Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=iedc20
Download by: [Dr Mohamed El Kassas] Date: 05 May 2017, At: 15:14
Expert Opinion on Drug Discovery
ISSN: 1746-0441 (Print) 1746-045X (Online) Journal homepage: http://www.tandfonline.com/loi/iedc20
Discovery and preclinical development ofdasabuvir for the treatment of hepatitis Cinfection
Mohamed El Kassas, Tamer Elbaz, Enas Hafez, Mohamed Naguib Wifi &Gamal Esmat
To cite this article: Mohamed El Kassas, Tamer Elbaz, Enas Hafez, Mohamed Naguib Wifi &Gamal Esmat (2017): Discovery and preclinical development of dasabuvir for the treatment ofhepatitis C infection, Expert Opinion on Drug Discovery, DOI: 10.1080/17460441.2017.1322955
To link to this article: http://dx.doi.org/10.1080/17460441.2017.1322955
Accepted author version posted online: 25Apr 2017.Published online: 05 May 2017.
Submit your article to this journal
Article views: 8
View related articles
View Crossmark data

DRUG DISCOVERY CASE HISTORY
Discovery and preclinical development of dasabuvir for the treatment of hepatitisC infectionMohamed El Kassasa, Tamer Elbazb, Enas Hafezc, Mohamed Naguib Wifid and Gamal Esmatb
aEndemic Medicine Department, Faculty of Medicine, Helwan University, Cairo, Egypt; bEndemic Hepatogastroenterology, Faculty of Medicine,Cairo University, Cairo, Egypt; cClinical Pharmacy Unit, New Cairo Viral Hepatitis Treatment Unit, Cairo, Egypt; dInternal Medicine Department,Faculty of Medicine, Cairo University, Cairo, Egypt
ABSTRACTIntroduction: Hepatitis C virus (HCV) is a leading cause of liver-related morbidity and mortality.Positively, the introduction of new directly-acting antivirals (DAAs) have led to dramatic improvementsin response rates to antiviral therapy. Furthermore, newer generations of DAAs have demonstratedbetter safety profiles as well as efficacy than older generations. Current treatment recommendations arebased on different combinations of DAAs. Current combination therapies rely on agents that target thedifferent steps of viral replication by using different molecules from various DAAs families.Areas covered: In this review, the authors summarize data from of one of the recently developed NS5Bpolymerase inhibitors, dasabuvir, formerly known as ABT-333. Herein, the authors discuss the drugdiscovery data for dasabuvir including data from preclinical, toxicological resistance studies. Theauthors also review dasabuvir’s clinical efficacy across various clinical challenges, in addition to itslimitations in clinical practice.Expert opinion: Dasabuvir represents an important medical advance when used as a combinationtherapy for HCV. Unfortunately, it does present limitations like low genotypic coverage and furtherresearch is still required to address some of the lingering issues
ARTICLE HISTORYReceived 31 January 2017Accepted 21 April 2017
KEYWORDSHepatitis C virus; dasabuvir;preclinical; drug discovery
1. Introduction
Hepatitis C virus (HCV) is a global pathogen and a leading cause ofmorbidity andmortality [1]. In the last 15 years, the seroprevalenceof HCV infection has increased to 2.8%, which accounts for 185million infections worldwide [2]. Chronic HCV infection is asso-ciated with the development of many complications like livercirrhosis, liver cell failure, hepatocellular cancer, and death [3].
In the past, administration of pegylated interferon andribavirin, administered for 24–48 weeks, was long consideredas the standard treatment therapy for HCV. However, thistreatment mode was found to be associated with severalside effects. Despite comparable treatment outcomesbetween low-middle income countries and well-resourcedcountries, the financial burden has been a considerable barrierfor healthcare systems in the former’s case [4–6].Consequently, there was a worldwide agreement to make aremarkable and dramatic shift in the treatment of HCV infec-tion in the present decade. Unfortunately, the first generationof new direct-acting antivirals (DAAs) that was administeredwith interferon and ribavirin showed several side effectsdespite having increased efficacy [7,8]. The second generationof DAA therapies showed higher cure rates and minimal sideeffects in Phase II or III trials [9]. This has led to the develop-ment of multiple DAA therapies. When given in combination,they rendered the need for interferon treatment unnecessary,leading to the emergence of the term ‘interferon-free regi-mens’ [10–12].
Combinations of DAAs that target different steps of viralreplication have significantly improved the efficacy of HCVtreatment by increasing its safety and tolerability. The dura-tion of therapy has also been shortened along with simplifiedtreatment algorithms. In addition, these therapies have signif-icantly reduced the public health burden of this disease. DAAsinclude inhibitors of HCV NS3/4A protease (telaprevir, boce-previr, and simeprevir), HCV NS5A protein (ledipasvir, dacla-tasvir), and the nucleotide analog NS5B polymerase inhibitors(sofosbuvir). One of the newly developed NS5B polymeraseinhibitors is dasabuvir. It was formerly known as ABT-333, andits chemical name is sodium 3-(3-tert-butyl-4-methoxy-5-{6-[(methylsulfonyl) amino] naphthalene-2-yl}phenyl)-2,6-dioxo-3,6-dihydro-2H-pyrimidin-1-ide hydrate [1:1:1]). While there ismuch information available on the use of DAA combinationsin clinical practice, there is limited available data on the dis-covery and development of each agent in these combinations.Thus, we conducted this review with the aim of collating theavailable data on the discovery and preclinical development ofdasabuvir.
