al. J Hand Surg Am 2018• Woo and al. J Hand Surg Am 2015
ISCHEMIA TIME < 12 H COLD OR 6 H WARM
Medical legal aspects +++

But it depends on:
ISCHEMIA TIME < 12 H COLD OR 6 H WARM

Tourniquet run
Debridement: experience dependant +++
Vessels and nerves: location and tagged
Venous graft pre-drawing
Out of tourniquet
Bone and tendon repair out of tourniquet run andvein location
Extensor repair
Flexor Digitorum Profundis FDP privileged(reparation of the FDS often foregone / finalfunction not improved)
TIME AND EFFICIENCY
GENERAL OPERATIVES PRINCIPLE OPERATIVE TIME

BONE REPAIR AND TENDONS REPAIR
Secure but fast out of tourniquet
Cup-and-ball (bilboquet) or internal screwsin transmetacarpal+
K-wires +++
Skeletal shortening
No external fixation
FDP Tsuge/ Kessler/ Mac Larnay
Extensor

Digit irrigation with heparine solution (40%of French surgeons according to FESUM)
24-gauge yellow catheter without cuttingextremity
Direct arterial anastomosis even crossed
9 or 10-0 Nylon interupted suture
Tamai’s disposable micro plastic clip
Dumont and al Chir Main 2010.
MICROSURGICAL TIME: ARTERIAL REPAIR

ARTERIAL REPAIR
Microsurgery is the safer anastomosispossible
Looping suture on the last 2 or 3 sutures inorder to leave the lumen open
Oblique cut in case of asymetrical sizemismatch

Forearm ++
Length in physiological tension to avoid« Kinking » phenomenon, origin ofturbulent flow and thrombosis
Tension free suture by 9-0 Nylon suture
This is a graft and not a bypass
Bypass
In case of extended arterial damages
MICROSURGICAL TIME: VENOUS GRAFT
Graft

Functionally important, however:
Time efficiency
Tension free neurorraphy ++ skeletal shortening
Nerve graft
Nerve guides? When synthetic, they causediscomfort and inflammatory reaction in thedigit area mostly in transmetacarpal
Vein conduits
Spare part fingers
Source: biotextiles2017blog
MICROSURGICAL TIME: NERVE REPAIR

The key to success
Vein patterns « Dorsal Ladder » CentralTerminal Dorsal Vein
11-0 Nylon
Tourniquet release vein distension andlocation
Lucas GL. J Hand Surg Am 1990. 10h
14h
Efficiency+++
MICROSURGICAL TIME: VENOUS REPAIR

TOURNIQUET RELEASE
Vessels anastomosis patency test
Vein graft condition
Papaverine and tepid serum
Digit coloration

SKIN CLOSURE AND DRESSING
This is the surgeon’s responsibility+++ andshould not delegated
Skin graft to avoid tension suture
Pulp free
Splint

POST-OPERATIVE CARE CONTROL
Trained nursing staff
Hourly (first 24 hrs), every two hrs (for thefollowing 72 hrs) (documented)
Pulp color / temperature / capillary refill
Rest in warm environment and no need forheating lamp
Tobacco exclusion
Psychological support as soon as possible
R. Vilain, Jeux De Mains, 1987

Personal relationship of trust betweenpatient and surgeon
Preferred interlocutor of the follow-up
Preferred interlocutor of salvatoryprocedures
PERSONALIZED POST-OPERATIVE CARE

