Embed Size (px)
Citation preview

ABSTRACT: Examination of tactile directional sensibility, i.e., the ability totell the direction of an object’s motion across the skin, has been recom-mended by several authors for examination of patients with somatosensorydisorders. Recent findings about the physiological mechanisms underlyingdirectional sensibility suggested possibilities to further improve the test. Inthe present investigation a test was constructed that allowed a semiquanti-fication of the directional sensibility of six body areas within 20 min. Normalvalues were obtained by testing healthy subjects (n = 40), and the normalvalues were compared to those obtained in a group of patients with tactilesymptoms (n = 20). Ten of the patients had abnormal sensory conduction inone or several nerves, and they also had abnormal directional sensibility.Hence, examination of directional sensibility, according to the present pro-tocol, provides a semiquantitative test that appears to be as sensitive aselectrophysiological measurement of conduction in detecting dysfunction in tac-tile nerves. © 1997 John Wiley & Sons, Inc. Muscle Nerve 20: 1414–1421, 1997Key words: touch; directional sensibility; nerve; neuropathy; conduction
DIRECTIONAL SENSIBILITY FORQUANTIFICATION OFTACTILE DYSFUNCTION
HÅKAN OLAUSSON, MD, PhD, 1* ULF NORRSELL, MD, PhD, 1,2
KARIN GOTHNER,1 and B. GUNNAR WALLIN, MD, PhD 3
1 Department of Physiology, Goteborg University, Medicinaregatan 11, S-413 90Goteborg, Sweden2 Division of Neurology, Department of Clinical Neuroscience, Goteborg University,Goteborg, Sweden3 Division of Clinical Neurophysiology, Department of Clinical Neuroscience,Goteborg University, Goteborg, Sweden
Received 29 January 1997; accepted 31 May 1997
During the past 50 years several authors (see below)have reported that the ability to tell the direction ofan object’s movement across the skin provides a use-ful test of disturbances in the tactile sense. Recentfindings concerning the physiological mechanismsunderlying tactile directional sensibility suggest thatthe test may be further improved.
PHYSIOLOGICAL MECHANISMS
Normally, a subject can tell the direction of an ob-ject’s motion across the skin after a movement ofonly a few centimeters. As originally noted morethan 100 years ago,2,4,5,26 tests for directional sensi-bility give results indicating higher cutaneous spatialresolution than those using static stimuli, e.g., two-point discrimination or localization of point stimu-
lation. In psychophysical experiments, the depen-dence of directional sensibility on stimulus load,distance, and speed has been carefully ana-lyzed.1,10,11,16 Furthermore, responses of single hu-man mechanoafferents,13,18,37,45 and neurons in theprimary somatosensory cortex of monkeys,23,28,52
have been recorded when using similar stimuli as inthe above-described psychophysical experiments.
Directional sensibility is likely to depend on theparallel processing of two different types of sensoryinformation, i.e., spatial information that varies withtime, and information about patterns of skin stretchinduced by friction.25,34,38 Spatially well-defined in-formation may be signaled by the slowly adaptingtype I (Merkel), field, and hair afferents. Informa-tion about patterns of skin stretch may be signaled bya population of slowly adapting type II afferents.37,45
Factors that influence the intensity of the responsesof single afferents, or the number of activated affer-ents, strongly influence directional sensibility. Thus,adequate perception depends on the length of themovement, the stimulated area, the stimulation load,
*Correspondence to: Dr. Håkan OlaussonContract grant sponsor: Swedish Medical Research Council; Contractgrant number: 2857; Contract grant sponsors: Royal Swedish Academy ofSciences; Goteborg Medical Society
CCC 0148-639X/97/111414-08© 1997 John Wiley & Sons, Inc.
1414 Tactile Directional Sensibility MUSCLE & NERVE November 1997

the coefficient of friction between the moving objectand the skin, and the degree of static skin tensiondetermined by the position of the subject.34–36,38
CLINICAL APPLICATIONS
Tests for directional sensibility have also been usedclinically for examining patients with tactile distur-bances of different genesis. In 1936, Foerster21 de-scribed patients with dorsal column lesions whocould perceive light touch but not the direction ofan object’s movement across the skin. Subsequentstudies have confirmed that patients with dorsal col-umn lesions usually have only a slight disturbance inthe ability to perceive tactile and pressure stimuli,whereas they have a severely impaired directionalsensibility.31,48 Based on a study of patients with spi-nal cord lesions who had abnormal directional sen-sibility but normal perceptions of light touch, pain,temperature, vibration, and joint position, Hankeyand Edis27 recommended that directional sensibilitytests should be incorporated in the routine clinicalsensory examination of such patients.
