Embed Size (px)
Citation preview

Q1 2012 Update
Disease State Primer: Type II Diabetes, Non-Insulins

Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on Type II Diabetes?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is Type II Diabetes?
• Presentation, diagnosis, classification
• Epidemiology by geography and patient segment
• Current care paradigm and clinical evidence
• Emerging care paradigm
11
• 12
• 13
• 14
• 15 – 21
• 22
III. Clinical Development Pipeline • Disease mechanism overview
• Clinical development pipeline mapping
• DPP-IV Inhibitors
• GLP-1 Agonists
• SGLT2 Inhibitors
• PPAR Modulators
• SIRT-1 Activators
• Glucokinase Activators
• NF-kB Inhibitors
24
• 25
• 26 – 28
• 29 - 30
• 31 - 34
• 35 - 36
• 37 – 38
• 39
• 40 - 41
• 42
IV. Commercial Landscape • Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
44
• 45 – 49
• 50
• 51 – 53
• 54 – 56
V. Appendix • Table of Acronyms
• Lumleian Team
• 58 – 59
• 60 - 61

Notes: 1These are a representative sub-set of the publicly available data sources
To ensure real-time knowledge, across disease states, our team of 30+ clinicians and Ph.D.
scientists maintain a comprehensive knowledge management platform, leveraging novel data
mining technology and proprietary analytics.
Data Mining
and Analytics
• Company presentations
• Earnings announcements
• Equity research coverage
• Investor relations transcripts
• Clinical trials
• Conference presentations
• Gene ontology
• Industry pipeline databases
• NIH grants
• Scientific literature & citations
• Business development transactions
• Venture capital investments
• Disease profiles
• Industry publications
• Sales and Rx data
• Treatment algorithms
• Advisory committee transcripts
• FDA and EMA filings
Scientific
& Clinical:
Financial:
Academic
Tech Transfer:
Competitive
Landscape:
• Early stage technologies
• Intellectual property filings
Business
Development:
Regulatory:
• Leverage data mining
technology to access
novel data sources
• Standardize, collate,
and link data sources
• Execute Lumleian’s
proprietary analytical
models
Universe of Public
Information1
• 30+ clinicians and
Ph.D. scientists
- Focused by area
of expertise
• 5 Ph.D. economists
and statisticians
Expert Validation
and Decision Support
4

Our efficient platform and our expertise based teams enable us to both deliver the highest
quality product and tailor our offer, to specific client needs: Either custom decision support or
more standardized research and analytics, e.g. disease state primers.
Decision
Support
• Clinical strategy
• Portfolio optimization
- Pre-Clinical
- Clinical
• Transaction support
- In licensing
- Out licensing Disease
State Primers
Proprietary
Analytics
• Asset valuation
• Epidemiologic forecasts
• Industry benchmarks
- Commercial
- Clinical Development
• Patient segment
valuations
• Promotional
response models
- Healthcare professional
- Direct to consumer
• Royalty monetization
Functional
Drill Downs
• Real-time clinical
data
- Trial strategies
- Results
• In licensing
assessments
- Pre-clinical
- Clinical
• Preliminary
due dilligence
- Scientific
- Clinical
- Commercial
• Disease overview
and care paradigm
• Clinical development
pipeline
• Commercial
landscape Customized
Standardized
5

What information is included in a disease state primer?
• Lumleian’s objective and fact based perspective on the relative attractiveness of investing in a given disease state • Disease overview and care paradigm
- Etiology, Diagnosis and patient segmentation, Global epidemiology, Treatment algorithm, Clinical evidence, Emerging care paradigm • Clinical Development Pipeline
- Validated industry pipeline for all assets in clinical development, Select mechanism of action profiles, trial designs and evidence • Commercial landscape
- Global, US, EU, Japan market and brand revenue, Pipeline forecasts, US growth decomposition, Promotional spend and messaging
What disease states are planned for 2012? • Autoimmune: Inflammatory Bowel Disease, Lupus, Multiple Sclerosis, Psoriasis, Rheumatoid Arthritis • Cardiovascular: Hyperlipidemia • Central Nervous System: Alzheimer’s Disease, Depression, Pain, Schizophrenia • Endocrine: Type II Diabetes, Obesity • Infectious Disease: Gram Negative Bacteria, Hepatitis C Virus • Oncology: Breast, Colorectal, Leukemia(s), Lung, Lymphoma(s), Melanoma, Ovarian, Pancreatic, Prostate • Pulmonary: Chronic Obstructive Pulmonary Disease, Idiopathic Pulmonary Fibrosis
Are disease state primers real-time, based on the latest validated scientific, clinical, and commercial data? • Quarterly primers are validated by our team: 30+ clinicians and Ph.D. scientists, 5 Ph.D. economists and statisticians • Primers are available at the end of quarter, incorporating new commercial and clinical data from the previous quarter
- Particulary dynaimc disease states are updated around key medical conferences, e.g. HCV post EASL in April and post AASLD in November
Do we create specific disease state primers and provide more in-depth functional information? • Yes, we plan to add disease states throughout ’12, per client interest • Yes, we are developing deep drills by function, e.g. Discovery, Clinical development, Business development, Commercial
Why did we create our disease state primers? • We were frustrated by having to repeatedly validate, standardize, and collate pipeline and commercial data • Portfolio optimization requires a standard framework to compare “apples to apples” investment decisions across disease states • Our primers began as a training tool; We require every decision scientist create one from scratch before supporting clients
What is a Lumleian’s disease state primer?
6

