Embed Size (px)
Citation preview

t
CLINICAL STUDY
Discriminant Analysis of Native Thoracic Aortic
Curvature: Risk Prediction for Endoleak Formation
After Thoracic Endovascular Aortic Repair
Hazuki Nakatamari, MD, Takuya Ueda, MD, PhD, Fumio Ishioka, DSc,Bhargav Raman, BS, Koji Kurihara, DSc, Geoffrey D. Rubin, MD,
Hisao Ito, MD, PhD, and Daniel Y. Sze, MD, PhD
ABSTRACT
Purpose: To determine the association of native thoracic aortic curvature measured from computed tomographic (CT) angiographycategorized by discriminant analysis with the development of endoleaks after thoracic endovascular aortic repair (EVAR).
Materials and Methods: Forty patients (28 men, 12 women; mean age, 74 y; range, 40–89 y) with aortic diseases treated with thoracicEVAR were evaluated. Diseases treated included atherosclerotic aneurysm (n � 27), penetrating atherosclerotic ulcer (n � 4), intramuralhematoma (n � 3), mycotic aneurysm (n � 3), and anastomotic pseudoaneurysm (n � 3). Quantitative analysis of native aortic morphologywas performed on preprocedural CT angiograms with an original customized computer program, and regional curvature indices in eachanatomic segment of the aorta were calculated. Patterns of native thoracic aortic morphology were analyzed by discriminant analysis. Theassociation between the morphologic pattern of the aorta and the presence and type of endoleak was assessed.
Results: After leave-one-out cross-validation methods had been applied, the sensitivity, specificity, and accuracy to detect endoleakformation in a new population group by discriminant analysis of the patterns of native aortic curvature were estimated as 84.0%,58.8%, and 73.8%, respectively. Compared with the no-endoleak group, the type Ia endoleak group had greater curvature at the aorticarch, the type Ib endoleak group had greater curvature at the thoracoabdominal junction, and the type III endoleak group had greatercurvature in the midportion of the descending aorta.
Conclusions: Discriminant analysis of native thoracic aortic morphology measured from CT angiography is a useful tool to predictthe risk of endoleak formation after thoracic EVAR and should be implemented during treatment planning and follow-up.
ABBREVIATIONS
EVAR � endovascular aneurysm repair, TEVAR � thoracic endovascular aortic repair
wt
dianmc
N
Tw
©
J
Since the United States Food and Drug Administrationapproved the first commercially available stent-graft prod-uct in 2005 (1), thoracic endovascular aortic repair (EVAR)has become widely accepted as a first-line option for thetreatment of a multitude of thoracic aortic diseases, includ-ing atherosclerotic aortic aneurysms, intramural hemato-mas, penetrating aortic ulcers, mycotic aneurysms, trau-matic aortic transections, and aortic dissections (1-4).Although thoracic EVAR has proven its safety and efficacy
From the Department of Radiology (H.N., T.U., H.I.), Chiba University Hospi-tal, 1-8-1 Inohana, Chuo-ku, Chiba-city, Chiba 260-8677, Japan; School of Law(F.I.) and Graduate School of Environmental Science (K.K.), Okayama Univer-sity, Okayama, Japan; Department of Radiology (T.U., B.R., D.Y.S.), StanfordUniversity School of Medicine, Stanford, California; and Department of Radi-ology (G.D.R.), Duke University Medical Center, Durham, North Carolina.Received September 27, 2010; final revision received February 16, 2011;
accepted February 22, 2011. Address correspondence to T.U.; E-mail:[email protected] Dith satisfactory short- to midterm results (5,6), the long-erm outcomes remain unproven.
Several studies have suggested that longstanding en-oleaks, particularly type I endoleaks, are the most signif-cant risk factor for postoperative aneurysmal expansionnd rupture (7). Although many investigators have recog-ized the contribution of aortic morphology to the achieve-ent of adequate device fixation and seal (8-10), the spe-
ific relationship between aortic curvature and the risk of
one of the authors have identified a conflict of interest.
his article includes an Appendix and Figure 3 that can be viewed online atww.jvir.org.