Sperry et al.42 used the directional sensibility testfor examining patients with ‘‘split-brain’’ symptomsafter cerebral commisurotomy. The patients couldverbally report the presence or absence of a tactilestimulus on the left hand but could not tell the di-rection of a line drawn on the palm of the samehand. Norrsell33 examined another group of pa-tients with ‘‘split-brain’’ symptoms and reported dis-turbed directional sensibility for verbal readouts onthe patients’ entire left body half, whereas thermaland touch sensibility were normal on both bodyhalves.
In a study of over 600 patients with a spectrum ofclinical disorders of the central and peripheral ner-vous systems, Bender et al.6 compared the test resultsof 14 different tests of somatosensory function in-cluding, e.g., directional sensibility, graphestesia,point localization, two-point discrimination, and vi-bration detection. Evaluation of directional sensibil-ity, and graphesthesia were found to be the clinicallymost useful tests, and the authors recommendedthem for routine sensory examinations. Since theresults of these two tests usually were similar, theysuggested that directional sensibility provides the es-sential input in graphesthesia. The directional testshould perhaps be preferred, since the methodologi-cal difficulties with graphesthesia (e.g., in what di-rection the symbol should be oriented, in what orderthe different parts of the symbol should be written,or the familiarity of the symbol) do not arise with thedirectional sensibility test.6
Tests for directional sensibility have also been
found to be more sensitive than light touch detec-tion, two-point discrimination, and thermal tests fordetecting sensory disturbances due to surgical inju-ries in the perioral region.3,14,15,17,19,22,24,30,32,49,53
REASONS TO IMPROVE THE TEST
Even if the directional sensibility tests describedabove were successful in detecting sensory distur-bances, there are several reasons why the test couldbe further improved. Except for the perioral region,no attempt has been made to quantify the direc-tional sensibility, and clinically useful normal valueshave never been reported. Some investigators haveused the contralateral body area as a control thatrestricts the test to unilateral disorders,33,48 or usedadjacent skin regions,49 which might be misleading,since the sensibility varies between different bodyareas.16,39,51 Others have used arbitrarily definednormal values.6,27 Moreover, the importance of skinstretch for directional sensibility has not been con-sidered, i.e., the force of friction caused by the stimu-lator, and the degree of static skin tension deter-mined by the position of the subject, have not beencontrolled.6,27,33,48
In the present investigation a test for directionalsensibility was constructed that took into account theimportance of friction, the degree of static skin ten-sion determined by the subject’s position, the stimu-lation distance, and the stimulation area. Using thistest normal values for different body parts were de-termined for healthy subjects of different ages. Tocheck the usefulness of the test, the individual resultsfor patients suspected to suffer from sensory neurop-athy were compared to the normal values. The pa-tient’s results in the directional sensibility test werealso compared to his/her results in a standard elec-trophysiological sensory conduction test. It will bedemonstrated that examination of directional sensi-bility, according to the present protocol, provides asemiquantitative test that is easy to perform, and ap-pears to be as sensitive as electrophysiological mea-surements of conduction in detecting dysfunction intactile nerves.
MATERIALS AND METHODS
The study included 40 healthy subjects and 20 pa-tients. Consent was obtained according to the Dec-laration of Helsinki. All tests for a single subject/patient were made on the same day, and in 10 of thehealthy subjects the directional sensibility test wasrepeated after 3–6 months in order to check repro-ducibility.
Normal Subjects. Three groups were examined:(A) 10 healthy subjects (5 women and 5 men) with
Tactile Directional Sensibility MUSCLE & NERVE November 1997 1415

a median age of 25 years (range 22–30) recruitedamong students at the local medical and dentalschools; (B) 10 healthy subjects (5 women and5 men) with a median age of 56 years (range 50–60), recruited among the full-time employees atthe Department of Physiology; (C) 20 subjects (10women and 10 men) born in 1922. They wererecruited among a group of subjects who had been
recently investigated within the framework of thegerontological and geriatric population studies inGoteborg.40,43 The investigation of these last subjectslasted for 1 day, and included a general somatic ex-amination with a questionnaire of 69–157 questions,urine and blood sampling and examinations, elec-trocardiogram, chest X ray, mobility estimation,hearing ability examination, and ophthalmiatric ex-amination. The inclusion criteria for the presentstudy were absence of neurological diseases, somato-sensory complaints, and/or diseases associated withneuropathy.