2. Discovery and preclinical development
2.1. Primary pharmacology
Dasabuvir is a new DAA with a novel mechanism of action. Itacts as a potent non-nucleoside inhibitor of RNA-dependentRNA-polymerase, encoded by the NS5B gene of HCV. It has a
CONTACT Mohamed El Kassas [email protected] Endemic Medicine Department, Faculty of Medicine, Helwan University, Cairo, Egypt
EXPERT OPINION ON DRUG DISCOVERY, 2017https://doi.org/10.1080/17460441.2017.1322955
© 2017 Informa UK Limited, trading as Taylor & Francis Group

high selectivity for RNA polymerase enzymes of genotype 1HCV as it binds to the palm I allosteric inhibitory site of theprotein. The concentration required for 50% inhibition (IC50)for clinical isolates ranges between 2.2 and 10.7 nM for 1a(strain H77) and 1b (strain Con1) strains of genotype 1 HCV.Dasabuvir inhibited replicon of genotype 1a and 1b strains atIC50 of 7.7 and 1.8, with a noticeable reduction in the inhibi-tory activity in the presence of 40% human plasma.Comparatively, a concentration of 900 nM was required forstrains 2a, 2b, 3a, and 4a polymerases. Simultaneously, itshowed a 7000-fold selectivity for HCV polymerases overhuman polymerases [13,14].
2.2. Discovery and chemistry
Dasabuvir is an aryl dihydrouracil derivative that binds to thepalm initiation pocket of HCV NS5B polymerase, a compoundidentified via throughput screening procedure of the aryldihydrouracil fragment [15]. It has an acceptable range ofpractical size for manufacturing and clinical activity. It doesnot exhibit stereoisomerism and is thermodynamically stable.It further has aqueous solubility, dissolution, and Caco-2 per-meability. The final sodium salt structure was confirmed bychemical assay after several manufacturing steps [16] and wascreated by AbbVie [2] (Table 1).
3. Pharmacokinetics
The oral administration of dasabuvir in many animal modelslike Sprague Dawley® rats, beagle dogs, and monkeys showedits rapid absorption rates with Tmax ranging from 1 to 3 h.Bioavailability was enhanced by two- to threefold when dasa-buvir was administered to fasted dogs compared to fed ones(Table 2) [17].
Intravenous studies illustrated that the volume of distribu-tion was mostly higher than 1.1 L/kg (Vss) in all animal species;t1/2 was 3.6, 2, and 19.9 h in rats, monkeys, and dogs, respec-tively. Different clearance values were observed in these ani-mals: 1.2 L/h kg in monkeys, 0.63 L/h kg in rats, and 0.04 L/h kg in dogs [17].
3.1. Repeated dose pharmacokinetics: a nonclinicaltoxicological study
Optimized lipid surfactant formulation of the free acid andaqueous suspension of the salt enhanced the solubility ofdasabuvir, resulting in its maximum exposure. The animalmodels used for this study were Sprague Dawley rats, fastedbeagle dogs, cynomolgus monkeys, mice, and New Zealandwhite rabbits. Maximal exposure was achieved in monkeys at adose of 200 mg with twofold increase in area under curve(AUC) upon repeated doses while the increase in exposure inthe case of the beagle dogs was 6.6-fold (maximal exposuredose 60 mg/kg). The mice showed no increase in AUC at doseshigher than 6000 mg/kg/day while Sprague Dawley rats wereobserved to produce no more than a minimal difference at adose higher than 200 mg/kg/day. The study on New ZealandWhite rabbits revealed a maximal exposure dose of 400 mg/kg. When the dose was increased to 500–700 mg, a highvariability was observed in AUC. If repeated doses wereapplied to pregnant rats, a threefold increase in accumulation(maximal exposure obtained at 400 mg/kg) occurred [14].
3.2. Absorption
Dasabuvir showed high permeability in the Caco-2 assay eva-luation. This indicates more than 70% absorption in a humancell with no active efflux activity [14].
4. Distribution
In the case of rats, the volume of distribution following intra-venous administration is approximately 4000 L, i.e. 33%, fol-lowing 5 mg/kg dose of dasabuvir. Dasabuvir is a highlyplasma proteins-bound drug. The unbound fraction of theparent drug (fu) is less than 0.01 while its metabolite (M1) is
Article highlights
● Dasabuvir is a direct-acting antiviral agent approved for use incombination therapy for treating hepatitis C infection.
● Dasabuvir acts by inhibiting NS5B polymerase, an enzyme requiredfor HCV replication.
● Dasabuvir has a proven and clear effective synergistic role when usedin combination with other DAAs despite showing moderate antiviralefficacy.
● The drug is safe and carries no major side effects with fewer require-ments for drug stoppage.
● Dasabuvir has limitations in terms of its limited genotypic coverage. Italso has difficulties in terms of its use in advanced cirrhotic patients.There is also a large pill burden when added to combination therapy.
Table 1. The chemical characteristics of dasabuvir.
IUPAC nameN-[6-[3-Tert-butyl-5-(2,4-dioxopyrimidin-1-yl)-2-
methoxyphenyl]naphthalen-2-yl]methanesulfonamide
2D chemicalformula
Associatedname(s):
ABT-333A-998821.5 (sodium salt);Sodium N-{6-[3-tert-butyl-5-(2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl)-2-methoxyphenyl] naphthalen-2-yl}methanesulfonamidehydrate
Generic name DasabuvirMolecularformula
C26H27N3O5S
Table 2. Pharmacokinetics of single oral dose.
Tmax (h) Cmax (µg/mL) Bioavailability (%)
Beagle dog 1.7a 2.33 964.5b 6.76 –5c 18.94 –
SD rat 3 0.13 21Monkey 3.5 0.011 4.5
a Dose 5 mg/kg; b fed dogs – dose 100 mg/kg of solution of the free acid; c fasteddogs – dose 100 mg/kg of solution of the free acid. SD: Sprague Dawley
2 M. EL KASSAS ET AL.

less protein bound (fu < 0.1) with higher free fractions than theparent drug, which may contribute to significant activity. Intissues of Long–Evans pigmented rats, dasabuvir was found inits highest concentrations in the liver and was minimal in eyelens, skin, and tissues protected by blood–brain barrier. Thedistributed drug concentration declined below the quantifica-tion level 24 h post-dose [17].
