Embed Size (px)
Citation preview

DIMORFISMO SESSUALE DELLE
PATOLOGIA DEL SISTEMA NERVOSO:
POSSIBILI TARGETS TERAPEUTICI


GENDER DIFFERENCES IN ALZHEIMER’S
DISEASE
Epidemiological studies support a higher prevalence and incidence in women
(Moreira et al., 2008)
At variance, to what observed in young male and old females, mitochondria of
young females are protected against the increased in peroxide production caused
by β-amyloid (Lloret et al., 2008)
Higher plaque load is observed in female than in male (Callahan et al., 2001)
In experimental models aged female animals are more sensitive to kainic acid.
Thus, females show increased hippocampal neurodegeneration, enahanced
astrocyte proliferation and higher levels of BDNF in hippocampus (Zhang et al.,
2008)
GENDER DIFFERENCES IN PARKINSON’S
DISEASE
The incidence is greater in men than in women (Benito-Leon et al., 2003; de Lau
et al., 2004; Van Den Eeden et al., 2003; Wooten et al., 2004).
Course and symptoms as well as pharmacological treatment are also gender
different (Fernandez et al., 2000; Haaxma et al., 2007; Homann et al., 2003;
Martinelli et al., 2003; Zappia et al., 2005).
Women tend to be older than men at symptom onset and present more often than
men a tremor dominant form of disease, which in turn is associated with a slower
disease progression. Moreover, at onset of the disease they have higher levels of
striatal dopamine binding than men (Haaxma et al., 2007).

GENDER DIFFERENCES IN EXPERIMENTAL
MODEL OF PARKINSON’S DISEASE
In mice model, male animals show a stronger depletion of dopamine
after intoxication with 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine
(MPTP) than female animals (Czlonkowska et al., 2006).
Inflammatory processes could have a role in this gender dependent
event. Namely, different gene expression profiles of pro-inflammatory
molecules, such as TNF , IL-6, IFN , IL-1 , occur in male and
female animals after MPTP injection (Czlonkowska et al., 2006).

SEX DIFFERENCES IN MULTIPLE SCLEROSIS
Multiple Sclerosis is more frequent in female than in male (ratio 2:1)(Noonan et al., 2002; Houzen et al., 2003; Orton et al., 2006; Schwendimann and Alekseeva, 2007 )
The disease mainly affects young and postpubertal women and most
commonly causes relapsing-remitting-type symptomatology.
Therefore, women showing a benign course (Hawkins and McDonnell, 1999)
Men have a worse prognosis. Indeed, they are affected in older age
and develop a more severe pathology, defined as a shorter time to
reach severe disability (Confavreux et al., 2003)
SEX DIFFERENCES IN SCHIZOPHRENIA
The risk is comparable, but sex differences occur in age of onset and
in course of the disease as well as in the response to treatment (Hafner,
2003; Halbreich & Kahn, 2003; Rao and Kolsch, 2003; Riescher-Rossler & Hafner, 2000)
Men usually experience first onset between 15 and 24 years. This is
about 3-4 years earlier than in women. A second increase of the
incidence occurs only in women between 45 and 54 years.
Men show more severe negative symptoms than women.
Women react better to antipsychotic therapy than men.
Functional (FMR) and morphometric studies show sex differences.

SEX DIFFERENCES IN AUTISM
Clinical and epidemiological studies indicate that boys are affected
more frequently than girls (ratio 4:1) (Fombonne, 1999, 2003;Volkmar
et al., 1993)
Male heterozygous reeler, at variance with female, have a reduced
number of Purkinje cells (Doulazmi et al., 1999; Hadj-Sahraoui et al.,
1996; Biamonte et al., 2009)

WHAT CAUSES PERIPHERAL NEUROPATHY?
Physical injury (trauma)
Systemic diseases:Diabetes mellitus
Kidney disorders
Hormonal imbalances
Vitamin deficiences
Alcoholism
Vascular damage and blood diseases
Connective tissue disorders and chronic inflammation
Cancers and benign tumors
Repetitive stress
Toxins
Infections and autoimmune disorders
Inherited forms of peripheral neuropathy

GENDER DIFFERENCES IN DIABETIC
NEUROPATHY
Diabetic neuropathy is more frequent in men than in women(Basit A. et al., 2004; Booya F. et al, 2005)
Males develop neuropathy approximately 4 years earlier than females(Aaberg M.L. et al., 2008)
Neuropathic pain and negative sensory symptoms are more frequent in
female, whereas atrophy is more frequent in male patients(Kiziltan M.E. & Benbir G., 2008)
Motor nerve conduction abnormalities and ulnar nerve involvement is
also more frequent and severe in males(Albers J.W. et al, 1996; Kiziltan M.E. et al., 2007; Kiziltan M.E. & Benbir G., 2008)

