Embed Size (px)
Citation preview
Dilatation and Curettage (D&C)
BSN III – F
Group 18
Dilatation and Curretage
It is a gynecological procedure in which the lining of the uterus (endometrium) is scraped away this procedure involves expanding or enlarging the entrance of a woman's uterus so that a thin, sharp instrument can scrape or suction away the lining of the uterus and take tissue samples.It is minor surgery performed in a hospital or ambulatory surgery center or clinic. D&C is usually a diagnostic procedure and seldom is therapeutic. It may stop bleeding for a little while (2-6 months), then the prior abnormal bleeding tends to return.
Purpose
D&C is commonly used to obtain tissue for microscopic evaluation to rule out cancer. The procedure may also be used to diagnose and treat heavy menstrual bleeding and to diagnose endometrial polyps and uterine fibroids. D&C can be used to remove pregnancy tissue after a miscarriage, incomplete abortion, or childbirth, or as an early abortion technique up to 16 weeks. Endometrial polyps may be removed, and sometimes benign uterine tumors (fibroids) may be scraped away.
A D&C is often used for the following conditions:
o Irregular bleeding: You may experience irregular bleeding from time to time, including spotting between periods. If the spotting develops into continuous midcycle bleeding, your health care provider may perform a D&C to investigate the cause of bleeding.
Too much bleeding: Bleeding with long, heavy periods, or bleeding after menopause, can signal a number of problems. These symptoms may not need immediate investigation. You may observe and record them. At some point, though, your doctor may look for a cause that is best detected with a hysteroscopy. Fibroids and polyps: These conditions are very common. In fact, they
are thought to occur in about 20% of all women. Fibroid tumors are noncancerous growths appearing in and on the uterus. Some even grow out from the uterine wall on a stalk. Fibroids can cause chronic pain and heavy bleeding. Polyps, like fibroids, are noncancerous growths and are a common cause of irregular bleeding. Polyps and fibroids can have symptoms that resemble other more serious causes of bleeding. Your doctor may still want to perform a hysteroscopy.
Endometrial cancer: Cancer is a scary word, especially when it is said about you. A D&C and hysteroscopy are often performed to make certain your symptoms are not caused by uterine cancer. It is, of course, important to detect cancer in its earliest, most curable stages
Therapeutic D&C: A D&C is often planned as treatment when the source of the problem is already known. One situation is an incomplete miscarriage or even full-term delivery when, for some reason, the uterus has not pushed out all the fetal or placental tissue inside of it. If tissue is left behind, excess bleeding can result, perhaps even life-threatening bleeding. This is an important reason why your doctor will want to remove any remaining tissue with a D&C.
Your health care provider will avoid D&C in the following situations, except when absolutely necessary:
there is a chance the surgical instruments that will enter the vagina and cervix can carry the bacteria from your vagina or cervix into your uterus. There is also an increased risk of injury to infected tissue. For these reasons, your doctor may prefer to wait until after the infection is cleared up with antibiotics before performing the D&C.
Blood clotting disorders: Doctors depend on the body's natural ability to clot to stop bleeding after curettage. Women with certain blood disorders are usually not given this surgery.
Serious medical problems: Heart and lung disease, for example, can make general, and sometimes local, anesthesia risky.
In fact, D&C is no longer performed as commonly as it was even a decade ago, thanks to advances in diagnosis (e.g., ultrasound and hysteroscopy) and nonsurgical hormonal (e.g., oral contraceptives) and antihormonal (e.g., Lupron) therapies.
Description D&C is usually performed under general anesthesia, although local or
epidural anesthesia can also be used. Using local anesthesia reduces risk and costs, but the patient will feel cramping during the procedure. The type of anesthesia used often depends upon the reason for the D&C.
