Embed Size (px)
Citation preview
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 1
Anders Nattestad, DDS, Ph.DProfessor and Director
Dept. of Oral and Maxillofacial Surgery
Medical emergencies in the dental office
1
• I am full time in academia for 20+ years with one day per week faculty practice at the school
• I have no financial interests in any company related to the field of dentistry or surgery
• I occasionally receive honorariums for speaking at events arranged by the industry
• My department are offered product samples and discounts on products from the industry
DisclaimerDisclaimer
2
Who am I?Who am I?
3
1981 - 2003 2004 - 2007 2007 -
• A basic understanding of the consequences of the most common medical conditions and their impact on safe dental care
• An understanding of safe parameters for vital signs• Knowing when say “Not now” to a patient with a serious medical condition asking for routine dental care
• Know when to ask for a medical consult and when not to ask
• Know what to do when “things” happen
Objectives – Medical emergencies in the dental office 1/2
Objectives – Medical emergencies in the dental office 1/2
4
• Take and record vital signs, recognizing safe parameters• Recognize medical emergencies and respond in a proper manner for the safety and well being of the patient including– Altered consciousness– Respiratory distress– Allergic reactions and – Chest pain
• Apply preventive measures to avoid medical emergencies
• Describe the indications and therapeutic actions of relevant emergency drugs
Objectives – Medical emergencies in the dental office 2/2
Objectives – Medical emergencies in the dental office 2/2
5
• 9:00 – 10:45 AM Medically complex patients
• 10:45 – 11:15 AM Break
• 11:15 AM – 12:30 PM Continued/Medical emergencies
• 12:30 – 1:30 PM Lunch• 1:30 – 2:45 PM Medical emergencies
• 2:45 – 3:00 PM Break• 3:00 – 4:30 PM Drugs and Dentistry• 4:30 – 5:00 PM Q & A
Program for the dayProgram for the day
6
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 2
7
• Overall recommendations– Do not be intimidated by a complex medical history and a very long list of drugs
– Take one disease and one drug at the time
– Use Peter Jacobson’s document:http://dental.pacific.edu/docs/patientProtocol/Medically_Complex.pdf
– Ask for advice when needed and…
Medically complex patientsMedically complex patients
Medical Hx
Physical evaluation
Vital signs
Tx planning
Tx
Monitoring during tx
Post‐medication
Follow‐up
Pre‐medication Refer pt out
Lab exams Medical consult
8
Medical consult?Medical consult?
9
• AMI in the last six months• Stroke in the last six months• Uncontrollered non‐compliant diabetics
• Blood pressure above 180/110*• HIV/AIDS with CD4 < 50* and/or platelet count < 60,000*
• INR > 3.5* and need tx with bleeding such as extractions
• Undiagnosed and untreated chest pain
Elective tx should be consideredpostponed in patients with
Elective tx should be consideredpostponed in patients with
*Individual assessment of the patient is necessary– do not treat numbers – treat patients
Medical Hx
Physical evaluation
Vital signs
Tx planning
Tx
Monitoring during tx
Post‐medication
Follow‐up
Pre‐medication Refer pt out
Lab exams Medical consult
10 11
ASA classificationASA classification
12
ASA physical status classASA physical status class• ASA I:A normal healthy patient• ASA II:A patient with mild systemic disease or significant health risk factor
• ASA III:A patient with severe systemic disease that is not incapacitating
• ASA IV:A patient with severe systemic disease that is a constant threat to life
• ASA V:A moribund patient who is not expected to survive without the operation
• ASA VI:A declared brain‐dead patient whose organs are being removed for donor purposes
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 3
13
ASA details of classificationASA details of classification• ASA I
Patients are considered to be normal and healthy. Patients are able to walk up one flight of stairs or two level city blocks without distress. Little or no anxiety. Little or no risk. This classification represents a "green flag" for treatment. The supervising DDS will not need to be made aware of the presence of this patient before treatment.
• ASA IIPatients have mild to moderate systemic disease or are healthy ASA I patients who demonstrate a more extreme anxiety and feartoward dentistry. Patients are able to walk up one flight of stairs or two level city blocks, but will have to stop after completion of the exercise because of distress. Minimal risk during treatment. This classification represents a "yellow flag" for treatment. The supervising DDS will need to be made aware of the presence of this patient before treatment. Examples: well‐controlled non‐insulin controlled diabetes, epilepsy, asthma, and/or thyroid conditions; ASA I with a respiratory condition, pregnancy, and/or active allergies.
• ASA IIIPatients have severe systemic disease that limits activity, but is not incapacitating. Patients are able to walk up one flight of stairs or two level city blocks, but will have to stop enroute because of distress. If dental care is indicated, stress reduction protocol and other treatment modifications are indicated. This classification represents a "yellow flag" for treatment. The supervisingDDS will need to be made aware of the presence of this patient and may want to examine patient and/or have medical consultation before treatment. Examples: angina pectoris, myocardial infarction or cerebrovascular accident history, insulindependent diabetes, congestive heart failure, chronic obstructive pulmonary disease.
• ASA IVPatients have severe systemic disease that limits activity and is a constant threat to life. Patients are unable to walk up one flight of stairs or two level city block. Distress is present even at rest. Patients pose significant risk since patients in this category have a severe medical problem of greater importance to the patient than the planned dental treatment. Whenever possible, electivedental care should be postponed until such time as the patient's medical condition has improved to at least an ASA III classification. This classification represents a "red flag" ‐ a warning flag indicating that the risk involved in treating the patient is too great to allow elective care to proceed. The supervising DDS will need to be consulted before proceeding with treatment.Examples: unstable angina pectoris, myocardial infarction or cerebrovascular accident within the last six months, high bloodpressure, severe congestive heart failure or chronic obstructive pulmonary disease, uncontrolled epilepsy, diabetes, or thyroid condition.
• ASA VPatients are moribund and are not expected to survive more than 24 hours with or without an operation. These patients are almost always hospitalized, terminally ill patients. Elective dental treatment is definitely contraindicated; however, emergency care, in the realm of palliative treatment may be necessary. This classification represents a “red flag" for dental care and any care is done in a hospital situation.
• ASA VIClinically dead patients being maintained for harvesting of organs.
• ASA‐E: Emergency operation of any variety (used to modify one of the above classifications, i.e., ASA III‐E).
14
http://www.asahq.org/http://www.asahq.org/
15
ASA classification examplesASA classification examplesClass Description Examples
1 A normal, healthy patient, without organic, physiologic or psychiatric disturbance Healthy patient with good exercise tolerance
2A patient with mild systemic disease, controlled medical conditions without significant systemic effects
Controlled hypertension, controlled diabetes mellitus without system effects, cigarette smoking without evidence of COPD, anemia, mild obesity, age less than 1 or greater than 70 years, pregnancy
3 A patient with severe systemic disease, having medical conditions with significant systemic effects intermittently associated with significant functional compromise
Controlled CHF, stable angina, old MI, poorly controlled hypertension, morbid obesity, bronchospastic disease with intermittent symptoms, chronic renal failure
4 A patient with severe systemic disease that is a constant threat to life, having medical conditions that are poorly controlled, associated with significant dysfunction or incapacity
Unstable angina, symptomatic COPD, symptomatic CHF, hepatorenal failure
5A moribund patient who is not expected to survive without the surgical procedure
Multiorgan failure, sepsis syndrome with hemodynamic instability, profound hypothermia, poorly controlled coagulopathy
Source: American Society of Anesthesiologists Relative Values Guide, 1999.
16
Blood pressure measurementBlood pressure measurement
• Next
17
Gold StandardGold Standard
18
Alternative devices for BP measurementAlternative devices for BP measurement
Xhttp://www.fda.gov/ora/compliance_ref/cpg/cpgdev/cpg310‐210.html
AAMI Criteria for accuracy is ±3 mm Hg or +/‐ 2% of reading (whichever is greater)
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 4
19
Validation studiesValidation studies
20
Blood pressure and ASA classificationBlood pressure and ASA classification
From Malamed: Sedation: A guide to patient management 21
BP Guidelines for Oral Surgery@UoPBP Guidelines for Oral Surgery@UoP
• Patients with pre‐hypertension (120‐139/ 80‐89 mm Hg) are good candidates for all dental procedures and can normally receive local anesthesia with epinephrine 1:100.000.
• Patients with mild to moderate hypertension (140‐180/90‐110 mm Hg) do not present an independent risk factor, but an overall assessment of the patient should be made including the complexity of the planned treatment. Although no scientific evidence is available, it is suggested to avoid the use of epinephrine in local anesthesia and in retraction cords.
• Patients with marked elevated BP ( > 180/110 mm Hg) should normally not be treated at our clinics, but referred for management of the elevated BP and come back for dental treatment later.
JADA Volume 135, May 2004
• HIV and AIDS• Diabetes• Cardiovascular diseases• Total joint replacements• Bleeding disorders
Medically complex patientsMedically complex patients
22
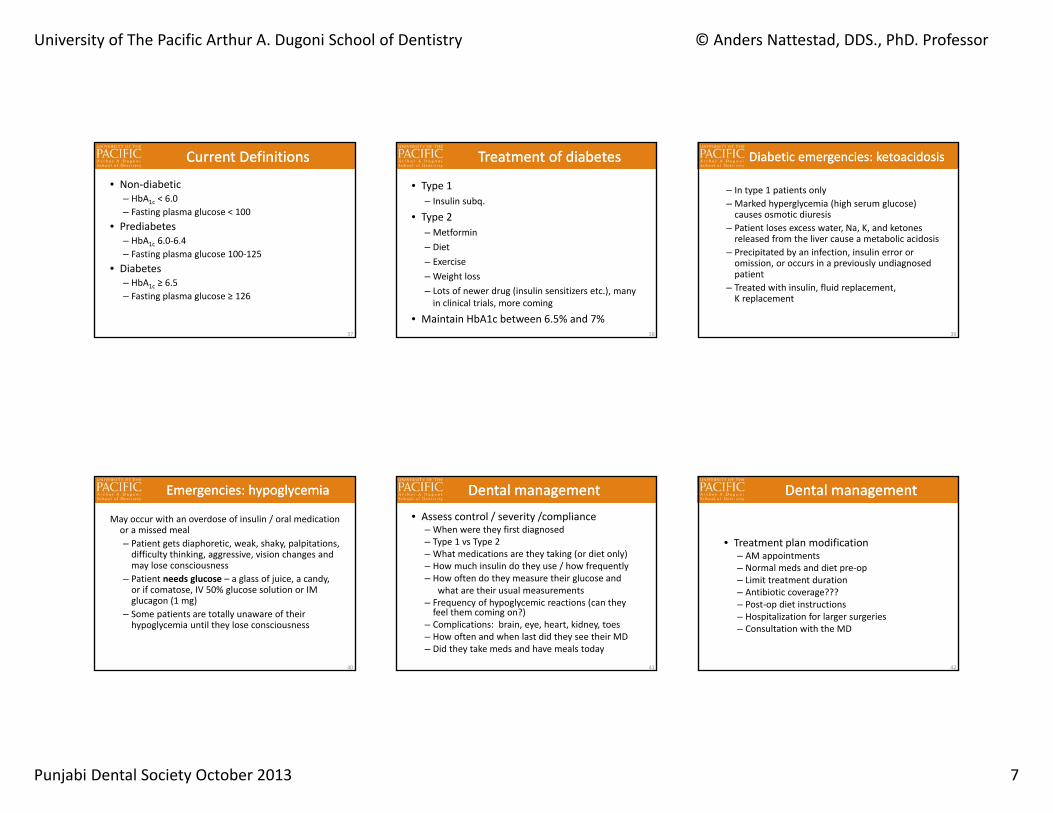
HIV and AIDS patientsHIV and AIDS patients
23
• First reported June 5, 1981 by CDC• Acquired immune deficiency syndrome• 33.2 million people live with the disease worldwide• AIDS has killed an estimated 2.1 million people• Over three‐quarters of these deaths occurred in sub‐Saharan
Africa• HIV is a retrovirus that primarily infects vital organs of the
human immune system such as CD4+ T cells
HIV and AIDSHIV and AIDS
24
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 5
• According to the US CDC definition, you have AIDS if you are infected with HIV and present with one of the following (selected from many more):– A CD4+ T‐cell count below 200 cells/µl (or a CD4+ T‐cell percentage of total lymphocytes of less than 15%) or you have one of the following illnesses:
– Candidiasis of bronchi, trachea, or lungs– Herpes simplex: chronic ulcer(s) (for more than 1 month)– Kaposi's sarcoma– Lymphoma– Pneumonia (recurrent)– Tuberculosis, disseminated
HIV or AIDS?HIV or AIDS?
