Embed Size (px)
Citation preview
Journal of Electrocardiology Vol. 30 No. 2 1997
Discrepant Drug Act ion of D i s o p y r a m i d e on ECG Abnormal i t i e s and Induct ion of
Ventricular Arrhythmias in a Pat ient With Brugada S y n d r o m e
Masaomi Chinushi, MD, Yoshifusa Aizawa, MD, Yusuke Ogawa, MD, Masami Shiba, MD, and Kazuyoshi Takahashi, MD
Abstract: An electrophysiologic study was attempted in a patient who expe- rienced cardiac arrest. Programmed electrical stimulation from the right ven- tricle, without the use of any drugs, induced ventricular fibrillation (VF) twice. Disopyramide prevented the induction of ventricular arrhythmia by rendering VF to a nonsustained polymorphic ventricular tachycardia when administered at 300 mg/day, and noninducible at 400 mg/day. However, ST- segment elevation and the rSr' pattern in leads V~-s characteristic of Brugada syndrome became exaggerated by disopyramide. Disopyramide exerted dis- crepant action on the electrocardiographic (ECG) abnormalities and induction of VF in this patient, suggesting the efficacy of antiarrhythmic drugs assessed by an electrophysiologic study may be unrelated to ECG abnor/nalities in cases of Brugada syndrome. Key words: ventricular fibrillation, Brugada syndrome, disopyramide.
In 1992, Brugada (I) repor ted eight patients wi th idiopathic ventr icular fibrillation (VF) charac- terized by right bundle b ranch block and ST-seg- m e n t elevat ion in the precordial leads. Such patients have since consti tuted a distinct clinical and electrocardiographic (ECG) category. The cause and m e c h a n i s m beh ind the ECG changes due to Brugada syndrome are not known.
A notable electrophysiologic finding was ob- served in a pat ient w h o exper ienced cardiac arrest. Disopyramide, a type la an t ia r rhy thmic drug, was
From the First Department of Internal Medicine, Niigata University School of Medicine, Niigata, Japan.
Reprint requests: Yoshifusa Aizawa, MD, First Department of Internal Medicine, Niigata University School of Medicine, 1-754 Asahimachi, Niigata 951, Japan.
© 1997 Churchill Livingstone
effective in prevent ing the induct ion of VE al- though ST-segment elevat ion and the rSr' pa t te rn of the precordial leads became exaggerated as found in Brugada syndrome (1). The drug's actions were discrepant, prevent ing VE but enhancing the ECG abnormalit ies.
