Embed Size (px)
Citation preview

DisclaimerDisclaimer
This slide kit presents data to support the rationale for This slide kit presents data to support the rationale for the use of the ADP-receptor antagonist clopidogrel in the use of the ADP-receptor antagonist clopidogrel in approved and non-approved indications approved and non-approved indications
The slide kit has been prepared for medical and The slide kit has been prepared for medical and scientific purposes, and cannot be considered as an scientific purposes, and cannot be considered as an inducement to use clopidogrel in non-registered inducement to use clopidogrel in non-registered indications indications
Neither Sanofi-Synthelabo nor Bristol-Myers Squibb Neither Sanofi-Synthelabo nor Bristol-Myers Squibb recommends the use of clopidogrel in any manner recommends the use of clopidogrel in any manner inconsistent with that described in the full prescribing inconsistent with that described in the full prescribing informationinformation

The CREDO TrialThe CREDO TrialCClopidogrel for the lopidogrel for the RReduction of eduction of EEventsvents
DDuring uring OObservationbservation

CClopidogrel for thelopidogrel for the RReduction of eduction of EEventsvents DDuring uring OObservationbservation
Steering CommitteeSteering Committee
Chair: Eric J.Topol, MDChair: Eric J.Topol, MD
Principal InvestigatorPrincipal Investigator
Steven R. Steinhubl, MDSteven R. Steinhubl, MD
The CREDO TrialThe CREDO Trial

Within 24 hoursWithin 24 hours
Incidence: 0.6%Incidence: 0.6%11
Acute Thrombosis
Subacute Thrombosis
Death
or MI
Within 4 weeksWithin 4 weeks
Incidence: 0.5%-5.7%Incidence: 0.5%-5.7%11
1 year1 year
Incidence: 15.8%Incidence: 15.8%22
11Mak K-H et al. Mak K-H et al. J Am Coll CardiolJ Am Coll Cardiol. 1996;27:494-503.. 1996;27:494-503. 22Steinhubl S et al. Steinhubl S et al. CirculationCirculation. 1999;100:18 (suppl): I-380. Abstract 1993.. 1999;100:18 (suppl): I-380. Abstract 1993.
Complications of Stent PlacementComplications of Stent Placement
Complications of Atherothrombotic DiseaseComplications of Atherothrombotic Disease
Early and Long-Term Risk of Ischemic EventsEarly and Long-Term Risk of Ischemic Events
Platelet Activation After PCIPlatelet Activation After PCI

00
1010
2020
3030
DaysDays
Placebo, No PretxPlacebo, No Pretx
Placebo + PretxPlacebo + Pretx
Abcix + PretxAbcix + Pretx
Abcix, No PretxAbcix, No Pretx
19.5%19.5%20.7%20.7%20.9%20.9%
28.5%28.5%
00 100100 200200 300300 365365
Pretx= Pre-treatmentPretx= Pre-treatmentSteinhubl S. Data presented at 1999 AHA Meeting, Atlanta, GA.Steinhubl S. Data presented at 1999 AHA Meeting, Atlanta, GA.
Risk of Death, MI, or Revascularization at 1 Year Follow-UpRisk of Death, MI, or Revascularization at 1 Year Follow-Up
% D
eath
, MI,
Tar
get
Ves
sel
% D
eath
, MI,
Tar
get
Ves
sel
Rev
ascu
lari
zati
on
Rev
ascu
lari
zati
on
EPISTENT: Importance of Pre-Treatment EPISTENT: Importance of Pre-Treatment with ADP-Receptor Antagonistswith ADP-Receptor Antagonists

††up to 12 months up to 12 months ‡‡plus ASA and other standard therapiesplus ASA and other standard therapies
Composite of CV-death or MI from randomization to end of follow-upComposite of CV-death or MI from randomization to end of follow-up††
Mehta et al. Mehta et al. Lancet. Lancet. 2001;358:527-533.2001;358:527-533.
PlaceboPlacebo‡‡ ClopidogrelClopidogrel‡‡
0.150.15
0.100.10
0.050.05
0.00.00 100100 200200 300300 400400
Days of follow-upDays of follow-up
12.6%12.6%
8.8%8.8%
P P = 0.002= 0.002N = 2658N = 2658
Cu
mu
lati
ve H
azar
d R
ate
Cu
mu
lati
ve H
azar
d R
ate
31%31%Relative RiskRelative Risk
ReductionReduction
PCI-CURE – Long-Term Efficacy PCI-CURE – Long-Term Efficacy of Clopidogrelof Clopidogrel