25
• Viral load– Low: 40‐500 copies/mL– High: 5,000‐10,000 copies/mL
• T‐helper CD4+ – Receptor for HIV– Normal value 400‐1200– Precautions to be taken when below 50– Good correlation with risk of infection– Can fluctuate as much as 30% especially in children
• Platelets (cells per mm3)– Normal 150,000 – 400,000– Lowest relative value for surgery: 60,000 (depending of type of surgery)
• How long is a lab test good for? (Use clinical judgment)– 3 months if CD4 was below 200– 6 months if CD4 was above 200
Assessment of lab valuesAssessment of lab values
26
• Without treatment, the median survival is 9‐11 years dependent on subtype of virus
• HAART (highly active antiretroviral therapy) increases survival to a median of 20 years
• Cause of death usually pulmonary infections
Treatment of HIV/AIDSTreatment of HIV/AIDS
27
• Avoid extractions when platelet count is below 60,000
• Avoid elective dental treatment when CD4 is well below 50
• If patient is on antiretrovirals, then labs every year
• If not, labs are good for 6 months if CD4 is above 200 and 3 months if below 200
Dental managementDental management
28
• What is it• How is it diagnosed• What does it mean• The diabetic emergency• Dental management of the diabetic patient
DiabetesDiabetes
29
• A metabolic disease caused by an absolute or relative lack of insulin resulting in abnormalities in carbohydrate, protein and lipid metabolism
• Insulin is a hormone released in response to rising levels of blood glucose. Acts by increasing cellular transport of glucose and increased storage of glucose
• Prevalence: 6% of the population or 18M people in America or 100 patients in an average dental practice patient population
Diabetes mellitus – what is it?Diabetes mellitus – what is it?
30

University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 6
• Type 1 diabetes – beta cells are immunologically destroyed, eventually no insulin is produced (10%)
• Type 2 diabetes – insulin secretion is reduced, target cells become relatively insulin resistant ( receptors and post‐receptor activity) (90%)
PathophysiologyPathophysiology
31
Type 1
• 10% of diabetics• Age of onset – young• Severe• Requires insulin• Normal build• Little genetic component• Autoimmune
Comparison of type 1 and 2 Comparison of type 1 and 2
Type 2
• 90% of diabetics• Age of onset – 40+• Mild• May require insulin, usually diet or oral hypoglycemics
• Obese• Strong genetic component 32
Symptoms of DiabetesSymptoms of Diabetes
• Polyuria (increased urination)• Polydipsia (increased drinking)• Weight loss• Weakness• Increased infections and impaired healing• Blurred vision
33
• Normal range of fasting blood glucose:82 to 110 mg/dL
• Shortly after eating, it may go up to 140 mg/dL• Diagnosis of DIABETES is based on
Random glucose>200 mg/dL + symptoms
orFasting glucose
>126 mg/dL on 2 occasions
Diagnosis of DiabetesDiagnosis of Diabetes
34
• Definition: percentage of glycatedhemoglobin
• Glycated hemoglobin forms over the lifespan of RBCs in proportion to degree of glycemia
• Provides an estimate of the level of glycemia over lifetime of an RBC, or approximately 90 days
What is the HbA1c?What is the HbA1c?
35
• Currently HbA1c is used as:– Measure of glycemic control in diabetics – Indicator of risk level for diabetes complications– Measure of quality of diabetes care
BackgroundBackground
36
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 7
• Non‐diabetic– HbA1c < 6.0– Fasting plasma glucose < 100
• Prediabetes– HbA1c 6.0‐6.4– Fasting plasma glucose 100‐125
• Diabetes– HbA1c ≥ 6.5– Fasting plasma glucose ≥ 126
Current DefinitionsCurrent Definitions
37
• Type 1– Insulin subq.
• Type 2– Metformin– Diet– Exercise– Weight loss– Lots of newer drug (insulin sensitizers etc.), many in clinical trials, more coming
• Maintain HbA1c between 6.5% and 7%
Treatment of diabetesTreatment of diabetes
38
– In type 1 patients only– Marked hyperglycemia (high serum glucose) causes osmotic diuresis
– Patient loses excess water, Na, K, and ketones released from the liver cause a metabolic acidosis
– Precipitated by an infection, insulin error or omission, or occurs in a previously undiagnosed patient
– Treated with insulin, fluid replacement, K replacement
Diabetic emergencies: ketoacidosisDiabetic emergencies: ketoacidosis
39
May occur with an overdose of insulin / oral medication or a missed meal– Patient gets diaphoretic, weak, shaky, palpitations, difficulty thinking, aggressive, vision changes and may lose consciousness
– Patient needs glucose – a glass of juice, a candy, or if comatose, IV 50% glucose solution or IM glucagon (1 mg)
– Some patients are totally unaware of their hypoglycemia until they lose consciousness
Emergencies: hypoglycemiaEmergencies: hypoglycemia
40
• Assess control / severity /compliance– When were they first diagnosed – Type 1 vs Type 2– What medications are they taking (or diet only)– How much insulin do they use / how frequently– How often do they measure their glucose and
what are their usual measurements– Frequency of hypoglycemic reactions (can they feel them coming on?)
– Complications: brain, eye, heart, kidney, toes– How often and when last did they see their MD– Did they take meds and have meals today
Dental managementDental management
41
• Treatment plan modification– AM appointments– Normal meds and diet pre‐op– Limit treatment duration– Antibiotic coverage???– Post‐op diet instructions– Hospitalization for larger surgeries– Consultation with the MD
Dental managementDental management
42
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 8
Dental managementDental management
• Take the patient’s blood glucose
• Device can be purchased online for $10‐$20
• 3 components– Meter– Lancet (some comes with Meter) ($0.10)
– Test strips ($0.10)
43
• video
How to measure glucose levelHow to measure glucose level
44
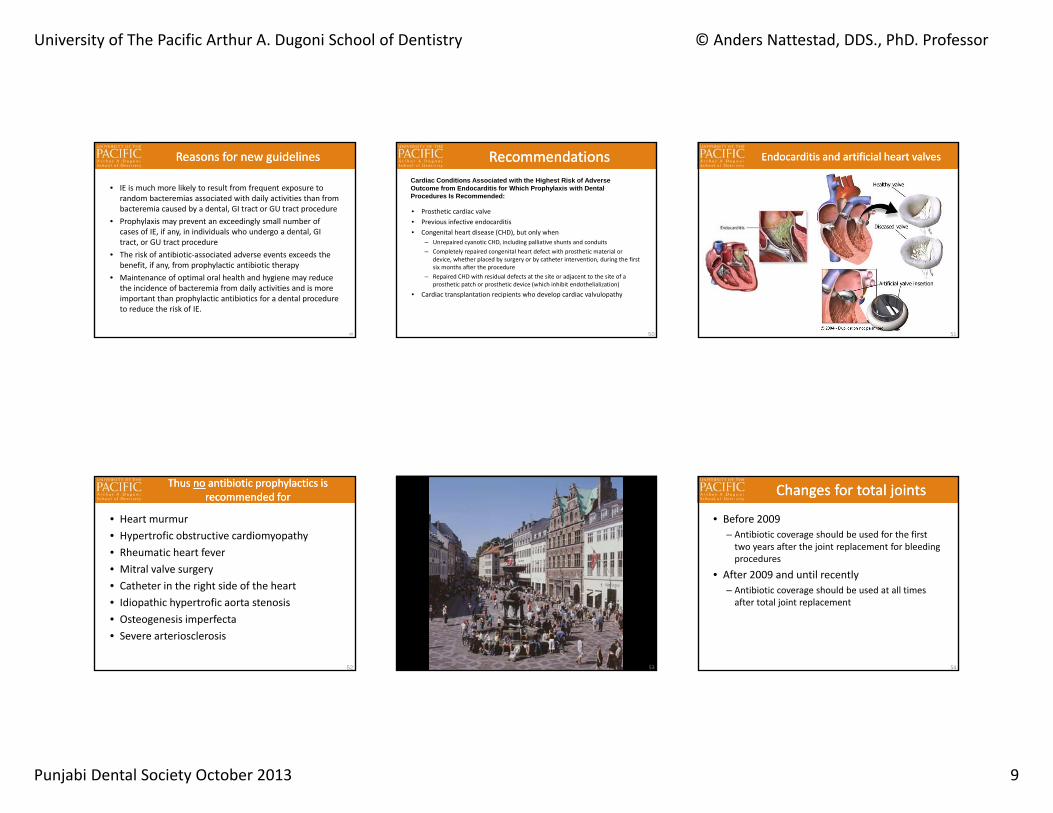
Sugar levels (80‐110 mg/dL)Sugar levels (80‐110 mg/dL)
http://en.wikipedia.org/wiki/Blood_sugar
45
46
Guidelines ‐ Prophylactic use of antibioticsGuidelines ‐ Prophylactic use of antibiotics
47
Guidelines for prophylactic antibiotics (CVD only)
Guidelines for prophylactic antibiotics (CVD only)
• AHA and ADA:“For decades, the American Heart Association (AHA) recommended that patients with certain heart conditions take antibiotics shortly before dental treatment. This was done with the belief that antibiotics would prevent infective endocarditis. The AHA recommends that most of these patients no longer need short‐term antibiotics as a preventive measure before their dental treatment”
48http://www.ada.org/prof/resources/topics/infective_endocarditis.asp 4/19/07
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 9
Reasons for new guidelinesReasons for new guidelines
• IE is much more likely to result from frequent exposure to random bacteremias associated with daily activities than from bacteremia caused by a dental, GI tract or GU tract procedure
• Prophylaxis may prevent an exceedingly small number of cases of IE, if any, in individuals who undergo a dental, GI tract, or GU tract procedure
• The risk of antibiotic‐associated adverse events exceeds the benefit, if any, from prophylactic antibiotic therapy
• Maintenance of optimal oral health and hygiene may reduce the incidence of bacteremia from daily activities and is more important than prophylactic antibiotics for a dental procedure to reduce the risk of IE.
49
RecommendationsRecommendations
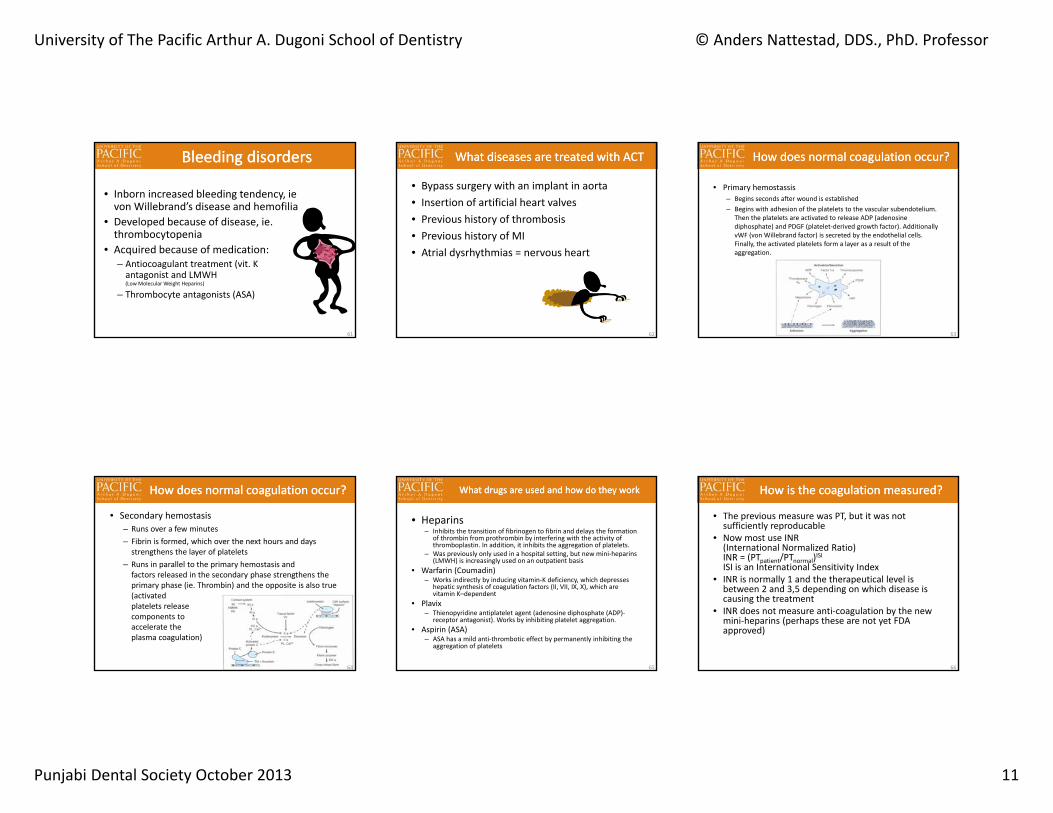
• Prosthetic cardiac valve• Previous infective endocarditis• Congenital heart disease (CHD), but only when
– Unrepaired cyanotic CHD, including palliative shunts and conduits– Completely repaired congenital heart defect with prosthetic material or
device, whether placed by surgery or by catheter intervention, during the first six months after the procedure
– Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization)
• Cardiac transplantation recipients who develop cardiac valvulopathy
50
Cardiac Conditions Associated with the Highest Risk of Adverse Outcome from Endocarditis for Which Prophylaxis with Dental Procedures Is Recommended:
Endocarditis and artificial heart valvesEndocarditis and artificial heart valves
51
Thus no antibiotic prophylactics is recommended for
Thus no antibiotic prophylactics is recommended for
• Heart murmur• Hypertrofic obstructive cardiomyopathy• Rheumatic heart fever• Mitral valve surgery• Catheter in the right side of the heart• Idiopathic hypertrofic aorta stenosis• Osteogenesis imperfecta• Severe arteriosclerosis
52 53
• Before 2009– Antibiotic coverage should be used for the first two years after the joint replacement for bleeding procedures
• After 2009 and until recently– Antibiotic coverage should be used at all times after total joint replacement
Changes for total jointsChanges for total joints
54
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 10
• The most current guidelines for managing patients with prosthetic joints is:
• Prevention of Orthopedic Implant Infection in Patients Undergoing Dental Procedure, jointly published by the American Dental Association (ADA) and the American Academy of Orthopedic Surgeons (AAOS), December 18, 2012
Changes with joint replacementChanges with joint replacement
55
“The practitioner might consider discontinuing the practice of routinely prescribing prophylactic antibiotics for patients with hip and knee prosthetic joint implants undergoing dental procedures”
Changes with joint replacementChanges with joint replacement
56
“The review committee was unable to recommend for or against the use of topical oral antimicrobials (Chlorhexidine 0.12%) in patients with prosthetic joint implants or other orthopedic implants undergoing dental procedures”
Changes with joint replacementChanges with joint replacement
57
“In the absence of reliable evidence linking poor oral health to prosthetic joint infection, it is the opinion of the work group that patients with prosthetic joint implants or other orthopedic implants maintain appropriate oral hygiene”
Changes with joint replacementChanges with joint replacement
58
• 1. NOT ROUTINELY RECOMMEND ANTIBIOTIC PREMEDICATION FOR PROSTHETIC HIP AND KNEES, AS PER RECOMMENDATION #1 ABOVE, SINCE THERE IS NO DATA TO SUPPORT THAT GIVING PROPHYLACTIC ANTIBIOTICS FOR DENTAL PROCEDURES, PREVENTS PROSTHETIC JOINT INFECTIONS.