Disease
Overview and
Care Paradigm
• Type II Diabetes is a chronic, multifactorial condition, with a number of serious comorbidities, including hypertension, dyslipidemia
and hyperglycemia; Type II Diabetes accounts for >90% of the total diabetes patient population
• Type II Diabetes necessitates a wide variety of treatments to adequately control the core hyperglycemic condition and the host of
co-morbidities and complications - Many therapeutic options are available for Type II Diabetes, including three key classes considered first and second line treatments
(Biguanides, Sulfonylureas, Glitazones)
- Subsequently, four classes of anti-diabetic agents are commonly used in third line prior to Insulin (DPP-IV Inhibitors, GLP-1 Agonists, α-
Glucosidase Inhibitors, and Glinides), although use earlier in the paradigm is growing
- DPP-IV fixed dose combinations have also become an important treatment option and are providing branded agents with a foothold in
earlier lines of treatment
Clinical
Development
Pipeline
• Lumleian validated 78 assets in clinical development, the majority of which have MoAs similar to currently marketed agents - DPP-IVs, GLPI-1s (as mono therapy and in combination with Long Acting Insulin), and PPARs are the most common mechanisms in the clinic,
but we believe pipeline assets will likely offer only incremental “clinical” benefit over marketed products
- That said, new formulations will likely provide significant patient benefit, e.g. once weekly GLP-1 Agonists (e.g. Bydureon, Dulaglutide, and
Syncria) and combination DPP-IVs and statins (e.g. MK-0431E) which offer a single co-pay and likely improved real-world control/compliance
• Although novel approaches to treat Type II Diabetes are in clinical development, limited knowledge exists about their side effects and
efficacy attributes over recently launched agents - Foremost, post Dapagliflozin’s complete response letter in January, are the follow on SGLT2 Inhibitors (Empagliflozin, Canagliflozin) and the
first SGLT1//2 dual inhibitor (LX4211)
• Avandia related safety concerns, leading to changes in trial design to evaluate impact on macro-vascular events, has resulted in longer,
larger, and more costly clinical trials and post-marketing requirements
• Substantial need exists for agents able to provide additional benefits, including weight loss, cardio-protection, reduced micro-vascular
complications, and durability; These agents will need clean profiles as has been made clear by recent FDA decisions, e.g. Galvus,
Bydureon, Dapagliflozin
Commercial
Landscape
• Global ‘11 brand revenue for non-Insulin drugs was ~$13.9B and is forecast to grow by ~3.1% annually through ‘15 driven by strong
market growth outside of the United States and new uptake globally, including follow on DPP-IV Inhibitors, once weekly GLP-1 Agonists
and potentially follow on SGLT2 Inhibitors, e.g. Empagliflozin and Canagliflozin - Cost pressure will continue to drive generic (Biguanides and Sulfonylureas) use in the future, reinforcing the need for differentiation; This
will be felt most acutely in the US with the Actos LoE in 08/12
- DPP-IV Inhibitors (fixed dose combinations) will gain share significantly in the US given the recent label change to Actos (bladder cancer
warning), the reduction in DTP advertising associated with Actos LoE (08/12), and Dapagliflozin’s recent FDA complete response letter
- GLP-1 Agonists will also gain share, and the approval of the first once weekly formulation marketed by a large pharma (e.g. Syncria and
Dulaglutide) may be a game changer, particularly with an indication for use in combination with Long Acting Insulin
Source: Lumleian perspective
Executive Summary: Type II Diabetes falls at the intersection of many conditions, and is
associated with a number of serious co-morbidities; Substantial need exists for agents able to
provide additional benefits, including weight loss and cardio-protection.
• The global
7

