Embed Size (px)
Citation preview
Ray Miller 8/18/2017
Direct Supply 1
Liz Jen
sen
, R
N, M
SN
, R
N-B
C
Clin
ical D
irecto
r, D
irect Su
pp
ly®
, In
c.
By Ray Miller, MSOSH, Dir. of Risk and Safety,
Direct Supply®, in a collaborative effort
With Liz Jensen, RNA MSN, RN-BC
Clinical Director, Direct Supply®, Inc.
2 2
Disclaimer
The materials, comments and other information
contained in this presentation are intended to provide
general information but not advice about certain
regulations and initiatives.
This information is not and not intended as legal or
other advice and each situation may vary depending
on the particular facts and circumstances.
You should not act upon this information without first
consulting with qualified legal counsel.
Thank You.
Ray Miller 8/18/2017
Direct Supply 2
3 3
Today’s Focus
• Aging (in AL is not new—what’s changed?)
• Frameworks
• Trends (Programs, Building Clinical Capacity and Services)
• Resources
4 4
Here’s what we’ve been told …
Seeking to Answer
“How can I improve the health and well being of my residents?”
• “We are concerned about residents with ______________”
• “Residents move in and quickly need an increased level of
care …”
• “We need to differentiate ourselves from our competitors”
• “Our acuity continues to rise … HELP!”
Ray Miller 8/18/2017
Direct Supply 3
5 5
What do YOUR Goals look like?
• “Meet the day-to-day needs of my residents”
• “Reduce the frequency of residents moving out”
• “Meet a specific need (memory care …) in my community”
• “I have insurance companies that want us to provide more
services to keep residents from going to the hospital”
• “Improve the health and wellness of my residents so they can
live in our community as long as possible”
6 6
Self-Check: Where are you?
“There is the expectation that we’ll do everything for them…
it’s part of our hospitality commitment”
Or “We are here to be your partner in helping you
live your life and stay healthy.”
At 65 years of age, this where I find myself:
“Everything you do for me you take from me!
“Help me to do it alone!”
Maria Montessori
Ray Miller 8/18/2017
Direct Supply 4
7 7
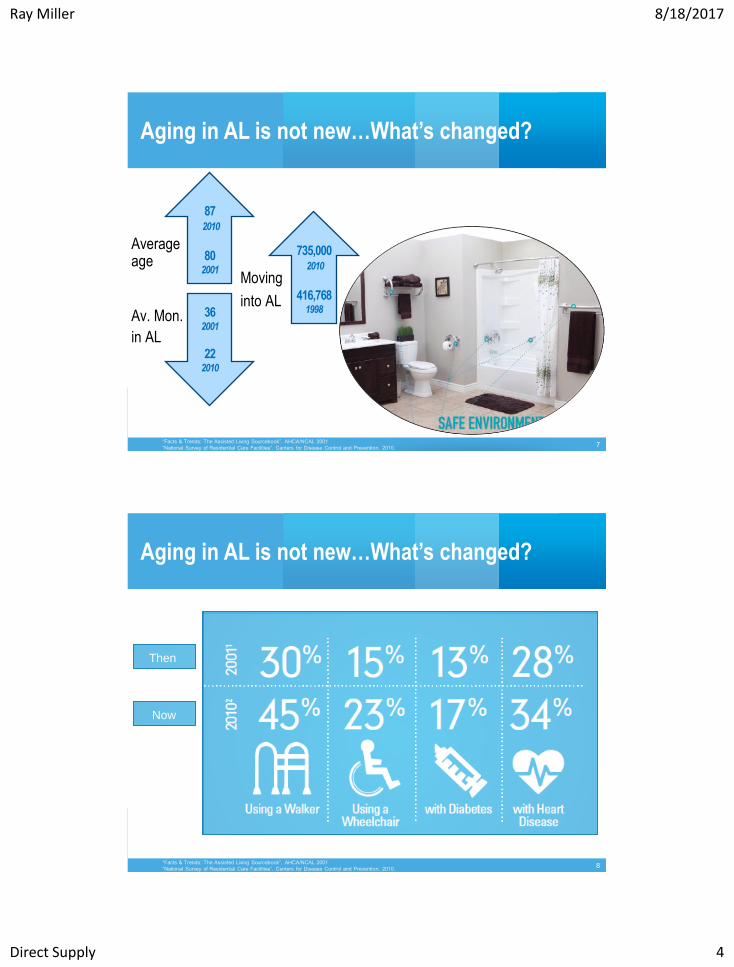
Aging in AL is not new…What’s changed?
“Facts & Trends: The Assisted Living Sourcebook”. AHCA/NCAL 2001
“National Survey of Residential Care Facilities”. Centers for Disease Control and Prevention, 2010.