TVR= Target Vessel RevascularizationTVR= Target Vessel Revascularization
11Steinhubl S, Ellis S, Wolski K, et al. Steinhubl S, Ellis S, Wolski K, et al. Circulation.Circulation. 2001;103:1403. 2001;103:1403. 22O’Shea, JC, Buller CE, Cantor WJ, et al. O’Shea, JC, Buller CE, Cantor WJ, et al. JAMA.JAMA. 2002;287 (5):618 – 21. 2002;287 (5):618 – 21.33Moliterno DJ, Yakubov SJ, DiBattiste PM, et al. Moliterno DJ, Yakubov SJ, DiBattiste PM, et al. Lancet. Lancet. 2002;360:355 – 360.2002;360:355 – 360.
--14.3%14.3%6.0%6.0%Abciximab + stentAbciximab + stent
--14.8%14.8%7.6%7.6%
TARGETTARGET33
Tirofiban + stentTirofiban + stent
17.5%17.5%14.2%14.2%6.9%6.9%
ESPRITESPRIT22
Eptifibatide + stentEptifibatide + stent
19.5%19.5%- - 5.3%5.3%
EPISTENTEPISTENT11
Abciximab + stentAbciximab + stent
1 Year1 Year6 Months6 Months30 Days30 Days
Event Rates in Active Compound ArmEvent Rates in Active Compound ArmSTUDYSTUDY & Treatment & Treatment
Death / MI / TVRDeath / MI / TVR
Outcomes After Stenting: Outcomes After Stenting: 30 Days - 1 Year30 Days - 1 Year

Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
CREDO Study RationaleCREDO Study Rationale
Need for early pre-treatmentNeed for early pre-treatment
– clopidogrel loading dose provides early benefit clopidogrel loading dose provides early benefit
– this early benefit is enhanced if a loading dose is given this early benefit is enhanced if a loading dose is given pre-procedurepre-procedure
Need for long-term treatmentNeed for long-term treatment
– patients undergoing PCI remain at high-risk for long-term patients undergoing PCI remain at high-risk for long-term cardiac eventscardiac events
• there is an increased incidence of death, MI, and there is an increased incidence of death, MI, and revascularization at 1 and 3-year following PCI (revascularization at 1 and 3-year following PCI (15%)15%)
• high event rates represent the ongoing process of high event rates represent the ongoing process of atherothrombosis elsewhere in coronary vasculature atherothrombosis elsewhere in coronary vasculature
– there is also a need for reducing thrombotic events in other there is also a need for reducing thrombotic events in other arterial beds (cerebrovascular and peripheral)arterial beds (cerebrovascular and peripheral)

UTVR= Urgent Target Vessel RevascularizationUTVR= Urgent Target Vessel Revascularization
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
CREDO ObjectivesCREDO Objectives
ObjectivesObjectives
– to evaluate the long-term effect of prolonged (1 year) to evaluate the long-term effect of prolonged (1 year) therapy with clopidogrel plus ASA and other standard therapy with clopidogrel plus ASA and other standard therapies, for reducing the composite endpoint therapies, for reducing the composite endpoint of MI, stroke, and death in patients undergoing urgent of MI, stroke, and death in patients undergoing urgent or elective PCI, with or without stentor elective PCI, with or without stent
– to evaluate the effect of pre-treatment with a clopidogrel to evaluate the effect of pre-treatment with a clopidogrel 300 mg loading dose on the composite of death (all-cause), 300 mg loading dose on the composite of death (all-cause), MI (Q- or non-Q-wave), or urgent target vessel MI (Q- or non-Q-wave), or urgent target vessel revascularization (UTVR) at Day 28, in patients who revascularization (UTVR) at Day 28, in patients who underwent PCI, with or without stentunderwent PCI, with or without stent
– to evaluate the safety of clopidogrel, specifically the to evaluate the safety of clopidogrel, specifically the frequency of major bleeding events and early frequency of major bleeding events and early discontinuation of study drugdiscontinuation of study drug

Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
CREDO EndpointsCREDO Endpoints
28 Day Endpoint28 Day Endpoint
– first occurrence of any component up to first occurrence of any component up to 28 days of the composite of:28 days of the composite of:
• death, MI, or UTVRdeath, MI, or UTVR 1 Year Endpoint1 Year Endpoint
– first occurrence of any component up to first occurrence of any component up to 1 year of the composite of: 1 year of the composite of:
• death, MI, or strokedeath, MI, or stroke

Clo
pid
og
rel
Clo
pid
og
rel
Arm
Arm
Pla
ceb
o
Pla
ceb
o
Arm
Arm
†† Plus other standard therapiesPlus other standard therapies* Both groups received clopidogrel 75 mg + ASA 325 mg at time of procedure* Both groups received clopidogrel 75 mg + ASA 325 mg at time of procedure
PCI*PCI* 28 Days28 Days
Placebo + Placebo + ASAASA†† (325 mg) (325 mg)
Pre-treatmentPre-treatment3-24 h before PCI3-24 h before PCI
Clopidogrel 300 mgClopidogrel 300 mg+ ASA+ ASA†† (325 mg) (325 mg)
Clopidogrel 75 mg QDClopidogrel 75 mg QD+ ASA+ ASA†† 325 mg QD 325 mg QD
Clopidogrel 75 mg QDClopidogrel 75 mg QD+ ASA+ ASA†† 325 mg QD 325 mg QD
RR
12 Months12 Months
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Placebo QDPlacebo QD+ ASA+ ASA†† (81-325 mg) QD (81-325 mg) QD
Clopidogrel 75 mg QDClopidogrel 75 mg QD+ ASA+ ASA†† (81-325 mg) QD (81-325 mg) QD
Overall Study Design Overall Study Design

Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Inclusion CriteriaInclusion Criteria
Patients aged > 21 yearsPatients aged > 21 years
– able to provide informed consentable to provide informed consent
– agree to comply with protocol-specified proceduresagree to comply with protocol-specified procedures Presenting with symptomatic CADPresenting with symptomatic CAD
– with objective evidence of ischemia, e.g.:with objective evidence of ischemia, e.g.:
• symptoms of angina pectoris or symptoms of angina pectoris or
• positive stress test or positive stress test or
• dynamic ECG changesdynamic ECG changes
– referred for elective or urgent PCIreferred for elective or urgent PCI
– candidate for either conventional angioplasty and/or primary candidate for either conventional angioplasty and/or primary intracoronary stent implantation intracoronary stent implantation

Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Exclusion CriteriaExclusion Criteria
Active internal bleeding or hx of hemorrhagic diathesisActive internal bleeding or hx of hemorrhagic diathesis
>50% stenosis of the left main coronary artery>50% stenosis of the left main coronary artery
Coronary anatomy not amenable to stent placementCoronary anatomy not amenable to stent placement
Planned staged interventional procedurePlanned staged interventional procedure
Failed PCI within 2 weeksFailed PCI within 2 weeks
Q-wave MI within 24 hoursQ-wave MI within 24 hours
Serum Creatinine Serum Creatinine 3.0 mg/dl3.0 mg/dl
ALT/AST >3x ULNALT/AST >3x ULN
IV GPIIb/IIIa antagonist within 7 daysIV GPIIb/IIIa antagonist within 7 days
Need for long-term anticoagulant or NSAID useNeed for long-term anticoagulant or NSAID use
Contraindications to antithrombotic/antiplatelet therapyContraindications to antithrombotic/antiplatelet therapy

n=2,116n=2,116
PP n=900PP n=900 PP n=915PP n=915
Clopidogrel pre-treatment Clopidogrel pre-treatment (loading dose 300 mg) (loading dose 300 mg) ++
clopidogrel long-term clopidogrel long-term (1 year)(1 year)
No pre-treatment No pre-treatment ++ clopidogrel short-term clopidogrel short-term
(28 days)(28 days)
ITT = Intent-to-Treat: All randomized patients (PP patients + patients who did not undergo PCI) ITT = Intent-to-Treat: All randomized patients (PP patients + patients who did not undergo PCI)
PP = Per Protocol: All patients who underwent PCI after randomizationPP = Per Protocol: All patients who underwent PCI after randomization
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
ITT n=1,063ITT n=1,063ITT n=1,053ITT n=1,053
Per-Protocol and Intent-to-Treat Per-Protocol and Intent-to-Treat PopulationsPopulations