Key
Questions
• Commercial Opportunity - How will late-stage pipeline agents with established mechanisms be able to achieve clinical and commercial differentiation in
a crowded market, particularly with payors and patients? Will patients convenience continue to be a key driver of market uptake?
- What will be the uptake in the US of the first once weekly GLP-1 Agonist, and how will it compete with the DDP-IV inhibitors,
given superior HbA1c control, safety concerns, and more convenient formulation?
- How will loss of patent exclusivity for key branded agents, e.g. Actos, impact the opportunity and entry point in the treatment
paradigm for future innovative approaches? What will be the positive spill over impact on DPP-IV Inhibitors?
• Clinical Development and Regulatory Risks - How will the global efficacy and safety requirements for novel therapies change? What will be the requirements for demonstrating outcomes
benefits and a favorable safety profile?
- What additional challenges exist that could pose trial and regulatory risks for sponsors looking to develop novel agents in this space?
Lumleian’s
Perspective
• Commercial Opportunity: The Type II Diabetes market represents an attractive long-term opportunity for companies willing
to dedicate resources to satisfy regulatory requirements and compete in a crowded market increasingly driven by patients and payors - The Type II Diabetes market will continue to grow, particularly in the mid-to-long-term, given the likelihood that large pipelines will support
future innovation; In the near term growth will be driven largely outside of the United States
- In the US significant opportunity exists for the DDP-IVs to gain share absent Actos marketing post LoE; Further recent Actos safety concerns
(e.g. bladder cancer) put payors in check and near-term we see the US as highly attractive for Januvia, Onglyza and Tradjenta • United States ‘11 brand revenue was ~$8.0B and is forecast to be flat in ’12 and decline in ’13 due to Actos LoE; Thereafter the market is forecast
to grow by an ~5.8% CAGR driven by the uptake of marketed and pipeline DPP-IV Inhibitors and GLP-1 Agonists
• We posit this uptake (consensus Wall Street estimates) is understated and believe DPP-IV share gains will be more aggressive given substantial
marketing investment, Actos LoE and safety concerns, and Dapagliflozin’s complete response letter
- Guidelines will continue to influence payer coverage, enabling entry of new premium-priced agents able to drive guideline
acceptance through clinically meaningful differentiation
- Payers are increasingly looking for relevant cost-benefit metrics (e.g., long-term mortality) over surrogate markers (e.g. HbA1c), placing a
premium on clinical outcomes data from trials
• Clinical Development and Regulatory Risk: FDA will necessitate long-term safety requirements and strong clinical trial design - Inclusion of more high-risk and better-controlled patients with lower baseline HbA1c levels will also make it more challenging to
demonstrate significant benefits for novel agents
- The majority of future market growth in 2020 and beyond will be dependent upon successful development of novel classes able to achieve
significant differentiation beyond HbA1c with clean safety profiles
- Leaders in Type II Diabetes need to pursue multiple clinical development programs, including established and innovative mechanisms, to
ensure continued presence and significant future market share; We see the market as particularly attractive for entrenched players
What are the key questions for 2012?
8

0
1
2
3
4
5
Level of Unmet Need Likelihood of Technical Success Regulatory Impetus
Source: Lumleian perspective
Type II Diabetes may offer significant returns for a company willing to make multiple high-risk/reward
investments – given generic availability, the regulatory environment, and need to invest heavily in
clinical development and marketing; We see it as particularly attractive for entrenched players to
invest in marketing and Phase IV studies; Strong regulatory capabilities are a requisite.
Average
Type II Diabetes: Relative Attractiveness of Greenfield Investment in Late Stage Clinical Development
High
Low
Type II
Diabetes
Required
Investment
Phase III Investment
• ~3,000 patients in 2 trials
• 3-5 years duration
• Show CV events including
CV mortality
Commercial Spend
• In July ’10 the average
brand spent ~$20 M a
month on promotion - Healthcare professional
(86% of spend)
- Direct to consumer
(14% of spend)
• DTC investment will likely
be important to educate
patients on HbA1c control,
e.g. once weekly GLP-1s
Phase IV Investment
• Current and future trials
will need to show CV
events and mortality - Trial and regulatory costs
could exceed $500 M for
a single asset
Level of
Unmet Need
Clinical Unmet Need
• High, focused on targeting
weight loss, specific
physiology, durability, and
greater standalone
efficacy
Global Epidemiology
• ~292 M prevalence ‘10
• ~2.1% CAGR ‘10-’15
Disease Burden
• Economic cost of $150-
$200B annually (US)
• Type II Diabetes is a major
cause of mortality and
results in 240,000 deaths
(US)
Significant Co-morbidities
• Type II Diabetes falls at
the intersection of many
conditions
Commercial
Attractiveness
Market Size
• ~$13.9 B market in ’11
Global Epidemiology
• ~290 M prevalence ‘10
• ~2.1% CAGR ‘10-’15
Market Expansion
• Significant opportunity
to penetrate globally,
e.g. DPP-IVs and GLP-1s
Generic Penetration
• ~70% TRx in US ‘10
• US/EU LoEs through ’15
- Actos (10/12)
• This creates a significant
opportunity for the DDP-
IVs absent Actos
marketing
- Actos safety concerns
put payors in check
Competitive Launches
• 13 Ph. III /US Reg. assets
• Dapagliflozin complete
response creates
opportunity for DPP-IVs
Likelihood of
Technical Success
Etiology
• Improved understanding
of complex physiology
Historic Phase III Failures
• Taspoglutide (Roche)
• Dutogliptin (Forest)
- Terminated
Clinical Challenges
• Improved HbA1c is
closely tied to
increased cases of
hypoglycemia
Differentiation vs. Existing
Therapies
• Syncria vs. Victoza in
its first phase III trial
Target Patient
Populations
• Need to target patients
with lower baseline
HbA1c that are better
controlled
Regulatory
Environment
Clinical Unmet Need
• Significant interest in
targeting co-morbidities
such as weight loss and
CV disease
Historical Precedents
• Intense focus on long-
term safety and CV risks
post Avandia
• Approval delays
resulting in new, longer
safety studies to satisfy
FDA concerns (e.g.,
Galvus, Bydureon,
Dapagliflozin)
• Challenging to show
significant and durable
efficacy improvements
Advocacy
• Highly active advocacy
but less involved
patient population
9