Case Report
In December 1994, a 41-year-old m a n was referred to our hospital for fur ther examina t ion of syncope attacks, the last of which resulted in a traf- fic accident. He did not have symptoms suggesting in f l ammatory disease or ischemic hear t disease.
The results f rom a physical and a neurological examina t ion taken on admission were normal . Hematologic and b lood-chemis t ry analyses were
133
134 Journal of Electrocardiology Voi. 30 No. 2 April 1997
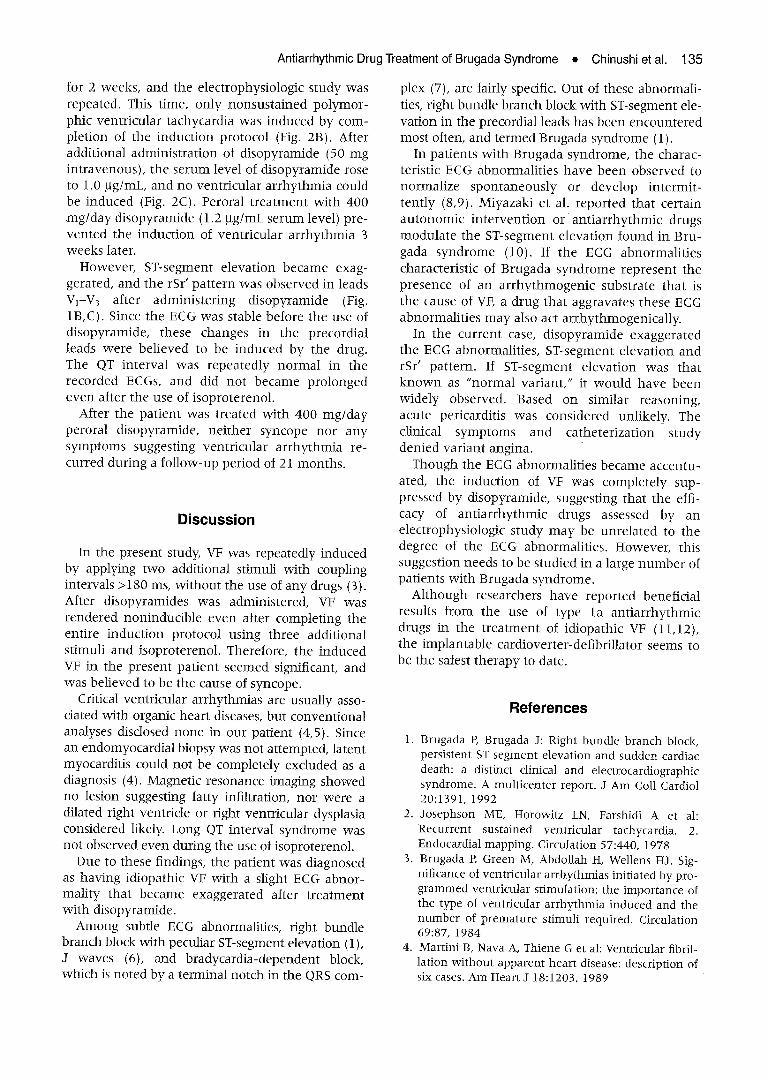
also normal. The two-dimensional echocardio- gram, treadmill exercise test, Holter electrocardio- gram, and electroencephalogram all showed nor- mal findings. The result of thallium-201 myocardial scintigraphy was not unusual, and mag- netic resonance imaging showed a healthy heart with no fatty infiltration. The coronary angiograms and both ventriculograms were normal, and the ejection fraction of the left ventricle was 70%. Intracoronary administration of methylergonovine did not induce coronary spasm. Also, the head-up tilting test resulted negative. However, the 12-lead ECG showed slight elevation of the ST-segment in leads V2 and V3 (Fig. 1A).
After obtaining informed consent, an electro- physiologic study was performed using the stan- dard technique. During endocardial mapping (2), no ECG abnormalities, including fractionation, low amplitude, or double potential, were recorded in any segment of the right ventricle. Electrical stimu- lation to the right atrium showed normal function- ing of the sinoatrial and atrioventricular nodes, and AH and HV intervals of 100 and 40 ms, respec- tively, during normal sinus rhythm.
To induce ventricular tachyarrhythmia, one to three additional stimuli and rapid pacing at cycle lengths up to 286 ms were used in two sites in the right ventricle and one site in the left ventricle before and after administering isoproterenol. The coupling intervals of the additional stimuli were always kept > 180 ms.
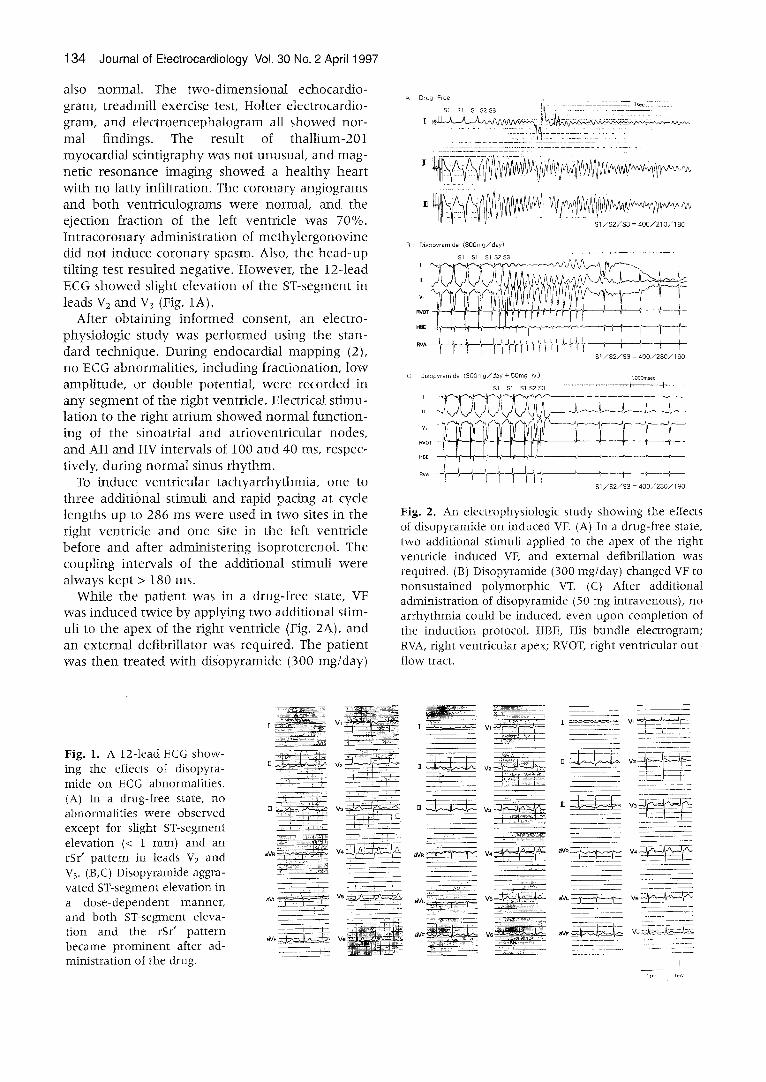
While the patient was in a drug-free state, VF was induced twice by applying two additional stim- uli to the apex of the right ventricle (Fig. 2A), and an external defibrillator was required. The patient was then treated with disopyramide (300 mg/day)
A Drug Free
SI Sl $I S2 $3 i~ -, - ................