* Plus ASA and other standard therapies* Plus ASA and other standard therapies
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Clopidogrel* Clopidogrel* Placebo*Placebo*(n=1,053)(n=1,053) (n=1,063)(n=1,063)
Age (mean, yearsAge (mean, yearsSD) SD) 61.5 61.5 11.211.2 61.8 61.8 11 11
Female (%)Female (%) 29.329.3 27.9 27.9
Diabetes (%) Diabetes (%) 27.527.5 25.425.4
Hyperlipidemia (%)Hyperlipidemia (%) 75.775.7 76.276.2
Hypertension (%)Hypertension (%) 67.467.4 69.669.6
Family history of premature CAD (%)Family history of premature CAD (%) 41.541.5 42.942.9
Prior MI (%)Prior MI (%) 33.533.5 34.434.4
Prior Stroke (%)Prior Stroke (%) 6.46.4 7.07.0
Prior PAD (%)Prior PAD (%) 9.79.7 10.310.3
Baseline Characteristics Baseline Characteristics

Chronic Medication at BaselineChronic Medication at Baseline
Clopidogrel* Clopidogrel* Placebo*Placebo* (n=1,053)(n=1,053) (n=1,063)(n=1,063)
Aspirin (%) Aspirin (%) 29.929.9 29.629.6
Beta-Blockers (%)Beta-Blockers (%) 63.163.1 65.5 65.5
Statin (%) Statin (%) 53.653.6 57.557.5
ACE-I (%)ACE-I (%) 33.033.0 34.234.2
CCB (%)CCB (%) 25.525.5 29.429.4
* Plus ASA and other standard therapies* Plus ASA and other standard therapies Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.

Clopidogrel* Clopidogrel* Placebo* Placebo* (n=900)(n=900)†† (n=915)(n=915)††
IV GPIIb/IIIa Antagonist Use (%) IV GPIIb/IIIa Antagonist Use (%) 47.4 47.4 43.343.3
Pre-Specified (%) Pre-Specified (%) 24.124.1 22.7 22.7
Bail-Out (%) Bail-Out (%) 23.323.3 20.620.6
* Plus ASA and other standard therapies * Plus ASA and other standard therapies †† PP=Per-ProtocolPP=Per-Protocol
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
During the Period of Initial PCIDuring the Period of Initial PCI
Use of IV GPIIb/IIIa AntagonistsUse of IV GPIIb/IIIa Antagonists

Clopidogrel*Clopidogrel* Placebo*Placebo*(n=1,053)(n=1,053) (n=1,063)(n=1,063)
Unstable angina (%) Unstable angina (%) 52.552.5 53.153.1
Recent MI (%) Recent MI (%) 14.314.3 13.113.1
Stable angina or other (%) Stable angina or other (%) 32.832.8 32.832.8
* Plus ASA and other standard therapies* Plus ASA and other standard therapies
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Clinical Diagnosis Requiring PCIClinical Diagnosis Requiring PCI

MI, Stroke, or Death – ITT PopulationMI, Stroke, or Death – ITT Population
* Plus ASA and other standard therapies* Plus ASA and other standard therapies
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Co
mb
ined
En
dp
oin
t C
om
bin
ed E
nd
po
int
Occ
urr
ence
(%
)O
ccu
rren
ce (
%)
Months From RandomizationMonths From Randomization
27% RRR27% RRRP=0.02P=0.02
Placebo*Placebo*Clopidogrel*Clopidogrel*
00
55
1010
1515
8.5%8.5%
11.5%11.5%
00 33 66 99 1212
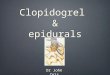
Long-Term (1 Year) Benefits of Long-Term (1 Year) Benefits of Clopidogrel in PCI PatientsClopidogrel in PCI Patients