Av. Mon.
in AL
87 2010
80 2001
36 2001
22 2010
735,000 2010
416,768 1998
Moving
into AL
Average age
8 8
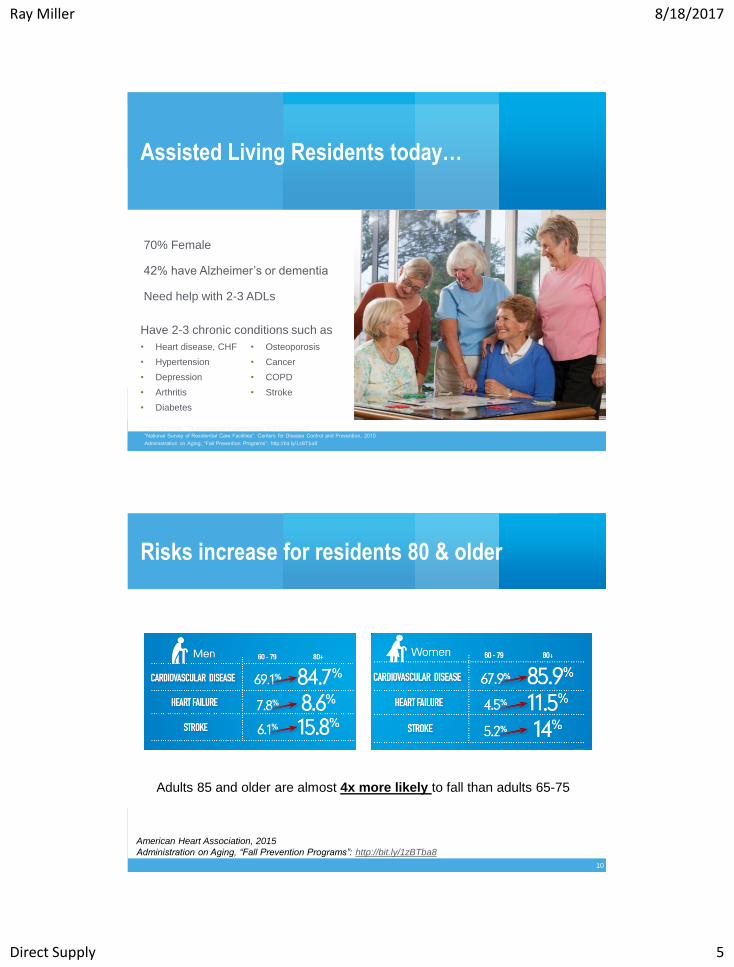
Aging in AL is not new…What’s changed?
“Facts & Trends: The Assisted Living Sourcebook”. AHCA/NCAL 2001
“National Survey of Residential Care Facilities”. Centers for Disease Control and Prevention, 2010.
Then
Now
Ray Miller 8/18/2017
Direct Supply 5
9 9
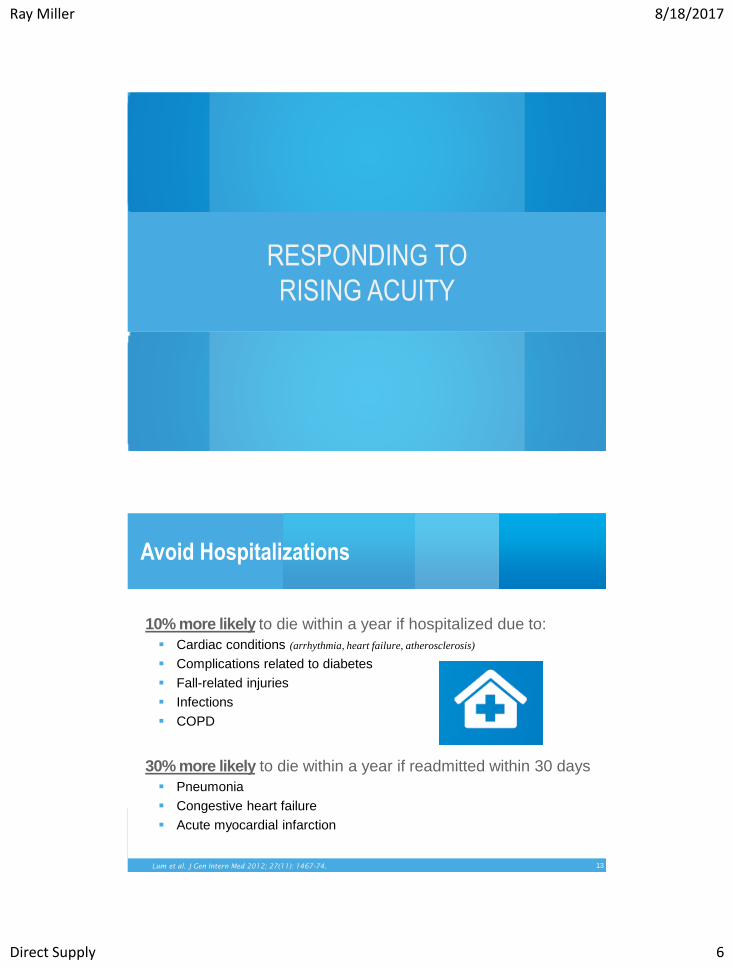
Assisted Living Residents today…
“Facts & Trends: The Assisted Living Sourcebook”. AHCA/NCAL 2001
“National Survey of Residential Care Facilities”. Centers for Disease Control and Prevention, 2010
Administration on Aging, “Fall Prevention Programs”: http://bit.ly/1zBTba8
70% Female
42% have Alzheimer’s or dementia
Need help with 2-3 ADLs
Have 2-3 chronic conditions such as
• Heart disease, CHF
• Hypertension
• Depression
• Arthritis
• Diabetes
• Osteoporosis
• Cancer
• COPD
• Stroke
10 10
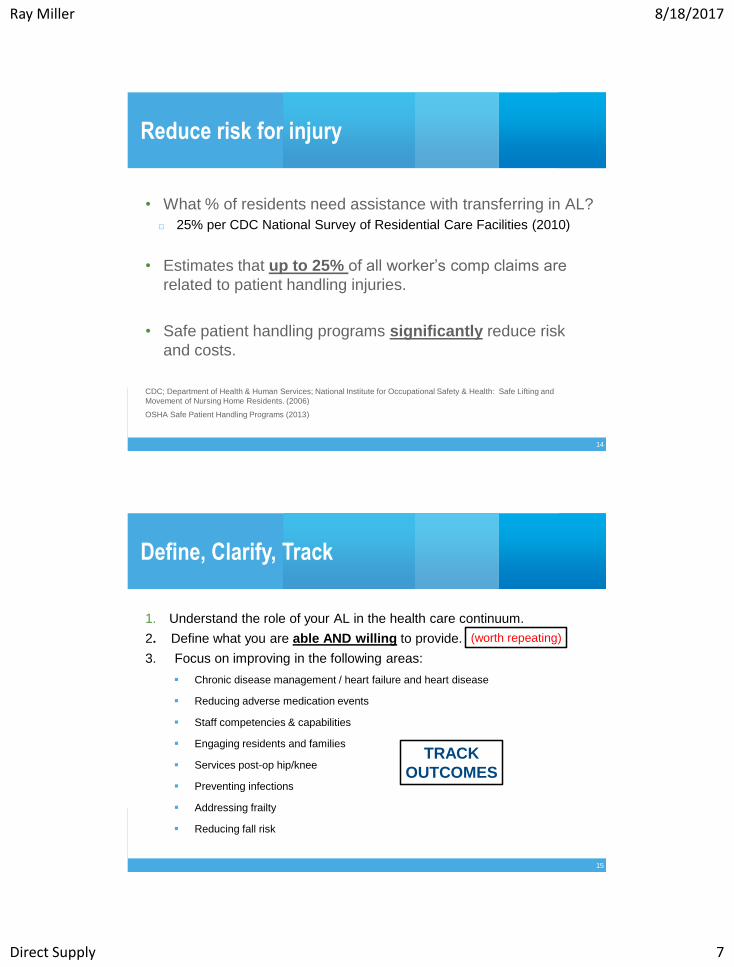
Risks increase for residents 80 & older
American Heart Association, 2015
Administration on Aging, “Fall Prevention Programs”: http://bit.ly/1zBTba8
Adults 85 and older are almost 4x more likely to fall than adults 65-75
Ray Miller 8/18/2017
Direct Supply 6
11
RESPONDING TO
RISING ACUITY
13 13
Avoid Hospitalizations
10% more likely to die within a year if hospitalized due to:
Cardiac conditions (arrhythmia, heart failure, atherosclerosis)
Complications related to diabetes
Fall-related injuries
Infections
COPD
30% more likely to die within a year if readmitted within 30 days
Pneumonia
Congestive heart failure
Acute myocardial infarction
Lum et al. J Gen Intern Med 2012; 27(11): 1467-74.
Ray Miller 8/18/2017
Direct Supply 7
14 14
Reduce risk for injury
• What % of residents need assistance with transferring in AL?
□ 25% per CDC National Survey of Residential Care Facilities (2010)
• Estimates that up to 25% of all worker’s comp claims are
