Embed Size (px)
Citation preview

470
LUNG DISEASE DUE TO INHALED DUSTBy K. M. A. PERRY, M.D., F.R.C.P.
Physician to the London and Royal Masonic Hospitals
There is gradual realization that there is a severeair pollution in the industrial areas of the worldand that this is a danger to the communities thatlive in them. In the week following the dense fogon December 8, 1952, there were 4,ooo deaths inexcess of those usual for the time of year, and thesewere attributed to acute bronchitis and its com-plications, resulting from the inhalation of thedioxide and trioxide of sulphur extruded by factoryand domestic chimneys (Beaver Report, I954).The air pollution of cities is constantly presentand the noxious substances are by no means con-fined to the oxides of sulphur. The concentrationsmay sometimes be higher in the factory than inthe city atmosphere. These lesser concentrationscertainly play an important part in the causationof chronic bronchitis and its resultant emphysemaand cor pulmonale, the death rate for these diseasesbeing i,6oo per million in Merseyside, comparedwith 6oo per million in East Anglia and Hamp-shire. It is, therefore, evident that strenuousefforts should be made to control fume and thusreduce air pollution, which produces disease in thewhole community. This is essentially industrialin origin, though it is not always classified asindustrial disease.
Dust DiseasesIt has been known since prehistoric times th at
dust will produce diseases of the lung. It must beof a particle size of less than 5s, to pass through thesmallest bronchioles and reach the alveoli. Somedusts are inert and, therefore, produce no tissuereaction in the lungs. They are important, how-ever, since they may be radio-opaque and, accord-ing to their atomic weight, produce shadows inradiographs-these often cause alarm to patientsand even doctors. Other dust will cause fibrosisand this disease has been called pneumonocoriosis(Greek: pneumon, lung; konis, dust), a wordsometimes incorrectly abbreviated to pneumo-coniosis. Yet other dusts will produce either asensitivity or inflammatory reaction. A few morehave been proved to be carcinogens and to con-tribute to the great increase in the incidence of
carcinoma of the lung. In I900 there were 273deaths in England and Wales from this condition;in 1920, 500; and in 1955, 17,272. It is possiblethat the part played by air pollution is greaterthan is at present realized.
Inert DustsThe most important dust to cause X-ray
shadowing is iron oxide. It occurs commonly inindustry: welders, oxy-acetylene cutters, polishers,tool makers, cutlery makers, foundry workers andhaematite miners have considerable exposure. Thelast two occupations involve exposure to a mixeddust, including silica, and in consequence silicosisis a recognized risk in these occupations. Theradiological shadowing in siderosis is discrete andnodular. The condition produces no symptoms,and it has been shown that if no more iron dustis inhaled the iron oxide is gradually eliminatedfrom the lung parenchyma and the shadowing willbe reduced. Histologically, in the lungs there ismuch amorphous pigment in the periarterial andperibronchial lymphatic channels and the alveolarsacs, but no fibrosis has been found either inlymph glands or in lung tissue.The Registrar-General's Supplementary Report
on Occupation Mortality in 1931 shows that therewere 123 deaths among II,452 welders, comparedwith an expected i6i on the basis of age rates forall males. This evidence alone shows conclusivelythat iron oxide is an inert dust in the lungs. Otherdusts which produce radiological shadowing inindustry are tin oxide, the atomic weight of tinbeing II7.8, and barium, which has an atomicweight of 137.4. Because of the higher atomicweight of these two metals, the shadowing is moredense than in the case of siderosis and the con-ditions have been called, respectively, stannosisand baritosis.
Silver polishers use rouge, which is iron oxide,and are, therefore, exposed to a dust which con-tains a mixture of silver and iron. X-rays of silverpolishers' lungs show the typical picture of reticula-tion. This is partly caused by iron oxide, and alsoin part caused by thei intra-vitam staining of the
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.406.470 on 1 August 1959. D
ownloaded from
PERRY: Lung Disease Due to Inhaled Dusts
elastic tissue of the arterial, alveolar and bronchialwalls with silver oxide.