Patients. Two consecutive series of 20 patients (9women and 11 men), aged 32–71 (median 52) years,were examined. They had been referred to the labo-ratory of clinical neurophysiology at Sahlgren’s Hos-pital, Goteborg, Sweden, with the specific question‘‘sensory neuropathy?’’
Directional Sensibility Tests. The healthy subjectswere examined by HO and KG. There were no sig-nificant differences in the results related to the ex-aminer. All patients were examined by HO.
All subjects/patients were sitting in a standardposition in a comfortable armchair, with obtuseangles at the elbow, knee, and ankle joints. The sub-jects could not see the skin area that was examined.The stimulations were made halfway between the el-bow and the wrist on the radial side of the forearm,halfway between the hip and the knee on the ventralside of the thigh, and halfway between the ankle andthe toes on the dorsum of the foot. These areas areinnervated by the lateral antebrachial cutaneousnerve (arm), the anterior cutaneous branches of thefemoral nerve (thigh), and the superficial peronealnerve (foot). The stimulated areas were shaved witha razor before the experiment, and marked alongthe longitudinal axes with ink dots. The stimulationswere distributed randomly over the marked surface.Neither normal subjects nor patients had any visibleskin damage in the examined areas. All examina-tions were made bilaterally except in 1 patient whoseleft arm and thigh were not examined.
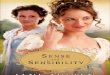
Stimulus. The stimulator (Fig. 1) was handheldand the contact probe consisted of a half-cylinder(diameter 4 mm, length 15 mm) covered by a finewoven fabric (Leukoplast, Hamburg, Germany). Thehalf-cylinder was attached at right angles to a metalrod with a smooth surface that could slide with mini-mal friction between bushings situated at the upperand lower ends of a pencillike outer casing. The
FIGURE 1. Handheld stimulator for examination of directionalsensibility. The rod (a) slides easily between bushings (b). Thecontact surface consists of a half-cylinder (c) covered by a finewoven fabric. The rod is asymmetrical to prevent rotation. Thestimulator is held perpendicular to the skin, and the vertical loadof the half-cylinder to the skin equals the weight of the metal rodand the half-cylinder. The vertical load is changed by addingweights to the metal rod.
1416 Tactile Directional Sensibility MUSCLE & NERVE November 1997

stimulator was held approximately perpendicular tothe skin. Hence, the vertical load of the half-cylinderon the skin was approximately equal to the weight ofthe half-cylinder and the metal rod, and remainedconstant when the outer casing was moved up ordown for several millimeters. The load could be setto either 8 or 16 g by adding weights to the rodinside the casing. The stimulator was moved with aspeed of approximately 10 mm/s.
Procedure. The examination was made with aforced two-choice procedure, and the order of theruns was right arm, right thigh, right foot, left foot,left thigh, and left arm. The subject/patient was in-structed that the probe would move in either distalor proximal direction and that the perceived direc-tion of motion should be reported, after removal ofthe stimulus. The subject/patient was free to use per-sonal expressions to describe the directions. Equalnumbers of trials in each direction were maintainedas far as possible. In preliminary experiments it wasfound that healthy young subjects were, in mostruns, able to tell the direction of motion for stimu-lation distances ù 10 mm using a stimulus load of 8g on the arms and 16 g on the thighs and feet. Pre-liminary experiments had also demonstrated a linearrelationship between the logarithms of the stimula-tion distances and correct responses, for all testedareas. Based on this knowledge the stimulation dis-tances in the experiments reported in this articlewere selected from a logarithmic series with a short-est distance of 10 mm (= 101), followed by 18 mm (=101.25) and 56 mm (= 10 1.75). The vertical load wasalways 8 g on the arms and 16 g on the thighs andfeet. The runs always started with a stimulation dis-tance of 18 mm, and the stimulations were contin-ued at this distance for 11 trials or less, until thesubject/patient had made either nine correct orthree wrong answers. If the subject/patient hadmade nine correct answers the run was continued ata 10-mm distance for 11 trials, and if he/she hadmade three wrong answers the run was continued ata 56-mm distance for 11 trials. The shortest distanceat which the subject/patient had ù 9 correct answerswas considered as an estimate of the directional sen-sibility. The probability of obtaining ù 9 correct an-swers out of 11 by chance is < 5% (binomial distri-bution). If the subject/patient had ù 3 wronganswers at the 56-mm distance the directional sensi-bility was denoted as > 56 mm. Thus, for each testedbody part the subject/patient obtained one of thefollowing values: 10 mm, 18 mm, 56 mm, or > 56mm. The different stimulation distances weremarked with ink on the skin. The examination pro-
tocol was governed by a computer, and a completeinvestigation lasted for about 20 min.
