-
Disease Mapping withWinBUGS and MLwiN
Andrew B. LawsonDepartment of Epidemiology and Biostatistics
University of South Carolina, USA
William J. BrowneSchool of Mathematical Sciences
University of Nottingham, UK
Carmen L. Vidal RodeiroDepartment of Epidemiology and
Biostatistics
University of South Carolina, USA
Innodata047085605X.jpg
-
Disease Mapping with
WinBUGS and MLwiN
-
STATISTICS IN PRACTICE
Advisory Editor
Stephen Senn
University College London, UK
Founding Editor
Vic Barnett
Nottingham Trent University, UK
Statistics in Practice is an important international series of
texts which provide
detailed coverage of statistical concepts, methods and worked
case studies in
specific fields of investigation and study.
With sound motivation and many worked practical examples, the
books
show in down-to-earth terms how to select and use an appropriate
range of
statistical techniques in a particular practical field within
each title’s special
topic area.
The books provide statistical support for professionals and
research workers
across a range of employment fields and research environments.
Subject areas
covered include medicine and pharmaceutics; industry, finance
and commerce;
public services; the earth and environmental sciences, and so
on.
The books also provide support to students studying statistical
courses applied
to the above areas. The demand for graduates to be equipped for
the work
environment has led to such courses becoming increasingly
prevalent at uni-
versities and colleges.
It is our aim to present judiciously chosen and well-written
workbooks to
meet everyday practical needs. Feedback of views from readers
will be most
valuable to monitor the success of this aim.
A complete list of titles in this series appears at the end of
the volume.
-
Disease Mapping withWinBUGS and MLwiN
Andrew B. LawsonDepartment of Epidemiology and Biostatistics
University of South Carolina, USA
William J. BrowneSchool of Mathematical Sciences
University of Nottingham, UK
Carmen L. Vidal RodeiroDepartment of Epidemiology and
Biostatistics
University of South Carolina, USA
-
Copyright # 2003 John Wiley & Sons Ltd, The Atrium, Southern
Gate, Chichester,West Sussex PO19 8SQ, England
Telephone (þ44) 1243 779777
Email (for orders and customer service enquiries):
cs-bookswiley.co.ukVisit our Home Page on www.wileyeurope.com or
www.wiley.com
All Rights Reserved. No part of this publication may be
reproduced, stored in a retrieval system ortransmitted in any form
or by any means, electronic, mechanical, photocopying,
recording,scanning or otherwise, except under the terms of the
Copyright, Designs and Patents Act 1988 orunder the terms of a
licence issued by the Copyright Licensing Agency Ltd, 90 Tottenham
CourtRoad, London W1T 4LP, UK, without the permission in writing of
the Publisher. Requests to thePublisher should be addressed to the
Permissions Department, John Wiley & Sons Ltd, The
Atrium,Southern Gate, Chichester, West Sussex PO19 8SQ, England, or
emailed to permreqwiley.co.uk, orfaxed to (þ44) 1243 770571.
This publication is designed to provide accurate and
authoritative information in regard to thesubject matter covered.
It is sold on the understanding that the Publisher is not engaged
in renderingprofessional services. If professional advice or other
expert assistance is required, the services of acompetent
professional should be sought.
Other Wiley Editorial Offices
John Wiley & Sons Inc., 111 River Street, Hoboken, NJ 07030,
USA
Jossey-Bass, 989 Market Street, San Francisco, CA 94103-1741,
USA
Wiley-VCH Verlag GmbH, Boschstr. 12, D-69469 Weinheim,
Germany
John Wiley & Sons Australia Ltd, 33 Park Road, Milton,
Queensland 4064, Australia
John Wiley & Sons (Asia) Pte Ltd, 2 Clementi Loop #02-01,
Jin Xing Distripark, Singapore 129809
John Wiley & Sons Canada Ltd, 22 Worcester Road, Etobicoke,
Ontario, Canada M9W 1L1
Library of Congress Cataloging-in-Publication Data
Lawson, Andrew (Andrew B.)Disease mapping with WinBUGS and MLwiN
/ Andrew B. Lawson, William J. Browne,Carmen L. Vidal Rodeiro.
p. cm. – (Statistics in practice)Includes bibliographical
references and index.ISBN 0-470-85604-1 (hbk. : alk. paper)1.
Medical geography. 2. Medical geography – Maps – Data
processing.
3. Epidemiology – Statistical methods. 4. Epidemiology – Data
processing. 5. Public healthsurveillance. I. Browne, William J.,
Ph.D. II. Vidal Rodeiro, Carmen L. III. Title. IV.Statistics in
practice (Chichester, England).
RA792.5.L388 2003615.4’2’0727–dc21 2003053782
British Library Cataloguing in Publication Data
A catalogue record for this book is available from the British
Library
ISBN 0–470–85604–1
Typeset in 10/12 pt by Kolam Information Services Pvt. Ltd,
Pondicherry, IndiaPrinted and bound in Great Britain by T J
International Ltd, Padstow, CornwallThis book is printed on
acid-free paper responsibly manufactured from sustainable forestry
in whichat least two trees are planted for each one used for paper
production.
