-
Dr. Darli
-
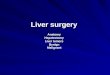
NNcvPortal & hepatic sinusoidhepatocyteGall
bladderHepatocyte injury by virus, alcohol or drugBallooning, fatty
change apoptosis or necrosis with variable distributionVascular
disease, congestion, infarctionInflammation, lymphocyte,
neutrophil, granulomaRegeneration,fibrosisCirrhosis
and?cancerexcretionCPVCPARASITES AND
TUMOURSconjugationAVD12345,6ItoRBC
-
1.Chronic passive venous congestion of the liver
CPVCConstrictive pericarditis, CCF are main causes for back
pressureCV are congested and centrilobular necrosis
occur.Periportal region: relatively less ischemia compare to the
hepatocytes.Alternate red color due to congestion and pale color
due to fat give nutmeg appearanceLong standing cases end up in
cardiac cirrhosiscan be the reason for nonspecific symptoms like
flatulence,indigestion and right hypochondrial discomfort
-
5. Cirrhosis of the liverOne of the top 10 causes of death in
the western world.It is characterized by:1. hepatocyte injury of
many causes.2. regeneration of remaining cells to form nodules.3.
fibrosis replacing the damaged tissue.4. loss of global
architecture because of the whole process.5. reorganised vascular
architecture resulting in shuntsCauses of the cirrhosis Alcoholic
60-70%Post viral infection-HBV 10%Biliary 5-10%Haemochromatosis
5%Wilsons disease, alfa-1 AT deficiencyCryptogenic (no known cause)
10-15%Others: galactosemia, cardiac, syphilis.
-
Pathogenesis***Extensive fibrosis with type I and III collagen
synthesis in the lobulesCells of Ito are the source of collagen.
They are stimulated by TNF-a, TGF b, IL, destruction of
extracellular matrix and toxins. Remaining cells regenerate into
irregular nodules.Fibrosis and nodule formation results in
disorganization of sinusoids, they become like capillaries and
hepatocyte isolation resulting in decreased secretion of albumin,
clotting proteins and lipoproteins. anastomosis results in high
pressure in capillaries and establishment of shunts.Bile duct
obliteration results in jaundice.Increased HP, hypoalbuminemia,
increased thoracic duct flow, osmotic effects, sodium retention all
lead to ascitis and edema. congestion leads to splenomegaly.
-
1. necrosis.2. regeneration->nodule.3. fibrosis.4. vascular
changePoint of no return32
-
Macronodular cirrhosis
-
Hepatic failure80-90% cell destruction- loss of functionVH,
drugs: INH, acetaminophen, mushroom, alcohol are some of the
causesGI bleed, infection, electrolyte disturbance, surgery, CCF
hasten failureC/F: Jaundice, hypoalbuminemia, hyperammonemia, fetor
hepaticus, palmar erythema, spider nevii. hypogonadism,
gynecomastia, ARDS, uremia, coagulopathy, encephalopathy,
hepatorenal syndrome and multi organ failure.
-
JaundiceYellow discoloration of skin & sclera due to excess
serum bilirubin. >40umol/l, (3mg/dl)Conjugated &
Unconjugated types Obstructive & Non Obstructive
(clinical)Pre-Hepatic, Hepatic & Post Hepatic typesJaundice -
Not necessarily liver disease *
-
Ascites in Cirrhosis
-
Gynaecomastia in cirrhosisPorta-systemic anastomosis: Prominent
abdominal veins.
-
Pathophysiology of portal
hypertensionEdemahypoalbuminaemiaAscitesSecondary
aldosteronismPortal hypertensionHypoalbuminemiaHematemesis- rupture
esophageal varices due to portal hypertensionSpidernaevi-
hyperestrogenismPurpura and bleed- reduced clotting factorsComa-
bacterial metabolitesInfection- reduced Kupffer cell no. and
function
-
Blood: Conjugated & UnconjugatedStool StercobilinUrine
Urobilinogen
-
Causes of PHTPre- sinusoidalPortal fibrosis due
toSarcoidosisSchistosomiasisHepatoportal
sclerosisCirrhosisSinusoidalCirrhosisPost- sinusoidalBudd-Chiari
syndrome (Thrombosis of hepatic veins)Tumors
Hemodynamic changes proximal or distal to sinusoids or at
sinusoid.