related to patient handling injuries.
• Safe patient handling programs significantly reduce risk
and costs.
CDC; Department of Health & Human Services; National Institute for Occupational Safety & Health: Safe Lifting and
Movement of Nursing Home Residents. (2006)
OSHA Safe Patient Handling Programs (2013)
15 15
Define, Clarify, Track
1. Understand the role of your AL in the health care continuum.
2. Define what you are able AND willing to provide.
3. Focus on improving in the following areas:
Chronic disease management / heart failure and heart disease
Reducing adverse medication events
Staff competencies & capabilities
Engaging residents and families
Services post-op hip/knee
Preventing infections
Addressing frailty
Reducing fall risk
TRACK
OUTCOMES
(worth repeating)

Ray Miller 8/18/2017
Direct Supply 8
16 16
Self Check:
What does rising acuity impact?
Attracting and retaining staff?
Regulatory citations?
Risk / Litigation?
Occupancy?
…
17
FRAMEWORKS

Ray Miller 8/18/2017
Direct Supply 9
18 18
Keeping in Mind--the Nursing Care Dilemma in AL
• Assisted Living Regulations
Varies by state
Limits on “skilled care”, care delivered by nurses
Often limits ability of nurses to practice at “Top of License”
• Nurse Practice Act
Understanding how to practice at “Top of License”
19 19
Adapting existing models
• Population Health
• Naylor’s Transitional Care Model
• Community Health Nursing Model

Ray Miller 8/18/2017
Direct Supply 10
20 20
Population Health
What is population health?
Health outcomes for a group of individuals
How are health outcomes defined in Assisted Living?
Health-related and Quality of Life
(No real standard definitions)
21 21
Naylor’s* “Transitions of Care Model”
Hirschman, K., Shaid, E., McCauley, K., Pauly, M., Naylor, M., (September 30, 2015) "Continuity of Care: The Transitional Care Model" OJIN: The Online Journal of Issues in Nursing Vol. 20, No. 3, Manuscript 1.