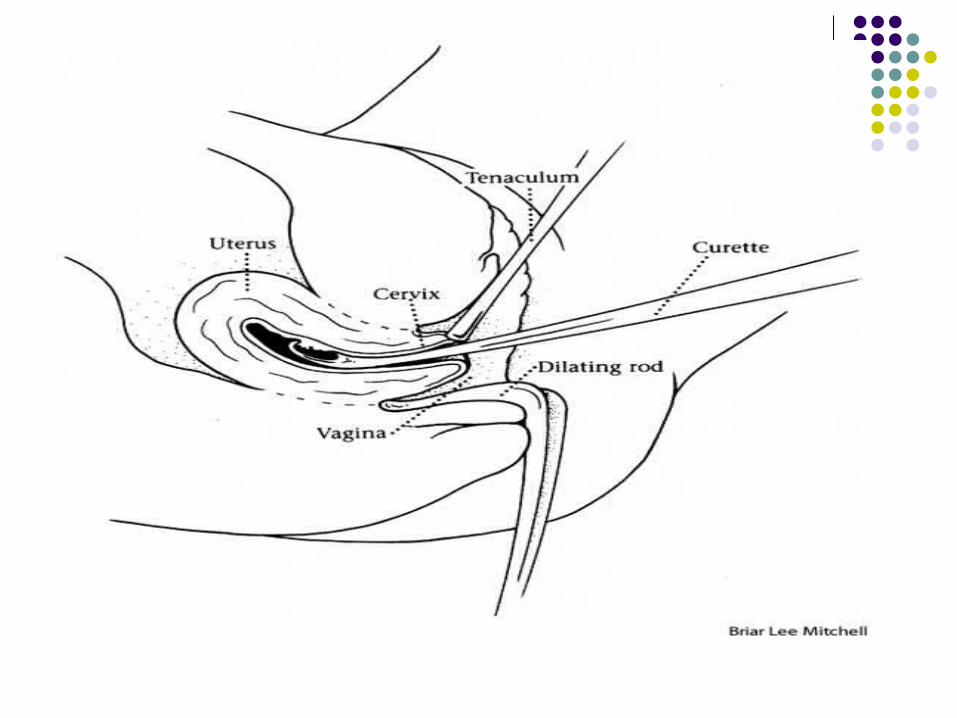
To begin the procedure (which takes only minutes to perform), the doctor inserts an instrument to hold open the vaginal walls, and then stretches the opening of the uterus to the vagina (the cervix). This is done by inserting a series of tapering rods, each thicker than the previous one, or by using other specialized instruments. The process of opening the cervix is called dilation.
Once the cervix is dilated, the physician inserts a spoon-shaped surgical device called a curette into the uterus. The curette is used to scrape away the uterine lining. One or more small tissue samples from the lining of the uterus or the cervical canal are sent for analysis by microscope to check for abnormal cells.
Although simpler, less expensive techniques such as a vacuum aspiration are quickly replacing the D&C as a diagnostic method, it is still often used to diagnose and treat a number of conditions, especially when cancer is suspected.
Preparation Because opening the cervix can be painful, sedatives may be
given before the procedure begins. Deep breathing and other relaxation techniques may help ease cramping during cervical dilation.
Aftercare A woman who has had a D&C performed in a hospital can
usually go home the same day or the next day. Many women experience backache and mild cramps after the procedure, and may pass small blood clots for a day or so. Vaginal staining or bleeding may continue for several weeks.
Most women can resume normal activities almost immediately. Patients should avoid sexual intercourse, douching, and tampon use for at least two weeks to prevent infection while the cervix is closing and to allow the endometrium to heal completely.
Risks The primary risk after the procedure is infection. Signs of
infection include: Fever severe cramps foul-smelling vaginal discharge A woman should report any of
these symptoms to her doctor, who can treat the infection with antibiotics before it becomes serious.
Hemorrhage: Heavy bleeding is rare, but it can happen if an instrument injures the walls of your uterus. It also can occur if an undetected fibroid is cut during curettage.
Infection: There is always a slight possibility of infection once instruments are inserted into the uterus. Most infections can be easily cured with antibiotics. Some can be very serious.
Cont….. Perforated uterus: This complication, though rare, is more common in women
who have a uterine infection at the time of the procedure, in elderly postmenopausal women, and if the procedure is being done for a miscarriage. If your doctor suspects this condition has developed, you may be asked to stay in the hospital for observation or further surgery.