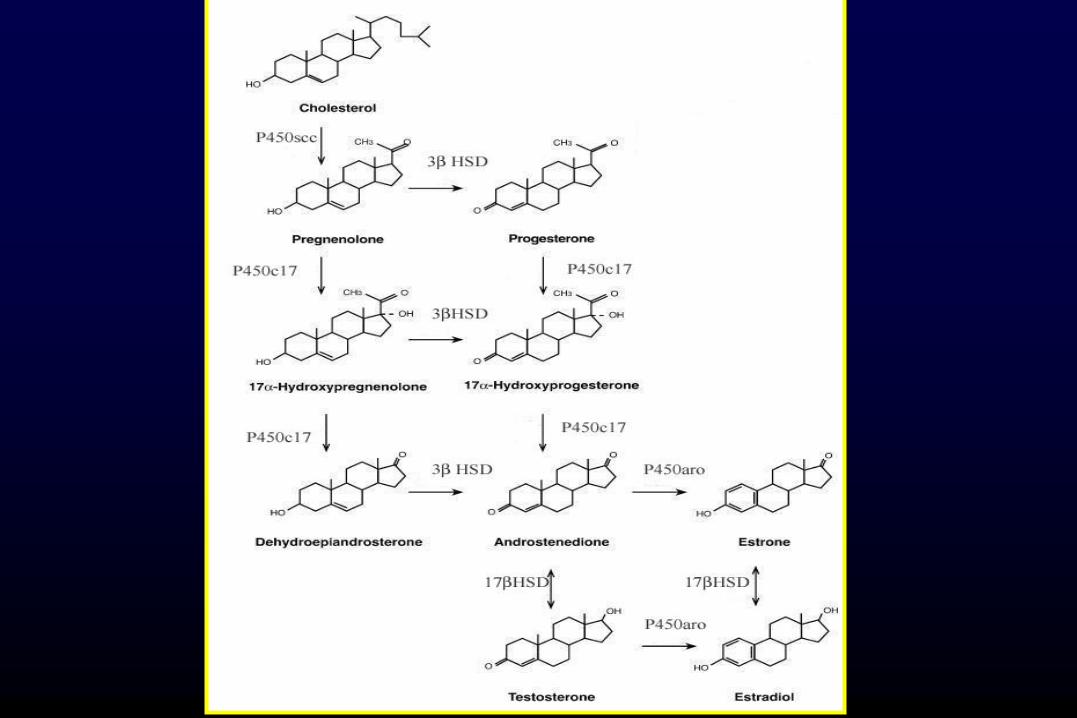
STEROID HORMONES
NEUROSTEROIDS
ENDOCRINE
PARACRINE AUTOCRINE

O
OH
O
HOH
O
O
5 -reductase
3 -hydroxysteroid-dehydrogenase
Progesterone
5 -pregnan-3,20-dione
(dihydroprogesterone, DHP)
5 -pregnan-3 -ol-20-one
(tetrahydroprogesterone, THP)

OH
HO H
O
OH
OH
OH
5 -reductase
3 -hydroxysteroid-dehydrogenase
Testosterone
5 -androstan-17 -ol-3-one
(dihydrotestosterone, DHT)
5 -androstan-3 ,17 -diol
(3 -diol)

CLASSICAL AND NON CLASSICAL
STEROID RECEPTORS
PROGESTERONE RECEPTOR
ANDROGEN RECEPTOR
ESTROGEN RECEPTOR
GLUCOCORTICOID RECEPTOR
MINERALOCORTICOID RECEPTOR
GABA-A RECEPTOR
GABA-B RECEPTOR
NMDA RECEPTOR
AMPA RECEPTOR
KAINATE RECEPTOR
SIGMA 1 RECEPTOR

Are gender differences in
neurodegenerative disorders
related to neuroactive
steroids?

In female rats, the fluctuation in hormonal levels during
estrous cycle affects the response of the brain to pathological
insults. For instance, neurotxic effect of kainic acid on
hippocampus of intact females rats is different depending on
the day of the estrous cycle on wich the neurotoxin is injected
(azcoitia et al. 1999).
Morning of estrous (i.e. 1 days after the peak of
estrogen)………No neuronal loss
Morning of proestrus (when peak of estrogen occurs) ……….
Loss of neurons
Ovariectomized rats …………..Loss of neurons

In premenopausal women parkinsonian symptoms have been
reported to worsen at the onset of menses, when estrogen
levels are low (Quinn & Marsden 1986).
Postmenopausally hormone replacement therapy has been
reported to improve symptoms (Saunders-Pullman et al.
1999), with a worsening on withdrawal of treatment (Sandyk
1989).
Women who underwent oophorectomy before the onset of
menopause had increased risk of parkinsonism compared
with referent women and he risk increased with younger age
at oophorectomy (Rocca et al, 2008).