• 2. IN SITUATIONS WHERE THE PATIENT IS MEDICALLY COMPROMISED AND MAY BE PRONE TO INFECTIONS, SUCH AS UNCONTROLLED DIABETES, CHRONIC STEROID USE OR IMMUNOSUPRESSED FOR ANY REASON, UNDERGOING CANCER CHEMOTHERAPY OR THE JOINT HAS BEEN INFECTED BEFORE, PREMEDICATION USING THE MEDICATIONS IN THE 2003 AAOS/ADA GUIDELINES AND THE CURRENT AHA GUIDELINE, WOULD BE THE MOST EFFECTIVE AGAINST COMMON ORAL ORGANISMS:
• o Amoxicillin (2 grams) or, if allergic, Clindamycin (600 mg), 30‐60 minutes before the appointment
• 3. PATIENTS WITH PROSTHETIC ORTHOPAEDIC IMPLANTS SHOULD MAINTAIN OPTIMUM ORAL HYGIENE, BUT SO SHOULD EVERYONE.
A practical clinical interpretation of the new guidelines is
A practical clinical interpretation of the new guidelines is
59 60
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 11
Bleeding disordersBleeding disorders
• Inborn increased bleeding tendency, ie von Willebrand’s disease and hemofilia
• Developed because of disease, ie. thrombocytopenia
• Acquired because of medication:– Antiocoagulant treatment (vit. K antagonist and LMWH (Low Molecular Weight Heparins)
– Thrombocyte antagonists (ASA)
61
What diseases are treated with ACTWhat diseases are treated with ACT
• Bypass surgery with an implant in aorta• Insertion of artificial heart valves• Previous history of thrombosis• Previous history of MI• Atrial dysrhythmias = nervous heart
62
How does normal coagulation occur?How does normal coagulation occur?
• Primary hemostassis– Begins seconds after wound is established– Begins with adhesion of the platelets to the vascular subendotelium.
Then the platelets are activated to release ADP (adenosine diphosphate) and PDGF (platelet‐derived growth factor). Additionally vWF (von Willebrand factor) is secreted by the endothelial cells. Finally, the activated platelets form a layer as a result of the aggregation.
63
How does normal coagulation occur?How does normal coagulation occur?
• Secondary hemostasis– Runs over a few minutes– Fibrin is formed, which over the next hours and days strengthens the layer of platelets
– Runs in parallel to the primary hemostasis and factors released in the secondary phase strengthens the primary phase (ie. Thrombin) and the opposite is also true (activated platelets release components to accelerate the plasma coagulation)
64
What drugs are used and how do they workWhat drugs are used and how do they work
• Heparins– Inhibits the transition of fibrinogen to fibrin and delays the formation
of thrombin from prothrombin by interfering with the activity of thromboplastin. In addition, it inhibits the aggregation of platelets.
– Was previously only used in a hospital setting, but new mini‐heparins (LMWH) is increasingly used on an outpatient basis
• Warfarin (Coumadin)– Works indirectly by inducing vitamin‐K deficiency, which depresses
hepatic synthesis of coagulation factors (II, VII, IX, X), which are vitamin K–dependent
• Plavix– Thienopyridine antiplatelet agent (adenosine diphosphate (ADP)‐
receptor antagonist). Works by inhibiting platelet aggregation. • Aspirin (ASA)
– ASA has a mild anti‐thrombotic effect by permanently inhibiting the aggregation of platelets
65
How is the coagulation measured?How is the coagulation measured?
• The previous measure was PT, but it was not sufficiently reproducable
• Now most use INR (International Normalized Ratio)INR = (PTpatient/PTnormal)ISIISI is an International Sensitivity Index
• INR is normally 1 and the therapeutical level is between 2 and 3,5 depending on which disease is causing the treatment
• INR does not measure anti‐coagulation by the new mini‐heparins (perhaps these are not yet FDA approved)
66
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 12
Traditional guidelinesTraditional guidelines
• Avoid using aspirin, NSAID og corticosteroids• Get the INR measured on the morning of a planned major bleeding treatment
• The warfarin is reduced or stopped a few days prior to the bleeding treatment and resumed on the following evening. Normally the INR will be reduced by 0.5‐1 per day when warfarin is stopped.
• The INR must be below 1,7
67
New informationNew information
68
New informationNew information
69
New informationNew information
70
New informationNew information
71
Alternative measures to secure hemostasisAlternative measures to secure hemostasis
• Use all local measures including– Removal of granulation tissue– Place an absorbable gelatin sponge with hemostatic agent (Surgicel)
– Suture after extraction • Let patient rinse with tranexamic acid 5% for two minutes several times daily
• If all other failes, refer to hospital where Vit. K can be given if indicated (Pts on Coumadin)
72
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 13
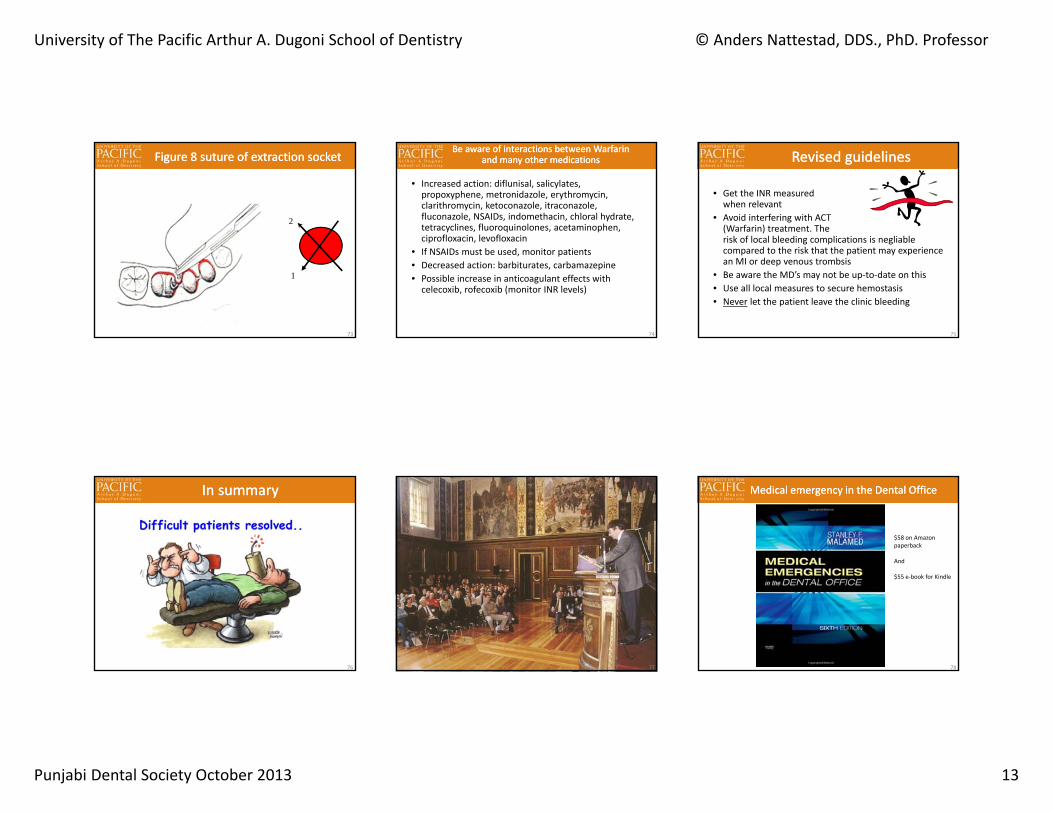
Figure 8 suture of extraction socketFigure 8 suture of extraction socket
1
2
73
Be aware of interactions between Warfarin and many other medications
Be aware of interactions between Warfarin and many other medications
• Increased action: diflunisal, salicylates, propoxyphene, metronidazole, erythromycin, clarithromycin, ketoconazole, itraconazole, fluconazole, NSAIDs, indomethacin, chloral hydrate, tetracyclines, fluoroquinolones, acetaminophen, ciprofloxacin, levofloxacin
• If NSAIDs must be used, monitor patients• Decreased action: barbiturates, carbamazepine• Possible increase in anticoagulant effects with celecoxib, rofecoxib (monitor INR levels)
74
Revised guidelinesRevised guidelines
• Get the INR measured when relevant
• Avoid interfering with ACT (Warfarin) treatment. The risk of local bleeding complications is negliable compared to the risk that the patient may experience an MI or deep venous trombsis
• Be aware the MD’s may not be up‐to‐date on this• Use all local measures to secure hemostasis• Never let the patient leave the clinic bleeding
75
In summaryIn summary
76 77 78
Medical emergency in the Dental OfficeMedical emergency in the Dental Office
$58 on Amazonpaperback
And
$55 e‐book for Kindle
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 14
79
Systemic ComplicationsSystemic Complications
• A survey of 3000 injection showed a complication frequency of 2.5%, of which none were serious. Other surveys show incidences of 5%
• On average, a dentist will do approx.2000 injections per year and thus have about 50‐100 complications per year
EpidemiologyEpidemiology
80
Systemic complications ‐ categoriesSystemic complications ‐ categories
•Non drug related reactions•Psychogenic reaction
•Adverse drug reactions• Toxic reactions•Allergic reactions
81
Psychogenic reactionsPsychogenic reactions
“Anxiety‐induced events are by far the most common adverse reaction associated with local anesthetics in dentistry. These may manifest in numerous ways, the most common of which is syncope. In addition, they may present with a wide variety of symptoms, including hyperventilation, nausea, vomiting and alterations in heart rate or blood pressure. Psychogenic reactions are often misdiagnosed as allergic reactions …
82
Systemic ComplicationsSystemic Complications Vasovagal syncopeVasovagal syncope
83 84
Vasovagal syncopeVasovagal syncopeThe initial event in a vasovagal syncopal episode is the stress‐induced release of increased amounts of catecholamines that cause a decrease in peripheral vascular resistance, tachycardia, and sweating. The patient may complain of feeling generalized warmth, nausea, and palpitations. As blood pools in the periphery, a drop in the arterial blood pressure appears, with a corresponding decrease in cerebral blood flow. The patient may then complain of feeling dizzy or weak. Compensatory mechanisms attempt to maintain adequate blood pressure, but they soon fade, leading to vagally mediated bradycardia. Once the blood pressure drops below levels necessary to sustain consciousness, syncope occurs
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 15
• If patient is not already lying down, change chair position to horizontal and consider a passive leg raise
• Cold compress on forehead• Inflict pain to get patientto react and wake
• Oxygen does not harm• Ammonia inhalants are quiteaggressive, but can be usedas a last resort
Syncope ‐ How to manage?Syncope ‐ How to manage?
85
Old description of the Trendelenburg position.
• Ask patients if they have ever experienced any problems when going to the dental office
• If patients are very anxious, consider using a short acting benzodiazepine 1 hour before the appointment (Xanax 0.5 mg)
• Have the patient lie back in the dental chair while giving anesthesia
How to prevent syncopeHow to prevent syncope
86
HyperventilationHyperventilation
Causes: –Acute anxiety attack, –Metabolic and endocrinologic disorders (hypoglycemia, hyperthyroidism, Cushing’s syndrome, pheochromocytoma).
87
Signs/Symptoms:1. Tachypnea2. Tachycardia3. Parasthesia around mouth
and fingers4. Tetany, cramps5. Nausea6. Faintness7. Diaphoresis8. Acute anxiety9. Shortness of breath
HyperventilationHyperventilationTreatment:1. Assure patient airway2. Reassure patient3. Slow down breathing4. Have patient “re‐breathe”
in a paper bag or mask
88
• The vast majority of medical emergency incidents are non drug related, but simply vasovagal syncope
• Alternative reasons include– Adverse drug reactions (toxicity)– Allergies
What else could it be?What else could it be?