4.1. Metabolism
Metabolism studies in all the experimental animal speciesrevealed the biotransformation of the parent drug in severalsteps, starting with the hydroxylation of the tert-butyl groupproducing the first active metabolite M1 [N-(6-(5-(2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl)-3-(1-hydroxy-2-methylpropan-2-yl)-2-methoxyphenyl)naphthalen-2-yl)methanesulfonamide],followed by chemical conversions including glucuronidation,sulfation, and secondary oxidation. The parent drug dasabuvirwas found in highest concentration in plasma, followed by M1metabolite. Other minor metabolites, such as M2, M3, M4, and
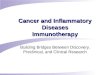
M5, were also detected in rats, mice, and humans [18]. Themetabolic pathway in humans consists of the oxidation ofdasabuvir, followed by conjugation and glucuronidationthrough several biotransformations with no induction or inhi-bition of cytochrome P450 (CYP450) (Figure 1) [18,19].
4.2. Excretion
Dasabuvir and its metabolites are primarily excreted via thebiliary route with a minimal amount of renal elimination.Following oral administration in humans, 94.4% of the totaldose was found in feces and 2.2% in urine with M1 metabolitebeing the most abundant. Comparatively, the parent form ofdasabuvir percentage was 26.2%, M2 15.2%, and M5 11.1%. Inrats, M3 metabolite was mostly found in feces, with lower than2% found in urine. In lactating Sprague Dawley rats, the parentdrug and its M1 metabolite were found in milk at ratios 77.5%and 8.2%, respectively. In dogs, the parent drug and M1metabolite were mostly found in feces [17].
Dasabuvir A-998821 (ABT-333) Parent drugMajor , detected in human, dogs, rat, and mice
M 1 metabolite (A-1041392; hydroxy)Major , detected in mouse , rat, and human
M2 – sulfate metaboliteMinor, detected in mouse, rat, and human
M3 – glucuronide Minor, detected in mouse , rat, and humanMajor metabolite in mouse on 5000 mg/kg/day on Day 160
M4- dehydrogenatedMinor , detected in mouse , rat, andhuman
M5 – carboxylic acid Minor , detected in mouse, rat, and human
Figure 1. Biotransformation of dasabuvir in humans and animals.
EXPERT OPINION ON DRUG DISCOVERY 3

5. Pharmacokinetics of drug–drug interactions
Data obtained from the in vitro studies of dasabuvir were con-firmed by subsequent clinical observation. Dasabuvir was foundto be moderately affected by CYP3A4, P-gp, OATP, and BCRP,whereas CYP2C8 was the most prominent metabolizing enzyme,which was confirmed by the increased dasabuvir plasma levelwhen coadministered with potent CYP2C8 inhibitor (gemfibro-zil). Furthermore, dasabuvir is a weak UGT1A1 inhibitor with noclinical interaction. The levels of UT1A4, 1A6, 1A9, and 2B7 sub-strates were found to be affected when coadministered withdasabuvir. In addition, no drug interaction was seen betweendasabuvir and drugs eliminated by the kidneys, since dasabuvir isnot a substrate or inhibitor of renal transport proteins, such asOAT1, OAT3, OCT1, OCT2, MATE1, and MATE2K [20].
6. Toxicological studies
6.1. Single-dose toxicity
Toxicological studies were performed using rodents and non-rodents. Due to the maximal exposure of dasabuvir obtained,the possibilities to conduct single-dose toxicity studies were low.Hence, dasabuvir could not be formulated in parenteral forms dueto its poor solubility in aqueous and nonaqueous vehicles [14].
6.2. Repeated dose toxicity
Repeated dose toxicity studies were conducted on both rodents(mice and rats) and non-rodents (dogs and rabbits). It was foundthat after multiple administrations of dasabuvir, its concentra-tion in the blood level was 16- and 62-fold higher in rats anddogs, respectively. These levels were higher than the projectedhuman exposure (13.6 μg h/mL) and were found to be welltolerated in both the species. An irritated gastrointestinal tractwas observed in mice at very high doses of the drug (6000–12,000 mg/kg/day) with no systemic effects, and this was thelone significant finding in all preclinical species tested [17].
A 6-month rat study reported some non-adverse findings:alveolar histiocytosis (at levels higher than 31 μg h/mL) andgranulomatous inflammation of the ileum (at levels higher than119 μg h/mL). A 9-month dog study demonstrated lymphoiddepletion (in males at levels higher than 184 μg h/mL) and ele-vated cholesterol, ALP, ALT, SDH, GGT, and total bilirubin at levelshigher than 500 μg h/mL. Dasabuvir had no effect on pharmaco-kinetics when combinedwith pegylated interferon or ribavirin anddid not exacerbate or induce new toxicological observations.Concerning the reproductive study, neither embryo-fetal (per-formed in rats and rabbits) nor mutagenic findings were observedwith negative pre/postnatal development. Carcinogenicity weretested in TgHars mice (at doses 200–6000 mg/kg/day) and in a 2-year rat study (at doses 50,200 and 800 mg/kg/day) to achieveblood levels of 265 and 264 μg h/mL inmice and rats, respectively,with negative carcinogenic outcomes [13,17].
6.3. Safety and secondary pharmacology
Secondary pharmacology of dasabuvir was evaluated in differ-ent studies to detect the effect of the drug on 75 receptors and
channels including G-protein-coupled receptors, ligand binding,and voltage gate receptors. An in vitro assay study of dasabuvirat a dose of 10 µM and a follow-up study at several dosesillustrated displacement of specific binding at different typesof receptors by different ratios, as mentioned in Table 3.
Due to the selective profile of these assays, dasabuvir can beconcluded to have no adverse effects mediated by receptors orion channels. In addition, several neurological evaluations,which include primary Irwin observations, spontaneous locomo-tor activity, nociception, pro/anticonvulsant evaluation, andfunctional observation battery tests, performed on rats at differ-ent doses gave no clinically significant negative outcomes. Theevaluation of respiratory system function revealed no change intidal volume or respiratory rate. No emesis or nausea wasobserved in the gastrointestinal evaluation of dasabuvir. Therewas no effect on sodium barbital latency (150 mg/kg-intraper-itoneal (IP))-induced sleep or sleep duration in rats or whencoadministered with ethanol (200 mg/kg-IP) [17]. Overall, itwas difficult highlighting any expected adverse events withthe clinical use of dasabuvir based on preclinical studies.
