-
#486231
Dimensions Health Corporation d/b/a Prince George’s Hospital
CenterMount Washington Pediatric Hospital, Inc.
Relocation of a General Acute Care Hospital and a Special
Hospital-PediatricMatter No. 13-16-2351
Responses to Second Completeness Questions Received 11/20/13
1. Regarding the response to Question #5, please provide the
followingclarifications and supporting information:
A. Evidence from either the Prince George's County government or
thePrince George's County Revenue Authority that documents
theirplans to construct a parking garage on the proposed
PGRMCmedical campus.
The County Government, or the Revenue Authority of Prince
George’s County (a
quasi-public corporation), will construct the parking facility
on the medical campus. The
County is working on the specifics of the financing model in
order to incorporate the
project in the upcoming capital improvement program as part of
the County Executive’s
Proposed FY 2015 operating and capital budgets. The County will
provide the proper
documents that will show the County’s / Revenue Authority’s
commitment in the March
2014 timeframe.
Dimensions has asked the County to send a letter to Dimensions,
stating its
intent to build the parking facility to be completed and
operational at the opening of the
proposed PGRMC. Once Dimensions receives this letter, it will
forward a copy to the
Maryland Health Care Commission.
B. While your response states that the parking garage will have
roomfor 1,200 parking spaces, Exhibit 29 indicates the parking deck
willhave 720 spaces. Please correct or explain this
apparentdiscrepancy.
The medical campus will have approximately 1,555 parking spaces
to serve the
proposed PGRMC. The parking spaces would include 720 parking
spaces in the
-
2#486231
parking facility (garage) and an additional 835 surface lot
parking spaces. The
previously stated number of 1,200 parking spaces for the parking
garage was an error.
These parking space numbers have been verified by HOK
Architects.
2. The application states that the proposed project will be
built on landdonated by Prince George's County (application, p.
13). Please disclosethe value of that land donation, and build that
cost into the project cost. Inaddition, the application and
additional information provided states that aparking garage is
being built by the County and that "... The parkinggarage is a
necessary component of the medical campus" (response tocompleteness
questions, p. 5). Upon further reflection, it is MRCC staffview
that the costs associated with the parking garage also
requireinclusion, if PGRMC will pay rent for the garage or benefit
from parking feerevenues. Will PGRMC pay rent and/or receive
payments or revenue fromgarage parking fees? If the answer is yes
to either, please also include thecosts of the parking garage in
the project budget and any revenues andexpenses it the various
versions of Table 3 that have been submitted andany that may be
modified in response to these questions. Resubmit thePROJECT BUDGET
to reflect the additional capital costs of land and, ifapplicable,
the parking garage.
PGHC has subdivided its response into component parts:
A. Value of the land donation.
The appraised value of the Powell property (approximately 8.49
acres) ranges
from $7.5 million to $8.2 million based upon two independent
appraisals of the Powell
parcel by both the County and Retail Properties of America,
Incorporated.
There are no current appraisals for the other 17 acre parcel.
The County
estimates that the value for the 17 acre parcel is approximately
$4.5 million. The Powell
property (8.49 acres) was appraised at a higher value per acre
because it has a
residential use development potential that is not available for
the 17-acre parcel.
Therefore, the total 25.5 acreage site is estimated to have a
value of
approximately $12,350,000.
-
3#486231
As requested by MHCC staff, the estimated value of the donated
land is being
included in the revised Project Budget, which is attached as
Exhibit 42.
B. Will PGRMC pay rent and/or receive payments or revenue from
theparking fee revenues? If the answer is yes to either, please
alsoinclude the costs of the parking garage in the project budget,
andany revenues or expenses.
No, the County Government or the Revenue Authority of Prince
George’s County
will own and operate the garage. PGRMC will be a customer. The
County/Revenue
Authority will collect parking fees from the general public at
an hourly rate. The County /
Revenue Authority would charge PGRMC a fixed amount for parking
spaces leased by
PGRMC for employees, physicians, etc. It is anticipated that
PGRMC would charge
employees (with some exemptions) for use of the parking facility
to help offset the cost
of leasing spaces from the County / Revenue Authority. However,
PGRMC will not
operate the garage, nor will it bear the garage’s operating
expenses or receive revenue
that the garage generates.
3. With respect to the table provided in response to Question 6,
pleaseprovide the following clarifications:
A. Does the reference included above in all instances refer to
theDiagnostic Imaging line? If not, for each line that indicates
thedepartment area is included above please specify the line
thatincludes the square footage.
The existing 17,854 square footage Diagnostic Imaging Space
includes existing
mammography, radiology, ultrasound, flouroscopy, CT, and nuclear
medicine space. In
addition, there are 327 square feet of radiology space in the
existing Emergency
Department.
-
4#486231
The proposed 18,702 square footage Diagnostic Imaging space
includes
proposed mammography, radiology, ultrasound, flouroscopy, CT,
MRI, nuclear
medicine, and bone density space.
PGHC plans an additional 2,240 SF for general radiology, 1,665
SF for CT, and
415 SF for ultrasound in the Emergency Department.
B. For bone density there is no proposed square footage or
reference toanother line in the Table. Please explain or correct
this omission.
The Existing Diagnostic Imaging space does not include bone
density services.
The proposed bone density services space is included in the
18,702 SF proposed
diagnostic imaging space.
C. For the department area for Angiography (the 8th line) the
tableindicates that the space is included above presumably in the
existingand proposed departmental area for Diagnostic Imaging
(seeprevious question), but for proposed capacity refers to
cardiaccatheterization. However, the table specifies departmental
areas forcardiac catheterization and other angiography. Please
correct thereferences or explain the difference between the
angiography on lineeight and the other angiography included with
cardiaccatheterization. If the two references to angiography refer
to twodifferent areas explain or correct the reference to
cardiaccatheterization in the proposed capacity column of the
firstangiography (line 8).
The “Existing Angiography” is included in the 3,939 square
footage of “Existing
Cardiac Catheterization and other Angiography” category (not in
the “Diagnostic
Imaging” category). The “Proposed Angiography” is included in
the 9,800 square
footage of “Proposed Cardiac Catheterization and other
Angiography” (not in the
“Diagnostic Imaging” category).
The revised Table appears below.
-
5#486231
EXISTING PROPOSED
DEPARTMENT DEPARTMENTAREAEXISTINGCAPACITY
DEPARTMENTAREA
PROPOSEDCAPACITY
Cancer Treatment – Medical 0 0 5,996 14
Cancer Treatment - Radiation Oncology 0 0 10,440 2
Diagnostic Imaging (DI) 17,854 18,702
Mammography See Note 1 1 See Note 2 2
Radiology See Note 1 2 See Note 2 3
Ultrasound See Note 1 4 See Note 2 2
Fluoroscopy See Note 1 2 See Note 2 1
Angiography See Note 3 See Note 3 See Note 4 See Note 4
Vascular lab 1,713 1 See Note 5 See Note 5
Echo / EKG / Vascular lab 1,363 4 2,944 4
EMG N/A 0 1,032 2
CT See Note 1 2 See Note 2 1
MRI Mobile 1 See Note 2 1
Nuclear Medicine See Note 1 2 See Note 2 2
Bone Density 0 0 See Note 2 1Cardiac Catheterization and
otherAngiography 3,939 4 9,800 4
Dialysis (acute and chronic) 1,166 8 1,740 6
Neonatal Intensive Care 2,272 24 15,100 24Endoscopy 5,398 3
1,900 2
Note 1: Existing 17,854 square footage Diagnostic Imaging space
includes ExistingMammography, Radiology, Ultrasound, Flouroscopy,
CT, and Nuclear Medicine space.
Note 2: Proposed 18,702 square footage Diagnostic Imaging space
includes ProposedMammography, Radiology, Ultrasound, Flouroscopy,
CT, MRI, Nuclear Medicine, and BoneDensity space.
Note 3: Existing Angiography is included in the 3,939 square
footage of Existing CardiacCatheterization and other
Angiography.
Note 4: Proposed Angiography is included in the 9,800 square
footage of Proposed CardiacCatheterization and other
Angiography.
Note 5: Proposed Vascular Lab is included in the 2,944 square
footage of Proposed Echo /EKG / Vascular lab. In the existing
facility, the vascular lab is located in space dedicated for
thelab. In the proposed facility, the vascular lab will share space
with Echo / EKG.
-
6#486231
4. The response to question #6 appears to indicate that PGHC
does notcurrently offer cancer treatment services. If this
observation is incorrect,please correct the zeros under existing
department area and capacity. Ifthis observation is correct,
explain where the service area populationcurrently receives such
services, and quantify the need for such servicesand the impact on
existing service providers of the establishment of thisservice at
PGRMC.
PGHC currently provides oncology (cancer) services on its campus
including
surgical oncology, and medical oncology services (including
infusion services on the 9th
Floor). PGHC wants to expand its complement of existing oncology
services by
providing radiation therapy services. The development of
radiation therapy services as
a component of PGHC’s existing oncology program would involve
the purchase of
major medical equipment (linear accelerator and other support
equipment), and it
would not be subject to a CON requirement. See COMAR
10.24.01.03.I(2)(d).
Dimensions’ vision is to develop a comprehensive cancer center
with a full array
of diagnostic and treatment services including radiation therapy
services. Dimensions’
goals include achieving Community Cancer Program (CCP)
accreditation from the
American College of Surgeons. There are also plans to have
discussions with
University of Maryland Medical Center’s Greenebaum Cancer Center
to assess any
collaborative opportunities between the two entities. The
University of Maryland
Marlene and Stewart Greenebaum Cancer Center (UMGCC) was
recently named a
National Cancer Institute (NCI)-designated cancer center. A
collaborative relationship
with UMMC could assist in improving local access to clinical
trial programs for cancer
patients residing in Prince George’s County.
