Embed Size (px)
Citation preview
Disclosures –Anne Brittain, PhD RT(R)
(M)(QM), CPHQ
I have no disclosures as it pertains to this educational activity.
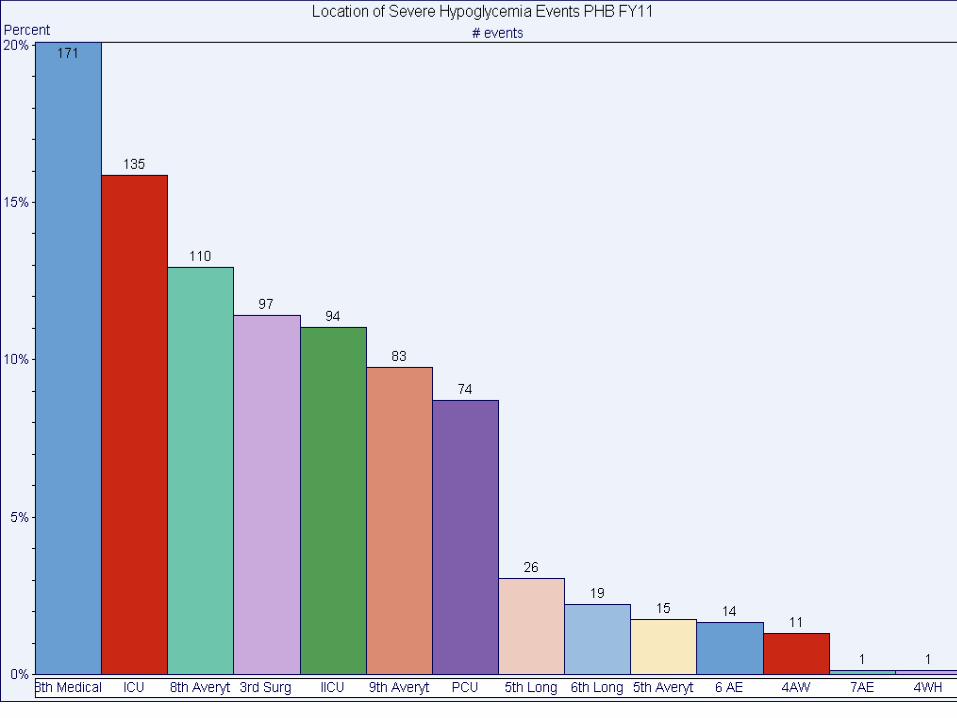
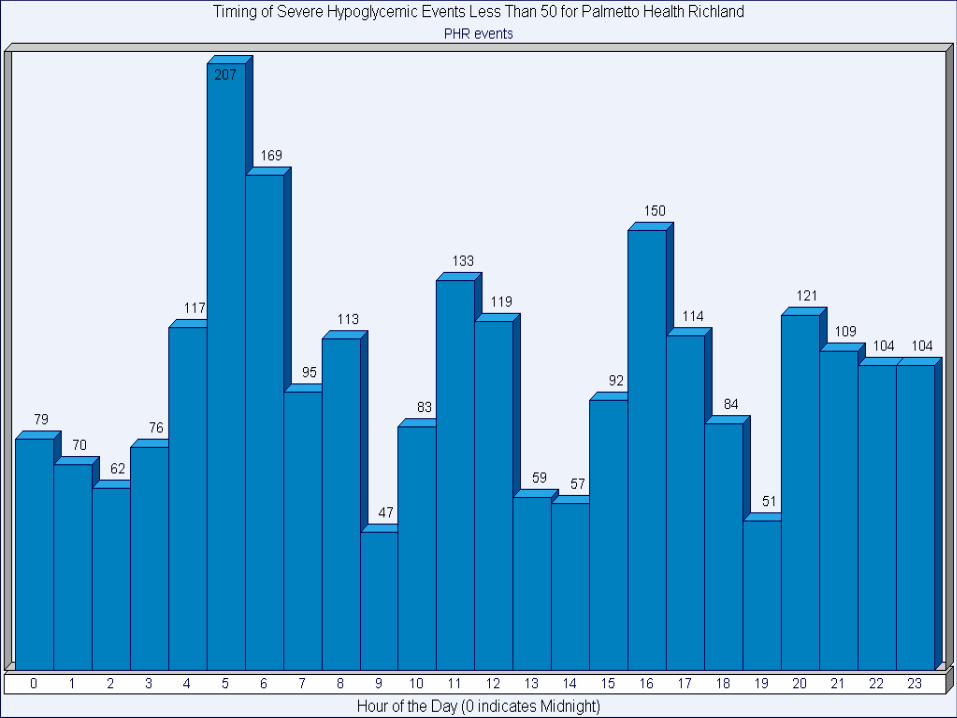
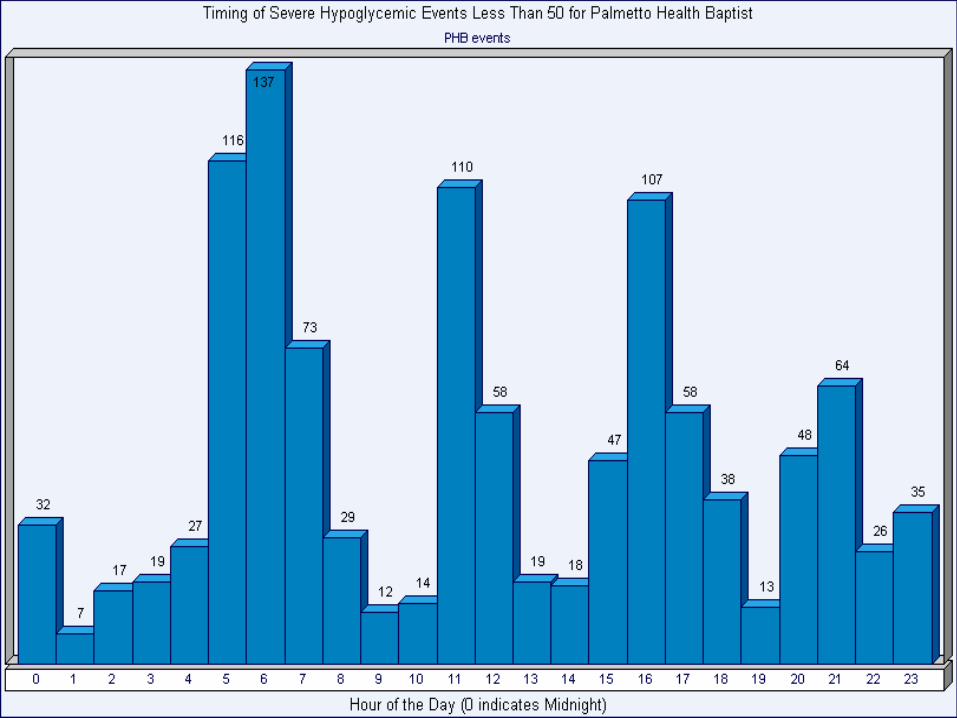