http://www.wileyeurope.comhttp://www.wiley.com
-
Contents
Preface ix
Notation xi
0.1 Standard notation for multilevel modelling xi
0.2 Spatial multiple-membership models and the MMMC notation
xii
0.3 Standard notation for WinBUGS models xii
1 Disease mapping basics 1
1.1 Disease mapping and map reconstruction 2
1.2 Disease map restoration 3
2 Bayesian hierarchical modelling 17
2.1 Likelihood and posterior distributions 17
2.2 Hierarchical models 18
2.3 Posterior inference 19
2.4 Markov chain Monte Carlo methods 20
2.5 Metropolis and Metropolis–Hastings algorithms 21
2.6 Residuals and goodness of fit 26
3 Multilevel modelling 29
3.1 Continuous response models 30
3.2 Estimation procedures for multilevel models 35
3.3 Poisson response models 38
3.4 Incorporating spatial information 42
3.5 Discussion 43
4 WinBUGS basics 45
4.1 About WinBUGS 45
4.2 Start using WinBUGS 47
4.3 Specification of the model 50
4.4 Model fitting 59
4.5 Scripts 64
4.6 Checking convergence 65
v
-
4.7 Spatial modelling: GeoBUGS 67
4.8 Conclusions 72
5 MLwiN basics 75
5.1 About MLwiN 75
5.2 Getting started 77
5.3 Fitting statistical models 84
5.4 MCMC estimation in MLwiN 94
5.5 Spatial modelling 104
5.6 Conclusions 113
6 Relative risk estimation 115
6.1 Relative risk estimation using WinBUGS 115
6.2 Spatial prediction 137
6.3 An analysis of the Ohio dataset using MLwiN 139
7 Focused clustering: the analysis of
putative health hazards 155
7.1 Introduction 155
7.2 Study design 156
7.3 Problems of inference 158
7.4 Modelling the hazard exposure risk 160
7.5 Models for count data 164
7.6 Bayesian models 166
7.7 Focused clustering in WinBUGS 167
7.8 Focused clustering in MLwiN 190
8 Ecological analysis 197
8.1 Introduction 197
8.2 Statistical models 198
8.3 WinBUGS analyses of ecological datasets 199
8.4 MLwiN analyses of ecological datasets 219
9 Spatially-correlated survival analysis 235
9.1 Survival analysis in WinBUGS 235
9.2 Survival analysis in MLwiN 237
10 Epilogue 251
Appendix 1: WinBUGS code for focused
clustering models 253
A.1 Falkirk example 253
A.2 Ohio example 256
vi Contents
-
Appendix 2: S-Plus function for conversion
to GeoBUGS format 263
Bibliography 267
Index 275
Contents vii
-
Statistics in Practice
Human and Biological Sciences
Brown and Prescott – Applied Mixed Models in Medicine
Ellenberg, Fleming and DeMets – Data Monitoring in Clinical
Trials:
A Practical Perspective
Lawson, Browne and Vidal Rodeiro – Disease Mapping with WinBUGS
and
MLwiN
Marubini and Valsecchi – Analysing Survival Data from Clinical
Trials and
Observation Studies
Parmigiani – Modeling in Medical Decision Making: A Bayesian
Approach
Senn – Cross-over Trials in Clinical Research, Second
Edition
Senn – Statistical Issues in Drug Development
Whitehead – Design and Analysis of Sequential Clinical Trials,
Revised
Second Edition
Whitehead – Meta-analysis of Controlled Clinical Trials
Earth and Environmental Sciences
Buck, Cavanagh and Litton – Bayesian Approach to Intrepreting
Archaeological
Data
Glasbey and Horam – Image Analysis for the Biological
Sciences
Webster and Oliver – Geostatistics for Environmental
Scientists
Industry, Commerce and Finance
Aitken – Statistics and the Evaluation of Evidence for Forensic
Scientists
Lehtonen and Pahkinen – Practical Methods for Design and
Analysis of Complex
Surveys, Second Edition
Ohser andMücklich – Statistical Analysis of Microstructures in
Materials Science
-
Preface
The analysis of disease maps has seen considerable development
over the last
decade. This development has been reflected in a fast-increasing
literature and
has been matched by the development of software tools. The
intersecting areas
of spatial statistical methods development and geographical
information
systems (GIS) have both witnessed this growth. With increasing
public health
concerns about environmental risks and even bioterrorism, the
need for good
methods for analysing spatial health data is immediate. Two
major software
tools have now been developed, which allow the modelling of
spatially-refer-
enced small area health data. These tools, MLwiN and WinBUGS,
both provide
facilities for sophisticated modelling of realistically complex
health data. Win-
BUGS was developed to allow the application of a wide range of
hierarchical
Bayesian models, exploiting modern computational advances, in
particular
Gibbs sampling. MLwiN was developed to allow the fitting of
models to multi-
level data where a natural parameter hierarchy exists.
Originally, this was
implemented using iterative likelihood and quasi-likelihood
estimation methods.
However, the most recent versions of the package have
implemented Bayesian
computational methodology and now have many parallel
capabilities. Increas-
ingly both packages are being used by researchers and also now
there is a desire
to be able to apply such methodology in practical public health
applications. In
response to this need, the authors have attempted to provide an
introduction to
the methods and types of applications where such modelling is
feasible. We do
not claim to provide a comprehensive text on disease mapping and
have
confined our attention to the main application of these methods
to counted
data, where numbers of cases are recorded within small
areas.
This book is designed to be of interest to final-year
undergraduate and
graduate level statistics and biostatistics students but will
also be of relevance
to epidemiologists and public health workers both in higher
education and
beyond. The book provides in the introductory chapters (Chapters
1–5) general
background to disease mapping, Bayesian hierarchical modelling
and multilevel
modelling approaches, and basic introductions to the use of
WinBUGS and
MLwiN. The latter part of the book is focused on application
areas, and is
divided between relative risk estimation (Chapter 6), focused
clustering (Chapter
7), ecological analysis (Chapter 8), and finally spatial
survival analysis (Chapter
ix
-
9). Throughout the book we provide clear descriptions of the
model program-
ming execution and analysis of and interpretation of results. We
have adopted
the philosophy that we would attempt to demonstrate how MLwiN
and Win-
BUGS approach the same data example, but also have included
examples where
either one or the other packages have limitations. We cannot
necessarily hope
to provide definitive answers to how modelling is to be
approached in every
case. However, we would hope that we provide useful pointers to
the issues and
potential benefits of the approaches described. As both MLwiN
and WinBUGS
are evolving packages, it is to be expected that features
described here may vary
in the future. However, we have done our best to describe the
current or soon-
to-be current form of the packages which is relevant to the
potential audience
for this published work. All the material described here is
available in WinBUGS
1.4 (see Section 4.8.2 for download information and website
www.mrc-bsu.
cam.ac.uk/bugs), and in MLwiN (see section 5.6.1 and website
http://multileve-
l.ioe.ac.uk/index.html for more details). Most datasets used in
this book are
available to download (with associated WinBUGS code) from the
site http://
www.sph.sc.edu/alawson/.