SIR, 2011
Vasc Interv Radiol 2011; 22:974–979
OI: 10.1016/j.jvir.2011.02.031

vH
uFtvtwommtdficpTcmmtappnt
ndova
Volume 22 � Number 7 � July � 2011 975
endoleak formation after thoracic EVAR has not been de-fined quantitatively to our knowledge. Quantitative defini-tion of risk would require a systematic, reproducible, ob-jective, evaluative algorithm of aortic morphology.
The quantitation of vascular curvature from medianflow-lumen centerlines has been used to characterize theabdominal aorta (11) and the coronary, cerebral (12), reti-nal, and iliac arteries (13). We applied this technique to thequantitative assessment of thoracic aortic morphology. Inaddition, we used the technique of discriminant analysis, astatistical method used to categorize groups of events bymeans of an array of quantitative variables, to predict therisk of endoleak formation based on subcategorization ofaortic morphology (14). The purpose of this study was toassess the impact of native thoracic aortic morphology onthe subsequent development of endoleaks after thoracicEVAR based on discriminant analysis of computed tomo-graphic (CT) angiography.
MATERIALS AND METHODS
PatientsThe institutional review board approved this retrospectivestudy and waived the requisite to obtain informed consentfrom patients. All patients had consented to their thoracic
Figure 1. Flowchart of patient eligibility and exclusions for theto the type of the endoleak observed. Two patients each had twoendoleak was included as a separate case. TEVAR � thoracic e
EVAR procedures, including the use of investigational de- s
ices. All patient data were handled in compliance with theealth Insurance Portability and Accountability Act.
Between April 2001 and September 2008, 121 consec-tive patients were enrolled prospectively in one of sixood and Drug Administration–sponsored clinical trials
esting the thoracic EXCLUDER or TAG stent-graft de-ices (W.L. Gore and Associates, Flagstaff, Arizona). Pa-ients with acute, subacute, or chronic aortic dissectionsere excluded from this study because of the complexitiesf aortic morphology characterization and the differentechanisms and definitions of endoleaks in the presence ofultiple lumina (15). Patients with acute traumatic aortic
ransections were also excluded, as the emergency proce-ural planning frequently required exceptions from the of-cial specified anatomic inclusion criteria, and led to asso-iated adverse events unique to this pathologic process. Allatients underwent CT angiography before thoracic EVAR.he routine postprocedural outpatient imaging protocol in-luded a follow-up CT angiogram by 1 month, another at 3onths if any issues including endoleaks were identified at 1onth, at 6 and 12 months after thoracic EVAR, and annually
hereafter. We excluded patients for whom preprocedural CTngiography was not available or was of inadequate quality,atients who were not followed for at least 6 months, andatients for whom information about endoleak occurrence wasot available. As a result, from the 121 enrolled patients, aotal of 40 patients (28 men, 12 women) were included in this
ontrol study. Patients were divided into five groups accordingent types of endoleaks (type Ia and III, type Ib and III), and eachscular aortic repair.
case-cdiffer
tudy. Their mean age was 74 years (range, 40–89 y; Fig 1).

otm
titcalarc
GAcptwdfbmwpeecdtrwttetcm
AAEtsvwa
SDesotarpw
976 � Native Thoracic Aortic Curvature and Risk of Endoleak in EVAR Nakatamari et al � JVIR
Patient demographic data and primary indications for thoracicEVAR are summarized in Table 1.
CT Angiography ProtocolCT angiography was performed with one of four models ofmultiple–detector row scanners, corresponding approximatelyto the date of examination and availability of new scanners:one eight-row scanner (LightSpeed Ultra; GE Medical Sys-tems, Milwaukee, Wisconsin); two 16-row scanners (Soma-tom Sensation 16 [Siemens, Forchheim, Germany] and Light-Speed Ultra 16 [GE Medical Systems]); and a 64-row scanner(Sensation 64; Siemens). CT angiographic scans were acquiredwith a 1.25-mm (eight-row scanner), 0.75-mm (16-row scanner),or 0.625-mm (64-row scanner) section thickness and were recon-structed at 0.6-mm intervals.