1. Screening
2. Staffing
3. Maintaining Relationships
4. Engaging Patients & Caregivers
5. Collaborating
6. Assessing / Managing Risks &
Symptoms
7. Educating/Promoting Self-
Management
8. Promoting Continuity
9. Fostering Coordination
Mary D. Naylor, PhD, RN, FAAN 1] Architect of the Transitional Care Model
2] Marian S. Ware Professor of Gerontology at the Univ. of PA. School of
Nursing, Philadelphia 3] Dir. of the New Courtland Center for Transitions and
Health at the Univ. of PA School of Nursing, Philadelphia, PA.
The Transitions of Care Model
encompasses a broad range of
services and environments
designed to promote the safe and
timely passage of patients
between levels of health care and
across care settings (Coleman &
Boult, 2003; Naylor, 2003).
Ray Miller 8/18/2017
Direct Supply 11
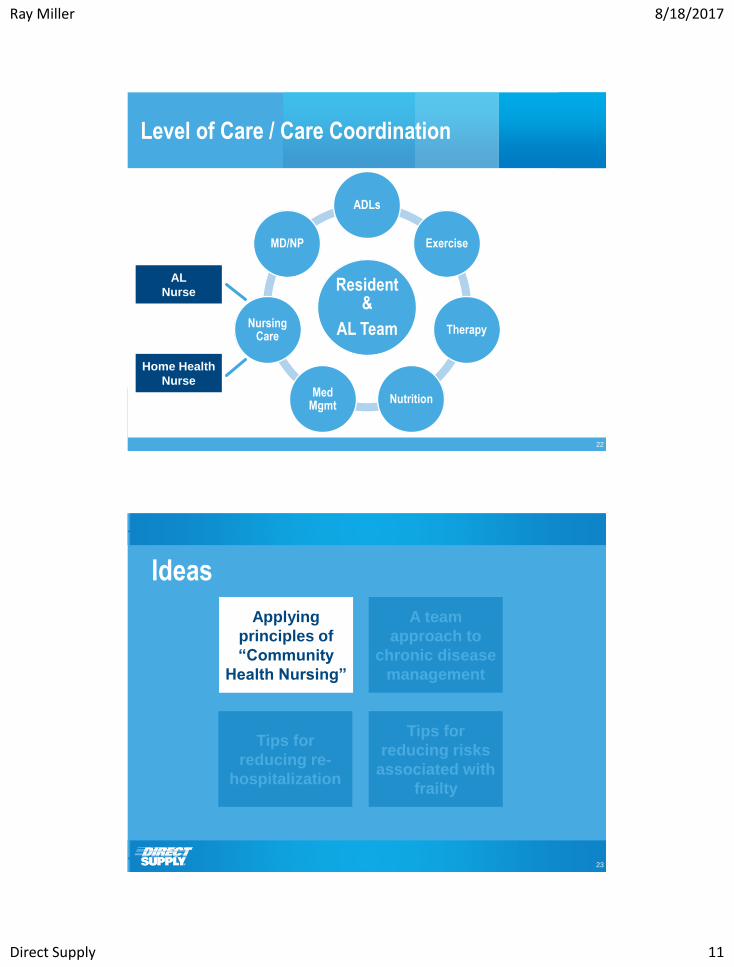
22 22
Resident &
AL Team
ADLs
Exercise
Therapy
Nutrition Med
Mgmt
Nursing Care
MD/NP
AL
Nurse
Level of Care / Care Coordination
Home Health
Nurse
23
Ideas
Applying
principles of
“Community
Health Nursing”
A team
approach to
chronic disease
management
Tips for
reducing re-
hospitalization
Tips for
reducing risks
associated with
frailty
Ray Miller 8/18/2017
Direct Supply 12
24
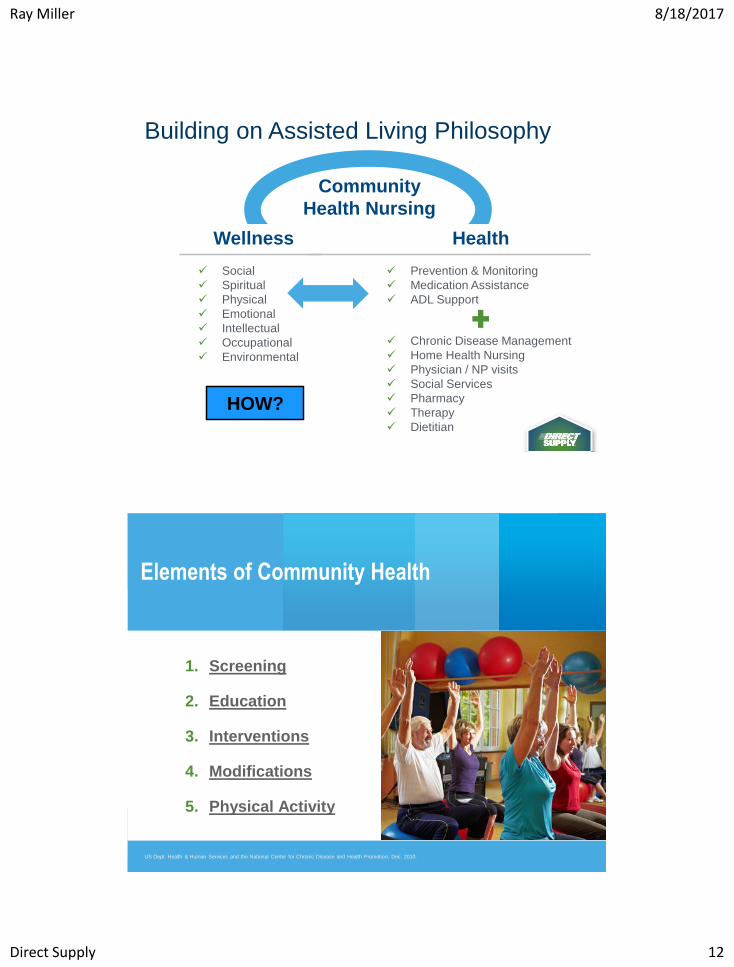
Building on Assisted Living Philosophy
Social
Spiritual
Physical
Emotional
Intellectual
Occupational
Environmental
Wellness
Prevention & Monitoring
Medication Assistance
ADL Support
Health
Chronic Disease Management
Home Health Nursing
Physician / NP visits
Social Services
Pharmacy
Therapy
Dietitian
Community
Health Nursing
HOW?