We would like to acknowledge the help and contribution of a
number of
people during the development of this work. First, we would like
to acknowledge
the help of the MLwiN project team, in particular Jon Rasbash,
Harvey Gold-
stein, Amy Burch, Lisa Brennan, Fiona Steele and Min Yang. We
would like to
thank Allan Clark, Robin Puett, Lance Waller, Tom Richards,
James Hebert,
Alastair Leyland, Sudipto Banerjee, Robert McKeown, Ken
Kleinman, Peter
Rogerson, Dan Wartenburg and Martin Kulldorff for support and
encourage-
ment in the project. In addition, we would like to acknowledge
the data
availability afforded by the sophisticated online public access
GIS layer system
developed by, amongst others, Guang Zhao of the South Carolina
Department of
Health and Environmental Control. Finally, the continuing
support and encour-
agement of Sian Jones and Rob Calver at Wiley Europe must be
acknowledged
and is much appreciated.
Andrew Lawson (Columbia, SC, USA)
William Browne (Nottingham, UK)
Carmen Vidal Rodeiro (Columbia, SC, USA)
March 2003
x Preface
-
Notation
In complex random effects models there is often a myriad of
different ‘standard’
notations to represent a statistical model. This is generally
because the models
were first discovered by many different authors at roughly the
same time and
each author had their own particular notation and style.
0.1 STANDARD NOTATION FOR MULTILEVEL
MODELLING
In this book, in the multilevel modelling sections, as we will
be using the MLwiN
software package, we will use the notation used by this software
package.
If we consider a three-level nested Normal model, then the
standard multi-
level model will be written as
yijk ¼ X� þ vk þ ujk þ eijk, vk � N(0, �2v ), ujk � N(0,�2u ),
eijk � N(0, �2e )
Here the fixed effects are represented by �, X is a design
matrix, and the randomeffects at levels 1, 2 and 3 are represented
by e, u, and v respectively. Level
1 units are indexed i, level 2 units j and level 3 units k.
There is a rather
unfortunate notational clash as in disease mapping e is
typically used to repre-
sent the expected counts. However, the level 1 residuals
disappear from the
equation in the Poisson response multilevel model which
minimizes confusion.
A three-level Poisson response model is typically written in
MLwiN as
yijk � Poisson(�ijk),log (�ijk) ¼ log (eijk)þ X� þ vk þ ujk,
vk �N(0, �2v ), ujk � N(0,�2u ):(1)
In standard disease mapping � is often used rather than �, and
the eijk is oftenput on the right-hand side of the equation.
xi
-
0.2 SPATIAL MULTIPLE-MEMBERSHIP MODELS AND
THE MMMC NOTATION
The disadvantage of the standard multilevel notation is that it
relies on the
nested structure of the model. Browne et al. (2001) consider
more general
random effect structures including crossed random effects and
multiple-mem-
bership structures. Rather than give an index for each
classification (level in a
nested structure) they instead use mapping functions to define
the unit in the
classification that a particular observation belongs. For
example let us consider
the three-level Poisson model and assume that the levels are
counties within
regions within nations. Then in the notation of Browne et al.
(2001) we can
write Equation (1) as follows:
yi � Poisson(�i),log (�i) ¼ log (ei)þ X� þ u(3)nation [i] þ
u
(2)region[i],
u(3)nation[i] �N(0, �
2u(3)), u
(2)region[i] � N(0, �
2u(2)):
So here we define all terms with respect to the lowest
(observation) level which
is labelled i. The functions nation[i] and region[i] are mapping
functions that
return the nation and region respectively that observation i
belongs to. As the
random part of the model consists of a set of classifications
which need not now
be ordered in terms of nesting (and if the model contained
crossed effects could
not) we simply define each set of random effects with the letter
u but include a
superscript that gives the classification a number. We start
numbering from 2 as
1 is reserved for the observation level.
The spatial multiple-membership models that we will consider
later can be
easily written in this notation as follows:
yi � Poisson(�i),log (�i) ¼ log (ei)þ X� þ
X
j2neigh(i)w
(3)i,j u
(3)j þ u
(2)region[i],
u(3)j �N(0, �2u(3)), u
(2)region[i] � N(0, �
2u(2)):
Here we have a set of region effects indexed by 2 and a set of
neighbour effects
that are indexed by 3.
0.3 STANDARD NOTATION FOR WinBUGS MODELS
In hierarchical models for disease maps, the notation commonly
used is slightly
different from that used in multilevel models. The basic Poisson
likelihood model
is defined as
xii Notation
-
yi � Poisson(ei�i),
where ei is the expected count and �i is the relative risk in
the ith small area.Note that in the notation of multilevel models,
�i ¼ ei�i. It is also common to useli ¼ ei�i, and this form is used
in Chapter 7.
Modelling focuses on �i. Here we assume this notation for all
the standardanalysis within WinBUGS. In addition to region specific
notation we also
introduce space–time notation with a second subscript denoting
the time period:
yik � Poisson(eik�ik):
Here, k denotes the relevant time period and the expected count
and relative risk
are allowed to vary over time periods.
When random effects are introduced into models it is usual to
denote region-
specific uncorrelated heterogeneity as vi, and correlated
heterogeneity for the
same unit as ui. This differs slightly from the convention in
multilevel models.
In each section the relevant notation for that section is
introduced and it is
hoped that any differences between sections will not create
difficulties for the
reader.
Notation xiii
-
1
Disease Mapping Basics
The representation and analysis of maps of disease incidence
data is now
established as a basic tool in the analysis of regional public
health. One of the
earliest examples of disease mapping is the map of the addresses
of cholera
victims related to the locations of water supplies given by Snow
(1854). In that
case, the street addresses of victims were recorded and their
proximity to
putative pollution sources (water supply pumps) was
assessed.