89 90
Adverse Drug Reactions ‐ ToxicAdverse Drug Reactions ‐ Toxic
• The toxicity of local anesthetics is a function of systemic absorption. High blood levels of the drug may be due to– Repeated injections – too high dose– Inadvertent intravascular administration– Increased susceptibility of the patient– Use of wrong drug (unlikely)
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 16
91
Clinical Manifestations of Local Anesthetic OverdoseClinical Manifestations of Local Anesthetic Overdose
92
Epinephrine overdoseEpinephrine overdose
93
Adverse Drug Reactions ‐ AllergyAdverse Drug Reactions ‐ Allergy
• Allergic reactions are extremely rare after introduction of the amide type of LA
• In cases of previous history of allergic reactions, a referral to a specialist or a hospital might be a good idea
94
Allergic reactionsAllergic reactions
Patients with sodium bisulfite allergy must not have LA with vasoconstrictor
Patients with sulfa allergy should not have articaine
AnaphylaxisAnaphylaxis
95 96
Allergic reactionsAllergic reactions
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 17
97
Management of allergic reactionsManagement of allergic reactions
98
Generalized anaphylaxisGeneralized anaphylaxis
• Acute life‐threatening allergic reaction• Can lead to death in a few minutes• Clinical signs:
– Skin reactions– Smooth muscle spasm of the gastrointestinal and genitourinary tracts and respiratory smooth muscle (bronchospasm)
– Respiratory distress– Cardiovascular collapse
99
Management of generalized anaphylaxisManagement of generalized anaphylaxis
• Administer 0.3 mg (0.15 mg for a child) epinephrine IM or subcutaneously (SC)
• Administer IM histamine blocker: 50 mg diphenhydramine (25 mg for a child) or 10 mg chlorpheniramine (5 mg for a child).
• Look out for bronchospasms and laryngeal edema
100
Contraindications for Local AnestheticsContraindications for Local Anesthetics
101
When something goes wrong..When something goes wrong.. Chain of survivalChain of survival
Call 911 CPR Defib Advanced Txin hospital
102
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 18
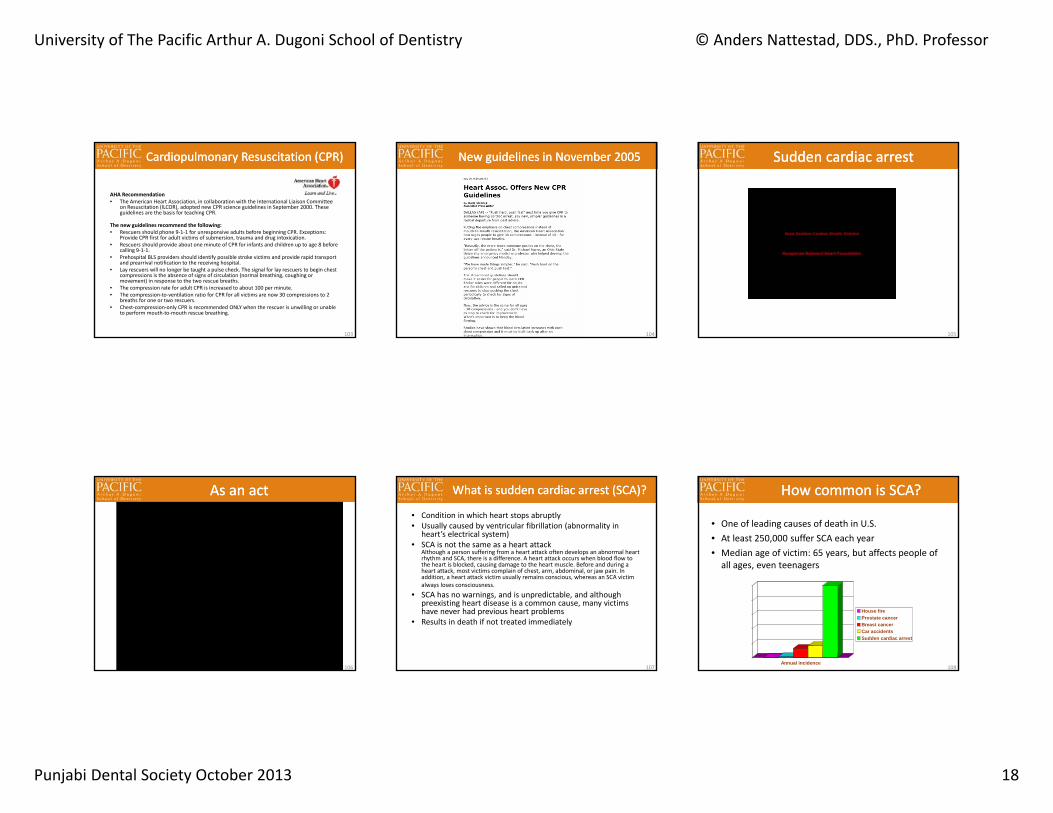
Cardiopulmonary Resuscitation (CPR)Cardiopulmonary Resuscitation (CPR)
AHA Recommendation• The American Heart Association, in collaboration with the International Liaison Committee
on Resuscitation (ILCOR), adopted new CPR science guidelines in September 2000. These guidelines are the basis for teaching CPR.
The new guidelines recommend the following:• Rescuers should phone 9‐1‐1 for unresponsive adults before beginning CPR. Exceptions:
Provide CPR first for adult victims of submersion, trauma and drug intoxication. • Rescuers should provide about one minute of CPR for infants and children up to age 8 before
calling 9‐1‐1. • Prehospital BLS providers should identify possible stroke victims and provide rapid transport
and prearrival notification to the receiving hospital. • Lay rescuers will no longer be taught a pulse check. The signal for lay rescuers to begin chest
compressions is the absence of signs of circulation (normal breathing, coughing or movement) in response to the two rescue breaths.
• The compression rate for adult CPR is increased to about 100 per minute. • The compression‐to‐ventilation ratio for CPR for all victims are now 30 compressions to 2
breaths for one or two rescuers. • Chest‐compression‐only CPR is recommended ONLY when the rescuer is unwilling or unable
to perform mouth‐to‐mouth rescue breathing.
103
New guidelines in November 2005New guidelines in November 2005
104
Sudden cardiac arrestSudden cardiac arrest
105
As an actAs an act
106
What is sudden cardiac arrest (SCA)?What is sudden cardiac arrest (SCA)?
• Condition in which heart stops abruptly• Usually caused by ventricular fibrillation (abnormality in
heart’s electrical system)• SCA is not the same as a heart attack
Although a person suffering from a heart attack often develops an abnormal heart rhythm and SCA, there is a difference. A heart attack occurs when blood flow to the heart is blocked, causing damage to the heart muscle. Before and during a heart attack, most victims complain of chest, arm, abdominal, or jaw pain. In addition, a heart attack victim usually remains conscious, whereas an SCA victim always loses consciousness.
• SCA has no warnings, and is unpredictable, and although preexisting heart disease is a common cause, many victims have never had previous heart problems
• Results in death if not treated immediately
107
How common is SCA?How common is SCA?
• One of leading causes of death in U.S.• At least 250,000 suffer SCA each year• Median age of victim: 65 years, but affects people of all ages, even teenagers
0
50000
100000
150000
200000
250000
Annual incidence
House fireProstate cancerBreast cancerCar accidentsSudden cardiac arrest
108
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 19
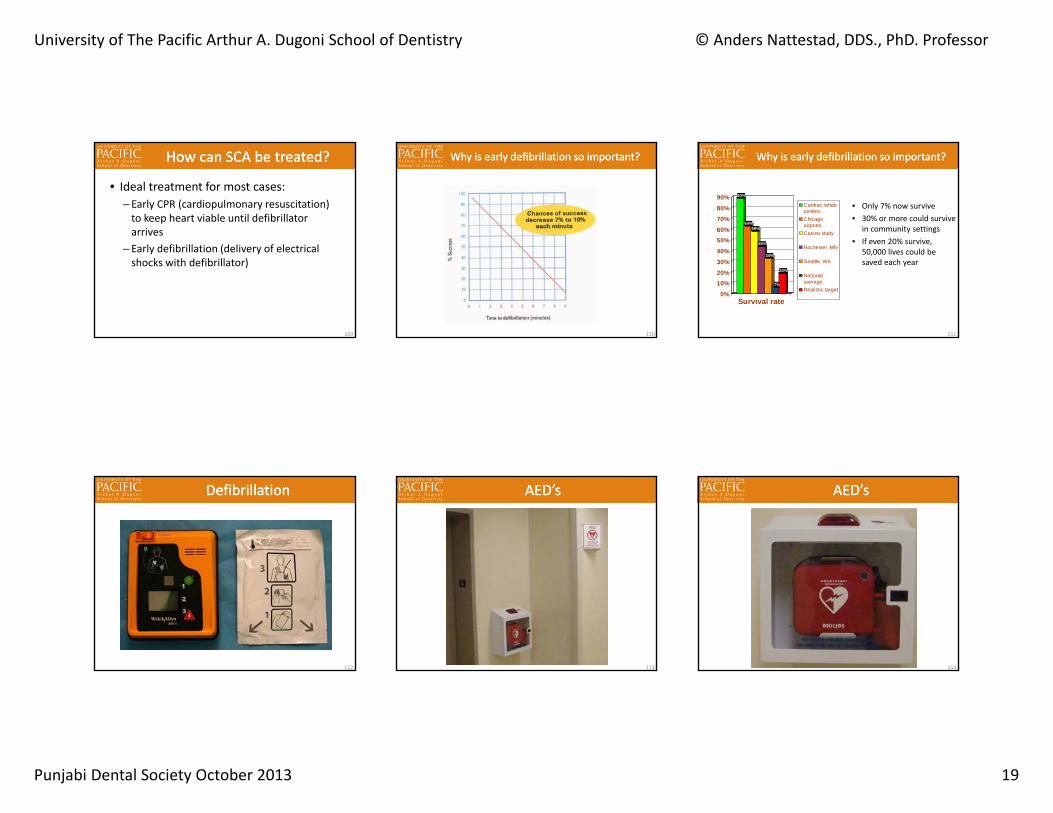
How can SCA be treated?How can SCA be treated?
• Ideal treatment for most cases: – Early CPR (cardiopulmonary resuscitation) to keep heart viable until defibrillator arrives
– Early defibrillation (delivery of electrical shocks with defibrillator)
109
Why is early defibrillation so important?Why is early defibrillation so important?
110
90%
64%59%
45%
34%
7%
20%
0%10%20%30%40%50%60%70%80%90%
Survival rate
Cardiac rehabcentersChicagoairportsCasino study
Rochester, MN
Seattle, WA
NationalaverageRealistic target
Why is early defibrillation so important?Why is early defibrillation so important?
• Only 7% now survive• 30% or more could survive
in community settings• If even 20% survive,
50,000 lives could be saved each year
111
DefibrillationDefibrillation
112
AED’sAED’s
113
AED’sAED’s
114
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 20
How to use an AEDHow to use an AED
Video demonstration
115
• Assess the patient• Monitor the patient
– Breathing– Oxygenation– Blood pressure– EKG– IV access– Drugs…
A Medical Emergency – What to do?A Medical Emergency – What to do?
116 117
ABCD AlgorithmABCD Algorithm
• Unresponsive patient (shake, shout and inflict pain all without reaction)
• Activate internal medical emergency response with a call to xxxx and say briefly what it is about and where (room number)
• Oral Surgery will bring crash cart including an AED (Automatic External Defibrillator)
• Oral Surgery will decide if a call to 911 should be made
118
ABCD AlgorithmABCD AlgorithmStart ABCD Airway: Open airway Breathing: Check breathing (look, listen and feel)
If breathing adequately, place in trendelburgs position (in chair with head maximum down) unless patient has symptoms of stroke. Monitor vital signs (pulse, breathing, BP and oxygenation (pulse-oxymeter), if all is normal and keeps being normal, wait for EMT to arrive and do an EKG. EMT will decide what next. If breathing inadequate, but all other vital signs normal, give passive oxygen with mask or nasal canula with flowrate of 12 L/Min
If not breathing:
Give two slow rescue breaths with bag on oxygen tank. Circulation: Monitor (look for breathing and pulse)
Yes, circulation found. Continue rescue breathing every 5 seconds (in children < 8 years: every three seconds). Monitor breathing and circulation every 30-60 seconds)
No circulation found
Perform CPR until AED is arrived and ready to attach Chest compressions (100 per minute) and rescue breathing (sequence: 30 compressions
and two breaths.
119
ABCD AlgorithmABCD Algorithm
Defibrillation when AED arrives: Power on AED Stop compressions and rescue breathing Attach electrodes as shown on illustration on electrode AED will analyze and shock as appropriate and instruct in further procedure (AED will shock
three times with increasing energy and will then ask for signs of circulation and if none ask for one minute of CPR. The AED will then shock another three times. This cycle will continuethree times.