Regarding the availability of radiation therapy services, there
are facilities
located in Washington D.C., Virginia, Montgomery County, and
Prince George’s
-
7#486231
County. The facilities located in Prince George’s County that
Dimensions is aware of
include the following:
1. 21st Century Oncology of Maryland: Greenbelt, Maryland
2. MedStar-RadAmerica: Joseph E. Coad Radiation Treatment
Center:
Clinton, Maryland
3. Doctors Regional Cancer Center: Bowie, Maryland and Lanham,
Maryland
Since radiation therapy services are generally provided on an
ambulatory basis,
it is difficult to quantify how many patients seek treatment at
the various locations within
and outside of Prince George’s County and therefore difficult to
quantify impact. From
2007-2009, Prince George’s County averaged approximately 3,056
newly diagnosed
cancer cases per year (DHMH Tumor Registry). Oncology
consultants have estimated
that approximately 45-50% of cancer patients will utilize
radiation therapy services,
while approximately 25% patients may require second course of
radiation treatment.
Dimensions believes that a market capture impact of 15% of
cancer patients from
Prince George’s County from facilities located in Washington
D.C., Virginia,
Montgomery County, and Prince George’s County should not have a
significant impact
on any one facility within the region. As with other components
of the proposed
PGRMC, it is the intent of Dimensions and the Prince George’s
County government to
have high quality comprehensive (secondary and tertiary) medical
care services
available within the County, so to make healthcare available to
those Prince George’s
County residents that are currently seeking their medical care
outside of Prince
George’s County.
-
8#486231
5. The response to Question #9 did not respond to the question
with respectto the capacity of the "Pediatric ED area" and the
staffing of the area. Staffalso finds that the response did not
adequately explain how the unit wouldfunction. Therefore, staff
requests the following information:
A. Will the observation component of the area only serve
pediatricpatients? If no, please explain. If yes, will there be any
otherdedicated observation beds to serve the adult patient
population? Ifyes, what is the size and location of the adult
observation beds? Ifno, where will adult observation patients be
housed?
The observation component of the pediatric area, will serve only
pediatric
patients. There will not be “dedicated” observation beds to
serve observation adult
population. Adult observation patients will be cared for in the
Universal Care Unit,
which will contain 68 beds.
B. Specify the number of patients that can be accommodated in
thisproposed unit at any given time.
Five patients can be accommodated in this proposed unit at any
given time.
Although there is one dedicated inpatient bed, all five beds
will be fully equipped to be
used as either pediatric observation or pediatric inpatient beds
based upon patient care
requirements. The beds will be staffed with pediatric emergency
room physician and
pediatric nursing staff. If the patient has a primary care
physician, care will be
collaborated with the patient’s primary care physician.
C. What has been the historical volume of pediatric ED visits
andpediatric observation days? What has been the variation in
thesevisits and days by day of the week and season? Submit daily
censusdata, if available. Submit projections for the ED visits and
pediatricobservation days following the relocation through 2021 and
describethe methodology.
While the Commission defines pediatrics for the purposes of
projected pediatric
inpatient beds as being between the ages of 0-14, PGHC, like
many hospitals,
-
9#486231
classifies all minors (ages 0-17) who come into the ED as
pediatric patients.1 Table 27
shows the Pediatric ED visits at PGHC by day of week and season
during FY2013.
Daily census data are provided in Exhibit 43A.
Table 27ED VisitsAge 0-17
PGHCFY 2013
Sunday Monday Tuesday Wednesday Thursday Friday Saturday Grand
Total
July-September 158 178 179 126 173 166 170 1,150
October-December 194 203 184 178 177 170 175 1,281
January-March 151 153 153 163 166 171 180 1,137
April-June 164 166 160 139 163 148 159 1,099
TOTAL 667 700 676 606 679 655 684 4,667
Source: PGHC
Table 28 shows the Pediatric Observation visits at PGHC by day
of week and
season during FY 2013. Daily census data are provided in Exhibit
43B. As the table
shows, PGHC currently admits very few patients as observation
patients. PGHC
currently does not have a pediatric hospitalist, and,
consequently, nearly all pediatric
patients who need observation are referred to other facilities,
most frequently,
Children’s National Medical Center (“CNMC”) in Washington, D.C.
Dimensions is
currently negotiating with CNMC to provide pediatric hospitalist
services at PGHC.
1 In PGHC’s bed need projections, pediatrics was defined as the
Commission defines it, ages 0-14.
-
10#486231
Table 28Observation Visits
Age 0-17PGHC
FY 2013
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
TotalJuly-September 4 4 4 5 4 4 6 31October-December 5 3 3 3 8 1 5
28January-March 5 4 4 5 0 6 1 25April-June 6 3 4 2 3 2 2 22TOTAL 20
14 15 15 15 13 14 106
Source: PGHC
PGHC anticipates that the number of patients retained for
observation will
increase dramatically once PGHC has a pediatric hospitalist.
PGHC is working with
CNMC and others to provide the appropriate services that will
enable children to be
seen near where they live, without the necessity or cost of
transport.
PGHC points the Commission to the Letter of Support filed in
Exhibit 18 from
Kurt Newman, MD, President and Chief Executive Officer of CNMC,
which states in
relevant part:
Children's National looks forward to working in collaboration
with theleadership of the new Prince George's County Regional
Medical Centerto assure uninterrupted access to the highest quality
of care to thechildren of the County. Specifically, Children’s
National supports thedevelopment of pediatric emergency department
services and pediatricshort stay beds at the regional medical
center and looks forward todiscussions regarding its provision of
emergency and acute care at thehospital. Children's National is
dedicated to working with the new regionalmedical center, its
leadership and County leadership to develop effectivecollaborations
and agreements that will assure seamless delivery ofhealth care
services for children by the providers of Children's National.
Projections of Pediatric Emergency visits are based on the same
approach as
the projections of ED visits set forth in the CON application.
The assumptions are
-
11#486231
straightforward and follow those in the application. Population
is based on Claritas
estimates and projections. Historical visits and transport
information are from internal
PGHC data.
Total Population 0-14, 2013 203,716ED Visits, PGHC, 0-14, 2013
3,638Estimated Transports, PGHC, 0-14, 2013 904Non-Transport Visits
2,734Use Rate of Non-Transport Visits/Population 0.013421Total
Population, 2021 213,710Non-Transport Visits 2021 2,868Estimated
Transports, 2013 9042013 Pop of Largo EMS Catchment Area 54,9332021
Pop of Largo EMS Catchment Area 55,367Pop Ratio 2021/2013
1.007891Projected Transports 911Total Projected Visits, Age 0-14
3,7792013 PGHC ED Visits, Age 15-17 1029Ratio of Age 15-17 2013
Visits/Age 0-14 Visits 0.282848Projected 2021 Visits Age 15-17
1,069Projected Total ED Visits, 2021 4,848
Currently, Pediatric observation days compose 0.5% of Pediatric
ED visits. As
stated above, PGHC anticipates that this will increase
dramatically when PGHC
provides Pediatric Hospitalist services.
In 2012, PGHC had 4,434 total observation days (all ages) and
52,309 ED visits.
This calculates to 8.5% of ED visits. (4,434 / 52,309 = 0.0848)
At this percentage,
PGHC would expect to have 411 pediatric observation days (4,848
x 0.848 = 410.9).
However, because of overlapping stays and the need to
accommodate peak periods,
PGHC has proposed four observation beds.
-
12#486231
D. At the bottom of page 9 you state that staffing efficiencies
can begained with this model compared to the traditional inpatient
model.Please quantify the staffing efficiencies that will be
achieved and theresultant cost savings. Compare the planned
staffing of the unit withthe staffing of the Hospital's current
pediatric unit.
Recent studies in Health Affairs and supported by the Advisory
Board Company
explain the efficiency of using observation units. These units
can be more efficient for
providing care to certain patients and can result in shorter
lengths-of-stay and lower
costs vs. admitting them to the hospital. According to one study
at Brigham and
Women’s Hospital, researchers found that utilizing an
observation unit could avoid
3,600 inpatient admissions per year at that hospital and save
$4.6 million per year.
Based on this study, the researchers found that the overall
savings to the U.S. health
care system would be $3.1 billion. However, only about one in
three hospitals in the
U.S. utilizes an observation unit.
To assess the impact of more widespread observation unit use,
researchers from
Brigham and Women's Hospital, Northwestern University, and Yale
University reviewed
data in 16 studies to determine the average cost savings per
observation unit visit.
They determined that each observation unit visit saves $1,572
compared to an inpatient
admission.
Staffing an inpatient pediatric unit requires a minimum of 4.5
paid FTEs of a
pediatric RN, a cost of approximately $350,000. This is
inefficient for an ADC of 1+. By
utilizing the pediatric emergency room staff, PGHC projects that
caring for the pediatric
patients in the observation room versus an inpatient unit will
require only 1.5 paid FTEs
for an average of one pediatric patient per day. This results in
a savings of 3.5 paid
-
13#486231
FTEs or approximately $233,000. Also, savings will be realized
in support staff (e.g.,
Unit Clerks) as these resources will also be shared.
References:
The Advisory Board Company: Emergency Departments Save by Using
Observation Units ByShane Williams, AIA, ACHA, LGB, practice area
leader for design at Array Architects(04/24/2013)
Brigham and Women’s Hospital, news release, Sept. 26, 2012.
Pediatric Observation Units in the US: A Systematic Review:
MichelleL. Macy, MD;
Christopher S. Kim, MD; Comilla Sasson, MD; MarieM. Lozon, MD;
and Matthew M.Davis,MD.
From the American Academy of Pediatrics: Pediatric Observation
Units. Gregory P. Conners,MD, MPH, MBA, Sanford M. Melzer, MD, MBA,
Committee On Hospital Care, and CommitteeOn pediatric Emergency
medicine.
6. With respect to the response to Question #13 please provide
the followingclarifications
A. The response indicates that the State contribution to the
project willbe $20 million per year from FY 2014 through FY 2017
and $120million in FY 2018 for a total of $200 million. However,
Exhibit 32indicates a commitment of $30 million in FY 2014 and a
total of $210million. Please correct or explain this
discrepancy.
Exhibit 32 shows a State capital commitment of $30,000,000 in
Fiscal Year 2014
for Prince George’s Hospital System (Dimensions Healthcare
System). Of the
$30,000,000 grant being provided, $20,000,000 is to be allocated
for the new regional
medical center (PGRMC) project. The remaining $10,000,000 is to
be allocated for
capital improvements for Laurel Regional Hospital.
B. The response also indicates that the State legislature will
be asked tocommit an additional $8 million dollars to bring the
total Statecommitment to $208 million. Please reconcile the need to
requestaddition funding with the response to A above.