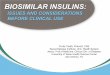
25.6 35.2 52.8 64.2 8.9
11.7
204.3
315.5
291.6
426.6
0
100
200
300
400
500
600
2010 2030
Sources: IDF Diabetes Atlas, fifth edition, 2011, International Diabetes Federations; American Diabetes Association, Practice guideline for the
treatment of Type II Diabetes (2008)
Notes: Global incidence and prevalence estimates exclude undiagnosed Type II Diabetes
Global Type II Diabetes prevalence was ~290M in ‘10, with an incidence of ~12.9M; Prevalence
is forecast to grow by ~2.1% to ~536M in ’30; US ’10 prevalence was ~25.6M in ‘10, with
incidence of ~1.9M; Obesity and aging are primary risk factors.
Moderate
Type II Diabetes Global Prevalence (M) Type II Diabetes US Prevalence by Patient Segment (M)
5.2 7.1
13.4
18.5
7.0
9.6 25.6
35.2
0
10
20
30
40
2010 2030
CAGR
(‘11-’30)
Mild:
1.5%
Severe:
Epidemiologic Studies: Solid bars Lumleian Estimate: Hashed bars
2010 Type II Diabetes Global Incidence (M)
Total=12.9M
• Weight: Obesity is the dominant risk factor with BMI over 30
• Age: Risk doubles every 5 years after the age of 45
• HDL cholesterol level: lower than 35 mg/dl will double the risk
of diabetes
• Blood pressure: Greater than or equal to 140/90 mmHg
• Genetics: Risk significant increase with a Type II Diabetes family
history
- Strong correlation with many metabolism related genes
• Sedentary lifestyle: Exercising fewer than three times a week
• Race: Diabetes occurs more often in Hispanic/Latino
Americans, African-Americans, Native Americans, Asian-
Americans, Pacific Islanders, and Alaska natives
• Pregnancy: Women who have had a baby weighing nine
pounds or more at birth have higher risk of Type II Diabetes
Primary Risk Factors
EU:
1.6%
JP
RW:
CAGR
(’11-’30)
2.1%
US:
1.0%
1.3%
2.3%
WW:
1.2%
Moder
ate:
2.0%
Secondary Risk Factors
1.9 2.1
0.3
8.6
0.0
1.5
3.0
4.5
6.0
7.5
9.0
10.5
US EU JP RW
14

Diagnosis:
Treatment:
First line:
Second line:
Third line:
Screening and Diagnosis (Current)
• Screening is based on blood tests of glycated hemoglobin (HbA1c)
level, a reading of greater than 6.5% is indicative of Type II
Diabetes
• Frequent HbA1c tests, in a fasting state, are used as a diagnostic
to evaluate disease control, progression and severity
Treatment (Current)
• Existing treatments provide symptomatic relief by improving
Insulin function and sensitivity
• First line: Metformin, Glitazone and Sulfonylurea are the first line
choices for moderate diabetic patients - Biguanides improve hyperglycemia primarily by suppressing glucose
production in the liver, e.g. Glucophage (Metformin)
- Glitazones activate PPARγ to increase Insulin sensitivity, e.g. Avandia
(Rosiglitazone), Actos (Pioglitazone)
- Sulfonylureas lower blood sugar by stimulating the release of Insulin
from pancreatic beta cells and by inducing increased activity of
intracellular Insulin receptors, e.g. Amaryl (Glimepiride), Prandin
(Repaglinide)
• Second line: DPP-IV Inhibitors and GLP-1 Agonists are used as
second line agents for severe diabetic patients and moderate
patients; DPP-IVs work by increasing the secretion of Insulin and
suppress the release of glucagon in the pancreas - DPP-IV Inhibitors: Januvia (Sitagliptin), Onglyza (Saxagliptin), Tradjenta
(Linagliptin), Galvus (Vildagliptin) in EU and Nesina (Alogliptin) in Japan
- GLP-1 Agonists: Byetta (Exenatide), Bydureon (Exenatide ER),Victoza
(Liraglutide)
• Third line: Insulin is used for severe diabetic patients either as
mono therapy or in combination with orals or GLP-1 Agonists
• Prognosis (Current) - Type II Diabetes is a life-long chronic disease
- Improper management leads to complications including non-traumatic
blindness and kidney failure
Mild 100<FPG<125
Severe FPG>300
Moderate 126<FPG<300
Biguanides Glitazones
Sulfonylureas
Initiate
DPP-IV Inhibitors
GLP-1 Agonists
Add /
Switch
HbA1c >6.5%
Sources: American Diabetes Association, Practice guideline for the treatment of Type II Diabetes (2008)
Treatment selection is guided by a number of factors; Standard of care is a step-wise treatment
approach, using a variety of therapeutic options; The clinical focus is primarily on getting patient blood glucose (e.g. HbA1c) to goal.
Insulin +/-
Oral anti-
diabetics
Diet control
Exercises
Disease Progression
15