Reproducibility. For 10 of the 72-year-old normalsubjects, the directional sensibility test was repeatedafter 3–6 months. Thirty-six of the results did notchange, 9 improved, and 15 became poorer.
Sensory Conduction Tests. Sensory conductionwas studied only in the patients. Skin temperaturewas measured on the dorsal side of the hand andfoot and if it was < 30°C the extremity was warmed.Sensory conduction velocities were determined anti-dromically in n. suralis and/or n. radialis superficia-lis. Sensory latencies, from the base of the digits tothe wrist, were determined in the median and ulnarnerves. Surface electrodes were used for stimulationand recording. Determinations were usually madebilaterally, which means that a maximum number ofeight nerves were examined for sensory conductionin each patient (cf. Table 1). Deviations > 2 SD fromlocally determined normal values were considered tobe pathological.
RESULTS
Normal Subjects. The directional sensibility in dif-ferent skin areas for the three normal groups are
Table 1. Summary of test results in patients.
PatientAge
(years)Directionalsensibility
Sensoryconduction
No. of nervesexamined for
sensoryconduction
HN 44 +++++ + 8UW 44 ++++ ++++++ 6HO 44 ++++ ++++++++ 8JO 53 ++++ ++++ 8GN 55 +++ ++++++++ 8DS 69 +++ +++++ 5VA 54 ++ ++++ 8RF 32 ++* ++++ 4ÅN 64 ++ + 6SE 71 + +++ 8CA 32 ++++++ − 8IS 66 +++++ − 6IG 51 + − 6AJ 36 + − 6AC 70 − − 8GS 61 − − 6BJ 51 − − 8HB 44 − − 6CH 40 − − 6AW 38 − − 6
+, abnormal test result in one skin area or nerve; −, normal test results.Directional sensibility was regularly examined in six different skin areas.*Only four different skin areas examined.
Tactile Directional Sensibility MUSCLE & NERVE November 1997 1417

illustrated in Figure 2A–C. There were neither sexdifferences nor side asymmetries in any group, sothe results from males and females and from theright and left body halves were pooled. The resultswere best in the 22–30-year-old group (A), slightlypoorer in the 50–60-year-old group (B), and poorestin the 72-year-old group (C). The two 56-mm valuesamong the 50–60-year-old subjects (Fig. 2B) werefound in the two oldest of the group, both 60 yearsof age.
Patients. The results of the directional sensibilitytest in the patients were poorer than in any of thenormal groups (Fig. 2D). In 18 skin areas the pa-tients were unable to report the direction of motioneven for the longest stimulation distance that wasused.
For each age group and skin area a directionalsensibility ø 95th percentile, of the distributionsshown in Figure 2A–C, was considered normal(Table 2). The directional sensibilities for the pa-tients were compared to these limits for normality ofthe patient’s age group. If a patient’s age did not fitin any of the reference groups, the nearest ‘‘older’’group was used for comparison, i.e., the values for
the 61-year-old patient were compared to the limitsobtained for the 72-year-old group. Using this defi-nition, 43 abnormal and 75 normal values werefound among the patients. Eleven abnormal valueswere on the arms, 11 on the thighs, and 21 on thefeet. Fourteen patients had one to six abnormal val-ues, with a median of three. The remaining 6 pa-tients had normal values in all areas tested.