The subject area of disease mapping has developed considerably
in recent
years. This growth in interest has led to a greater use of
geographical or spatial
statistical tools in the analysis of data both routinely
collected for public health
purposes and in the analysis of data found within ecological
studies of disease
relating to explanatory variables. The study of the geographical
distribution
of disease can have a variety of uses. The main areas of
application can
be conveniently broken down into the following classes: (1)
disease mapping,
(2) disease clustering, and (3) ecological analysis. In the
first class, usually the
object of the analysis is to provide (estimate) the true
relative risk of a disease of
interest across a geographical study area (map): a focus similar
to the processing
of pixel images to remove noise. Applications for such methods
lie in health
services resource allocation, and in disease atlas construction
(see, for example,
Pickle et al., 1999). The second class, that of disease
clustering, has particular
importance in public health surveillance, where it may be
important to be able
to assess whether a disease map is clustered and where the
clusters are located.
This may lead to examination of potential environmental hazards.
A particular
special case arises when a known location is thought to be a
potential pollution
hazard. The analysis of disease incidence around a putative
source of hazard
is a special case of cluster detection called focused
clustering. The third class,
that of ecological analysis, is of great relevance within
epidemiological research,
as its focus is the analysis of the geographical distribution of
disease in
relation to explanatory covariates, usually at an aggregated
spatial level.
Many issues relating to disease mapping are also found in this
area, in addition
to issues relating specifically to the incorporation of
covariates.
1
Disease Mapping with WinBUGS and MLwiN A. Lawson, W. Browne and
C. Vidal Rodeiro
# 2003 John Wiley & Sons, Ltd ISBN: 0-470-85604-1 (HB)
-
In this volume, we focus on the issues of modelling. While the
focus here is on
statistical methods and issues in disease mapping, it should be
noted that the
results of such statistical procedures are often represented
visually in mapped
form. Hence, some consideration must be given to the purely
cartographic
issues that affect the representation of geographical
information. The method
chosen to represent disease intensity on the map, be it colour
scheme or
symbolic representation, can dramatically affect the resulting
interpretation of
disease distribution. It is not the purpose of this review to
detail such cognitive
aspects of disease mapping, but the reader is directed to some
recent discussions
of these issues (MacEachren, 1995; Monmonier, 1996; Pickle and
Hermann,
1995; Walter, 1993).
1.1 DISEASE MAPPING AND MAP RECONSTRUCTION
To begin, we consider two situations which commonly arise in
studies of the
geographic distribution of disease. These situations are defined
by the form of
the mapped data which arises in such studies. First a study area
or window
is defined and within this area for a fixed period of time the
locations of cases
of a specified disease are recorded. These locations are usually
residential
addresses (street address or, at a higher spatial scale, zip
code (USA) or post
code unit (UK) ). When such addresses are known it is possible
to proceed
by direct analysis of the case locations. This is termed
case-event analysis.
Often this analysis requires the use of point process models and
associated
methodology. This form of analysis is reviewed in Lawson (2001,
Chapters 4
and 5) and elsewhere (see, for example, Elliott et al. (2000,
Chapter 6) ).
Due to the requirements of medical confidentiality, it is often
not possible
to obtain data at this level of resolution and so resort must be
made to the
analysis of counts of cases within small areas within the study
window. These
small areas are arbitrary regions usually defined for
administrative purposes,
such as census tracts, counties, municipalities, electoral wards
or health
district regions. Data of this type consist of counts of cases
within tracts and
the analysis of this data is termed tract count analysis. In
this volume we focus
exclusively on tract count analysis. An example of the analysis
of case-event
data with a Bernouilli model using WinBUGS is given in Congdon
(2003,
Chapter 7).
Essentially the count is an aggregation of all the cases within
the tract. By
aggregation, the individual case spatial references (locations)
are lost and
therefore any georeference of the count is related to the tract
‘location’. Often
this is represented by the tract centroid. In a chosen study
window there is
found to be m tracts. Denote the counts of disease within the m
tracts as
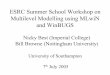
{yi}, i ¼ 1, . . . , m. Figure 1.1 displays a tract count
example.This example is of the 46 counties of South Carolina in
which were collected
the congenital abnormality death counts for the year 1990.
2 Disease mapping basics
-
0
7
1
5
11
5
16
0
17
4
00
1
1
71
3
0
0
8
2
13
7
0
8
0
3
2
41
110
1
2
3
3
8
6
143
11
6
0
1
5
Figure 1.1 South Carolina congenital abnormality deaths 1990 by
counties.
1.2 DISEASE MAP RESTORATION
1.2.1 Simple statistical representations
The representation of disease-incidence data can vary from
pictorial representa-
tion of counts within tracts, to the mapping of estimates from
complex models
purporting to describe the structure of the disease events. In
this section, we
describe the range of mapping methods from simple
representations to model-
based forms. The geographical incidence of disease has as its
fundamental unit
of observation, the address location of cases of disease. The
residential address
(or possibly the employment address) of cases of disease
contains important
information relating to the type of exposure to environmental
risks. Often,
however, the exact address locations of cases are not directly
available, and
one must use instead counts of disease in arbitrary
administrative regions, such
as census tracts or postal districts.
1.2.1.1 Crude representation of disease distribution
The simplest possible mapping form is the depiction of disease
rates at specific
sets of locations. For counts within tracts, this is a pictorial
representation of the
number of events in the tracts plotted at a suitable set of
locations (e.g., tract
centroids). The locations of case-events within a spatially
heterogeneous popu-
lation can display a small amount of information concerning the
overall pattern
of disease events within a window. However, any interpretation
of the structure
Disease map restoration 3
-
of these events is severely limited by the lack of information
concerning the
spatial distribution of the background population which might be
‘at risk’ from
the disease of concern and which gave rise to the cases of
disease. This popula-
tion also has a spatial distribution and failure to take account
of this spatial
variation severely limits the ability to interpret the resulting
case-event map. In
essence, areas of high density of ‘at risk’ population would
tend to yield high
incidence of case-events and so, without taking account of this
distribution,
areas of high disease intensity could be spuriously attributed
to excess disease
risk.