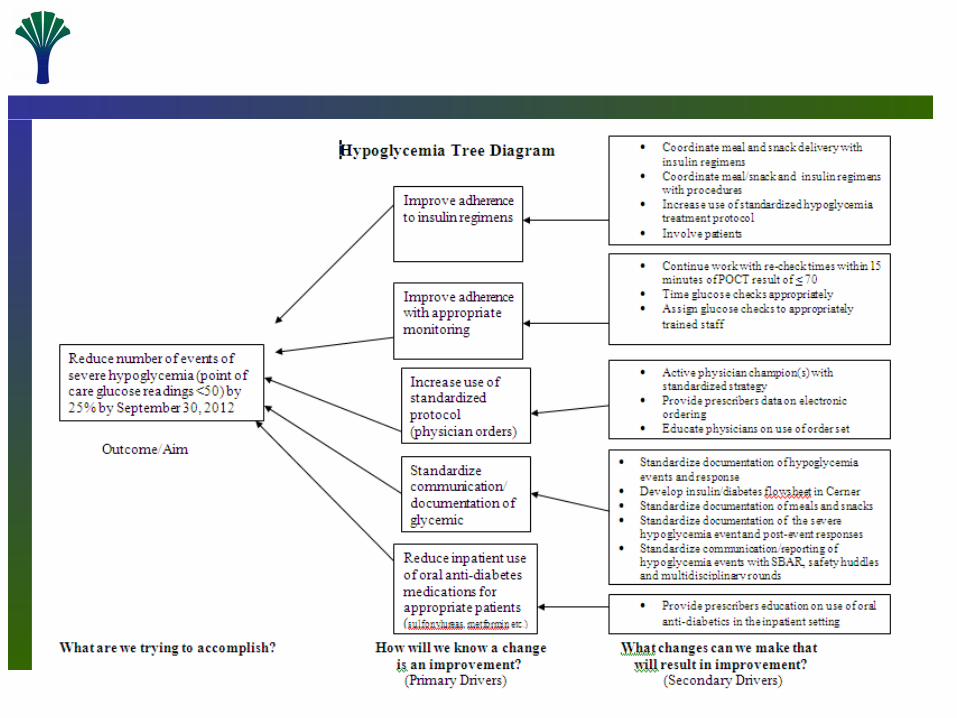
Reduction of Severe Hypoglycemia (<50mg/dL)
Goal: Reduce events of severe hypoglycemia 5% by the end of FY12.
Baseline Data
Out of 407,063 point of care blood glucose checks, there were 2,646 (0.64%) events of severe hypoglycemia as a system.
