Embed Size (px)
Citation preview

www.elsevier.com/locate/braindev
Brain & Development 29 (2007) 251–253
Case report
Disappearance of frontal N30 component of median nerve stimulatedSSEPs in two young children with abnormal striatal lesions
Yosuke Kato a,*, Chisako Fukuda a, Yoshihiro Maegaki b, Takehiko Inoue b,Rika Hiraiwa c, Hisayuki Hiraiwa c, Kousaku Ohno b, Yutaka Tomita a
a Department of Pathobiological Science and Technology, School of Health Science, Faculty of Medicine,
Tottori University, 86 Nishi-cho, Yonago 683-8503, Japanb Department of Child Neurology, Institute of Neurological Sciences, Faculty of Medicine, Tottori University, Yonago, Japan
c Eastern Shimane Rehabilitation Hospital for The Disabled, Matsue, Japan
Received 7 February 2006; received in revised form 5 September 2006; accepted 7 September 2006
Abstract
Median nerve stimulated short-latency somatosensory evoked potentials (MN-SSEPs) were performed in two young childrenwith extrapyramidal symptoms. Brain MRI showed bilaterally symmetric striatal lesions in both cases. The subcortical components(N9, N11, N13, N18, P11, and P13) and the parietal component (N20) were normally detected, whereas the frontal component(N30) was not detected bilaterally in either case. In conclusion, our findings suggest that frontal N30 disappearance could beobserved since as early as young childhood and it may pathophysiologically reflect severe dysfunction in the extrapyramidal system.� 2006 Elsevier B.V. All rights reserved.
Keywords: MN-SSEPs; N30; Extrapyramidal symptom; Striatum; Early childhood
1. Introduction
Median nerve stimulated short-latency somatosenso-ry evoked potentials (MN-SSEPs) are effectively exam-ined for physiological evaluation of extrapyramidalmotor disorders since the origins of many SSEP compo-nents have been relatively well identified. Although thefrontal N30 component of MN-SSEPs appears abnor-mal in several diseases characterized by extrapyramidalmotor dysfunction in adulthood [1–3] and adolescent[4], the precise nature and the site of origin has not yetbeen identified.
We have previously shown that the amplitude of thefrontal N30 declined or disappeared in adults with ath-etotic cerebral palsy, due to perinatal hypoxia, suggest-
0387-7604/$ - see front matter � 2006 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2006.09.002
* Corresponding author. Tel.: +81 859 38 6389; fax: +81 859 386380.
E-mail address: [email protected] (Y. Kato).
ing that frontal N30 reduction may reflect severedysfunction in the basal ganglia [4,5]. In the presentstudy, MN-SSEPs were performed in two young chil-dren with lesions in the caudate nucleus and putamendemonstrated on brain MRI.
2. Patients and methods
2.1. Patients
Case 1: The first patient was a 6-year-old boy whosedevelopment in infancy was normal. At about 2 years ofage, he began to fall frequently, and motor developmentalmost arrested. He walked slowly with extension of thelegs, and tried to run with difficulty taking initial steps.He also appeared clumsy, rigid in the upper limbs andmade facial grimaces. Then he showed choreoathetoticmovement in the upper limbs, and his phonation became

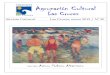
Fig. 1. T2-weighted MRI of Case 1 (6 years of age) (A) and Case 2 (1year and 1 month of age) (B). High intensity lesions localized at thebilateral caudate nucleus and putamen were observed in both cases.
252 Y. Kato et al. / Brain & Development 29 (2007) 251–253
disturbed. At 6 years of age, high intensity lesions of T2-weighted image localized at the bilateral caudate nucleusand putamen were demonstrated on MRI examination(Fig. 1A).
Case 2: The second patient was a boy aged 1 year and2 months who developed normally until 6 months afterbirth. At about 10 months of age, he showed unsteadi-ness in head control, restlessness, clumsiness andmarked choreoathetosis in the limbs. Then he developeddystonic head posture, dysphagia and lost the ability tostand with support. At the age of 1 year and 1 month,high intensity lesions localized at the bilateral caudatenucleus and putamen were observed on T2-weightedMRI examination (Fig. 1B).
2.2. MN-SSEPs
After informed consent was obtained from the par-ents, MN-SSEPs were performed in the awake or lightsleep state with the Nihon Kohden Neuropack 8MEB-4208 apparatus. The median nerve was stimulatedat the wrist at a frequency of 4 or 5 Hz just above themotor threshold strength. Scalp electrodes were placed
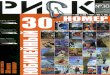
Fig. 2. MN-SSEPs of age-matched normal subject (5 years of age) (A
on F3, F4, C3 0, C4 0 (2 cm behind C3 and C4) accordingto the 10/20 international system. Reference electrodeswere placed at Erb’s point contralateral to the stimula-tion side, ear lobes, and Fz. Five hundred or a thousandsweeps were averaged for all trials. Each trial wasrepeated at least twice to confirm reproducibility. Theanalysis time was 60 ms, and the filtering bandwidthwas set at 20–3000 Hz.
3. Results
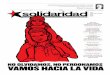
MN-SSEPs recordings of patients and age-matchednormal subjects (5 years old and 1 year old) are shownin Figs. 2 and 3. The subcortical components (N9,N11, N13, N18, P11, and P13) and the parietal compo-nent (N20) were found normally in both cases. In con-trast, the frontal component (N30) was not detected ineither case.
4. Discussion
The origin of the frontal N30 might be in a dipole ofthe posterior bank of the central sulcus [6], while otherssuggested that its origin might be in the supplementarymotor area (SMA) [7], either area receiving major inputfrom the striatum relayed by the thalamic nuclei. There-fore, several disorders that disturb striatal function, suchas Parkinson’s disease [1] or Huntington’s disease [2],show N30 reduction in most cases, in contrast to its highamplitude in patients with dystonia [3]. From a physio-logical perspective, the amplitude of the frontal N30 innormal adults was recently reported to decrease duringvoluntary movement in the upper extremity [8]. Thisfinding, called the striatal ‘‘sensory gating’’ effect, sug-gested the relationship between motor preparation andfrontal N30 reduction. As described above, the attitude
) and Case 1 (6 years of age) (B). N30 was not observed in (B).