In the case of counts of cases of disease within tracts, similar
considerations
apply when crude count maps are constructed. Here, variation in
population
density also affects the spatial incidence of disease. It is
also important to consider
how a count of cases could be depicted in amapped
representation. Countswithin
tracts are totals of events from the whole tract region. If
tracts are irregular, then
a decision must be made to either ‘locate’ the count at some
tract location (e.g.
tract centroid, however defined) with suitable symbolization, or
to represent the
count as a fill colour or shade over the whole tract (choropleth
thematic map). In
the former case, the choice of location will affect
interpretation. In the latter case,
symbolization choice (shade and/or colour) could distort
interpretation also,
although an attempt to represent the whole tract may be
attractive.
In general, methods that attempt to incorporate the effect of
background ‘at
risk’ population (termed: at risk background) are to be
preferred. These are
discussed in the next section.
1.2.1.2 Standardized mortality/morbidity ratios and
standardization
To assess the status of an area with respect to disease
incidence, it is convenient
to attempt to first assess what disease incidence should be
locally ‘expected’ in
the tract area and then to compare the observed incidence with
the ‘expected’
incidence. This approach has been traditionally used for the
analysis of counts
within tracts. Traditionally, the ratio of observed to expected
counts within
tracts is called a Standardized Mortality/Morbidity Ratio (SMR)
and this ratio is
an estimate of relative risk within each tract (i.e., the ratio
describes the odds of
being in the disease group rather than the background group).
The justification
for the use of SMRs can be supported by the analysis of
likelihood models with
multiplicative expected risk (see, for example, Breslow and Day,
1987). In
Section 1.2.3.1, we explore further the connection between
likelihood models
and tract-based estimators of risk. Figure 1.2 displays the SMR
thematic map for
congenital abnormality deaths within South Carolina, USA, for
the year 1990
based on expected rates calculated from the South Carolina
1990–1998 state-
wide rate per 1000 births.
Define yi as the observed count of the case disease in the ith
tract, and ei as the
expected count within the same tract. Then the SMR is defined
as:
4 Disease mapping basics
-
Congenital abnormality deathsSMR 1990 using 8 year rate
1.51 to 4.1 (9)1.09 to 1.51 (9)0.78 to 1.09 (9)0.5 to 0.78 (9)0
to 0.5 (10)
Figure 1.2 South Carolina congenital abnormality deaths 1990:
SMRs.
b��i ¼ yiei: (1:1)
In this case it must be decided whether to express the b��i as
fill patterns in eachregion, or to locate the result at some
specified tract location, such as the
centroid. If it is decided that these measures should be
regarded as continuous
across regions then some further interpolation of b��i must be
made (see, forexample, Breslow and Day, 1987, pp. 198–9).
SMRs are commonly used in disease map presentation, but have
many
drawbacks. First, they are based on ratio estimators and hence
can yield large
changes in estimate with relatively small changes in expected
value. In the
extreme, when a (close to) zero expectation is found the SMR
will be very large
for any positive count. Also the zero SMRs do not distinguish
variation in
expected counts, and the SMR variance is proportional to 1=ei.
The SMR isessentially a saturated estimate of relative risk and
hence is not parsimonious.
1.2.2 Informal methods
To circumvent the problems associated with SMRs a variety of
methods have
been proposed. Some of these are relatively informal or
nonparametric and
others highly parametric. In the rest of this volume we will
concentrate on
the model-based relative risk estimation methods. However, it is
useful here to
present briefly some notes on alternative methods.
One approach to the improvement of relative risk estimation is
to employ
smoothing tools on SMRs to reduce the noise. These tools could
be based on
Disease map restoration 5
-
interpolation methods, or more commonly on nonparametric
smoothers such as
kernel regression (Nadaraya-Watson, local linear) (Bowman and
Azzalini,
1997), and partition methods (Ferreira et al., 2002). A variety
of exploratory
data analysis (EDA) methods have also been advocated (see, for
example,
Cressie, 1993). These methods usually require the estimation of
a smoothing
constant which describes the overall behaviour of the relative
risk surface. Some
local methods are also available. Generalized additive models
have also been
proposed and these have the advantage of allowing the
incorporation of covari-
ates (see, for example, Kelsall and Diggle, 1998).
1.2.3 Basic models
When more substantive hypotheses and/or greater amounts of prior
informa-
tion are available concerning the problem, then it may be
advantageous to
consider a model-based approach to disease map construction.
Model-based
approaches can also be used in an exploratory setting, and if
sufficiently general
models are employed then this can lead to better focusing of
subsequent
hypothesis generation. In what follows, we consider first
likelihood models for
case event data and then discuss the inclusion of extra
information in the form
of random effects.
1.2.3.1 Likelihood models
Usually the basic model for case-event data is derived from the
following
assumptions:
(1) Individuals within the study population behave independently
with respect
to disease propensity, after allowance is made for observed or
unobserved
confounding variables.
(2) The underlying at risk background intensity has a continuous
spatial
distribution, within a specified boundary.
(3) The case-events are unique, in that they occur as single
spatially separate
events.
Assumption (1) above allows the events to be modelled via a
likelihood
approach, which is valid conditional on the outcomes of
confounder variables.
Further, assumption (2), if valid, allows the likelihood to be
constructed with
a background continuous modulating intensity function
representing the ‘at
risk’ background. The uniqueness of case-event locations is a
requirement of
point process theory (the property called orderliness: see, for
example, Daley and
Vere-Jones, 1988), which allows the application of
Poisson-process models in
this analysis. Assumption (1) is generally valid for
non-infectious diseases. It
6 Disease mapping basics
-
may also be valid for infectious diseases if the information
about current
infectives were known at given time points. Assumption (2) will
be valid at
appropriate scales of analysis. It may not hold when large areas
of a study
window include zones of zero population (e.g.
harbours/industrial zones). Often
models can be restricted to exclude these areas however.
Assumption (3) will
usually hold for relatively rare diseases but may be violated
when households
have multiple cases and these occur at coincident locations.
This may not be
important at more aggregate scales, but could be important at a
fine spatial
scale. Remedies for such non-orderliness are the use of
de-clustering algo-
rithms (which perturb the locations by small amounts), or
analysis at a higher
aggregation level. Note that it is also possible to use a
conventional case-control
approach to this problem (Diggle et al., 2000).