When EMT arrives, inform them of the sequence of events and associated vital signs. Document the incident to the associate dean for clinical services using a standard form available online under DENINFO – Medical Emergencies
Acute Angina PectorisAcute Angina Pectoris
Cause: Diminished blood supply to myocardium due to an imbalance between myocardial oxygen supply and demand.
120
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 21
Signs/Symptoms:1.Chest pain –substernal pressure or crushing sensation. May radiate to neck, left shoulder and down arm, and left side of jaw.
Acute Angina PectorisAcute Angina Pectoris
Treatment:1. Place patient in supine position.2. Assure patient airway.3. Administer nitroglycerine – if patient’s
prescription not available – administer 0.3 mg sublingually.
4. If pain persists five minutes after nitroglycerine dose, repeat administration.
5. If still no response, repeat nitroglycerine and administer 100% oxygen.
6. If angina does not subside – concerned that myocardial infarction is developing. Transfer to emergency room.
121
Myocardial InfarctionMyocardial Infarction
Cause: Inadequate supply of oxygen to myocardium.
122
Signs/Symptoms:1. Chest pain – substernal pressure
or crushing sensation, may radiate to neck, left shoulder, down arm, left side of jaw.
2. Feeling of impending doom;3. Nausea.4. Pale and diaphoretic.
Myocardial InfarctionMyocardial InfarctionTreatment:1. Usually does not respond to
nitroglycerine.2. Administer 100% oxygen.3. Position patient in semi‐sitting
position.4. Transport to medical facility
immediately.• Note: Narcotics for pain should
be avoided initially, so as not to interfere with differential diagnosis, but if desired give Demerol 25‐75 mg IM or IV.
123
Asthmatic AttackAsthmatic Attack
Cause: Reversible bronchospasm.Two Subtypes: – Extrinsic or allergic type is caused by environmental allergens.
– Intrinsic (endogenous) type – mechanism inducing attacks is unknown.
124
Signs/Symptoms:1. Wheezing2. Effortless inspiration, prolonged
expiration 3. Compressed chest4. Severe attack
a. Tachypnea (>35) or Bradypnea(<12)
b. Exhaustion; altered consciousness
c. Use of accessory muscles of respiration
d. Cyanosise. Silent chest (i.e. no wheezing
with dyspnea and tachypnea)
Asthmatic AttackAsthmatic AttackTreatment:1. Put patient in sitting position;
assure patient airway; give 100% oxygen
2. Two inhalations of albuterol3. If no response to albuterol,
and in severe attacks, administer epinephrine
4. Contact patient’s physician
125
SeizuresSeizures
Causes: –Neurologic disorders – Syncope –Drug toxicity –Hypoxia
126
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 22
Signs/Symptoms:1. Involuntary or bizarre
movements2. Tongue biting3. Loss of consciousness
SeizuresSeizures
Treatment:1. Assure patient airway2. Protect patient from
damage to self3. Administer 100%
oxygen 4. Place soft/padded bite
protector 5. Transport to medical
facility
127
• Focus on– Monitoring– Airway maintenance– Capnography– Reversal agents
IV sedation emergenciesIV sedation emergencies
128
Oral IM IV Inhalation
Light sedation Yes with knowledge
Yes with more knowledge
Not necessary Nitrous only
Moderate sedation
Cannot be done safely
Tricky Yes, good combo
Not safe, IV is better
Deep sedation Cannot be done safely
Dangerous because of lack of titration
Yes, but airway skills required
Not safe, IV is better
General anesthesia
Cannot be done safely
Unsafe even with intubation
Requires intubation
Requiresintubation
Levels and drug deliveryLevels and drug delivery
129
130
Reversal agents / emergency drugsReversal agents / emergency drugs• Epinephrine• Naloxone (narcan)
– An opioid antagonist which binds to CNS opioid receptors to displace opioid agonists
– Reverses respiratory depression and sedation associated with opioids– Very safe = used freely if drug overdose is suspected
• Flumazenil– Binds to GABA receptors in the CNS to reverse effects of
benzodiazepines• Atropine
– Anticholinergic ‐ Used when significant bradycardia or asystole• Ephedrine
– Sympathomimetic ‐ used for hypotension
Reversal Agents: FlumazenilReversal Agents: Flumazenil
• The half‐life of oral BZDs may be >12 hrs; flumazenil’s half‐life is only ~45 min.
• Patients will require monitoring for 1 hr. after last dose of flumazenil
131 132
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 23
133
Medical EmergenciesEquipment and drugsMedical EmergenciesEquipment and drugs
• Crash Cart
134
Oxygen for emergenciesOxygen for emergencies
• Content– Oxygen tank– AMBU bag incl. mask
and reservoir
• Indication: All patients undergoing a medical emergency with free airways
• If the patient is not breathing, use reservoir to give rescue breathing
• The normal flow is about 6 liters per minute
• Maintain oxygen until EMT arrives
135
Update on medical emergenciesUpdate on medical emergencies
• Pulse‐oximeter
136
Assessment of glucose levelAssessment of glucose level
• Blood glucose
Normal level70‐125 mg/dl
137
Blood pressureBlood pressure
138
Emergency medicationsEmergency medications
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 24
139
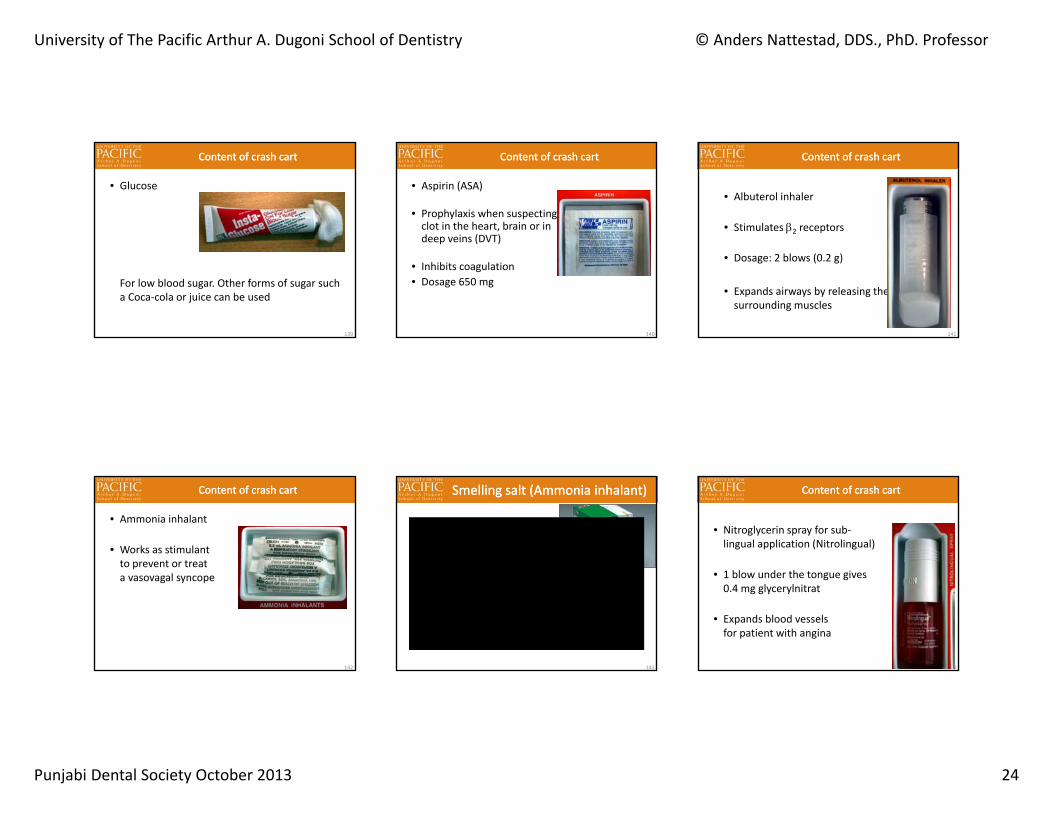
Content of crash cartContent of crash cart
• Glucose
For low blood sugar. Other forms of sugar such a Coca‐cola or juice can be used
140
Content of crash cartContent of crash cart
• Aspirin (ASA)
• Prophylaxis when suspecting clot in the heart, brain or in deep veins (DVT)
• Inhibits coagulation• Dosage 650 mg
141
Content of crash cartContent of crash cart
• Albuterol inhaler
• Stimulates 2 receptors
• Dosage: 2 blows (0.2 g)
• Expands airways by releasing the surrounding muscles
142
Content of crash cartContent of crash cart
• Ammonia inhalant
• Works as stimulantto prevent or treata vasovagal syncope
Smelling salt (Ammonia inhalant)Smelling salt (Ammonia inhalant)
143 144
Content of crash cartContent of crash cart
• Nitroglycerin spray for sub‐lingual application (Nitrolingual)
• 1 blow under the tongue gives0.4 mg glycerylnitrat
• Expands blood vesselsfor patient with angina
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 25
145
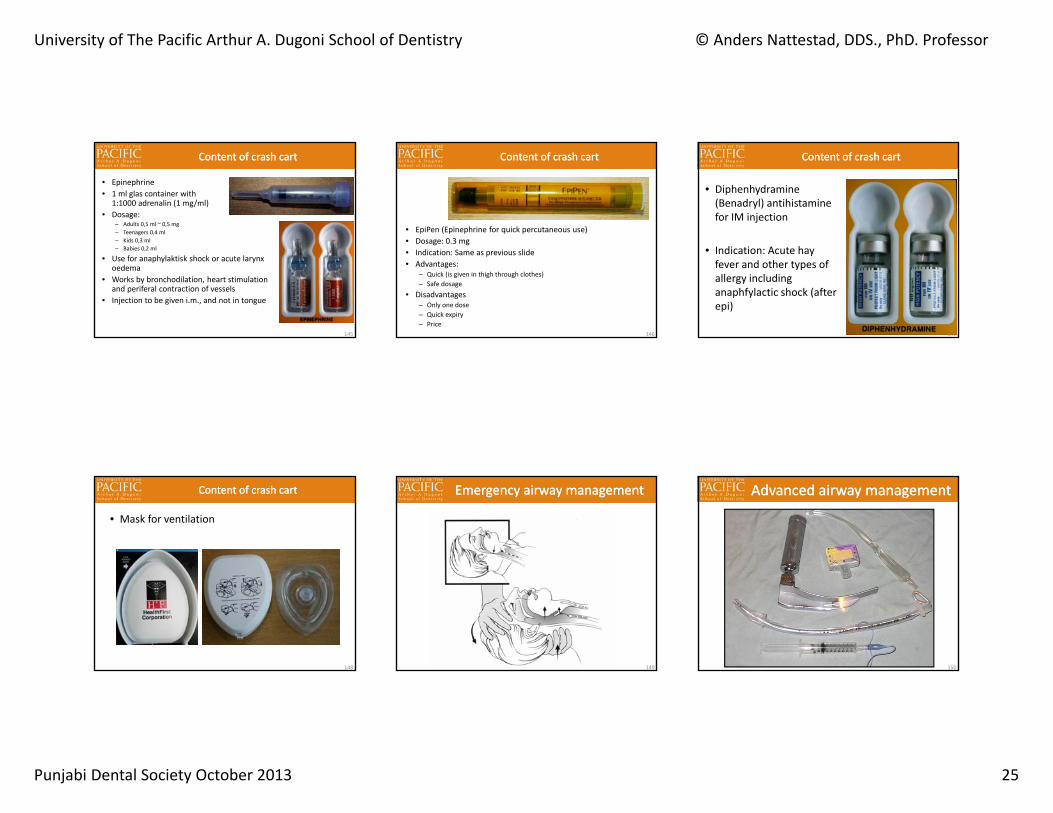
Content of crash cartContent of crash cart
• Epinephrine • 1 ml glas container with
1:1000 adrenalin (1 mg/ml)• Dosage:
– Adults 0,5 ml ~ 0,5 mg– Teenagers 0,4 ml– Kids 0,3 ml– Babies 0,2 ml
• Use for anaphylaktisk shock or acute larynx oedema
• Works by bronchodilation, heart stimulation and periferal contraction of vessels
• Injection to be given i.m., and not in tongue
146
Content of crash cartContent of crash cart
• EpiPen (Epinephrine for quick percutaneous use)• Dosage: 0.3 mg • Indication: Same as previous slide• Advantages:
– Quick (is given in thigh through clothes)– Safe dosage
• Disadvantages– Only one dose– Quick expiry– Price
147
Content of crash cartContent of crash cart
• Diphenhydramine (Benadryl) antihistaminefor IM injection
• Indication: Acute hay fever and other types of allergy including anaphfylactic shock (after epi)
148
Content of crash cartContent of crash cart
• Mask for ventilation
149
Emergency airway managementEmergency airway management
150
Advanced airway managementAdvanced airway management
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 26
151
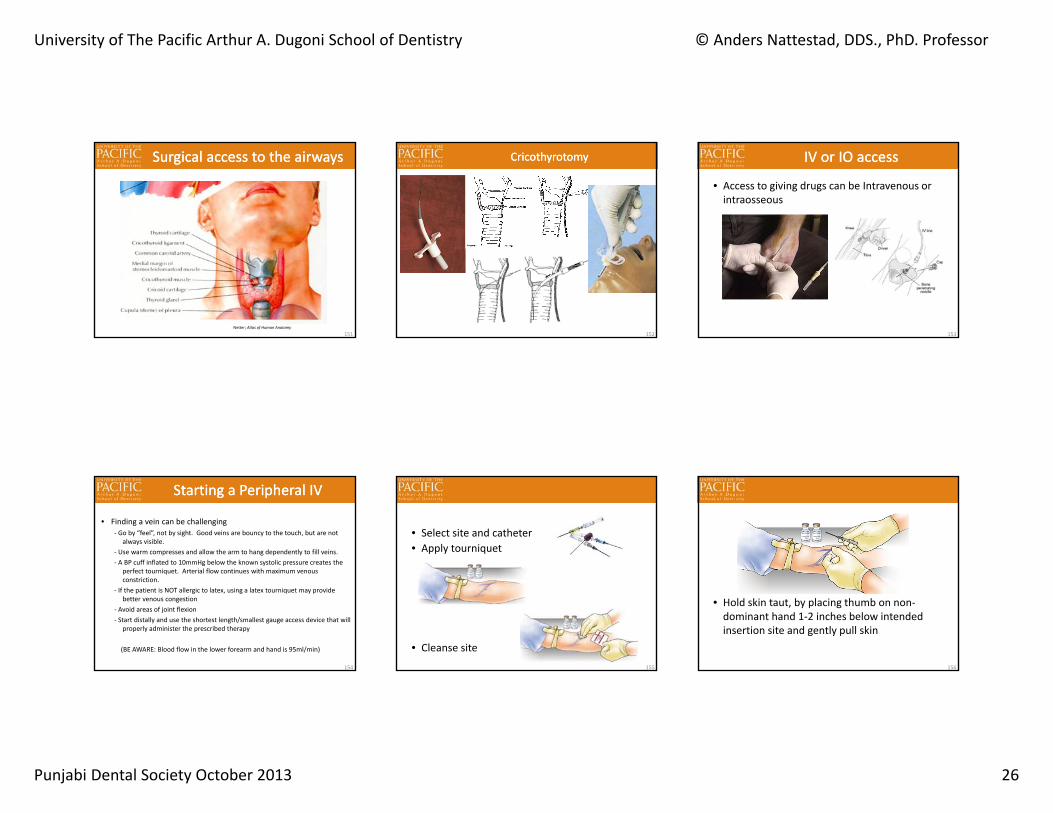
Surgical access to the airwaysSurgical access to the airways
Netter; Atlas of Human Anatomy
152
Cricothyrotomy Cricothyrotomy
• Access to giving drugs can be Intravenous or intraosseous
IV or IO accessIV or IO access
153
Starting a Peripheral IVStarting a Peripheral IV
• Finding a vein can be challenging‐ Go by “feel”, not by sight. Good veins are bouncy to the touch, but are not
always visible.‐ Use warm compresses and allow the arm to hang dependently to fill veins.‐ A BP cuff inflated to 10mmHg below the known systolic pressure creates the
perfect tourniquet. Arterial flow continues with maximum venous constriction.