Exhibit 32 includes excerpts of the State’s capital budget plan,
which shows the
State’s plan to partially fund the proposed regional medical
center (PGRMC) in the
amount of $200,000,000. The FY2014 commitment for the PGRMC
project is
-
14#486231
$20,000,000, followed by plans to provide grants of $20,000,000
in fiscal years 2015,
2016, and 2017, and a $120,000,000 grant in FY2018. The
five-year State Capital
Budget prepared during the 2013 legislative session currently
includes $200,000,000 for
the regional medical center project. The MOU participants will
meet with State
legislators this fall to ask that an additional $8,000,000 in
funding be placed in the
State’s Capital Budget to achieve the original capital funding
amount agreed to be
committed by Prince George’s County and the State ($208,000,000
each). Dimensions
will keep the MHCC staff advised of its progress in obtaining an
additional funding
commitment of $8,000,000 from the State.
If the additional $8,000,000 is not funded by the State, then
the $8,000,000
shortfall in funds will be acquired either through a Prince
George’s County community
capital campaign program and/or if necessary, additional
borrowing for funds (issuance
of long-term debt).
7. Regarding Question #14, please provide information on the
most recenthistory and success of Dimensions Health Corporation in
(1) issuingbonds on the bond market and (2) obtaining loans from
banks. Providedetails on the most recent type of bonds issued on
behalf of Dimensions,including the length of the bonds and interest
rate.
1994 Series Bonds
As of June 30, 2013, approximately $53.5 million of the Series
1994 Bonds
remained outstanding. These 30-year bonds were composed of two
parts with interest
rates of 5.38% and 5.3%. As part of its commitment to this
project, Prince George’s
County has recently assumed and paid off the remaining balance
of these bonds on
behalf of the Corporation.
-
15#486231
Other Long Term Debt
The Corporation has had much success securing a number of
capital leases,
primarily for the acquisition of equipment and other long term
debt for various projects.
From 1996 through 2013 the Corporation has carried outstanding
capital lease
obligations ranging from less than $1 million to $4.3 million
for acquisition of various
types of equipment. Currently, the Corporation has approximately
$5 million in capital
leases on its balance sheet. The table below depicts some of the
more recent activities.
Year Amount Borrowed2008 $2.8 million2009 $1.0 million2011 $1.1
million2012 $1.3 million2013 $2.1 million
In 2013, the Corporation received a letter of commitment to
finance $9 million, of
approximately $20 million of its intended spend on a new
Electronic Medical Records
(EMR) system.
The Corporation also has trust mortgage with a balance of $3.0
million as of
June 30, 2013 with a three-year adjustable interest rate of
3.25%.
8. Regarding the response to Question #23, please provide the
following:
A. The 10-year utilization forecasts from Sg2 and Milliman
(summarydata should be sufficient), and explain the forecast
methodology.
Below is a table from Sg2 for the years of 2013, 2018 and 2023
averaged across
the US population. The table outlines the forecasted number of
discharges for the US,
total US projected population and the number of discharges per
1,000 population.
-
16#486231
YearProjected USDischarges
Projected USPopulation
Discharges per 1,000Population
2013 39,568,076 314,861,807 125.66807122018 39,137,520
325,322,193 120.30387362023 38,101,000 335,782,579 113.4692577
The table above illustrates a projected national ten-year
decline of total
discharges of 3.7% and a projected national inpatient
utilization rate decline of 9.7%.
The table below shows Sg2’s national inpatient forecast by year,
illustrating
factors that are considered in their forecast model. Factors
considered include the
population growth, economic factors, changes in healthcare
technology, policy
formation, and changes in provision of care. Exhibit 44 is a
document that goes into
more detail on Sg2’s modeling for inpatient forecasting.
In regards to Sg2’s forecasting model, the following graph shows
how the
individual factors impact the projected forecast of inpatient
discharges.
Sg2National Inpatient ForecastImpact Factor 2013 2014 2015 2016
2017 2018 2019 2020 2021 2022 2023Index 39,568,076 39,568,076
39,568,076 39,568,076 39,568,076 39,568,076 39,568,076 39,568,076
39,568,076 39,568,076 39,568,076Population 420,391 840,782
1,261,173 1,681,564 2,101,955 2,522,347 2,942,738 3,363,129
3,783,520 4,203,911Epidemiology 227,899 453,722 673,030 876,606
1,056,518 1,200,741 1,287,231 1,325,207 1,327,255 1,315,373Economy
51,142 129,087 249,666 387,261 527,176 584,209 581,680 531,231
480,164 428,483Policy 204,795 278,861 325,196 371,776 420,903
444,482 426,398 410,203 411,155 415,835Innovation and Technology
-135,815 -280,739 -437,862 -609,127 -775,892 -919,361 -1,044,784
-1,169,181 -1,290,715 -1,412,04730-Day Readmissions -228,209
-468,056 -714,231 -900,138 -1,033,407 -1,143,116 -1,214,873
-1,289,961 -1,368,361 -1,446,357Potentially Avoidable Admissions
-66,878 -200,157 -431,151 -766,680 -1,097,362 -1,368,320 -1,582,872
-1,726,768 -1,873,544 -2,022,210Systems of CARE -228,286 -490,145
-822,788 -1,226,180 -1,630,448 -1,964,818 -2,237,276 -2,479,372
-2,713,841 -2,950,064Grand Total 39,568,076 39,813,115 39,831,432
39,671,109 39,383,159 39,137,520 38,924,239 38,726,318 38,532,563
38,323,709 38,101,000
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 10
YearGrowthSg2 Forecast 39,568,076 39,813,115 39,831,432 39,671,109
39,383,159 39,137,520 38,924,239 38,726,318 38,532,563 38,323,709
38,101,000 -3.7%Population-based Only 39,568,076 39,988,467
40,408,858 40,829,249 41,249,640 41,670,032 42,090,423 42,510,814
42,931,205 43,351,596 43,771,987 10.6%
-
17#486231
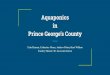
The following graph shows a 10-year trend line, as estimated by
Milliman, an
actuarial firm with claims data for about half of the nation’s
commercial insurers, in a
private study conducted in 2011 for Kaufman, Hall &
Associates. According to Milliman,
“moderate” levels of management are likely to be more
representative of aggregate best
practice for overall levels of medical service utilization, with
inpatient admissions per
1,000 projected to drop from 103 in 2011 to 88 in 2021. Loosely
managed healthcare
markets are expected to see declines to reach the 104 discharges
per 1,000 population
utilization rate. According to Kaufman Hall & Associates,
Milliman’s projected utilization
rates are exclusive of newborn discharges. The Sg2 inpatient
forecasts include newborn
discharges. Therefore, anyone studying these forecasted
inpatient rates needs to
recognize this difference for comparison purposes. Generally,
newborn/neonatal
discharges represent approximately 9-10% of total inpatient
discharges for a population
segment (Source: Sg2 forecast model). Given this assumption, the
Milliman projected
moderate managed care inpatient utilization rate for 2021 would
be approximately 97-98
discharges per 1,000 population.
11%3% 1%
1%-4%
-4%
-5%
-7%-4%
Pop. Epi. Policy Econ. I&T 30 DayReadm.
PAA Sys ofCARE
GrandTotal
2013 - 2023 National by Impact Factor
-
18#486231
Figure 5. Milliman Projections for Inpatient Use Rates for Total
Population (2011-2021)
Source: Private study conducted in 2011 by Milliman for Kaufman,
Hall & Associates, Inc.
Based on the national forecasts and current inpatient
utilization rates of Prince
George’s County, Dimensions concluded to reduce MSGA utilization
rates by
approximately 11% over the projection period. In comparison to
forecasted utilization
rates by Sg2, the projected utilization rates being projected
for the PGRMC service area
are significantly lower than what is being projected for
national rates by Sg2. This is
illustrated below.
NationalPrince George's County Source: Sg2
2012 Total Discharges (incl. Births) 95,8502012 Total Population
891,455
2012 PG County Use Rate 107.52 125.67 (1) -14.4%
Prince George's Regional Medical Center Service Area
2018 Projected Discharges (incl. Births) 96,0942018 Projected
Population 975,840
2018 PGRMC Service Area Use Rate 98.47 120.30 -18.1%
% Change -8.4% -4.3%
PG vs.Nation
(1) - 125.67 represents the 2013 National utilization rate. The
PG County utilization rate isbased on 2012 data.
-
19#486231
Therefore Dimensions has appropriately taken into account
healthcare reform,
population health management principles, and the Maryland
Medicare Waiver initiative
in the development of its inpatient utilization forecasts for
the PGRMC service area.
B. Specify the applicable geographic area for the admission
rates,ALOS, and population shown on pages 20 through 22.
Baseline (FY2012) use rates and ALOS were calculated using
FY2012 actual
data from the current (PGHC) service area by cohort (defined on
pages 24-25 – Table
6). The populations shown on the bottom of page 21 for the years
2012 and 2021
represent the projected PGRMC service area by cohort (defined on
pages 51-52, 85-88,
182 and Tables 7, 11, and 25).
C. Provide a detailed explanation of how the 2012 and 2013 use
ratesand ALOS that appear on pages 20 and 21 were calculated.
FY2012 actual data were utilized for the PGHC current service
area to calculate
use rates and ALOS by cohort. For MSGA (15-64) use rate, the
calculation was 47,122
discharges in the service area / 768,254 population in the
service area X 1,000 for a use
rate of 61.34/1,000 population. For MSGA (15-64) ALOS, the
calculation was 21,740
total LOS for service area / 4,115 total service area cases for
an ALOS of 5.28.
FY2013 ALOS and use rates were projected after the baseline
FY2012 figures
were calculated. Annual changes from 2012 to 2018 were assumed
based on
achievement of the Statewide ALOS, as well as achievement of
initiatives in place at
PGHC during FY2013 and thereafter.
-
20#486231
D. Provide a more detailed explanation of how the ALOS in the
table onthe top of page 21 were projected.
FY2012 actual ALOS was used as a starting point. PGHC has
implemented
initiatives to decrease ALOS and has programs planned to further
improve its position.
Achievement of these initiatives would place PGHC at the
Statewide ALOS, which has
been reflected in the Application.