Clopidogrel*Clopidogrel* Placebo*Placebo*EndpointsEndpoints (n=1053)(n=1053) (n=1063)(n=1063) RRRRRR 95% CI95% CI
MI, Stroke, deathMI, Stroke, death 8.58.5 11.511.5 26.926.9 (3.9,44.4)(3.9,44.4)
MI, deathMI, death†† 7.97.9 10.410.4 24.024.0 (-0.9,42.7)(-0.9,42.7)
DeathDeath†† 1.71.7 2.32.3 24.624.6 (-38.9,59.1)(-38.9,59.1)
MIMI†† 6.76.7 8.48.4 20.820.8 (-8.4,44.2)(-8.4,44.2)
StrokeStroke†† 0.90.9 0.90.9 10.010.0 (-21.3,24.0)(-21.3,24.0)
* Plus ASA and other standard therapies* Plus ASA and other standard therapies
† † The study was not powered to detect a treatment effect with clopidogrel in individual components The study was not powered to detect a treatment effect with clopidogrel in individual components of the composite endpoint. of the composite endpoint.
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
% of patients with events% of patients with events
Long-Term (1 Year) Benefits of Long-Term (1 Year) Benefits of ClopidogrelClopidogrel

* Plus ASA and other standard therapies* Plus ASA and other standard therapies
0.60.6 0.80.8 1.01.0 1.21.2
IV GP IIb/IIIa Inhibitor UseIV GP IIb/IIIa Inhibitor Use YesYes (N=826) (N=826) NoNo (N=1289)(N=1289)ACSACS YesYes (N=1407)(N=1407) NoNo (N=694)(N=694)DiabetesDiabetes YesYes (N=560)(N=560) NoNo (N=1556)(N=1556)StentStent YesYes (N=1616)(N=1616) NoNo (N=500)(N=500)MaleMale (N=1510)(N=1510)FemaleFemale (N=606)(N=606)
OverallOverall (N=2116)(N=2116)
28.828.8 26.526.5
27.627.6 22.722.7
11.211.2 32.832.8
28.828.8 19.019.0 24.524.5 32.132.1
26.926.9
0.40.4Hazard ratio (95% CI)Hazard ratio (95% CI)
Placebo*Placebo*BetterBetter
Clopidogrel*Clopidogrel*BetterBetter RRRRRR
(52.4 to -6.5)(52.4 to -6.5)(49.3 to -6.6)(49.3 to -6.6)
(47.8 to -0.4)(47.8 to -0.4)(53.2 to -27.6)(53.2 to -27.6)
(46.2 to -46.8)(46.2 to -46.8)(51.6 to 6.8)(51.6 to 6.8)
(47.4 to 3.6)(47.4 to 3.6)(57.0 to -52.6)(57.0 to -52.6)(45.5 to -4.6)(45.5 to -4.6)
(58.9 to -12.1)(58.9 to -12.1)
(44.3 to 3.9)(44.3 to 3.9)
95% CI95% CI
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
SubgroupSubgroup
Consistent Long-Term Benefit of Consistent Long-Term Benefit of Clopidogrel: MI, Stroke, or Death Clopidogrel: MI, Stroke, or Death at 1 Yearat 1 Year

Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
1 Year Results:1 Year Results:ConclusionsConclusions
Clopidogrel plus aspirin and other standard therapy Clopidogrel plus aspirin and other standard therapy demonstrated a 27% RRR (p=0.02) in the combined endpoint demonstrated a 27% RRR (p=0.02) in the combined endpoint of MI, stroke, and death compared to placebo plus aspirinof MI, stroke, and death compared to placebo plus aspirin
The benefit was consistent in all patient subgroups The benefit was consistent in all patient subgroups evaluatedevaluated
In the CREDO trial patients received standard In the CREDO trial patients received standard of care in the US:of care in the US:
– almost half of patients received IV GP IIb/IIIa antagonists, almost half of patients received IV GP IIb/IIIa antagonists, and clopidogrel showed an incremental benefit on top of IV and clopidogrel showed an incremental benefit on top of IV GP IIb/IIIa therapyGP IIb/IIIa therapy
– short time to PCI: 3 to 24 hours (per protocol); short time to PCI: 3 to 24 hours (per protocol); mean = 9.8 hoursmean = 9.8 hours

