Embed Size (px)
Citation preview
3/5/21
Leslie Russek; Clarkson 1
Hypermobility 101:An Introduction to Having Hypermobility or
Ehlers-Danlos Syndrome
Leslie N Russek, PT, DPT, PhD, OCSClarkson University, Canton-Potsdam Hospital, Potsdam, NY
Slide handouts are available at: https://webspace.clarkson.edu/~lrussek/hsd.html
1
DISCLAIMER
• I cannot provide individual medical advice in this presentation• The information provided here is generally applicable to HSD/hEDS,
but your personal situation may be different.• You should discuss options with your healthcare provider before
starting a new management approach.
Russek: Hypermobility 101 2
2
3/5/21
Leslie Russek; Clarkson 2
Learning ObjectivesAt the end of this session, participants will be able to:
1. Describe common signs and symptoms of hypermobility
2. Identify common comorbidities, such as Postural Orthostatic Tachycardia Syndrome (POTS) and Mast Cell Activation Syndrome (MCAS)
3. List reasons for common pain complaints, and what can be done to manage these problems
4. Identify several strategies for managing pain, once “issues with the tissues” have been addressed
Russek: Hypermobility 101 3
3
Hypermobility Lecture Series Schedule
• Friday 3/5/21: Hypermobility 101: Basics of HSD/hEDS and self-care
• Friday, 3/12/21: Hypermobility 102: POTS and POTS self-care, basics of MCAS
• Changed!: THURSDAY 3/18/21 : Hypermobility 103: Pain management in HSD/hEDS
• Tentatively 3/26/21: Hypermobility 104: Safe exercise selection and progression with
HSD/hEDS
• Tentatively 4/2/21: Hypermobility 105: HSD/hEDS in children and teens
• Tentatively 4/9/21: Hypermobility 106: Gut issues in HSD/hEDS, POTS, MCAS• Tentatively 4/16/21: Hypermobility 107: Fatigue in HSD/hEDS and POTS (NEW)
Russek: Hypermobility 101 4
4
3/5/21
Leslie Russek; Clarkson 3
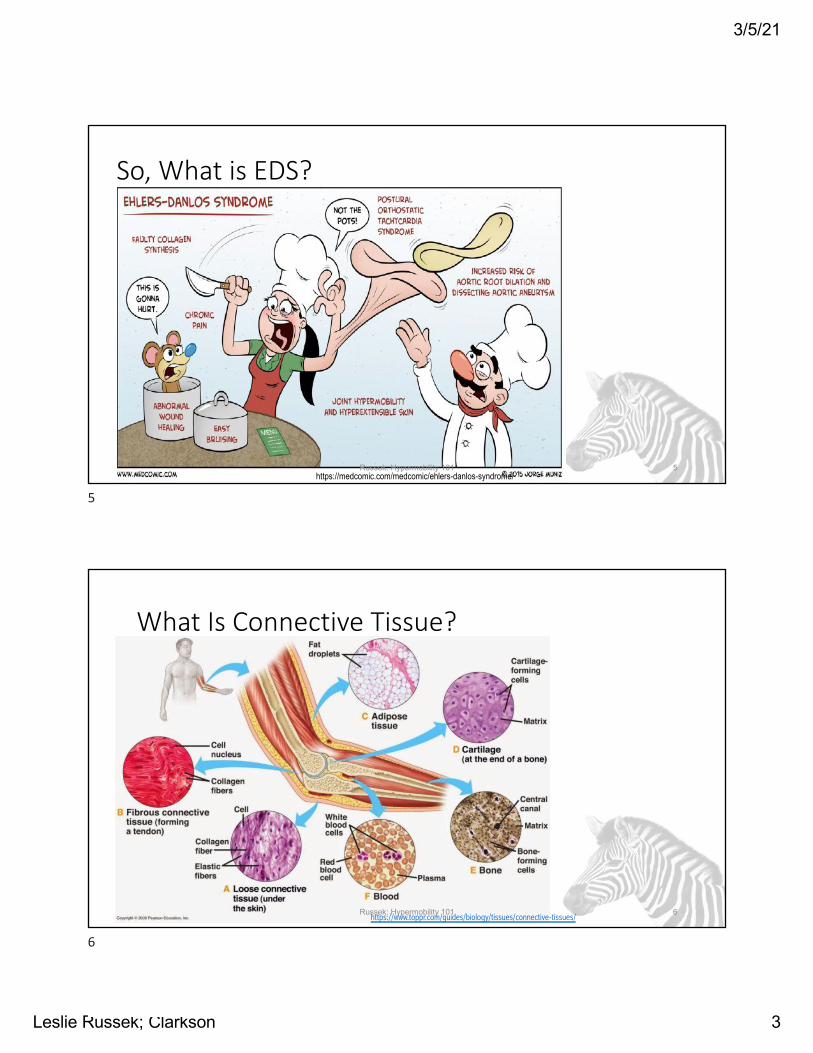
https://medcomic.com/medcomic/ehlers-danlos-syndrome/
So, What is EDS?
Russek: Hypermobility 101 5
5
What Is Connective Tissue?
Russek: Hypermobility 101 6https://www.toppr.com/guides/biology/tissues/connective-tissues/
6
3/5/21
Leslie Russek; Clarkson 4
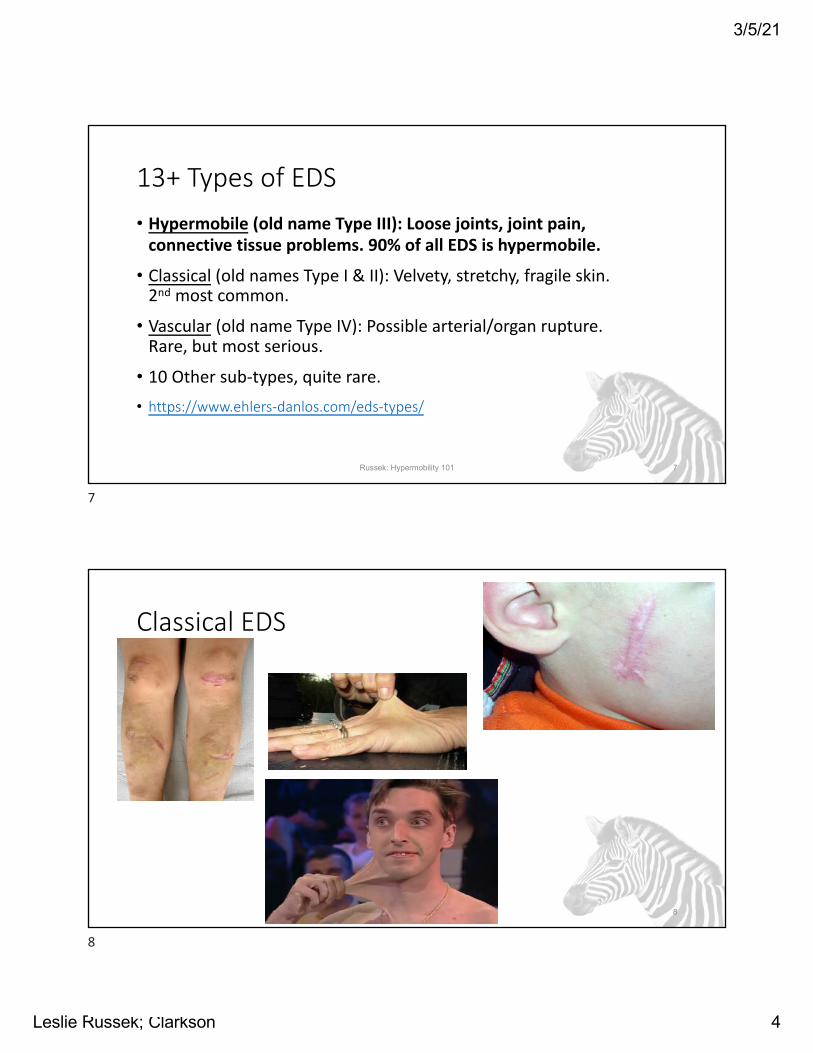
13+ Types of EDS• Hypermobile (old name Type III): Loose joints, joint pain,
connective tissue problems. 90% of all EDS is hypermobile.
• Classical (old names Type I & II): Velvety, stretchy, fragile skin. 2nd most common.
• Vascular (old name Type IV): Possible arterial/organ rupture. Rare, but most serious.