Nonionic iodinated contrast medium (350 mgI/mL)was injected through an antecubital vein at a rate of 4–6mL/s, tailored to the body weight of the patient (16). Thetotal volume of contrast medium administered was deter-mined as the product of the scan time plus 8 secondsmultiplied by the injection rate. The arterial phase of theinjection was determined by using automated bolus trigger-ing. A delayed acquisition for the assessment of endoleakswas also obtained 90 seconds after contrast medium injec-tion in all CT angiograms obtained after thoracic EVAR.
Image AnalysisThe median centerline and the margin of the aortic flow lumenwere extracted from the ascending aorta through the celiacartery with a previously reported analytical tool (11,13,17)(Fig 2). The mean diameter and the curvature (�) of the aorticflow lumen were calculated at 1-mm increments along themedian luminal centerline. The detailed methods for thesemorphologic analyses are described in the Appendix (avail-able online at www.jvir.org). For anatomic landmarks, therigins of the brachiocephalic artery, the celiac artery, andhe proximal and distal aneurysm necks were mapped to the
Table 1. Clinical Features of Study Patients (N � 40)
Characteristic Value
Age (y)
Mean 74
Range 40–89
Sex
Male 28 (70)
Female 12 (30)
Aortic pathologic process treated
Atherosclerotic aneurysm 27 (67.5)
Penetrating atherosclerotic ulcer 4 (10.0)
Intramural hematoma 3 (7.5)
Mycotic aneurysm 3 (7.5)
Anastomotic pseudoaneurysm 3 (7.5)
Note.—Values in parentheses are percentages.
edian centerline, and the longitudinal distances between i
hese landmarks were recorded. The lower limit of the prox-mal neck was defined as the point where the outer diameter ofhe aorta exhibited a change of 15% or more in the minor axis,ompared with the diameter just below the left subclavianrtery for the lower limit of the proximal neck, and the upperimit of the distal neck was defined as that above the celiacrtery. The curvature of the aortic flow lumen was plottedelative to the longitudinal position along the median luminalenterline path (Fig 2b).
rouping by Endoleak Formationboard-certified radiologist with 12 years of experience in
ardiovascular radiology retrospectively reviewed all post-rocedural CT angiograms to establish the presence andype of endoleak. Assessment of endoleaks was performedith postprocedural CT angiograms by following a stan-ard, previously reported method (4,7,18). This assessmentor endoleak formation was performed with the investigatorlinded to the original radiologic reports and all subsequentorphologic quantification. The result was then comparedith the final clinical report at the time of primary inter-retation. In the event of a discrepancy, the case wasvaluated by a second radiologist with 13 years of experi-nce with thoracic EVAR, who settled the discrepancy byonsensus with the primary retrospective reviewer. En-oleaks were classified based on the standardized classifica-ion for EVAR (7,18). Patients with early endoleaks thatesolved spontaneously within 1 month after thoracic EVARere classified in the no-endoleak group. When more than one
ype of endoleak was present in a patient, each endoleak wasreated as an independent case. Seventeen patients had nondoleak, 21 patients had one endoleak, and two patients hadwo endoleaks, resulting in a total of 42 cases that wereategorized into five groups (Fig 1). Endoleaks occurred 0–82onths (mean, 28.5 mo) after thoracic EVAR.
dverse Events After Thoracic EVARcomprehensive survey of adverse events after thoracic
VAR was performed by a review of all hospital records,rial records, and imaging studies. Endoleaks treated byurgical repair, additional stent-graft placement, or inter-entional embolization were targeted. Repeat interventionsere also tallied, whether open surgical or endovascular,
nd the indications for repeat intervention were recorded.
tatistical Analysisiscriminant analysis was used to classify the future risk of
ndoleak formation by type (19). Detailed methods are de-cribed in the Appendix (available online at www.jvir.rg) (20). The results of discriminant analysis were translatedo sensitivity, specificity, accuracy, positive predictive value,nd negative predictive value to precisely predict the occur-ence and type of actual observed endoleaks. Concordance ofredicted risk of endoleak formation by discriminant analysisas assessed by the percentage of the error of categorization
nto the different endoleak groups. To assess the predictive

col1ldccr
ess9nevrva
g7
dwrwtecwrca
dwwap
Ec(
ional i
Volume 22 � Number 7 � July � 2011 977
reliability of this discriminant analysis for a future patientpopulation, we performed leave-one-out cross-validation (17).