Co
mb
ined
En
dp
oin
t C
om
bin
ed E
nd
po
int
Occ
urr
ence
(%
)O
ccu
rren
ce (
%)
Days From RandomizationDays From Randomization
No-PT - Placebo*No-PT - Placebo*
PT- Clopidogrel*PT- Clopidogrel*
00
55
1010
00 77 1414 2121 2828
PT = Pre-treatmentPT = Pre-treatment
*Plus ASA and other standard therapies*Plus ASA and other standard therapies
Death, MI, UTVR- PP PopulationDeath, MI, UTVR- PP Population
18.5% 18.5% RRRRRR
P=0.23P=0.23
99
88
11
44
33
22
77
66
8.3%8.3%
6.8%6.8%
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al.
JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Early Effects of Pre-treatment with Early Effects of Pre-treatment with Clopidogrel – 28 Day ResultsClopidogrel – 28 Day Results

0.40.4 0.60.6 0.80.8 1.01.0 1.21.2
Hazard ratio (95% CI)Hazard ratio (95% CI)
3 to <6 hrs3 to <6 hrs 7.97.9 7.07.0 893 893
6 to 24 hr6 to 24 hr 5.85.8 9.4 9.4 851 851
RRR -13.4RRR -13.4P=NSP=NS
RRR 38.6RRR 38.6P=0.05P=0.05
RRR 18.5RRR 18.5P=0.23P=0.23Overall CREDO ResultsOverall CREDO Results
NN PT-Clopidogrel*PT-Clopidogrel* No-PT*No-PT*
Events (%)Events (%)No-PTNo-PTBetterBetter
PT-ClopidogrelPT-ClopidogrelBetterBetter
PT= Pre-treatmentPT= Pre-treatment
* Plus ASA and other standard therapies* Plus ASA and other standard therapies
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Effect of Timing of Loading Dose:Effect of Timing of Loading Dose:28 Day Endpoint - Death, MI, UTVR28 Day Endpoint - Death, MI, UTVR

Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Day 28 Results:Day 28 Results:ConclusionsConclusions
Pre-treatment with a clopidogrel loading dose Pre-treatment with a clopidogrel loading dose (300 mg) provided a favorable trend towards a (300 mg) provided a favorable trend towards a reduction in the composite of MI, death, and reduction in the composite of MI, death, and UTVR (18.5% RRR, p=0.23) UTVR (18.5% RRR, p=0.23)
Data suggest a greater benefit (RRR=38.6%, Data suggest a greater benefit (RRR=38.6%, p=0.05) when a clopidogrel loading dose was p=0.05) when a clopidogrel loading dose was given given 6 hours prior to PCI6 hours prior to PCI
The benefit of clopidogrel was incremental to the The benefit of clopidogrel was incremental to the use of IV GP IIb/IIIa antagonists, with a use of IV GP IIb/IIIa antagonists, with a favorable safety profilefavorable safety profile

Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Incremental Benefit of Treatment with Incremental Benefit of Treatment with Clopidogrel from 29 Days to 1 YearClopidogrel from 29 Days to 1 Year
In the ITT analysis, a 19.7% RRR was obtained In the ITT analysis, a 19.7% RRR was obtained for the reduction of the combined endpoint of for the reduction of the combined endpoint of death, MI, and stroke at 28 days with death, MI, and stroke at 28 days with pre-treatment of clopidogrelpre-treatment of clopidogrel
Continued treatment with clopidogrel from day Continued treatment with clopidogrel from day 29 to 1 year was associated with a further 37.4% 29 to 1 year was associated with a further 37.4% RRR (p=0.04) for the combined endpoint of RRR (p=0.04) for the combined endpoint of death, MI, and strokedeath, MI, and stroke