Asherman syndrome: This complication is rare and involves the formation of scar tissue in the uterus, caused by aggressive scraping or abnormal reaction to the scraping. Thick scars can result, which can fill up the uterus completely. This can cause your menstrual periods to stop and make you infertile (unable to get pregnant).
Missed disease: Studies indicate that only 10-20% of the endometrial cavity is actually scraped during a D&C, so there is a chance the disease could go undetected. This is why the procedure is seldom done without a hysteroscopy anymore.
D&C is a surgical operation, which carries certain risks associated with general anesthesia. Rare complications include puncture of the uterus (which usually heals on its own) or puncture of the bowel or bladder (which requires further surgery to repair)
Normal Results
Results are considered normal if no unusual thickening, growths, or cancers are found. Removal of the uterine lining causes no side effects, and may be beneficial if the lining has thickened so much that it causes heavy periods. The uterine lining soon grows again normally, as part of the menstrual cycle.
Abnormal Results Some types of uterine thickening, called hyperplasia, are considered abnormal.
Simple hyperplasia is a benign condition in which the uterine lining becomes thicker and with more endometrial glands. In complex hyperplasia, another condition where the uterine lining has thickened, the endometrial glands are crowded together. In 80% of cases these conditions will improve, and there is little risk of cancer. Only 1% of simple hyperplasia and 3% of complex hyperplasia will become cancerous.
Atypical hyperplasia is a more serious finding. In this type of endometrial thickening, the cells are abnormal. Twenty-nine percent of women with atypical hyperplasia develop cancer. In fact, in 17% to 25% of women with atypical hyperplasia who have a hysterectomy within one month of diagnosis, a carcinoma is found elsewhere in the endometrium.A D&C is not a fool-proof procedure because only a portion of the uterine lining is sampled. Therefore, it is possible for a cancer to be missed. Because of this, patients with atypical hyperplasia must have another D&C in three or four months. Combining a hysteroscopy (a procedure where a physician can see the lining of the uterus using a special tool) with D&C may increase the accuracy of the diagnosis in some cases. However, this combination is not recommended when endometrial carcinoma is suspected because of the possibility that the hysteroscopy itself can aid in the spread of cancer through the fallopian tubes.
ANATOMY AND PHYSIOLOGY
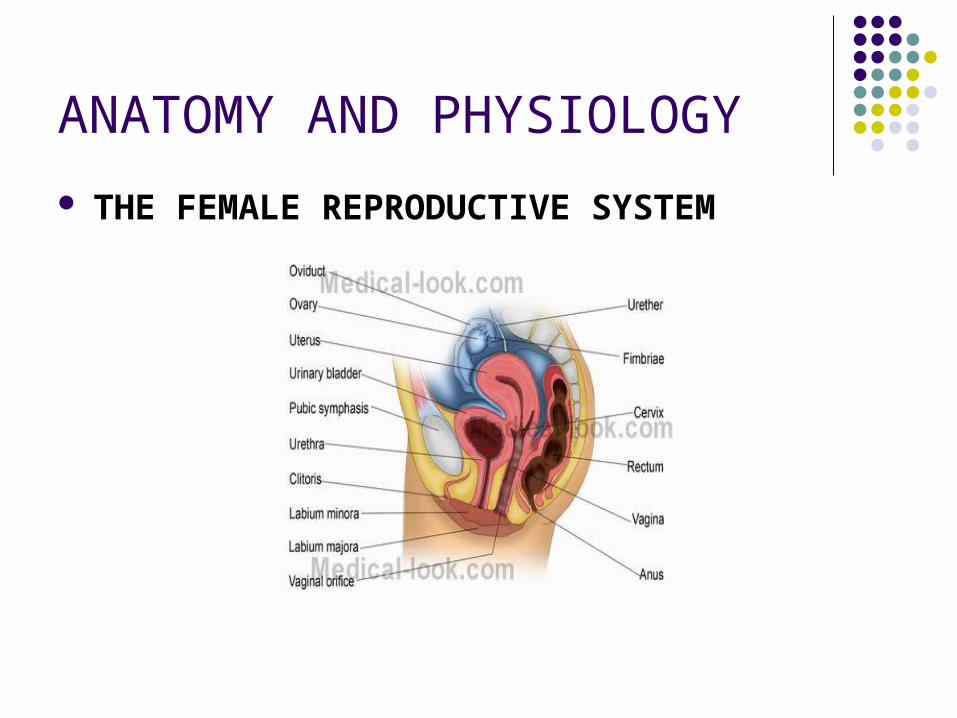
THE FEMALE REPRODUCTIVE SYSTEM
Cont…. The female reproductive system is designed to carry out several functions. It
produces the female egg cells necessary for reproduction, called the ova or oocytes. The system is designed to transport the ova to the site of fertilization. Conception, the fertilization of an egg by a sperm, normally occurs in the fallopian tubes. After conception, the uterus offers a safe and favorable environment for a baby to develop before it is time for it to make its way into the outside world. If fertilization does not take place, the system is designed to menstruate (the monthly shedding of the uterine lining). In addition, the female reproductive system produces female sex hormones that maintain the reproductive cycle.