RESULTS
The computer-based curvature analysis was completed suc-cessfully in all 40 patients. Figure 3 (available online atwww.jvir.org) illustrates the mean and SD of the curvatureindex at each segment, separated by endoleak type. Thetype 0 no-endoleak group showed a peak curvature of 0.29cm�1 at segment 4 (segments illustrated in Fig 3), whichcorresponded to a sharp curve at the aortic arch. The type Iaendoleak group showed a constant curvature index of ap-proximately 0.2 cm�1 throughout the segments 1–5, whichorresponded to a constant large curvature index through-ut the aortic arch. The type Ib endoleak group showed aarge curvature index of more than 0.15 cm�1 at segments2–14, which corresponded to redundancy and sharp angu-ation at the thoracoabdominal junction. The type III en-oleak group showed a large curvature of more than 0.2m�1 at segments 4–8, which corresponded to a largeurvature index in the midportion of the descending tho-acic aorta.
Tables 2 and 3 summarize the results of the risk ofndoleak formation predicted by discriminant analysis. Theensitivity, specificity, and accuracy to predict endoleak irre-pective of the type of endoleak were 100%, 76.5%, and0.5%, respectively (Table 2). Among all patients, discrimi-ant analysis categorized 83.3% of patients into the correctndoleak type risk group (Table 3). The positive predictivealue and negative predictive value were 86.2% and 100%,espectively (Table 2). After applying leave-one-out cross-alidation methods, we estimated the sensitivity, specificity,
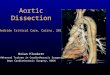
Figure 2. (a) Preprocedural volume-rendered three-dimensionVAR shows an atherosclerotic aneurysm extending from the denterline was calculated and superimposed (arrow). The curvcm�1), measured at 1-cm intervals. The aorta showed strong an
curvature was plotted as a function of location along the medianand distal necks were determined, corresponding to the location ofcorresponded to the three angulated regions on the three-dimens
nd accuracy to detect endoleak formation in a new population
roup by discriminant analysis to be 84.0%, 58.8%, and3.8%, respectively.
Seven cases were misclassified into an incorrect en-oleak risk group by discriminant analysis. Two casesith observed type Ib endoleaks were categorized incor-
ectly into the type Ia and type III risk groups, and oneith type III endoleaks was categorized incorrectly into
he type Ia risk group. One case of an observed type IIndoleak was misclassified into the no-risk group. Inontrast, three cases without any observed endoleaksere categorized into a risk group—two into the type Ia
isk group and one into the type Ib group. Incorrectategorizations based on curvature indices did not showny recognizable patterns or tendencies.
Among 25 observed endoleaks, 10 (eight type I en-oleaks and two type II endoleaks) resolved spontaneouslyithout any additional treatment. Eight type I endoleaksere small leaks, all diagnosed in the late phase without the
ppearance of contrast medium extravasation in the arterialhase.
angiographic image in an 84-year-old woman before thoracicrtic arch to the descending thoracic aorta. The median luminalndex was calculated as the inverse of the radius of curvaturen at three distinct regions (arrowheads). (b) The corresponding
line of the flow lumen of the aorta. The locations of the proximaldian centerline. The high peaks over 0.19 cm�1 of curvature index
mage (arrowheads). (Available in color online at www.jvir.org.)
Table 2. Predictive Matrix for Presence of Endoleak FromDiscriminant Analysis
Predicted
Observed
Endoleak (�) Endoleak (�) Total
Endoleak (�) 13 0 13
Endoleak (�) 4 25 29
Total 17 25 42
Note.—Sensitivity was 100%, specificity was 76.5%; positivepredictive value was 86.2%, and negative predictive valuewas 100%.
al CTistal aoature igulatiocenterthe me
Ten endoleaks remained unchanged during follow-

top
mpbcydt
archmewcep
fa
sUcbcwttsI
tjwafapfadecleFsmvmdn
nEpr
978 � Native Thoracic Aortic Curvature and Risk of Endoleak in EVAR Nakatamari et al � JVIR
up, without evidence of aneurysmal enlargement, andhave not required any additional treatment. Repeat inter-ventions for endoleaks were performed in five patients:one patient underwent surgical repair, two patients un-derwent additional stent-graft placement, and two pa-tients underwent additional embolization of the left sub-clavian artery.