Comparison with Sensory Conduction Tests. Tenpatients had lowered conduction in one or more ofthe examined tactile nerves, and all of those patientsalso had abnormal directional sensibility in at leastone skin area (Table 1). In addition, 4 patients hadsensory disturbances according to the directional
FIGURE 2. Directional sensibility for different body parts in different groups: (A) healthy subjects 22–30 years old; (B) healthy subjects50–60 years old; (C) healthy subjects 72 years old; (D) patients 32–71 years old. The patients had been referred for neurophysiologicalexaminations with the specific question ‘‘sensory neuropathy?’’ The y-axes show the number of observations, and the x-axes show thedirectional sensibility expressed as the shortest distance needed for reliable directional discrimination.
Table 2. Normal values for directional sensibility.
22–30 years, old 50–60 years, old 72 years, old
Arms ø 10 mm ø 10 mm ø 18 mmThighs ø 18 mm ø 18 mm ø 56 mmFeet ø 10 mm ø 18 mm ø 56 mm
Values ø 95th percentile are shown for different age groups and skinareas.
1418 Tactile Directional Sensibility MUSCLE & NERVE November 1997

test but normal results in the sensory conductiontests (cf. Discussion). Six patients had normal resultsfor both types of tests.
DISCUSSION
With a psychophysical test it is possible to detectdamage along certain pathways, and it should beadvantageous to use a test that is based on a sensoryfunction with extensively investigated pathways. Di-rectional sensibility requires highly coordinated in-formation from a population of mechanoafferents(see above), and intact dorsal columns,47,48 involvesthe cerebrum since it requires intact cerebral com-missures,33,42 and is likely to depend on activity inthe primary somatosensory cortex.23,28,50,52
Methodological Considerations. The shortest dis-tance at which a subject/patient could report thedirection of motion reliably was considered as anestimate of the directional sensibility for the testedskin area. The friction between the stimulator andthe skin influences the activation of stretch recep-tors. Therefore, the vertical load on the stimulatorand the part of the stimulator making contact withthe skin was the same for all subjects/patients, i.e.,there was a constant force of friction. Even though ahigher load was used on the thighs and feet (16g)than on the arms (8 g), the average performance wasbetter in the arms (Fig. 2). This may be explained bydifferences in mechanical properties of the skin,9
differences in the distribution of peripheral recep-tors,45,46 or differences in the central processing ofafferent information from the different skin areas.12
Directional sensibility is also influenced by differ-ences in static skin tension caused by different jointangles.38 Therefore, care was taken that the sub-jects/patients were sitting in similar positions.
Directional sensibility above the 95th percentilefor healthy subjects was considered abnormal. Thislimit was chosen for conventional reasons.12
When the test for directional sensibility was re-peated a second time for the 72-year-old subjects, themajority of results remained unchanged, some im-proved, and some became poorer. Similar variationshave been reported for other tests involving vibra-tion, tactile stimuli, and thermal stimuli.20 Ninety-fifth percentile values were calculated also from theresults of the second examination of the oldest nor-mal group. The use of these alternative values didnot change the classification of patients as normal orabnormal.
Normal Subjects. The poorest directional sensibil-ity was found in the oldest group. This is perhaps not
surprising, since age-related changes (e.g., demyelin-ation and remyelination as well as axonal degenera-tion and regeneration) have been reported for hu-man myelinated and unmyelinated peripheralnerves.8,44 The numbers of peripheral receptors de-crease with increasing age as well.7,8 Indeed, age-related degeneration of mechanoreceptors takesplace at higher rate than degeneration of the nervefiber.41 The directional sensibility was poorest in thefeet of the elderly, which suggests that decreasingsensibility due to ageing follows the same pattern asneuropathy. However, the poorer directional sensi-bility among the elderly may also be explained byage-related changes in the mechanical properties ofthe skin.9,29
Patients. To check the usefulness of the normalvalues, the directional sensibility test was applied to agroup of patients suffering from tactile disturbancesindicative of sensory neuropathy. The patients’ re-sults from the directional test were compared to his/her results from electrophysiological measurementsof conduction in sensory nerves. This comparisonwas considered most appropriate, since electrophysi-ological tests are likely to be most objective. In addi-tion, several authors have already compared tests ofdirectional sensibility with other psychophysical sen-sory tests (see above). For instance, Bender et al.6
reported that their test of directional sensibility wasmore sensitive than tests of point localization or vi-bration detection in detecting peripheral neuropa-thy.