E. Please provide at least five year historical use rates and
averagelengths of stay for each service comparable to the use rate
andALOS reported on pages 20 and 21 including for each of the two
agegroups used for MSGA volume projections.
Prince George's Hospital Center5-Year Utilization Rate
History
FY2008 FY2009 FY2010 FY2011 FY2012MSGA (15-64) 68.0 69.5 66.7
64.6 61.3MSGA (65+) 309.1 310.5 304.2 304.9 283.2
Prince George's Hospital Center5-Year Average Length of Stay
History
FY2008 FY2009 FY2010 FY2011 FY2012MSGA (15-64) 4.44 4.42 4.44
4.71 5.28
MSGA (65+) 6.62 6.20 6.67 6.17 6.68
F. With respect to the population, the table on the bottom of
page 21reports a population 15+ of 764,050 in the first line which
ispresumably for 2012. However, application page 90 reports a
2012population 15+ of 678,831. Please correct or explain the why
thesenumbers are different.
764,050 represents the MSGA population in FY2012 for the PGRMC
projected
service area. The 678,831 population represented a prior version
of the analysis that
-
21#486231
did not include the addition of four zip codes to the service
area that are not in Prince
George’s County. A revised table has been prepared. See Exhibit
45.
G. Identify the year represented by the projected population on
line 7 ofthe table.
2021.
H. Explain how the total population on lines 1 and line 7
werecalculated. Why do the totals not equal the MSGA total column
plusthe pediatric column?
The PGRMC service area zip codes were utilized for each cohort.
Claritas data
(based on Census) was obtained for 2000 – 2022 by zip code. Line
1 uses the 2012
population for each zip code in the defined projected PGRMC
service area by cohort.
Line 7 uses the projected 2021 population for the same defined
service area.
The total column has an incorrect formula. The 892,770
represents PSY + PED
population in 2012 and the 960,166 represents PSY + PED
population in 2021. The
total 2012 population should be 932,177 and the projected 2021
population should be
1,000,045. This changes the 2012 patient days per capita (total)
to 0.49 (from 0.52),
and 2021 patient days per capita (total) to 0.43 (from 0.44).
The revised percent
change in total patient days per capita is -13.8% (from
-14.0%).
MSGA
15-64 65+ Total OB PED PSY Total
2012Projected Population 666,304 97,746 764,050 169,791 168,128
724,643 932,177AdmissionRate/1,000 61.34 283.22 62.58 20.16
5.25
Admissions 40,869 27,683 68,552 10,626 3,390 3,803
ALOS 5.28 6.68 2.83 2.63 5.45
Patient Days 215,914 184,968 400,882 30,121 8,927 20,712
460,642Patient Days perCapita 0.32 1.89 0.52 0.18 0.05 0.03
0.49
-
22#486231
MSGA
15-64 65+ Total OB PED PSY Total
2021Projected Population 679,026 148,524 827,550 161,617 172,495
787,672 1,000,045AdmissionRate/1,000 54.46 251.47 61.33 20.16
5.25
Admissions 36,982 37,350 74,332 9,913 3,478 4,133
ALOS 4.47 5.39 2.65 2.63 5.76
Patient Days 165,433 201,467 366,900 26,253 9,159 23,808
426,120Patient Days perCapita 0.24 1.36 0.44 0.16 0.05 0.03
0.43
% Change -24.8% -28.3% -15.5% -8.4% 0.0% 5.7% -13.8%
I. While your response cites " . . . an 11.5 decline in MSGA use
ratesbetween 2012 and 2021," virtually all of that decline will
have takenplace by FY 2014. Please explain how this assumption is
consistentwith the State's "Waiver Proposal," which seeks reduced
utilizationthrough population health measures and moving patients
to lessintensive settings.
The State’s Waiver proposal is aimed at reducing the overall
cost of healthcare
expense with emphasis on reducing utilization and costs
associated with hospital care.
The goal would be to have the State’s inpatient utilization
rates, readmission rates, and
other hospital utilization benchmarks be comparable or better
than the national
averages. The inpatient forecasting model for PGRMC takes into
account trends in
population health management as well as current national
inpatient utilization
forecasts.
The assumptions of the inpatient forecasting model take into
consideration a
number of factors including: (1) the current Prince George’s
County inpatient
utilization rate in comparison to national and State inpatient
utilization rates (currently
Prince George’s County has a lower inpatient utilization rate
than the national
average); (2) projected increase in over-65 population for
Prince George’s County
-
23#486231
(Prince George’s County is forecasted to have a higher growth
rate of senior
population in comparison to overall State’s growth rate of the
“over-65” population);
and (3) the current environment where improvements have already
been made in
reducing inpatient cases (conversion of one-day inpatient stays
into observation cases,
progress on reducing readmissions / avoidable admissions,
etc.).
The projected inpatient utilization declines were reviewed and
finalized after
reviewing national forecasts from Sg2 and Milliman. Dimensions
concluded that it
would be appropriate to decrease the utilization rates in the
early years of the
projection period and have stable rates in the later projection
years. Dimensions
believes that the later years in the projection model will see
utilization rate decline
drivers (e.g., reductions of readmission rates, reduced
avoidable admissions, medical
home management initiatives, etc.) offset by the increased
demands of inpatient care
driven by the increasing over-65 age population within Prince
George’s County.
9. Regarding response to Question #25, please provide the
followingclarifications:
A. In your response to question 25 you state: " . . . The
requestreflects an increase of 7% in rates, calculated as 40% of
incrementaldepreciation and interest on the new construction." What
is the basisof the assumption that HSCRC will allow incremental
depreciationand interest at 40%?
Historically, hospitals that qualify for an increase in rates to
cover a portion of
capital costs are eligible for up to 50% of incremental capital
costs. While there is no
capital project funding methodology in place today, PGHC is
confident that an
appropriate rate amount will be approved. The 40% funding
assumption was utilized,
which obviously reflects a lower amount than the 50% historical
level.
-
24#486231
B. Has PGHC andlor UMMS had communication with HSCRC regardinga
rate increase for the proposed project? If yes, please describe
thecommunications especially as they relate to the likelihood
ofreceiving approval for a rate increase under the current
methodologycited in your response to Question 25 and/or
alternativemethodologies.
Prior to filing its CON application, PGHC met with the HSCRC
Staff and
discussed the revenue assumptions that are included in the CON
application.
PGHC looks forward to working with the HSCRC Staff to develop a
responsive and
effective rate structure, likely under a new waiver agreement
and with modifications
to existing methodologies. It is expected that the new waiver
policies will include a
newly developed capital project funding policy which could
potentially include higher
rate increases for capital than included in the CON
application.
10. This project assumes "repatriation" of patients from
hospitals in theDistrict and in VA. With regard to that group of
patients:
A. Quantify the volume that will come from such hospitals and
theamount of revenue associated with that volume?
As provided in Exhibit 27 of the CON Application, 1,611
admissions are
projected to be recaptured from the District of Columbia and 178
from Virginia.
Applying PGHC’s approved FY 2013 charge per case of $14,029
would result in gross
revenue of approximately $25 million in current dollars. Outside
of Maryland,
hospitals negotiate their own rates with payers, thus we are not
able to estimate the
current net patient revenue associated with specific hospitals
in the District of
Columbia or Virginia.
-
25#486231
B. How do payments by Medicare and commercial insurers differ
forsimilar patients receiving care in the District vs. Maryland?
Submitan estimate of the expected savings or increase in cost to
Medicareand to private insurers that would result from the
projectrepatriation. Explain how this estimate was developed.
Payment levels outside the State of Maryland are difficult to
estimate. However,
PGHC has analyzed both AHA published national payment levels as
well as previous
studies prepared in the State of Maryland comparing regulated
vs. national payment
levels.
Commercial payers nationally (and assumed to be the same in the
District) pay
approximately 135% of cost. In Maryland, under the HSCRC, PGHC
estimates that
commercial payers pay between 110% and 115% of costs. Under
these assumptions,
commercial payers are likely paying 20% less in Maryland.
Medicare would obviously pay more in Maryland than it would
under the national
payment system (PPS and OPPS). While no recent computations have
been
developed, based on analyses done a few years ago, the Medicare
inpatient payment
difference was approximately 21%.
11. Regarding Question #30, please respond to the following:
A. Please provide a copy of the Strategic Cardiovascular
Business Plandiscussed on p. 30 - 31, which includes the Market
Assessment andthe Operational Assessment. Please provide the
national and PrinceGeorge's County PCI and cardiac surgery
utilization rates discussedon p. 30.
Copies of the Executive Summary of Dimensions’ Cardiovascular
Program
Strategic Business Plan and the Market Assessment associated
with the Business
Plan are attached, collectively, as Exhibit 46. The full
Business Plan is not
included because it contains confidential and sensitive
commercial information that
-
26#486231
may cause competitive harm to Dimensions and PGHC if disclosed
publicly.
Dimensions believes the Executive Summary and Market Assessment
provide
sufficient detail to address the Commission’s inquiry about
Dimensions’ plan to
strengthen the delivery of cardiovascular services at PGHC.
Also, to protect the
sensitive and confidential commercial information contained in
the Executive
Summary and the Market Assessment, certain limited text was
redacted, as
indicated in the documents. In addition, as indicated, several
typographical errors
were corrected from the original documents, although these
errors were not
material to the Dimensions Board’s consideration of the Business
Plan.
In connection with the Market Assessment, PGHC calculated
cardiovascular
utilization rates as set forth below:
COMPARISON OF CARDIOVASCULAR USE RATE CALCULATIONS(PER 1,000
POPULATION)
PROCEDURE /SOURCE
Claritas 2011Estimates
PrinceGeorge'sCounty
Nat'l HospitalDischargeSummary
Report2010
(Nat’l Rate)
AHA 2012Report(2009Data)
Nat’l Rate
PrinceGeorge's
County ActualExperienceRate 2010
Use RateApplied to2016 Pop.
Proj.Prince
George’sCounty
PCI 2.69 2.02 2.44 1.72 1.99
Cardiac Surgery 1.02 1.09 1.25 0.64 .87
Note: Cardiac surgery includes CABG, Valves and “other” major
cardiothoracic procedures.
Prince George’s County has a lower utilization rate for cardiac
surgery in
comparison to national rates. One reason may be the shortage of
needed primary care
-
27#486231
physicians in the County, possibly causing an under-diagnosing
of cardiovascular
disease and the need for procedural intervention.