DISCUSSION
Many investigators have reported that the diameter andlocation of landing zones are the most significant riskfactors for early endoleak formation after thoracic EVAR(7,21,22). In addition to the risk factors associated withearly endoleaks, Czerny et al (23) reported that late en-doleaks occurring more than 6 months postoperatively reflecta different but overlapping set of independent risk factors.Although the results of that study (23) suggested that theortuosity of the aortic arch may independently affect the riskf endoleak formation, the association between aortic mor-hology and endoleak formation has not been fully delineated.
Correlation between aortic morphology and endoleak for-ation requires an objective method to evaluate aortic mor-
hology. In the present study, we evaluated aortic morphologyy quantitative assessment of curvature by using the medianenterline method. In addition, we applied discriminant anal-sis to assess the curvature profile. This algorithm was vali-ated by its accurate prediction of the risk of endoleak forma-ion with 100% sensitivity and 76.5% specificity.
All patients with observed endoleaks, except for one withtype II endoleak, were categorized successfully into a high-
isk group. Four patients with no observed endoleaks wereategorized incorrectly into a high-risk group, a relativelyarmless false-positive finding with little impact on decision-aking other than encouraging vigilant follow-up. Type II
ndoleaks were difficult to predict because they are associatedith coverage of branch vessels, and therefore have little
orrelation with aortic curvature. With these few exceptions, thevaluation of aortic morphology by using discriminant analysis
Table 3. Predictive Matrix for Type of Endoleak From Discrim
Predicted Endoleak Type 0 Type Ia
Type 0 14 0
Type Ia 2 9
Type Ib 1 0
Type II 0 0
Type III 0 0
Total 17 9
Correct (%) 82.4 100.0
Erroneous (%) 17.6 0.0
roved to be a reliable method to predict the potential risk of p
uture endoleaks, and may become useful in planning proceduresnd in aiding in decision-making for patient follow-up protocols.
Also, the rate of type I endoleak formation in the presenttudy was higher than those previously reported (7). Recently,eda et al (24) suggested the significance of the “bird-beak
onfiguration”—the radiologic finding of a wedge-shaped gapetween the undersurface of the stent-graft and the aortic wallaused by a lack of apposition of the device to the aorticall—to the risk of type I and III endoleaks. They suggested
hat many small type I endoleaks had been misrecognized asype II endoleaks from small branches, and they found aignificant correlation between type I endoleaks and large typeI endoleaks from the left subclavian artery (24).
The present study has some limitations. First, although wereated 121 patients with thoracic EVAR, the number of sub-ects who met the inclusion criteria for this retrospective studyas small. Second, we excluded aortic dissections from the
ssessment because of the differing mechanisms of endoleakormation compared with aortic aneurysms (15). Patients withortic transections were also excluded because of frequentrotocol deviations and lack of adequate preprocedural timeor planning and morphologic quantification (25). Third, wessessed the landing zones without reference to the actualevice placement in postprocedural studies. Fourth, this studyvaluated only the association between endoleaks and aorticurvature. Other potential contributing parameters, such as theength of the proximal and distal landing zones, aortic diam-ter, and length and number of stent-grafts, were not assessed.ifth, we did not evaluate the persistence of endoleaks or otherubsequent outcomes of endoleaks, such as aneurysm enlarge-ent and rupture. Finally, our rate of endoleak formation was
ery high (59.5%), likely because of our high-sensitivity,ultiphasic, rapid-bolus imaging technique, resulting in the
etection of small and subtle leaks of unknown clinical sig-ificance.
In summary, native thoracic aortic morphology is a sig-ificant factor in predicting endoleak formation after thoracicVAR. Discriminant analysis of native thoracic aortic mor-hology from CT angiography is a useful tool to predict theisk of endoleaks, and may be incorporated into preprocedural
nalysis
Observed Endoleak
Type Ib Type II Type III Total
0 1 0 15
1 0 1 13
4 0 0 5
0 1 0 1
1 0 7 8
6 2 8 42
66.7 50.0 87.5 83.3
33.3 50.0 12.5 16.7
inant A
lanning and postprocedural surveillance protocols.