25 25
Elements of Community Health
US Dept. Health & Human Services and the National Center for Chronic Disease and Health Promotion; Dec. 2010.
1. Screening
2. Education
3. Interventions
4. Modifications
5. Physical Activity

Ray Miller 8/18/2017
Direct Supply 13
26 26
Conduct a Community Assessment
WHAT ARE THE TOP:
• 5 health-impacting diagnosis or conditions?
• 5-10 most frequently prescribed medications?
• 3 health/well-being-impacting incident types (past year)?
WHAT % OF RESIDENTS:
_______ Require transfer or mobility assistance by staff?
_______ Exercise at least 2-3 days per week?
_______ Have at least a HS education?
_______ Use oxygen regularly?
_______ Use wheelchairs?
_______ Use walkers?
_______ Smoke?
In my Community:
65%
10%
57%
??%
25%
45%
25%
(HD = 70%; Diabetes = 40%); ???% Arthritis
(Metoprolol, Lasix, Lipitor, Metformin, Aspirin)
(fall w/ injury, fall wo injury, med error)
Community Health Approach
27 27
Screening • Blood pressure checks, Cholesterol screening
Risk Identification • Smoking cessation classes; Medication management
Environmental Modifications • Health stations to check own blood pressure, weight or provide in apartment
• Exercise equipment—improve the gym
Health Education • Speakers, discussion sessions on heart disease, exercise, smoking cessations
• 1:1 Medication education with nurse, NP or pharmacist
Promoting Physical Activity • Daily exercise classes; Walking club; Personal trainer
Community Health Approach / Heart Disease (Team-based approach – a proven model)

Ray Miller 8/18/2017
Direct Supply 14
28 28
Community Health Approach /
Arthritis & Other Mobility Issues
Screening • Fall Risk Assessments—Individual, Environmental
• Transfer Assessment
Risk Identification • Medication changes
• Pain management / functional activities, exercise and sleep
• Wheelchair, walker, cane checks
Environmental Modifications • Transfer devices, Lifts, Grab bars bathrooms, Lighting, Exercise equipment
Health Education • Speakers, discussion sessions
• 1:1 Medication education with nurse, NP or pharmacist
Promoting Physical Activity • Exercise classes, massage therapy, stretching
30
Ideas
Tips for
reducing re-
hospitalization
Tips for
reducing risks
associated with
frailty
Applying
principles of
“Community
Health Nursing”
A team
approach to
individual
chronic disease
management

Ray Miller 8/18/2017
Direct Supply 15
31 31
Framework for Individual Care
Assisted Living Nursing: A Manual for Management and Practice edited by Dr. Ethel Mitty, EdD, RN, Dr. Barbara Resnick, PhD, CRNP, FAAN, Sandra Flores, RN
• Optimizing function -- Self-
care assistance and
support
• Decision making capacity
• Medication Management
• Service/Care Planning
• Health promotion
• Assessments
“Help me to do it alone!” Maria Montessori
32 32
Individual Care / Heart Failure
Define, Understand, Educate (Resident & Staff):
□ Exacerbation: Causes & Symptoms
□ Care Considerations & Monitoring
□ Engagement & Exercise
□ Nutrition & Fluid Intake
□ Advance Directives
□ Medications
REALITY:
A resident with
HF is at high risk
for a decline in
health
Ray Miller 8/18/2017
Direct Supply 16
33 33
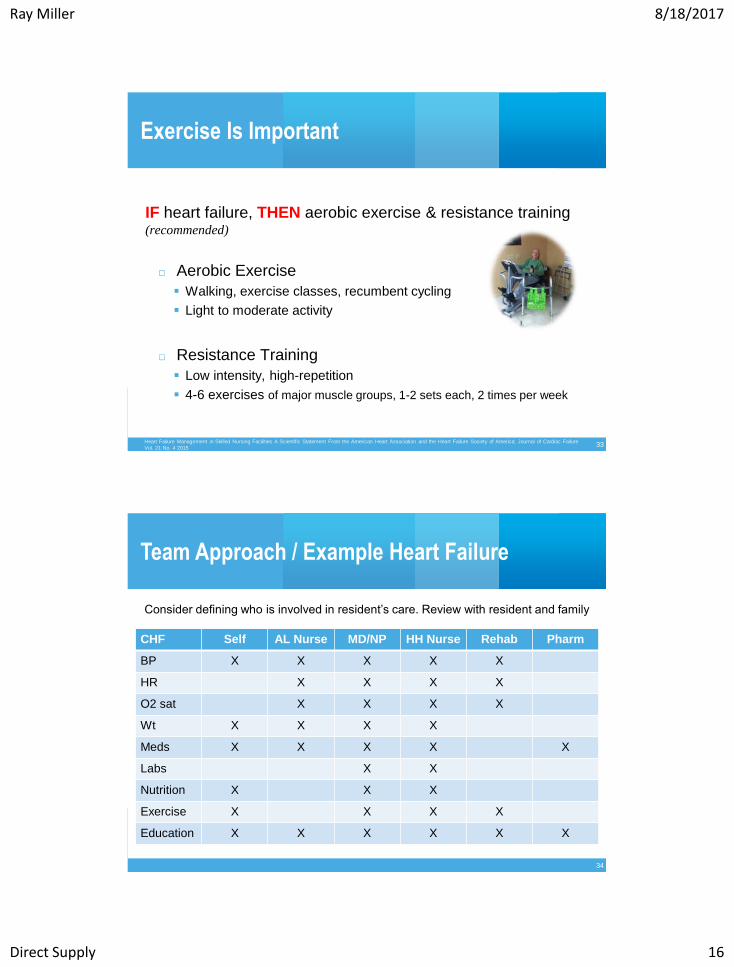