B. Please provide the name of the D.C. hospitals and the number
ofcardiac surgery cases performed on Prince George's
Countyresidents in 2010 and more recent years, if available.
Based on hospital inpatient data of Maryland, the District of
Columbia, and
Virginia, below is a table showing cardiac surgery cases of
Prince George’s County
residents.
Location FY 2010 FY 2011 FY 2012D.C. Hospitals
Washington Hospital Center 244 244 236George Washington
University Hospital 27 19 12Howard University Hospital 5 -
-Childrens Hospital NMC 36 40 42
Total D.C. Hospitals 312 303 290Virginia Hospitals 20 12 17Total
Cardiac Surgery Patients in Prince George’s County 556 543 498
C. What are the strategies and outreach efforts that PGRMC will
employto rebuild confidence among local cardiologists and the
communityfor the cardiac surgery program?
Dimensions’ initial strategy to rebuild confidence is to
complete the
implementation of initiatives outlined in the business plan as
well as the program’s
operational/infrastructure enhancement plan, which includes new
cardiac surgery
leadership provided by University of Maryland, increased
staffing ratios, new equipment,
additional staff training, re-vamping of patient care plans,
etc. The primary focus is on
improving the overall patient and physician experience, as well
as demonstrating high
quality outcomes. Operational enhancement will be an ongoing
strategy.
An additional key strategy is to enhance communication and
collaboration among
the cardiovascular physicians and PGHC administration.
-
28#486231
Additional initiatives to re-build confidence among
cardiologists and the
community include:
CARDIOLOGISTS
Both formal and informal grassroots marketing activities will
beimplemented to inform cardiologists of changes in the cardiac
surgeryprogram. For example, one-on-one meetings will be convened
to discuss(a) qualifications of new surgeon/chief of cardiac
surgery; (b) thecardiologist’s preference of post-patient care
involvement; and (c) level ofsatisfaction.
The chief of cardiac surgery personally will call the referring
cardiologistafter each consult and surgery to discuss referred
patient.
PGHC will create a collaborative Heart Team among cardiac
surgery andthe cardiologists to review quality of service provided
andappropriateness of care.
The cardiologists, along with the chief of cardiac surgery, will
participateon PGHC CV service line steering committees, which will
enhancecollaboration and communication.
Grand rounds on cardiac surgery cases and medical staff CME
programswill be conducted. The cardiac surgeon will conduct 3-4
continuingeducation classes for the cardiologists. Topics will be
based onpreferences of the cardiologists, as well as need
determined by the chiefof cardiac surgery.
Performance dashboards for the CV program will be shared with
thecardiologists.
The CV Service Line administrator personally will meet
individually withthe cardiologists on a regular basis to review
changes and discuss anyconcerns.
COMMUNITY
Dimensions and PGHC are in the process of finalizing a
“grassroots”cardiovascular specific marketing plan to focus on
education aboutcardiovascular disease signs and symptoms, when and
how to accesscare, treatment options, and rehabilitation services.
A CV specificspeaker’s bureau will be established and offered to
communityorganizations such as churches, senior centers, Lions Club
and others.During these events, information about PGHC’s
cardiovascular programand physicians will be mentioned and handout
material will be provided.
A formal “closed loop” cardiovascular screening program will
bedeveloped in collaboration with physicians. Closed loop program
refers toensuring appropriate follow-up with individuals identified
to be at highrisk.
Dimensions/PGHC will continue to collaborate with Prince
George’sHealth Department, University of Maryland Medical System,
and otherorganizations to address the shortage of primary care
physicians in the
-
29#486231
county, as well as improving cardiovascular and coronary heart
diseasemortality rates.
Dimensions will also collaborate with local cardiologists to
improveaccess to cardiology care via various strategies such as
physicianrecruitment, outreach clinic development and expansion to
new sites inthe county.
Dimensions will evaluate need and opportunities to have
cardiologists aswell as cardiovascular surgeons see and follow-up
patient visits atdesignated primary care clinics in Prince George’s
County.
As the program matures and results are documented, a traditional
marketingplan will be developed to promote the program to the
community.
D. Organizationally, will PGRMC or the University of Maryland
MedicalSystem control the administration and costs of operating the
cardiacsurgery program?
The cardiac surgery program will be Dimensions’ program. Costs
associated
with the program will be managed by Dimensions. However,
Dimensions is currently
working very closely with the University of Maryland Medical
System and University of
Maryland School of Medicine in developing an effective,
high-quality cardiac surgery
program at PGHC.
Dimensions has contracted with the University of Maryland School
of Medicine
(Faculty Practice Inc. / University of Maryland Surgical
Associates, P.A.) to provide
cardio-thoracic surgeon resources for the cardiac surgery
program. A full-time cardio-
thoracic (CT) surgeon has been recently recruited for Dimensions
and will begin
performing cases at PGHC on or before April 1, 2014. This CT
surgeon will also serve
as Medical Director/Chief of Cardiac Surgery for the cardiac
surgery program and will
be involved in quality assurance initiatives. Three other
cardio-thoracic surgeons from
University of Maryland have obtained privileges at PGHC to
provide additional
coverage. In addition, the Division Chief of Cardiac Surgery at
the University of
-
30#486231
Maryland School of Medicine is contracted by Dimensions to
function as Senior
Administrator of Cardiac Surgery at PGHC.
Dimensions is currently working with the University of Maryland
Medical Center
(UMMC), to arrange for UMMC to provide consultation services
related to clinical staff
training, pre and post-surgical care protocols, and other
support services related to the
cardiac surgery program at Dimensions. UMMC has been sharing
cardiac surgery care
plans and providing training opportunities for PGHC nursing and
physician extenders.
The PGHC cardiac surgery operating team will also be training
with the UMMC team.
Dimensions and UMMC are in the process of finalizing a formal
consultative agreement
related to additional staff training, as well as a contract for
perfusion services whereby
UMMC will oversee the management of perfusion services at
PGHC.
12. Regarding the response to Question #35, please provide the
followingclarifications and additional information:
A. Submit clear statements of assumptions for the revenue
expenseprojections submitted as Exhibits 36 and 37 especially
assumptionsabout the HSCRC update factor and inflationary increases
inexpenses.
Please see Exhibits 47 and 47 for assumptions for the revenue
and expense
projection submitted as Exhibits 36 and 37. Specifically, all
assumptions are the same
as presented in the CON application except the variable cost
factor is adjusted from
85% to 50% per your request.
-
31#486231
B. Regarding the Patient Mix in Exhibits 36 & 37, explain
the basis forthe projected increase in the percent of days and
revenue fromMedicare and commercial insurance and the projected
decrease inthe percentages from Medicaid.
The change in patient mix presented in Exhibits 36 and 37 is
driven by the
recapture of volume. It was assumed that the recaptured volume
would be 40%
Medicare and 60% Commercial insurance patients, which
approximates the historical
payer mix of the targeted volumes going into D.C. and Virginia.
This assumption results
in the increase in the percent of days and revenue for Medicare
and commercial payers
and a resulting decrease in Medicaid volumes as compared to
total patient days and
total revenue.
13. In addition your response to Question #35 states that "...
if the HSCRCdecided to change to the 50 per cent variable cost
factor, it would haveimplications on other assumptions including
but not limited to, increasingrates through the update factor above
inflation.", please respond to thefollowing:
A. Please identify what rate increase would be required to
support theproject if indeed HSCRC uses the 50 variable cost
factor. Also, forthe sake of gaining insight into how the
assumption on variable costreimbursement affects rates, what rate
increase would be required ifHSCRC used a 100 variable cost
factor?
It is important to note that PGHC has been subject to an 85%
variable cost
factor over recent years as volumes declined. The volumes that
are projected to
increase with the opening of a new facility are intended to
recapture those lost
volumes. The same 85% variability cost factor should, therefore,
be applied to these
recaptured volumes.
To support the project, it is assumed PGHC needs to achieve a
1.7% operating
margin by FY 2021. To achieve the same operating margin as
presented in the CON
-
32#486231
application, PGHC would need a 12% rate increase if the HSCRC
uses the 50%
variable cost factor, and a 5% rate increase if the HSCRC uses
the 100% variable cost
factor. No other assumptions were changed between the three
models except for the
variable cost factor and the computed rate increase.
B. You are encouraged to present alternative projections of
revenuesand expenses that include other changes beyond the variable
costfactor. If you submit such an alternative, please provide it
withinflation and, if possible without inflation. Submit a clear
statementof assumptions such as HSCRC update factors, and
projectedinflationary increases in expenses. Show how key changes
inrevenues and expenses are calculated.
The model presented in the CON application is based on current
methodologies
established by the HSCRC. While a new Medicare waiver agreement,
if implemented,
would likely change many of the existing rate methodologies,
PGHC does not wish to
speculate on what potential changes in methodology will be
implemented in the future,
and therefore, does not provide alternative revenue projections
at this time.
14. Regarding the response to Question #46, please provide the
following:
A. Submit the calculations for Exhibit 27 columns 2, 4, 6, and 8
detailingthe impact on each hospital by zip code especially as
thecalculations relate to changes in market share.
Calculations to arrive at Exhibit 27 are provided in Exhibit 49.
Workbooks are
separated by cohort.
B. With respect to column 8 explain and show how the changes
inmarket share by service projected in Table 13 (Application page
92)were converted to the changes in the number of discharges for
eachhospital listed in Exhibit 27.
After determining change in market share by service as shown in
Table 13, the
recapture assumptions were broken down further to split between
DC/VA and MD
-
33#486231
recapture. After determining change in market share by service
as shown in Table 13,
the recapture assumptions were broken down further to split
between DC/VA and MD
recapture. This was done by analyzing the data on the admissions
of Service Area
residents to hospitals in Washington, D.C. and the Public Health
Study performed by
the University of Maryland School of Public Health, which
identified outmigration as an
issue to be addressed by the establishment of a new regional
medical center. PGHC
made reasonable assumptions about the ability to attract people
back to Maryland
based on specialty and discussions with physicians and hospital
leadership.
Discharges assumed to be recaptured from the DC/VA marketplace
were spread
pro-rata based on each hospital’s current ownership of that
market. Discharges
assumed to be recaptured from the MD marketplace were spread
pro-rata based on
each hospital’s current ownership of that market.