6.3.1. Cardiovascular effects of dasabuvirDasabuvir’s cardiovascular effect was evaluated in two in vitrostudies using cardiac Purkinje fiber and hERG current changedetection. A glucagon-like peptide (GLP) hERG in vitro assayshowed that an IC50 of 0.3 µg/mL concentration inhibitedhERG potassium current, which was much lower than thatpredicted concentration believed to be effective in humans.In vitro investigation of Purkinje fibers showed no prolonga-tion in action potential duration up to the highest concentra-tion tested (14.93 µg/mL).
The cardiovascular effects of dasabuvir on anesthetizeddogs were evaluated in three different studies at three differ-ent dose ranges (low, mild, and high doses). In a high and middose study, dasabuvir was found to induce increased meanarterial pressure (MAP) of 7 mmHg and the shortening of theQT interval (14 ms) at plasma concentration range of 0.32–1.85 µg/mL. These effects were found to be independent ofthe plasma concentration of the drug, but were related to therate of infusion. These are evidenced by the results of a lowdose study in which no presser effects on MAP or QT intervalwere observed even though the blood concentrations wereraised to higher concentrations (as high as 0.7 μg/mL).
A GLP conscious dog study showed no negative observa-tion on blood pressure, heart rate, and ECG parameters atdoses of 1 and 3 mg/kg. Comparatively, a mild reduction inblood pressure (13 mmHg) occurred 2 h post dosing at a doseof 10 mg/kg (corresponding to a plasma concentration of6190 ng/mL) [17] (Table 4).
Table 3. Displacement of specific binding by dasabuvir at different types ofreceptors.
V1a receptor (percentage ofinhibition)
Cl− (percentage ofinhibition)
Dose (µM) 10 82% 102%0.1 1% 3%0.3 3% 10%1 14% 55%3 54% 94%
4 M. EL KASSAS ET AL.

7. Resistance profile
The survival of the replicon-containing cell in mediumscontaining higher concentrations of dasabuvir (up to 10-or 100-fold the IC50) has led to the discovery of resistantvariants. Indeed, it still retains full activity against variantsresistant to polymerase inhibitors, suggesting that the com-bined therapy of dasabuvir with NS3/NS4A protease inhibi-tor (ABT-450) plus ritonavir and NS5A inhibitor (ABT-267)will provide a promising resistance barrier with a high treat-ment outcome as evidenced by the results of phase 3clinical trials [14].
Replicon variants with reduced dasabuvir susceptibilitywere identified by the application of higher concentrationsof dasabuvir (10–100 fold >IC50) in HCV replicon-containingcell lines 1a and 1b, plated together with G418. The vastmajority of cells could not survive after 3 weeks of treatment,but those cells that managed to survive formed colonies thatcontained the resistant variants. These variants were furtheridentified by the gradual elevation of dasabuvir concentration,and each variant was isolated at the specific correspondingdasabuvir concentration; 43% of colonies were found to con-tain S556G variant at 10-fold increased concentration.However, the C316Y variant was found to be most predomi-nant at a 100-fold higher concentration (than the IC50) with40% prevalence. Y448C, C451R, and S556G were found toconstitute 20% of the total variants. By mutagenesis, aminoacids were substituted and introduced to 1a (H77) and 1b(con) to evaluate the effects of these variants on dasabuvirIC50. In 1a (H77) replicon and at concentrations which were 10-fold higher than the IC50 of dasabuvir, A395G, M414T, N444K,S556G, S556N, and S565F variants granted 10–32-fold resis-tance while variants like C316Y, Y448C, and Y448H granted940-fold dasabuvir resistance at the same concentration.C451R and D559G variants could not be detected due totheir poor replicability [10]. Regarding genotype 1b (con1)variants, C316Y and M414T, were the most predominant at10-fold concentration (higher than IC50). The impact of eachvariant on dasabuvir resistance is illustrated in Table 5 [14].
In brief, C316Y was found to be the most resistant variantthat showed approximately 1400-fold increased resistance todasabuvir over genotype 1a and 1b. One cell culture studyusing combined treatment of dasabuvir with ribavirin andparitaprevir (NS3/4A protease inhibitor) or ombitasvir (NS5Ainhibitor) revealed synergistic pattern [21].
8. Clinical efficacy
Clinical evaluation, through several phases of clinical testing,had dasabuvir demonstrate great activity with sustained vir-ologic response (SVR) rates greater than 90% when combinedwith ombitasvir/paritaprevir and ritonavir with or without riba-virin when used for the treatment of genotype 1 chronichepatitis C patients. This 3D regimen was recently approvedby the FDA and was created by AbbVie [21].
Fifty-eight phase 1 clinical trials were performed to evalu-ate the effect of dasabuvir on healthy subjects including stu-dies to detect drug–drug interactions in addition to 25 phase2 clinical trials performed on HCV-infected patients (some areillustrated in Table 6) [21].
The antiviral activity of dasabuvir was tested as a compo-nent of an interferon-containing regimen in a placebo con-trolled trial. Patients with GT1a and GT1b chronic hepatitis Cinfection were randomized to four groups. The placebo con-trol (GT1a/1b) patients received interferon and ribavirin for28 days while the three treatment groups received fixeddoses of dasabuvir at 300, 600 and 1200 mg b.i.d., respectivelyas a monotherapy for the first 2 days followed by 26 days ofinterferon and ribavirin. Ten out of the 24 patients from thetreatment group showed HCV RNA <LLOQ at the end of thestudy while none in the placebo group showed such anachievement [31].