* Plus ASA and other standard therapies* Plus ASA and other standard therapies †† 101 patients underwent CABG in the clopidogrel group101 patients underwent CABG in the clopidogrel group‡‡ 99 patients underwent CABG in the placebo group99 patients underwent CABG in the placebo groupITT=Intent-To-Treat populationITT=Intent-To-Treat population
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
881717 Non-CABGNon-CABG
55556464 CABGCABG
0.120.1263 (5.9%)63 (5.9%)‡‡81 (7.7%)81 (7.7%)††ProceduralProcedural
0.280.288 (0.8%)8 (0.8%)13 (1.2%)13 (1.2%)Non-proceduralNon-procedural
0.070.0771 (6.7%)71 (6.7%)93 (8.8%)93 (8.8%)AnyAny
P-valueP-valuePlacebo* Placebo* (n=1,063)(n=1,063)
Clopidogrel* Clopidogrel* (n=1,053)(n=1,053)Major BleedingMajor Bleeding
Safety Outcomes: Major Bleeding Safety Outcomes: Major Bleeding Events One-Year Results ITTEvents One-Year Results ITT

0.340.347 (1.3%)7 (1.3%)11 (2.3%)11 (2.3%) No (n=991)No (n=991)
>0.99>0.999 (2.3%)9 (2.3%)9 (2.1%)9 (2.1%) Yes (n=823)Yes (n=823)
IV GP IIb/IIIa use – IV GP IIb/IIIa use –
(PPP only)(PPP only)
0.120.1236 (3.4%)36 (3.4%)‡‡50 (4.7%)50 (4.7%)††ProceduralProcedural
0.370.374 (0.4%)4 (0.4%)1 (0.1%)1 (0.1%)Non-proceduralNon-procedural
0.240.2440 (3.8%)40 (3.8%)51 (4.8%)51 (4.8%)AnyAny
P-valueP-valueNo No
pre-treatment* pre-treatment* (n=1,063)(n=1,063)
Pre-treatmentPre-treatmentwith clopidogrel* with clopidogrel*
(n=1,053)(n=1,053)Major BleedingMajor Bleeding
* Plus ASA and other standard therapies* Plus ASA and other standard therapies †† 101 patients underwent CABG in the clopidogrel group101 patients underwent CABG in the clopidogrel group‡‡ 99 patients underwent CABG in the placebo group99 patients underwent CABG in the placebo groupITT=Intent-To-Treat populationITT=Intent-To-Treat populationPPP= Per Protocol populationPPP= Per Protocol population
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Safety Outcomes: Major Bleeding Safety Outcomes: Major Bleeding Events 28 Days ITT ResultsEvents 28 Days ITT Results

* Plus ASA and other standard therapies* Plus ASA and other standard therapies
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Overall Safety Outcomes: Overall Safety Outcomes: Conclusions at 1 YearConclusions at 1 Year
When clopidogrel was continued for a full year When clopidogrel was continued for a full year there was no statistically significant increase in there was no statistically significant increase in major bleeding (8.8% clopidogrel* vs. 6.7% major bleeding (8.8% clopidogrel* vs. 6.7% placebo*, p=0.07)placebo*, p=0.07)
Minor bleedings rates were comparable (5.3% Minor bleedings rates were comparable (5.3% clopidogrel* vs. 5.6% placebo*, p=0.84)clopidogrel* vs. 5.6% placebo*, p=0.84)
No fatal bleeds or intracranial hemorrhages No fatal bleeds or intracranial hemorrhages were observedwere observed

* Plus ASA and other standard therapies* Plus ASA and other standard therapies
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al. JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
CREDO - General ConclusionsCREDO - General Conclusions
Long-term results at 1 year demonstrate that clopidogrel* Long-term results at 1 year demonstrate that clopidogrel* provided a 27% RRR (p=0.02) in the combined endpoint provided a 27% RRR (p=0.02) in the combined endpoint of MI, stroke, and deathof MI, stroke, and death
The results indicate an increased benefit of pre-treatment The results indicate an increased benefit of pre-treatment with clopidogrel ³6 hrs prior to PCI (RRR 38%, p=0.05)with clopidogrel ³6 hrs prior to PCI (RRR 38%, p=0.05)
Clopidogrel* provided incremental benefit between Day Clopidogrel* provided incremental benefit between Day 29 and 1 year (37.4% RRR, p=0.04)29 and 1 year (37.4% RRR, p=0.04)
In the CREDO trial patients received standard of care in In the CREDO trial patients received standard of care in the USthe US
The benefit was consistent through all patient subgroups The benefit was consistent through all patient subgroups evaluated and independent of the background therapy evaluated and independent of the background therapy including ASA, with a favorable safety profileincluding ASA, with a favorable safety profile