All patients were asked for their opinion of thedirectional sensibility test, and they regarded it as areasonable task that was easy to understand. Alsopatients with directional sensibility ù 56 mm couldperceive the movement of the stimulator, althoughthey were not able to tell the direction of the move-ment. Similar findings have been reported byBender et al.6 and Wall and Noordenbos.48
All patients who had abnormal conduction inone or several sensory nerves also had abnormal di-rectional sensibility. Thus, the directional test seemsto be as sensitive as electrophysiological measure-ments of conduction in detecting dysfunction in tac-tile nerves. An explanation may be that optimal di-rectional sensibility demands orderly presentedinformation from the different afferents that are in-volved, i.e., about the successive activation of adja-cent receptive fields and the pattern of activation ofstretch receptors (see above).
Two patients (HN and ÅN, Table 1) had abnor-mal conduction in only one of the tested nerves, but
Tactile Directional Sensibility MUSCLE & NERVE November 1997 1419

these patients had borderline values for several othernerves as well.
Four patients had abnormal directional sensibil-ity despite normal sensory conduction. Patient CA(Table 1), who had abnormal directional sensibilityin all examined skin areas, was later successfullytreated for sarcoidosis. Her poor directional sensibil-ity was explained as affection of the central nervoussystem by sarcoidosis. Patient IS (Table 1) had ab-normal directional sensibility in five skin areas. Shealso had allodynia to heat stimuli, and increased de-tection thresholds of warmth and cold, and is sus-pected to have a lesion of the central nervous system.
In summary, examination of tactile directionalsensibility provides a semiquantitative test that is easyto perform, and appears to be sensitive in detectingtactile disturbances along relatively well-definedpathways. Our findings support previous authors’suggestion that the test may have the potential forbecoming a clinical routine method. A comparisonbetween directional sensibility and several other testsof somatosensory function for patients with diabeticneuropathy is under way.
The authors thank Dr. Michael Matousek and the Department ofGeriatric Medicine, Vasa Hospital, Goteborg, for promoting con-tacts with the 72-year-old subjects. Dr. Kelvin Edward Jones kindlyread and advised on the text.
REFERENCES
1. Ahringsmann H, Buch A: Ueber die Wahrnehmung von Be-wegten Reizen auf der Haut. Z Biol 1926;84:541–552.
2. Aubert H, Kammler A: Untersuchungen uber den Druck- undRaumsinn der Haut. J Moleschotts Untersuchungen Naturlehre1858;5:145–179.
3. Bailey PH, Bays RA: Evaluation of long term sensory changesfollowing mandibular augmentation procedures. J Oral Max-illofac Surg 1984;42:722–727.
4. Basler A: Uber die Grosse der mit der Haut eben wahrnem-baren Bewegungen. Pflugers Arch Physiol 1910;132:494–510.
5. Basler A: Uber das Erkennen von Bewegungen mittelst desTastgefuhls. Pflugers Arch Physiol 1910;136:368–401.
6. Bender MB, Stacy C, Cohen J: Agraphesthesia. A disorder ofdirectional cutaneous kinesthesia or a disorientation in cuta-neous space. J Neurol Sci 1982;53:531–555.
7. Bolton CF, Winkelmann RK, Dyck PJ: A quantitative study ofMeissner’s corpuscles in man. Neurology 1966;16:1–9.
8. Caruso G, Nilsson J, Crisci C, Nolano M, Massini R, Lullo F:Sensory nerve findings by tactile stimulation of median andulnar nerves in healthy subjects of different ages. Electroen-cephalogr Clin Neurophysiol 1993;89:392–398.
9. Cua AB, Wilhelm K-P, Maibach HI: Elastic properties of hu-man skin: relation to age, sex, and anatomical region. ArchDermatol Res 1990;282:283–288.
10. de Cillis O: Absolute thresholds for the perception of tactualmovement. Arch Psychol 1944;41:1–52.
11. Dreyer DA, Hollins M, Whitsel BL: Factors influencing cuta-neous directional sensitivity. Sens Processes 1978;2:71–79.