For detailed calculations by cohort, refer to Exhibit 49.
C. Regarding column 6 and the relocation methodology described
onApplication pages 88 and 89, please discuss why the
expectedchanges in market share are so great (i.e., zip code 20716
from 6.9 to22.1 and zip code 20710 from 30.8 to 4.5) given current
patientpreferences and relationships with the caregivers.
The expected changes in market share are a direct function of
the Commission’s
own methodology outlined in Commissioner Barbara McLean’s
proposed decision on
the CON application for the relocation of Washington Adventist
Hospital (Docket No.
09-15-2295) (see Proposed Decision, pp. 157-162). The
methodology is discussed in
the application on pages 84-90. Projected market shares in the
new location are
determined based on relative proximity.
-
34#486231
EXHIBITS
42. Revised Project Budget43. A. Daily Census Data FY2013—ED
Visits (Age 0-17)
B. Daily Census Data FY2013—Observation Admissions (Age 0-17)44.
Sg2 Analytics Frequently Asked Questions45. Table 12 Revised ODS
Analysis46. Cardiovascular Services Business Plan Executive Summary
and Market Assessment47. Assumptions for revenue and expense
projection in Exhibit 3648. Assumptions for revenue and expense
projection in Exhibit 3749. Calculations for Exhibit 27
TABLES
27. Daily ED Visits (Age 0-17) FY 201328. Daily Observation
Visits (Age 0-17) FY 2013
-
blrRectangle
-
blrRectangle
-
EXHIBIT 42
-
EXHIBIT 42REVISED PROJECT BUDGET
1. Capital Costs:a. New Construction HOSPITAL/ACC Central
Utility Plant Total
(1) Building $257,572,688 $9,646,917 $267,219,605(2) Fixed
Equipment (not included in construction $0(3) Land Purchase
$12,350,000 $12,350,000(4) Site Preparation $23,904,693 $895,307
$24,800,000(5) Architect/Engineering Fees $17,350,181 $649,819
$18,000,000(6) Permits (Building, Utilities, Etc.) $5,397,834
$202,166 $5,600,000
SUBTOTAL $316,575,395 $11,394,210 $327,969,605
b. Renovations(1) Building(2) Fixed Equipment (not included in
construction(3) Architect/Engineering Fees(4) Permits (Building,
Utilities, Etc.)
SUBTOTAL $0 $0 $0
c. Other Capital Costs(1) Major Movable Equipment $107,000,000
$31,000,000 $138,000,000(2) Minor Movable Equipment $42,400,000
$42,400,000(3) Contingencies $38,555,957 $1,444,043 $40,000,000
(4)
Other (Specify) UMMS PM, Builder's Risk,Commissioning/Testing,
Warehousing, Testing,Traffic Study, Davis Langdon, CM
Pricing,Scheduling, Helipad, Survey, Risk Assesment,Code review,
ICRA, MET Testing, CurtainwallTesting, Legal, Office Consolidation,
Enabling $15,600,000 $15,600,000
SUBTOTAL $203,555,957 $32,444,043 $236,000,000
TOTAL CURRENT CAPITAL COSTS (a - c) $520,131,352 $43,838,253
$563,969,605
d. Non-Current Capital Costs(1) Inflation $26,488,323 $992,072
$27,480,395(2) Capitalized Construction Interest $46,574,555
$3,925,445 $50,500,000
TOTAL PROSOSED CAPITAL COSTS $593,194,230 $48,755,770
$641,950,000 (a - e)
2. Financing Cost and Other Cash Requirements:
a. Loan Placement Fees $6,560,758.68 $539,241.32 $7,100,000.00
b. Bond Discount c. Legal Fees (CON Related) $184,810 $15,189.90
$200,000
d. Legal Fees (Other) $92,405 $7,594.95 $100,000e. Printing
f. Consultant FeesCON Application Assistance $277,215 $22,784.84
$300,000Other (Specify) $277,215 $22,784.84 $300,000
g. Liquidation of Existing Debt h. Debt Service Reserve Fund
$16,355,694 $1,344,305.83 $17,700,000 i. Principal Amortization
Reserve Fund j. Other (Specify)
TOTAL (a - j) $23,748,098 $1,951,901.69
3. Working Capital Startup Costs $109,200,000
TOTAL USES OF FUNDS (1 - 3) $726,142,328 $50,707,671.79
$776,850,000
B. Sources of Funds for Project:
1 Cash2 Pledges: Gross __________,
less allowance foruncollectables __________
3 Gifts, bequests4 Interest income (gross) $15,100,0005
Authorized Bonds $224,200,000
Bond Proceeds - Bridge Loan $128,000,000Bond Repayment with
State Grants -$128,000,000
6 Mortgage7 Working capital loans8 Grants or Appropriation
(a) Federal(b) State $208,000,000(c) Local $208,000,000(c) Local
(Site) $12,350,000
9 Other (Line of Credit) $109,200,000
TOTAL SOURCES OF FUNDS (1 - 9) $776,850,000
-
EXHIBIT 43
-
Exhibit 43ADaily ED Visits
PGHCAge 0-17FY 2013
Day VisitsSun. July 01, 2012 11Mon. July 02, 2012 11Tue. July
03, 2012 16Wed. July 04, 2012 12Thur. July 05, 2012 17Fri. July 06,
2012 12Sat. July 07, 2012 12Sun. July 08, 2012 10Mon. July 09, 2012
15Tue. July 10, 2012 17Wed. July 11, 2012 7Thur. July 12, 2012
10Fri. July 13, 2012 6Sat. July 14, 2012 15Sun. July 15, 2012
15Mon. July 16, 2012 11Tue. July 17, 2012 15Wed. July 18, 2012
4Thur. July 19, 2012 12Fri. July 20, 2012 15Sat. July 21, 2012
8Sun. July 22, 2012 6Mon. July 23, 2012 16Tue. July 24, 2012 17Wed.
July 25, 2012 7Thur. July 26, 2012 18Fri. July 27, 2012 9Sat. July
28, 2012 16Sun. July 29, 2012 10Mon. July 30, 2012 17Tue. July 31,
2012 11Wed. August 01, 2012 9Thur. August 02, 2012 13Fri. August
03, 2012 13Sat. August 04, 2012 9Sun. August 05, 2012 9Mon. August
06, 2012 12
Day VisitsTue. August 07, 2012 11Wed. August 08, 2012 9Thur.
August 09, 2012 13Fri. August 10, 2012 13Sat. August 11, 2012 8Sun.
August 12, 2012 12Mon. August 13, 2012 12Tue. August 14, 2012
11Wed. August 15, 2012 5Thur. August 16, 2012 10Fri. August 17,
2012 12Sat. August 18, 2012 19Sun. August 19, 2012 12Mon. August
20, 2012 8Tue. August 21, 2012 10Wed. August 22, 2012 11Thur.
August 23, 2012 6Fri. August 24, 2012 20Sat. August 25, 2012 8Sun.
August 26, 2012 15Mon. August 27, 2012 12Tue. August 28, 2012
18Wed. August 29, 2012 13Thur. August 30, 2012 13Fri. August 31,
2012 18Sat. September 01, 2012 16Sun. September 02, 2012 13Mon.
September 03, 2012 22Tue. September 04, 2012 15Wed. September 05,
2012 12Thur. September 06, 2012 19Fri. September 07, 2012 8Sat.
September 08, 2012 17Sun. September 09, 2012 11Mon. September 10,
2012 12Tue. September 11, 2012 16Wed. September 12, 2012 7
-
Exhibit 43A - Daily ED Visits (Age 0-17) FY 2013
2
Day VisitsThur. September 13, 2012 19Fri. September 14, 2012
15Sat. September 15, 2012 12Sun. September 16, 2012 10Mon.
September 17, 2012 18Tue. September 18, 2012 11Wed. September 19,
2012 17Thur. September 20, 2012 10Fri. September 21, 2012 15Sat.
September 22, 2012 19Sun. September 23, 2012 14Mon. September 24,
2012 12Tue. September 25, 2012 11Wed. September 26, 2012 13Thur.
September 27, 2012 13Fri. September 28, 2012 10Sat. September 29,
2012 11Sun. September 30, 2012 10Mon. October 01, 2012 10Tue.
October 02, 2012 18Wed. October 03, 2012 12Thur. October 04, 2012
12Fri. October 05, 2012 12Sat. October 06, 2012 13Sun. October 07,
2012 10Mon. October 08, 2012 15Tue. October 09, 2012 10Wed. October
10, 2012 14Thur. October 11, 2012 12Fri. October 12, 2012 11Sat.
October 13, 2012 16Sun. October 14, 2012 13Mon. October 15, 2012
12Tue. October 16, 2012 13Wed. October 17, 2012 14Thur. October 18,
2012 12Fri. October 19, 2012 12Sat. October 20, 2012 12Sun. October
21, 2012 11Mon. October 22, 2012 12Tue. October 23, 2012 16Wed.
October 24, 2012 16
Day VisitsThur. October 25, 2012 13Fri. October 26, 2012 12Sat.
October 27, 2012 3Sun. October 28, 2012 14Mon. October 29, 2012
7Tue. October 30, 2012 15Wed. October 31, 2012 15Thur. November 01,
2012 11Fri. November 02, 2012 16Sat. November 03, 2012 19Sun.
November 04, 2012 19Mon. November 05, 2012 17Tue. November 06, 2012
11Wed. November 07, 2012 13Thur. November 08, 2012 11Fri. November
09, 2012 17Sat. November 10, 2012 11Sun. November 11, 2012 16Mon.
November 12, 2012 16Tue. November 13, 2012 18Wed. November 14, 2012
9Thur. November 15, 2012 18Fri. November 16, 2012 14Sat. November
17, 2012 13Sun. November 18, 2012 10Mon. November 19, 2012 13Tue.
November 20, 2012 11Wed. November 21, 2012 12Thur. November 22,
2012 10Fri. November 23, 2012 11Sat. November 24, 2012 11Sun.
November 25, 2012 12Mon. November 26, 2012 16Tue. November 27, 2012
10Wed. November 28, 2012 7Thur. November 29, 2012 12Fri. November
30, 2012 14Sat. December 01, 2012 12Sun. December 02, 2012 18Mon.