Another phase 2 randomized double-blind study investi-gated a dasabuvir–interferon combined regimen. Treatment ofnaïve patients was randomized to three groups that received400 mg dasabuvir b.i.d. for 3 days followed by a combinedregimen or dasabuvir with a standard dose of interferon andribavirin. The second group received the same treatment regi-men with a dasabuvir dose changed to 800 mg b.i.d. Anotherthird control group had a placebo with interferon and riba-virin. After a 12-week study period, group 1 achieved 87.5%SVR while the other two groups achieved 62.5% (group 2) and18.2% (control group) SVR. Further subgroup analysis demon-strated higher response rates for GT1b compared to GT1a(1.45 vs. 0.82). Although dasabuvir showed great SVR enhance-ment results compared to the usual standard care of therapy,it was not a commonly prescribed combination [32].
Table 4. Dose range of the in vitro and in vivo dasabuvir studies.
Doses
In vitro study hERG current using stablytransfected HEK beagle
0.0336, 0.0944, 0.571 µg/mL0.4, 1.4, 4.3 µg/mL
Cardiac Purkinje fiber usingfiber beagle
0.18, 1.43,14.93 µg/mL
In vivo study Anesthetized dog Low dose: 0.001, 0.003,0.010 mg/kg/min IV
Mild dose: 0.003, 0.011,0.032 mg/kg/min IV
High dose: 0.011,0.032,0.105 mg/kg/min IV
Conscious dog 1, 3, 10 mg/kg PO
GLP controlled study doses to block hERG (IC50 = 0.3 µ/mL). GLP: glucagon-likepeptide; IC50: 50% inhibition; IV: intravenous.
Table 5. The impact of each variant on dasabuvir resistance.
Genotype 1a (H77)A395G 10–32-fold increase in resistanceM414TN444KS556GS556NS565FC316Y 940-fold increase in resistanceY448CY448HGenotype 1b (con1)S556G 11-fold increase in resistanceS368T 47–139-fold increase in resistanceN411SM414TA553VC445F 16-fold increase in resistanceC451SI585VC316Y 1569-fold increase in resistance
EXPERT OPINION ON DRUG DISCOVERY 5

Numerous large studies have been conducted to detect theSVR achievement rates of dasabuvir containing regimens indifferent patient populations, such as treatment experiencedversus naïve patients, cirrhotics versus non-cirrhotics andthose with HIV coinfection (Table 7). In general, dasabuvir-included regimens demonstrated great efficacy and safety inthe management of different patient groups suffering fromchronic HCV.
9. Conclusion
Dasabuvir is an RNA-dependent RNA polymerase enzyme withselective activity restricted to genotype 1a and 1b, which wascreated after a screening campaign of the dihydrouracil frag-ment. Preclinical studies demonstrated its positive features forbiological activity. These studies were conducted using tissuecultures, rodents, and non-rodents including dogs and rabbits.They further illustrated that dasabuvir has accepted pharma-cokinetic properties allowing its administration for subjects inphase 1 clinical trials. In terms of adverse drug events, sec-ondary pharmacological studies investigating the action ofdasabuvir on different types of receptors showed no notice-able receptor-mediated effect on different body systems
including the gastrointestinal, respiratory, and cardiovascularsystems at the recommended doses. Repeated dose studiesrevealed no harmful effects of the compound on the repro-ductive system nor carcinogenicity or mutagenicity. Regardingdrug–drug interactions, preclinical pharmacological in vitrostudies revealed some drug–drug interactions, mainly attribu-ted to CYP2C8 inhibitors (the main metabolizing enzyme ofdasabuvir) with no other noticeable important interactions,indicating a truly eliminated drug.
10. Expert opinion
Dasabuvir is a non-nucleoside analog that binds to polymeraseenzyme outside its active site. This class of drug is less wellrepresented in the current HCV treatment armamentarium eventhough they are used as ‘add-on’ drugs to other combinationsof drugs from other drug classes. Review of the various pre-clinical and clinical trials clearly showed the effective role ofdasabuvir in the management of chronic HCV and its impact ondifferent genotypes, mostly genotype 1a and 1b. Generally, thisdrug is considered safe and carries no major side effects.Dasabuvir is proven to have a clear effective synergistic rolewhen added to a combination therapy with other DAAs despite
Table 6. Different registered clinical trials including dasabuvir.
Study IDClinicalTrials.gov ID No. Study purpose Design Phase
M10-687 [22] NCT00768690 A study in healthy adult subjects to evaluate the safety, tolerability, and pharmacokinetics ofmultiple doses of ABT-333
Randomizeddouble-blind
Phase 1
M10-351 [23] NCT00696904 Study of ABT-333 in both healthy volunteers and hepatitis C virus (HCV) + genotype 1-infectedsubjects
RandomizedDouble-blind
Phase 1
M10-459 [24] NCT00726882 A follow-up assessment of resistance to ABT-333 in hepatitis C virus (HCV)-infected subjectswho have received ABT-333 in ABT-333 studies
Single-groupopen-label
Phase 2
M10-687 [25] NCT00768690 A study in healthy adult subjects to evaluate the safety, tolerability, and pharmacokinetics ofmultiple doses of ABT-333
Randomizeddouble-blind
Phase 1
M11-031 [26] NCT00909636 A study to assess the safety, tolerability, and pharmacokinetics of multiple ascending doses ofthe ABT-333 tablet
Randomizeddouble-blind
Phase 1
M11-032 [27] NCT00895102 Bioavailability of ABT-333 tablet versus First in Human (FIH) capsule formulation and safety,tolerability, and PK study of single oses of ABT-333 in healthy volunteers
Randomizeddouble-blind
Phase 1
M14-108 [28] NCT02052349 Bioavailability of ABT-333 within the gastrointestinal tract in healthy subjects Single-groupopen-label
Phase 1
M10-351 [29] NCT00726882 A follow-up assessment of resistance to ABT-333 in hepatitis C virus (HCV)-infected subjectswho have received ABT-333 in ABT-333 studies
Single-groupopen-label
Phase 2
M11-603 [30] NCT01716585 Efficacy and safety of ABT-450, ritonavir, ABT-267 and ABT-333 with ribavirin in HCV G1treatment-naïve adults.