PHARMACOLOGICAL SUPPORT
Use of anticoagulants vary widely amongmicrosurgeons
Arterial platelet aggregation is the underlyingcause of arterial thrombosis Aspirin
Fibrin clotting is the underlying cause of venousthrombosis Heparin
Dextran reduces erythrocyte aggregation andplatelet adhesiveness however, can cause acuterenal failure and cerebral oedema
Bleeding risks of antithrombotic therapy. Fitzmaurice. BMJ 2002
PGE-1 in replantation and free tissue transfer: early preliminary experience., Rodriguez and al. Microsurgery 2007
Effect of anticoagulation and inhibition of platelet aggregation on arterail versus, Venous microvascular thrombosis, Li and al. Ann Plast Surg 1995
Topical and systemic anticoagulation in the treatment of absent or compromised venous outflow In replanted fingers. Han and al. J Hand Surg Am 2000
Blood loss associated with anticoagulation in patients with replanted digits, Fumas and al. J Hand Surg Am 1992
No More Than Two
Aspirin 160 mg per day during 15 to 30 days
Low-molecular-weight heparin (LMWH) duringrecovery phase in prophylactic dosage
Anticoagulation therapy in microsurgery: a review. Askari and al. J Hand Surg Am 2006
Etude multicentrique sur la prévention de la thrombose en microchirurgie du membre supérieur. Enquête auprès de la Fesum, Dumont and al. Chir Main 2010
A phase II trial of intraluminal irrigation with RHTF pathway to prevent thrombosis in free flap surgery. Khoury and al. Plast reconstr Surg 2001
Anticoagulation following digital replantationBuckley and al. J Hand Surg Am 2011

PHARMACOLOGICAL SUPPORT
Leeches (Hirudo Medicinalis) up to three days
Bloodletting action
Hirudin >>>> Heparin
Aeromonas hydrophila
Not forcefully removed

COMPLICATIONS
Venous Thrombosis = First cause ofreplantation failure
Arterial thrombosis 3X> but the salvage rate ofdigital replantation complicated by arterialthrombosis is 30% whereas only 7% forvenous occlusion
Maximum risk during first 48 hrs
Speed Reaction < 24 -36 hrs
Removal of the dressing to release anyextrinsic compression
Return to the OR for anastomosis revision

Care should commence as soon as possibleonce vascular survival is confirmed.
Depends upon the strength of theosteosynthesis
Intrinsic part of the functional results
REHABILITATION CARE
www.materiel-pla-medical.fr

CONSENSUAL
INDICATIONS

Again--- many thanks for your recent letter and article. All I can say is congratulations; and I only wish I could have done it.
Successful replantation of a completely cut-off thumb. Komatsu and Tamai. Plastic Reconstr Surg 1968.
THE THUMB

Merle Classification
Merle and al. Chirurgie 1984.
The particularity of thehuman thumb positionmakes it uncomfortable forsurgery and even more sofor the microsurgery.
EVERYTHING MUST BE DONE DUE TO HIGH LEVEL OF HANDICAP

WHEN LOCAL ANASTOMOSIS IS POSSIBLE

WHEN LOCAL ANASTOMOSIS IS NOT POSSIBLE
When local anastomosis is difficult pre placement of venous interposition graft.
Proximal anastomosis at the snuff box.

30 year old man
Mixed crush and stripping injury
No dorsal vein available only dorsal collateraland ulnar palmar artery in the amputated part
PINCH TAKES PRIORITY OVER MOBILITY
EVEN IF IT SEEMS COMPLICATED…

Fukui and al. J Hand Surg Am 1990.
ARTERIO VENOUS SHUNT IN DIGIT REPLANTATION
Ulnar palmar artery anastomosed
Dorsal artery anastomosed with radial dorsal vein

Le lambeau cerf-volantFoucher. Ann Chir 1978.
VENOUS FLOW-THROUGH KITE FLAP
IN CASE OF DORSAL VEIN AND SKIN DEFECT

PRIMARY THUMB RECONSTRUCTION WITH SPARE FINGERS
When the thumb is missing
In case of multiple digit amputations
But not everything

WAIT AND SEE TO PRESERVE THE FUTURE
Delayed reconstruction by index stump pollicization wrapped with a partial great toe transfer
Barbato and al. J Hand Surg Eur 1998

DISTAL REPLANTATIONS
Good indications
Distal to FDS insertion
Simultaneous procedure on amputated part and hand
DIP Fusion and skeletal shortening
• Replantations digitales distales, Dautel and al. La Main 1997.• Fingertip replantation, Hatori and al. J Hand Surg Am 2007.• Distal and very distal digital replantations., Foucher. Br J Plast Surg 1992.• Twenty years’ experience of limb replantationreview of 293upper extremity
replants., Tamai S. J Hand Surg Am 1982.