December 03, 2012 16Tue. December 04, 2012 15Wed. December 05, 2012
15
-
Exhibit 43A - Daily ED Visits (Age 0-17) FY 2013
3
Day VisitsThur. December 06, 2012 18Fri. December 07, 2012
14Sat. December 08, 2012 13Sun. December 09, 2012 22Mon. December
10, 2012 25Tue. December 11, 2012 18Wed. December 12, 2012 23Thur.
December 13, 2012 14Fri. December 14, 2012 16Sat. December 15, 2012
17Sun. December 16, 2012 23Mon. December 17, 2012 23Tue. December
18, 2012 21Wed. December 19, 2012 15Thur. December 20, 2012 22Fri.
December 21, 2012 14Sat. December 22, 2012 16Sun. December 23, 2012
13Mon. December 24, 2012 13Tue. December 25, 2012 8Wed. December
26, 2012 13Thur. December 27, 2012 12Fri. December 28, 2012 7Sat.
December 29, 2012 19Sun. December 30, 2012 13Mon. December 31, 2012
8Tue. January 01, 2013 12Wed. January 02, 2013 20Thur. January 03,
2013 25Fri. January 04, 2013 16Sat. January 05, 2013 14Sun. January
06, 2013 9Mon. January 07, 2013 15Tue. January 08, 2013 9Wed.
January 09, 2013 19Thur. January 10, 2013 14Fri. January 11, 2013
15Sat. January 12, 2013 24Sun. January 13, 2013 10Mon. January 14,
2013 17Tue. January 15, 2013 16Wed. January 16, 2013 18
Day VisitsThur. January 17, 2013 15Fri. January 18, 2013 9Sat.
January 19, 2013 7Sun. January 20, 2013 16Mon. January 21, 2013
11Tue. January 22, 2013 11Wed. January 23, 2013 11Thur. January 24,
2013 11Fri. January 25, 2013 4Sat. January 26, 2013 20Sun. January
27, 2013 11Mon. January 28, 2013 7Tue. January 29, 2013 11Wed.
January 30, 2013 18Thur. January 31, 2013 11Fri. February 01, 2013
10Sat. February 02, 2013 9Sun. February 03, 2013 9Mon. February 04,
2013 9Tue. February 05, 2013 13Wed. February 06, 2013 10Thur.
February 07, 2013 4Fri. February 08, 2013 17Sat. February 09, 2013
12Sun. February 10, 2013 12Mon. February 11, 2013 17Tue. February
12, 2013 18Wed. February 13, 2013 19Thur. February 14, 2013 10Fri.
February 15, 2013 17Sat. February 16, 2013 16Sun. February 17, 2013
13Mon. February 18, 2013 7Tue. February 19, 2013 9Wed. February 20,
2013 8Thur. February 21, 2013 19Fri. February 22, 2013 24Sat.
February 23, 2013 14Sun. February 24, 2013 15Mon. February 25, 2013
15Tue. February 26, 2013 10Wed. February 27, 2013 11
-
Exhibit 43A - Daily ED Visits (Age 0-17) FY 2013
4
Day VisitsThur. February 28, 2013 10Fri. March 01, 2013 12Sat.
March 02, 2013 18Sun. March 03, 2013 16Mon. March 04, 2013 19Tue.
March 05, 2013 11Wed. March 06, 2013 8Thur. March 07, 2013 10Fri.
March 08, 2013 10Sat. March 09, 2013 11Sun. March 10, 2013 10Mon.
March 11, 2013 12Tue. March 12, 2013 11Wed. March 13, 2013 7Thur.
March 14, 2013 9Fri. March 15, 2013 16Sat. March 16, 2013 10Sun.
March 17, 2013 7Mon. March 18, 2013 16Tue. March 19, 2013 14Wed.
March 20, 2013 7Thur. March 21, 2013 15Fri. March 22, 2013 12Sat.
March 23, 2013 12Sun. March 24, 2013 11Mon. March 25, 2013 8Tue.
March 26, 2013 8Wed. March 27, 2013 7Thur. March 28, 2013 13Fri.
March 29, 2013 9Sat. March 30, 2013 13Sun. March 31, 2013 12Mon.
April 01, 2013 4Tue. April 02, 2013 12Wed. April 03, 2013 10Thur.
April 04, 2013 12Fri. April 05, 2013 11Sat. April 06, 2013 10Sun.
April 07, 2013 17Mon. April 08, 2013 15Tue. April 09, 2013 11Wed.
April 10, 2013 6
Day VisitsThur. April 11, 2013 10Fri. April 12, 2013 12Sat.
April 13, 2013 18Sun. April 14, 2013 10Mon. April 15, 2013 19Tue.
April 16, 2013 14Wed. April 17, 2013 18Thur. April 18, 2013 15Fri.
April 19, 2013 10Sat. April 20, 2013 5Sun. April 21, 2013 5Mon.
April 22, 2013 11Tue. April 23, 2013 13Wed. April 24, 2013 11Thur.
April 25, 2013 11Fri. April 26, 2013 16Sat. April 27, 2013 16Sun.
April 28, 2013 21Mon. April 29, 2013 15Tue. April 30, 2013 13Wed.
May 01, 2013 6Thur. May 02, 2013 13Fri. May 03, 2013 15Sat. May 04,
2013 9Sun. May 05, 2013 15Mon. May 06, 2013 17Tue. May 07, 2013
16Wed. May 08, 2013 12Thur. May 09, 2013 8Fri. May 10, 2013 14Sat.
May 11, 2013 18Sun. May 12, 2013 10Mon. May 13, 2013 13Tue. May 14,
2013 14Wed. May 15, 2013 11Thur. May 16, 2013 10Fri. May 17, 2013
8Sat. May 18, 2013 15Sun. May 19, 2013 15Mon. May 20, 2013 10Tue.
May 21, 2013 6Wed. May 22, 2013 18
-
Exhibit 43A - Daily ED Visits (Age 0-17) FY 2013
5
Day VisitsThur. May 23, 2013 21Fri. May 24, 2013 11Sat. May 25,
2013 6Sun. May 26, 2013 14Mon. May 27, 2013 16Tue. May 28, 2013
16Wed. May 29, 2013 13Thur. May 30, 2013 11Fri. May 31, 2013 9Sat.
June 01, 2013 7Sun. June 02, 2013 14Mon. June 03, 2013 17Tue. June
04, 2013 7Wed. June 05, 2013 5Thur. June 06, 2013 18Fri. June 07,
2013 12Sat. June 08, 2013 15Sun. June 09, 2013 7Mon. June 10, 2013
7Tue. June 11, 2013 9
Day VisitsWed. June 12, 2013 7Thur. June 13, 2013 10Fri. June
14, 2013 10Sat. June 15, 2013 21Sun. June 16, 2013 11Mon. June 17,
2013 8Tue. June 18, 2013 14Wed. June 19, 2013 16Thur. June 20, 2013
11Fri. June 21, 2013 5Sat. June 22, 2013 8Sun. June 23, 2013 13Mon.
June 24, 2013 14Tue. June 25, 2013 15Wed. June 26, 2013 6Thur. June
27, 2013 13Fri. June 28, 2013 15Sat. June 29, 2013 11Sun. June 30,
2013 12Grand Total 4667
-
Exhibit 43BDaily Observation Admissions
PGHCAge 0-17FY 2013
Day AdmissionsSat. July 07, 2012 1Mon. July 09, 2012 1Sat. July
14, 2012 1Thur. July 19, 2012 1Fri. July 20, 2012 1Thur. July 26,
2012 1Sat. July 28, 2012 1Sun. July 29, 2012 1Wed. August 01, 2012
1Fri. August 03, 2012 1Sat. August 04, 2012 1Tue. August 07, 2012
1Mon. August 13, 2012 1Sat. August 18, 2012 1Mon. August 20, 2012
1Tue. August 21, 2012 2Fri. August 24, 2012 1Sun. August 26, 2012
1Mon. August 27, 2012 1Tue. August 28, 2012 1Wed. August 29, 2012
1Thur. August 30, 2012 1Sun. September 02, 2012 1Wed. September 05,
2012 2Sat. September 15, 2012 1Sun. September 16, 2012 1Thur.
September 20, 2012 1Fri. September 21, 2012 1Wed. September 26,
2012 1Wed. October 10, 2012 1Sat. October 13, 2012 1Thur. October
18, 2012 2Thur. October 25, 2012 1Fri. October 26, 2012 1Wed.
October 31, 2012 1Thur. November 01, 2012 1Mon. November 05, 2012
1
Day AdmissionsThur. November 08, 2012 1Sat. November 17, 2012
1Sun. November 18, 2012 1Mon. November 19, 2012 1Tue. November 20,
2012 1Wed. November 21, 2012 1Thur. November 22, 2012 1Sat.
November 24, 2012 2Mon. November 26, 2012 1Sun. December 02, 2012
2Tue. December 04, 2012 1Thur. December 06, 2012 1Sun. December 09,
2012 2Thur. December 20, 2012 1Sat. December 22, 2012 1Tue.
December 25, 2012 1Sun. January 06, 2013 1Wed. January 09, 2013
1Mon. January 14, 2013 1Fri. January 18, 2013 1Sun. January 20,
2013 1Sun. January 27, 2013 1Fri. February 08, 2013 2Sun. February
10, 2013 1Tue. February 19, 2013 2Fri. February 22, 2013 1Mon.
February 25, 2013 1Fri. March 01, 2013 1Tue. March 05, 2013 1Wed.
March 06, 2013 3Mon. March 11, 2013 1Wed. March 13, 2013 1Fri.
March 15, 2013 1Sat. March 16, 2013 1Mon. March 18, 2013 1Tue.
March 19, 2013 1Sun. March 24, 2013 1
-
Exhibit 43B - Daily Observation Admissions (Age 0-17) FY
2013
2
Day AdmissionsThur. April 04, 2013 1Sat. April 06, 2013 1Sun.
April 07, 2013 2Tue. April 16, 2013 1Sun. April 28, 2013 1Tue.