Randomizeddouble-blind
Phase 3
M12-187 [13] PK and safety of multiple oral doses of paritaprevir/r, ombitasvir, and dasabuvir taken whilenonfasting in healthy adult subjects.
Randomizedopen-label
Phase 1
M12-189 [13] PK, safety, and tolerability of ketoconazole with ombitasvir/paritaprevir/r taken with andwithout dasabuvir in healthy subjects.
Randomizedopen-label
Phase 1
M12-196 PK, safety, and tolerability of gemfibrozil (CYP2C8 inhibitor) with dasabuvir and paritaprevir/r inhealthy subjects.
Open-label Phase 1
M12-197 PK, safety, and tolerability of a single dose of diazepam or hydrocodone bitartrate/acetaminophen with ombitasvir, paritaprevir/r and dasabuvir in healthy adult subjects.
Open-label Phase 1
M12-198 PK, safety, and tolerability of a single dose of warfarin on paritaprevir/rand ombitasvir and/ordasabuvir in healthy subjects
Open-label Phase 1
M12-199 PK, safety, and tolerability of a single or repeated dose of omeprazole in healthy subjects. Open-label Phase 1M12-200 PK, safety, and tolerability of rosuvastatin or pravastatin on paritaprevir/r with ombitasvir and/
or dasabuvir.Open-label Phase 1
M12-201 PK, safety, andtolerability of a single dose of digoxin on paritaprevir/r and ombitasvir with orwithout dasabuvir in healthy subjects
Open-label Phase 1
M12-202 PK, safety, and tolerability of darunavir and ritonavir with ombitasvir/paritaprevir/r with orwithout dasabuvir
Open-label Phase 1
M12-204 PK, safety, and tolerability of a single dose of escitalopram or duloxetine with ombitasvir,paritaprevir/r with and without dasabuvir on the PK, safety, and tolerability in healthysubjects.
Open-label Phase 1
M12-205 PK, safety, and tolerability of combined oral contraceptive containing EE + NGM withombitasvir/paritaprevir/r with or without dasabuvir
Open-label Phase 1
NGM: norgestimate; EE: ethinyl estradiol; PK: pharmacokinetics.
6 M. EL KASSAS ET AL.

showing a moderate antiviral efficacy when used alone.Accordingly, dasabuvir cannot be considered as a backboneor even a key player in treatment therapies. However, it isstrongly recommended to be used in combination with otherDAAs from different classes. This explains its real success whenpresented as the ‘combo’ or ‘3D’ regimen for the effectivemanagement of HCV where it proved to have the potentialfor successful viral eradication. The main limitations in the useof dasabuvir include its exclusive genotype 1a and 1b activityand the requirement for a longer duration of therapy whenused in treating genotype 1a cirrhotic patients. Indeed, theinability in using this drug with CHILD B cirrhotic patientsbecause of possible serious adverse events and its limitedgenotypic coverage represent its main weak points.Furthermore, the discovery of some variants resistant to dasa-buvir necessitates the need to use the drug in combination witha NS3/NS4A protease inhibitor and NS5A inhibitor in order toprovide a therapy with an increased resistance barrier.Currently, dasabuvir has been licensed along with paritaprevir/ritonavir, ombitasvir, and ribavirin. This combination of drugs iswell tolerated with an acceptable safety profile that could havean impact on a patient’s adherence to therapy and helps reducethe occurrence of resistance. That being said, the presence ofdasabuvir in a combination will lead to a higher pill burden,which can negatively influence compliance. Another drawbackof this combination therapy approach is the appearance ofdrug-drug interaction issues due to the multitude of drugsbeing used together with each drug in the combination havingits own metabolism mechanism. Post-marketing studies are stillwarranted to further elucidate the generalizability of dasabuvirand its safety.
The availability of different treatment options and strate-gies to manage HCV is one of the cornerstones in the treat-ment of such diseases. Combination therapies that consist ofmedications from various treatment classes help to enhancethe response and potentiate the treatment barrier to resis-tance. Ongoing research with HCV medications are highlight-ing the discovery of safe and effective therapies that targetother mechanisms to increase the response to therapy,
shorten the duration, or even replace a drug like ribavirinwithout impairing the clinical efficacy of the treatment. Thus,dasabuvir is a good addition to the HCV treatment module,but there are still major issues that need to be addressed inHCV drug discovery.
Acknowledgment
This manuscript was language edited by ManuscriptEdit by Reseapro.
Funding
This paper was not funded.
Declaration of interest
The authors have no relevant affiliations or financial involvement with anyorganization or entity with a financial interest in or financial conflict withthe subject matter or materials discussed in the manuscript. This includesemployment, consultancies, honoraria, stock ownership or options, experttestimony, grants or patents received or pending, or royalties.
References
Papers of special note have been highlighted as either of interest (•) or ofconsiderable interest (••) to readers.
1. Cooke GS, Lemoine M, Thursz M, et al. Viral hepatitis and the globalburden of disease: a need to regroup. J Viral Hepat. 2013;20:600–601.
2. Mohd Hanafiah K, Groeger J, Flaxman AD, et al. Global epidemiol-ogy of hepatitis C virus infection: new estimates of age-specificantibody to HCV seroprevalence. Hepatology. 2013;57:1333–1342.
3. Lauer GM, Walker BD. Hepatitis C virus infection. N Engl J Med.2001;345:41–52.
4. Ford N, Kirby C, Singh K, et al. Chronic hepatitis C treatment out-comes in low- and middle-income countries: a systematic reviewand meta-analysis. Bull WHO. 2012;90:540–550.
5. Ford N, Singh K, Cooke GS, et al. Expanding access to treatment forhepatitis C in resource-limited settings: lessons from HIV/AIDS. ClinInfect Dis. 2012;54:1465–1472.