1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
Volume 22 � Number 7 � July � 2011 979
ACKNOWLEDGMENTS
We thank Kuniyoshi Hayashi for his helpful comments andadvice on the statistical discussion. We thank Hiroshi Suitofor his advisory support on the mathematical contents.
REFERENCES
1. Chu MW, Forbes TL, Kirk Lawlor D, Harris KA, Derose G. Endovascularrepair of thoracic aortic disease: early and midterm experience. VascEndovasc Surg 2007; 41:186–191.
2. Nienaber CA, Fattori R, Lund G, et al. Nonsurgical reconstruction ofthoracic aortic dissection by stent-graft placement. N Engl J Med 1999;340:1539–1545.
3. Greenberg RK, O’Neill S, Walker E, et al. Endovascular repair of tho-racic aortic lesions with the Zenith TX1 and TX2 thoracic grafts: interme-diate-term results. J Vasc Surg 2005; 41:589–596.
4. Svensson LG, Kouchoukos NT, Miller DC, et al. Expert consensusdocument on the treatment of descending thoracic aortic disease usingendovascular stent-grafts. Ann Thorac Surg 2008; 85(Suppl):S1–S41.
5. Demers P, Miller DC, Mitchell RS, et al. Midterm results of endovas-cular repair of descending thoracic aortic aneurysms with first-generationstent grafts. J Thorac Cardiovasc Surg 2004; 127:664–673.
6. Verhoye JP, Miller DC, Sze D, Dake MD, Mitchell RS. Complicatedacute type B aortic dissection: midterm results of emergency endovas-cular stent-grafting. J Thorac Cardiovasc Surg 2008; 136:424–430.
7. Parmer SS, Carpenter JP, Stavropoulos SW, et al. Endoleaks afterendovascular repair of thoracic aortic aneurysms. J Vasc Surg 2006;44:447–452.
8. Bortone AS, De Cillis E, D’Agostino D, de Luca Tupputi Schinosa L.Endovascular treatment of thoracic aortic disease: four years of experi-ence. Circulation 2004; 110:II262–II267.
9. Appoo JJ, Moser WG, Fairman RM, et al. Thoracic aortic stent grafting:improving results with newer generation investigational devices. J Tho-rac Cardiovasc Surg 2006; 131:1087–1094.
10. Serag AR, Bergeron P, Mathieu X, Piret V, Petrosyan A, Gay J.Identification of proximal landing zone limit for proper deployment ofaortic arch stentgraft after supra-aortic great vessels transposition. J Car-diovasc Surg 2007; 48:805–807.
1. Wolf YG, Tillich M, Lee WA, Rubin GD, Fogarty TJ, Zarins CK. Impactof aortoiliac tortuosity on endovascular repair of abdominal aortic aneu-
rysms: evaluation of 3D computer-based assessment. J Vasc Surg 2001;34:594–599.
2. Bullitt E, Gerig G, Pizer SM, Lin W, Aylward SR. Measuring tortuosityof the intracerebral vasculature from MRA images. IEEE Trans MedImaging 2003; 22:1163–1171.
3. Tillich M, Bell RE, Paik DS, et al. Iliac arterial injuries after endovascularrepair of abdominal aortic aneurysms: correlation with iliac curvature anddiameter. Radiology 2001; 219:129–136.
4. Bellin MF, Renard-Penna R, Conort P, et al. Helical CT evaluation ofthe chemical composition of urinary tract calculi with a discriminantanalysis of CT-attenuation values and density. Eur Radiol 2004; 14:2134 –2140.
5. Sze DY, van den Bosch MAAJ, Dake MD, et al. Factors portendingendoleak formation after thoracic aortic stent-graft repair of aortic dis-section. Circ Cardiovasc Intervent 2009; 2:105–112.
6. Fleischmann D, Miller DC. Clinical 3D and 4D imaging of the thoracicaorta. In: Hodler J, Schulthess GK, Zollikofer CL, eds. Diseases of theheart, chest and breast. New York: Springer, 2007; 119–130.