Type II Diabetes Pipeline: Current (N=78)
Mechanism
of Action
US
Reg./Phase
III
(N=13)
Phase II
(N=39)
Phase I
(N=24)
Insulin Release
Promoters
DPP-IV Inhibitors 2 10
GLP-1 Agonists 4 3 4
Glucose Metabolism
Targeting MoAs
Glucokinase
Activators 3 1
PPAR Modulators 1 5 1
SIRT-1 Activators 2
Others 4 3
Immune System
Targeting MoAs
IL-1 Inhibitors 3 2
NF-kB Inhibitors 1 1
Others 1 1
Glucose Uptake
Targeting MoAs
SGLT2 Inhibitors 4 3 2
SGLT1 Inhibitors 1
Others 1 5 10
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations, pipeline
presentations, analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; CenterWatch
Insulin Release Promoters (e.g. DPP-IV Inhibitors and GLP-1 Agonists) dominate the
industry’s late stage pipeline; Glucose Metabolism Targeting MoAs and Glucose Uptake
Targeting MoAs are also being pursued.
Type II Diabetes Pipeline: Recent History
• Multiple MoAs are in the clinic, including: - DPP-IV Inhibitors
- GLP-1 Agonists
- Glucokinase Activators
- IL-1 and NF-kB Inhibitors
• In recent FDA reviews and advisory panels, safety
has received notable emphasis
• Risk vs. benefit concerns have stymied multiple
submissions: - Nesina (Takeda)
- Galvus (NVS)
- Bydureon (Amylin), approved 01/12
- Dapagliflozin (BMS), complete response letter 01/12
Type II Diabetes Pipeline: Upcoming Catalysts
• Nesina/Liovel (Takeda) PDUFA (03/12)
• Lyxumia (SNY/Zealand) - FDA NDA filing, Q2 ’12
- Filed for approval with EMA (11/11)
• Syncria (GSK/HGS) - Top line phase III results (US trials), H2 ’12
• Dulaglutide (BI/LLY) - The AWARD trial reads-out initial Phase III
data in 2H ‘12
26

Source: May M, Novo awaits green light for diabetes drug, Nature Biotechnology, 27, 682-687, (2009)
Nesina, a DPP-IV Inhibitor under FDA review, hopes to compete with three marketed agents
based on a comparable risk-benefit profile; A key differentiator is the Liovel formulation
combining Alogliptin and Pioglitazone; Actos bladder cancer concerns are a red flag.
Physiology • DPP-IV is an enzyme expressed by most of cell types
that increases blood glucose and decreases Insulin
secretion through degradation of GLP-1 - In Type II diabetics, over expression of DPP-IV disrupts
GLP-1 increasing blood glucose level
Hypothesized
Mechanism
• Inhibits DPP-IV function to protect GLP-1 and increase
Insulin secretion - Nesina, now under FDA regulatory review, shows a
comparable efficacy and safety profile vs. marketed
products
- Pioglitazone safety concerns are a red flag for Liovel, and
the FDA issued a warning for Actos in July ‘11; Use has
been suspended in some European countries, e.g. France
and Germany
- Adverse effects, including nasopharyngitis (the common
cold), headache, nausea, hypersensitivity and skin
reactions, have been observed in clinical studies
• In particular skin lesions with blistering observed in
nonhuman primate toxicology were a primary concern
for the FDA in issuing Galvus (NVS) a complete response
US Reg. / Phase III • Nesina / Liovel (Takeda)
Phase II • SYR-472 (Takeda) • PF-4971729 (PFE) • MK-3102 (MRK) • GRC8200 (Glenmark) • Carmegliptin (Roche) • KRP-104 (ActivX) • Teneligliptin (Mitsubishi Tanabe) • Gemigliptin (LG Life Sciences) • SK-0403 (Sanwa Kagaku) • MK-0431E (MRK)
- Sitagliptin/Atorvastatin
Pipeline
29

Clinical Results (Phase III)
Efficacy: • Significant mean change from baseline HbA1c levels (p<0.001), for both 12.5 mg and 25 mg Nesina doses
vs. placebo
• HbA1c was reduced by more than 7% in 47% (12.5 mg) and 44% (25 mg) patients treated with Nesina
• Reduced effectiveness at 12.5mg and 25mg QD is modest and in line with the class
Safety: • In all mono therapy and combination Phase III studies, Nesina was well tolerated, however CV data did not met FDA’s
guideline, largely due to short Phase III trial length
Lumleian Commentary: • Takeda reached agreement with FDA on the design of a CV outcomes study which will enroll 5,400 patients
• Takeda is also pursuing Liovel (a fixed-dose Alogliptin/Pioglitazone combination), that was recently approved in Japan
• We are optimistic regarding approval as mono therapy in April, but are circumspect regarding combination approval
Phase II Program (Completed) Phase III Program (Completed)
Patient Segment: • Moderate Type II Diabetes • Moderate Type II Diabetes
Studies:
(Target Enrollment)
• Single Phase II (N=265) • Two Phase III studies (N=329 and 480) and
EXAMINE study of CV events ongoing (N=5,400)
Comparator: • Placebo • Placebo
Dosing: • 6.25; 12.5; 25; 50; 100 mg QD • 6.25; 12.5; 25 mg QD
Duration: • 12 weeks • 16 weeks (EXAMINE study 5 years)
Primary End-Points: • Efficacy: Change from baseline in HbA1c • Efficacy: Change from baseline in HbA1c
• CV events: Time from randomization to the occurrence
of the primary major adverse cardiac events
Secondary End-Points: • Efficacy: Change from baseline in HbA1c
• Efficacy: Change from baseline in fasting plasma glucose
• Efficacy: Change from baseline in HbA1c
• Efficacy: Change from baseline in fasting plasma glucose
• Efficacy: Change from baseline in body weight
Sources: Company press releases; 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; FDA.gov
EXAMINE study (CV safety) and recent bladder cancer concerns with Actos will likely be focal
points at Nesina and Liovel’s PDUFA (April 25th); We are optimistic regarding approval as mono
therapy, but are circumspect regarding combination approval.
30

Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
Notes: Branded sales excludes generic revenues and Insulins; Pipeline includes: Aleglitazar, Canagliflozin, Lyxumia, and Nesina; *Includes pipeline
revenues
Global ‘11 brand revenue for non-Insulin drugs was ~$13.9B and is forecast to grow by ~3.1%
annually through ‘15 driven by strong growth outside of the United States and new product
launches, including follow on DPP-IV inhibitors and once weekly GLP-1 Agonists.
$10.4 $12.1
$13.9 $15.1 $14.7
$15.7 $16.6
$0.0
$10.0
$20.0
09A 10A 11A 12F 13F 14F 15F
’11 Revenue
($B)
’10–’11A
CAGR
’11-’12F
CAGR
’12–’15F
CAGR
Global &
Pipeline $13.9 15.7% 8.5% 3.1%
US* $8.0 10.6% -0.4% -2.2%
EU* $3.2 52.6% 20.7% 8.7%
JP* $1.4 -5.1% 19.8% 7.9%
RW* $1.3 6.9% 21.1% 8.9%
EU
US
JP
RW
Type II Diabetes Global Brand Revenue ($B)
Updated: 02/15/12
Actual: Solid bars Consensus Wall Street Forecast: Hashed bars
Global
Pipeline
Baseline Epidemiological Growth (Prevalence)
• US: 1.6% • EU: 1.0% • JP: 1.3%
Recent and Anticipated New Product Launches - Global
• Novo Nordisk: Victoza (03/11)
• Eli Lilly/Boerhinger Ingelheim: Tradjenta (08/11)
• Takeda: Nesina (’12)
• Sanofi/Zealand: Lyxumia (‘13)
• Roche: Aleglitazar (’13)
Recent and Anticipated New Product Launches - Japan
• Takeda: Liovel, Alogliptin and Pioglitazone (09/11)
• Takeda: Nesina (04/10)
• JNJ/Mitsubishi Tanabe: Canagliflozin (’13)
Recent and Anticipated Line Extensions
• Merck: Janumet XR, Sitagliptin and Metformin QD (02/12)
• Amylin: Bydureon, Exenatide ER (01/12)
• Eli Lilly/Boerhinger: Jentadueto, Tradjenta and Metformin (01/12)
• Merck: Juvisync, Sitagliptin and Simvastatin (10/11)
Recent and Anticipated Loss of Exclusivity
• US: Avandia (09/11), Actos (08/12)
45

Sources: Consensus estimates based on publicly available equity research forecasts that have been updated in the past 12 months (since 1/1/11);
Consensus estimate is the ‘straight line’ average with each bank’s forecast weighted equally
Notes: These forecasts are not representative of Lumleian’s viewpoint; Ad-hoc Lumleian develops its own forecasts
for clients based on its proprietary analytics and research; Pipeline includes: Aleglitazar, Canagliflozin, Lyxumia, and Nesina
Global Pipeline Assets Wall Street Consensus Forecast ($B)
Wall Street consensus estimates forecast new products will increase the ‘15 global market by
~$1.5B, driven largely by anticipated launches for Takeda’s Nesina, a DPP-IV Inhibitor, outside
Japan, Roche’s NF-kB Modulator Aleglitazar, and Sanofi’s GLP-1 Agonist Lyxumia.
Wall Street Consensus Forecast: Hashed bars
$0.2
$0.7
$1.1
$1.5
$0.0
$1.0
$2.0
09A 10A 11A/F 12F 13F 14F 15F
Canagliflozin (JNJ)
Aleglitazar (Roche)
Lyxumia (SNY)
Nesina (Takeda)
Updated: 02/15/12
Nota Bene: Dapagliflozin forecast omitted, premised
on recent FDA complete response
Global Aleglitazar (Roche)
Equity Research Forecasts ($B)
Global Nesina (Takeda)
Equity Research Forecasts ($B)
Global Lyxumia (SNY)
Equity Research Forecasts ($B)
$0.0
$0.5
$1.0
12F 13F 14F 15F
Thousa
nds
0
0.5
1
12F 13F 14F 15F
Thousa
nds
0
0.3
0.6
12F 13F 14F 15F
Thousa
nds
15F Consensus: $0.3B 15F Consensus: $0.8B 15F Consensus: $0.3B
50