Exercise Is Important
Heart Failure Management in Skilled Nursing Facilities A Scientific Statement From the American Heart Association and the Heart Failure Society of America; Journal of Cardiac Failure
Vol. 21 No. 4 2015
IF heart failure, THEN aerobic exercise & resistance training (recommended)
□ Aerobic Exercise
Walking, exercise classes, recumbent cycling
Light to moderate activity
□ Resistance Training
Low intensity, high-repetition
4-6 exercises of major muscle groups, 1-2 sets each, 2 times per week
34 34
Team Approach / Example Heart Failure
CHF Self AL Nurse MD/NP HH Nurse Rehab Pharm
BP X X X X X
HR X X X X
O2 sat X X X X
Wt X X X X
Meds X X X X X
Labs X X
Nutrition X X X
Exercise X X X X
Education X X X X X X
Consider defining who is involved in resident’s care. Review with resident and family
Ray Miller 8/18/2017
Direct Supply 17
35 35
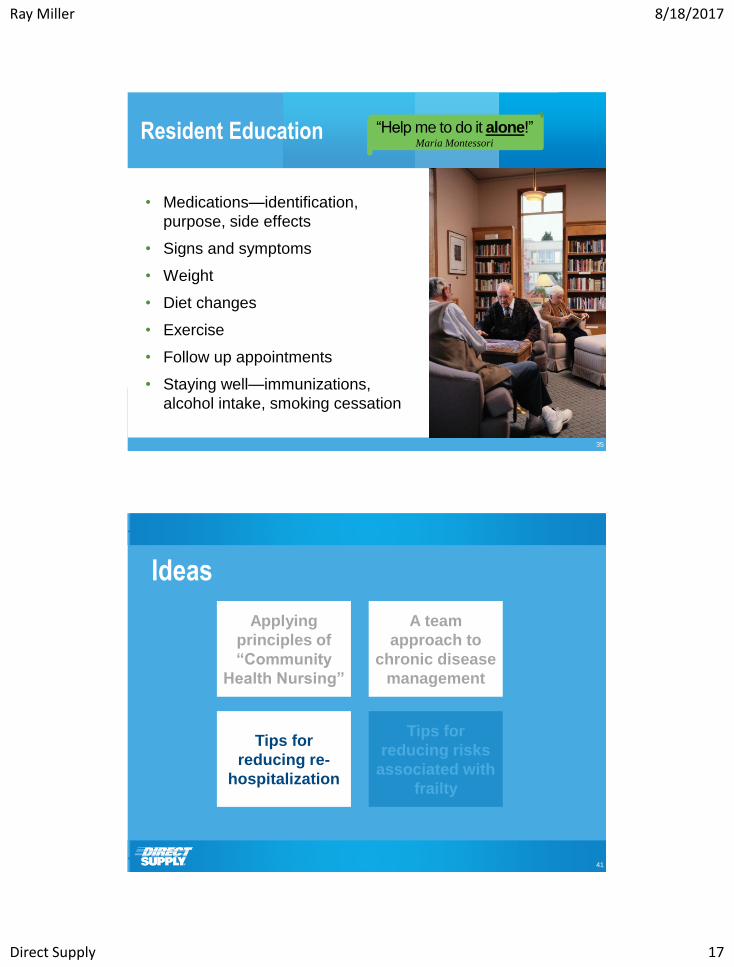
Resident Education
• Medications—identification,
purpose, side effects
• Signs and symptoms
• Weight
• Diet changes
• Exercise
• Follow up appointments
• Staying well—immunizations,
alcohol intake, smoking cessation
“Help me to do it alone!” Maria Montessori
41
Ideas
Tips for
reducing risks
associated with
frailty
Applying
principles of
“Community
Health Nursing”
A team
approach to
chronic disease
management
Tips for
reducing re-
hospitalization
Ray Miller 8/18/2017
Direct Supply 18
42 42
Care Models & Expanded Services – What we’ve seen
EXPAND:
• MD & NP Partnerships (On-site clinic hours; Home visits)
• Nursing staff (Hours; Expertise)
• Therapy services
OFFER:
• Social Service support
• Expanded Dietitians services
ENGAGE: Pharmacist Consultants
43 43
Clinical Competencies / Capabilities – Focus Areas
Knowledge Skill Ability/Attitude
• Community Health
Nursing
• Gerontological Care
• Risk Management
• Care Coordination
• Geriatric Nursing
Assessment
• Clinical / Technical
• Documentation
• Communication
• Delegation
• Education & Training
Ray Miller 8/18/2017
Direct Supply 19
44 44
Ideas for Improving Competencies – How To Focus
Knowledge
• Gero Nurse Preparation Course http://app1.unmc.edu/geronurseprep/
• Hartford Institute for Geriatric Nursing http://www.hartfordign.org/ (free)
• INTERACT Tools http://interact2.net/ (free)
• Access to MD, NP, PA, Therapists
• Online education
Skills
• Skills lab
• Stop & Watch Tool; SBAR Tool
• Simulation learning / manikins, live
Ability/Attitude
• Safe environment
• Opportunity to Practice
45 45
Reducing Re-hospitalization – Evidence-based strategies
Risk Identification / Stratification Process (for return to hospital)
• Risk level identified on move in (ongoing)
• Current or recent / recurring infection
• History of Falling (w/ or w/o injury)
• Hospitalized in past 12 months
• 2-3 co-morbid conditions
• Community-specific …
INTERACT • Early Identification / STOP & WATCH
• Clinical Decision Support
• SBAR
Root Cause Analysis (Each hospitalization)

Ray Miller 8/18/2017
Direct Supply 20
46
INTERACT https://interact2.net/assisted_living.aspx
Endorsed by American Assisted
Living Nursing Association
“The advent and use of these
Assisted Living specific tools will