• 10 Other sub-types, quite rare.• https://www.ehlers-danlos.com/eds-types/
Russek: Hypermobility 101 7
7
Classical EDS
Russek: Hypermobility 101 8
8
3/5/21
Leslie Russek; Clarkson 5
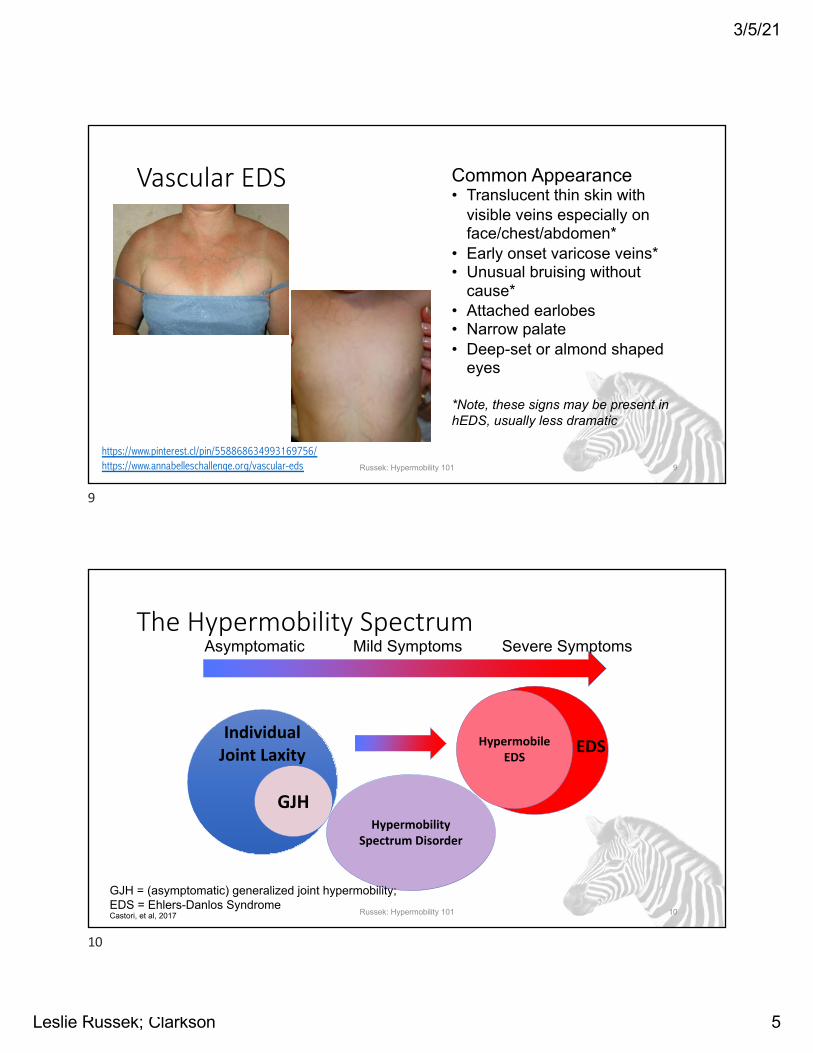
Vascular EDS
Russek: Hypermobility 101 9
https://www.pinterest.cl/pin/558868634993169756/https://www.annabelleschallenge.org/vascular-eds
Common Appearance• Translucent thin skin with
visible veins especially on face/chest/abdomen*
• Early onset varicose veins*• Unusual bruising without
cause*• Attached earlobes• Narrow palate• Deep-set or almond shaped
eyes
*Note, these signs may be present in hEDS, usually less dramatic
9
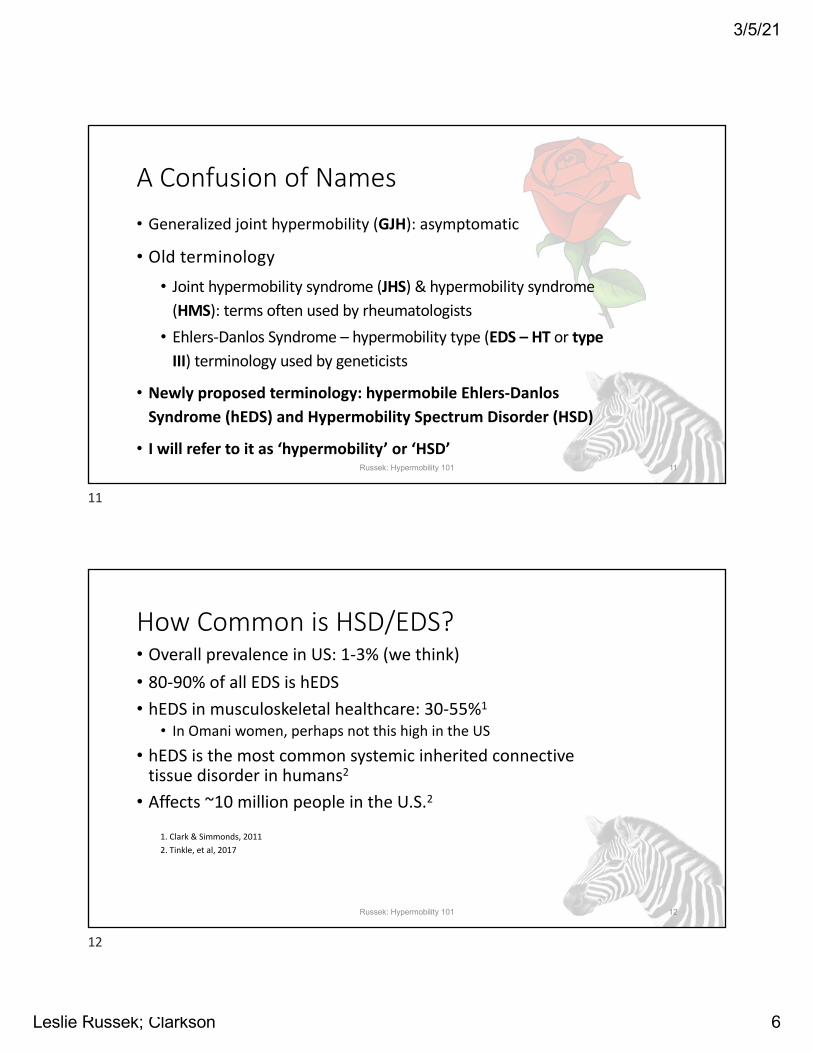
The Hypermobility Spectrum
Russek: Hypermobility 101 10
Individual Joint Laxity
GJH
Hypermobile EDS
Asymptomatic Mild Symptoms Severe Symptoms
GJH = (asymptomatic) generalized joint hypermobility; EDS = Ehlers-Danlos SyndromeCastori, et al, 2017
Hypermobility Spectrum Disorder
EDS
10
3/5/21
Leslie Russek; Clarkson 6
A Confusion of Names• Generalized joint hypermobility (GJH): asymptomatic
• Old terminology• Joint hypermobility syndrome (JHS) & hypermobility syndrome
(HMS): terms often used by rheumatologists• Ehlers-Danlos Syndrome – hypermobility type (EDS – HT or type
III) terminology used by geneticists
• Newly proposed terminology: hypermobile Ehlers-Danlos Syndrome (hEDS) and Hypermobility Spectrum Disorder (HSD)
• I will refer to it as ‘hypermobility’ or ‘HSD’Russek: Hypermobility 101 11
11
How Common is HSD/EDS?• Overall prevalence in US: 1-3% (we think)• 80-90% of all EDS is hEDS• hEDS in musculoskeletal healthcare: 30-55%1
• In Omani women, perhaps not this high in the US
• hEDS is the most common systemic inherited connective tissue disorder in humans2
• Affects ~10 million people in the U.S.2
1. Clark & Simmonds, 20112. Tinkle, et al, 2017
Russek: Hypermobility 101 12
12
3/5/21
Leslie Russek; Clarkson 7
Symptoms Through the Life Span1. Hypermobile phase
• Hypermobile joints• Clumsiness/motor delay• Constipation/diarrhea• Abdominal hernias
2. Pain phase• Chronic fatigue• Unrefreshing sleep• Chronic back pain• Chronic muscle
pain/cramps• Strains, sprains• Dislocations• Anxiety
3. Pain + phase• Memory/cognitive
problems• Gastric reflux• Recurrent abdominal pain• Numbness & tingling• Racing heart• Incontinence/UTI
4. Stiffness phase• Tendonosis/tendon rupture• Chronic gastritis• Stiffness
• Castori et al, 2011• Tinkle et al, 2017
Russek: Hypermobility 101 13
13
CRITERION 1 – Generalized Joint HypermobilityOne of the following selected:
� ≥6 pre-pubertal children and adolescents � ≥5 pubertal men and woman to age 50 Beighton Score: /9 � ≥4 men and women over the age of 50
If Beighton Score is one point below age- and sex-speci"c cut o#, two or more of the following must also be selected to meet criterion: � Can you now (or could you ever) place your hands $at on the $oor without bending your knees? � Can you now (or could you ever) bend your thumb to touch your forearm? � As a child, did you amuse your friends by contorting your body into strange shapes or could you do the splits? � As a child or teenager, did your shoulder or kneecap dislocate on more than one occasion? � Do you consider yourself “double jointed”?
CRITERION 2 – Two or more of the following features (A, B, or C) must be presentFeature A ("ve must be present)
� Unusually so% or velvety skin � Mild skin hyperextensibility � Unexplained striae distensae or rubae at the back, groins, thighs, breasts and/or abdomen in adolescents, men or pre-pubertal women
without a history of signi"cant gain or loss of body fat or weight � Bilateral piezogenic papules of the heel � Recurrent or multiple abdominal hernia(s) � Atrophic scarring involving at least two sites and without the formation of truly papyraceous and/or hemosideric scars as seen in classical EDS � Pelvic $oor, rectal, and/or uterine prolapse in children, men or nulliparous women without a history of morbid obesity or other known
predisposing medical condition � Dental crowding and high or narrow palate � Arachnodactyly, as de"ned in one or more of the following:
(i) positive wrist sign (Walker sign) on both sides, (ii) positive thumb sign (Steinberg sign) on both sides � Arm span-to-height ratio ≥1.05 � Mitral valve prolapse (MVP) mild or greater based on strict echocardiographic criteria � Aortic root dilatation with Z-score >+2
Feature A total: /12
Feature B � Positive family history; one or more "rst-degree relatives independently meeting the current criteria for hEDS
Feature C (must have at least one) � Musculoskeletal pain in two or more limbs, recurring daily for at least 3 months � Chronic, widespread pain for ≥3 months � Recurrent joint dislocations or frank joint instability, in the absence of trauma
CRITERION 3 - All of the following prerequisites MUST be met1. Absence of unusual skin fragility, which should prompt consideration of other types of EDS
2. Exclusion of other heritable and acquired connective tissue disorders, including autoimmune rheumatologic conditions. In patients with an acquired CTD (e.g. Lupus, Rheumatoid Arthritis, etc.), additional diagnosis of hEDS requires meeting both Features A and B of Criterion 2. Feature C of Criterion 2 (chronic pain and/or instability) cannot be counted toward a diagnosis of hEDS in this situation.
3. Exclusion of alternative diagnoses that may also include joint hypermobility by means of hypotonia and/or connective tissue laxity. Alternative diagnoses and diagnostic categories include, but are not limited to, neuromuscular disorders (e.g. Bethlem myopathy), other hereditary disorders of the connective tissue (e.g. other types of EDS, Loeys-Dietz syndrome, Marfan syndrome), and skeletal dysplasias (e.g. osteogenesis imperfecta). Exclusion of these considerations may be based upon history, physical examination, and/or molecular genetic testing, as indicated.
Diagnosis:
Diagnostic Criteria for Hypermobile Ehlers-Danlos Syndrome (hEDS)This diagnostic checklist is for doctors across
all disciplines to be able to diagnose EDS
Patient name:
Distributed by
The clinical diagnosis of hypermobile EDS needs the simultaneous presence of all criteria, 1 and 2 and 3.