Sensitivity ReactionsThere is little doubt that certain dusts of organic
origin will produce a sensitivity reaction in thelung, which results in attacks of shortness of breathwith a wheeze. This is probably the result ofoedema of the bronchial wall and over-activity ofthe bronchial mucosal glands, producing narrowingof the smaller bronchioles. Pollens and the dustof wheat and grain are notorious for giving riseto this condition, and it therefore occurs mostlyin millers and bakers. Hair dandruff will alsoproduce such a reaction, and this will be foundin hairdressers and those concerned with thecare of horses or other fur-bearing animals, in-cluding furriers. The complex salts of platinumalso cause an irritation to the nasal passage, throatand trachea. The symptoms are repeated sneezing,followed by tightness of the chest, shortness ofbreath and a wheeze. The symptoms persist aslong as the worker remains in the factory, butabout half an hour after he has left they subside.Radiograms reveal no abnormality.
Organic vegetable dusts have been reportedfrom all over the world as producing pulmonaryreactions. Farmer's lung, which was first de-scribed in England in I932, occurs particularly inhaymakers, but it has been described in all harvestworkers and was in Scandinavia called Thresher'slung. A similar reaction has been described in teatasters, and the disease ' broken wind ' in horses isprobably a similar disease.
In the earlier stages of the war a disease wasfound in those who worked with bagasse, which issugar cane after the sugar has been extracted.Respiratory disease is common in cotton workersand has been called byssinosis. In all these diseasesthe vegetable material seems to be contaminatedby fungi, and many writers have ascribed thedisease to these organisms. They are consistentlypresent in all the dusts, but they are probably notthe immediate cause, though it is possible that byproducing toxic substances they indirectly con-tribute to the aetiology of the condition.Of these diseases, that caused by cotton is by
far the most important in this country. As earlyas i8i8 Jackson drew attention to the fact thatthose who worked in the cotton industry, particu-larly card-room workers, suffered from a charac-teristic respiratory disease. Foreign literature onthe condition is scanty, but it has been reportedfrom both Germany and the United States. Theexact method by which the disease is produced isstill a matter of uncertainty. The protein fractionof card-room dust is capable of producing inflam-matory lesions in animals and the characteristic
course of the disease is suggestive of an acquiredhypersensitivity, but the primarily toxic qualitiesof the protein prevent the condition from beingregarded as purely allergic.
Cotton arrives in England in tightly com-pressed bales and it is the workers who are engagedon the earlier processes who are involved; thosewho open the bales and those who work on thecarding engines, particularly the strippers andgrinders. After working for several years inthe dusty atmosphere the patient begins tosneeze and develop a dry and irritating cough,with a tight feeling in the chest and restrictedintake of breath. To start with the symptoms aretemporary and pass off in a few days, but theyreturn after a short absence from work, such as aweekend, and it is for this reason that the con-dition is sometimes called 'Monday morningfever,' ' mill fever' and 'factory fever.' Disable-ment and incapacity for work does not occur untilthe man has been exposed to the dust for io yearsor more, when the symptoms may become moresevere and persistent, and the patient developattacks of shortness of breath associated with awheeze, shallow breathing, cough and a smallamount of sticky, mucoid sputum. The diseaseprogresses and finally arrives at an incurable stageso that many of these workers die before the ageof fifty from right-sided heart failure.The physical signs and X-ray findings are in no
way different from those associated with chronicbronchitis and emphysema. Necropsies also revealno specific changes in the lung. Death frequentlyresults from cor pulmonale.