7. Paik DS, Beaulieu CF, Jeffrey RB, et al. Automated flight path planningfor virtual endoscopy. Med Phys 1998; 25:629–637.
8. Rubin GD, Paik DS, Johnston PC, Napel S. Measurement of the aortaand its branches with helical CT. Radiology 1998; 206:823–829.
9. Veith FJ, Baum RA, Ohki T, et al. Nature and significance of endoleaksand endotension: summary of opinions expressed at an internationalconference. J Vasc Surg 2002; 35:1029–1035.
0. Fisher RA. The use of multiple measurements in taxonomic problems.Ann Eugenics 1936; 7:179–188.
1. Piffaretti G, Mariscalco G, Lomazzi C, et al. Predictive factors for en-doleaks after thoracic aortic aneurysm endograft repair. J Thorac Cardio-vasc Surg 2009; 138:880–885.
2. Tse LW, MacKenzie KS, Montreuil B, Obrand DI, Steinmetz OK. Theproximal landing zone in endovascular repair of the thoracic aorta. AnnVasc Surg 2004; 18:178–185.
3. Czerny M, Grimm M, Zimpfer D, et al. Results after endovascular stentgraft placement in atherosclerotic aneurysms involving the descendingaorta. Ann Thorac Surg 2007; 83:450–455.
4. Ueda T, Fleischmann D, Dake MD, Rubin GD, Sze DY. Incompleteendograft apposition to the aortic arch: bird-beak configuration increasesrisk of endoleak formation after thoracic endovascular aortic repair. Ra-diology 2010; 255:645–652.
5. Tehrani HY, Peterson BG, Katariya K, et al. Endovascular repair of
thoracic aortic tears. Ann Thorac Surg 2006; 82:873–877.
979.e1 � Native Thoracic Aortic Curvature and Risk of Endoleak in EVAR Nakatamari et al � JVIR
APPENDIX: METHOD FOR QUANTIFICATION OF AORTIC MORPHOLOGY
Mean orthogonal diameters of the aortic flow lumen and the aortic curvature were calculated according to a previously reportedmethod (1–3). Briefly, the contrast-enhanced flow channel from CT angiographic data was extracted by means of three-dimensionalseeded region growing (4). After the contrast-enhanced aortic lumen was segmented (4,5), three points were manually selected withinthe aorta at the aortic root, the most superior part of the aortic arch, and the level of the origin of the left renal artery in the abdominalaorta. These points defined the limit of calculation of the median luminal centerline of the aortic lumen. The median centerline wasthen computed by means of a median axis transform, which uses repeated morphologic erosion operations that thin the segmented flowchannel while maintaining a connected set of points that defines the median axes through the aorta (5,6).
Subsequently, orthogonal cross-sections of the aortic flow lumen were automatically created at every millimeter along the path (7).From these cross-sections, the cross-sectional area of the aortic flow lumen was calculated as the sum of all identified pixel dimensions.The mean diameter (D) was calculated at 1-mm increments along the centerline as follows:
D � 2�CSA ⁄ �
The curvature index (�) was calculated as the inverse of the radius of curvature (in cm�1) at discrete intervals (in this study, weset 10-mm intervals along the aortic centerline) and mathematically expressed by the following equation:
� � � X' � X� � ⁄ � X'�3
where X= is the magnitude of the first derivative vector of the path, X� is the second derivative vector of the path, and the cross(�) denotes the vector cross-product.
Discriminant Analysis to Predict Type of Endoleak Formation
Multiple discriminant analysis was used for the prediction of endoleak formation (7). S-PLUS software (Mathematical Systems,Tokyo, Japan) was used for the discriminant analysis.
For the standardization of the aorta, the lengths from the brachiocephalic artery to the celiac artery from all cases were adjustedas the reference length. Then, the aorta was divided into 14 segments (ie, 1–14), and the mean curvature index for each segment wascalculated as the explanatory variables (x1�x14). The length between the proximal neck and the distal neck was defined as theindependent parameter of the disease length in each case (x15). x16 and x17 are defined for the parameters of disease location (x16 is1 when the position of the proximal neck is located in the proximal half of the entire aorta and is 0 otherwise; x17 is 1 when the positionof the distal neck is located in the distal half of the entire aorta and is 0 otherwise).