6. Davies A, Singh KP, Shubber Z, et al. Treatment outcomes oftreatment-naïve hepatitis C patients coinfected with HIV: a
Table 7. Large studies on administration of dasabuvir.
Study name Phase Design Purpose
CO-PILOT study [33] Phase 2 Open-label To assess the efficacy of paritaprevir/ritonavir combined with dasabuvir at two different dosesAVIATOR [34] Phase 2 Open-label 8-, 12-, and 24-week study in treatment of naïve and null responder, non-cirrhotic patients using
different doses of ABT-450/rit+ dasabuvir + RBVSAPPHIRE-I [35] Phase 3 Double-blinded 12-week study in treatment of naïve non-cirrhotic using Dasabuvir/ABT-
450/RTV/ombitasvir/ribavirin regimenSAPPHIRE-II [36] Phase 3 Double-blinded 12-week study in treatment of experienced non-cirrhotic patients using Dasabuvir/ABT-
450/RTV/Ombitasvir/ribavirin regimenTURQUOISE-I [37] Phase 2 Open-label 12-week study in the treatment of HCV/HIV coinfected patients using dasabuvir/ABT-
450/RTV/ombitasvir/ribavirin regimen + atazanavir or raltegravirTURQUOISE-II [38] Phase 3 Open-label 12- and 24-week study for the treatment of in naïve or experienced cirrhotic patients using dasabuvir/
ABT-450/RTV/ombitasvir/ribavirin regimen
PEARL II [39] Phase 3 Open-label 12-week study for the treatment of GT 1b in experienced patients using dasabuvir/ABT-450/rit/ombitasvir with and without ribavirin
PEARL – III [39,40] Phase 3 Double-blinded 12-week study for the treatment of GT 1b in naïve patients using dasabuvir/ABT-450/rit/ombitasvir withand without ribavirin (placebo replacing ribavirin)
PEARL – IV [39] Phase 3 Double-blinded 12-week study for the treatment of GT 1a in naïve patients using dasabuvir/ABT-450/rit/ombitasvir withand without ribavirin (placebo replacing ribavirin)
CORAL – I [41] Phase 2 Open-label 12- and 24-week period study for the treatment of post liver transplantation in naïve HCV patients withmild or no fibrosis
EXPERT OPINION ON DRUG DISCOVERY 7

systematic review and meta-analysis of observational cohorts. PLoSOne. 2013;8:e55373.
7. Jacobson IM, McHutchison JG, Dusheiko G, et al. Telaprevir forpreviously untreated chronic hepatitis C virus infection. N Engl JMed. 2011;364:2405–2416.
8. PoordadF,McCone J Jr, BaconBR, et al. Boceprevir for untreated chronicHCV genotype 1 infection. N Engl J Ned. 2011;364:1195–1206.
9. Lawitz E, Lalezari JP, Hassanein T, et al. Sofosbuvir in combinationwith peginterferon alfa-2a and ribavirin for non-cirrhotic, treat-ment-naive patients with genotypes 1, 2, and 3 hepatitis C infec-tion: a randomised, double-blind, phase 2 trial. Lancet Infect Dis.2013;13:401–408.
10. Lawitz E, Poordad F, Kowdley KV, et al. A phase 2a trial of 12-weekinterferon-free therapy with two direct-acting antivirals (ABT-450/r,ABT-072) and ribavirin in IL28B C/C patients with chronic hepatitisC genotype 1. J Hepatol. 2013;59:18–23.
11. Lawitz E, Poordad FF, Pang PS, et al. Sofosbuvir and ledipasvirfixed-dose combination with and without ribavirin in treatment-naive and previously treated patients with genotype 1 hepatitis Cvirus infection (LONESTAR): an open-label, randomised, phase 2trial. Lancet. 2014;383:515–523.
12. Everson GT, Sims KD, Rodriguez-Torres M, et al. Efficacy of aninterferon- and ribavirin-free regimen of daclatasvir, asunaprevir,and BMS-791325 in treatment-naive patients with HCV genotype 1infection. Gastroenterology. 2014;146:420–429.
13. AbbVie. Dasabuvir investigator’s brochure, Edition 8. 2015 June 10.14. Kati W, Koev G, Irvin M, et al. In vitro activity and resistance
profile of dasabuvir, a nonnucleoside hepatitis C viruspolymerase inhibitor. Antimicrob Agents Chem. 2015;59(3):1505–1511.
• Characterization of the molecular target of dasabuvir.15. Liu Y1, Lim BH, Jiang WW, et al. Identification of aryl dihydrouracil
derivatives as palm initiation site inhibitors of HCV NS5B polymer-ase. Bioorg Med Chem Lett. 2012;22(11):3747–3750.
16. NewDrugsApproval, Monthly achieves May 2014. Dasabuvir[Online], Available from: https://newdrugapprovals.org/2014/05/page/6/(Accessed 5 January 2017).
17. European Medicines Agency. European public assessment report(EPAR) for Exviera. [Online], Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medic i n e s / 0 0 3 8 3 7 / h u m a n _ m e d _ 0 0 1 8 3 3 . j s p & m i d =WC0b01ac058001d124. (Accessed 2 January 2017).
18. Shen J, Serby M, Reed A, et al. Metabolism and disposition ofhepatitis C polymerase inhibitor dasabuvir in humans. DrugMetabolism and Disposition. 2016;44(8):1139–1147.
19. Maring C, Wagner D, Hutchinson D, et al. Preclinical potency,pharmacokinetic and ADME characterization of ABT-333, a novelnon-nucleoside HCV polymerase inhibitor. J Hepatol. 2009;50(1):S347.
20. Badri PS, King JR, Polepally AR, et al. Dosing recommendations forconcomitant medications during 3D anti-HCV therapy. ClinPharmacokinet. 2016;55:275–295.
21. Trivella JP1, Gutierrez J, Martin P. Dasabuvir: a new direct antiviralagent for the treatment of hepatitis C. Expert Opin Pharmacother.2015;16(4):617–624.