Richland-1,795 Events
Baptist-851 Events
Project Plan- 1st Five Weeks
• Establish cross campus team- Senior Leader, Physician Champion, Nursing Leader, Diabetes Education, CQPS-PIT, Pharmacy, Nutrition, Nursing Education, Endocrinology
• Select initial pilot units• Establish team aim and outcome/process
measures• Educate team on PI methodologies to be used • Complete process mapping• Determine opportunities
Project Plan- 6th week and beyond
• PDSA planning– Begin small, but fast, for initial trials (e.g. 1 pt,
1 day, 1 unit, etc.)– Perfect change (2 weeks max per unit/area)– Expand trials/Spread change
• Revise Policies & PGR’s, as needed
• Devise system to monitor hardwiring of improved process
Contact Information
• Anne Brittain-296-2308 [email protected]
• MaryJane Phipps-296-3622 [email protected]
• Heather Mann-296-3392 [email protected]
DisclosuresI have no relevant financial
relationships with any commercial interests related to the content of this
activity – Shahid Aziz, MDFellow, Endocrinology
Inpatient Glucose Management
Shahid Aziz, MDFellow, Endocrinology
Hospital-related Hyperglycemia
• Upon admission: diagnosed diabetes, undiagnosed diabetes, illness-related hyperglycemia (assess for outpatient control: meter readings, HbA1c)
• Hospital course: glucose targets, adjustment and titration, education and teaching, safety
• At discharge: planning, self-management skills• Follow-up
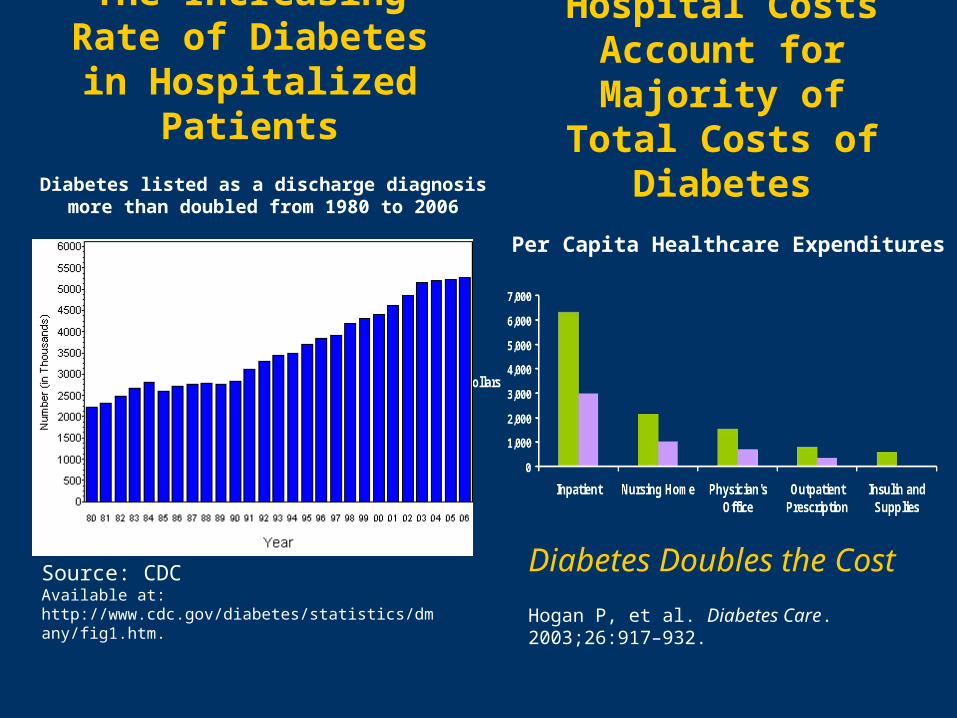
The Increasing Rate of Diabetes in
Hospitalized Patients
Source: CDCAvailable at: http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm.
Per Capita Healthcare Expenditures
Hospital Costs Account for Majority
of Total Costs of Diabetes
Hogan P, et al. Diabetes Care. 2003;26:917–932.
Diabetes Doubles the Cost
Diabetes listed as a discharge diagnosis more than doubled from 1980 to 2006
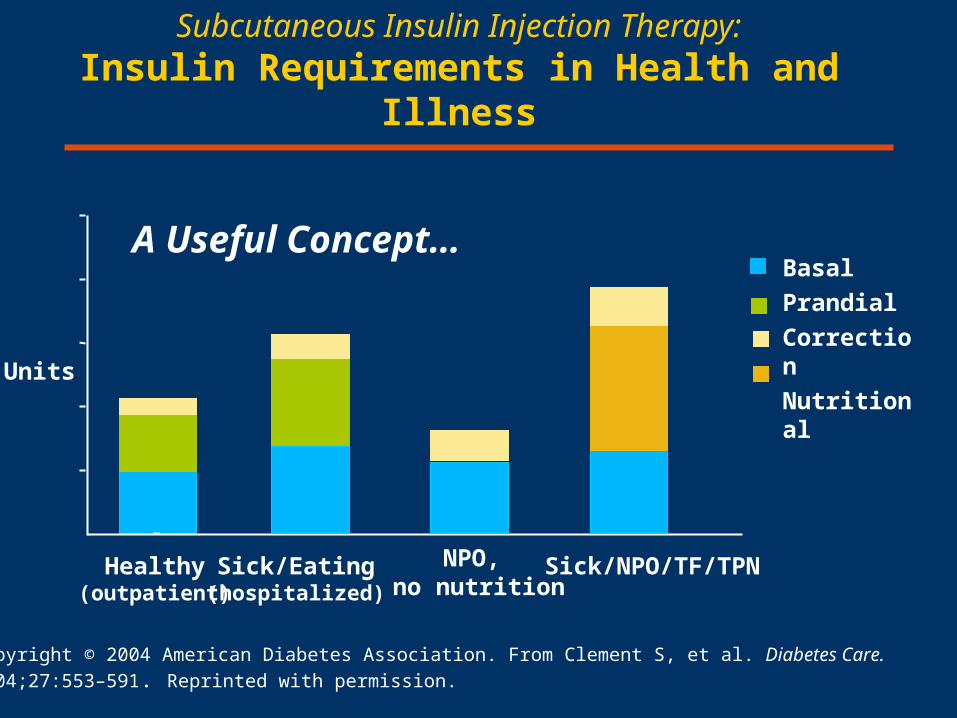
Subcutaneous Insulin Injection Therapy:Insulin Requirements in Health and Illness
Copyright © 2004 American Diabetes Association. From Clement S, et al. Diabetes Care.
2004;27:553–591. Reprinted with permission.