In the case of observed counts of disease within tracts, the
Poisson-process
assumptions given above mean that the counts are Poisson
distributed with, for
each tract, a different expectation. Often at this point a
simplifying assumption is
made where the ith tract count expectation is regarded as being
a function of a
parameter within a model hierarchy, without considering the
spatial continuity
of the intensity. This assumption leads to considerable
simplifications and the
distribution of the tract counts is often assumed to be
yi � Poisson(ei�i),
where �i is assumed to be a constant relative risk parameter. In
this definitionthe expected value of the count is a multiplicative
function of the expected
count/rate (ei) and a relative risk. This is the classic model
assumed in many
disease mapping studies. The log-likelihood associated with this
model is, bar a
constant, given by:
l ¼Xmi¼1
yi ln (ei�i)�Xmi¼1
ei�i:
Note that by differentiation the saturated maximum likelihood
estimator of �i isjust yi=ei, the SMR.
This model makes a number of assumptions. First it is assumed
that any
excess risk in a tract will be expressed beyond that described
by ei. For example,
the expected rate (ei) can be estimated in a variety of ways.
Often external
standardization is used, where known supra-regional rates for
different age �sex groups are applied to the local population in
each tract. The use of external
standardization alone to estimate the expected counts/rates
within tracts may
provide a different map from that provided by a combination of
external stand-
ardization and measures of tract-specific deprivation (e.g.
deprivation indices
(Carstairs, 1981) ). If any confounding variables are available
and can be
included within the estimate of the at risk background, then
these should be
Disease map restoration 7
-
considered for inclusion. Examples of confounding variables
could be found
from national census data, particularly relating to
socioeconomic measures.
These measures are often defined as ‘deprivation’ indicators, or
could relate to
lifestyle choices. For example, the local rate of car ownership
or percentage
unemployed within a census tract or other small area, could
provide a surrogate
measure for increased risk, due to correlations between these
variables and poor
housing, smoking lifestyles, and ill-health. Hence, if it is
possible to include such
variables, then any resulting map will display a close
representation of the ‘true’
underlying risk surface. When it is not possible to include such
variables, it is
sometimes possible to adapt a mapping method to include
covariates of this type
within regression setting.
1.2.3.2 Fixed effects
Usually the focus of attention when more sophisticated models
are applied in
disease mapping is the relative risk. Hence, all the models we
will examine in
this volume will be models for the {�i}. One simple model for
the relative riskswould be to suppose that there could be a spatial
trend or long-range variation
over the study area. To do this we can construct a model which
is a function of
the spatial coordinates of the tract centroids: {x1i, x2i}
representing eastings and
northings, say. Simple forms of spatial trend can be modelled by
using the
centroid coordinates or functions of the coordinates as
covariates and assuming
a regression-type model. As the relative risks must be positive
it is usual to
model the logarithm of the relative risk as a linear function.
Hence, in this case
we could have:
�i ¼ exp{�0 þ �1x1i þ �2x2i}: (1:2)
This model includes a constant rate (exp {�0}) which captures
the overall rateacross the whole study region, and two linear
parameters: �1,�2. This modeldescribes a planar trend across the
study region, and can be easily extended to
include higher-order trend surfaces by adding power functions of
the coordinates.
Here we have used centroid locations as covariates, and indeed
this model can be
generalized simplywhenyouobserveother covariatesmeasuredwithin
the tracts.
For example it may be possible to include deprivation scores for
each tract or
census variables such as percentage unemployed or percentage car
ownership. In
general, assume that the intercept (constant rate) term is
defined for a variable x0iwhich is 1 for each tract. Hence we can
specify the model compactly as
�i ¼ exp{xib},
where x is a m� p matrix consisting of p� 1 covariates, b is a
p� 1 parametervector and xi denotes the ith observation row of
x.
8 Disease mapping basics
-
This type of fixed effect model can be fitted in conventional
statistical pack-
ages which allow Poisson regression or log-linear modelling. The
glm function
in R or S-Plus with a log link and log offset of the {ei} can be
used, for example.
1.2.3.3 Random effects
In the sections above some simple approaches to mapping counts
within tracts
have been described. These methods assume that once all known
and observ-
able confounding variables are included then the resulting map
will be clean of
all artefacts and hence depicts the true excess risk surface.
However, it is often
the case that unobserved effects could be thought to exist
within the observed
data and that these effects should also be included within the
analysis. These
effects are often termed random effects, and their analysis has
provided a large
literature both in statistical methodology and in
epidemiological applications
(see, for example, Manton et al., 1981; Tsutakawa, 1988; Breslow
and Clayton,
1993; Clayton, 1991; Best and Wakefield, 1999; Lawson, 2001;
Richardson,
2003). Within the literature on disease mapping, there has been
a considerable
growth in recent years in modelling random effects of various
kinds. In the
mapping context, a random effect could take a variety of forms.
In its simplest
form, a random effect is an extra quantity of variation (or
variance component)
which is estimable within the map and which can be ascribed a
defined
probabilistic structure. This component can affect individuals
or can be associ-
ated with tracts or covariates. For example, individuals vary in
susceptibility to
disease and hence individuals who become cases could have a
random com-
ponent relating to different susceptibility. This is sometimes
known as frailty.
Another example is the interpolation of a spatial covariable to
the locations of
case events or tract centroids. In that case, some error will be
included in the
interpolation process, and could be included within the
resulting analysis of
case or count events. Also, the locations of case-events might
not be precisely
known or subject to some random shift, which may be related to
uncertain
residential exposure. Finally, within any predefined spatial
unit, such as tracts
or regions, it may be expected that there could be components of
variation
attributable to these different spatial units. These components
could have
different forms depending on the degree of prior knowledge
concerning the
nature of this extra variation. For example, when observed
counts, thought to
be governed by a Poisson distribution, display greater variation
than expected
(i.e. variance> mean), it is sometimes described as
overdispersion. This over-dispersion can occur for various reasons.