April 30, 2013 1Wed. May 01, 2013 1Thur. May 02, 2013 1Fri. May 03,
2013 1Sat. May 11, 2013 1Sun. May 19, 2013 2
Day AdmissionsTue. May 21, 2013 1Fri. May 24, 2013 1Tue. May 28,
2013 1Mon. June 03, 2013 1Wed. June 12, 2013 1Sun. June 16, 2013
1Mon. June 17, 2013 1Mon. June 24, 2013 1Thur. June 27, 2013 1
106
-
EXHIBIT 44
-
Confidential and Proprietary © 2013 Sg2 | 1.28.13
www.sg2.com
Sg2 Analytics
Frequently Asked Questions
-
Sg2 Analytics: 2013 Frequently Asked Questions
2 Confidential and Proprietary © 2013 Sg2 | www.sg2.com
Table of Contents
Sg2 Analytics Overview
............................................................................................................................................................
3
Dashboards
..............................................................................................................................................................................
4
Drill-Down Analysis
...................................................................................................................................................................
7
Methodology
.............................................................................................................................................................................
9
-
Sg2 Analytics: 2013 Frequently Asked Questions
3 Confidential and Proprietary © 2013 Sg2 | www.sg2.com
Sg2 Analytics Overview
Q: How do Sg2 Analytics help health care organizations?
A: Sg2 Analytics help organizations prepare for the next decade
in health care, examining the cumulative
effects and interdependencies of key factors driving change in
utilization. Hundreds of organizations rely
on Sg2 Analytics to support service line development, program
investment, innovation adoption, facility
design, performance improvement and strategic planning across
the care continuum.
Q: What is the Sg2 Impact of Change® forecasting model?
A: Sg2’s Impact of Change model forecasts demand for health care
services over the next decade, examining
the cumulative effects and interdependencies of key impact
factors driving change in utilization. Using
both disease-based and MS-DRG–based analyses, the forecast
provides a comprehensive picture of how
patients will access inpatient and outpatient services along the
continuum of care.
Note: In the inpatient setting, the Systems of CARE factor
includes the impact of potentially avoidable admissions
and 30-day readmissions, which can be viewed and analyzed
separately from the other System of CARE impacts in
the forecast.
CARE = Clinical Alignment and Resource Effectiveness; MS-DRG =
Medicare severity diagnosis-related group.
Q: How do Sg2 Analytics integrate the Impact of Change®
forecasting model?
A: Unlike traditional population-based estimates, Sg2’s
comprehensive forecast examines the cumulative
effects and interdependencies of the key factors that drive
change in the utilization of health care services
over a 10-year period. (See the Methodology section on page 8
for more information on the Impact of
Change methodology.)
Q: What is a disease-based forecast?
A: Sg2’s disease-based forecast predicts demand for inpatient
and outpatient services based on Sg2’s
proprietary CARE Group methodology. It forecasts utilization
based on clinical categorizations of ICD-9
diagnosis codes called CARE Families (diseases). CARE Groups
split CARE Families according to the
procedures used to treat the disease or condition. The CARE
Families cut across the inpatient and
outpatient care settings so that organizations can account for
how demand for services will shift between
care settings over time.
-
Sg2 Analytics: 2013 Frequently Asked Questions
4 Confidential and Proprietary © 2013 Sg2 | www.sg2.com
Q: What is the value of a disease-based forecast?
A: Forecasting models based solely on units of payment (eg,
MS-DRGs) do not fully account for changes in
disease states and the actual delivery of care. A disease-based
forecast provides a comprehensive picture
of how patients will access the health care system, including
both inpatient and outpatient services, based
on the prevalence of disease. In doing so, it allows
organizations to identify clinical areas in which to
invest, and informs the allocation of resources across inpatient
and outpatient services. It also supports
the design of more effective marketing/business development
strategies and community outreach plans.
With disease-based forecasting, Sg2 Analytics provide
information that is relevant to different members of
an organization’s leadership team:
Business developers and marketing leaders know that the planning
process starts with the patient. Disease-based forecasting helps
business leaders to understand their market and uncover
opportunities for growth.
Clinical and service line leaders can use disease-based
forecasting to predict which patients will be coming through the
system, how and where they should be treated, and what services
they will need.
Q: What is an MS-DRG–based forecast?
A: An MS-DRG–based forecast predicts demand for health care
services based on units of payment
(Medicare severity diagnosis-related groups). Sg2’s forecasting
model was originally developed using an
MS-DRG–based model for inpatient services. In 2009, Sg2 expanded
its offerings to include inpatient and
outpatient disease-based forecasts that use Sg2’s proprietary
CARE Group methodology. The 2012
National Demand Forecast utilizes MS-DRG Grouper v29.
CFOs and budget planners continue to use MS-DRG–based forecasts
as a tool for building and managing
budgets based on quantified demand.
Q: Why measure performance across the System of CARE?
A: Health care reform suggests that hospitals and health care
systems will increasingly take on more risk and
have more responsibility for managing patients’ overall health,
rather than just the services they provide in
the hospital. Therefore, Sg2 has developed metrics that serve as
proxies for performance for the pre-
acute, acute and post-acute care settings. These metrics are
summarized in the Value Index, a unique
performance score for each Sg2 client.
Q: How do I identify opportunities for performance
improvement?
A: The Organization Performance module contains dashboards that
pre-calculate opportunities for
performance improvement. The intent of this reporting structure
is to expedite opportunity identification
and your organization’s performance improvement process. As
such, these opportunities are prioritized
from largest to smallest at the bottom portion of each dashboard
page. In order to better understand how
these opportunities were calculated or to understand how to take
action to achieve these opportunities,
please contact your organization’s Director of Strategic
Analytics for recommendations.
Dashboards
Q: How do I export data from the dashboards to Excel?
A: From any dashboard, click on the chart or graph from which
you would
like to download data. A blue box will appear around the chart
or graph.
Next, hover your cursor over the export icon at the bottom of
the
page and select either Data or Crosstab and then click
Download.
Once the CSV file is generated, you can choose to either open
or
save it.
-
Sg2 Analytics: 2013 Frequently Asked Questions
5 Confidential and Proprietary © 2013 Sg2 | www.sg2.com
Q: What is the difference between Data and Crosstab?
A: Exporting to Data provides you with an unformatted extract
of
the data contained within a graph or table. For example,
Data
provides every unique combination of measure and year.
Exporting to Crosstab maintains the basic structure of how
the data are presented within a graph or table. For example,
Crosstab provides every year with its own column.
Q: How do I export data from the dashboards to an image or
PDF?
A: To export to an image or PDF, scroll down to the toolbar and
click
on the export icon.
Select Image to export to a PNG file or Print to PDF to export
to
a PDF and then click Download. Once the files are generated,
you can choose either to open or save them.
Q: How do I print?
A: You can print the graphs by using the print function
available in your Internet browser, or by exporting to
Image or Print to PDF and using the print function within your
image viewing program.
Data tables can be printed by exporting to Excel (via Data or
Crosstab) and using the print function
within Excel.
Q: Can I defer a layout update in the dashboard pages? Can I do
the same in the drill-downs?
A: Yes. By clicking the symbol in the toolbar at the bottom of
the dashboard pages, you will defer a layout
update. This means you can make your filter selections without
an immediate update to the graphs. To
update the layout, simply unselect the defer layout option. In
the drill-downs, click the Defer Layout Update
button on the right side of the page. When placing fields in the
filter, column and row areas, the layout will
not update until you click the Update button.
Q: In the Organization Performance module, what do the red,
yellow and green colors signify?
A: Each color indicates different levels of performance,
according to percentile-based categorizations. Green
indicates that performance is at or above the “leading
performer” category, corresponding to the 75th
percentile or better. Yellow indicates the “standard performer”
category, corresponding to performance
between the 25th and 75th percentile. Red indicates performance
at or below the “lagging performer”
category, corresponding to performance below the 25th
percentile.
Q: What is “Sg2 Expert Analysis”? How do I use this feature?
A: Sg2 Expert Analysis is a feature available in the National
Demand Forecast module. When you see the Sg2
Expert Analysis box, you can click on the bars in the graph to
the left to read Sg2 experts’ rationale behind
the forecast at the service line, CARE Family and procedure
levels.
All Sg2 Expert Analyses are available in PDF format in the
Analytics Support section of the online Learning
Center.
Q: How do I export the entire national forecast in the National
Demand Forecast module?
A: 1. Click on the CARE Group or MS-DRG report tabs.
2. Click on the View Data table button.
3. Click on the XLS Download Full Forecast link.
-
Sg2 Analytics: 2013 Frequently Asked Questions
6 Confidential and Proprietary © 2013 Sg2 | www.sg2.com
Q: Can I share customized forecasts from the IoC Express module
with other colleagues?
A: Yes. On the Profile page in the IoC Express module, select
“Share this forecast” under the Share with your
colleagues section. You will be asked to select an organization
and identify eligible colleagues.
-
Sg2 Analytics: 2013 Frequently Asked Questions
7 Confidential and Proprietary © 2013 Sg2 | www.sg2.com
Q: Why am I seeing this message?
A: The Sg2 Web site is optimized to work in the following Web
browser versions. Please reference the links
below to update your preferred browser or contact your
information technology department for further
assistance.
Internet Explorer 8
http://windows.microsoft.com/en-US/internet-explorer/downloads/ie-8
Internet Explorer 7
http://www.microsoft.com/windows/Internet-explorer/default.aspx
Firefox 3+ http://www.mozilla.com/firefox/
Safari 3+ http://www.apple.com/safari/download/
Google Chrome http://www.google.com/chrome
Drill-Down Analysis
Q: Where can I use the Defer Layout Update option in the
Drill-Down Analysis?
A: The Defer Layout Update option works when using the design
box on the right. When this option is
selected, you must click the Update button to refresh your
view.
Q: How are cumulative percent changes calculated?
A: In the Market Demand Forecast and Organization Demand
Forecast modules, percent changes are
between a given year and the base year.
-
Sg2 Analytics: 2013 Frequently Asked Questions
8 Confidential and Proprietary © 2013 Sg2 | www.sg2.com
Q: How do I filter results?
A: To filter data, select the button in the Viewing Pane header
above the specific Row Area category. Next,
use the drop-down menu to select the dimensions you want to
include/exclude in your analysis. The
button outline will appear darker for all filtered
dimensions.
Q: How do I sort by dimensions and measures?
A: To sort by dimensions, right click on the name of the
dimension