. . . . . . . . . . . r . . . . .
i f i . . . . . . . . . . . . . . . . . . . . . .
! :E I. L 7 : ~:: "
B : Disopyramide ( 3 0 0 m g / d a y )
12 SI/$2/$3 = 400/230/I O0
C : Diso~yramide (300rag/day + 50mg iv,) lOOOmse~
$1 $1 $1 $2S3 . . . . . . . . . . . . . . . . . . . I I ~
S1/$2/$3 = 400/230/1 ~0
Fig. 2. An electrophysiologic study showing the effects of disopyramide on induced VF. (A) In a drug-free state, two additional stimuli applied to the apex of the right ventricle induced VE and external defibrillation was required. (B) Disopyramide (300 mg/day) changed VF to nonsustained polymorphic VT. (C) After additional administration of disopyramide (50 mg intravenous), no arrhythmia could be induced, even upon completion of the induction protocol. HBE, His bundle electrogram; RVA, right ventricular apex; RVOT, right ventricular out- flow tract.
Fig. I. A 12-lead ECG show- ing the effects of disopyra- mide on ECG abnormalities. (A) In a drug-free state, no abnormalities were observed except for slight ST-segment elevation (< 1 mm) and an rSr' pattern in leads v2 and V3. (B,C) Disopyramide aggra- vated ST-segment elevation in a dose-dependent manner, and both ST-segment eleva- tion and the rSr' pattern became prominent after ad- ministration of the drug.
[ Vl
--- " !-.~ w ~ h ' i ~ -
~v~ ~ _ _ , , - T ~ v , ~
~v,_~. ~ ' ~ w ~h.:.~-'7%--,-~:~ 1 1 -q
I ..... _ v , ~
][ = v2 ~ _
aVL
v ,
~ w ~ : _ w
r
Antiarrhythmic Drug Treatment of Brugada Syndrome • Chinushi et al. 135
for 2 weeks, and the electrophysiologic study was repeated. This time, only nonsustained polymor- phic ventricular tachycardia was induced by com- pletion of the induction protocol (Fig. 2B). After additional administration of disopyramide (50 mg intravenous), the serum level of disopyramide rose to 1.0 btg/mL, and no ventricular arrhythmia could be induced (Fig. 2C). Peroral treatment with 400 my/day disopyramide (1.2 btg/mL serum level) pre- vented the induction of ventricular arrhythmia 3 weeks later.
However, ST-segment elevation became exag- gerated, and the rSr' pattern was observed in leads VI-V3 after administering disopyramide (Fig. 1B,C). Since the ECG was stable before the use of disopyramide, these changes in the precordial leads were believed to be induced by the drug. The QT interval was repeatedly normal in the recorded ECGs, and did not became prolonged even after the use of isoproterenol.
After the patient was treated with 400 my/day peroral disopyramide, neither syncope nor any symptoms suggesting ventricular arrhythmia re- curred during a follow-up period of 21 months.
Discussion
In the present study, VF was repeatedly induced by applying two additional stimuli with coupling intervals >180 ms, without the use of any drugs (3). After disopyramides was administered, VF was rendered noninducible even after completing the entire induction protocol using three additional stimuli and isoproterenol. Therefore, the induced VF in the present patient seemed significant, and was believed to be the cause of syncope.