Others
DPP-4
GLP-1
Glitazone
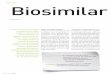
Sources: SDI (IMS) Promotion Audits, Kantar Media Research 2010 - 2011
Note: Insulins are excluded; Healthcare Professional (HCP) spend includes marketing to physicians, nurse practitioners, physician assistants through marketing
& event promotions, journals, and online promotions; Direct to Consumer (DTC) includes marketing channels in television, radio, newspapers, magazines,
outdoor advertisements, and internet; 3MR (3 months rolling) compares avg. monthly spend for the 3 months 10/11-8/11 vs. the 3 months 7/11-5/11
In the three months ending October ‘11 total promotional spend grew ~14.9%; Healthcare
professional spend grew ~11.6% with DPP-IV Inhibitors accounting for ~60% of spend; Direct to
Consumer spending grew in October with Januvia launching the first campaign since Q1 ‘11.
$0
$50
$100
N D J F M A M J J A S O
Millions
HCP DTC
$0
$50
$100
N D J F M A M J J A S O
Others Glitazone
GLP-1 DPP-IV
$0
$15
$30
N D J F M A M J J A S O
Others
Glitazones
GLP-1
DPP-IV
• ~$105.3M was spent on total promotion in October, a ~14.7%
increase (3 month rolling), with ~86% of the expenditure
focused on health care professionals
– DDP-IV Inhibitors accounted for ~61% of HCP spend, and the average
brand (Januvia, Onglyza, and Tradjenta) spent ~$18.5M in October
• Class DTP spending rose in parallel with Tradjenta approval (08/11)
– GLP-1 Agonists (Byetta, Victoza) spent on average ~$10.2M in October
• After two quarters of inactivity, Januvia launched a DTC
campaign in September, spending ~$13M in October
- Onglyza did not pursue DTC advertising, nor did either of the two
GLP-1 Agonists
$105.3M
(10/11)
$91.6M
(10/11)
Exelon
$13.8M
(10/11)
2010 2011
Total Promotional Spend ($M)
Healthcare Professional Spend ($M) Direct to Consumer Spend ($M)
2010 2011
2010 2011
Share of
Wallet CAGR
(Oct-11) (3MR)
HCP 86.9% 11.6%
DTC 13.1% 84.1%
Share of
Voice CAGR
(Oct-11) (3MR)
DPP-IV 60.8% 12.2%
GLP-1 22.3% -4.5%
Glitazones 10.0% 33.9%
Others 5.7% 17.2%
Share of
Voice CAGR
(Oct-11) (3MR)
DPP-IV 95.1% 165.5%
GLP-1 3.0% -18.8%
Glitazones 0.1%
Others 1.9%
14.9% (3MR)
CAGR
11.6% (3MR) CAGR 84.1% (3MR) CAGR
Updated: 02/15/12
54

Table of Acronyms (1 of 2)
11A 2011 Actual
12F 2012 Forecast
2H Second Half
3MR Three Months Rolling
ABT Abbott
ANLG-B Analog-B
AMG Amgen
AMPK Adenosine Monophosphate-Activated
Protein Kinase
AZN AstraZeneca
B Billions
BI Boerhinger-Ingelheim
BID Bis in Die (Twice daily)
BMS Bristol-Myers Squibb
CAGR Compound Annual Growth Rate
CCL2 Chemokine (C-C Motif) Ligand 2
CCR2 chemokine (C-C Motif) Receptor 2
CHF Congestive Heart Failure
CMS Centers for Medicare & Medicaid
Services
CV Cardiovascular
dL Deciliter
DPP-IV Dipeptidyl peptidase-4
DTC Direct to Consumer
EU European Union
FDA US Food and Drug Administration
FPG Fasting Plasma Glucose
GI Gastrointestinal
GLP-1 Glucagon-Like Peptide-1
GPR119 G Protein-Coupled Receptor 119
GSK GlaxoSmithKline
HbA1c Glycosylated Hemoglobin
HCP Health Care Professional
HDL High-Density Lipoprotein
IDF International Diabetes Federation
IgG2 Immunoglobulin G 2
IL-1 Interleukin-1
JNJ Johnson and Johnson
JP Japan
kg Kilogram
LLY Eli Lilly
LoE Loss of Exclusivity
LT Long Term
M Millions
mg Milligrams
µg Microgram
mmHG millimeters of Mercury
MoA Mechanism of Action
MRK Merck
MTD Month to Date
N Number
NDA New Drug Application
NF-kB Nuclear factor Kappa-Light-Chain-
Enhancer of Activated B Cells
NOVO Novo Nordisk
NVS Novartis
PCP Primary Care Physician
PFE Pfizer
Ph. Phase
Ph.D. Doctor of Philosophy
PPAR Peroxisome Proliferator-Activated
Receptors
PPARγ Peroxisome Proliferator-Activated
Receptors Gamma
PPG Postprandial Plasma Glucose
Q1 First Quarter
Q2 Second Quarter
Q3 Third Quarter
Q4 Fourth Quarter
QD Quaque Die (Once Daily)
QTD Quarter To Date
58

Table of Acronyms (2 of 2)
Reg. Reglatory
RN Registered Nurse
ROCH Roche
RW Rest of World
Rx Prescription
SGLT Sodium-Dependent Glucose
Cotransporter
SIRT Sirtuin (Silent Mating Type Information
Regulation 2 Homolog)
SNY Sanofi-Aventis
SOC Standard of Care
SS Statistically Significant
SSD Statistically Significant Difference
Type II
Diabetes Type II Diabetes
TRx Total Prescriptions
US United States
WW World Wide
Yrs. Years
YTD Year to date
59