12. Dyck PJ, Karnes J, O’Brien PC, Zimmerman IR: Detectionthresholds of cutaneous sensation in humans, in Dyck PJ,Thomas PK, Griffin JW, Low PA, Poduslo JF (eds): PeripheralNeuropathy. Philadelphia, Saunders, 1993, pp 706–728.
13. Edin BB, Essick GK, Trulsson M, Olsson KÅ: Receptor encod-ing of moving tactile stimuli in humans: I. Temporal patternof discharge of individual low-threshold mechanoreceptors. JNeurosci 1995;15:830–847.
14. Essick GK: Comprehensive clinical evaluation of perioral sen-sory function. Oral Maxillofac Surg Clin North Am 1992;4:503–526.
15. Essick GK, Afferica T, Aldershof B, Nestor J, Kelly D, WhitselB: Human perioral directional sensitivity. Exp Neurol 1988;100:506–523.
16. Essick GK, Bredehoeft KR, McLaughlin DF, Szaniszlo JA: Di-rectional sensitivity along the upper limb in humans. Somato-sens Mot Res 1991;8:13–22.
17. Essick GK, Dolan PJ, Turvey TA, Kelly DG, Whitsel BL: Effectsof trauma to the mandibular nerve on human perioral direc-tional sensitivity. Arch Oral Biol 1990;35:785–794.
18. Essick GK, Edin BB: Receptor encoding of moving tactilestimuli in humans: II. The mean response of individual low-threshold mechanoreceptors to motion across the receptivefield. J Neurosci 1995;15:848–864.
19. Essick GK, Whitsel BL, Dolan PJ, Kelly DG: Effects of traverselength on human perioral directional sensitivity. J Neurol Sci1989;93:175–190.
20. Fagius J, Wahren LK: Variability of sensory threshold deter-mination in clinical use. J Neurol Sci 1981;51:11–27.
21. Foerster O: Symptomatologie der Erkrankungen des Rucken-marks und seiner Wurzeln, in Bumke O, Foerster O (eds):Handbuch der Neurologie. Berlin, Springer, 1936, vol 5, pp1–403.
22. Frost DE, Gregg JM, Terry BC, Fonseca RJ: Mandibular inter-positional and onlay bone grafting for treatment of mandibu-lar bony deficiency in the edentulous patient. J Oral MaxillofacSurg 1982;40:353–360.
23. Gardner EP, Costanzo RM: Neuronal mechanisms underlyingdirection sensitivity of somatosensory cortical neurons inawake monkeys. J Neurophysiol 1980;43:1342–1354.
24. Ghali GE, Epker BN: Clinical neurosensory testing: practicalapplications. J Oral Maxillofac Surg 1989;47:1074–1078.
25. Gould WR, Vierck CJ, Luck MM: Cues supporting recognitionof the orientation or direction of movement of tactile stimuli,in Kenshalo DR (ed): Sensory Functions of the Skin of Humans.Proceedings of the Second International Symposium on the SkinSenses. New York, Plenum Press, 1979, pp 63–73.
26. Hall GS, Donaldson HH: Motor sensations on the skin. Mind1885;10:557–572.
27. Hankey GJ, Edis RH: The utility of testing tactile perceptionof direction of scratch as a sensitive clinical sign of posteriorcolumn dysfunction in spinal cord disorders. J Neurol Neuro-surg Psychiatry 1989;52:395–398.
28. Hyvarinen J, Poranen A: Movement-sensitive and directionand orientation-selective cutaneous receptive fields in thehand area of the post-central gyrus in monkeys. J Physiol(Lond) 1978;283:523–537.
29. Leveque JL, de Rigal J, Agache PG, Monneur C: Influence ofageing on the in vivo extensibility of human skin at a lowstress. Arch Dermatol Res 1980;269:127–135.
30. Naples RJ, Van Sickels JE, Jones DL: Long-term neurosensorydeficits associated with bilateral sagittal split osteotomy versusinverted ‘L’ osteotomy. Oral Surg Oral Med Oral Pathol 1994;77:318–321.
31. Nathan PW, Smith MC, Cook AW: Sensory effects in man oflesions of the posterior columns and of some other afferentpathways. Brain 1986;109:1003–1041.
32. Nishioka GJ, Zysset MK, Van Sickels JE: Neurosensory distur-bance with rigid fixation of the bilateral sagittal split osteot-omy. J Oral Maxillofac Surg 1987;45:20–26.