SilicosisSilicosis is a fibrosis of the lung caused by the
inhalation of free crystalline silica or quartzparticles. It is the most disabling of all the dustdiseases, yet the precise method by which thesilica causes the disease is not yet established. Itwas thought to be mechanical in origin, beingcaused by the movement of the lung on the sharpcrystals, until in I932 Gardner, in Saranac Lakelaboratories, showed that carborndum (siliconcarbide) crystals, which are just as sharp and hardas those of silica itself, do not produce the diseasein animals. It was then suggested that silica wentinto solution in the phagocytes forming silicic acidand when this was released, as a result of destruc-tion of the phagocyte by infection, either tubercu-lous or non-tuberculous fibrosis resulted. This isknown as the Solubility Theory. It seems mostimprobable, since silicic acid is one of the mostinnocuous of substances it is possible to inject intothe human body. However, in I933 Kettle showedthat by mixing iron oxide with the silica theamount of fibrosis produced in the lung was
August 1959 471
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.406.470 on 1 August 1959. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL
greatly reduced, and the similar finding withaluminium oxide has led to it being used with theidea of treating and preventing silicosis. There isno doubt that mixture with other substances has aprofound influence on the reaction produced inthe lung, and as iron and aluminium slow down theprocess, so alkali appears to accelerate it. This isof great importance in industry, since no industrialdust is a pure dust and, therefore, it is frequentlydifficult to forecast what effect it will have. Itseems certain that the causation of the diseaseresults from some physico-chemical processaround freshly fractured quartz crystals.The classical pathological picture of silicosis is
that of a discrete nodular fibrosis. The fibroblastsforming the nodule have a typical laminatedappearance, which causes the structure of thenodule to resemble the cut surface of an onion.The nodules gradually increase in number andtend to drift outwards towards the pleura. In thelater stages the nodules, particularly in the upperparts of the lung, conglomerate and form massiveareas which tend to undergo degeneration.
Pure silicosis occurs in metalliferous miners,granite quarry workers, metal grinders and sand-stone masons. The most rapidly developingvariety of silicosis which has been reported wasthat encountered in workers engaged in the manu-facture of scouring powders, which are a mixture,of silica, soap and alkali. Women died within aperiod of three years.The symptom caused by the disease is shortness
of breath. This may be exaggerated by catarrhalbronchial infection which leads to cough withsticky sputum and, later, tightness of the chestand a wheeze. There is no doubt that pulmonarytuberculosis is a frequent complication of thedisease-it predisposes to the development of sili-cosis, and silicosis equally predisposes to tubercu-losis. The respiratory impairment can be demon-strated by the reduced vital capacity, maximumbreathing capacity and increased residual air, aswell as a reduction in the blood oxygen tension.Radiograms of the chest show, first, reticulation,then nodulation and, finally, massive shadowing.Later, opacities develop in the mediastinal glands,which become outlined and look like a bunch ofgrapes.
Yearly X-rays can be taken of the workers and,should the disease be seen to be progressive orshould there be the least suggestion of the develop-ment of massive shadowing, they should be wtmoved from exposure to dust at a time when theywill have suffered no disability and will then beable to engage in alternative employment.
Pneumoconiosis of CoalworkersPneumoconiosis of coalminers is the most im-
portant dust disease in the British Isles. Theexistence of the disease in South Wales has beenknown for a century. Thackrah, in i83I, recog-nized that colliers were liable to develop ' miner'sasthma,' and the condition was subsequentlydescribed as the ' scourge of the mines.' With theintroduction of compensation certificates, the in-cidence has rapidly increased. The dust inhaledby coalminers is a mixture of coal, silicates, andsilica. There is no doubt that the quantity of dustinhaled has an important bearing on the incidenceof the disease in different mines. In the past it hasbeen generally thought that the disease was morereadily caused by anthracite than by other coaldusts. It has, however, been shown that the an-thracite mines have been badly ventilated and,therefore, the quantity of dust inhaled by workersin them has been high; a fact which probablyexplains the high incidence in those mines in thepast. With the installation of better ventilation,which has coincided with the greater developmentof mechanical methods in bituminous and steamcoal mines, the quantity of dust in the atmosphereof the different categories of mines have approxi-mated more close to each other, so that there wouldappear not to be a great difference in incidence inthe different categories of mines.When the dust is inhaled into the lungs, it
forms characteristic coal foci. A delicate fibrosisdevelops round these foci and this may proceed tothe development of hard collagen tissue. Theygradually fade into an unaffected lung tissue.Around these coal foci develop areas of honey-combing or focal emphysema. This focal emphy-sema is the characteristic picture of the disease,and it is this destruction of healthy lung and itsreplacement by fibrosis and focal emphysemawhich causes the disability in the disease.