DOB: DOV: Evaluator:
v9
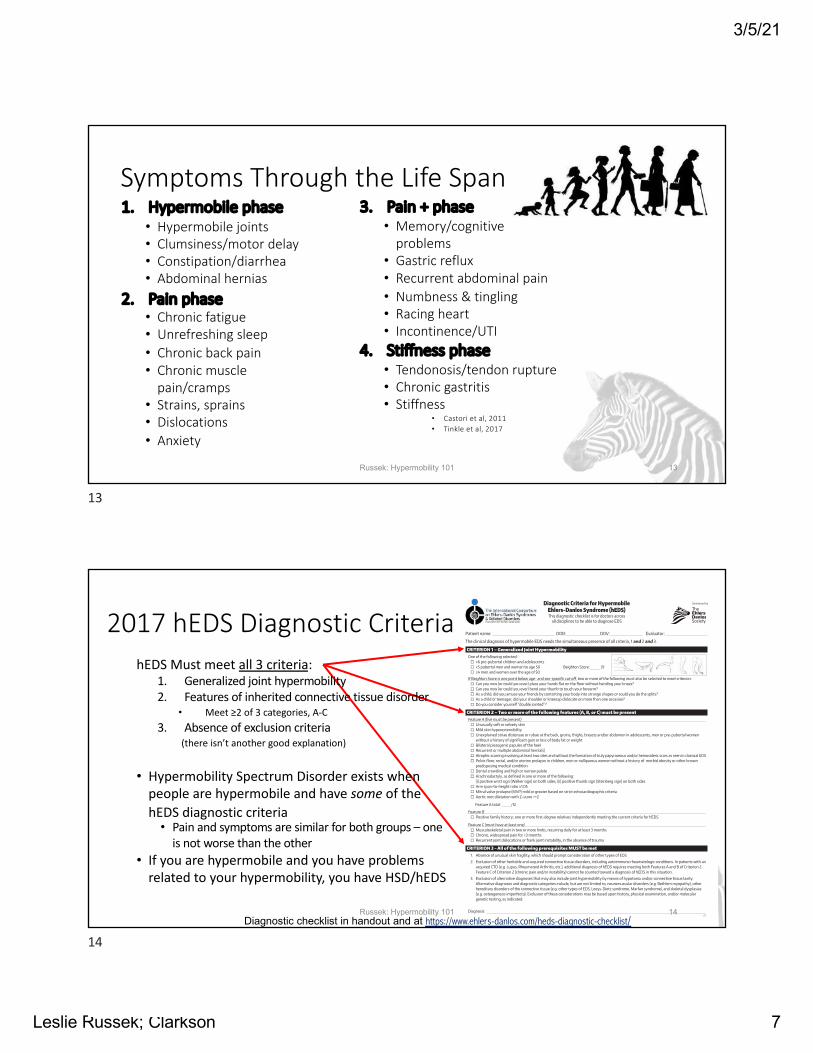
2017 hEDS Diagnostic CriteriahEDS Must meet all 3 criteria:
1. Generalized joint hypermobility2. Features of inherited connective tissue disorder
• Meet ≥2 of 3 categories, A-C3. Absence of exclusion criteria
(there isn’t another good explanation)
• Hypermobility Spectrum Disorder exists when people are hypermobile and have some of the hEDS diagnostic criteria• Pain and symptoms are similar for both groups – one
is not worse than the other• If you are hypermobile and you have problems
related to your hypermobility, you have HSD/hEDS
Russek: Hypermobility 101 14Diagnostic checklist in handout and at https://www.ehlers-danlos.com/heds-diagnostic-checklist/
14
3/5/21
Leslie Russek; Clarkson 8
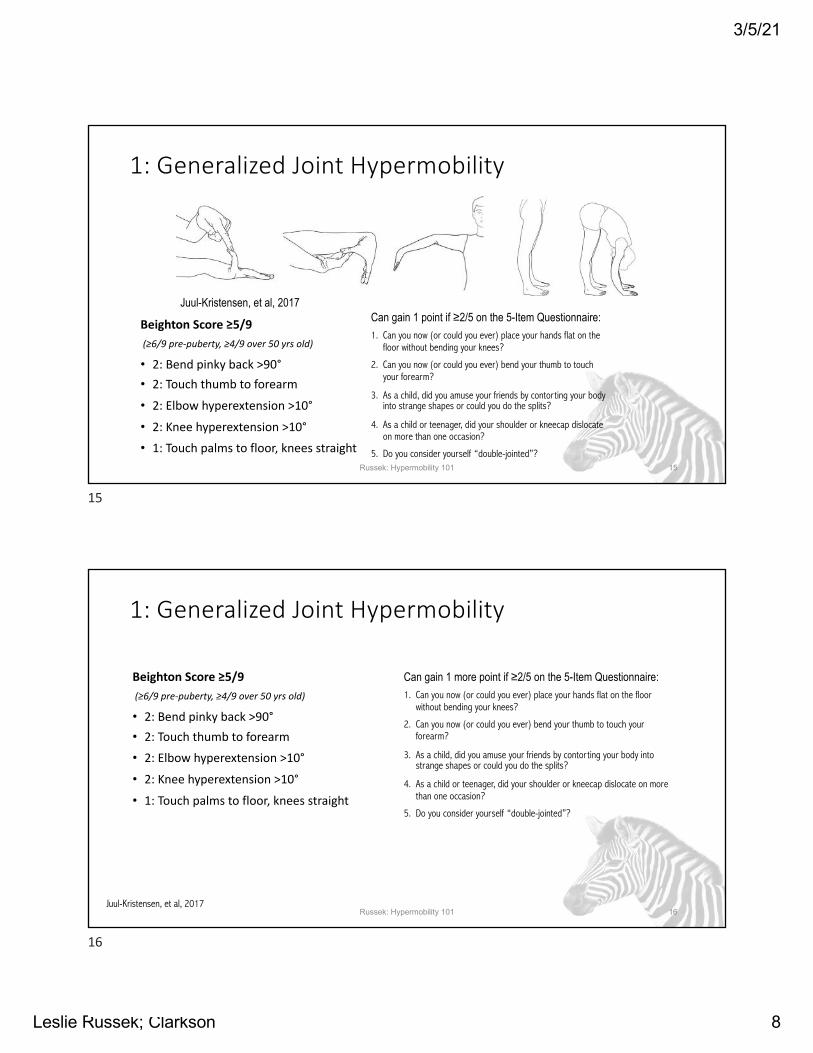
1: Generalized Joint Hypermobility
Beighton Score ≥5/9 (≥6/9 pre-puberty, ≥4/9 over 50 yrs old)
• 2: Bend pinky back >90°• 2: Touch thumb to forearm
• 2: Elbow hyperextension >10°
• 2: Knee hyperextension >10°
• 1: Touch palms to floor, knees straight
Can gain 1 point if ≥2/5 on the 5-Item Questionnaire:1. Can you now (or could you ever) place your hands flat on the
floor without bending your knees?
2. Can you now (or could you ever) bend your thumb to touch your forearm?
3. As a child, did you amuse your friends by contorting your body into strange shapes or could you do the splits?
4. As a child or teenager, did your shoulder or kneecap dislocate on more than one occasion?
5. Do you consider yourself “double-jointed”?Russek: Hypermobility 101 15
Juul-Kristensen, et al, 2017
15
1: Generalized Joint Hypermobility
Beighton Score ≥5/9 (≥6/9 pre-puberty, ≥4/9 over 50 yrs old)
• 2: Bend pinky back >90°• 2: Touch thumb to forearm
• 2: Elbow hyperextension >10°
• 2: Knee hyperextension >10°
• 1: Touch palms to floor, knees straight
Can gain 1 more point if ≥2/5 on the 5-Item Questionnaire:1. Can you now (or could you ever) place your hands flat on the floor
without bending your knees?
2. Can you now (or could you ever) bend your thumb to touch your forearm?
3. As a child, did you amuse your friends by contorting your body into strange shapes or could you do the splits?
4. As a child or teenager, did your shoulder or kneecap dislocate on more than one occasion?
5. Do you consider yourself “double-jointed”?
Russek: Hypermobility 101 16Juul-Kristensen, et al, 2017
16
3/5/21
Leslie Russek; Clarkson 9
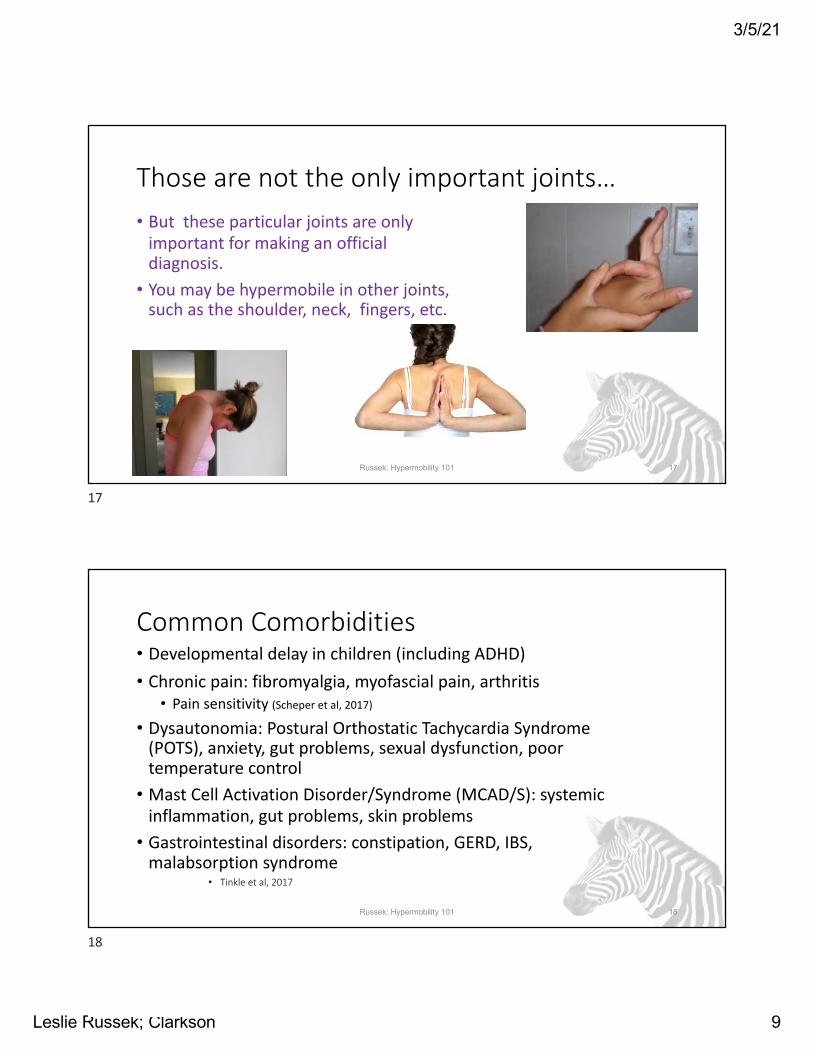
Those are not the only important joints…• But these particular joints are only
important for making an official diagnosis.
• You may be hypermobile in other joints, such as the shoulder, neck, fingers, etc.