Critical ventricular arrhythmias are usually asso- dated with organic heart diseases, but conventional analyses disdosed none in our patient (4,5). Since an endomyocardial biopsy was not attempted, latent myocarditis could not be completely excluded as a diagnosis (4). Magnetic resonance imaging showed no lesion suggesting fatty .infiltration, nor were a dilated right ventricle or right ventricular dysplasia considered likely. Long QT interval syndrome was not observed even during the use of isoproterenol.
Due to these findings, the patient was diagnosed as having idiopathic VF with a slight ECG abnor- mality that became exaggerated after treatment with disopyramide.
Among subtle ECG abnormalities, right bundle branch block with peculiar ST-segment elevation (1), J waves (6), and bradycardia-dependent block, which is noted by a terminal notch in the QRS com-
plex (7), are fairly specific. Out of these abnormali- ties, right bundle branch block with ST-segment ele- vation in the precordial leads has been encountered most often, and termed Brugada syndrome (1).
In patients with Brugada syndrome, the charac- teristic ECG abnormalities have been observed to normalize spontaneously or develop intermit- tently (8,9). Miyazaki et al. reported that certain autonomic intervention or antiarrhythmic drugs modulate the ST-segment elevation found in Bru- gada syndrome (10). If the ECG abnormalities characteristic of Brugada syndrome represent the presence of an arrhythmogenic substrate that is the cause of VE a drug that aggravates these ECG abnormalities may also act arrhythmogenically.
In the current case, disopyramide exaggerated the ECG abnormalities, ST-segment elevation and rSr' pattern. If ST-segment elevation was that known as "normal variant," it would have been widely observed. Based on similar reasoning, acute pericarditis was considered unlikely. The clinical symptoms and catheterization study denied variant angina.
Though the ECG abnormalities became accentu- ated, the induction of VF was completely sup- pressed by disopyramide, suggesting that the effi- cacy of antiarrhythmic drugs assessed by an electrophysiologic study may be unrelated to the degree of the ECG abnormalities. However, this suggestion needs to be studied in a large number of patients with Brugada syndrome.
Although researchers have reported beneficial results from the use of type la antiarrhythmic drugs in the treatment of idiopathic VF (11,12), the implantable cardioverter-defibrillator seems to be the safest therapy to date.
References
1. Brugada P, Brugada J: Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol 20:1391, 1992
2. Josephson ME, Horowitz LN, Farshidi A et al: Recurrent sustained ventricular tachycardia. 2. Endocardial mapping. Circulation 57:440, 1978
3. Brugada P, Green M, Abdollah H, Wellens HJ. Sig- nificance of ventricular arrhythmias initiated by pro- grammed ventricular stimulation: the importance of the type of ventricular arrhythmia induced and the number of premature stimuli required. Circulation 69:87, 1984
4. Martini B, Nava A, Thiene Get al: Ventricular fibril- lation without apparent heart disease: description of six cases. Am Heart J 18:1203, 1989

136 Journal of Electrocardioiogy Vol. 30 No. 2 April 1997
5. Lemery R, Brugada P, Bella PD et al: Ventricular fib- rillation in six adults without overt heart disease. J Am Coll Cardiol 13:911, t989
6. Bjerregaad P, Gussak DI, Kotar SL et al: Recurrent syncope in a patient with prominent J wave. Am Heart J 127:1426, 1994
7. Aizawa Y, Tamura M, Chinushi M et al: Idiopathic ventricular fibrillation and bradycardia-dependent intraventricular block. Am Heart J 126:1473, 1993
8. Brugada J, Brugada P: Right bundle branch block, ST segment elevation and sudden cardiac death. Symptomatic, asymptomatic and intermit tent form. Pacing Clin Electrophysiol 18:95 I, 1995
9. Sumiyoshi M, Nakata Y, Hisaoka T: A case of idio- pathic ventricular fibrillation with incomplete right
bundle branch block and persistent ST segment ele- vation. Jpn Heart J 34:661, 1993
10. Miyazaki % Mitamura H, Miyoshi S e t al: Autonomic and ant iarrhythmic drug modulat ion of ST segment elevation in patients with Brugada syndrome. J Am Coil Cardiol 7 : i06I , 1996
l 1. Belhassen B, Shapira I, Shoshani D et al: Idiopathic ventricular fibrillation: inducibility and beneficial effects of class I ant iarrhythmia agents. Circulation 75:809, 1987
12. Aizawa Y, Naitoh N, Washizuka T et al: Electrophysi- ological findings in idiopathic recurrent ventricular fibrillation: special reference to mode of induction, drug testing, and long-term outcomes. Pacing Clin Electrophysiol 19:929, 1996