Superimposed on this histological picture ofsimple pneumoconiosis, there may be fibrosisresulting from infection, either tuberculous or non-tuberculous. These massive areas of fibrosisoccur principally in the upper halves of the lungs,especially in the posterior segment of the upperlobe and the apical segment of the lower. Theyare composed of dense, black tissue of a hard,-rubbery consistency, and they usually have a smallcavity in the centre which may contain some blackliquid. Many workers think these lesions areessentially tuberculous in origin. This may be so,but if they are, they run an attenuated course and,both histologically and clinically, there is fre-quently no evidence of tuberculosis. At thepresent time, miners have regular routine X-raysof -their lungs and the disease can, therefore,usually be detected before any symptoms de--velop.
'The essential symptom resulting from the
August I959472
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.406.470 on 1 August 1959. D
ownloaded from

PERRY: Lung Disease Due to Inhaled Dusts
destruction of normally-functioning alveoli isshortness of breath. To start with, this mayoccur only on exertion, but it becomes graduallyprogressive. Later the men may develop a coughfrom bronchitis. When this is associated with thebreaking down of large areas of diseased lung theremay be sputum, and if the black fluid from thecentre of an area of massive fibrosis is coughed up,the symptom has been called melanoptysis. Whenthe first radiological changes are seen, it is unlikelythat there will be any abnormal physical signs but,as the disease develops, the patients become dys-pnoeic and, eventually, orthopnoeic. They mayget clubbing of their fingers, their chests becomebarrel-shaped, and respiratory movements arepoor. Sometimes there is flattening of the chestbelow the clavicle, and often hyper-resonance overthe bases. The air entry may become diminishedand, when bronchitis develops, coarse crepitationsare heard throughout the lungs.
In the early stages the X-ray appearances are ofa fine net-work, sometimes sharp and lace-like inpattern, or, more often, blurred in appearance,scattered throughout the whole of both lung fields,and well marked at the periphery. As the diseasebecomes more advanced, multiple, discreteshadows, 2-3 mm. in diameter, are scatteredthroughout the lung fields. These later may co-alesce or conglomerate, so that massive shadowsdevelop. When these occur there is usually evi-dence of basal emphysema. As the disease pro-gresses, the vital capacity andmaximum ventilatorycapacity are usually below normal, and the residualair is increased. Exercise tolerance tests are alsobelow standard. It is frequently found that whenthese symptoms are present there is a rising bloodsedimentation rate. This is probably the result ofsuperimposed infection, which may be either acatarrhal bronchitis or pulmonary tuberculosis. Ifa man is removed from exposure to the dust beforemassive conglomerations have developed, thedisease does not progress but, when these lesionshave developed, it nearly always pursues a slowcourse, but one which may progress rapidly, evenif the man is no longer in contact with thedust.Once a diagnosis has been made, the patient
should be removed from further exposure to coaldust. If this is done in the early stages he will beable to do full-time work in other industries, butif it is left until the disease is far advanced he willbecome a respiratory invalid. Inhalations of alu-minium dust have been used to attempt to cure thedisease. It is impossible to see what beneficialeffect these may have, and there is certainly noscientific evidence that they produce any change inthe course of the disease, though, frequently, theworkers express the faith that they are better.
SilicatesSilicate dusts are widespread in industry and
their effect on the lung is variable. Asbestos andtalc produce severely disabling diseases, and evendeath-whereas it takes many years for china clayand mica to produce any noticeable changes andthen they are slight.