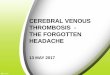
ISHIKAWA CLASSIFICATION
Predetermines the possibility of repairing both an artery and a vein
From Zone 3 and above, the possibility of nerve, vein and artery repair
Nerve repair difficult above tuft zone
Suzuki and Ishikawa. Br J Plastic Surg 1993.

DISTAL ARTERY ANASTOMOSIS
Pulp central artery even more so with the detour of the arcade to permit length gain in case of artery defect and favor end-to-end anastomosis, in order to avoid a venous graft in this minute environment.
Ultra micro anastomosis 11-0 NYLON/50µm needle
First back wall repair: free clamp suture
Harris and al. Br J Past Surg 1981

WHEN VENOUS REPAIR IS POSSIBLE
Success rates of distal amputation to the DIP have been reported between 70 to 90%
Post-operative outcomes are favorable

Suzuki and al. Br J Plast Surg 1993.
Last Resort: Artery only replantation with controlled bleeding, leeches and AC therapy
3 or more anticoagulation agents increase the blood transfusion to 50%
Furnas and al. J Hand Surg Am 1992Buntic and al. J Hand Surg Am 2010
VENOUS REPAIR CAN BE DIFFICULT IN ZONES 2 AND 3
A-V fistula by anastomosing a second available artery to a palmar vein

SKIN CLOSURE IN DISTAL REPLANTATIONS
De-eperdimization of the stump skin, of the amputated part and the proximal digit bank, on 1-2mm closure is made then overlaying the two de-epidermized surfaces which increase the cutaneous surface contact and venous neoconnections

ZONE 3 REPLANTATION

MULTIPLE DIGIT AMPUTATIONS
Distal Multiple Digit Amputations
Attempts all digits with priority to the thumb
The Problems:
Proximal complex crush injury amputations
Multiple digit amputations and soft tissue loss

MULTIPLE DIGIT COMPLEX INJURY
Team concept for strategic decisions and multiple surgeons for simultaneous surgeries
Each patient is unique
Replantation priorities
Creative use of « spare parts bank » the most usable part in the most effective position with priority to the THUMB
Foucher. Ann Chir 1980.

MULTIPLE DIGIT COMPLEX INJURY
Additional procedure flap can lead to failure
Abdominal flap is uncomfortable
Local pedicle flap as forearm interrupts an artery flow

STRATEGIC DECISION MAKING IS THE MAIN POINT
Revascularisation attempt in the famous area up to the Flexor digitorum superficialis tendon insertion leads to poor functional outcome
This case can be discussed in other ways

USEFUL FUNCTION OF THE HAND
The number of digits useful for replantation drives the process along with the equilibrium for the most useful function of the hand
In any case the index postion is the one to be least considered
Rad
ial side fo
r pin
ch
Uln
ar side fo
r grasp

TRANSMETACARPAL AMPUTATION
This is a challenge in efficiency
Ischemia of the intrinsic muscles with resultant sclerosis and contracture
Vascularization of intrinsic muscles by palmar arcade
Resection of the involved intrinsic musculature and adequate metacarpal shortening (at least 12mm) should be considered
Meyer and alJ Bone Joint Surg Br 1976.

BLOOD FLOW RESTORATION
Direct VY vein graft
Direct arterial anastomosis when possible
or
VY venous graft
Foot dorsal arcade

Potency of one common digital vessel provides blood flow to all fingers through transverse and commissural skin arteries
Nakamura and al. J Microsurgery 1980.
Tonkin and al. J Hand Surg Br 1988.Salmon M, Masson 1936
BLOOD FLOW RESTORATION

TRANS METACARPAL REPLANTATION

RING FINGERS AVULSION

COMPLETE RING FINGER AVULSION
Challenging procedure
Controversial replantation
Undeserved badreputation

STAGE DESCRIPTION
I Circulation adequate with or without skeletal injury
II Circulation inadequate, no skeletal injury
IIA Arterial circulation inadequate only
IIB Venous circulation inadequate only
III Circulation inadequate with fracture or joint injury present
IIIA Arterial circulation inadequate only
IIIB Venous circulation inadequate only
IV Complete Amputation
IVd Amputation distal to the FDS* insertion
IVp Amputation proximal to the FDS insertion
* FDS: FlexorDigitalSuperficialis
• Urbaniak and al. J Hand Surg Am 1981• Kay et al. J Hand Sur Am 1989• Adani et al. J Reconstr Micro 1996
RING FINGER AMPUTATION