Russek: Hypermobility 101 17
17
Common Comorbidities• Developmental delay in children (including ADHD)• Chronic pain: fibromyalgia, myofascial pain, arthritis
• Pain sensitivity (Scheper et al, 2017)
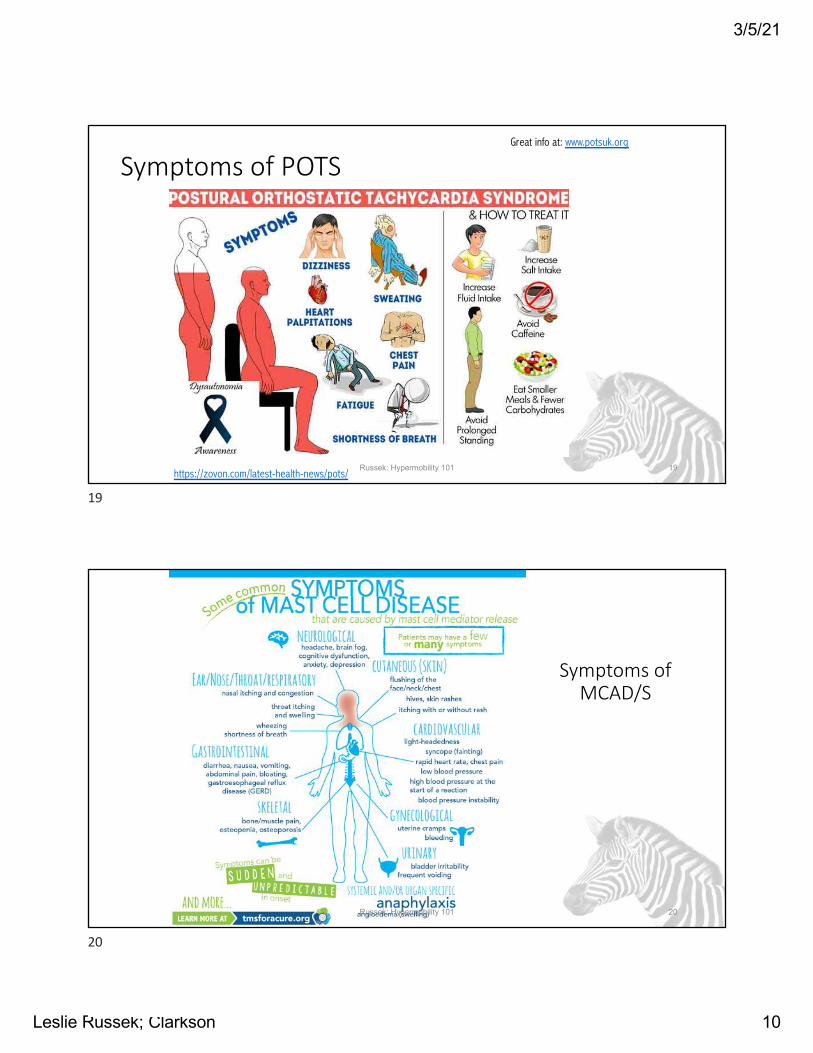
• Dysautonomia: Postural Orthostatic Tachycardia Syndrome(POTS), anxiety, gut problems, sexual dysfunction, poor temperature control
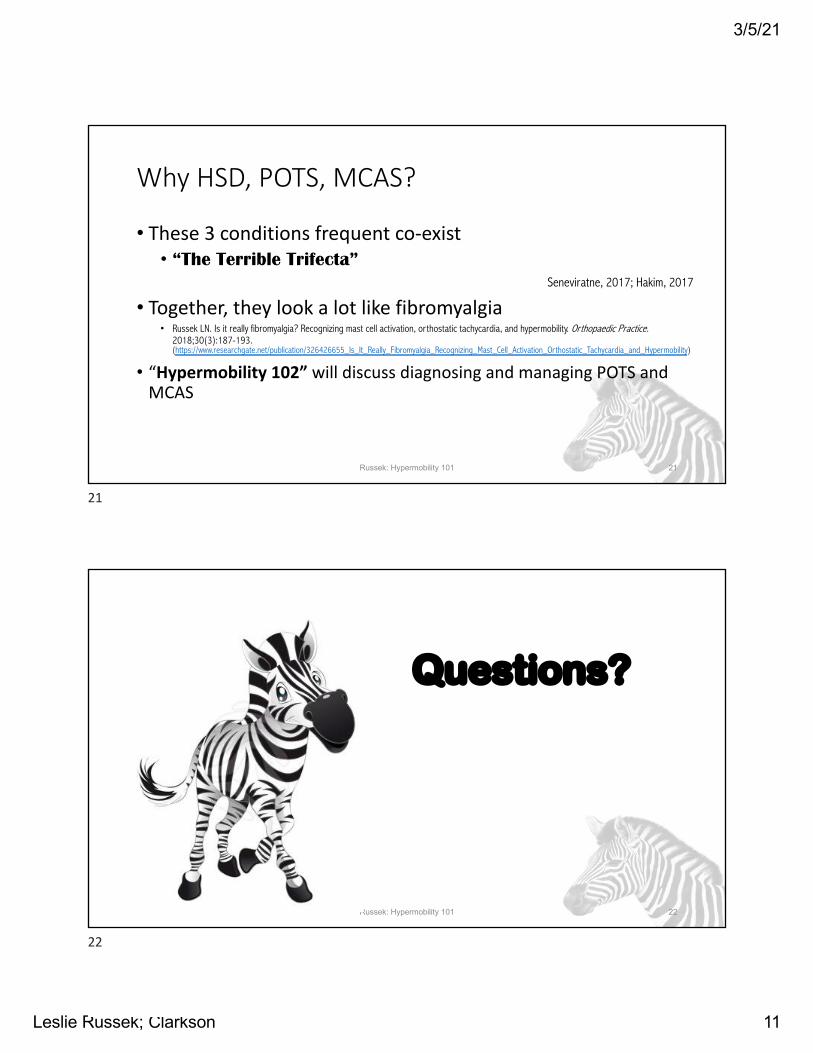
• Mast Cell Activation Disorder/Syndrome (MCAD/S): systemic inflammation, gut problems, skin problems
• Gastrointestinal disorders: constipation, GERD, IBS, malabsorption syndrome
• Tinkle et al, 2017
Russek: Hypermobility 101 18
18
3/5/21
Leslie Russek; Clarkson 10
Symptoms of POTS
Russek: Hypermobility 101 19https://zovon.com/latest-health-news/pots/
Great info at: www.potsuk.org
19
Symptoms of MCAD/S
Russek: Hypermobility 101 20
20
3/5/21
Leslie Russek; Clarkson 11
Why HSD, POTS, MCAS?
• These 3 conditions frequent co-exist• “The Terrible Trifecta”
Seneviratne, 2017; Hakim, 2017
• Together, they look a lot like fibromyalgia• Russek LN. Is it really fibromyalgia? Recognizing mast cell activation, orthostatic tachycardia, and hypermobility. Orthopaedic Practice.
2018;30(3):187-193. (https://www.researchgate.net/publication/326426655_Is_It_Really_Fibromyalgia_Recognizing_Mast_Cell_Activation_Orthostatic_Tachycardia_and_Hypermobility)
• “Hypermobility 102” will discuss diagnosing and managing POTS and MCAS
Russek: Hypermobility 101 21
21
Questions?
Russek: Hypermobility 101 22
22
3/5/21
Leslie Russek; Clarkson 12
Common Complaints and Why They Occur
Russek: Hypermobility 101 23
23
Musculoskeletal Problems in EDS• Being hypermobile, alone, does not necessarily
cause pain • There are many people who are hypermobile and pain
free• HOWEVER… being hypermobile makes you more
vulnerable to musculoskeletal imbalances that cause pain & instability• Ligaments are loose
• Joints slip out of alignment, or gravity pulls them out• Tight muscles pull loose joints out of alignment
• Body awareness (proprioception) is decreased• Muscles have often become weak
• Better understanding can help you become less vulnerable, and have less pain and instability
Russek: Hypermobility 101 24
24
3/5/21
Leslie Russek; Clarkson 13
Examples: Common Problems
• Ankle: Traumatic ankle sprain• Knee: Patellofemoral knee pain• Hips: Trochanteric pain syndrome (aka “bursitis”)• Spine: Muscle spasm • Shoulder: Instability/subluxation/dislocation• Neck: Trigger points pain• Hands: Joint instability• Nerve problems
Russek: Hypermobility 101 25
25
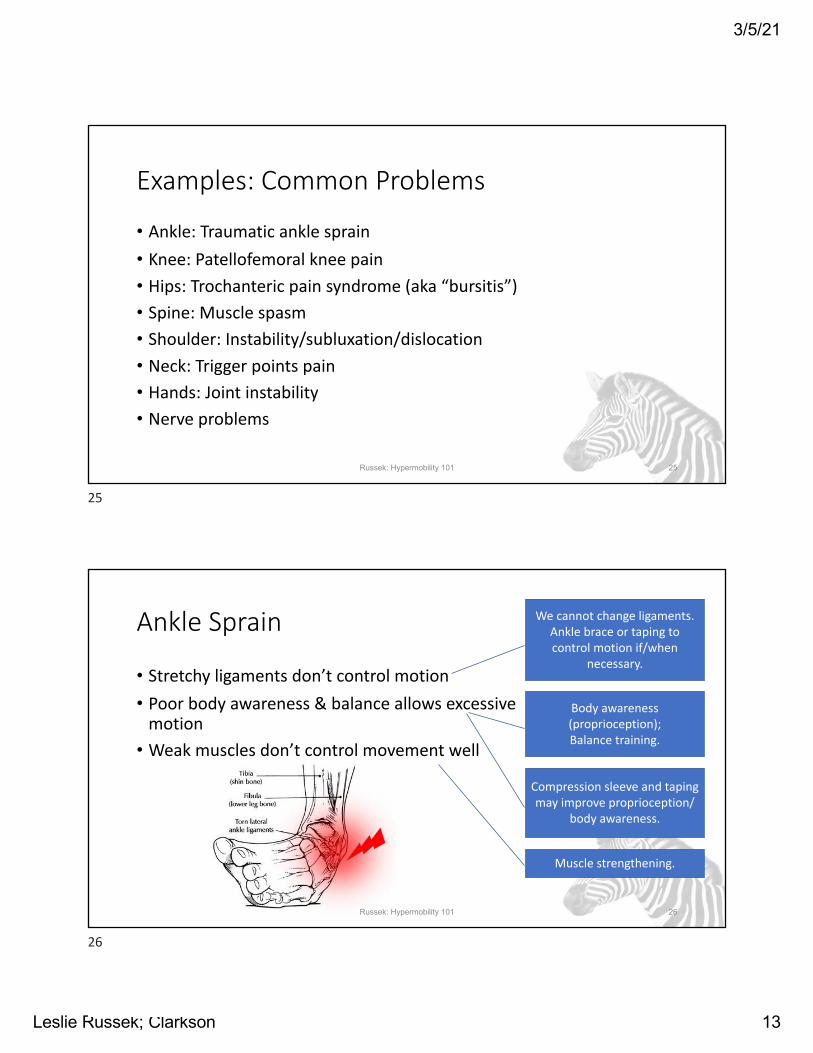
Ankle Sprain
• Stretchy ligaments don’t control motion• Poor body awareness & balance allows excessive
motion• Weak muscles don’t control movement well
We cannot change ligaments.Ankle brace or taping to control motion if/when
necessary.