During menopause the female reproductive system gradually stops making the female hormones necessary for the reproductive cycle to work. When the body no longer produces these hormones a woman is considered to be menopausal.
What parts make-up the female anatomy? The female reproductive anatomy includes internal and external structures. The
function of the external female reproductive structures (the genital) is twofold: To enable sperm to enter the body and to protect the internal genital organs from infectious organisms. The main external structures of the female reproductive system include:
EXTERNAL FEMALE GENITALIA
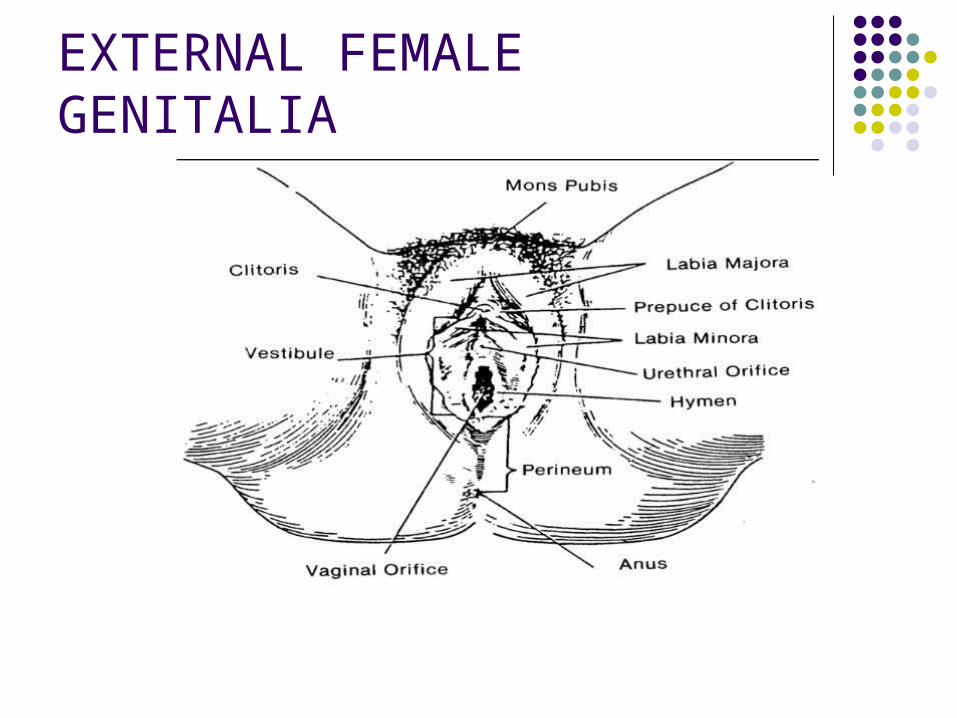
Cont….. The external organs of the female reproductive
system include the mons pubis, labia majora, labia minora, vestibule, perineum, and the Bartholin's glands. As a group, these structures that surround the openings of the urethra and vagina compose the vulva, from the Latin word meaning covering.
a. Mons Pubis. This is the fatty rounded area overlying the symphysis pubis and covered with thick coarse hair.
b. Labia Majora. The labia majora run posteriorly from the mons pubis. They are the 2 elongated hair covered skin folds. They enclose and protect other external reproductive organs.
