Embed Size (px)
Citation preview

150
Chaudhary P et alMay-August 2012; Vol 10 (No.2);150-152
Discitis after spinal anaesthesia
__________________________________________________Address for correspondenceDr Pashupati ChaudharyAssociate Professor, Department of OrthopaedicsBP Koirala Institute of Health Sciences, DharanEmail: [email protected]
¡ Case Report
Discitis after spinal anaesthesia in lower limb surgery in orthopaedics
P Chaudhary1, BP Shrestha1, GP Khanal1, R Maharjan1, R Rijal1, SR Paneru1, DK Yadav2
1Department of Orthopaedics and 2SPH &CMB.P.Koirala Institute of Health Sciences, Dharan, Nepal
Abstract
Spinal Anaesthesia has its own complications from beginning of its use but due to lowerincidence of its complications, its popularity has continued to increase world wide. Wepresent a case of 51 year old gentleman who had undergone removal of implant (plate fromtibia and Rush nail from femur) at Orthopaedic Depatment of B.P.Koirala Institute ofHealth Sciences, Dharan, Nepal with complain of low back pain with radiation to rightlower limb, decreased sensation, difficulty in voiding following a surgery.We report this casefor its rarity and unique characteristics and to heighlight the importance of bits timely treatmentso that serious neurological complications do not occur.
Keywords: epidural abscess, discitis, spinal anaesthesia
IntroductionSpinal Anaesthesia is one of the most common modeof given anaesthesia to perform lower limb surgeryin Orthopaedics. Spinal anaesthesia is accompaniedby many definite and terrible dangers which are fartoo little appreciated by surgeons andanaesthesiologists. Neurological complications, someof them serious, sometimes occur following spinalanaesthesia. In the majority of the relatively fewcases in which they occur, they are caused by factorswhich can be obviated. Rigid adherence to definedsafeguards will reduce the incidence of complicationsand overcome most of the objections to theprocedure.1
Case descriptionsA 51 year old gentleman from remote hilly areashad alleged history of RTA 7 years back for whichhe had undergone ORIF+Plating for both tibia and
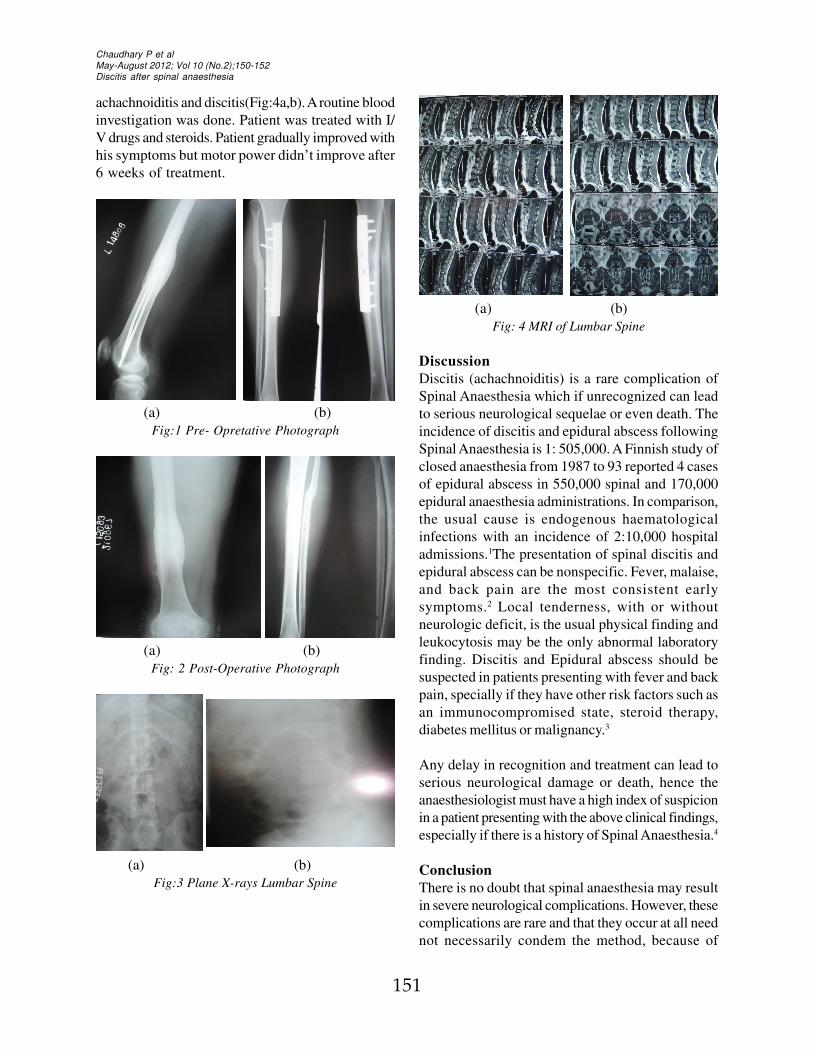
femur outside. After 3 months of post operativeperiod, there were implant failure ie femoral platebroke. He reported to department of Orthopaedics,B.P.Koirala Institute of Health Sciences, Dharan withbroken plate in femur without bony union. He wasoperated with Rush nails after removing broken platefrom femur (Fig:1a,b). He was on susequent followup and fracture in both tibia and femur were unitedboth clinically and radiologically in 6th post operativemonth.This time he was operated for removal ofimplant (Fig:2 a,b). The total anaesthetic time was 3hours.Anaesthesiologist had given 0.5 ml of heavybuvupacaine solution using 24G spinal needle,Anaesthesia was given in between L4/L5 disc spacein first attempt. As anaesthetic effect wore off,patients begun to complain of pain in the back whichis radiating down to the legs.He had difficulty ofvoiding urine. There were scattered areas ofhyposthesia on sciatic nerve distribution. On motorexamination, EHL on right side was 0/5. There wereno history of fever and no meningismus were present.Plane X-ray of lumbar spine was done which did notshow any abnormality (Fig:3a,b). MRI scanning ofL/S spine was done which was suggestive of