33. Norrsell U: Defects in tactile directional sensitivity after fore-brain commissurotomy in man. Nature 1973;245:41–42.
34. Norrsell U, Olausson H: Human tactile directional sensibilityand its peripheral origins. Acta Physiol Scand 1992;144:155–161.
1420 Tactile Directional Sensibility MUSCLE & NERVE November 1997

35. Norrsell U, Olausson H: Spatial cues serving the tactile direc-tional sensibility of the human forearm. J Physiol (Lond) 1994;478:533–540.
36. Olausson H: The influence of spatial summation on humantactile directional sensibility. Somatosens Mot Res 1994;11:305–310.
37. Olausson H, Kakuda N, Vallbo ÅB: Afferent messages servingtactile directional sensibility in man. Abstract for the FourthIBRO World Congress of Neuroscience, 1995; abstract no. D2.14.
38. Olausson H, Norrsell U: Observations on human tactile di-rectional sensibility. J Physiol (Lond) 1993;464:545–559.
39. Rath EM, Essick GK: Perioral somesthetic sensibility: do theskin of the lower face and the midface exhibit comparablesensitivity? J Oral Maxillofac Surg 1990;48:1181–1190.
40. Rinder L, Roupe S, Steen B, Svanborg A: Seventy-year-oldpeople in Gothenburg. A population study in an industrial-ized Swedish city: I. General presentation of the study. ActaMed Scand 1975;198:397–407.
41. Schmidt RF, Wahren IK, Hagbarth KE: Multiunit neural re-sponses to strong finger pulp vibration: I. Relationship to age.Acta Physiol Scand 1990;140:1–10.
42. Sperry RW, Gazzaniga MS, Bogen JE: Interhemispheric rela-tionships: the neocortical commissures; syndromes of hemi-sphere disconnection, in Vinken PJ, Bruyn GW (eds): Hand-book of Clinical Neurology. Amsterdam, North-Holland, 1969,vol 4, pp 273–290.
43. Steen B, Djurfeldt H: The gerontological and geriatric popu-lation studies in Gothenburg, Sweden. Z Gerontol 1993;26:163–169.
44. Thomas PK, Ochoa J, Berthold C-H, Carlstedt T, CorneliusonO: Microscopic anatomy of the peripheral nervous system, inDyck PJ, Thomas PK, Griffin JW, Low PA, Poduslo JF (eds):
Peripheral Neuropathy. Philadelphia, Saunders, 1993, vol 1, pp28–91.
45. Vallbo ÅB, Olausson H, Wessberg J, Kakuda N: Receptive fieldcharacteristics of tactile units with myelinated afferents in thehairy skin of human subjects. J Physiol (Lond) 1995;483:783–795.
46. Vallbo ÅB, Olausson H, Wessberg J, Norrsell U: A system ofunmyelinated afferents for innocuous mechanoreception inthe human skin. Brain Res 1993;628:301–304.
47. Vierck C Jr: Tactile movement detection and discriminationfollowing dorsal column lesions in monkeys. Exp Brain Res1974;20:331–346.
48. Wall PD, Noordenbos W: Sensory functions which remain inman after complete transection of dorsal columns. Brain1977;100:641–653.
49. Walter JM, Gregg JM: Analysis of postsurgical neurologic al-teration in the trigeminal nerve. J Oral Surg 1979;37:410–414.
50. Warren S, Hamalainen HA, Gardner EP: Objective classifica-tion of motion- and direction-sensitive neurons in primarysomatosensory cortex of awake monkeys. J Neurophysiol 1986;56:598–622.
51. Weinstein S: Intensive and extensive aspects of tactile sensi-tivity as a function of body part, sex, and laterality, in Ken-shalo DR (ed): The Skin Senses. Springfield, IL, Charles C.Thomas, 1968, pp 195–222.
52. Whitsel BL, Roppolo JR, Werner G: Cortical information pro-cessing of stimulus motion on primate skin. J Neurophysiol1972;35:691–717.
53. Zaytoun HS, Phillips C, Terry BC: Long-term neurosensorydeficits following transoral vertical ramus and sagittal splitosteotomies for mandibular prognathism. J Oral MaxillofacSurg 1986;44:193–196.
Tactile Directional Sensibility MUSCLE & NERVE November 1997 1421