• Frank Deane, Ph.D. is a Director of Decision Science and Founder of Lumleian. Frank has over ten years experience
working with life science companies and concurrently holds an appointment in the department of strategy at the
Carroll School of Management, Boston College, where he teaches ‘Strategic Issues in Pharma and Bio-Tech,’ to MBA
students. Prior to founding Lumleian, Frank was a director with Leerink Swann and a case team leader with Bain,
where he gained substantial operational experience growing and operating a diverse set of businesses. Frank
entered consulting after spending three years in the bio-pharmaceutical industry with Eli Lilly, supporting portfolio
optimization and business unit strategic planning. He began his career, as a quantitative risk analyst working at
BlackRock. Frank earned a Ph.D. in econometrics from the Krannert School of Management at Purdue University,
where his dissertation focused on applying game theory and statistical modeling to optimize pharmaceutical sales
and marketing resources. Frank has a bachelor of arts in economics from Princeton University.
As a leadership team, we designed Lumleian’s business model based on our collective
experience in: academic R&D, bio-pharmaceutical industry, equity research and strategy
consulting …
• Mark Hochstetler, MBA is a Director of Decision Science at Lumleian. Mark has over ten years experience working
with life science companies. Prior to joining Lumleian, Mark served as the CFO at OPK Biotech, which focuses on
developing oxygen therapeutics for the treatment of anemia, ischemia, and trauma. Before segueing to industry,
Mark spent 5 years as a strategy consultant and equity research analyst at Leerink Swann, where he covered:
Array, Arqule, Ariad, Celgene, Chelsea, Cougar, Cubist, Genentech, GTx, Hana, Idenix, InterMune, Kosan,
Millennium, MGI Pharma, Onyx, Poniard and Vertex. Mark earned an MBA from Duke University’s Fuqua School of
Business with a concentration in health sector management. Mark has a bachelor of arts in political science from
Stanford University.
• Sarah Haigh Molina, Ph.D. is a Manager of Decision Science at Lumleian, where she leads the Academia and Non-
profit practice. Sarah has over ten years experience working and researching in the life sciences. Prior to joining
Lumleian, Sarah was an Assistant Professor of Medicine at Boston University School of Medicine where she served
as the Director of High-throughput Screening. Before returning to academia, Sarah was US Operations Manager at
Molecular Cytomics. Sarah earned a Ph.D. in biology from York University, an MBA from Boston University with a
concentration in entrepreneurship, and a bachelors of science in biochemistry from Dundee University.
60

… Having lived the client experience, we know quality is paramount, and pioneered our
approach with quality and process efficiency as dual mantras.
• Jean Kung, M.S.E, MBA as Manager of Process Efficiency and Quality Control oversees day-to-day operations and
finances at Lumleian and has over five years experience working in the life sciences. Jean designed the process
by which Lumleian efficiently and effectively creates and quarterly updates its disease state primers and serves as
the final point of quality control. Prior to joining Lumleian, Jean served as a contract project manager to various
life science clients. Before entrepreneurship, Jean was a clinical research associate at Health Policy Associates
and a researcher at the Harris Orthopedic Biomaterials and Biomechanics Laboratory, Massachusetts General
Hospital. Jean earned a masters of science in biological engineering from Cornell University and an MBA in the
Health Sector Management Program from Boston University with a concentration in operations and technology
management. Jean has a bachelor of science in biological engineering, also from Cornell University.
• Morgen Caroll, MBA as Manager of the Customer Experience at Lumleian, aspires to provide Lumleian's clients with
superior care and service based on their particular needs. Morgen brings over five years life science experience
and has a background in Marketing, Sales, and Public Relations. Prior to joining Lumleian, Morgen worked at
GlaxoSmithKline, with responsibility for the company’s flagship cardiology and endocrinology products. At
GlaxoSmithKline, Morgen was a primary care and specialty care sales representative while serving as a liaison
between product management teams and field sales. As a representative, Morgen consistently ranked in the top
10% of GSK’s sales force, despite working in an inner city territory with significant access challenges. Prior to
entering the life sciences Morgen worked on the sales and marketing staff at Philadelphia Magazine and Food &
Wine Magazine. Morgen earned an MBA from the Villanova School of Business with a concentration in marketing,
and a bachelor of arts in English from Gettysburg College.
• Qingwei Sun, M.S.E, MPH as a Decision Science Analyst oversees secondary data collection, synthesis and analysis
and designed analytical methodologies fundamental to Lumleian’s knowledge management platform. KM
database. Using meta-analysis method, he aggregates the clinical and commercial data required to generate
Lumleian’s disease state primers. His work has wide application in product development, portfolio management,
and investment strategy for both large pharmaceutical companies and emerging bio-techs. Qingwei, who is fluent
in Chinese and Japanese, leads our work with Asian clients. Qingwei joined Lumleian after obtaining a Master of
Science degree from Harvard School of Public Health. He earned both Bachelor and Master of Engineering degrees
from Kyoto University, Japan, concentrating in materials science.
61