Asbestos is, therefore, much the most importantof these substances from the health point of view.It is essentially iron-magnesium-aluminium sili-cate but, mineralogically, there are two maintypes. Hornblende or amphibole, in which ironis present in large quantities and which is fre-quently blue in colour. It is produced exclusivelyin South Africa and is widely used in this country.Chrysotile is white and in it magnesium pre-dominates; it is mined in Canada, Rhodesia,Transvaal, Australia, Italy and Russia. The word' asbestos ' is derived from the Greek and means' unconsumable.' The crushed rock can beseparated to an extreme degree of fineness and,therefore, its needle-like crystals can be carded,spun into yarn and woven into cloth. Asbestos isalso used extensively for thermal insulation. It isalso ground and mixed with cement and plasticsto make insulating slabs, boarding, and brakelinings. The dust produced in these various pro-cesses is mostly less than 5s, in diameter.The first recorded case of asbestosis was re-
ported from Charing Cross Hospital in I907,seven years after the patient's death. The accountwas a full story of the disease. The patient diedat the age of 34, being the last survivor of io menwho had worked in a carding room where asbestoswas being carded. They had all died at about theage of 30 with respiratory disease. The recordedpatient had worked in the carding room for I4years. Necropsy revealed extensive, diffuse pul-monary fibrosis and the lungs were found to con-tain asbestos bodies. After this, many cases wererecorded, but it was not until 1930 that activeefforts were made to suppress the disease by theintroduction of exhaust ventilation.
Clinically, the striking symptom is shortness ofbreath of gradually increasing intensity. There isoften a dry cough. Clubbing of the fingers isfrequently a prominent physical sign but, in thelungs in the early stage of the disease, crepitationsare few or absent, but later rales throughout thelungs develop. Radiologically, the most charac-teristic feature is the ' shaggy I outline of the heartshadow, but the fine fibrosis may cause a ' groundglass' appearance throughout the lung fields andthe subpleural thickening may be evident, particu-larly in the interlobar fissures. Examination of thesputum will reveal the presence of asbestos bodies.
Pathologically, pleural adhesions are extensiveand dense, and there are often thick, subpleural
August I1959 'A7y3copyright.
on 12 July 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.406.470 on 1 A
ugust 1959. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
plaques of fibrous tissue. There is increasedconsistency of the lung and there may be largeareas of fibrous condensation which is tough andstony hard. Emphysema is extensive but localizedto the lower and apical parts of the lungs. Pneu-mothorax sometimes occurs. Histologically, thereis generalized fibrosis with diffuse thickening ofthe alveolar walls, while throughout the lung tissuecharacteristic asbestos bodies may be seen.
In recent years, patients with asbestosis haveshown no particular susceptibility to develop pul-monary tuberculosis, but the incidence of car-cinoma appears to have been about 15 per cent.This is much higher than in the general com-munity and it is of particular interest that it isdivided equally between the sexes.The patients usually die from right-sided heart
failure. Throughout, this disease is much morea clinical one than a radiological one-which is amarked contrast with silicosis. While themechanism which produces silicosis is still un-decided, there is little doubt that in the case ofasbestosis it is mechanical in origin, resulting fromthe trauma and mechanical irritation produced bya combination of the long, needle-like crystal, andthe rhythmic movement of the lung and heart.
Talc, or french chalk, is a silicate somewhatsimilar to asbestos. It is a hydrated-magnesiumsilicate. Mineralogically, it is known as steatite,tremolite, anthophylite and asbestine. It is usedin industries as a filler for paper, soaps andpaints; for leather dressing, the manufacture ofrubber motor tyres, making electric switchboards,and for heat insulation for steam pipes. SinceI896 it has been known to be capable of producinglung disease, but it has only been in recent years,and especially in the past io, that it has beenappreciated that there was any considerablenumber of cases. Asbestine being a crystallinesubstance of much the same shape as asbestos, it isnot surprising that a disease clinically similar toasbestosis results; a feature of the histology beingthe presence of bodies similar to asbestos bodies.The principle difference in the two diseases is theslower rate of progress which occurs in talcosis.