‐ If the patient is NOT allergic to latex, using a latex tourniquet may provide better venous congestion
‐ Avoid areas of joint flexion‐ Start distally and use the shortest length/smallest gauge access device that will
properly administer the prescribed therapy
(BE AWARE: Blood flow in the lower forearm and hand is 95ml/min)
154
• Select site and catheter• Apply tourniquet
• Cleanse site155
• Hold skin taut, by placing thumb on non‐dominant hand 1‐2 inches below intended insertion site and gently pull skin
156
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 27
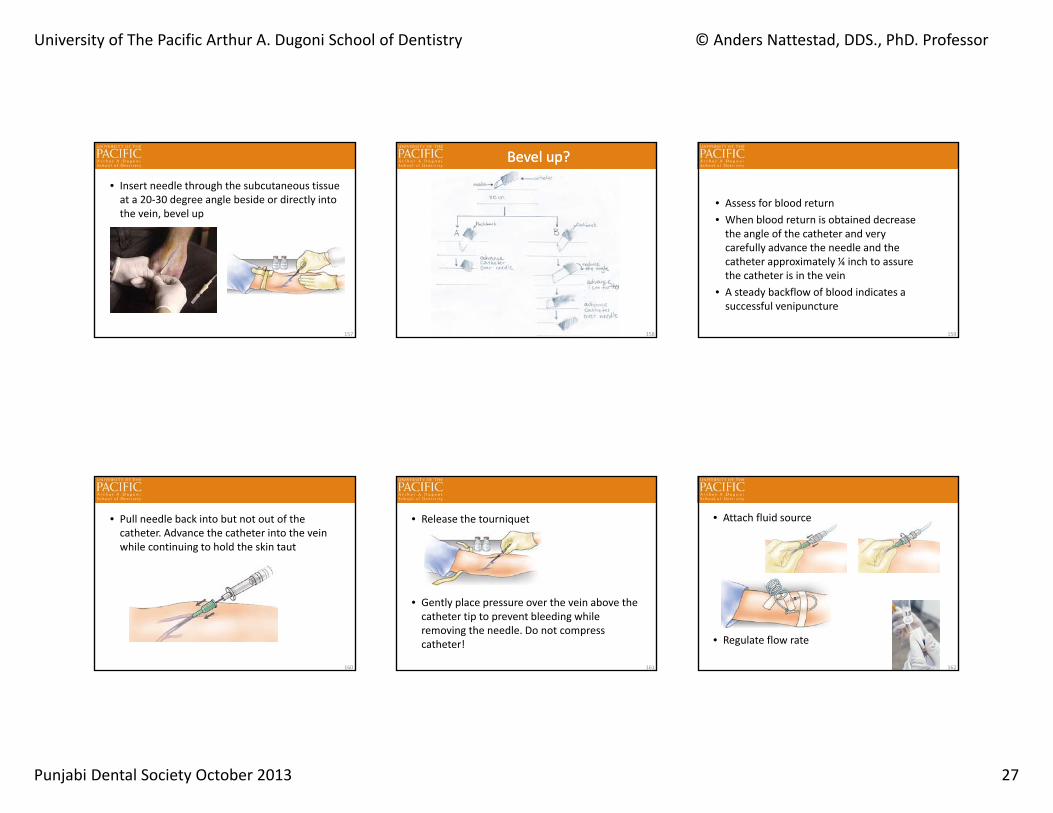
• Insert needle through the subcutaneous tissue at a 20‐30 degree angle beside or directly into the vein, bevel up
157
Bevel up?Bevel up?
158
• Assess for blood return• When blood return is obtained decrease the angle of the catheter and very carefully advance the needle and the catheter approximately ¼ inch to assure the catheter is in the vein
• A steady backflow of blood indicates a successful venipuncture
159
• Pull needle back into but not out of the catheter. Advance the catheter into the vein while continuing to hold the skin taut
160
• Release the tourniquet
• Gently place pressure over the vein above the catheter tip to prevent bleeding while removing the needle. Do not compress catheter!
161
• Attach fluid source
• Regulate flow rate
162
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 28
IO (intraosseous) accessIO (intraosseous) access
http://www.waismed.com/BIGmovie.html163 164 165
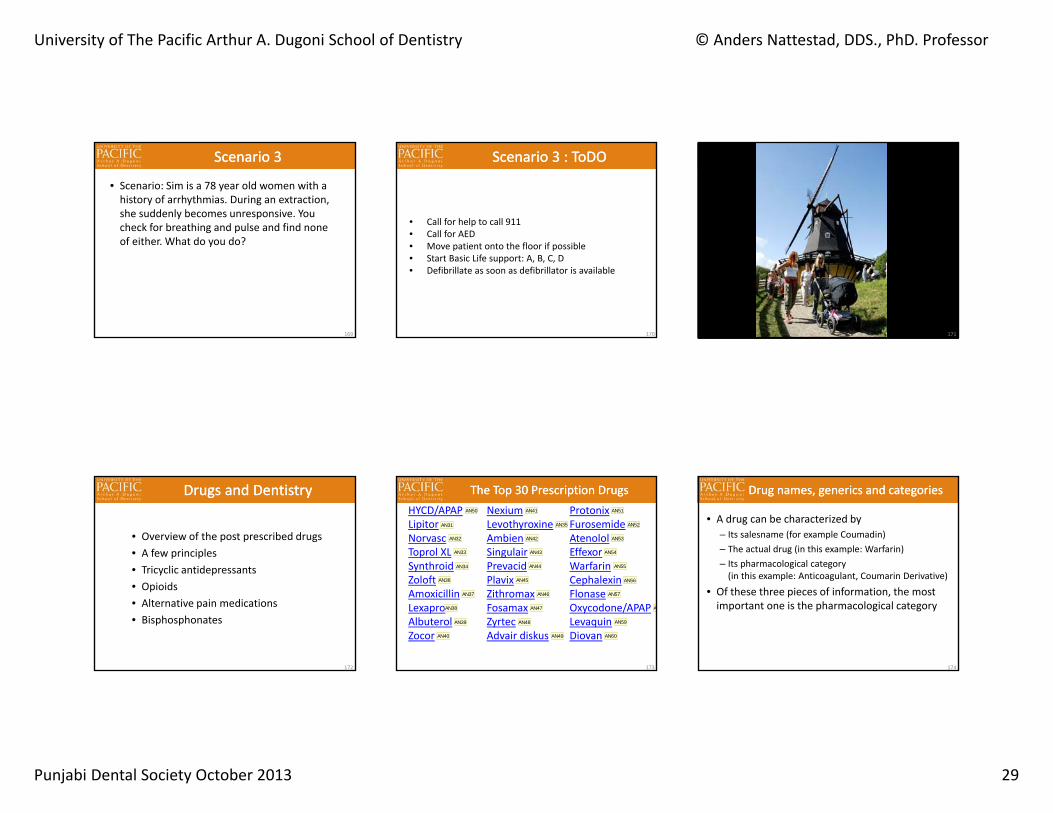
Scenario 1Scenario 1
• Scenario: Sim is an 18 year old male sitting in chair having local anesthesia applied and just after administration he complains of being dizzy and just after that he faints. You check for breathing and pulse, and find that both are normal. What do you do?
166
Scenario 1 : ToDOScenario 1 : ToDO
• Call faculty • Place chair in maximum trendelburg and bend legs
towards chest• Get patient attention with talk or contact, inflicting
pain is optional, ammonium salt is optional• Placement of cold cloth on forehead is optional• Place puls‐ox to monitor oxygenation of the blood,
Passive flow oxygen can be provided if Puls‐Ox reading is low (< 95)
167
Scenario 2Scenario 2
• Scenario: Sim is a 65 year old overweight Man with a history of high blood pressure. His BP is 160/100 and he is on a diuretic and a calcium channel blocker, both of which he has not been taking for over two weeks for financial reasons. During impression for a crown on #3 he complains of severe chest pain radiating out into his left arm and develops nausea and shortness of breath. What do you do?
168
Chest pain algorithmChest pain algorithm
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 29
169
Scenario 3Scenario 3
• Scenario: Sim is a 78 year old women with a history of arrhythmias. During an extraction, she suddenly becomes unresponsive. You check for breathing and pulse and find none of either. What do you do?