Cont…. c. Labia Minora. The labia minora are 2 smaller folds enclosed
by the labia majora. They protect the opening of the vagina and urethra.
d. Vestibule. The vestibule consists of the clitoris, urethral meatus, and the vaginal introitus.
The clitoris is a short erectile organ at the top of the vaginal vestibule whose function is sexual excitation.
The urethral meatus is the mouth or opening of the urethra. The urethra is a small tubular structure that drains urine from the bladder.
The vaginal introitus is the vaginal entrance. e. Perineum. This is the skin covered muscular area between
the vaginal opening (introitus) and the anus. It aids in constricting the urinary, vaginal, and anal opening. It also helps support the pelvic contents.
Cont….
f. Bartholin's Glands (Vulvovaginal or Vestibular Glands). The Bartholin's glands lie on either side of the vaginal opening. They produce a mucoid substance, which provides lubrication for intercourse.
INTERNAL FEMALE ORGANS
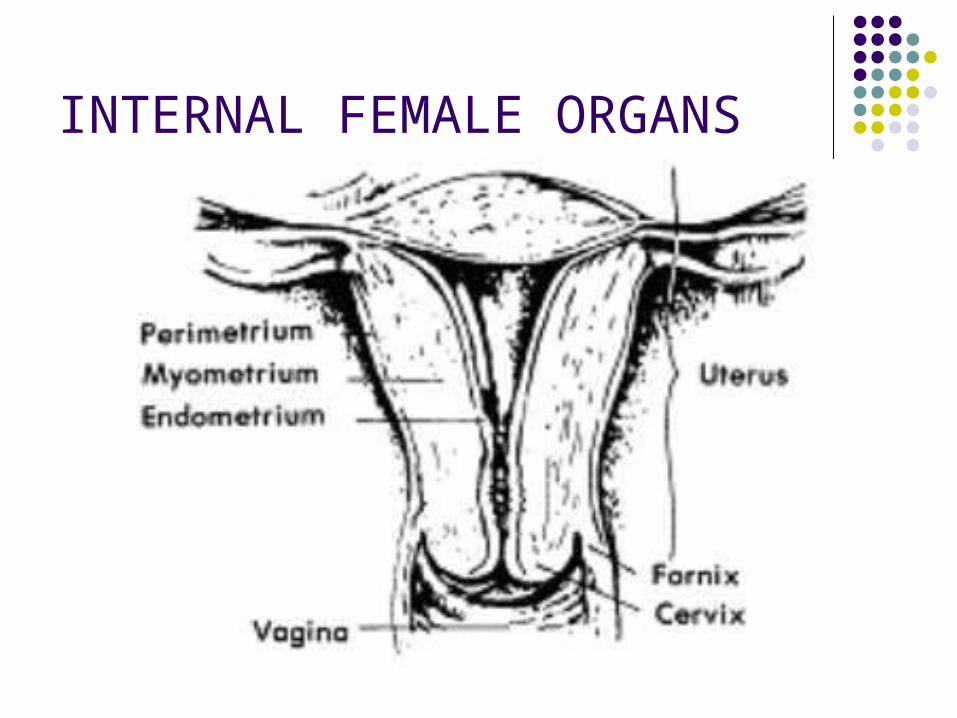
Cont…. The internal organs of the female consists of the uterus, vagina,
fallopian tubes, and the ovaries. a. Uterus. The uterus is a hollow organ about the size and shape
of a pear. It serves two important functions: it is the organ of menstruation and during pregnancy it receives the fertilized ovum, retains and nourishes it until it expels the fetus during labor.
Location: The uterus is located between the urinary bladder and the rectum. It is suspended in the pelvis by broad ligaments.