China clay or kaolin, is a hydrated silica ofaluminium, and is at the present time an importantexport from this country to the United States. Itis used extensively in the manufacture of fine artpaper, but also is an important ingredient in chinaand earthenware pottery, and is used in the makingof cotton cloth, paint and soap. The largestdeposits of china clay in the world are found inCornwall. Workers have been engaged in theindustry throughout their lives and throughoutthe century and have not appeared to suffer anyill effects. During the past io years, however,radiological surveys have shown that X-ray
changes do occur after many years of exposure tothe dust. These consist of fine mottling, mostmarked in middle zones and at the bases. Massiveshadows have also been found in a few workers.These workers have few symptoms and it isprobable that the dust does not produce great, ifany, disability.
Silimanite is an aluminium silicate found inIndia and used as a refractory material in themanufacture of porcelain. It breaks into pris-matic crystals and not needles like asbestos. Whilethere is some evidence that radiological changesmay result from exposure, there is little evidencethat it produces a disabling disease.
Mica, or shale, is an aluminium-magnesiumsilicate which is widely distributed in nature, andis extensively used commercially. Diatomaceousearth-also known as diatomite, kieselguhr andferina fossil-and Tripoli are hydrated, amor-phous minerals of organic origin and generally con-sidered to be varieties of opal. All these substanceshave been recorded as producing X-ray changes,and it is probable they all produce some pulmonaryfibrosis. However, the disability that results isslight.
CarcinomaIn the Middle Ages, Agricola and Paracelsus
drew attention to the associationship of lungdisease and mining in the mountains of Saxony.They called it the ' mountain disease.' In the lasthalf of the last century it became known that aboutthree-quarters of the miners in this area developed,and died from, a pulmonary disease after about 20years work in the mines; during the presentcentury this disease has been shown to be lungcancer.The main ores in the area are the sulphides and
arsenides of nickel and cobalt. In the southernside of the area there is a high content of pitch-blende and radium. The disease has, therefore,been ascribed variously to arsenic, cobalt and radio-activity. But carcinoma of lung has also beenshown to occur in workers engaged on refiningnickel, in which process there is escape of muchdust which has a high content of arsenic. It hasalso been shown that the incidence of carcinoma inchemical workers, manufacturing arsenical sheep-dips, is twice as high as in the normal population.
It is also possible that arsenic may account forthe world-wide increase in the mortality rate forcarcinoma of lung in males, since cigarette fumecontains 2.5 to 3.5 mg. arsenious oxide per cubicmeter.There is also much evidence that mono-