151
Chaudhary P et alMay-August 2012; Vol 10 (No.2);150-152Discitis after spinal anaesthesia
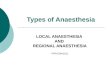
achachnoiditis and discitis(Fig:4a,b). A routine bloodinvestigation was done. Patient was treated with I/V drugs and steroids. Patient gradually improved withhis symptoms but motor power didn’t improve after6 weeks of treatment.
(a) (b)Fig:1 Pre- Opretative Photograph
(a) (b)Fig: 4 MRI of Lumbar Spine
DiscussionDiscitis (achachnoiditis) is a rare complication ofSpinal Anaesthesia which if unrecognized can leadto serious neurological sequelae or even death. Theincidence of discitis and epidural abscess followingSpinal Anaesthesia is 1: 505,000. A Finnish study ofclosed anaesthesia from 1987 to 93 reported 4 casesof epidural abscess in 550,000 spinal and 170,000epidural anaesthesia administrations. In comparison,the usual cause is endogenous haematologicalinfections with an incidence of 2:10,000 hospitaladmissions.1The presentation of spinal discitis andepidural abscess can be nonspecific. Fever, malaise,and back pain are the most consistent earlysymptoms.2 Local tenderness, with or withoutneurologic deficit, is the usual physical finding andleukocytosis may be the only abnormal laboratoryfinding. Discitis and Epidural abscess should besuspected in patients presenting with fever and backpain, specially if they have other risk factors such asan immunocompromised state, steroid therapy,diabetes mellitus or malignancy.3
Any delay in recognition and treatment can lead toserious neurological damage or death, hence theanaesthesiologist must have a high index of suspicionin a patient presenting with the above clinical findings,especially if there is a history of Spinal Anaesthesia.4
ConclusionThere is no doubt that spinal anaesthesia may resultin severe neurological complications. However, thesecomplications are rare and that they occur at all neednot necessarily condem the method, because of
(a) (b)Fig: 2 Post-Operative Photograph
(a) (b)Fig:3 Plane X-rays Lumbar Spine

152
Chaudhary P et alMay-August 2012; Vol 10 (No.2);150-152
Discitis after spinal anaesthesia
careful analysis, it appears that most of them can beavoided. Trauma and infection may be preventedby scrupulus attension to technique
References1. Lalla RK, Joshi MC, Sridhar Sahni MS H MJAFI
2005; 61: 186-187
2. Hilavin ML. Spinal epidural abscess: A 10 yearprospective study. Neurology 1990; 27:177-84.
3. Aromaa U, Lahdensuu M, Cozanitis DA. Severecomplications associated with epidural and spinalanaesthesias in Finland1987-93. A study basedon patient insurance claims. ActaAnaesthesiology Scand 1997; 41(4):445-52.
4. Deardre Chao, Anil Nanda. Spinal epiduralabscess: A diagnostic challenge. Am FamPhysician 2002; 65:1341-6.