become a standard part of quality
improvement….AALNA sees this
system as an innovative approach to
improving communication by more
directly empowering our caregivers
and improving our relationships with
each other, residents, families and
physicians.”
47
Can be completed
by any caregiver

Ray Miller 8/18/2017
Direct Supply 21
50
Can be completed by
non-licensed
caregivers in assisted
living
51 51
What should caregivers be looking for? (heart failure)
• Shortness of breath
• Shortness of breath
when lying flat
• Shortness of breath
at night /cough
• Edema; Ascites
(swelling)
• Fatigue
• Confusion or
delirium
• Nausea, abdominal
pain or distension
• Decline in:
• Exercise tolerance
• Food intake
• Functional status

Ray Miller 8/18/2017
Direct Supply 22
53
Ideas
Applying
principles of
“Community
Health Nursing”
A team
approach to
chronic disease
management
Tips for
reducing re-
hospitalization
Tips for
reducing risks
associated with
frailty
54 54
1. RESIDENT: 70+ yrs. OR Significant, chronic, illness-related weight loss (>5%)
2. PHYSICIAN: “Screened for sarcopenia & frailty?” “Results?” (ICD-10 code M62.84)
3. BY WHO / WHEN: Therapy; move-in
4. HOW: SARC-F tool
5. FOCUS ON:
• Exercise (resistance AND aerobic)
• Caloric and protein support
• Reduced polypharmacy
• Vitamin D
Identifying Sarcopenia, Reducing Risk for Frailty
Morley, J., Vellas, B., et al. Frailty Consensus: A Call to Action. Journal of American Medical Directors Association. June 2013; 14(6): 392-397
*ORIGINALLY: “an age-associated loss of muscle mass …” RECENTLY: “… a decline
in muscle function (either walking speed or grip strength) associated with loss of muscle mass.”
https://www.researchgate.net/publication/243966215_SARC-F_A_Simple_Questionnaire_to_Rapidly_Diagnose_Sarcopenia *

Ray Miller 8/18/2017
Direct Supply 23
55 55
The “E” Word…
“A multi-component exercise intervention program…
of strength, endurance and balance training … best
strategy for: 1] improving gait, balance and strength
… 2] reducing the rate of falls in elderly individuals…
3] maintaining their functional capacity during aging”
Cadore, E.L., Rodriquez-Manas, L., Sinclair, A., Izquierdo, M. (2013). Effects of Different Exercise Interventions on Risk of Falls, Gait
Ability, and Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Research. Vol. 16, Number 2, 2013.
56 56
The “E” Word -- Exercise Plan
Cadore, E.L., Rodriquez-Manas, L., Sinclair, A., Izquierdo, M. (2013). Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and
Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Research. Vol. 16, Number 2, 2013.
Resistance Training • 2-3x / wk.; 3 sets of 8-12 reps
• 20-30% intensity and work-up (80%)
• Integrate into daily activities (e.g., sit to stand)
Endurance Training • Start at 5-10 mins first weeks; progress to 15-30 min
• Monitor Rate of Perceived Exertion (RPE) intensity (e.g.12-14 RPE)
• Walking (change pace & direction), step ups, stair climbing, stationary cycling
Balance Training • Integrate multiple exercises(e.g., multi-direction weight shift, heel-toe walking,
standing on one leg, weight transfers, line walking)
How can we
inspire the
desire to
exercise?