THE RECIPE
Short hemi-Bruner incision at DIP joint for artery location
No sheath splitting
Skeletal osteosynthesis using a needle cap as protection
The use of a vein graft increase the vascular success
Firstly: vein graft distally anastomosed

RING FINGER REPLANTATION
Subcutaneous passage of the venous graft and repositioning of the degloving part helped by sterile liquid vaseline
Proximal anastomosis close to the common palmar artery bifurcation
Dorsal veins anastomosis with Vilain flag cutaneous venous flap
Nerve repair difficult (stretching injury) the stretched nerve is inserted distal in the sheath in neurotization procedure
• Vilain. Plast Reconstr Surg 1973.

EARLY MOBILISATION OF THE UNINJURED PIP JOINT
Under medical care control
In order to avoid stiffness

LONG TERM RESULT
• TAM / 157• Hamouya and al. J Hansurg 2018

BECAUSE….
Young adults
Cold intolerance decrease with time
Stiffness is unusual if PIP joint useful
Low sensitivity does not affect function
Less than 10% of base metacarpal resections
Only one among replanted fingers
Even if primary resection has been recommended by few authors
In case of uninjured PIP. At least attempt replantation

SURGICAL EFFICIENCY FOR OPTIMIZED OUTCOMES IN DIGIT REPLANTATION

Basic Thumb Variation
Ring Finger Multi-digit and Transmetacarpal
1 Osteosynthesis 1 Arterial graft on amputated part
1 Arterial graft on amputated part
1 Osteosynthesis
2 Extensor tendon repair
2 Osteosynthesis 2 Osteosynthesis
2 Extensor tendon repair
3 Flexor tendon repair
3 Proximal arterial anastomosis
3 Proximal arterial anastomosis
3 Vein repair/ Venous flap
4 Arterial repair/ reconstruction
4 Extensor tendon repair
4 Arterial repair/ reconstruction
4 Flexor tendon repair
5 Nerve repair/ reconstruction
5 Flexor tendon repair
5 Nerve repair or neurotization
5 Arterial repair/ reconstruction
6 Vein repair/ reconstruction
6 Nerve repair/ reconstruction
6 Vein repair/ Venous flap
6 Nerve repair/ reconstruction
7 Skin Closure 7 Vein repair/ Venous flap
7 Skin Closure 7 Skin Closure
8 Dressing and splint
8 Skin Closure 8 Dressing and splint
8 Dressing and splint
9 Dressing and splint
: with or without tourniquet
Basic Thumb Variation
Ring Finger Multi-digit and Transmetacarpal
1 Osteosynthesis 1 Arterial graft on amputated part
1 Arterial graft on amputated part
1 Osteosynthesis
2 Extensor tendon repair
2 Osteosynthesis 2 Osteosynthesis
2 Extensor tendon repair
3 Flexor tendon repair
3 Proximal arterial anastomosis
3 Proximal arterial anastomosis
3 Vein repair/ Venous flap
4 Arterial repair/ reconstruction
4 Extensor tendon repair
4 Arterial repair/ reconstruction
4 Flexor tendon repair
5 Nerve repair/ reconstruction
5 Flexor tendon repair
5 Nerve repair or neurotization
5 Arterial repair/ reconstruction
6 Vein repair/ reconstruction
6 Nerve repair/ reconstruction
6 Vein repair/ Venous flap
6 Nerve repair/ reconstruction
7 Skin Closure 7 Vein repair/ Venous flap
7 Skin Closure 7 Skin Closure
8 Dressing and splint
8 Skin Closure 8 Dressing and splint
8 Dressing and splint
9 Dressing and splint
: with or without tourniquet
GUIDE TO WORKFLOW EFFICIENCY IN DIGIT REPLANTATION
1 o
r more
tourn
iquet ru
ns

CONCLUSION
EFFICIENCY DEPENDS ON LEARNING, TRAINING AND EXPERIENCE
+ =
SURVIVAL TISSUE DOES NOT EQUATE WITH FUNCTIONAL AND AESTHETIC OUTCOME