Body awareness (proprioception);Balance training.
Compression sleeve and taping may improve proprioception/
body awareness.
Russek: Hypermobility 101 26
Muscle strengthening.
26
3/5/21
Leslie Russek; Clarkson 14
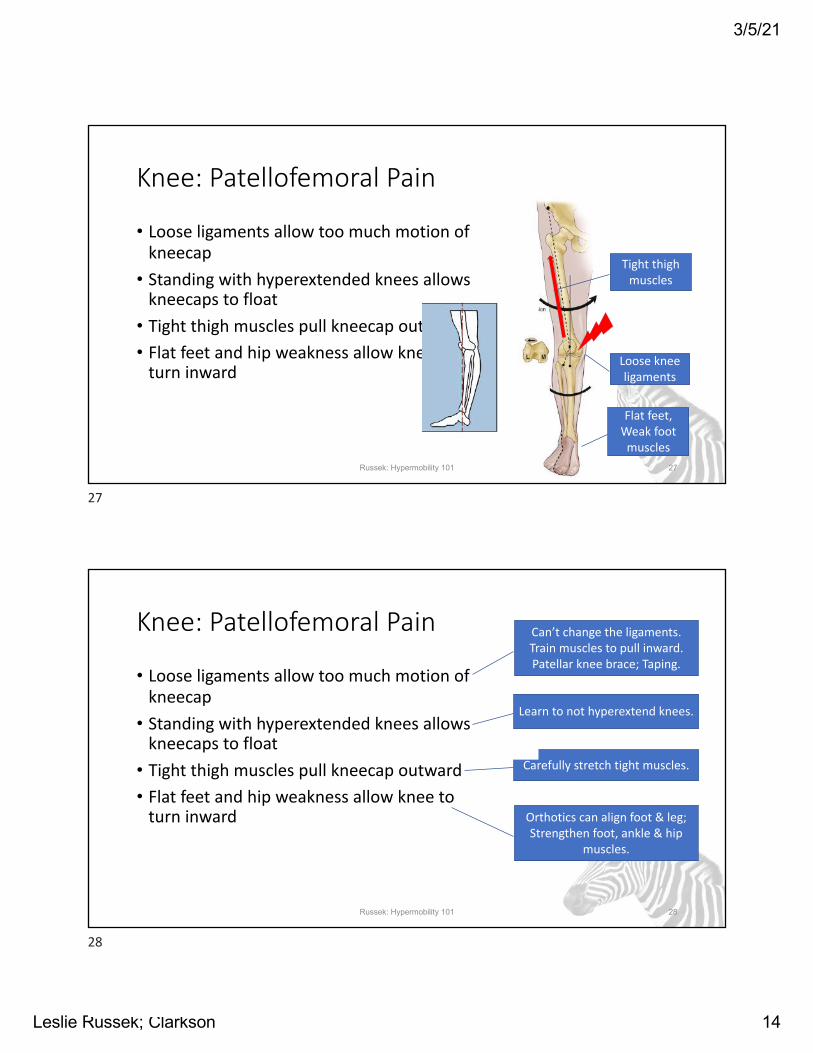
Knee: Patellofemoral Pain
• Loose ligaments allow too much motion of kneecap
• Standing with hyperextended knees allows kneecaps to float
• Tight thigh muscles pull kneecap outward• Flat feet and hip weakness allow knee to
turn inwardLoose knee ligaments
Tight thigh muscles
Flat feet,Weak foot
musclesRussek: Hypermobility 101 27
27
Knee: Patellofemoral Pain
• Loose ligaments allow too much motion of kneecap
• Standing with hyperextended knees allows kneecaps to float
• Tight thigh muscles pull kneecap outward• Flat feet and hip weakness allow knee to
turn inward
Can’t change the ligaments.Train muscles to pull inward.Patellar knee brace; Taping.
Carefully stretch tight muscles.
Orthotics can align foot & leg;Strengthen foot, ankle & hip
muscles.
Learn to not hyperextend knees.
Russek: Hypermobility 101 28
28
3/5/21
Leslie Russek; Clarkson 15
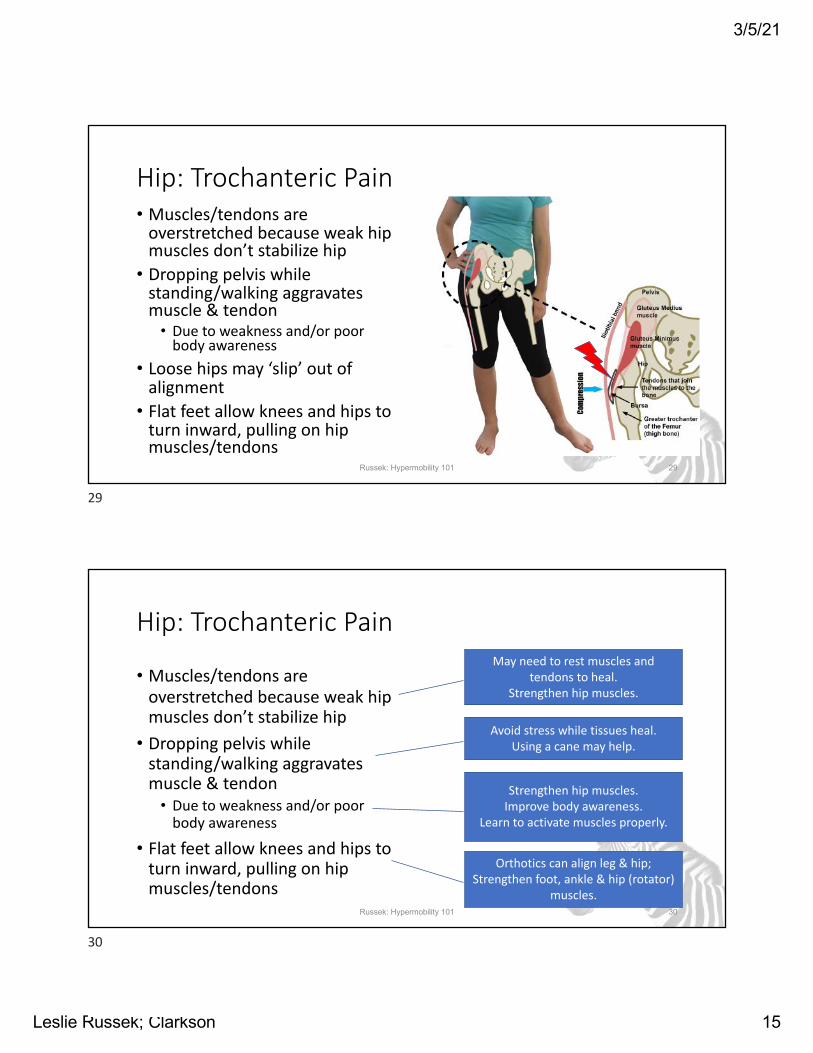
Hip: Trochanteric Pain• Muscles/tendons are
overstretched because weak hip muscles don’t stabilize hip
• Dropping pelvis while standing/walking aggravates muscle & tendon
• Due to weakness and/or poor body awareness
• Loose hips may ‘slip’ out of alignment
• Flat feet allow knees and hips to turn inward, pulling on hip muscles/tendons
Russek: Hypermobility 101 29
29
Hip: Trochanteric Pain
• Muscles/tendons are overstretched because weak hip muscles don’t stabilize hip
• Dropping pelvis while standing/walking aggravates muscle & tendon
• Due to weakness and/or poor body awareness
• Flat feet allow knees and hips to turn inward, pulling on hip muscles/tendons
May need to rest muscles and tendons to heal.
Strengthen hip muscles.
Strengthen hip muscles.Improve body awareness.
Learn to activate muscles properly.
Orthotics can align leg & hip;Strengthen foot, ankle & hip (rotator)
muscles.
Avoid stress while tissues heal.Using a cane may help.
Russek: Hypermobility 101 30
30
3/5/21
Leslie Russek; Clarkson 16
Low Back: Spasm
• Muscles tense to brace unstable spine • Poor body awareness leads to using
improper muscles or overusing proper muscles
• Using wrong muscles to breathe increases muscle tension
• Pain and fear of moving increases muscle spasm
Picture from https://www.spineuniverse.com/conditions/back-pain/muscle-spasms-leading-cause-back-pain-not-primary-cause
Russek: Hypermobility 101 31
31
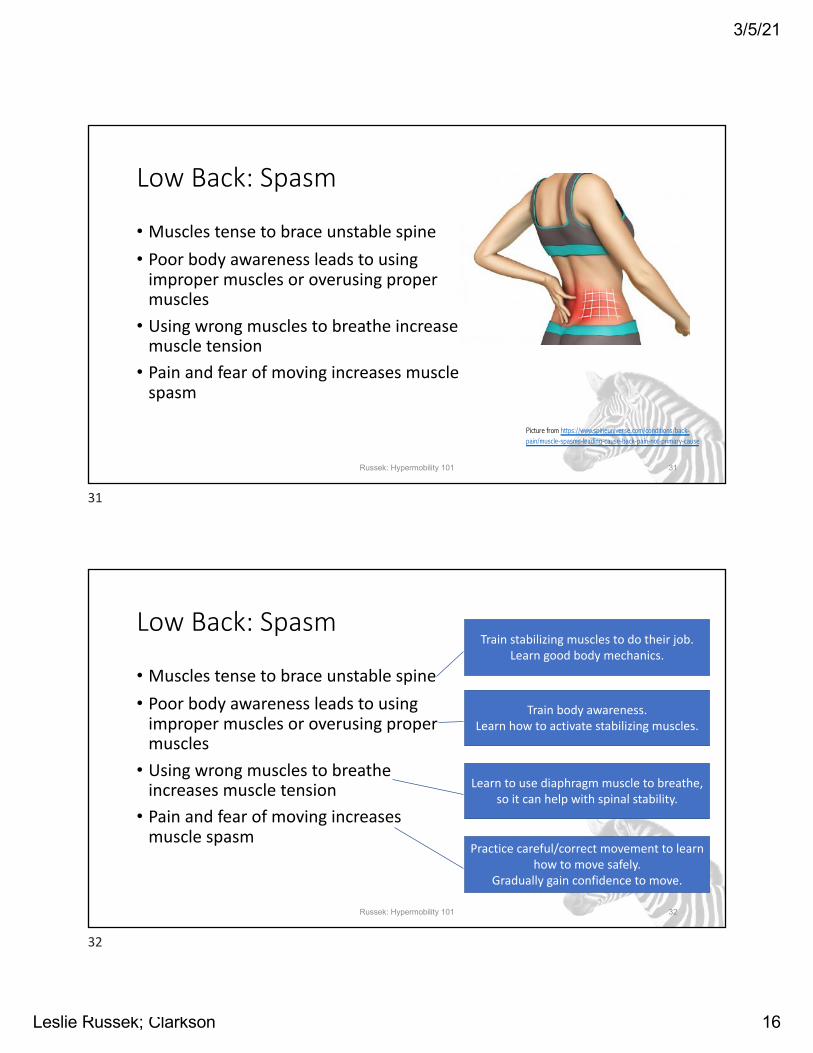
Low Back: Spasm
• Muscles tense to brace unstable spine • Poor body awareness leads to using
improper muscles or overusing proper muscles
• Using wrong muscles to breathe increases muscle tension
• Pain and fear of moving increases muscle spasm
Russek: Hypermobility 101 32
Train stabilizing muscles to do their job.Learn good body mechanics.