MULTIPLE SCLEROSIS
(EXPERIMENTAL AUTOIMMUNE ENCEPHALOMYELITIS)
SEX STEROIDS
MENSTRUAL CYCLE PREGNANCY MENOPAUSE

ASSESSMENT OF NEUROACTIVE STEROIDS BY LIQUID
CHROMATOGRAPHY –TANDEM MASS SPECTROMETRY

SPINAL CORD CEREBELLUM CORTEX SCIATIC NERVE PLASMA
PREG
PROG
DHP
THP
Isopregnanolone
T
DHT
3α-diol
DHEA
17β-estradiol
= = =
=
= =
=
= = =
u.d.l
u.d.l
= =

imm
uniz
atio
n
scor
e
0
1
2
3
4
5
relapseacute remission
Dark-Agouti rat

sco
re/s
ectio
n
0
10
20
30
40
50
60
*
MEAE FEAE
(6)
(6)

PREGNENOLONE
PROGESTERONE
DIHYDROPROGESTERONE
TETRAHYDROPROGESTERONE
ISOPREGNANOLONE
TESTOSTERONE
DIHYDROTESTOSTERONE
3ALPHA-DIOL
EFFECT OF EAE ON NEUROACTIVE STEROID LEVELS
SPINAL CORD PLASMA

DHP
THP
ISOPREGNANOLONE
PROG receptor
GABA-A receptor

DHT 3ALPHA-DIOL
AR GABA-A receptor ER BETA

PREGNENOLONE
PROGESTERONE
DIHYDROPROGESTERONE
TETRAHYDROPROGESTERONE
ISOPREGNANOLONE
TESTOSTERONE
DIHYDROTESTOSTERONE
3ALPHA-DIOL
EFFECT OF DIABETES ON NEUROACTIVE STEROID LEVELS
SCIATIC NERVE

pg
/mg
tiss
ue
M MF F
WT HZ
pg
/mg
tiss
ue
0
10
20
30
40
50
60
70
0
5
10
15
20
25# #
M MF F
WT HZ
pg
/mg
tiss
ue
0
10
20
30
40
50
60
70
M MF F
WT HZ
pg
/mg
tiss
ue
#§
M MF F
WT HZ
0
25
50
pg
/mg
tiss
ue
0
pg
/mg
tiss
ue
M MF F
WT HZ
M MF F
WT HZ
§ #
10
20
30
40
50
60
70
§§
0
1
2
3
4
5
6
7
WT HZ WT HZ
pg
/mg
tiss
ue
0
1
2
3
4
5
6
7
M MF F
§§
pg
/mg
tiss
ue
§§
M MF F0
1
2
3
4
5
6
7
< LOQ < LOQ < LOQ
< LOQ< LOQ < LOQ < LOQ < LOQ
PREG PROG
DHP 3α, 5α THP
3β, 5α THP T
DHT 3α-diol
LOQ, limit of quantification
# P < 0.01
§ P < 0.001

pg
/mg
tiss
ue
+/+ +/+rl/+ rl/+
P5 P15
0.0
0.1
0.2
0.3
0.4
0.5
0.6
* **
0
5
10
15
pg
/mg
tiss
ue
+/+ +/+rl/+ rl/+P5 P15
****
0.00
0.05
0.10
0.15
0.20
0.25
+/+ +/+rl/+ rl/+P5 P15
pg
/mg
tiss
ue
** ***
0.1
0.2
0.3
0.4
pg
/mg
tiss
ue
+/+ +/+rl/+ rl/+P5 P15
*
< LOQ < LOQ
LEVELS OF NEUROACTIVE STEROIDS IN
MALE CEREBELLUM
TESTOSTERONE DHT
3α-DIOL 17β-DIOL

LEVELS OF NEUROACTIVE STEROIDS IN
FEMALE CEREBELLUM
0.0
0.2
0.4
pg
/mg
tiss
ue
+/+ +/+rl/+ rl/+P5 P15
0
4
8
+/+ +/+rl/+ rl/+P5 P15
pg
/mg
tiss
ue
< LOQ
12
pg
/mg
tiss
ue
+/+ +/+rl/+ rl/+P5 P15
0.0
0.2
0.4*
pg
/mg
tiss
ue
+/+ +/+rl/+ rl/+P5 P15
0.08
0.04
0.00
TESTOSTERONE DHT
3α-DIOL 17β-DIOL

TESTOSTERONE
DHT 17β-Estradiol

PREGNENOLONE
CHOLESTEROL
Inner
mitochondrial
membrane
VDAC
PBROuter
mitochondrial
membrane
ADC
DBS
P450scc: cytochrome P450side-chain cleavage.
VDAC: voltage-dependent anion channel
BDS: benzodiazepine-binding site
ADC: adenine nucleotide carrier
A WORKING MODEL OF PBR FUNCTION
CHOLESTEROL
PREGNENOLONE
This step of trasporting
cholesterol from cytoplasm
into the inner mitochondrial
membrane is the primary point
of control in the acute
stimulation of steroidogenesis
Steroid synthesis

CONCLUSIONS
-The levels of neuroactive steroids present in male and female CNS
are different in control animals and differently affected by pathology.
-These modifications may affect the result of therapy based on
neuroactive steroids and may suggest new therapeutic strategies.
-The findings here reported may represent an important background
for new sex oriented therapy neuroactive steroid-based for
neurodegenerative disorders.