Categoric dependent variables to assess each endoleak risk were determined by linear discriminant functions with x1�x17 variablesby multiple discriminant analysis (Z0, ZIa, ZIb, ZII, and ZIII for no risk of endoleak and risk of types Ia, Ib, II, and III endoleaks,respectively):
Z0 � �118.926 � 3.185x1 � 0.531x2 � 2.382x3 � 0.112x4 � 0.357x5 � 1.743x6 � 0.650x7 � 2.065x8 � 1.469x9 � 1.307x10
� 2.920x11 � 2.820x12 � 1.165x13 � 1.192x14 � 0.113x15 � 15.775x16 � 2.848x17
ZIa � �125.894 � 3.130x1 � 0.302x2 � 2.335x3 � 0.210x4 � 0.509x5 � 1.857x6 � 0.896x7 � 1.510x8 � 0.769x9�0.882x10
� 3.344x11 � 3.146x12 � 1.299x13 � 1.162x14 � 0.114x15 � 19.909x16 � 5.262x17
ZIb � �121.679 � 2.656x1 � 0.010x2 � 2.242x3 � 0.063x4 � 0.239x5 � 1.885x6 � 1.041x7 � 1.382x8 � 0.749x9�1.185x10
� 2.560x11 � 2.365x12 � 0.750x13 � 1.498x14 � 0.103x15 � 19.260x16 � 6.235x17
ZII � �108.314 � 2.626x1 � 0.274x2 � 1.860x3 � 0.354x4 � 0.197x5 � 2.282x6 � 0.492x7 � 1.656x8 � 0.670x9�0.638x10
� 2.829x11 � 2.484x12 � 1.048x13 � 1.144x14 � 0.108x15 � 18.533x16 � 2.651x17
ZIII � �125.915 � 2.821x1 � 0.292x2 � 2.476x3 � 0.299x4 � 0.435x5 � 1.888x6 � 1.099x7 � 1.376x8 � 0.660x9�0.924x10
� 3.109x11 � 3.001x12 � 1.035x13 � 1.301x14 � 0.154x15 � 19.647x16 � 5.554x17
The risk group of the case was determined by the highest number of a Z value among all Z values, which were calculated byapplying x1�x17 values to the equations.
REFERENCES
1. Wolf YG, Tillich M, Lee WA, Rubin GD, Fogarty TJ, Zarins CK. Impact of aortoiliac tortuosity on endovascular repair of abdominal aortic aneurysms: evaluationof 3D computer-based assessment. J Vasc Surg 2001; 34:594–599.

Volume 22 � Number 7 � July � 2011 979.e2
2. Tillich M, Bell RE, Paik DS, et al. Iliac arterial injuries after endovascular repair of abdominal aortic aneurysms: correlation with iliac curvature and diameter.Radiology 2001; 219:129–136.
3. Rubin GD, Paik DS, Johnston PC, Napel S. Measurement of the aorta and its branches with helical CT. Radiology 1998; 206:823–829.4. Lorensen WE, Cline HE. Marching cubes: a high-resolution 3D surface construction system. Comput Graph 1987; 21:163–169.5. Paik DS, Beaulieu CF, Jeffrey RB, Rubin GD, Napel S. Automated flight path planning for virtual endoscopy. Med Phys 1998; 25:629–637.6. Paik DS, Beaulieu CF, Jeffrey RB, et al. Automated flight path planning for virtual endoscopy. Med Phys 1998; 25:629–637.7. Fisher RA. The use of multiple measurements in taxonomic problems. Ann Eugenics 1936; 7:179–188.
Figure 3. Graphs of the curvature index for the different patient groups: (a) type 0, (b) type Ia, (c) type Ib, (d) type II, and (e) type III endoleak. Thelengths from the brachiocephalic artery to the celiac artery for all cases were adjusted as the reference length, and the total length of the thoracicaorta was divided into 14 segments (S1–S14). The mean curvature index and SD calculated for each segment were plotted.