Train body awareness. Learn how to activate stabilizing muscles.
Learn to use diaphragm muscle to breathe, so it can help with spinal stability.
Practice careful/correct movement to learn how to move safely.
Gradually gain confidence to move.
32
3/5/21
Leslie Russek; Clarkson 17
Shoulder Instability
• Loose ligaments allow too much movement
• Weak muscles don’t hold shoulder in its proper place
• Poor body awareness allows excess motion
• Poor motor control allows shoulder to slip
• Poor alignment of the shoulder leads to subluxation
Russek: Hypermobility 101 33
Normal shoulder Unstable shoulder
Picture from: https://orthop.washington.edu/patient-care/articles/shoulder/atraumatic-shoulder-instability.html
33
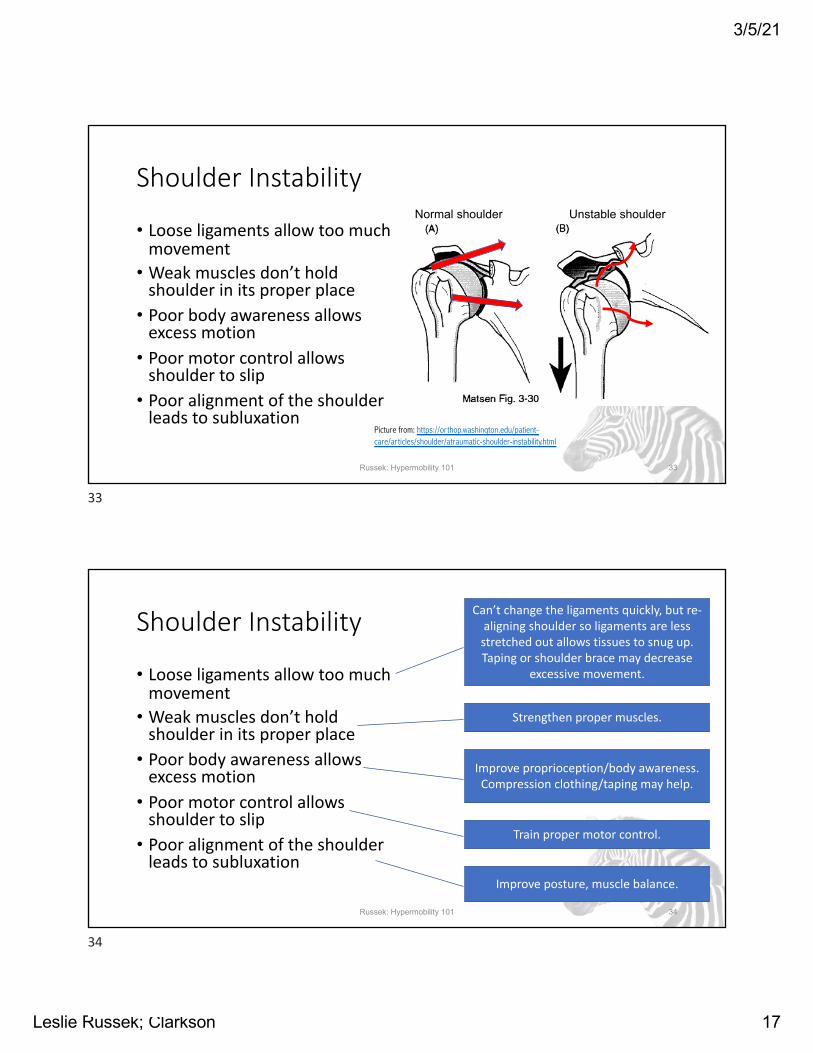
Shoulder Instability
• Loose ligaments allow too much movement
• Weak muscles don’t hold shoulder in its proper place
• Poor body awareness allows excess motion
• Poor motor control allows shoulder to slip
• Poor alignment of the shoulder leads to subluxation
Russek: Hypermobility 101 34
Can’t change the ligaments quickly, but re-aligning shoulder so ligaments are less stretched out allows tissues to snug up. Taping or shoulder brace may decrease
excessive movement.
Strengthen proper muscles.
Improve proprioception/body awareness. Compression clothing/taping may help.
Train proper motor control.
Improve posture, muscle balance.
34
3/5/21
Leslie Russek; Clarkson 18
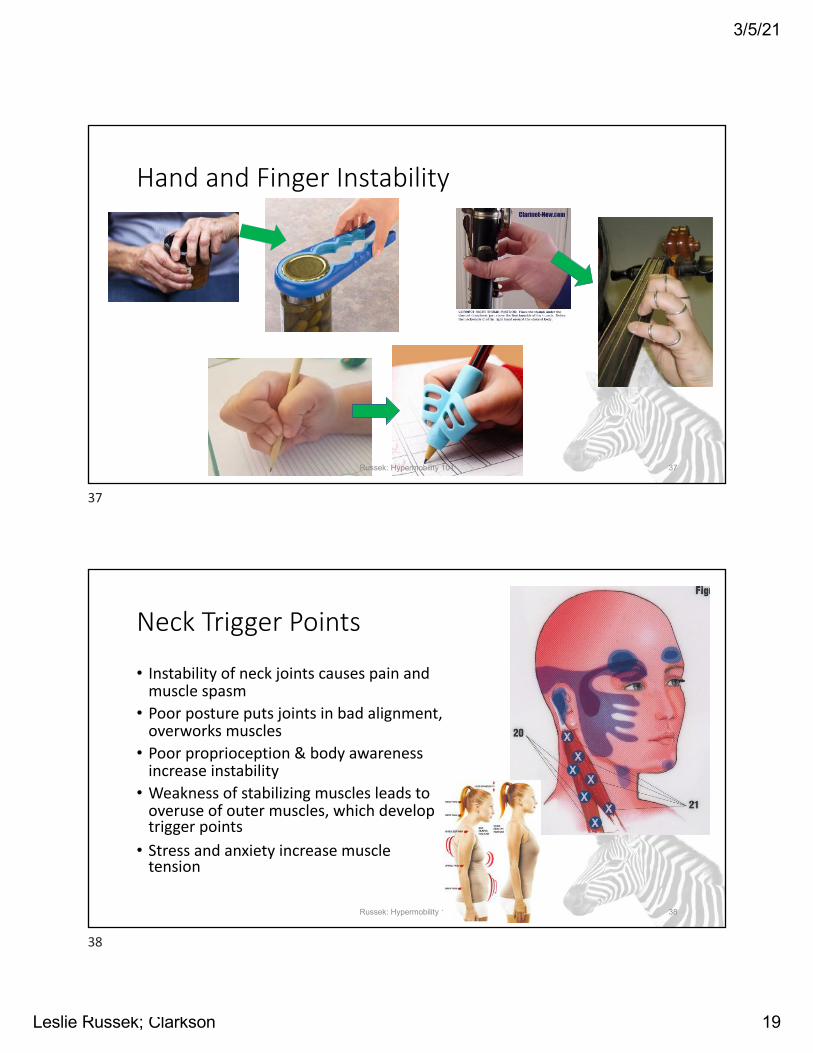
Hand and Finger Instability
• Loose ligaments allow too much movement and movement in wrong directions
• Stress on joints due to use• Using too much force because of
laxity or poor body awareness• Overuse of finger muscles
causes trigger points
Russek: Hypermobility 101 35
35
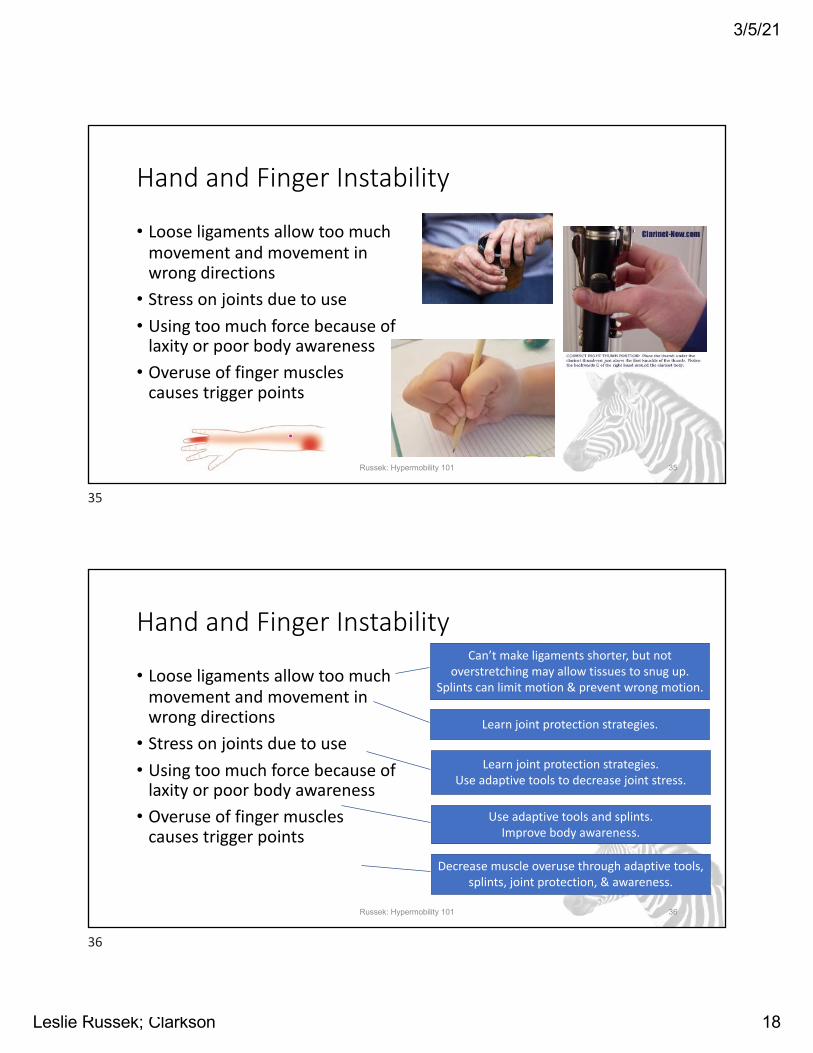
Hand and Finger Instability
• Loose ligaments allow too much movement and movement in wrong directions
• Stress on joints due to use• Using too much force because of
laxity or poor body awareness• Overuse of finger muscles
causes trigger points
Russek: Hypermobility 101 36
Can’t make ligaments shorter, but not overstretching may allow tissues to snug up.