Units
Healthy(outpatient)
Sick/Eating(hospitalized)
Sick/NPO/TF/TPN
Basal
Prandial
Correction
Nutritional
NPO, no nutrition
A Useful Concept…
Strategies and Protocols for Achieving Inpatient
Glycemic Control
• Continuous variable-rate IV insulin drip
• Regular insulin
• Subcutaneous basal/bolus therapy
• Long-acting and rapid-acting insulin
• Premix / biphasic insulin • For selected patients
transitioning to outpatient care
Protocol Implementation
• Multidisciplinary team
• Administration support
• Pharmacy & Therapeutics Committee approval
• Forms (orders, flowsheets)
• Education: nursing, pharmacy, physicians & NP/PA
• Monitoring/Quality Assessment
Glucose Control in the Hospital and Inpatient Outcomes
A challenge and an opportunity to favorably impact patient care
• Open-heart surgery – Portland Diabetic Project 1987-2005
• Acute MI – DIGAMI 1 1995-99 DIGAMI 2 Eur Heart J 2005
• Surgical ICU – Leuven trial 1 N Engl J Med 2001
• Medical ICU – Leuven trial 2 N Engl J Med 2006
Indications for IV Insulin Drip
Think broad.…• DKA
• Hyperosmolar Hyperglycemic state (HHS)
• Postoperative period following open-heart surgery
• Critical care illness (surgical/medical)
• Myocardial infarction (MI) or cardiogenic shock
• NPO status in Type 1 diabetes
• Perioperative care
• TPN
• High-dose glucocorticoid therapy
• Organ transplantation
• Labor and delivery
What should the glucose targets be using IV insulin (insulin drip)
in critically ill patients?
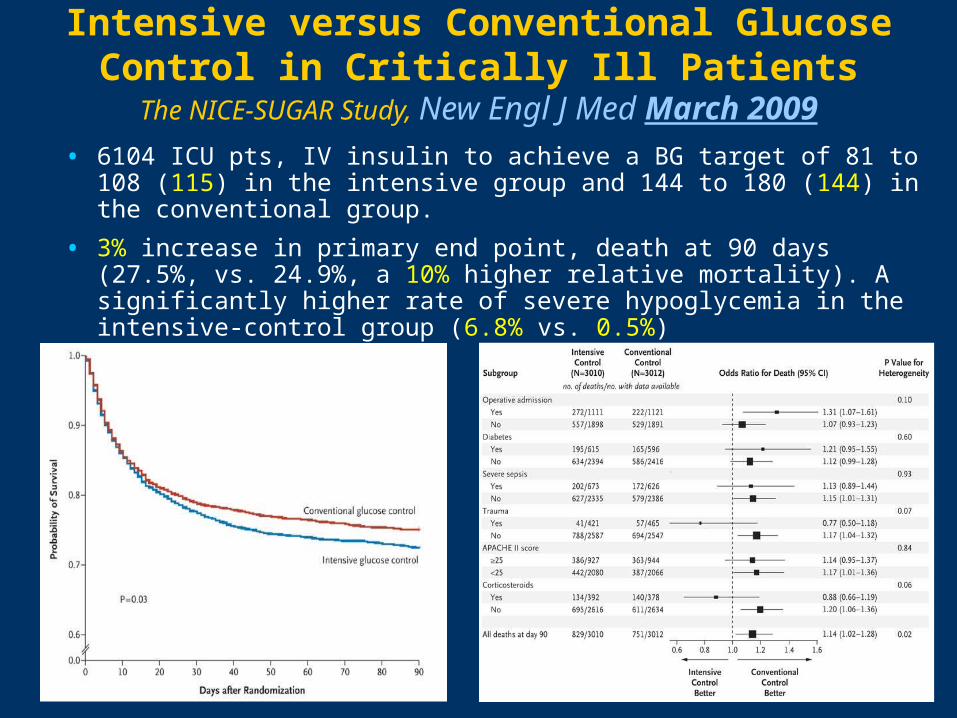
Intensive versus Conventional Glucose Control in Critically Ill Patients
The NICE-SUGAR Study, New Engl J Med March 2009
• 6104 ICU pts, IV insulin to achieve a BG target of 81 to 108 (115) in the intensive group and 144 to 180 (144) in the conventional group.
• 3% increase in primary end point, death at 90 days (27.5%, vs. 24.9%, a 10% higher relative mortality). A significantly higher rate of severe hypoglycemia in the intensive-control group (6.8% vs. 0.5%)
Optimal Glucose Targets in Hospital Patients:
The ADA-ACE Consensus Statement based on the results of NICE-SUGAR
Diabetes Care, May 2009
Critically ill patients
• Use IV insulin in the majority of patients in the ICU setting
• Maintain glucose levels between 140 and 180 mg/dL
• Targets less than 110 mg/dL are NOT recommended
Noncritically ill (floor) patients
• Recommendations are based on “clinical experience and judgment”
• Premeal glucose targets should generally be <140 mg/dL
• Random glucose values <180 mg/dL
Protocol Implementation: a multidisciplinary effort
The Ideal IV Insulin Protocol
• Easily ordered and implemented
• Effective (gets to goal quickly)
• Safe (minimal risk of hypoglycemia)
Converting to Subcutaneous Insulin
• Establish 24-hour insulin requirement• Extrapolate from average over last 6–8 hours – if stable
• Give one-half amount as basal, rest as bolus
• Transition: stop drip half hour after a small SC dose of short-acting insulin and a SC dose of long-acting (basal) insulin
• Monitor a.c. (before meal) t.i.d., h.s.
• Correct all premeal blood glucose > 150 mg/dL
• Hospitalized patients often require high insulin doses to achieve target glucose
• Initial dose: Basal insulin 0.15 units / kg; titrate! based on am reading
• Provide both basal and bolus (prandial or nutritional) coverage
• Patients often need supplemental or correction insulin for premeal hyperglycemia
• Use of “Sliding Scale” Insulin Alone is Discouraged!