Divisions of the uterus: The uterus consists of the body or corpus, fundus, cervix, and the isthmus. The major portion of the uterus is called the body or corpus. The fundus is the superior, rounded region above the entrance of the fallopian tubes. The cervix is the narrow, inferior outlet that protrudes into the vagina. The isthmus is the slightly constricted portion that joins the corpus to the cervix.
Walls of the uterus: The walls are thick and are composed of three layers: the endometrium, the myometrium, and the perimetrium. The endometrium is the inner layer or mucosa. A fertilized egg burrows into the endometrium (implantation) and resides there for the rest of its development. When the female is not pregnant, the endometrial lining sloughs off about every 28 days in response to changes in levels of hormones in the blood. This process is called menses. The myometrium is the smooth muscle component of the wall. These smooth muscle fibers are arranged. In longitudinal, circular, and spiral patterns, and are interlaced with connective tissues. During the monthly female cycles and during pregnancy, these layers undergo extensive changes. The perimetrium is a strong, serous membrane that coats the entire uterine corpus except the lower one fourth and anterior surface where the bladder is attached.
Cont…. b. Vagina. Location: The vagina is the thin in walled muscular tube about 6 inches long
leading from the uterus to the external genitalia. It is located between the bladder and the rectum.
Function: The vagina provides the passageway for childbirth and menstrual flow; it receives the penis and semen during sexual intercourse.
c. Fallopian Tubes Location: Each tube is about 4 inches long and extends medially from each
ovary to empty into the superior region of the uterus. Function: The fallopian tubes transport ovum from the ovaries to the uterus.
There is no contact of fallopian tubes with the ovaries. Description: The distal end of each fallopian tube is expanded and has finger-
like projections called fimbriae, which partially surround each ovary. When an oocyte is expelled from the ovary, fimbriae create fluid currents that act to carry the oocyte into the fallopian tube. Oocyte is carried toward the uterus by combination of tube peristalsis and cilia, which propel the oocyte forward. The most desirable place for fertilization is the fallopian tube.
Cont… b. Vagina. Location: The vagina is the thin in walled muscular tube about 6 inches long leading from
the uterus to the external genitalia. It is located between the bladder and the rectum. Function: The vagina provides the passageway for childbirth and menstrual flow; it
receives the penis and semen during sexual intercourse. c. Fallopian Tubes Location: Each tube is about 4 inches long and extends medially from each ovary to empty
into the superior region of the uterus. Function: The fallopian tubes transport ovum from the ovaries to the uterus. There is no
contact of fallopian tubes with the ovaries. Description: The distal end of each fallopian tube is expanded and has finger-like
projections called fimbriae, which partially surround each ovary. When an oocyte is expelled from the ovary, fimbriae create fluid currents that act to carry the oocyte into the fallopian tube. Oocyte is carried toward the uterus by combination of tube peristalsis and cilia, which propel the oocyte forward. The most desirable place for fertilization is the fallopian tube.
d. Ovaries Functions: The ovaries are for oogenesis-the production of eggs (female sex cells) and for
hormone production (estrogen and progesterone).
Dilation and Curettage Preparation
Depending on the type of anesthesia used, your doctor's instructions before a D&C will most likely include the following:
Avoid unnecessary drugs: A few days before your D&C, stop taking drugs such as aspirin, which can cause increased risk of bleeding, and any over-the-counter medications, such as cold tablets and laxatives. Avoid alcohol and tobacco use. Many surgeons now recommend you stop taking any herbal supplements at least 2 weeks before surgery. Talk with your doctor about all medications you take.
Chronic conditions: Your doctor will probably want your other medical problems to be under good control before the surgery. For example, if you have uncontrolled high blood pressure, you may be put on a strict treatment plan in or out of the hospital to improve your blood pressure. This is important to avoid any unnecessary complications during the D&C procedure.
Cont……
Eating and drinking: Your doctor will also instruct you not to eat or drink for 12 hours before your D&C if it is done under general anesthesia (you are completely asleep) or for 8 hours before a local or regional (eg, spinal) anesthesia (just the lower portion of your body is numbed and you have no feeling) is used.