170
Scenario 3 : ToDOScenario 3 : ToDO
• Call for help to call 911• Call for AED• Move patient onto the floor if possible• Start Basic Life support: A, B, C, D• Defibrillate as soon as defibrillator is available
171
• Overview of the post prescribed drugs• A few principles• Tricyclic antidepressants• Opioids• Alternative pain medications• Bisphosphonates
Drugs and DentistryDrugs and Dentistry
172
HYCD/APAPLipitorNorvascToprol XLSynthroidZoloftAmoxicillinLexaproAlbuterolZocor
The Top 30 Prescription DrugsThe Top 30 Prescription DrugsNexiumLevothyroxineAmbienSingulairPrevacidPlavixZithromaxFosamaxZyrtecAdvair diskus
ProtonixFurosemideAtenololEffexorWarfarinCephalexinFlonaseOxycodone/APAPLevaquinDiovan
173
AN31
AN32
AN33
AN34
AN35
AN36
AN37
AN38
AN39
AN40
AN41
AN42
AN43
AN44
AN45
AN46
AN47
AN48
AN49
AN50 AN51
AN52
AN53
AN54
AN55
AN56
AN57
AN
AN59
AN60
• A drug can be characterized by– Its salesname (for example Coumadin)– The actual drug (in this example: Warfarin)– Its pharmacological category (in this example: Anticoagulant, Coumarin Derivative)
• Of these three pieces of information, the most important one is the pharmacological category
Drug names, generics and categoriesDrug names, generics and categories
174
Slide 173
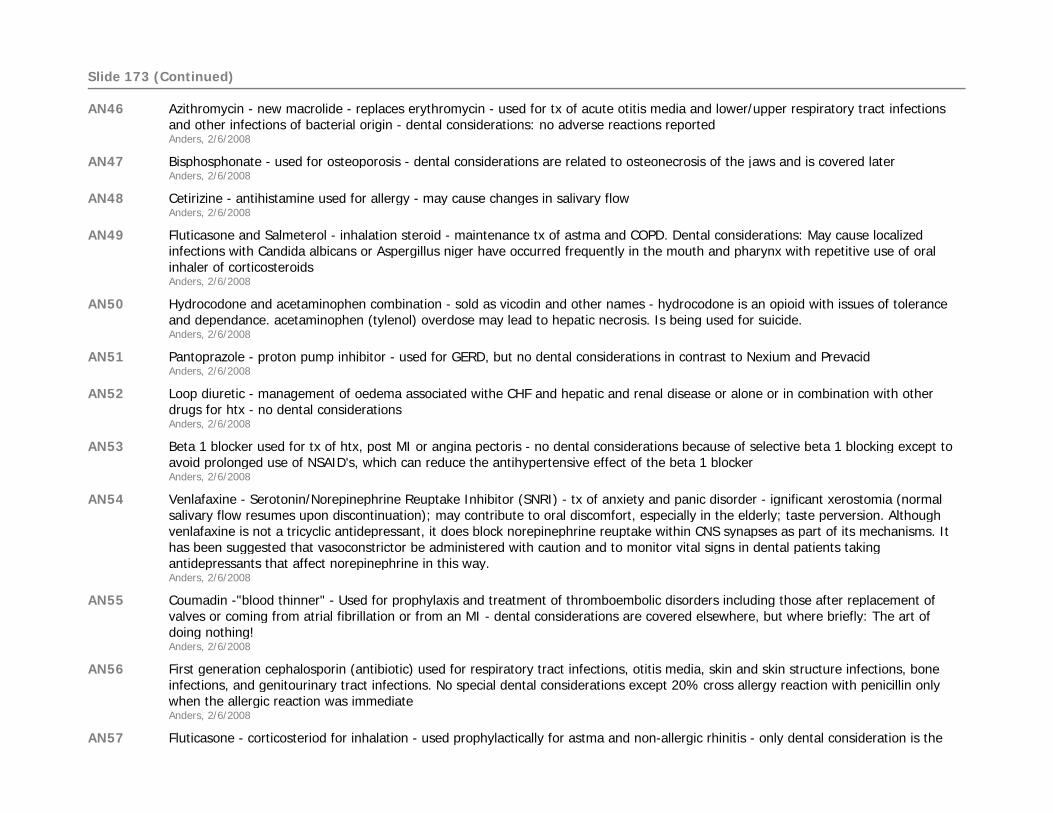
AN31 Lower cholesterol - no dental considerationsAnders, 2/6/2008
AN32 Amlopidine - Calcium Channel blocker - lower blood pressure - rare gingival hyperplasia compared to other CCB'sAnders, 2/6/2008
AN33 Metropolol - beta 1 blocker - used to lower HTX and treat angina pectorisAnders, 2/6/2008
AN34 Levothyroxine - thyroid replacement therapy for patients with hypothyroidism - be aware of many dental considerations for patients with hypothyroidism.Anders, 2/6/2008
AN35 Generic - thyroid replacement therapy for patients with hypothyroidismAnders, 2/6/2008
AN36 Sertraline - Antidepressant - SSRI - increased suicide in young individuals - xerostomia and bruxism reported - no problems with local anesthesia with epiAnders, 2/6/2008
AN37 Broad spectrum antibiotic - used for prophylactic tx - be aware of tightening indication for its use - long term use may lead to candiasisAnders, 2/6/2008
AN38 Escitalopram - Antidepressant SSRI type - same dental consideration and suicide warning as ZoloftAnders, 2/6/2008
AN39 Beta 2 agonist = brochodilator - used for astma and COPD - only dental consideration is the risk of xerostomiaAnders, 2/6/2008
AN40 Simvastatin - reduce cholesterol - no dental considerationsAnders, 2/6/2008
AN41 Esomeprazole - proton pump inhibitor - Used for erosive esophagitis; symptomatic gastroesophageal reflux disease (GERD) and as partof a multidrug regimen for Helicobacter pylori eradication in patients - Dental consideration: Can cause xerostomiaAnders, 2/6/2008
AN42 Zolpidem - Non-benzodiazepine hypnotics - used for insomnia - only dental consideration is xerostomiaAnders, 2/6/2008
AN43 Montelukast - Leukotriene Receptor Antagonist - Prophylaxis and chronic treatment of asthma; relief of symptoms of seasonal allergic rhinitis - 2% of patients complain of dental pain related to taking the drug - mechanism is unknownAnders, 2/6/2008
AN44 Lansoprazole - Proton pump inhibitor - same issues as with NexiumAnders, 2/6/2008
AN45 Clopidogrel - antiplatelet agent- popular term blood thinner - used to prevent MI, Stroke and DVT's - dental considerations covered later in this lectureAnders, 2/6/2008
Slide 173 (Continued)
AN46 Azithromycin - new macrolide - replaces erythromycin - used for tx of acute otitis media and lower/upper respiratory tract infections and other infections of bacterial origin - dental considerations: no adverse reactions reportedAnders, 2/6/2008
AN47 Bisphosphonate - used for osteoporosis - dental considerations are related to osteonecrosis of the jaws and is covered later Anders, 2/6/2008
AN48 Cetirizine - antihistamine used for allergy - may cause changes in salivary flowAnders, 2/6/2008
AN49 Fluticasone and Salmeterol - inhalation steroid - maintenance tx of astma and COPD. Dental considerations: May cause localized infections with Candida albicans or Aspergillus niger have occurred frequently in the mouth and pharynx with repetitive use of oral inhaler of corticosteroidsAnders, 2/6/2008
AN50 Hydrocodone and acetaminophen combination - sold as vicodin and other names - hydrocodone is an opioid with issues of tolerance and dependance. acetaminophen (tylenol) overdose may lead to hepatic necrosis. Is being used for suicide. Anders, 2/6/2008
AN51 Pantoprazole - proton pump inhibitor - used for GERD, but no dental considerations in contrast to Nexium and PrevacidAnders, 2/6/2008
AN52 Loop diuretic - management of oedema associated withe CHF and hepatic and renal disease or alone or in combination with other drugs for htx - no dental considerationsAnders, 2/6/2008
AN53 Beta 1 blocker used for tx of htx, post MI or angina pectoris - no dental considerations because of selective beta 1 blocking except to avoid prolonged use of NSAID's, which can reduce the antihypertensive effect of the beta 1 blockerAnders, 2/6/2008
AN54 Venlafaxine - Serotonin/Norepinephrine Reuptake Inhibitor (SNRI) - tx of anxiety and panic disorder - ignificant xerostomia (normal salivary flow resumes upon discontinuation); may contribute to oral discomfort, especially in the elderly; taste perversion. Although venlafaxine is not a tricyclic antidepressant, it does block norepinephrine reuptake within CNS synapses as part of its mechanisms. It has been suggested that vasoconstrictor be administered with caution and to monitor vital signs in dental patients taking antidepressants that affect norepinephrine in this way.Anders, 2/6/2008
AN55 Coumadin -"blood thinner" - Used for prophylaxis and treatment of thromboembolic disorders including those after replacement of valves or coming from atrial fibrillation or from an MI - dental considerations are covered elsewhere, but where briefly: The art of doing nothing!Anders, 2/6/2008
AN56 First generation cephalosporin (antibiotic) used for respiratory tract infections, otitis media, skin and skin structure infections, bone infections, and genitourinary tract infections. No special dental considerations except 20% cross allergy reaction with penicillin only when the allergic reaction was immediateAnders, 2/6/2008
AN57 Fluticasone - corticosteriod for inhalation - used prophylactically for astma and non-allergic rhinitis - only dental consideration is the
Slide 173 (Continued)
possibility for localzed candida infectionsAnders, 2/6/2008
AN58 Schedule II opioid (narcotic) - same concerns with APAP as HYCD/APAP. Also consider misuse by overprescribing. Street name oxy, OCand illbilly heroinAnders, 2/6/2008
AN59 Levofloxacin - Quinolone antibiotic, Treatment of mild, moderate, or severe infections caused by susceptible organisms. Includes the treatment of community-acquired pneumonia, including multidrug resistant strains of S. pneumoniae (MDRSP); nosocomial pneumonia; chronic bronchitis. Dental consideration: Use epi with great care because Lavequin prolongs the QT interval and the effect of epi on that is uncertain at this time.Anders, 2/6/2008
AN60 Valsartan - Angiotensin II Receptor Blocker - used for hypertension - no dental considerationsAnders, 2/6/2008
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 30
• Anticoagulant– Coumarin Derivative (Coumadin/warfarin)– Antiplatelet agent (Plavix/Clopidogrel)– Salicylate (Aspirin/Acetylsalicylic Acid)
• Antihypertensive– Beta 1 blocker (Atenolol)– Calcium channel blocker (Norvasc/Amlodipine)– Ace inhibitor (Lisinopril)– Diuretics (Hydroclorothiazide (HCTZ))
• Anti‐anxiety– Benzodiazapines (Valium/Diazepam or better Xanax/Alprazolam)– Nonbenzodiazepine Anxiolytics and Hypnotics (Diphenhydramine)– Barbiturates (Pentobarbital)
Main and minor drug category examplesMain and minor drug category examples
Drug categories: http://www.fda.gov/cder/handbook/category.htm 175
Tricyclic antidepressantsTricyclic antidepressants
176
• The tricyclic antidepressants blocks re‐uptake noradrenaline and serotonin
• Thus the concentration of these two neurotransmitters is elevated and neuronal activity increased.
• In the early 1990s the TCAs accounted for approximately 50% of all new prescriptions written for depression however, 40% of patients become non‐compliant with the medication because of their significant antimuscarinic side effects
• These include xerostomia (in 50% of patients), urinary retention, constipation, increased intra‐ocular pressure, cardiac arrhythmias, and postural hypotension
• Patients’ may not tolerate vasoconstrictors in local aneshesiawell
TCAsTCAs
177
• Levonordefrin and norepinephrine are absolutely contraindicated in patients receiving tricyclic antidepressants since dysrhythmias may occur (epinephrine dose should be kept to a minimum).
TCA and vasoconstrictors in localTCA and vasoconstrictors in local
178
OpioidsOpioids
179 180
Analgetics ‐ OpioidsAnalgetics ‐ Opioids
• Effects– Binds to opioid receptors thereby reducing the nociceptive response
– Works centrally and peripherally
• Adverse effects– Development of tolerance and addiction– Respiratory depression– Nausea
• Precautions– Drug interactions– Respiratory disease
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 31
181
Opioid ClassesOpioid Classes
• Agonist: Analgesic, No ceiling, – Respiratory depression
• i.e. Morphine, Codeine, Fentanyl
• Agonist‐Antagonist: Analgesic, Ceiling – No respiratory depression
• Talwin, Stadol, Nubain
• Antagonist: no analgesic effect– blocks agonist action
• Narcan (naloxone)
• Codeine (Schedule II)(Schedule III in these combos)
– w/ASA, 30/325 mg• Empirin w/codeine®
– w/APAP, 30/325 mg• Tylenol w/codeine®
Drug overview: OpioidsDrug overview: Opioids
182
– Usual single dose• 30‐60 mg
– Dosage interval• q4‐6h
– 60 mg is equivalent to 650 mg of ASA or APAP
• Hydrocodone (Schedule II alone)(Schedule III in these combinations)– w/ASA
• 5/325 mg– Lortab ASA®
– w/ibuprofen • 7.5/200 mg
– Vicoprofen®– w/APAP
• 5‐7.5‐10/325 mg – Norco• 5/500 mg – Lortab, Vicodin• 7.5‐10/500 – Lortab• 7.5/750 mg – Vicodin ES
Drug overview: OpioidsDrug overview: Opioids
183
– Usual single dose• 5‐10 mg
– Dosage interval• q4‐6h
– 10 mg of is equivalent to codeine 60‐80 mg
• Oxycodone (Schedule II both alone and in combinations)– w/ASA
• 5/325 mg– Percodan®
– w/APAP
• 5/325 mg– Percocet®
– With Ibuprofen
• 5/400 mg– Combunox®
– Usual single dose
• 5 mg
Drug overview: OpioidsDrug overview: Opioids
184
– Dosage interval
• q4‐6h– 10 mg is equivalent to 90 mg
of codeine
• Gastropathy– Nausea and vomiting
• Direct stimulation of the chemoreceptor trigger zone
– Constipation• Decreased gastric motility
Opioid side‐effectsOpioid side‐effects
185
• Intolerance– Allergic reactions are rare
– Histamine release from mast cells
• Peripheral vasodilation
• Orthostatic hypotension
• Tolerance – Specific opioid– Dosage– Frequency of use– Develops to most adverse effects as rapidly as to analgesic effects.
– Cross‐tolerance
Opioid side‐effectsOpioid side‐effects
186
• Dependence– Patients who take opioids for acute pain
• Rarely experience euphoria and
• Even more rarely develop psychological dependence or addiction
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 32
• Toxicity – Miosis– Dyspnea or apnea– Hypotension
• Shock
– Sedation– Stupor – Coma– Convulsions
Opioid side‐effectsOpioid side‐effects
187
– Treatment• Apnea and coma
– Naloxone• Convulsions
– Diazepam
188
Oxycodone dependencyOxycodone dependency
189
NY Times ‐ December 27, 2005 NY Times ‐ December 27, 2005 • “Lately, she has been playing with one of the strongest opiates
and potentially addictive painkillers ever created, Oxycontin. She downs a few with a single shot of vodka and calls the combination "the sorority girl's diet cocktail," because it simultaneously allows for a stronger kick of inebriation and far fewer calories than mere alcohol alone.”