Use of Subcutaneous Insulin
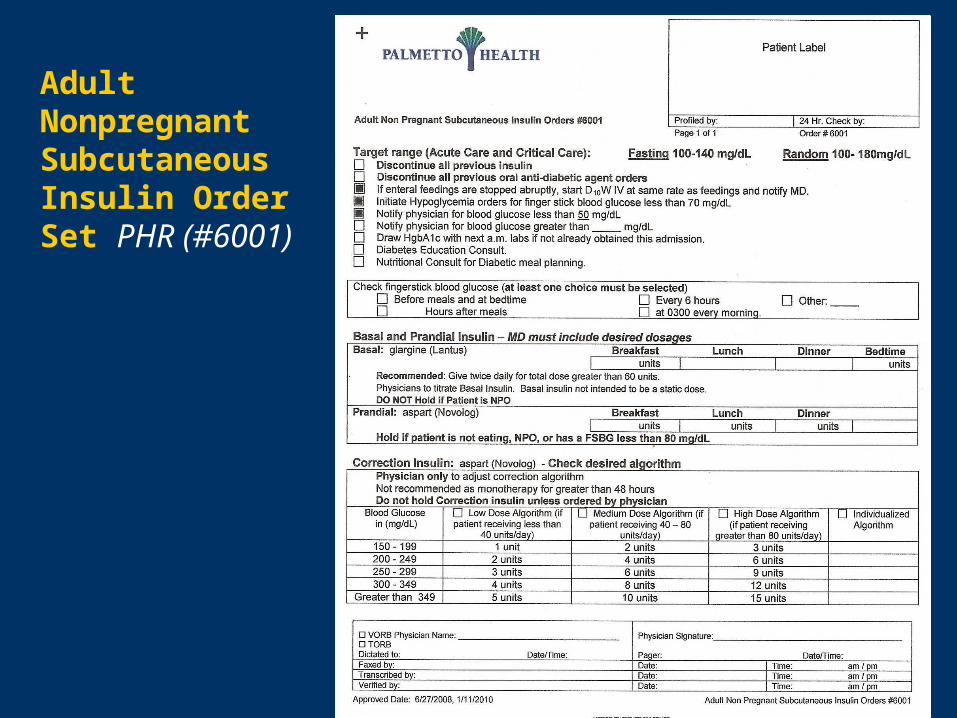
Adult Nonpregnant Subcutaneous Insulin Order Set PHR (#6001)
What is the Role of ‘Sliding Scale’ Insulin?
• Sliding scale is retroactive / reactive coverage, treats hyperglycemia after it happens, may lead to glycemic excursions
• Should not be used as the sole method of insulin administration
• Quickly add, or adjust, the basal insulin dose and add scheduled bolus insulin if necessary
Risk Factors for Hypoglycemia in Inpatients
• Advanced age
• Decreased oral intake
• Chronic renal failure
• Liver disease
• Beta-blockers
• Inadequate glucose monitoring
• Lack of coordination between dietary, nursing, and transportation; mistiming of insulin and food
Key components of hypoglycemia prevention and management
protocolEndocrine Society Practice Guideline, Jan 2012
• Hospital-wide definitions for hypoglycemia and severe hypoglycemia.
• Guidance on discontinuation of sulfonylurea therapy and other oral hypoglycemic medications at the time of hospital admission.
• Directions for adjustments in insulin dose and/or administration of dextrose-containing iv fluids for both planned and sudden changes in nutritional intake.
• Specific instructions for recognition of hypoglycemia symptoms, treatment, and timing for retesting depending on glucose levels and degree of the patient's neurological impairment and for retesting of glucose levels.
• Standardized form for documentation and reporting of hypoglycemic events, including severity, potential cause(s), treatment provided, physician notification, and patient outcome.
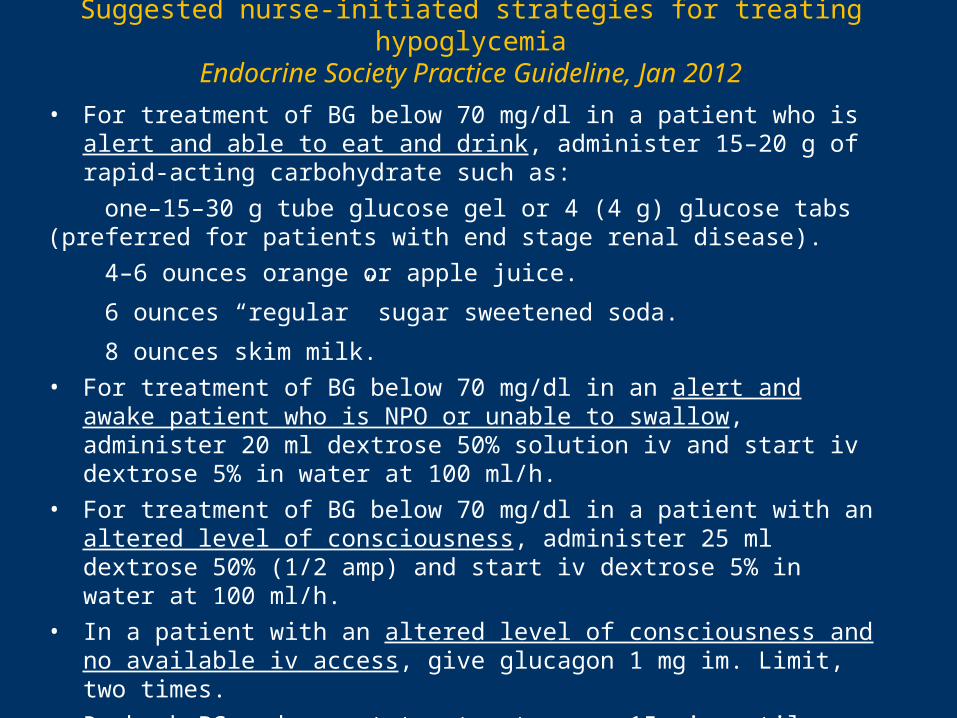
Suggested nurse-initiated strategies for treating hypoglycemia
Endocrine Society Practice Guideline, Jan 2012
• For treatment of BG below 70 mg/dl in a patient who is alert and able to eat and drink, administer 15–20 g of rapid-acting carbohydrate such as:
one–15–30 g tube glucose gel or 4 (4 g) glucose tabs (preferred for patients with end stage renal disease).
