Embed Size (px)
Citation preview

Disease and Public Health
Lecture 11
Medicine, Disease and Society in Britain, 1750 - 1950

Lecture Themes and Outline
• Disease, mortality and demography– McKeown thesis– More recent interpretations
• Three diseases prevalent in c18th and c19th demonstrating varying degrees of state intervention with varying degrees of success– Smallpox – inoculation, vaccination, protests– TB/phthisis – nutrition vs state intervention– Cholera – widespread public health reforms:
sanitation

Smallpox

Edward Jenner (1749-1823)

Cartoon by James Gillray on vaccination against Smallpox using Cowpox serum, 1802., Engraving-hand colour

“It is often assumed that vaccination measures were the means by which the disease was brought under control. This assumption is founded on ignorance of the real limitations of vaccination measures, and undervalues the crucial contribution of associated preventive practices in reducing the incidence and mortality from the disease. Although vaccination was the tool which permitted the eradication of smallpox, the simple availability of vaccination would never have resulted in the eradication of the disease. In the evolution of the methods by which vaccination was made effective, the British smallpox experience, and that of London in particular, is of central importance”
Anne Hardy, The Epidemic Streets (1993): 111

c. 1930

Cholera Outbreaks
• 1826 – second global pandemic, travelled from Asia
• 1831-2 - first hits Britain• 1849 – second British epidemic• 1853-4 • 1865-6

Edwin Chadwick (1800-1890)
1842, Report on the Sanitary Condition of the Working Population of Great Britain.
See Christopher Hamlin 1998 for more details

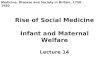
John Snow (1813-1858)

Snow’s map of Broad Street

‘King Cholera’

Public Health Legislation
• 1848 Public Health Act • 1855,1860 and 1863 Nuisance
Removal Acts• 1866 Sanitary Act• 1872 Public Health Act• 1875 Public Health Act • 1889 Infectious Diseases Notification
Act

ConclusionSuccess of public health reforms and state
intervention? Links to mortality decline
Varied from disease to disease:• Smallpox – first effective medical intervention,
state interference, but also opposition, importance of social factors, vaccination just the tool
• TB – state invention after disease had reached it’s peak. Improved nutrition and living standards usually seen as cause of decline, but still debated
• Cholera – linked with the first wide scale sanitary and public health reform. Widespread state intervention, which was reactionary. Largely successful
Others? E.g. Measles – decline not the result of sanitary reform but raised living standards, nutrition

‘In order to re-create the epidemiological landscapes of the past and track the routes and pathways of the world’s major epidemics, we need to understand these dynamics in an ever-changing natural and human world. The ecological and biological chains of disease transmission – where and how each epidemic is spread; the environmental parameters and constraints – geographical and seasonal variations in the natural and physical world; the demographic variables – the density and age structure of a population needed to support an epidemic disease, levels of contact and crowding, and the prior immunological experiences of a community; the multifactorial social, economic, domestic, and personal factors that enter into the equation – standards of living, the nutritional status of a host population, its level of domestic and public hygiene, patterns of residence, occupation, and migration – have each combined with a multitude of elusive factors, from disease mutations to animal-human disease transfers, to govern and determine the spread of each epidemic disease and its global impact.’
Mary Dobson, ‘Epidemics and the Geography of Disease’, in Irvine Loudon (ed.), Western Medicine: An Illustrated History (Oxford: Oxford University Press, 1997), pp. 187-8.