Increased portal vascular resistance and intrahepatic shunting
between high pressure hepatic artery and portal veinsPathogenesis
of portal HT
-
Primary carcinoma liverCan be hepatocellular (90%)
/cholangiocarcinoma (10%)Most common visceral cancerIn developing
countries vertical transmission of infection from mother to baby
leading to carrier state and cancer occurs around 40yrIn developed
countries after 60yrs because of cirrhosis due to HCV or alcohol or
hemochromatosis
-
Pathogenesis.HBV virion integrates and as regeneration occurs
mutations take place. protein X is producedIt has insulin
GF-property and binds to p53 resulting in its growth suppressor
activity.Aflotoxins in some food integrate with liver cell DNA and
mutating p53,(in subsaharan Africa and china genetically people may
lack enzymes for detoxifying aflotoxins)Cirrhosis due to HCV or
alcohol
-
Morphology.Gross.as unifocal nodule, multifocal nodule or
diffusely infiltrative type. All cause liver enlargementNodule may
look pale or greenishInvasion of tumour to portal vein/IVF seen
Microscopy.pattern varies from well differentiated to highly
anaplasticTrabecular, acinar, pseudoglandular patterns can
occur.Features of anaplasia, inreased N:C ratio, nucleoli and
intranuclear inclusions.
-
SECONDARY TUMOURSMetastasis to liver from other organs is more
common than primaryMetastasis from cancer anywhere in the body can
be found in liver. Most from breast, lung, colon and stomach
caLiver is enlarged, nodular with umbilicationThey can be
asymptomatic.
-
Liver cystsSimple cyst / Polycystic diseaseSmall multiple cyts
(10-20mm)Hydatid cystsEchinococcus granulosusLamainated fibrous
wallNumerous daughter cysts-rupture- anaphylactic shock in
sensitized patientsCholedocheal cystsRare, intra or extrahepatic
cysts of bile ductsPredispose to cholangitis
-
Acute pancreatitisAutodigestion of the pancreas by its escaped
enzymes Clinical features (Symptoms) Pain
(sudden,intense,continuous, upper abdomen back, bizarre
position)
Nausea and VomitingInvestigations: 1-Blood testsSerum amylase
and lipase levels may be slightly elevated in chronic pancreatitis;
high levels are found only during acute attacks of
pancreatitis.
-
-Abdominal x-ray: Pancreatic calcifications, often considered
pathognomonic of chronic pancreatitis, are observed in
approximately 30% of cases.
-
Etiology: (GET SMASHED)G: Gallstone.(common)E: Ethanol. T:
Truma.. S: Steroid.. M: Mumps.A: Alcoholism (common) or
autoimmune.S: Scorpion bits.H: Hyperlipidemia.E: ERCP.D: Drugs:
Thiazide, Azathioprine.
-
Pathophysiology:When the activation of digestive proenzymes
occurs in pancreatic duct system or aciner cells, the inflammation
is the result. Oedema or obstruction of ampulla of veter resulting
in reflexes Of bile into pancreatic duct or to acinar
cells.Pancreas shows edema & necrosis.(10%-30% mortality
rate).The release of digestive enzymes lead to fat necrosis in the
pancreas &peritoneal cavity.
DDx:Perforated peptic ulcer.Acute cholecystitis & biliary
colic.Acute Int obstruction.Renal colic.DKA.
-
Clinical Features:Hx :Abdomenal pain: sever, stay 12-24h after
eating a large meal or consuming alcohol,rediate to the back or to
the shoulder, pain is worse by walking or laying supine &
better after sitting or leaning forward.N &V.Shock in sever
case.Severe acute pancreatitis may cause dehydration and low blood
pressure. The heart, lungs, or kidneys can fail. If bleeding occurs
in the pancreas, shock and even death may follow.Abd Ex:Tenderness
in epigastric & guarding of Abd muscles.Mild Abd distention( if
the purulytic ileus develop).In sever advanced case:Grey turners
sign.Cullens sign.
-
Investigation:Serum amylase; It stays 48-72h then become
normal.Serum lipase; (diagnostic test) It elevated for 7-14
days.Other: -WBC (15000-30000). -LDH>500 U/dl - Glucose. -
Albumin. - Ca in serum. - AST.Bilurbin,Alkaline Ph. - ABG show
Hypoxia.
-
Xray of Abdomen: -gall stones. -Sentinel loop: air filled SI in
the LUQ. -Colon cut off sign: gas-filled seg of transverous colon
abruptly ending at the area of pancreatic inflammation.
U/S: -Gall stones. -Bilary obstruction. -Psudocyst.