4–6 ounces orange or apple juice.
6 ounces “regular” sugar sweetened soda.
8 ounces skim milk.
• For treatment of BG below 70 mg/dl in an alert and awake patient who is NPO or unable to swallow, administer 20 ml dextrose 50% solution iv and start iv dextrose 5% in water at 100 ml/h.
• For treatment of BG below 70 mg/dl in a patient with an altered level of consciousness, administer 25 ml dextrose 50% (1/2 amp) and start iv dextrose 5% in water at 100 ml/h.
• In a patient with an altered level of consciousness and no available iv access, give glucagon 1 mg im. Limit, two times.
• Recheck BG and repeat treatment every 15 min until glucose level is at least 80 mg/dl.
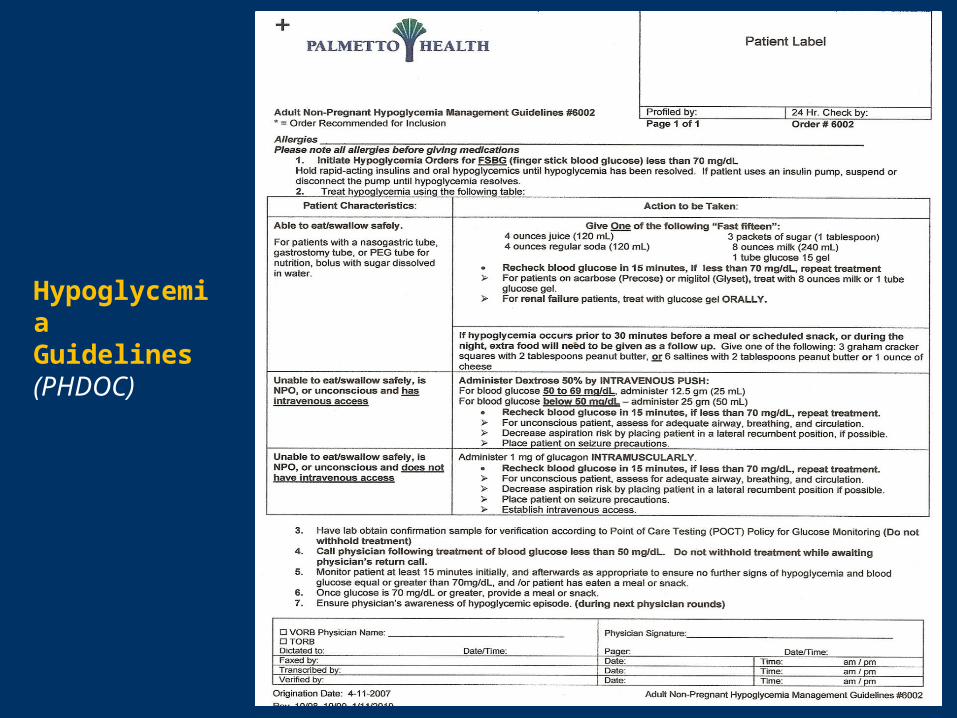
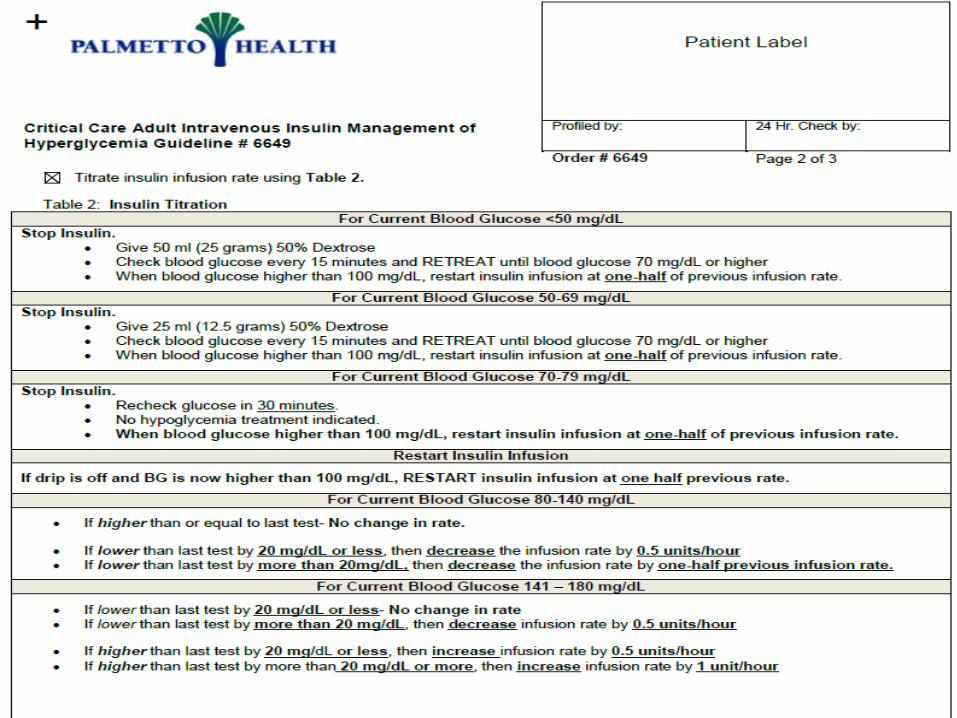
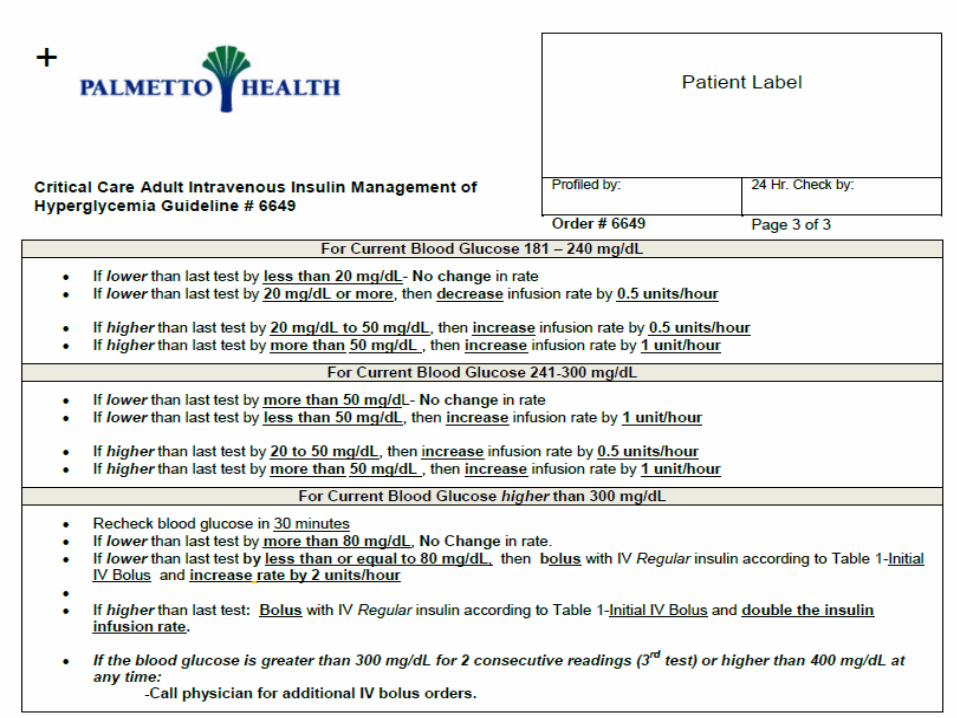
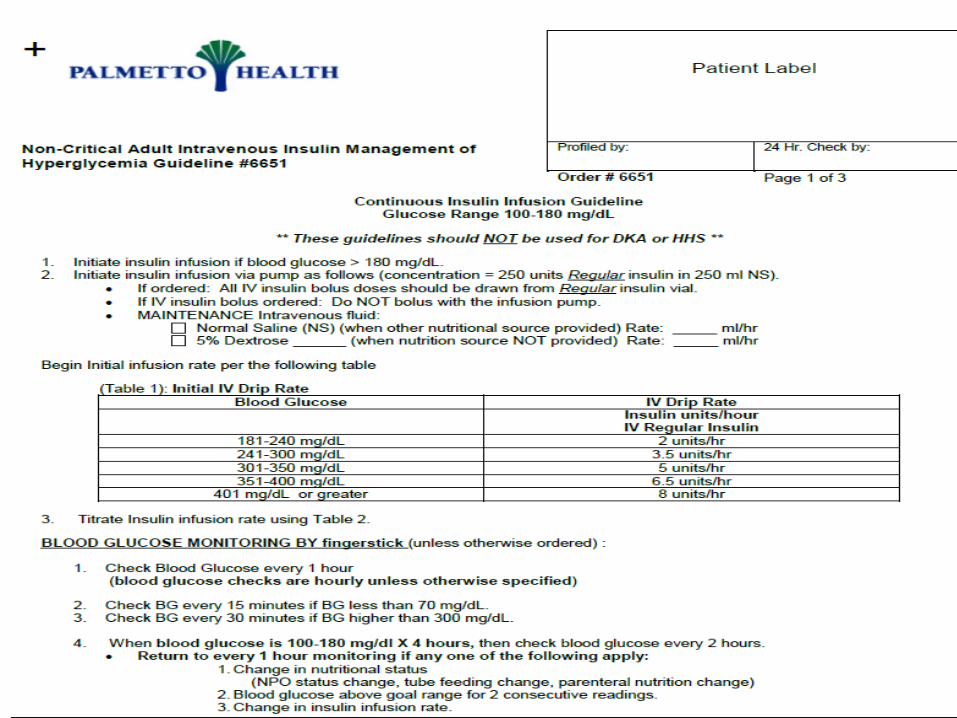
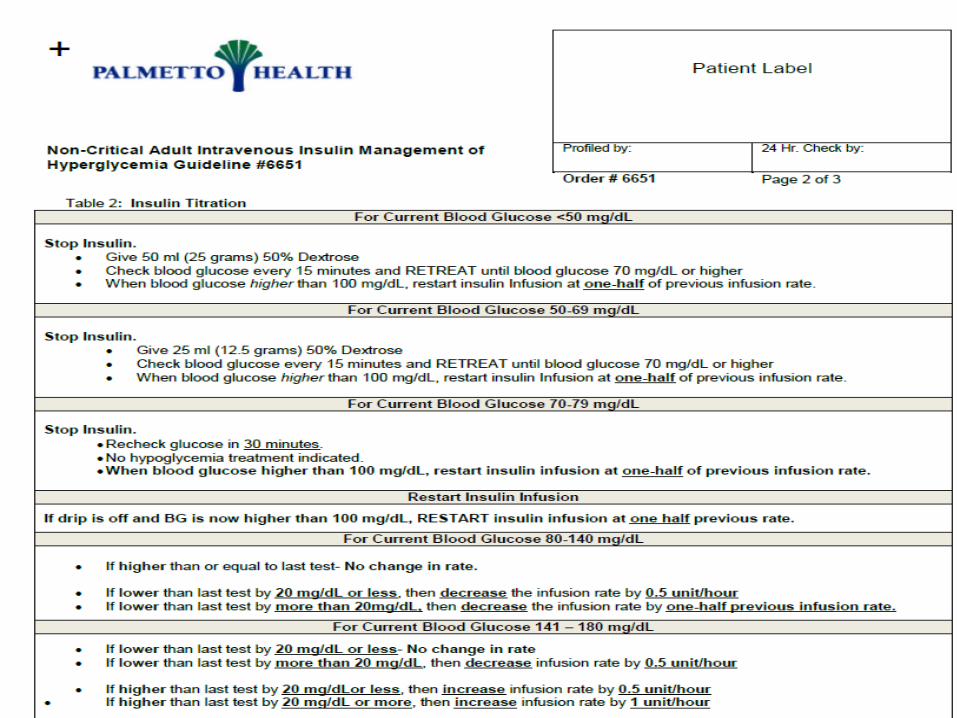