Ray Miller 8/18/2017
Direct Supply 24
57 57
Five Major Motivators
https://www.hindawi.com/journals/tswj/2014/329397/
Eighteen older residents from two nursing homes in Taiwan:
1. 8 participants: to enrich their lives
2. 7 participants: a previously cultivated habit
3. 6 participants: eagerness for returning home
4. 10 participants: fear of becoming totally dependent
5. 6 participants: improving mood state (avoiding / enhancing)
The Scientific World Journal, Volume 2014 (2014), Article ID 329397: Motivators for Physical Activity among Ambulatory Nursing Home Older Residents
“The motivators reported in this study should be considered when
designing physical activity programs. These motivators can be
used to encourage, guide, and provide feedback to support older
residents in maintaining physical activity.”
58 58
Reduce Fall & Injury Risk for Residents
• Consider programs to support transfer and lift assistance
• Evaluate residents for the level of support needed:
□ Level of dependence on care staff
□ Weight bearing ability
□ Cognitive status
□ Size of resident
• Evaluate on move-in, with change in condition and at least
every 6-12 months.
Ray Miller 8/18/2017
Direct Supply 25
59 59
Reduce Caregiver Injury Risk
1. Assessments: Functional, Posterior
2. Assisting from floor (post-fall)
3. Applying barrier creams
4. Bariatric Residents
5. Vehicle Transfer
6. Hygiene Care
7. Repositioning
8. Transfers
9. Dressing
10. Toileting
11. Weights
12. …
61 61
A “New” Discussion -- Assist Devices in Assisted Living
Readiness Assessment
1. Residents
2. Equipment
3. Culture
4. Management Engagement
5. Program Policy & Procedure
Successful Implementation
1. Mentors
2. Hands-on Training
3. R & S & M Buy--in
4. Sustained Change
5. Safety Committee monitors & modifies
S

Ray Miller 8/18/2017
Direct Supply 26
62
Applying ADLs to Equipment Selection (Assessment)
Category 4: Total Dependent:
□ Floor Lift
Category 3: Moderate / Extensive / Maximum Assist:
□ Sit-to-Stand Assist
□ Floor Lift
Category 2: Minimum Assist:
□ Non-powered assist devices
□ Sit-to-stand Assist
Category 1: Limited Assist
Category 0: Independent
Applying ADLs to Equipment Selection
63
CODE 4: Total Dependence
Full staff performance every time
CODE 3: Extensive Assistance
Resident involved in activity, staff
provide weight-bearing support
CODE 2: Limited Assistance
Resident highly involved in activity,
staff provide guided maneuvering of
limbs or other non-weight-bearing
support
CODE 0: Independent
No help or staff oversight at any time
This document is intended to provide general information but not advice about regulations and initiatives. This information is not and not intended as legal or other advice, and each situation may vary depending on the particular facts and circumstances. You should not
act upon this information without first consulting with qualified legal counsel.
Resident Capability &
Lift/Assist Equipment
Matching Options Based on industry best practices
and CMS RAI V 3.0 Section G
Multi-Functional
Lift
DRAFT DOCUMENT
Multi-Functional
Lift
Multi-Functional
Lift
CODE 1: Supervision
Oversight, encouragement
or cueing

Ray Miller 8/18/2017
Direct Supply 27
65
66

Ray Miller 8/18/2017
Direct Supply 28
69
RESOURCES
70 70
Capabilities / Products & Tools
Chronic Disease Management
• Scales
• BP cuffs, stethoscopes
• Vital signs monitor, pulse oximetry
• Resident education / Transitional Care Kits
Improving Endurance, Strength, Balance & Cognition
• Group classes
• Adding “fitness” in addition to rehab space
• In-apartment exercises, hand weights, resistance bands
• Adding equipment to assess & improve balance, cognition, endurance, strength
Reducing risk
• Fall injury / hip protection, adjustable height beds, lifts, grab bars etc;
• Exercise to improve balance, strength and endurance
• Lifts to reduce resident and staff injury

Ray Miller 8/18/2017
Direct Supply 29
72 72
Summary
• Consider implementing community health principles to guide
the develop of health and wellness programming
• Engage the entire team (both internal and external)
• Engage the Residents in their own care
• Invest in staff education (improved care & retention)
• Utilize your partners, resources, share best practices
73
Ideas
Applying
principles of
“Community
Health Nursing”
A team
approach to
chronic disease
management
Tips for
reducing re-
hospitalization
Tips for
reducing risks
associated with
frailty
Ray Miller 8/18/2017
Direct Supply 30
Liz Jen
sen
, R
N, M
SN
, R
N-B
C
Clin
ical D
irecto
r, D
irect Su
pp
ly®
, In
c.
Ray Miller, MSOSH, in a collaborative effort with
By Liz Jensen, RNA MSN, RN-BC
Clinical Director, Direct Supply®, Inc.
By Ray Miller, MSOSH, Dir. of Risk and Safety,
Direct Supply, in a collaborative effort
With Liz Jensen, RNA MSN, RN-BC
Clinical Director, Direct Supply®, Inc.
Thank You
For Your
Participation