Preliminary tests: On the day before or day of the procedure, your doctor may want to obtain certain routine blood, urine, and other tests to be sure no problems have been missed.
During the Procedure Anesthesia Local anesthesia: If you have a local anesthetic, you will lie on
your back in the standard pelvic examination position: legs apart and your knees drawn up. Your doctor will insert an instrument called a speculum into your vagina to hold the vagina wall apart. The doctor or assistant will then clean the inner and outer vagina, including the cervix, with a cleaning solution. The doctor will then steady the cervix with a clamp and inject a local anesthetic into the cervix on either side. This is called a paracervical block and relieves pain from the dilating of the cervix. It does not numb any of the rest of the body.
Spinal anesthesia: A needle is placed in the lower back, usually while the patient is sitting up. Anesthetic is injected through this needle into the spinal fluid that surrounds the spinal cord. This causes numbness usually from the level of the belly button on down. It wears off in 1-3 hours.
Cont….
General anesthesia: If general anesthesia is given, you will not be aware of anything including the cleaning step, after you lose consciousness. You will lie on the table with an anesthesiologist or nurse anesthetist at your head. You may be given an injection of medication to relax you and to dry up any oral secretions. You will then receive an intravenous fast-acting anesthetic and immediately fall asleep for the procedure.
Cont… Dilation (the first step): While grasping the cervix with a clamp, the
doctor will pass a thin, flexible piece of metal called a sound to determine the depth and angle of the uterus. These measurements allow the doctor to know how far into the uterus the curette can be safely inserted. The usual method of dilation is to insert a thin, smooth metal rod gently along the vaginal canal and up into the tiny cervical opening. The rod is left in place for a moment, then withdrawn and replaced by a slightly larger rod. This process is repeated until the cervix has expanded to about the width of a finger. This method takes about 10 minutes. If you are under local anesthesia, you may experience crampy discomfort caused by stretching of the cervical muscles to accommodate the rods. Another method being used with increasing frequency is to insert laminaria tents (cigarette-shaped pieces of a special dried seaweed) into the cervix 8-20 hours before the procedure. The laminaria absorb water from the tissues and swell up, slowly distending and dilating the cervical canal. This is less traumatic than using the metal dilators.
Cont…. Hysteroscopy and curettage (the second step): After
dilation, your doctor holds the vagina open again with the speculum. The doctor may also reach into the cervix with a tiny spoon to obtain a specimen of the cervical lining. At this point, the hysteroscope is usually inserted into the uterus so that the doctor may look at the inside of the uterus. The doctor may see fibroids, polyps, or overgrowths of the endometrium. At that time, instruments may be inserted through the hysteroscope and biopsy, or removal, of these things may be accomplished.
Cont….. The doctor will now place a slightly longer and larger curette
through the dilated cervix and up into the uterus. This is a metal loop on the end of a long, thin handle. With steady, gentle strokes, the doctor will scrape or suction the uterine wall. This tissue is sent to the lab for analysis. When the curettage is completed, the instruments are removed.
If under local anesthesia, you will probably experience a tugging sensation deep in your abdomen as the curetting is performed. If this is too painful, you should tell the doctor, who may then order pain medicine.
The entire procedure, including curettage takes about 20 minutes. At the end, you may have cramps. This may last about 30 minutes
After the Procedure Cramps, like menstrual cramps, will probably be your strongest
sensation immediately after a D&C. Although most women experience cramps for less than an hour, some women may have cramps for a day or longer.
You may also have some light bleeding for several days. You will most likely be placed in the recovery room immediately after the
procedure. Most hospitals and outpatient clinics will keep you for an hour or until you become fully awake. You will need to arrange for a ride home.
It is suggested that you do not drive for at least 24 hours after anesthesia. This is recommended even after a sedative/local anesthesia because these drugs can temporarily impair your coordination and response time.
Naproxen or ibuprofen are usually given for relief from cramping. Narcotics are seldom, if ever, needed for the pain following the D&C.