Splints can limit motion & prevent wrong motion.
Learn joint protection strategies.
Learn joint protection strategies.Use adaptive tools to decrease joint stress.
Use adaptive tools and splints.Improve body awareness.
Decrease muscle overuse through adaptive tools, splints, joint protection, & awareness.
36
3/5/21
Leslie Russek; Clarkson 19
Hand and Finger Instability
Russek: Hypermobility 101 37
37
Neck Trigger Points
• Instability of neck joints causes pain and muscle spasm
• Poor posture puts joints in bad alignment, overworks muscles
• Poor proprioception & body awareness increase instability
• Weakness of stabilizing muscles leads to overuse of outer muscles, which develop trigger points
• Stress and anxiety increase muscle tension
Russek: Hypermobility 101 38
38
3/5/21
Leslie Russek; Clarkson 20
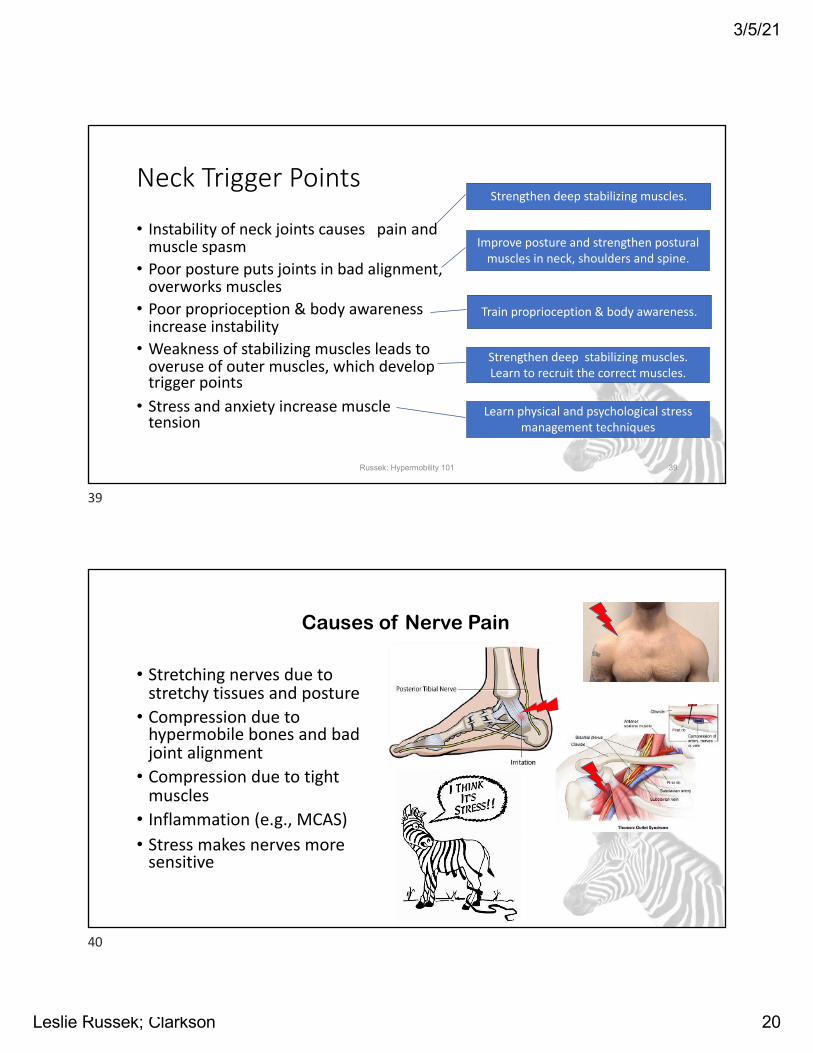
Neck Trigger Points
• Instability of neck joints causes pain and muscle spasm
• Poor posture puts joints in bad alignment, overworks muscles
• Poor proprioception & body awareness increase instability
• Weakness of stabilizing muscles leads to overuse of outer muscles, which develop trigger points
• Stress and anxiety increase muscle tension
Russek: Hypermobility 101 39
Strengthen deep stabilizing muscles.
Train proprioception & body awareness.
Strengthen deep stabilizing muscles.Learn to recruit the correct muscles.
Improve posture and strengthen postural muscles in neck, shoulders and spine.
Learn physical and psychological stress management techniques
39
40
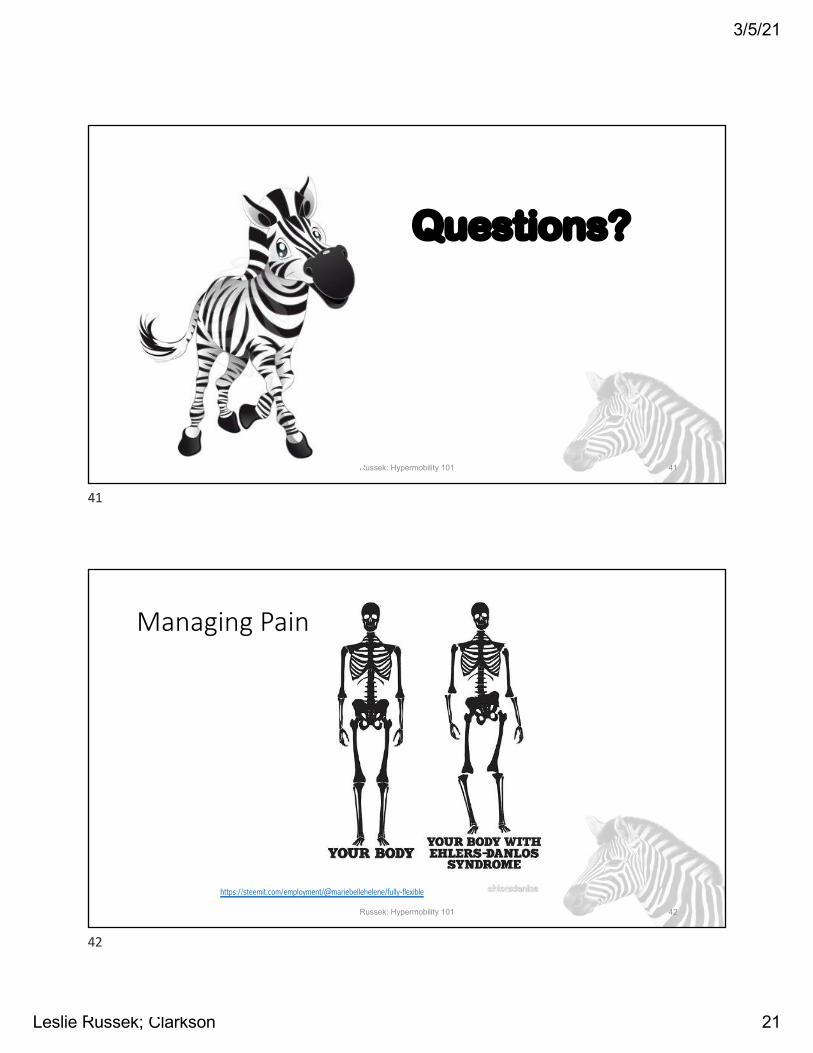
• Stretching nerves due to stretchy tissues and posture
• Compression due to hypermobile bones and bad joint alignment
• Compression due to tight muscles
• Inflammation (e.g., MCAS)• Stress makes nerves more
sensitive
Causes of Nerve Pain
40
3/5/21
Leslie Russek; Clarkson 21
Questions?