• “The most recent Monitoring the Future report, the continuing study of teenage drug use conducted by the University of Michigan and the National Institutes of Drug Abuse since 1975, found that 5.5 percent of all high school seniors abused Oxycontin, up from 4 percent in 2002. Oxycontin abuse has increased 26 percent since 2002 among 8th, 9th and 12th graders.“
“Teens abuse prescription drugs more than any other illicit street drug except marijuana”
www.theantidrug.comwww.theantidrug.com
190 191
Analgetics ‐ NNTAnalgetics ‐ NNT
• NNT (Number Needed to Treat) is a measure of efficacy of a drug. It shows how many patients you have to treat before one additional patient responds to therapy
• A drug is said to work when patient reaches 50% pain releif
• The smaller the NNT the better• A perfect drug would have an NNT of 1
http://www.medicine.ox.ac.uk/bandolier/booth/painpag/Acutrev/Analgesics/Leagtab.htmlOr Google: Oxford pain
Common analgetics NNT’sCommon analgetics NNT’s
192
0
1
2
3
4
5
6
Tylenol 1 gram ASA 1 gram Tylenol 650 mgand codeine 60
mg
Ibuprofen 600mg
Diclofenac 100mg
Piroxicam 40 mg
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 33
• Compared 400 mg ibuprofen with 2.5, 5 and 10 mg oxycodone
• Only 10 mg oxycodone was superior to 400 mg ibuprofen alone
• Opioid adverse effects were dose‐related• 65% drowsy, 20% nauseated & 16% vomited at 10 mg oxycodone
Results from Dionne, R. J. Oral Max. Surg. 57:673, 1999Results from Dionne, R. J.
Oral Max. Surg. 57:673, 1999
193
• Adverse events are expressed as the number needed to harm (NNH): the number of patients that must receive a treatment to observea side‐effect or a complication in one more patient than in the placebo group
NNHNNH
194 195
Analgetics – Ceiling effectAnalgetics – Ceiling effect
• Ceiling effect is when an increased dose will not give increased effect
• ASA and acetaminophen 4‐6 g• Ibuprofen (NSAID) 2400 mg• Celebrex (Cox‐2 inhibitor) 200 mg• Vioxx (Cox‐2 inhibitor) 50 mg
196
Cost per dayCost per day
• Tylenol (Acetaminophen) $0.10• Ibuprofen (NSAID cox‐1 inhibitor) $1.00• Lortab ES (7.5/750) $2.00
• Celebrex (celecoxib Cox‐2 inhibitor) $3.50• Percocet (oxycodone/acetaminophen) $6.00
197
Guidelines – Postoperative pain management
Guidelines – Postoperative pain management
198
Guidelines – Postoperative pain management
Guidelines – Postoperative pain management
• Routinely recommend Ibuprofen 600 mg qid with first dose taken immediately following the extraction or surgery. Additional Tylenol may be taken per need respecting the 4 gram per day maximum dose.
• In cases of more severe pain or contraindication for Ibuprofen, prescribe Lortab or Vicodin 5/500, 7.5/500 or 7.5/750 (hydrocodone and acetaminophen). The maximum daily dose is 8 tabs for 5/500 and 6 tabs for 7.5/500 and 5 tabs for 7.5/750 doses. Additional Ibuprofen 600 mg qid can be taken (except when contraindicated).
• Due to addition liability of the opiate analgesics treatment for postoperative pain should be limited to 2‐3 days after extraction. In addition the opioids is associated with high incidence of CNS side effects such as nausea (30‐40%) and vomiting (15‐23%).
RecommendationRecommendation
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 34
199
Guidelines – postoperative pain management
Guidelines – postoperative pain management
• Pre‐emptive analgesic effect?– Does it help taking the pain medication already before the procedure like one day before?
• There is no pre‐emptive effect of NSAID’s, but there are for opioids.
• However, there is plenty of good reason to give the analgesia before the local anesthesia wears off.
Bisphosphonates and BRONJBisphosphonates and BRONJ
200
Relative Potency and risk of BP’sRelative Potency and risk of BP’s
• Oral administration Potency Risk– Etidronate (Didronel) 1– Tiludronate (Skelide) 10– Pamidronate (Aredia) 100– Alendronate (Fosamax) 1,000 0.1‐0.3%– Risedronate (Actonel) 10,000
• Oral and IV administration– Ibandronate (Boniva) 10,000
• IV administration– Zolendronic acid (Zometa) >100,000 0.8‐12%
201
• Dental exam (screening) before use of IV bisphosphonates (just like with radiation therapy)
• Avoid elective surgery for patients on or off IV bisphosphonates such as dental implants
• If patients have been taking oral bisphosphonates for less than 3 years, discontinuation of oral bisphosphonates for a period of 3 months prior to and 3 months after elective invasive dental may lower the risk of BRONJ (drug holiday)
Clinical consequences of BP’sClinical consequences of BP’s
AAOMS Position paper on BONJ - J Oral Maxillofac Surg 65:369-376, 20072009 update: http://www.aaoms.org/docs/position_papers/bronj_update.pdf
202
Surgeon General Report (2004)– 40% of American women > 50 yo. will experience an osteoporotic fracture
– 13% of men 50 yo. same– By 2020 it is estimated that 50% of all Americans over the age of 50 will be at risk of developing osteoporosis
– Direct cost expenditures for 1.3 million fractures per yr = $14 billion +
Osteoporosis is a BIG problem!Osteoporosis is a BIG problem!
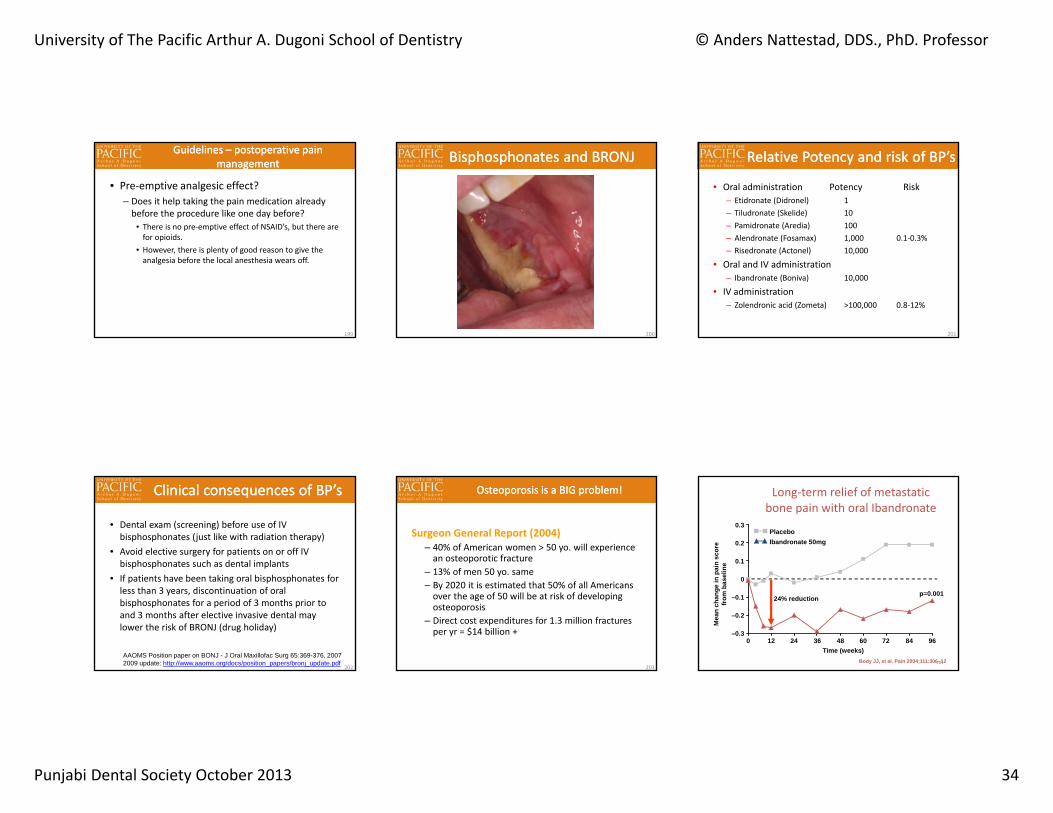
203Body JJ, et al. Pain 2004;111:306–12
Long‐term relief of metastaticbone pain with oral Ibandronate
Mea
n ch
ange
in p
ain
scor
efr
om b
asel
ine
0.3
0.2
0.1
0
–0.1
–0.2
–0.3
Time (weeks)0 12 24 36 48 60 72 84 96
p=0.001
PlaceboIbandronate 50mg
24% reduction
204
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 35
Extractions and IV bisphosphonatesExtractions and IV bisphosphonates
205
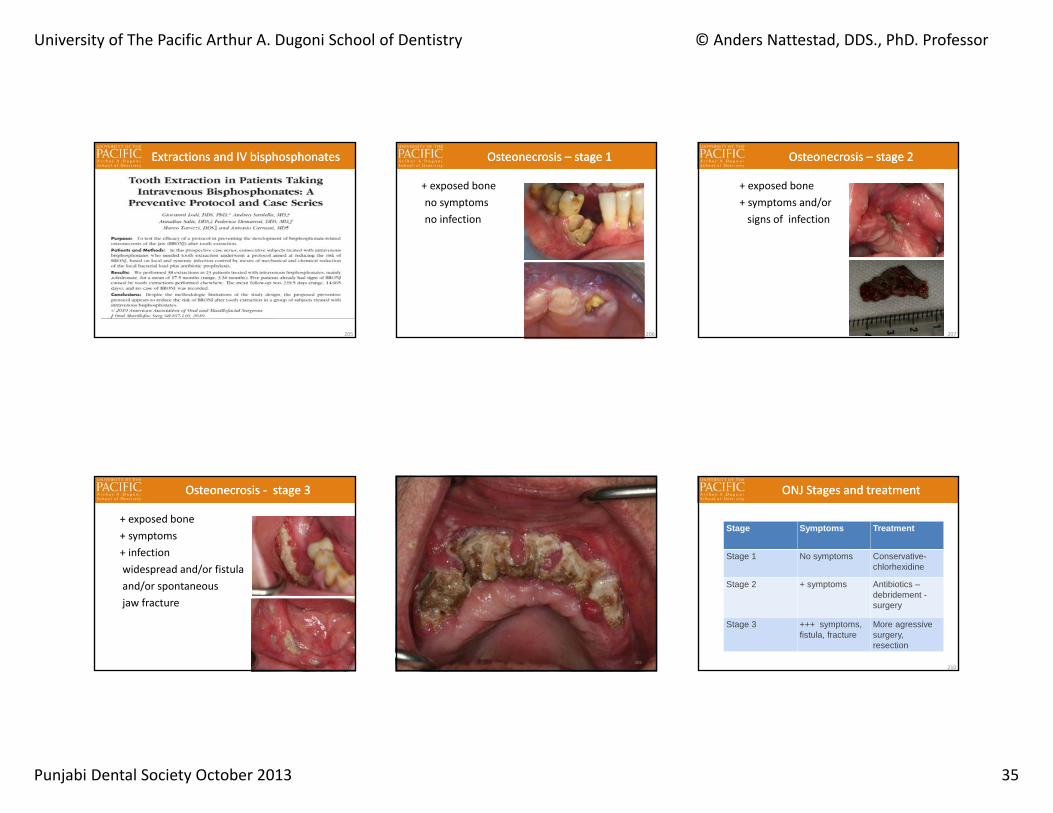
+ exposed bone no symptoms no infection
Osteonecrosis – stage 1Osteonecrosis – stage 1
206
+ exposed bone+ symptoms and/orsigns of infection
Osteonecrosis – stage 2Osteonecrosis – stage 2
207
+ exposed bone + symptoms + infectionwidespread and/or fistulaand/or spontaneous jaw fracture
Osteonecrosis ‐ stage 3Osteonecrosis ‐ stage 3
208209
ONJ Stages and treatmentONJ Stages and treatment
Stage Symptoms Treatment
Stage 1 No symptoms Conservative-chlorhexidine
Stage 2 + symptoms Antibiotics –debridement -surgery
Stage 3 +++ symptoms, fistula, fracture
More agressivesurgery, resection
210
University of The Pacific Arthur A. Dugoni School of Dentistry © Anders Nattestad, DDS., PhD. Professor
Punjabi Dental Society October 2013 36
Precautions ‐ 1Precautions ‐ 1
• Take medical history on all patients • Document in your chart• Most patients do not know what ”bisphosphonate” is
• They may know ”Zometa” or ”Fosamax”• Ask the patient to bring a medication list
211
Precautions ‐ 2Precautions ‐ 2
• Oral surgery:• Osteoporosis patients: Tx in your practice• Cancer patients on high dose BP: refer to Oral & Maxillofacial Surgeon
• ONJ‐patients:• Refer to Oral & Maxillofacial Surgeon
212213