-
CT: (is the dignostic even with normal amylase). -enlarged
pancreas. -Psudocyst. -Abscess & hemorrhage. -Presence of gas
bubbles in CT scan indicate pancreatic abscess.
-
COMPLICATION:Shock & renal failure:(pancritic necrosis is
association with leakage of fluid in the pancreatic bed & also
illus with fluid filled the bowl leading to tubular necrosis).Hypo
Ca: sequestration of Ca in fat
necrosis.(sponification)Hypoalbuminemia: Capillary
permeability.Hyperglucemia: due to disruption of pancreatic islets.
Hypoxia: Resp distress.
-
6- Pancreatic : -Necrosis. -Abscess. -Pseudocystis:a
circumscribed collection of fluid rich in pancreatic enzymes,
blood, and necrotic tissue, typically located in the lesser sac of
the abdomen. Pancreatic pseudocysts are usually complications of
pncreatitis. The prefix pseudo- (Greek for "false") distinguishes
them from true cysts, which are lined by epithelium; pseudocysts
are lined with granulation tissues.
7- GI: -UGI Bleeding. -duodenal obstruction. -Gastric or
duodenal erosion. -splenic or portal vein thrombosis. - compression
by pancreatic mass. - compression of common bile duct.
-
Assesment of severity (Ransons Criteria)3 or more indicate sever
pancreatitis:Age > 55 Y/O.Blood glucose > 200 mg/dl.WBC >
16000AST > 250 IU/L.Serum LDH >350 IU/L.
-
Development of the following in the first 48h indicate a
worsening porgnosis: (PANCREAS)P: PO2 < 8KPa.A: Age > 55y.N:
Neutrophil > 15000000000L.C: Calcium 16 mmol/L)E: Enzymes:
-LDH>600 iu/L. -AST >200 iu/L.A: Albumin: 10 mm0l/L.
-
Chronic Pancreatitis:
Is chronic inflammatory disease characterized by fibrosis &
dustruction of exocraine pancreatic tissues.Both forms of
pancreatitis occur more often in men than women. Chronic
pancreatitis often develops in people who are between the ages of
30 and 40.EtiologyAlcoholism.(common)Malnutrition.Stnosis of
ampulla of veter.
-
C/F:Abd pain.Weight loss, Aneroxia, Avoidness of food bcz of
post- prandial pain, Malabsorbtion.Steatorrhea.On Ex: Epigastric
pain.
Abd xray : clacified pancreas.U/S AbdCT Abd: :
atrophy,clacification.ERCP.Investigation
-
What is Pancreatic CancerA disease in which malignant (cancer)
cells are found in the tissues of the pancreas
4th leading cause of death from cancer in males5th in
femalesAffects people at 70-80 y/o60-80% occur at the head of the
pancreas
-
Laboratory TestsBLOOD TESTS:Amylase: (normal value: 30-110 U/L)
the blood level of amylase is usually significantly
elevated>>Critical value: >Normal values: bilirubin=
0.2-1.3 mg/dl , phosphatase= 38-126 U/L>>8-12 hours fasting
for more accurate results
CEA (Carcinoembryonic antigen): a tumor marker used as a
monitoring toolNormal Value:
-
CA 19-9 (Cancer Antigen 19-9) testing: Cancer antigen 19-9 (CA
19-9) is aproteinthat exists on the surface of certain cancer
cells. >>a tumor marker for pancreatic cancer; it may be used
to monitor for cancer recurrence but is not useful for detection or
diagnosis>>Normal Value: >CA 19-9 >37 U/mL result may
indicate pancreatic cancer >>CA 19-9 is elevated in about 70%
of people with advancedpancreatic cancer
Computed tomography (CT) scan: useful for detecting pancreatic
masses and checking for metastasized cancerBiopsy: used to confirm
diagnosis of cancer, often in conjunction with CT scan.
-
The primary filtering element for the blood. Acts as a filter
against foreign organisms that infect the blood stream.The site of
red blood cell and platelet storage.Filters out old red blood cells
and recycles them.
-
TUMORSSpleen - mostly secondary involvementnon-Hodgkins Lymphoma
most common malignancyMain Tx: Chemo +/- RTSpleen is the primary
site10% Hodgkins disease30% of resected spleens (staging procedure)
have (+) histologyHairy cell leukemiaResect for symptomatic
splenomegalyImproved survivalCML & CLLsymptomatic splenomegaly
= splenectomy