Hypoglycemia Guidelines (PHDOC)
What about Oral Agents?• Insulin is the preferred medication in hospitalized
patients
• Oral agents may be contraindicated or simply ineffective
• In general, avoid continuing or starting oral agents in inpatients, except in relatively healthy patients e.g. elective surgery
• At discharge, inpatient “survival skills” education for pts initiated on insulin; plan in advance!
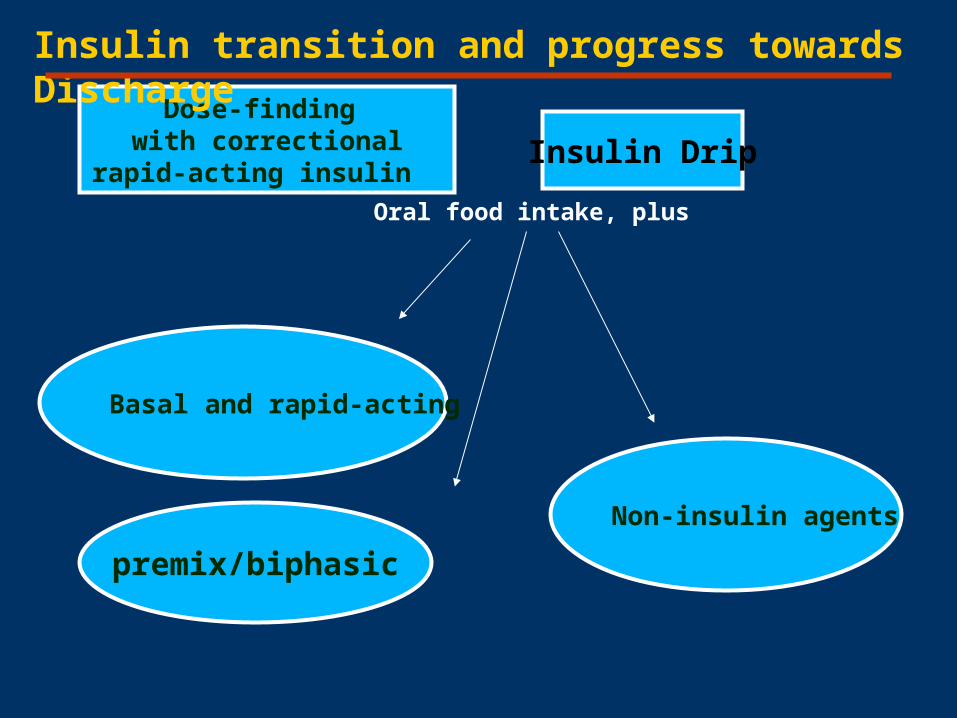
Insulin Drip
Non-insulin agents
premix/biphasic
Dose-finding with correctional rapid-
acting insulin
Insulin transition and progress towards Discharge
Oral food intake, plus
Basal and rapid-acting
Discharge Planning starts well before discharge!
• Establish a stable regimen of diet and meds well in advance of anticipated discharge
• Refresher in self-care issues, monitoring, nutrition, and diabetes teaching (“survival skills”) with inpatient diabetes educator
• Don’t be afraid to determine a different medication/insulin regimen if necessary discharge
• Arrange for comprehensive diabetes class and follow up physician visit within 2 weeks of discharge
Keys to Euglycemia in the Inpatient Setting
Take-home Points• Be aware of glucose targets
• Plan ahead: IV insulin, transition from IV to SC, discharge planning
• Communicate with patients and other health care professionals
South Carolina Guidelines for Diabetes Care – 2011
released September 2011
Available at:•http://www.scdhec.gov/health/chcdp/diabetes/clinical.htm •http://clinicaldepartments.musc.edu/medicine/divisions/endocrinology/dsc
Evidence-based recommendations from:•American Diabetes Association•American Association of Clinical Endocrinologists•American Association of Diabetes Educators





