Often it arises when clustering occurs
in the counts at a particular scale. It can also occur when
considerable numbers
of cells have zero counts (sparseness), which can arise when
rare diseases are
mapped. In spatial applications, it is important furthermore to
distinguish two
basic forms of extra variation. First, as in the aspatial case,
a form of independ-
ent and spatially uncorrelated extra variation can be assumed.
This is often
Disease map restoration 9
-
called uncorrelated heterogeneity (see, for example, Besag et
al., 1991). Another
form of random effect is that which arises from a model where it
is thought that
the spatial unit (such as case-events, tracts or regions) is
correlated with neigh-
bouring spatial units. This is often termed correlated
heterogeneity. Essentially, this
form of extra variation implies that there exists spatial
autocorrelation between
spatial units (see, for example, Cliff and Ord (1981) for an
accessible introduction
to spatial autocorrelation). This autocorrelation could arise
for a variety of
reasons. First, the disease of concern could be naturally
clustered in its spatial
distribution at the scale of observation. Many infectious
diseases display such
spatial clustering, and a number of apparently non-infectious
diseases also cluster
(see, for example, Cuzick and Hills, 1991; Glick, 1979). Second,
autocorrelation
can be induced in spatial disease patterns by the existence of
unobserved environ-
mental or frailty effects. Hence the extra variation observed in
any application
could arise from confounding variables that have not been
included in the
analysis. In disease mapping examples, this could easily arise
when simple
mapping methods are used on SMRs with just basic age–sex
standardization.
In the discussion above on heterogeneity, it is assumed that a
global measure
of heterogeneity applies to a mapped pattern. That is, any extra
variation in
the pattern can be captured by including a general heterogeneity
term in the
mapping model. However, often spatially-specific heterogeneity
may arise
where it is important to consider local effects as well as, or
instead of, general
heterogeneity. To differentiate these two approaches, we use the
term specific
and nonspecific heterogeneity. Specific heterogeneity implies
that spatial loca-
tions are to be modelled locally; for example, clusters of
disease are to be
detected on the map. In contrast, ‘nonspecific’ describes a
global approach to
such modelling, which does not address the question of the
location of effects. In
this definition, it is tacitly assumed that the locations of
clusters of disease can be
regarded as random effects themselves. Hence, there are strong
parallels be-
tween image processing tasks and the tasks of disease
mapping.
Random effects can take a variety of forms and suitable methods
must be
employed to provide correctly estimated maps under models
including these
effects. In this section, we discuss simple approaches to this
problem from a
frequentist, multilevel and Bayesian viewpoint.
A frequentist approach. In what follows, we use the term
‘frequentist’ to
describe methods that seek to estimate parameters within a
hierarchical model
structure. The methods do assume that the random effects have
mixing (or prior)
distributions. For example a common assumption made when
examining tract
counts is that yi � Poisson(ei�i) independently, and that �i �
Gamma(�,�). Thislatter distribution is often assumed for the
Poisson relative risk parameter and
provides for a measure of overdispersion relative to the Poisson
distribution
itself, depending on the �,� values used. The joint distribution
is now given bythe product of a Poisson likelihood and a gamma
distribution. At this stage a
choice must be made concerning how the random intensities are to
be estimated
or otherwise handled. One approach to this problem is to average
over the
10 Disease mapping basics
-
values of �i to yield what is often called the marginal
likelihood. Having averagedover this density, it is then possible
to apply standard methods such as max-
imum likelihood. This is usually known as marginal maximum
likelihood (see,
for example, Bock and Aitkin, 1981; Aitkin, 1996b). In this
approach, the
parameters of the gamma distribution are estimated from the
integrated likeli-
hood. A further development of this approach is to replace the
gamma density
with a finite mixture. This approach is essentially
nonparametric and does not
require the complete specification of the parameter distribution
(see, for
example, Aitkin, 1996a).
Although the example specified here concerns tract counts, the
method
described above can equally be applied to case-event data, by
inclusion of a
random component in the intensity specification.
A Bayesian approach. It is natural to consider modelling random
effects
within a Bayesian framework. First, random effects naturally
have prior distri-
butions and the joint density discussed above is proportional to
the posterior
distribution for the parameters of interest. Hence, the
development of full Bayes
and empirical Bayes (posterior approximation) methods has
progressed natur-
ally in the field of disease mapping. The prior distribution(s)
for the (u, say)parameters in the intensity specification ei�i,
have hyperparameters (in thePoisson–gamma example above, these were
�,�). These hyperparameters canalso have hyperprior distributions.
The distributions chosen for these param-
eters depend on the application. In the full Bayesian approach,
inference is
based on the posterior distribution of u given the data.
However, as in thefrequentist approach above, it is possible to
adopt an intermediate approach
where the posterior distribution is approximated in some way,
and subsequent
inference may be made via ‘frequentist-style’ estimation of
parameters or by
computing the approximated posterior distribution. In the
tract-count example,
approximation via intermediate prior-parameter estimation would
involve the
estimation of � and �, followed by inference on the estimated
posterior distribu-tion (see, for example, Carlin and Louis, 1996,
pp. 67–8).
For count data, a number of examples exist where independent
Poisson
distributed counts (with constant within-tract rate) are
associated with prior
distributions of a variety of complexity. The earliest examples
of such a Bayesian
mapping approach can be found in Manton et al. (1981) and
Tsutakawa
(1988). Also, Clayton and Kaldor (1987) developed a Bayesian
analysis of
a Poisson likelihood model where yi has expectation ei�i, and
found thatwith a prior distribution given by �i � Gamma(�,�), the
Bayes estimate of �i isthe posterior expectation:
yi þ �ei þ �
: (1:3)
Hence one could map directly these Bayes estimates. Now, the
distribution of �iconditional on yi is Gamma(yi þ �, ei þ �) and a
Bayesian approach would
Disease map restoration 11
-
South Carolina empirical Bayes mean RRestimates congenital
abnormality deaths 1990
1.51 to 3.96 (8)1.09 to 1.51 (9)0.78 to 1.09 (10)0.51 to 0.78
(8)0.01 to 0.51 (11)
Figure 1.3 Empirical Bayes mean relative risk (RR)
estimates.
require summarization of �i from this posterior distribution. In
practice, this isoften obtained by generation of realizations from
this posterior and then the
summarizations are empirical (e.g.MarkovChainMonteCarlo
(MCMC)methods).