Russek: Hypermobility 101 41
41
Managing Pain
Russek: Hypermobility 101 42
https://steemit.com/employment/@mariebellehelene/fully-flexible
42
3/5/21
Leslie Russek; Clarkson 22
General Self-Care and Wellness• Sleep hygiene• Fatigue management• POTS self-management• Diet and gastrointestinal wellness• Psychological & social wellness• Body mechanics/ergonomics
• Braces & splints
• Pacing, prioritization, activity/exercise selection• Appropriate exercise/activity
Russek: Hypermobility 101 43
43
Pain Management: Tissues
• Fix the “Issues with your tissues”!• EDS pain is not ‘all in your head’
• Many types of chronic pain are known to continue after tissues have healed
• HOWEVER, in EDS, stress on tissues is persistent, so tissues often don’t heal.• EDS has “persistent pain,” which is different from
“chronic pain.”• Your neural processing of pain may be amplified
(typical of chronic pain), but that is not the only problem.• Psychological pain management can sometimes help, but
won’t fix “issues with your tissues”Russek: Hypermobility 101 44
44
3/5/21
Leslie Russek; Clarkson 23
FYI: Visceral Referred Pain “Issues”• Visceral tissues (internal organs) can
refer pain• Pain referral can irritate tissues at the
referral site • This can cause tissue irritation at the
referral site• Example: intestinal problems can
cause trigger points in abdominal muscles, which then hurt
• Gebhart, 2016
Russek: Hypermobility 101 45
45
Pain Management: Interventions
• Controlling pain, once you have managed “issues with your tissues”…• Modalities:
• Ice for joint inflammation and severe muscle spasm• Heat for muscle achiness and mild spasm• TENS to decrease pain in muscles or joints
• Topical ointments• Mentholated, anti-inflammatory, (capsaicin)
• Manual therapy• For muscle or fascial pain and restrictions• To improve joint alignment
• Managing neuroplasticity…Russek: Hypermobility 101 46
AKA: Electromassager
46
3/5/21
Leslie Russek; Clarkson 24
Benefits of Exercise/Activity
• Regular (appropriate) exercise/activity reduces pain• Protects against chronic pain onset • Sedentary lifestyle increases risk of chronic pain
• Protects against autonomic dysfunction (POTS)• Improves function• Improves sleep quality, decreases fatigue• Mind-body practice, such as Pilates, yoga, Tai Chi enhance
body awareness and relaxation• Improves mood, decreases anxiety• Decreases systemic inflammation
Russek: Hypermobility 101 47
Lima et al, 2017Sabharwal, 2016Ambrose, 2015
47
Not All Exercises Are Appropriate• For exercise to be helpful and not harmful, it must be:• The correct exercise (for you, now)• Done correctly (proper motor control)• At the correct dose (intensity, time/reps)• Not overstressing other joints or muscles
• There is no protocol appropriate for everyone with EDS/HSD
• Avoid:• Positions that overstretch joints• High impact sports/activities• Sudden head-up postural change• Excessive weight lifting/carrying, joint distraction
• Start low, go slow!Russek: Hypermobility 101 48
48
3/5/21
Leslie Russek; Clarkson 25
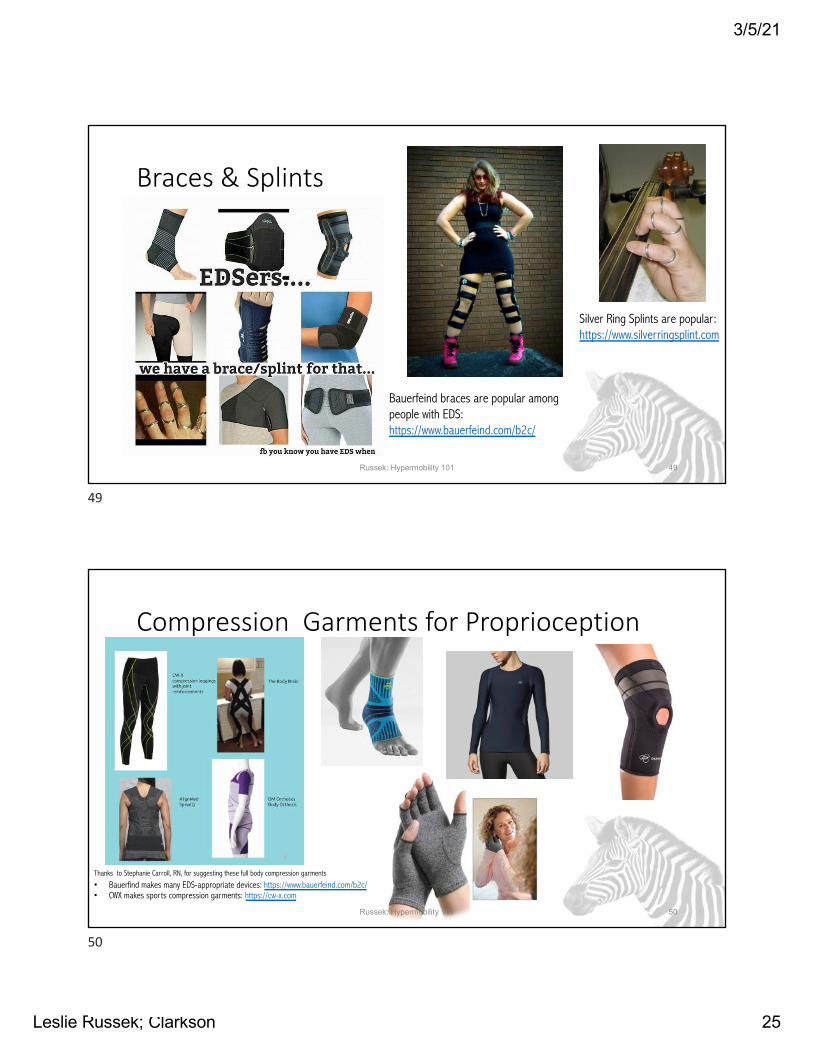
Braces & Splints
Russek: Hypermobility 101 49
Bauerfeind braces are popular among people with EDS: https://www.bauerfeind.com/b2c/
Silver Ring Splints are popular: https://www.silverringsplint.com
49
Compression Garments for Proprioception
Russek: Hypermobility 101 50
Thanks to Stephanie Carroll, RN, for suggesting these full body compression garments
• Bauerfind makes many EDS-appropriate devices: https://www.bauerfeind.com/b2c/• CWX makes sports compression garments: https://cw-x.com
50
3/5/21
Leslie Russek; Clarkson 26
Medications• Little definitive research evidence for medications• NSAIDs for true inflammation
• NSAIDs may slow tissue healing, aggravate GI Sx• Tricyclics, anti-seizure, SNRI meds for neuropathic pain• Topical analgesics and anti-inflammatory medications• Acetaminophen• Cautions:
• Opiates for short term use only• Muscle relaxers may aggravate instability
Russek: Hypermobility 101 51
Chopra, 2017Tinkle, 2017
51
HSD: Surgery Precautions
• Surgery is less likely to be successful in people with HSD/hEDS• Tissues are more fragile• Blood vessel fragility increases bleeding
• Surgery is only effective 34% of the time (Rombaut, 2011);
• 50% as often as non-hypermobile pts?• Tissue healing is delayed (Ericson, 2017)
• Special procedures for skin sutures: closer together, leave sutures in longer (Burcharth, 2012)
Russek: Hypermobility 101 52
52
3/5/21
Leslie Russek; Clarkson 27
Pain Management: Neuroplasticity• Even though there are real, physical issues with your
body, neuroplasticity (nerve learning) can change pain processing in your brain: “Sensitization”
• This is “volume control” for pain• Stress, anxiety, negative thinking, depression all turn
up the “volume control”• Physical interventions often do not work for this
type of pain..
Russek: Hypermobility 101 53
53
Managing Neuroplasticity• Relaxation training:
• Diaphragmatic or slow breathing• Meditation, “Tapping,” etc.• Stress management• Biofeedback, e.g., HRV, breathing (can now be done with smart-phone apps)
• Hope, gratitude, positive attitude• Find help with this approach on-line
• http://www.aci.health.nsw.gov.au/chronic-pain• Curable app: www.curablehealth.com
Russek: Hypermobility 101 54
54
3/5/21
Leslie Russek; Clarkson 28
Additional Resources• EDS-specific
• Ehlers-Danlos Society: www.ehlers-danlos.com• Educator’s Guide to EDS: https://ehlers-danlos.com/wp-content/uploads/Educator-Parent-Guide-2016.pdf
• Hypermobility Syndromes Association: www.hypermobility.org• My website (with slide handouts) https://webspace.clarkson.edu/~lrussek/hsd.html• Job Accommodation Network EDS guideline: https://askjan.org/disabilities/Ehlers-Danlos-Syndrome.cfm• POTS: www.potsuk.org• MCAS: https://www.tmsforacure.org
• Potsdam Fibro/EDS Support Group: https://webspace.clarkson.edu/~lrussek/pfsg.html
• Chronic pain related• Extensive Self-management guide for patients: https://kr.ihc.com/ext/Dcmnt?ncid=521195887• Web site for chronic pain management, with sections for adults with pain, children with pain, and health
professionals. Each module has a short educational video. http://www.aci.health.nsw.gov.au/chronic-pain• Trigger point management: Valerie De Laune, Pain Relief with Trigger Point Self-Help (book)
Russek: Hypermobility 101 55
55
Summary• You can learn to manage the “Issues with your tissues” by:
• Identifying and addressing contributing factors• Learning joint protection strategies• Doing appropriate exercises, motor control, body awareness
training to address those contributing factors• Using orthotics, braces, splints, or taping when appropriate
• Pain management strategies also help:• General wellness• Physical approaches• Psychological approaches
Russek: Hypermobility 101 56
56
3/5/21
Leslie Russek; Clarkson 29
Questions?
Russek: Hypermobility 101 57
57
Journal Article References• Ambrose KR, Golightly YM. Physical exercise as non-pharmacological treatment of chronic pain: Why and when. Best Practice & Research Clinical Rheumatology.
2015;29(1):120-130.• Burcharth J, Rosenberg J. Gastrointestinal surgery and related complications in patients with Ehlers-Danlos syndrome: a systematic review. Dig Surg. 2012;29(4):349-
357.• Castori M, Sperduti I, Celletti C, Camerota F, Grammatico P. Symptom and joint mobility progression in the joint hypermobility syndrome (Ehlers-Danlos syndrome,
hypermobility type). Clin Exp Rheumatol. 2011;29(6):998-1005.• Castori M, Tinkle B, Levy H, Grahame R, Malfait F, Hakim A. A framework for the classification of joint hypermobility and related conditions. Am J Med Genet C Semin
Med Genet. 2017;175(1):148-157.• Chopra P, Tinkle B, Hamonet C, et al. Pain management in the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):212-219.• Clark CJ, Simmonds JV. An exploration of the prevalence of hypermobility and joint hypermobility syndrome in Omani women attending a hospital physiotherapy service.
Musculoskeletal Care. 2011;9(1):1-10.• Ericson WB, Jr., Wolman R. Orthopaedic management of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):188-194.• Gebhart GF, Bielefeldt K. Physiology of Visceral Pain. Compr Physiol. 2016;6(4):1609-1633. • Hakim A, O'Callaghan C, De Wandele I, Stiles L, Pocinki A, Rowe P. Cardiovascular autonomic dysfunction in Ehlers-Danlos syndrome-Hypermobile type. Am J Med Genet
C Semin Med Genet. 2017;175(1):168-174.• Lima LV, Abner TSS, Sluka KA. Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena. J Physiol. 2017;595(13):4141-4150.• Rombaut L, Malfait F, De Wandele I, et al. Medication, surgery, and physiotherapy among patients with the hypermobility type of Ehlers-Danlos syndrome. Arch Phys
Med Rehabil. 2011;92(7):1106-1112.• Russek LN. Is it really fibromyalgia? Recognizing mast cell activation, orthostatic tachycardia, and hypermobility. Orthopaedic Practice. 2018;30(3):187-193. Available
on-line at: https://www.researchgate.net/publication/326426655_Is_It_Really_Fibromyalgia_Recognizing_Mast_Cell_Activation_Orthostatic_Tachycardia_and_Hypermobility
• Sabharwal R, Rasmussen L, Sluka KA, Chapleau MW. Exercise prevents development of autonomic dysregulation and hyperalgesia in a mouse model of chronic muscle pain. Pain. 2016;157(2):387-398.
• Seneviratne SL, Maitland A, Afrin L. Mast cell disorders in Ehlers-Danlos syndrome. Am J Med Genet C Semin Med Genet. 2017;175(1):226-236.• Tinkle B, Castori M, Berglund B, et al. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome Type III and Ehlers-Danlos syndrome hypermobility type):
Clinical description and natural history. Am J Med Genet C Semin Med Genet. 2017;175(1):48-69.
Russek: Hypermobility 101 58
58
3/5/21
Leslie Russek; Clarkson 30
Russek: Hypermobility 101 59
Thank You!
59