•• Clinical demonstration of efficacy.22. Abbott. A study in healthy adult subjects to evaluate the safety,
tolerability, and pharmacokinetics of multiple doses of ABT. In:ClinicalTrials.gov [Internet]. Bethesda (MD): National Library ofMedicine (US); 2010. cited 2016 Dec 11. Available from: https://clinicaltrials.gov/ct2/show/NCT00768690
23. Abbott. Study of ABT-333 in both healthy volunteers and hepatitisC virus (HCV) + genotype 1-infected subjects. In: ClinicalTrials.gov[Internet]. Bethesda (MD): National Library of Medicine (US; 2010.cited 2016 Dec 11. Available from: https://clinicaltrials.gov/ct2/show/NCT00696904
24. AbbVie. A follow-up assessment of resistance to ABT-333 in hepa-titis C virus (HCV)-infected subjects who have received ABT-333 inABT-333 studies. In: ClinicalTrials.gov [Internet]. Bethesda (MD):
National Library of Medicine (US; 2014. cited 2016 Dec 11.Available from: https://clinicaltrials.gov/ct2/show/NCT00726882
25. Abbott. A study in healthy adult subjects to evaluate the safety,tolerability, and pharmacokinetics of multiple doses of ABT-333. In:ClinicalTrials.gov [Internet]. Bethesda (MD): National Library ofMedicine (US; 2010. cited 2016 Dec 11. Available from: https://clinicaltrials.gov/ct2/show/NCT00768690
26. Abbott. A study to assess the safety, tolerability, and pharmacoki-netics of multiple ascending doses of the ABT-333 tablet. In:ClinicalTrials.gov [Internet]. Bethesda (MD): National Library ofMedicine (US; 2010. cited 2016 Dec 11. Available from: https://clinicaltrials.gov/ct2/show/NCT00909636
27. Abbott. Bioavailability of ABT-333 tablet versus First in Human (FIH)capsule formulation and safety, tolerability and PK study of single dosesof ABT-333 in healthy volunteers. In: ClinicalTrials.gov [Internet].Bethesda (MD): National Library of Medicine (US; 2010. cited 2016 Dec11. Available from: https://clinicaltrials.gov/ct2/show/NCT00895102
28. AbbVie. Bioavailability of ABT-333 within the gastrointestinal tractin healthy subjects. In: ClinicalTrials.gov [Internet]. Bethesda (MD):National Library of Medicine (US; 2014. cited 2016 Dec 11. Availablefrom: https://clinicaltrials.gov/ct2/show/NCT02052349
29. AbbVie. A follow-up assessment of resistance to ABT-333 in hepa-titis C virus (HCV)-infected subjects who have received ABT-333 inABT-333 studies. In: ClinicalTrials.gov [Internet]. Bethesda (MD):National Library of Medicine (US; 2014. cited 2016 Dec 11.Available from: https://clinicaltrials.gov/ct2/show/NCT02052349
30. AbbVie. A study to evaluate chronic hepatitis C infection. In:ClinicalTrials.gov [Internet]. Bethesda (MD): National Library ofMedicine (US); 2015. cited 2016 Dec 11. Available from: https://clinicaltrials.gov/ct2/show/NCT01716585
31. Rodriguez-Torres M, Lawitz E, Cohen D. Treatment-naive, HCV gen-otype 1-infected subjects show significantly greater HCV RNAdecreases when treated with 28 days of ABT-333 plus peg inter-feron and ribavirin compared to peg interferon and ribavirin alone.Hepatology. 2009;50(Suppl 4):91A.
32. Gaultier I, Cohen D, Dumas E, et al. 12-week efficacy and safety ofABT-072 or ABT-333 with pegylated interferon + ribavirin, following3-day monotherapy in genotype 1 HCV infected treatment-naivesubjects [abstract1329]. 21st Conference of the Asian PacificAssociation for the Study of the Liver (APASL); 17-20 February2011; Bangkok, Thailand.
33. Poordad F, Lawitz E, Kowdley KV, et al. Exploratory study of oralcombination antiviral. N Engl J Med. 2013;368(1):45–53.
34. Kowdley KV, Lawitz E, Poordad F, et al. Phase 2b trial of interferon-free therapy for hepatitis C virus genotype 1. N Engl J Med.2014;370(3):222–232.
35. Feld JJ, Kowdley KV, Coakley E, et al. Treatment of HCV with ABT-450/r-ombitasvir an dasabuvir with ribavirin. N Engl J Med.2014;370(17):1594–1603.
36. Zeuzem S, Jacobson IM, Baykal T, et al. Retreatment of HCV withABT-450/rombitasv and dasabuvir with ribavirin. N Engl J Med.2014;370(17):1604–1614.
37. Eron JJ, Lalezari J, Slim J, et al. Safety and efficacy of ombitasvir -450/r and dasabuvir and ribavirin in HCV/HIV-1 co-infected patientsreceiving atazanavir or raltegravir ART regimens. J Int AIDS Soc.2014;17(4 Suppl 3):19500.
38. Poordad F, Hezode C, Trinh R, et al. ABT-450/r-ombitasvir andDasabuvir with ribavirin for hepatitis C with cirrhosis. N Engl JMed. 2014;370(21):1973–1982.
39. Ferenci P, et al. ABT-450/r-ombitasvir and dasabuvir with or withoutribavirin for HCV. N Engl J Med. 2014;370(21):1983–1992. PEARL III andIV.
40. Ferenci P, Nyberg A, Enayati P, et al. PEARL III: 12 weeks of ABT-450/R/267 + ABT-333 achieved SVR in >99% of 419 treatment-naiveHCV genotype 1B-infected adults with or without ribavirin. JHepatol. 2014;60(1):S527.
41. Kwo PY, Mantry PS, Coakley E, et al. An interferon-free antiviralregimen for HCV after liver transplantation. N Engl J Med.2014;371:2375–2382.
8 M. EL KASSAS ET AL.