Figure 1.3 displays the empirical Bayes estimates under the
Poisson–gamma
model with � and � estimated as in Clayton and Kaldor. Note that
in contrast tothe SMR map (Figure 1.2), Figure 1.3 presents a
smoother relative risk surface.
Other approaches and variants in the analysis of simple mapping
models have
been proposed by Tsutakawa (1988), Marshall (1991) and Devine
and Louis
(1994). In the next section, more sophisticated models for the
prior structure of
the parameters of the map are discussed.
1.2.4 Advanced Bayesian models
Many of the models discussed above can be extended to include
the specification
of prior distributions for parameters and hence can be examined
via Bayesian
methods. In general, we distinguish here between empirical Bayes
methods and
full Bayes methods, on the basis that any method which seeks to
approximate
the posterior distribution is regarded as empirical Bayes
(Bernardo and Smith,
1994). All other methods are regarded as full Bayes. This latter
category
includes maximum a posteriori estimation, estimation of
posterior functionals,
as well as posterior sampling.
12 Disease mapping basics
-
1.2.4.1 Empirical Bayes methods
The methods encompassed under the definition above are
wide-ranging, and
here we will only discuss a subset of relevant methods. The
first method
considered by the earliest workers was the evaluation of
simplified (constrained)
posterior distributions. Manton et al. (1981) used a direct
maximization of a
constrained posterior distribution, Tsutakawa (1988) used
integral approxima-
tions for posterior expectations, while Marshall (1991) used a
method of
moments estimator to derive shrinkage estimates. Devine and
Louis (1994)
further extended this method by constraining the mean and
variance of the
collection of estimates to equal the posterior first and second
moments.
The second type of method which has been considered in the
context of
disease mapping is the use of likelihood approximations. Clayton
and Kaldor
(1987) first suggested employing a quadratic normal
approximation to a Pois-
son likelihood, with gamma prior distribution for the intensity
parameter of the
Poisson distribution and a spatial correlation prior. Extensions
to this approach
lead to simple generalized least squares (GLS) estimators for a
range of likeli-
hoods (Lawson, 1994; 1997).
A third type is the Laplace asymptotic integral approximation,
which has
been applied by Breslow and Clayton (1993) to a generalized
linear modelling
framework in a disease mapping example. This integral
approximation method
allows the estimation of posterior moments and normalizing
integrals (see, for
example, Bernardo and Smith, 1994, pp. 340–4). A further, but
different,
integral approximation method is where the posterior
distribution is integrated
across the parameter space: that is, the nuisance parameters are
‘integrated out’
of the model. In that case the method of nonparametric maximum
likelihood
(NPML) can be employed (Bock and Aitkin, 1981; Aitkin, 1996b;
Clayton and
Kaldor, 1987). Another possibility is to employ Linear Bayes
methods (Marshall,
1991).
1.2.4.2 Full Bayes methods
Full posterior inference for Bayesian models has now become
available, largely
because of the increased use of MCMC methods of posterior
sampling. The first
full sampler reported for a disease mapping example was a Gibbs
sampler
applied to a general model for intrinsic autoregression and
uncorrelated hetero-
geneity by Besag et al. (1991). Subsequently, Clayton and
Bernardinelli (1992),
Breslow and Clayton (1993) and Bernardinelli et al. (1995) have
adapted this
approach to mapping, ecological analysis and space–time
problems.
This has been facilitated by the availability of general Gibbs
sampling pack-
ages such as BEAM and BUGS (GeoBUGS and WinBUGS). Such Gibbs
sampling
methods can be applied to putative source problems as well as
mapping/eco-
logical studies. Alternative, and more general, posterior
sampling methods, such
Disease map restoration 13
-
as the Metropolis–Hastings algorithm, are currently not
separately available in
a packaged form, although these methods can accommodate
considerable
variation in model specification. WinBUGS does provide such
estimators when
non-convex posterior distributions are encountered.
Metropolis–Hastings algo-
rithms have been applied in comparison to approximate maximum a
posteriori
(MAP) estimation by Lawson et al. (1996) and Diggle et al.
(1998); hybrid
Gibbs–Metropolis samplers have been applied to space–time
problems by Waller
et al. (1997). In addition, diagnostic methods for Bayesian MCMC
sample output
have been discussed for disease mapping examples by Zia et al.
(1997). Devel-
opments in this area have been reviewed recently (Lawson et al.,
1999; Elliott
et al., 2000; Lawson, 2001).
1.2.5 Multilevel modelling approaches
An alternative to the above specification can be considered
where a log-linear
form is specified:
�i ¼ exp{�0 þ vi},
where the random term has a zero mean Gaussian distribution,
i.e. vi � N(0,�2v )and �2v is the variance of the random effects
v.
This model may be rewritten (in terms of counts rather than
rates) as
yi � Poisson(�i), log(�i) ¼ log(ei)þ �0 þ vi:
Here �i ¼ ei�i and the log(ei) are treated as known ‘offset’
terms.Generally, multilevel models (see, for example, Goldstein,
1995) are fitted
to data that possess levels of clustering in their structure. In
disease mapping
and geographical applications in general such levels would be
different levels of
geographical aggregation, for example, census tracts nested
within counties
nested within countries. For each level of geography we could
then fit normally
distributed random effects so for example if we had data on
census tracts nested
within counties we could fit
yij � Poisson(�ij), log(�ij) ¼ log(eij)þ �0 þ vj þ uij,
where both the county and tract random effects have Gaussian
distributions, i.e.
vj � N(0, �2v ) and uij � N(0,�2u ).Poisson response multilevel
models can be fitted using either frequentist or
Bayesian approaches. Frequentist approaches generally involve
some approxi-
mations, for example the software package MLwiN (Rasbash et al.,
2000) uses
quasi-likelihood methods that involve Taylor series
approximations (Goldstein,
1991; Goldstein and Rasbash, 1996) to transform the problem so
that it can be
14 Disease mapping basics