chromates are carcinogens: 64 per cent. of a groupof workers in seven chromate plants in the UnitedStates died from cancer of the lung, compared with
August I 959474
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.406.470 on 1 August 1959. D
ownloaded from
August I959 PERRY: Lung Disease Due to Inhaled Dusts 475
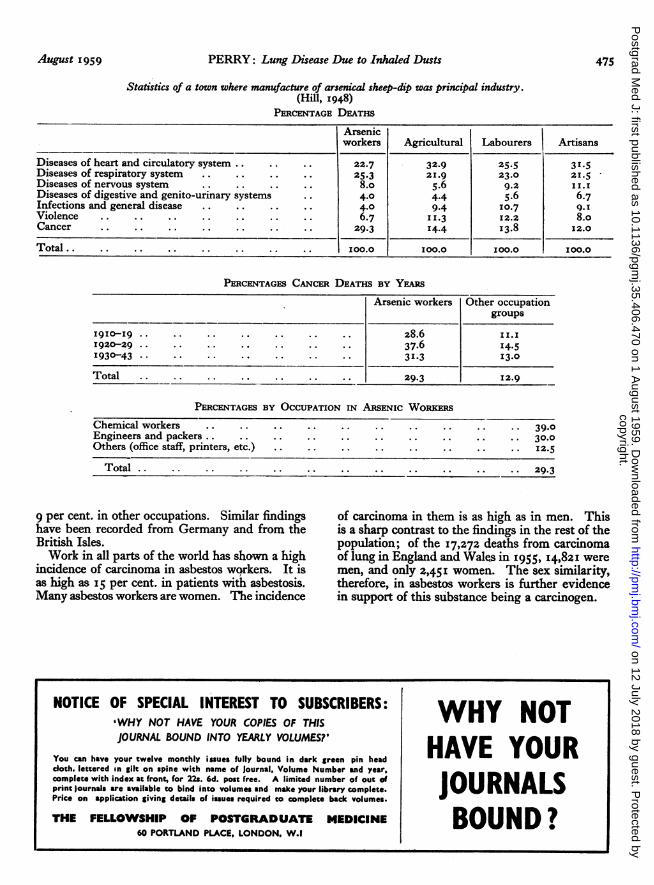
Statistics of a town where manufacture of arsenical sheep-dip was principal industry.(Hill, 1948)
PERCENTAGE DEATHS
Arsenicworkers Agricultural Labourers Artisans
Diseases of heart and circulatory system .. .. .. 22.7 32.9 25.5 31.5Diseases of respiratory system .. .. .. .. 25.3 21.9 23.0 21.5Diseases of nervous system . .. .. .. 8.o 5.6 9.2 11.1Diseases of digestive and genito-urinary systems .. 4.0 4.4 5.6 6.7Infections and general disease .. .. .. .. 4.0 9.4 10.7 9.IViolence .. .. .. .. .. .. .. 6.7 11.3 12.2 8.oCancer .. .. .. .. .. .. .. 29.3 14-4 13.8 12.0
Total . .. .. .. .. .. .. . 100.0 100.0 100.0 100.0
PERCENTAGES CANCER DEATHS BY YEARS
Arsenic workers Other occupationgroups
1920-29 .. .. .. .. .. .. .. 37.6 14.51930-43 .. .. .. .. .. .. .. 31x3 13.0
Total .. .. .. .. .. .. .. 29.3 12.9
PERCENTAGES BY OCCUPATION IN ARSENIC WORKERSChemical workers .. .. .. .. .. .. .. .. .. .. 39.0Engineers and packers .. .. .. .. .. .. .. .. .. 30.0Others (office staff, printers, etc.) .. .. .. .. .. .. .. .. 12.5
Total . . . . . . . . . . . . 29.3
9 per cent. in other occupations. Similar findingshave been recorded from Germany and from theBritish Isles.Work in all parts of the world has shown a high
incidence of carcinoma in asbestos wqrkers. It isas high as I5 per cent. in patients with asbestosis.Many asbestos workers are women. The incidence
of carcinoma in them is as high as in men. Thisis a sharp contrast to the findings in the rest of thepopulation; of the 17,272 deaths from carcinomaof lung in England and Wales in 1955, I4,821 weremen, and only 2,45I women. The sex similarity,therefore, in asbestos workers is further evidencein support of this substance being a carcinogen.
NOTICE OF SPECIAL INTEREST TO SUBSCRIBERS: VN'WHY NOT HAVE YOUR COPIES OF THISJOURNAL BOUND INTO YEARLY VOLUMES?' HAVE
You can have your twelve monthly igaues fully bound in dark green pin head Y O U Rcloth. lettered in gilt on spine with name of Journal, Volume Number and year,complete with index at front, for 22s. 6d. post free. A limited number of out of flhlprint journals ireavtioible to bind into volumes and make your library complute.Price on applcation giving details of issuesrequired eo complete back volumes.
THE FELLOWSHIP OF POSTGRADUATE MEDICINE BOU60 PORTLAND PLACE, LONDON, W.l
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.406.470 on 1 August 1959. D
ownloaded from





