Fig. 3. MN-SSEPs of age-matched normal subject (1 year of age) (A) and Case 2 (1 year and 2 months of age) (B). N30 was not observed in (B).
Y. Kato et al. / Brain & Development 29 (2007) 251–253 253
of frontal N30 is influenced by a few factors, whichshows a clear contrast to a rather simple correspondenceof afferent input to N20 production. The nature and siteof origin of the frontal N30 remains controversial inadults. Disturbance in the circuitry of the extrapyrami-dal system might result in inhibitory or facilitative stria-tal gate effect in adults.
We previously reported that the amplitude of thefrontal N30 decreased or disappeared in adult patientswith athetotic cerebral palsy especially due to perinatalhypoxia, suggesting that frontal N30 reduction mayreflect the sequela of severe destructive damage in thebasal ganglia [4,5]. The constant existence of the frontalN30 in MN-SSEPs during very young childhood wasnot discussed until our recent report that those compo-nents were detected in all normal controls over 3 yearsof age [9]. Then, we proceeded to ascertain its existencein younger children and empirically found the constantappearance of frontal N30 in 9 normal younger children(from 4 months to 1 year and 9 months; mean 12months). Therefore, evidence that the frontal N30 com-ponent could not be detected in two young children withbilaterally symmetric striatal lesions in this study wouldindicate a relationship between frontal N30 disappear-ance and striatal lesions even in young children. In con-clusion, frontal N30 disappearance in MN-SSEPs mayreflect severe dysfunction of the striatum even as earlyas in very young childhood. This finding will contributeto prognostic diagnosis of extrapyramidal motor distur-bance in very young children.
References
[1] Rossini PM, Traversa R, Boccasena P, Martino G, Passarelli F,Pacifici L, et al. Parkinson’s disease and somatosensory evokedpotentials: apomorphine-induced transient potentiation of frontalcomponents. Neurology 1993;43:2495–500.
[2] Topper R, Schwarz M, Podoll K, Domges F, Noth J. Absence offrontal somatosensory evoked potentials in Huntington’s disease.Brain 1993;116:87–101.
[3] Reilly JA, Hallett M, Cohen LG, Tarkka IM, Dang N. TheN30 component of somatosensory evoked potentials in patientswith dystonia. Electroencephalogr Clin Neurophysiol1992;84:243–7.
[4] Fukuda C, Tomita Y, Maegaki Y, Kubota N. Frontal N30 ofmedian nerve SSEPs for evaluation of movement disorders withdestructive basal ganglia deficits. Neuropediatrics 2003;34:205–10.
[5] Ueno M, Fukuda C, Tomita Y. Frontal N30 of median nerveSSEPs and the brain image of basal ganglia in patients withathetotic cerebral palsy (in Japanese). No To Hattatsu (Tokyo)2006;38:373–4.
[6] Allison T, McCarthy G, Wood CC, Darcey TM, Spencer DD,Williamson PD. Human cortical potentials evoked by stimulationof the median nerve. I. Cytoarchitectonic areas generating short-latency activity. J Neurophysiol 1989;62:694–710.
[7] Desmedt JE, Cheron G. Non-cephalic reference recording of earlysomatosensory potentials to finger stimulation in adult or agingnormal man: differentiation of widespread N18 and contralateralN20 from the prerolandic P22 and N30 components. Electroen-cephalogr Clin Neurophysiol 1981;52:553–70.
[8] Murase N, Kaji R, Shimazu H, Katayama-Hirota M, Ikeda A,Kohara N, et al. Abnormal premovement gating of somatosensoryinput in writer’s cramp. Brain 2000;123:1813–29.
[9] Fukuda C, Tomita Y, Maegaki Y. P22 and N30 of median nerveSSEPs: independence of the frontal waves from parietal waves [inJapanese]. No To Hattatsu (Tokyo) 2002;34:295–9.